Embed Size (px)
Citation preview
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2016
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1205
Airway management in anaesthesiacare
– professional and patient perspectives
KATI KNUDSEN
ISSN 1651-6206ISBN 978-91-554-9534-3urn:nbn:se:uu:diva-281905

Dissertation presented at Uppsala University to be publicly examined in Brömssalen, Gävlesjukhus, Lasaretsleden 1, Gävle, Friday, 20 May 2016 at 13:00 for the degree of Doctorof Philosophy (Faculty of Medicine). The examination will be conducted in Swedish.Faculty examiner: Ingegerd Bergbom (Institutionen för vårdvetenskap och hälsa, GöteborgsUniversitet).
AbstractKnudsen, K. 2016. Airway management in anaesthesia care. – professional and patientperspectives. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty ofMedicine 1205. 56 pp. Uppsala: Acta Universitatis Upsaliensis. ISBN 978-91-554-9534-3.
Background: Careful airway management, including tracheal intubation, is important whenperforming anaesthesia in order to achieve safe tracheal intubation. Aim: To study airwaymanagement in anaesthesia care from both the professional and patient perspectives. Methods:11 RNAs performed three airway tests in 87 patients, monitored in a study-specificquestionnaire. The tests usefulness for predicting an easy intubation was analysed (Study I).68 of 74 anaesthesia departments in Sweden answered a self-reported questionnaire aboutthe presence of airway guidelines (Study II). 20 anaesthesiologists were interviewed; aphenomenographic analysis was performed to describe how anaesthesiologists' understandalgorithms for management of the difficult airway (Study III). 13 patients were interviewed;content analysis was performed to describe patients' experiences of being awake fiberopticintubated (Study IV). Results: The Mallampati classification is a good screening test forpredicting easy intubation and intubation can be safely performed by RNAs (Study I). Thepresence of airway guidelines in Swedish anaesthesia departments is poorly implemented (StudyII). Algorithms can be understood as law-like rules, a succinct plan to follow in difficult airwaysituations, an action plan kept in the back of one's mind while creating flexible and versatilepersonal algorithms, or as consensus guidelines based on expert opinion in order to be followedin clinical practice (Study III). One theme emerged describing experiences of being awakeintubated; feelings of being in a vulnerable situation but cared for in safe hands, described infive categories: a need for tailored information, distress and fear of the intubation, acceptanceand trust of the staff's competence, professional caring and support, and no hesitation about newawake intubation (Study IV). Conclusions: The Mallampati classification is a good screeningtest for predicting easy intubation, when the airway assessment is performed in a structuredmanner by RNAs. The presence of airway guidelines in Swedish anaesthesia departments waspoorly implemented and should receive higher priority. Algorithms need to be simple and easyto follow and based on the best available scientific evidence. Tailored information about what toexpect, ensuring eye contact, and giving breathing instructions during the procedure may reducepatients' feeling distress.
Keywords: Airway management, algorithm, awake intubation, professional and patientperspective
Kati Knudsen, Department of Public Health and Caring Sciences, Box 564, UppsalaUniversity, SE-75122 Uppsala, Sweden.
© Kati Knudsen 2016
ISSN 1651-6206ISBN 978-91-554-9534-3urn:nbn:se:uu:diva-281905 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-281905)

To my family Bent & Olivia

4
5
List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Knudsen, K., Högman, M., Larsson, A., Nilsson, U. The best
method to predict easy intubation: a quasi-experimental pilot study. J Perianesth Nurs. 2014; 29: 292-297.
II Knudsen, K., Pöder, U., Högman, M., Larsson, A., Nilsson, U. A nationwide postal questionnaire survey: The presence of air-way guidelines in anaesthesia department in Sweden. BMC Anesthesiol. 2014; 14:25. Epub 2014 Apr 7.
III Knudsen, K., Pöder, U., Nilsson, U., Högman, M., Larsson A., Larsson J. Anaesthesiologists’ understanding of algorithms for management of the difficult airway – a qualitative interview study. Submitted.
IV Knudsen, K., Nilsson, U., Högman, M., Pöder, U. Awake intu-bation creates feelings of being in a vulnerable situation but cared for in safe hands. Submitted.
Reprints were made with permission from the respective publishers.

6
7
Contents
Preface .......................................................................................................... 11
Introduction ................................................................................................... 13 Preoperative airway assessment ............................................................... 14 Managing a difficult airway ..................................................................... 17
Airway guidelines and algorithms ....................................................... 17 Airway management from a professional perspective ............................. 18 Anaesthesia and intubation from a patient perspective ............................ 19
Rationale for the thesis .................................................................................. 21
Aims .............................................................................................................. 22 Study I ...................................................................................................... 22 Study II ..................................................................................................... 22 Study III ................................................................................................... 22 Study IV ................................................................................................... 22
Methods ........................................................................................................ 23 Design ...................................................................................................... 23 Sample and setting ................................................................................... 24
Study I .................................................................................................. 24 Study II ................................................................................................ 24 Study III ............................................................................................... 24 Study IV ............................................................................................... 24
Procedures ................................................................................................ 25 Study I .................................................................................................. 25 Study II ................................................................................................ 25 Study III ............................................................................................... 25 Study IV ............................................................................................... 25
Data collection .......................................................................................... 26 Study I .................................................................................................. 26 Study II ................................................................................................ 27 Studies III and IV ................................................................................ 27
Data analysis ............................................................................................ 28 Study I .................................................................................................. 28 Study II ................................................................................................ 29 Study III ............................................................................................... 29

8
Study IV ............................................................................................... 30
Ethical considerations ................................................................................... 31
Results ........................................................................................................... 33 Study I ...................................................................................................... 33 Study II ..................................................................................................... 34 Study III ................................................................................................... 35 Study IV ................................................................................................... 35
Discussion ..................................................................................................... 37 Summary of findings ................................................................................ 37 Airway management and guidelines from a professional perspective ..... 37 Anaesthesia and intubation from a patient perspective ............................ 41 Methodological considerations................................................................. 42
Clinical implications ..................................................................................... 45
Conclusions ................................................................................................... 46
Svensk sammanfattning (Swedish summary) ............................................... 47
Acknowledgements ....................................................................................... 50
References ..................................................................................................... 51
9
Abbreviations
ASA
American Society of Anesthesiologists
RNA Registered Nurse Anaesthetist SFAI Svensk förening för Anestesi och
Intensivvård WHO World Health Organisation DAS Difficult Airway Society

11
Preface
During my 20 years of working experience as a registered nurse anaesthetist (RNA) in anaesthesiology, I have observed the different ways a patient’s airway can be assessed before undergoing anaesthesia. I especially remem-ber a situation in which an overweight middle-aged patient went into the operating room for emergency abdominal surgery. My intuition told me that he would probably be difficult to ventilate and intubate due to his beard, obesity, and short neck. Despite being at high risk for difficult intubation I felt that we did not do anything to prepare him or ourselves for a difficult airway, such as shaving his beard in advance or having an alternative plan available on how to secure the airway. At that point I began to think of how we could prepare patients and ourselves when performing endotracheal intu-bations so we do not jeopardise patient safety. The inability to secure a free airway is not only an emotionally stressful situation for the patients, but challenging for the anaesthesia professional. The present studies will help us gain a deeper understanding and new knowledge about how these situations could be experienced, from both professional and patient perspectives.


13
Introduction
Careful airway management, including endotracheal intubation, is important when performing anaesthesia in order to achieve safe endotracheal intuba-tion [1]. Endotracheal intubation is usually performed after the induction of general anaesthesia when the patients are asleep. When a difficult airway is expected, fiberoptic intubation is the recommended option to secure the air-way and is performed before the induction of general anaesthesia when the patient is still awake [2]. Depending on whether the intubation is performed in an asleep or awake state, the patient experiences varying degrees of anxi-ety when undergoing intubation [3]. In general, women are more anxious than men [4], and patients who have experienced awake fiberoptic intubation report more discomfort and suffocation than patients who have undergone traditional endotracheal intubation [5]. To alleviate feelings of anxiety, it is important that patients are well-informed about the procedures, which in-creases their feelings of calm and security when undergoing anaesthesia. Psychologically preparing the patient for an awake intubation is essential, as this can be highly discomforting for the patient [6].
In Sweden, with a population of more than nine million people, approxi-mately 500 000 general anaesthesia procedures are performed annually [7]. There is wide variation in estimations of the incidence of difficult intubation and depends on differences in study design, assessment tools [8], and how difficult airways are defined [9]. On the basis of a report written by a re-searcher in the US, difficult face mask ventilation combined with difficult intubation occurs in approximately 1 of every 250 cases annually [10], whereas in a review by Cook & MacDougall-Davis [11], the incidence of difficult intubation was estimated to be approximately 1 in 2000 in the elec-tive setting and approximately 1 in 300 during rapid sequence induction. However, in the literature it is unclear how many of those anaesthetic proce-dures are performed in the awake state.

14
Preoperative airway assessment Preoperative airway assessment is important when planning anaesthesia in order to achieve safe endotracheal intubation [1]. Whether the intubation is performed in an anaesthetised or awake state, the patients should undergo preoperative airway assessment before inducing general anaesthesia. The purpose of this assessment is to psychologically preparing patients for anaes-thesia and to make anaesthesia professional aware of those patients who are likely to be easy or difficult to intubate. Studies have shown that pre-operative airway assessment before surgery helps identify patients at risk of difficult ventilation and intubation [12, 13], improving patient safety. Ac-cording to the fourth national audit project in the UK, the majority of airway problems occur during elective surgery in seemingly healthy patients [14]. Individual patient characteristics, such as the presence of a beard, short neck, limited mouth opening, poor dental status, male sex, increased Mallampati classification, and obesity, are associated with intubation difficulties [15, 16].
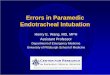
In 1983, Mallampati [17] developed a simple bedside test for assessing the patient’s airway before inducing anaesthesia. Using this test, adult pa-tients can be divided into four classes according to the individual anatomical structures observed in their mouth while they are sitting in an upright posi-tion with the mouth opened wide and the tongue hanging out without phona-tion. Figure 1 describes Mallampati classification I–IV.
Figure 1. Mallampati classification I–IV. Class I: soft palate, uvula, and faucial pillars can be seen. Class II: soft palate, faucial pillars, and portion of the uvula can be seen. Class III: soft palate and base of the uvula can be seen. Class IV: only the hard palate can be seen. "Illus-trated by O. Wall, University of Gävle"
The Mallampati test revealed a significant relationship between the ease of intubation and individual anatomical structures seen in the mouths of adult patients [17]. However, the test has been criticised as not being specific enough when used alone [18] due to variability from one person to another. For example, patients who were expected to have a difficult airway had an
Class I Class II Class III Class IV
15
easy intubation, and vice versa, when the test was used alone. Khan et al. [19] compared the Mallampati classification with the upper lip bite test, ster-nomental distance, thyromental distance, and interincisor distance in 309 patients. Nineteen patients were difficult to intubate and no significant dif-ference was found based on gender. However, significant differences were found between the Mallampati test and laryngeal view [19]. Other studies [20, 21] comparing the Mallampati test and the patient’s position (sitting and supine) have found that the Mallampati test in a supine position is a better predictor of difficult endotracheal intubation than the test in a sitting posi-tion. On the other hand, the Mallampati test with the patient in a sitting posi-tion is associated with a higher percentage of easy intubations compared to the supine position [20]. Therefore, Bindra et al. [20] recommended per-forming the Mallampati test in both the supine and sitting positions to obtain a better assessment.
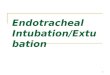
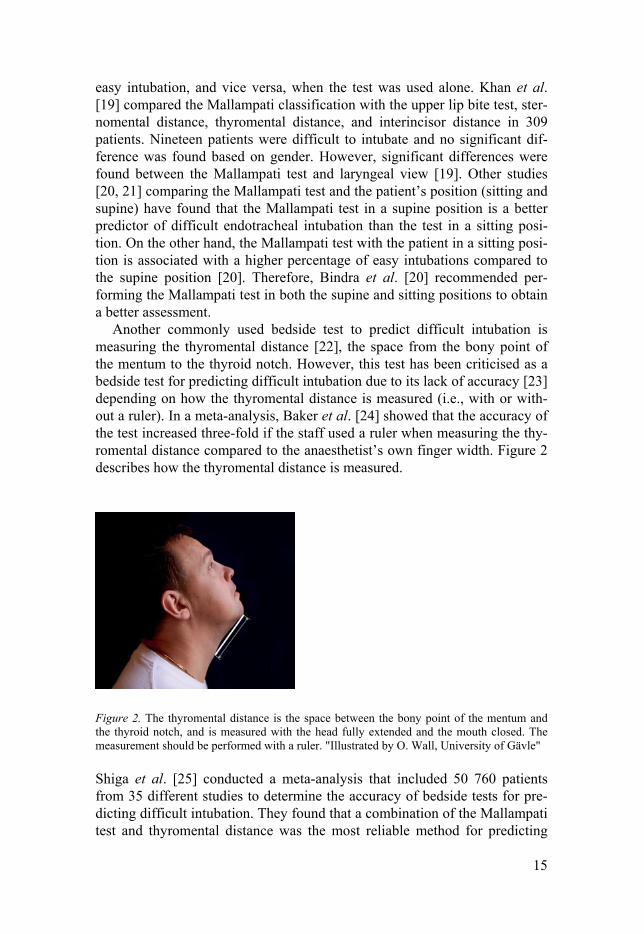
Another commonly used bedside test to predict difficult intubation is measuring the thyromental distance [22], the space from the bony point of the mentum to the thyroid notch. However, this test has been criticised as a bedside test for predicting difficult intubation due to its lack of accuracy [23] depending on how the thyromental distance is measured (i.e., with or with-out a ruler). In a meta-analysis, Baker et al. [24] showed that the accuracy of the test increased three-fold if the staff used a ruler when measuring the thy-romental distance compared to the anaesthetist’s own finger width. Figure 2 describes how the thyromental distance is measured.
Figure 2. The thyromental distance is the space between the bony point of the mentum and the thyroid notch, and is measured with the head fully extended and the mouth closed. The measurement should be performed with a ruler. "Illustrated by O. Wall, University of Gävle"
Shiga et al. [25] conducted a meta-analysis that included 50 760 patients from 35 different studies to determine the accuracy of bedside tests for pre-dicting difficult intubation. They found that a combination of the Mallampati test and thyromental distance was the most reliable method for predicting
16
difficult intubation. On the other hand, Rosenstock et al. [26] conducted a qualitative interview study to explore how anaesthesiologists manage an unanticipated difficult airway, finding that only five of 24 patients were ex-amined using more than two airway tests before endotracheal intubation, as recommended by the American Society of Anesthesiologists (ASA) guide-lines [1].
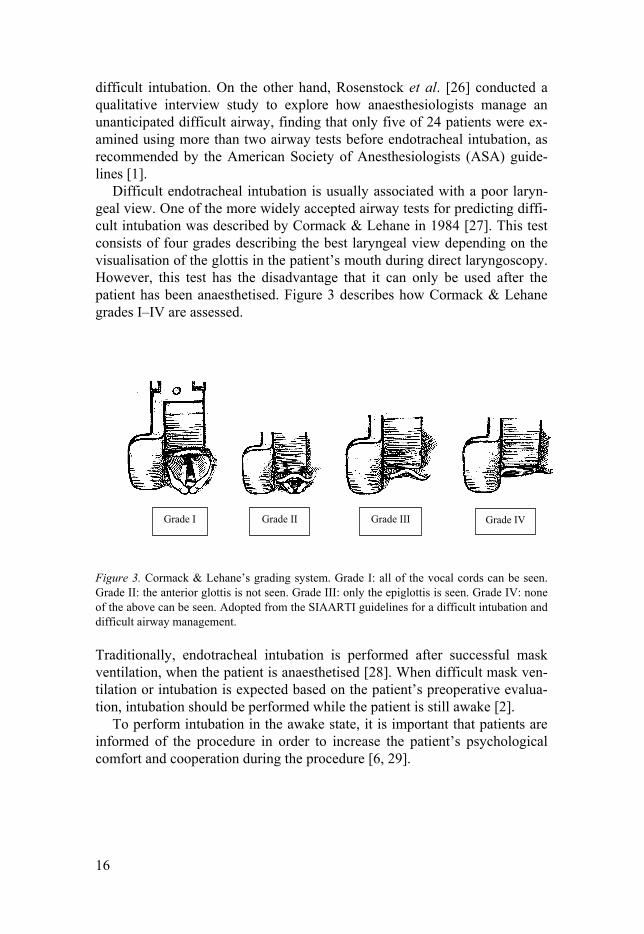
Difficult endotracheal intubation is usually associated with a poor laryn-geal view. One of the more widely accepted airway tests for predicting diffi-cult intubation was described by Cormack & Lehane in 1984 [27]. This test consists of four grades describing the best laryngeal view depending on the visualisation of the glottis in the patient’s mouth during direct laryngoscopy. However, this test has the disadvantage that it can only be used after the patient has been anaesthetised. Figure 3 describes how Cormack & Lehane grades I–IV are assessed.
Figure 3. Cormack & Lehane’s grading system. Grade I: all of the vocal cords can be seen. Grade II: the anterior glottis is not seen. Grade III: only the epiglottis is seen. Grade IV: none of the above can be seen. Adopted from the SIAARTI guidelines for a difficult intubation and difficult airway management.
Traditionally, endotracheal intubation is performed after successful mask ventilation, when the patient is anaesthetised [28]. When difficult mask ven-tilation or intubation is expected based on the patient’s preoperative evalua-tion, intubation should be performed while the patient is still awake [2].
To perform intubation in the awake state, it is important that patients are informed of the procedure in order to increase the patient’s psychological comfort and cooperation during the procedure [6, 29].
Grade I Grade II Grade III Grade IV

17
Managing a difficult airway Managing a difficult airway when inducing anaesthesia is one of the most challenging tasks for anaesthesia professionals. Failure to secure the airway, even for a few minutes, may increase the risk of hypoxic brain damage and harm the patients, causing stress for the professionals caring for them [1,14, 30]. When presented with a difficult airway in clinical practice, such as dur-ing an emergency, there is no time to think about what has gone wrong. In-stead, the airway must be prioritised and a plan B considered for securing the airway [1, 31]. Therefore, in such critical situations, anaesthesia profession-als must not only be technically skilled, but also have communicative, cogni-tive, and behavioural competence in making decisions [32, 33]. Furthermore, when a difficult airway is expected, there is a strong consensus among ex-perts that specific strategies can improve patient outcomes when performing anaesthesia [14].
Airway guidelines and algorithms In order to promote safer airway procedures, airway guidelines have been published to help anaesthesia professionals manage patient airways when they fail. One of the first published guidelines for the management of a diffi-cult airway was developed by the American Society of Anesthesologists (ASA) in 1993 [34] and updated in 2003 [35] and 2013 [1]. As a lack of consensus exists in the literature regarding the definition of a difficult air-way, the ASA [1] defined a difficult airway as:
“…the clinical situation in which the conventionally trained anesthesi-ologist experiences difficulty with face mask ventilation of the upper airway, difficulty with tracheal intubation, or both” (page 251, ASA 2013).
Since then, various forms of clinical guidelines and algorithms that describe procedures for managing a difficult airway have been published in Canada [31] and the UK [36], followed by the European [37] and Scandinavian countries [38]. Despite their purpose to enable safer procedures, there is an ongoing debate regarding their relevance and usefulness in clinical practice [39]. Regarding the differences between clinical guidelines and algorithms, guidelines are systematically developed recommendations in the form of standardised guidance that one ought to take into account when making deci-sions. According to the World Health Organisation (WHO) [40], clinical guidelines are defined as:
“…systematically developed evidence-based statements which should assist the anaesthesia personnel, recipients and other stakeholders to secure optimal treatment for all patients, regardless of by whom or where the pa-tients are treated” (page 2, WHO 2003).

18
International and national guidelines can be modified and local guidelines can be developed, but they cannot guarantee any specific outcomes and, therefore, following them is not absolutely required. However, clinical guidelines should summarise good practices and side steps from such proto-cols to benefit the individual patient should be encouraged [41]. The advan-tage of using guidelines in clinical practice is that they can remind anaesthe-sia professionals of problems that could occur in daily practice. Deciding to follow clinical guidelines may come down to the fact that these are standard regimens for the average patient and sometimes lack scientific evidence to support their recommendations [42].
In contrast, according to the ASA [1], an algorithm is defined as a form of decision tree that describes step by step how to safely manage difficult air-ways. The use of cognitive aids such as algorithms improves patient safety only if they are well-designed and accompanied by training [43]. Marshall & Mehra [44], who video-observed anaesthesia providers’ skills during a “can´t intubate can’t ventilate scenario”, found that a cognitive aid presented as algorithms improved the anaesthesia providers’ skills during the simula-tion.
Despite airway guidelines being developed and recommended to achieve safer airway procedures [1, 45], adherence to clinical guidelines and algo-rithms is generally described as poor [46] and being influenced by the anaes-thesia professionals’ individual experiences, beliefs, and attitudes when making decisions in clinical practice [47]. Even if the purpose of using algo-rithms is safer practice [1], there is no strong evidence of benefits for any specific guidelines for the management of a difficult airway; there is, how-ever, strong agreement that a pre-planned approach may lead to improved patient outcomes [1, 44].
Airway management from a professional perspective The anaesthesiologist has the primary responsibility of assessing the pa-tient’s airway prior to anaesthesia and planning for their anaesthetic proce-dure [37]. In Sweden, RNAs have a graduate diploma in specialist nursing in anaesthesia care, with or without a master’s degree [48]. The RNAs’ clinical work and education differ between European countries and the rest of the world [49]. In Sweden, RNAs are allowed to start, maintain, and end general anaesthesia in healthy patients (i.e., ASA physical status I-II) after prescrip-tion by an anaesthesiologist [48]. In contrast, in some states in the US [50], certified RNAs are allowed to independently administer anaesthesia to pa-tients without the supervision of anaesthesiologists and under their own au-thority [51].
The management of a difficult airway during anaesthesia is a challenging and stressful situation [52] that anaesthesia professionals may sometimes be
19
involved in during their clinical work. In daily practice, RNAs and anaesthe-siologists work closely as a team and have many overlapping skills that pro-vide safer care for the patient during their anaesthesia [53]. In Sweden, an-aesthesiologists are usually responsible for several operating rooms at the same time and serve as support for RNAs, who do much of the work around the patients during and after anaesthesia. The RNA is often the first person the patient meets when they arrive in the operating room. When the patient is in a state of unconsciousness or anaesthetised and cannot make their own voice or choices heard, the RNA is professionally responsible for their care, needs, and well-being. The RNAs act as the patients’ advocate to protect them from harm [54], observing and evaluating the patient’s responses to the anaesthesia and ensuring that the patient’s individual needs are met. When a difficult airway is expected or the anaesthesia does not proceed as planned, the RNAs and anaesthesiologists work together in the best interest of the patient [48].
Anaesthesia and intubation from a patient perspective For both awake and asleep intubation, patients worry about being anaesthe-tised and intubated [3]. Patients undergoing anaesthesia worry about being anaesthetised and intubated [55, 56] more as the date of the surgery ap-proaches [4]. Those with previous anaesthesia experience are less anxious than those who have never undergone anaesthesia [55, 56]. Patients who perceive stress and worry about the anaesthesia and surgery preoperatively report more postoperative anxiety and discomfort [55]. In addition, patients experience more anxiety regarding general anaesthesia than local anaesthesia [56], and women generally exhibit more anxiety about having anaesthesia than men [4, 55, 56]. Patients who have experienced an awake endotracheal intubation report more feelings of discomfort, sensation of suffocation, and hoarseness than those who undergo a traditional endotracheal intubation [56].
According to Burkle et al. [57], it is important to inform patients about their planned anaesthesia so they can weigh their own individual risks and benefits before undergoing anaesthesia. A systematic review [58] showed that preoperative communication and dialogue between patients and health-care professionals is important for improving the quality of care. It has also been found that if patients discuss their thoughts and feelings with a nurse anaesthetist and if a harmonious atmosphere in the operating room can be created, patients feel secure and cared for [59]. If patients are informed and know what will happen to them, it can reduce their fear of the unknown [60] and calm them preoperatively [61]. Patients have concerns about having anaesthesia and this cannot be overlooked or underestimated. The need for
20
more individualised information and support are of importance for the pa-tient and may allay anxiety [62].

21
Rationale for the thesis
In clinical practice, careful airway assessment is important when performing endotracheal intubation and to the quality of care. The aim of preoperative airway assessment is to identify patients who will probably be easy or diffi-cult to intubate in order to improve patient safety [1]. This is important be-cause, in Sweden, RNAs are allowed to induce and maintain general anaes-thesia without the direct supervision of an anaesthesiologist, in accordance with specified protocols and agreements [48]. In addition, in clinical prac-tice, it is not always the same anaesthesia professional that preoperatively assesses the patient’s airway and then performs the endotracheal intubation. Therefore, systematic and detailed documentation of the patient’s airway is important for improving patient safety. Several anaesthesia societies, both national and international [1, 36-38, 63], have published guidelines and algo-rithms to assist anaesthesia professional in managing a difficult airway. Even if the purpose is to provide safer practices, there is wide variability in the adherence to guidelines and algorithms in anaesthesia practice [47]. Thus, the use of guidelines and algorithms is influenced by human factors, such as personality, individual experience, scientific beliefs, and attitudes, when making decisions in clinical practice [47]. In addition, how a difficult airway should be managed depends on the anaesthesia providers’ individual techni-cal and non-technical skills and on the specific situation [64]. Studies have also been published on how to support anaesthesia professionals when as-sessing the patient’s airway prior to anaesthesia and how to safely perform an endotracheal intubation [13, 65], but no nationwide studies have de-scribed the presence of airway management guidelines or variations in the ways anaesthesiologists understand the phenomenon ´airway algorithm´ when acting in and handling critical airway situations. When a difficult intu-bation is expected, the recommended option for securing the airway is awake fiberoptic intubation [2, 28], but little is known in the available literature on how patients experience this procedure. To the best of my knowledge, no study has explored patients’ experiences of being awake intubated. Preopera-tive experiences, such as anxiety and worries about anaesthesia and surgery, have been explored [55, 56]. From the patients’ perspective, feedback about their experiences with awake fiberoptic intubation is useful information that may contribute to changes in caring for patients, thereby improving the qual-ity of care.
22
Aims
The overall aim of the present thesis was to study airway management in anaesthesia care from both professional and patient perspectives.
Study I The specific aim was to investigate whether the Mallampati classification, thyromental, and Cormack & Lehane grades are useful tests for predicting an easy intubation.
Study II The specific aim was to explore the presence of airway guidelines in Swed-ish anaesthesia departments.
Study III The specific aim was to deepen our knowledge about how anaesthesiologists comprehend algorithms for the management of difficult airways.
Study IV The specific aim was to describe patient experiences of being awake fiber-optic intubated.
23
Methods
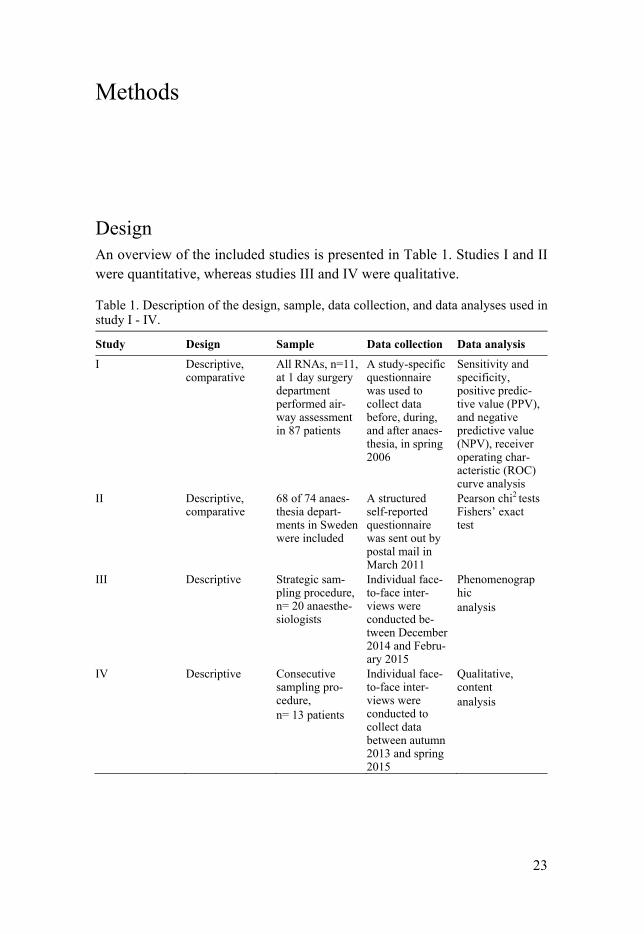
Design An overview of the included studies is presented in Table 1. Studies I and II were quantitative, whereas studies III and IV were qualitative.
Table 1. Description of the design, sample, data collection, and data analyses used in study I - IV.
Study Design Sample Data collection Data analysis
I Descriptive, comparative
All RNAs, n=11, at 1 day surgery department performed air-way assessment in 87 patients
A study-specific questionnaire was used to collect data before, during, and after anaes-thesia, in spring 2006
Sensitivity and specificity, positive predic-tive value (PPV), and negative predictive value (NPV), receiver operating char-acteristic (ROC) curve analysis
II Descriptive, comparative
68 of 74 anaes-thesia depart-ments in Sweden were included
A structured self-reported questionnaire was sent out by postal mail in March 2011
Pearson chi2 tests Fishers’ exact test
III Descriptive
Strategic sam-pling procedure, n= 20 anaesthe-siologists
Individual face-to-face inter-views were conducted be-tween December 2014 and Febru-ary 2015
Phenomenographic analysis
IV Descriptive Consecutive sampling pro-cedure, n= 13 patients
Individual face-to-face inter-views were conducted to collect data between autumn 2013 and spring 2015
Qualitative, content analysis

24
Sample and setting
Study I All RNAs in one department were recruited over a 4-month period in 2006. The airways of 100 patients were assessed by RNAs who were directly in-volved in the patients’ routine care. Inclusion criteria were adult patients
> 17 years of age who were scheduled to undergo general anaesthesia re-quiring endotracheal intubation and were ASA physical status I or II. Pa-tients undergoing emergency anaesthesia and patients who were pregnant or had a body mass index > 35 kg/m2 were excluded from the study. This hospi-tal provides anaesthesia services for both inpatient and outpatient surgery and was organised as part of a larger county hospital in the County Council of Gävleborg, which had 275 000 inhabitants at the time of the study. The day surgery department served approximately 3300 patients annually and was chosen as the research setting because the RNAs routinely conduct pre-operative airway evaluations and intubate all patients as part of their routine work.
Study II A structured self-reported questionnaire concerning the presence of guide-lines for airway management was sent out in March 2011 to directors or assistant directors of Swedish anaesthesia departments (n = 74). The anaes-thesia departments were identified by the Swedish Association of Local Au-thorities and Regions [66].
Study III A strategic sampling procedure was used to maximise the variation in which anaesthesiologists understand algorithms. According to Bowden & Green [67], 20-30 interview participants is enough to ensure sufficient variation. Twenty anaesthesiologists from one university and three county hospitals in Sweden were invited to participate in the study. The study was conducted between December 2014 and February 2015. The inclusion criteria were a minimum 2 years of working clinical experience in anaesthesiology. Anaes-thesiologists not involved in direct patient care were excluded.
Study IV A consecutive sampling procedure was used and participants recruited from one university hospital and three county hospitals in the middle part of Swe-den. The study was conducted between autumn 2013 and spring 2015. Inclu-

25
sion criteria were patients > 18 years of age admitted to the anaesthesia de-partment for planned or unplanned awake fiberoptic intubation who were able to speak and understand the Swedish language. Patients planned to un-dergo regional anaesthesia or who had undergone planned or unplanned awake fiberoptic intubation in the past were excluded from the study.
Procedures Study I Information and educational instruction regarding the study aim and proce-dures were provided by Kati Knudsen (KK) 2 weeks before the study started. All patients underwent airway evaluation at the time of the preoperative visit, and after the anaesthesia were finished. The airway was evaluated by the same RNA who then performed the anaesthesia to reduce assessment error. The patients’ airways were evaluated during the daytime, Monday through Friday. All patients received general anaesthesia according to the hospital’s local standard and were intubated with a 7-mm (for women) or 8-mm (for men) endotracheal tube using a Macintosh laryngoscope.
Study II The directors received written information about the purpose of the study and were asked to fill out the questionnaire and return in a prepaid and ad-dressed envelope. Informed consent was given by returning the question-naire. Reminders were sent out twice. Those who did not respond within 3 months of the second reminder were reminded a third time by telephone.
Study III The head of each anaesthesia department was contacted via e-mail and asked to distribute written invitation letters about the study purpose and procedures to all anaesthesiologists who worked in their departments. Two weeks later, during a workplace meeting, the anaesthesiologists were verbally informed about the study by KK in person and an appointment for the interview set up. Anaesthesiologists who volunteered for the study provided written informed consent before the interview started. All interviews were conducted by KK in the daytime in a quiet room over the course of 1 week at each workplace.
Study IV Before the study started, patients received written and verbal information about the study purpose and procedure from the anaesthesiologists during

26
their preoperative meeting. A consecutive sampling procedure was used and individual face-to-face interviews performed. Each participant was inter-viewed twice. The first interview was conducted at a place chosen by the patient, such as the hospital or their own home. The second, follow-up inter-view was conducted over the telephone 4 weeks after the first interview in order to give the patient an opportunity to clarify and verify what had been said. Written informed consent was obtained before the interviews started.
Data collection Study I A study-specific questionnaire was developed by KK based on clinical ex-perience assessing and performing endotracheal intubations independently, as well as on a brief review of existing airway tests in the literature [34, 63]. The questions were then evaluated and revised by a health care worker as an expert in the field to ensure face validity. The next step was to discuss the specific questions within the research group experienced in quantitative methods in order to improve their clarity and establish content validity. The questionnaire was developed in three parts: before, during, and after anaes-thesia. Part one consisted of Mallampati classification scores I–IV (See Fig-ure 1) and the thyromental distance. The thyromental distance (i.e., the dis-tance between the bony point of the mentum to the thyroid notch with the head fully extended) was measured with a 25-cm ruler while the patient’s mouth was closed (See Figure 2). Part two consisted of Cormack & Lehane grades I–IV (See Figure 3) and documentation of the number of intubation attempts according to the ASA recommendations [34]. These airway tests have been used and validated in multiple studies as “golden standards” for predicting a difficult intubation [68, 69]. Part three consisted of the RNA’s judgement of the intubation conditions being experienced as easy or diffi-cult. These were documented and categorised using a four-grade scale as follows: quite easy, easy, somewhat difficult, or difficult. In addition, sex, age, weight, and height were documented, as well as data regarding the RNA’s years of experience.
The following scores were considered to be predictors of easy endotra-cheal intubation: Mallampati classification I–II, thyromental distance ≥ 10 cm, Cormack & Lehane grade I–II, and less than two intubation attempts. Mallampati classification III–IV and Cormack & Lehane grade III–IV were categorised as difficult intubations, as well as a thyromental distance ≤ 10 cm and two or more intubation attempts. RNA scores of “quite easy” and “easy” were considered easy intubations, whereas “somewhat difficult” and “difficult” were considered difficult intubations.
27
Study II The questions in study II concerned the presence of airway management guidelines in anaesthesia departments in Sweden. The eight questions con-cerned whether the department had 1) an airway algorithm, 2) written patient information in the case of a difficult airway, 3) guidelines for difficult air-ways, 4) guidelines for preoperative airway assessment, 5) guidelines for rapid sequence intubation, 6) guidelines for criteria on when to perform an awake intubation, 7) instructions for awake fiberoptic intubation, and 8) a prescription for when an RNA or anaesthesiologist should perform an en-dotracheal intubation. In addition, two background questions were included about hospital type and the number of general anaesthesia procedures per-formed per year.
All responses to the questions were dichotomised (yes or no), and if the respondent answered “yes” to any question they were asked to attach and return copies of their current guidelines. Guidelines for regional anaesthesia or other commonly used guidelines, such as preoperative fasting, were ex-cluded. The director was also asked to attach the department’s anaesthetic record form in order to review whether a fill-out “box” of airway elements was pre-printed as a checklist. The questionnaires were returned by postal mail in pre-addressed return envelopes.
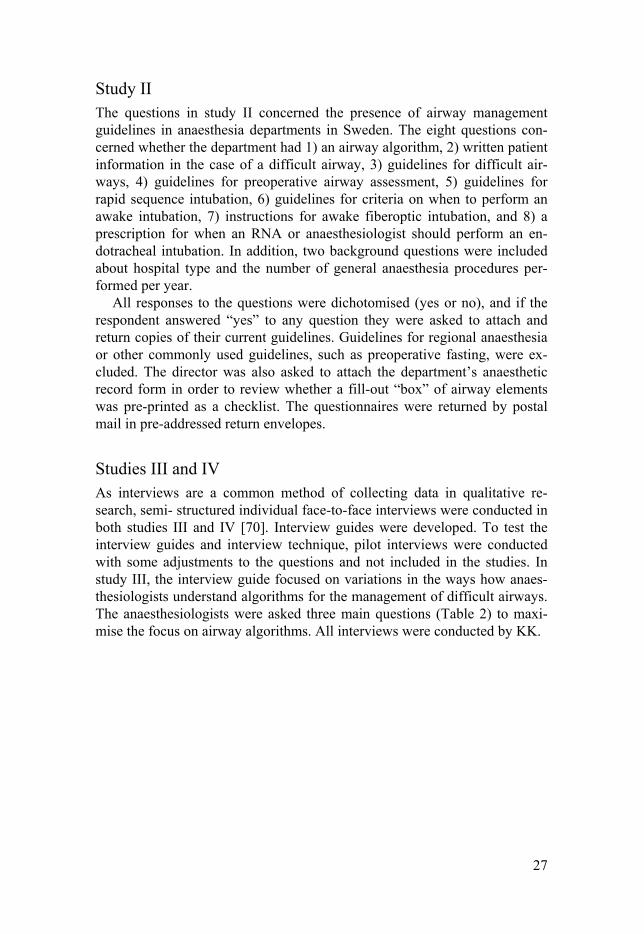
Studies III and IV As interviews are a common method of collecting data in qualitative re-search, semi- structured individual face-to-face interviews were conducted in both studies III and IV [70]. Interview guides were developed. To test the interview guides and interview technique, pilot interviews were conducted with some adjustments to the questions and not included in the studies. In study III, the interview guide focused on variations in the ways how anaes-thesiologists understand algorithms for the management of difficult airways. The anaesthesiologists were asked three main questions (Table 2) to maxi-mise the focus on airway algorithms. All interviews were conducted by KK.
28
Table 2. Interview guide for questions used in Study III on anaesthesiologists views on algorithms, including probing questions. 1. Can you give a concrete example of an event when you observed a difficult airway? 2. What do you think about algorithms, which might also be referred to as guidelines, proto-cols, or decision aids? 3. Can you describe a situation where you felt that you were successful or not successful in managing a difficult airway? Probing questions were: “Did you use an algorithm that helped you manage the situation?” “What do you mean”? “Can you give more examples”? “What did you think would happen”? “Is there anything else you would like to add”?
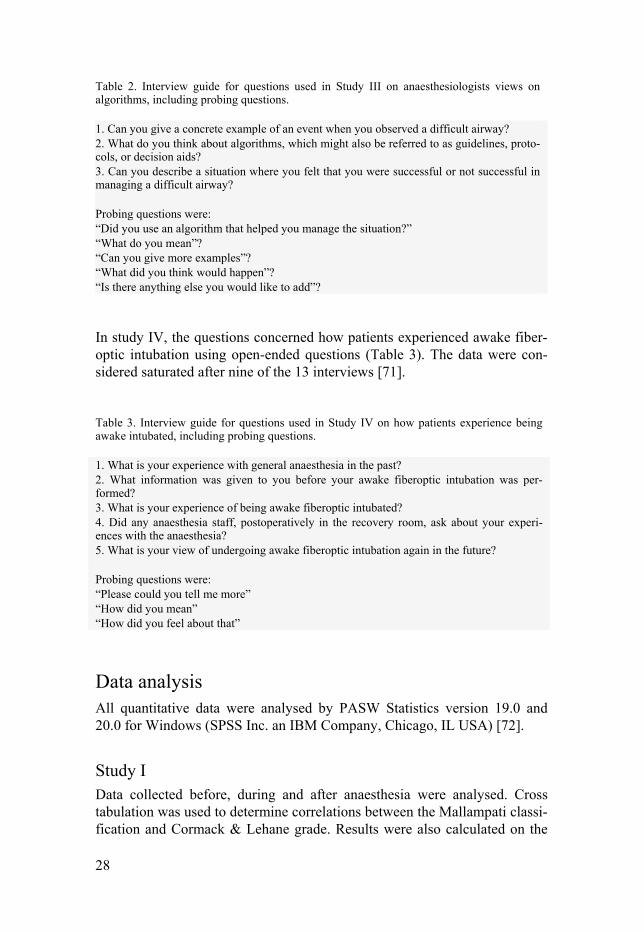
In study IV, the questions concerned how patients experienced awake fiber-optic intubation using open-ended questions (Table 3). The data were con-sidered saturated after nine of the 13 interviews [71].
Table 3. Interview guide for questions used in Study IV on how patients experience being awake intubated, including probing questions. 1. What is your experience with general anaesthesia in the past? 2. What information was given to you before your awake fiberoptic intubation was per-formed? 3. What is your experience of being awake fiberoptic intubated? 4. Did any anaesthesia staff, postoperatively in the recovery room, ask about your experi-ences with the anaesthesia? 5. What is your view of undergoing awake fiberoptic intubation again in the future? Probing questions were: “Please could you tell me more” “How did you mean” “How did you feel about that”
Data analysis All quantitative data were analysed by PASW Statistics version 19.0 and 20.0 for Windows (SPSS Inc. an IBM Company, Chicago, IL USA) [72].
Study I Data collected before, during and after anaesthesia were analysed. Cross tabulation was used to determine correlations between the Mallampati classi-fication and Cormack & Lehane grade. Results were also calculated on the

29
basis of sensitivity and specificity for the Mallampati classification, thy-romental distance, and Cormack & Lehane grade used to predict the ease of intubation. Sensitivity was defined in terms of the percentage of correctly -predicted easy intubations as a proportion of all intubations that were truly easy: [true easy intubations/(true easy intubations + false difficult intuba-tions)]. Specificity was defined in terms of the percentage of correctly pre-dicted difficult intubations as a proportion of all intubations that were truly difficult: [true difficult intubations/(false easy intubations + true difficult intubations)]. In addition, the positive predictive value (PPV) and negative predictive value (NPV) were calculated if the test was clinically useful. The PPV was defined in terms of the percentage of correctly predicted easy intu-bations as a proportion of all predicted easy intubations: [true easy/(true easy + false easy)]. The NPV was defined in terms of the percentage of correctly identified difficult intubations as a proportion of all predicted difficult intu-bations: [true difficult/false difficult + true difficult]. The thyromental dis-tance was measured and the results divided into two levels: >10 cm or < 10 cm. A receiver operating characteristic (ROC) curve [72] was applied to de-termine the optimal cut-off level. Each cut-off value was plotted against sensitivity on the vertical axis and 1-specificity on the horizontal axis. The optimal cut-off value was the value in the upper leftmost position. In addi-tion, continuous variables were described using means and standard devia-tions (SDs), and categorical variables as frequencies and percentages [72].
Study II Descriptive statistics were used to describe each hospital type (university, county, and private). For comparisons between hospital type and the avail-ability of written airway guidelines, cross tabulation was used and analysed by Pearson's chi-square tests. Data are expressed as mean and SD, number, or percentage. A p-value < 0.05 was considered significant [72].
Study III The interviews were transcribed verbatim by a professional transcript com-pany. The audio-recorded interviews were listened to by KK and checked against the transcribed text. Qualitative phenomenographic analysis was performed in five steps [73]: 1. The printouts were read and re-read several times to achieve overall com-prehension of the interview. 2. In each interview, the parts of the texts where the anaesthesiologists de-scribed experiences using algorithms in difficult airway situations or re-flected on such experiences were marked.

30
3. The marked parts of the text with descriptions of ‘what’ and ‘how’ the anaesthesiologist thought about algorithms were summarised into one pre-liminary ‘way of understanding’ for each interview. 4. The resulting 20 ‘ways of understanding’ were compared and, based on similarities and differences, grouped into different categories. 5. Each category was discussed regarding its accuracy, going back to the interview texts and revising the category description. In the final analysis, four categories of understanding were revealed.
Three of the researchers conducted the analysis and reassessed the cate-gories to enhance the rigour of the analysis [72]. After steps 1-4, the catego-ries of descriptions that emerged were discussed with all fellow researchers until a consensus was reached [73]. The research team has experience in interviewing and qualitative methods, and one researcher had experience specifically in the phenomenographic method. All researchers except one had experience from working in anaesthesiology.
Study IV The interviews were audio-recorded and transcribed verbatim by the first author. Inductive qualitative content analysis was performed in several steps as described by Graneheim & Lundman [74]. The goal of content analysis is to gain an understanding of the phenomenon being studied [75]. This study aimed to describe patients’ experiences with awake intubation. To get a sense of the whole text, the analysis began by reading the interviews repeat-edly. Meaning units from the interviews that corresponded with the aim of the study were identified and marked with a number. The numbered meaning units were then condensed and shortened into codes, which were compared regarding differences and similarities for sorting into subcategories and cate-gories in dialogue with the co-authors (manifest content analysis). After all data were categorised, one theme was formulated. Verbatim quotations were given to illustrate each category and to ensure credibility and transferability [74]. During the analysis procedure, the categories were discussed and re-evaluated in order for the researcher to confirm the outcome. The research team had a pre-understanding of the phenomena being studied from work in anaesthesiology and/or intensive care, which was actively reflected upon during the analysis to minimise interpretive bias.

31
Ethical considerations
Formal approval from ethics committee was not required, according to Swedish national legislation and directives [76, 77] at the time study I was conducted, as no intervention was performed and no personal data were ob-tained. To protect the interest of the people involved in the study I, the an-aesthesia department involved reviewed the research protocol and approved the study without any changes. Throughout the research, ethical issues were considered carefully and in accordance with the Declaration of Helsinki [78].
Ethical consideration is important when conducting research involving vulnerable participants [79], such as when there is a risk that a participant may be affected by physical or mental discomfort or harm related to the re-search procedures. The potential risks and benefits associated with the re-search study were taken into account. As the study procedure included stan-dardised care and were part of their routine airway assessments, and no addi-tional or new intervention was implemented, there were no foreseeable risks involved in the study. In study I, the primary focus was on how RNAs can independently perform the airway assessment and intubation in patients. To protect the patients’ rights, all were orally informed that the focus was on the involved RNAs. The patients were also informed that their participation did not change their usual care and that the obtained data would be coded in a way that they would not be identified. Study II was a national survey of the presence of written airway guidelines and did not involve sensitive personal material or data. Therefore, this research is not subject to Swedish law and no ethical approval was sought.
The Regional Ethical Review Board in Uppsala, Sweden, approved stud-ies III-IV (Diary no. 2012/546 and 2014/491, respectively). All participants received both oral and written information about the studies’ purpose and procedures before the studies began. To protect the participants’ confidenti-ality, they were informed that the obtained data were coded in a manner that was not linked to the particular participants’ name or hospital. To protect all of the involved participants, they were also informed that their participation was strictly voluntary and that they could withdraw at any time, without explanation, and that this withdrawal would not affect their employment or care. The participants involved in studies III and IV were also informed that the interviews should be audio-recorded, transcribed, coded, and stored so that no one could be identified, neither in person nor in the workplace. Writ-ten informed consent was obtained before the studies started. The partici-

32
pants were also informed that the collected data would be kept in a way that access was limited to the research team only. Participants were also given contact information for the researcher, should they have further questions or want to discuss their concerns related to their involvement in the studies.
33
Results
Study I A total of 11 RNAs performed airway assessments on 87 patients (68 women, 19 men). Most of the RNAs had worked for more than 10 years (n=61 patients, 71%); 25% of patients were seen by RNAs who had worked 3-6 years (n=22) and 5% (n=4) by those who had worked less than 3 years. The mean patient age was 42 (± 11) years, mean weight 71 (± 14) kg, and mean height 168 (± 9) cm. Thirteen patients were excluded due to incom-plete documentation of the data.
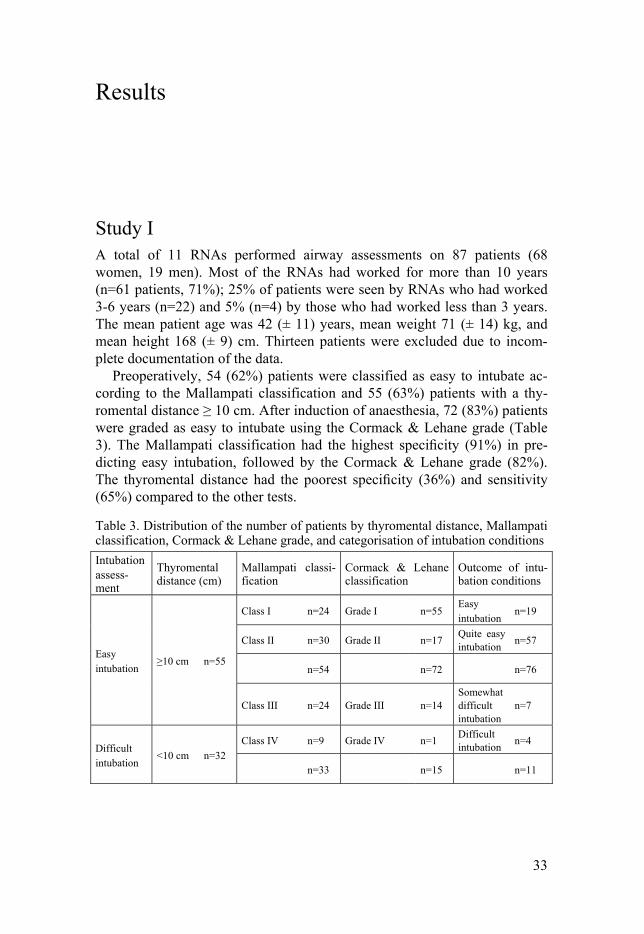
Preoperatively, 54 (62%) patients were classified as easy to intubate ac-cording to the Mallampati classification and 55 (63%) patients with a thy-romental distance ≥ 10 cm. After induction of anaesthesia, 72 (83%) patients were graded as easy to intubate using the Cormack & Lehane grade (Table 3). The Mallampati classification had the highest specificity (91%) in pre-dicting easy intubation, followed by the Cormack & Lehane grade (82%). The thyromental distance had the poorest specificity (36%) and sensitivity (65%) compared to the other tests.
Table 3. Distribution of the number of patients by thyromental distance, Mallampati classification, Cormack & Lehane grade, and categorisation of intubation conditions
Intubation assess-ment
Thyromental distance (cm)
Mallampati classi-fication
Cormack & Lehane classification
Outcome of intu-bation conditions
Easy intubation
≥10 cm n=55
Class I n=24 Grade I n=55 Easy intubation
n=19
Class II n=30 Grade II n=17 Quite easy intubation
n=57
n=54 n=72 n=76
Class III n=24 Grade III n=14 Somewhat difficult intubation
n=7
Difficult intubation
<10 cm n=32
Class IV n=9 Grade IV n=1 Difficult intubation
n=4
n=33 n=15 n=11

34
Sixty-two percent of the patients (54/33) were easy to intubate according to the Mallampati classification (i.e., required less than two intubation at-tempts). Seventeen percent (15/72) of the patients were difficult to intubate according to the Cormack & Lehane grade and required two or more intuba-tions attempts. The agreement between the number of intubation attempts and the RNA scoring of intubation conditions was 86%. The agreement be-tween the RNAs’ subjective assessments and the Mallampati classification was 72%.
Study II Of the 74 directors, 68 returned the questionnaire, a response rate of 92%. These completed questionnaires were received from 53 county hospitals, 9 university hospitals, and 6 private hospitals. The highest number of general anaesthesia procedures per year was performed by the university hospitals (mean 14 389 ± 7674), followed by county hospitals (mean 5646 ± 4143), and the private hospitals had the fewest anaesthesia procedures per year (mean 4063 ± 1837). No significant difference was found between the hospi-tals regarding the percentage of written guidelines for airway management, except for guidelines on difficult airways (p = 0.049). Eight of the nine uni-versity hospitals reported having guidelines for difficult airways, compared to only 25 of the 53 county hospitals and 2 of the 6 private hospitals.
A total of 214 guidelines were reported by the anaesthesia departments, 67% of which (n=132) were not verified by an attachment. Of the attached guidelines, 21% (n=46) were followed as recommendations of the SFAI [63] and 17% (n=36) of the attached guidelines were developed by the local an-aesthesia department. Twenty-nine of the 68 departments (43%) had guide-lines for preoperative airway assessment. Forty-six departments (68%) had a pre-planned intubation plan, in the form of an airway algorithm, in the case of failed intubation. Thirty-five departments (52%) had guidelines for a dif-ficult airway, and 35 departments (52%) had an anaesthesia problem card that they gave to the patient in the case of a difficult airway. Guidelines for how to perform awake fiberoptic intubation were available in 14 (21%) of the departments, whereas criteria for when to perform an awake intubation were available in 18 (26%) of the departments. In total, 21 (31%) of the de-partments attached guidelines for emergency rapid sequence intubation. A prescription for when the RNA could carry out the endotracheal intubation was reported by 16 (24%) of the departments.
Fifty-one (75%) departments sent their anaesthesia record form for re-viewing pre-printed airway tests. In 35 (69%) of these records, tooth status was the most common pre-printed preoperative airway test, followed by the thyromental distance (25%); sternomental distance (8%) was the least com-mon pre-printed airway test. In 23 (45%) departments, the Cormack & Le-

35
hane grade and evaluation of the extubation conditions were the most com-mon pre-printed airway test after the anaesthesia was finished, whereas the number of intubation attempts was pre-printed in only 6 (12%) of the at-tached anaesthesia records.
Study III Twenty anaesthesiologists volunteered to participate in the study (5 women, 15 men). Their age ranged from 29 to 68 years (median 39 years), and their clinical experience as anaesthesiologists ranged from 2 to 39 years (median 3.5 years).
Four categories of how an algorithm could be understood were identified: 1) a normative plan for procedures to be followed in difficult airway situa-tions, i.e., law-like rules that must be followed; 2) a succinct plan to follow in difficult airway situations; i.e., a decisional or cognitive aid; 3) an action plan adaptable to the needs of the individual patient and the clinical situa-tion, to be kept in mind when creating a personal algorithm based on experi-ence; 4) a set of guidelines collected by a consensus of experts for proce-dures in managing the difficult airway based on scientific evidence and ex-pert opinions.
In the first category, the algorithm could be understood as a normative plan for procedures to be followed in difficult airway situations. For exam-ple, when an incident happens, one must be able to defend one’s choices of action. If one has diverted from the algorithm based on personal knowledge and experience, the reasons for this diversion must be clearly declared to avoid future critique. In the second category, an airway algorithm could be understood as a plan to follow in a difficult airway situation. For example, plans B and C are ready as back-ups in stressful situations and to avoid for-getting any important steps in the procedure. In the third category, the algo-rithm could be seen as an action plan adaptable to the needs of the individual patient and the clinical situation that can be kept in mind when creating a personal algorithm based on experience. In the last category, algorithms derived from scientific knowledge provide guidance, ideas, and recommen-dations for how to act.
Study IV A total of 15 patients were invited to participate in the study, two of whom declined (1 man, 1 woman) without any specific reason. Ten of the patients had previous experience with general anaesthesia and three of the patients were receiving anaesthesia for the first time. Of the 13 included patients (7 men, 6 women), eight were interviewed preoperatively and five postopera-

36
tively. The reasons for awake fiberoptic intubation were rheumatoid arthritis (n=2), thyroidectomy (n=2), pharyngeal abscess (n=2), oropharynx cancer (n=1), mandibular surgery (n=2), neck immobility (n=3), and acute throat bleeding (n=1).
From the patient interviews, one main theme emerged: feelings of being in a vulnerable situation but cared for in safe hands. This theme was revealed in the following five categories with 15 subcategories: 1) a need for tailored information, 2) distress and fear of the intubation, 3) acceptance and trust of the staff’s competence, 4) professional caring and support, 5) no hesitation about new awake intubation. Patients described different concerns about how they wished to be involved and how much information was needed be-fore the intubation was performed. A lack of information about what to ex-pect was noted. Knowing that they should undergo awake fiberoptic intuba-tion was emotionally stressful due to the fear of throwing up during the pro-cedure, provocation of the gag reflex by the tube, and fear of the local anaes-thetics. For some of the patients, their fears became reality during the procedure when the local anaesthetic solution was sprayed into the throat and the injection into the cricothyroid membrane evoked feelings of discom-fort, coughing, and suffocation. The patients expressed that this was the most unpleasant experience during the whole procedure. The fiberoptic intubation was extremely painful for some patients when the tube was inserted, despite local anaesthetics. On the other hand, patients who had experienced upper intestinal gastroscopy procedures in the past stated that an awake intubation was nearly the same phenomenon and nothing to fear. Patients described feeling more involved when the anaesthetists made eye contact with them and saw how they reacted during the procedure.
Some patients revealed that they felt overwhelmed by the information they were given and wanted less specific information about the equipment used. Instead, they wanted more information about how they would be cared for in the operating room, including breathing instructions and eye contact. Undergoing awake intubation was an acceptable experience for most pa-tients, though some found it to be painful and terrifying because they felt they could not breathe or communicate during the procedure itself.
37
Discussion
Summary of findings The aim of this thesis was to study airway management in anaesthesia care from both professional and patient perspectives. Study I pointed out that the Mallampati classification is a good screening test for predicting easy intuba-tion and that intubation can be safely performed by RNAs. Despite the rec-ommendations of locally adopted airway guidelines, study II affirmed that the presence of airway guidelines in Swedish anaesthesia departments is poorly implemented. According to the findings from study III, algorithms can be understood in four different ways: as law-like rules, as a succinct plan to follow in difficult airway situations, as an action plan kept in the back of one’s mind while creating flexible and versatile personal algorithms, or as consensus guidelines based on expert opinion in order to be followed in clinical practice. Study IV revealed one main theme; feelings of being in a vulnerable situation but cared for in safe hands, which is described in five categories as follows: a need for tailored information, distress and fear of the intubation, acceptance and trust of the staff’s competence, professional car-ing and support, and no hesitation about new awake intubation.
Airway management and guidelines from a professional perspective Study I pointed out that the Mallampati classification is a good screening test to predict an easy intubation. Of the 87 included patients, most patient were easy to intubate according to the Mallampati classification I-II, and required less than two intubations attempts and by definition classified as easy intuba-tion by the ASA [1].
According to the ASA [1], all patients scheduled for general anaesthesia and tracheal intubation should be considered for preoperative airway as-sessment. However, these assessments have been reported to often be in-completely documented or lacking [14]. The results from study II agree with this, as the presence of guidelines for airway management in our depart-ments could be improved. For instance, surprisingly few departments re-ported have guidelines for preoperative airway assessment. Adequate airway assessments and detailed documentation of patient airways are important,

38
especially when the endotracheal intubation is not always carried out by the same anaesthesia professional that performed the preoperative airway as-sessment. From a professional safety perspective, it is important to perform a preoperative airway assessment in advance, when the patient is still awake, to give the anaesthetists enough time to be prepared for alternative airway approaches. Research has shown that a previous history of difficult endotra-cheal intubation is a strong risk factor for intubation problems in the future [80].
In study II, few departments reported they have prescriptions for when RNAs can carry out endotracheal intubation, despite RNAs being allowed to maintain and intubate patient airways independently. In Sweden, they are allowed to induce and perform general anaesthesia independently in healthy adult patients with ASA physical status I and II according to specified proto-cols and agreements [48]. Standardised, structured documentation of the patients’ airway assessment, as recommended by the ASA [1], may make the anaesthesia professionals aware and prepared for using the right competence at the right time to ensure patient safety, that adequate airway devices are readily available, and that there is supervision from a more experienced an-aesthesiologist who is able to assist the RNA and secure the airway if needed. Based on the preoperative airway evaluation, a test that can predict easy intubation beforehand, such as the Mallampati classification, is a valu-able tool in clinical practice. This test facilitates the decision about who should carry out the intubation, the RNA or the anaesthesiologist, when there is still time to plan for an alternative airway approach.
Airway guidelines and algorithms for managing patients’ airways within anaesthesia care have been recommended by several anaesthesia societies and by the Swedish National Board of Health and Welfare [1, 36-38, 80]. Despite these recommendations, study II demonstrated that the presence of airway management guidelines is generally poorly implemented in Swedish anaesthesia departments. One reason for a lack of local adopted airway guidelines in Swedish anaesthesia departments could be a lack of time and, perhaps, knowledge about how to create evidence-based guidelines. A lack of knowledge and practical skills in handling a difficult airway and adher-ence to guidelines have also been found in Danish [81], German [82], and Canadian anaesthesia departments [83]. The ASA recommends practice guidelines being adopted and modified according to the department's own needs and constraints. As airway guidelines are not an absolute requirement, the development of such guidelines may not be a priority for departments. The results from study III are consistent with previous studies, which affirm that human factors, such as the professional’s knowledge and beliefs, influ-ence compliance with or deviation from the guidelines [47].
Some researchers have argued that algorithms are a useful cognitive aid to achieve safer airway procedures [44]. However, the results from study III argue that, before airway algorithms can be used, it must be ensured that

39
they are easy to follow, without too many steps, because in a stressful situa-tion too many steps would be difficult to memorise. As stated by Smith & Alderson [41], guidelines should be as short and concise as possible; if they are too descriptive they appear to limit professionals’ judgement. The au-thors further advocated that guidelines need to be based on the best available scientific evidence and a broad consensus to improve patient outcomes. Study III showed that algorithms for the management of difficult airways can be understood in four ways: as law-like rules, as a succinct plan to fol-low in difficult airway situations, as an action plan kept in the back of one’s mind while creating flexible and versatile personal algorithms, or as consen-sus guidelines based on expert opinion. One barrier against using guidelines such as algorithms is that they do not take the individual anatomical charac-teristics of a patient (e.g., a tonsil tumour) or a specific situation into ac-count. For instance, it was explained that algorithms are developed for the “average” patient and are not applicable to all kinds of patients and situa-tions:
“An algorithm is a useful tool, but you need to tailor it for each individual
patient… a useful support, like a crutch... but patients are also different; they have various conditions and anatomy, and one must take these factors into account... “(Study III)
Thus, algorithms may be more useful in clinical practice if they could be designed in a more efficient and practical manner. In addition, algorithms need to be based on a simple principle and easy to follow in order to be im-plemented. A systematic review by Ebben et al. [84] highlighted that there is a gap between guidelines and clinical practice. One reason for this gap is that guidelines contain too many recommendations to adhere to when making choices. They emphasised that if guidelines could be translated into more efficient, practical and feasible algorithms, it would be easier to adhere to them. Goldhaber-Fiebert & Howard [85] recently reported that cognitive aids, such as algorithms, cannot be implemented powerfully if they are not developed from evidence-based practice. A study on the use of evidence- based guidelines for mechanical ventilation in a Swedish intensive care set-ting reported similar findings [86]. However, anaesthesia professionals’ manage difficult airways on their own during critical situations based on their own knowledge and beliefs [47]. According to Polanyi [87], knowledge can be divided into two different categories, namely tacit knowledge and explicit knowledge, and can be used to explain how individuals handle spe-cific situations. He described tacit knowledge as an individual’s intuitively acquired knowledge that is developed through experiences and difficult to verbalise, whereas explicit knowledge is knowledge acquired by reading the medical literature and sharing specific information. However, he argued that individuals need both tacit and explicit knowledge when acting in and han-

40
dling specific situations. In other words, knowing how to adopt and use, for example, guidelines and algorithms in clinical practice requires both tacit knowledge and the support of explicit knowledge.
A common opinion among anaesthesiologists in study III was that you must have experienced a real situation before you are able to use algorithms, and this requires training and clinical experience. This is consistent with the findings of a systematic review of 13 studies examining the number of en-dotracheal intubations a novice intubator must perform using direct laryngo-scopy to achieve expertise with the procedure [88]. In elective circum-stances, a novice intubator needed to perform at least 50 endotracheal intu-bations on patients before successfully mastering the airway procedures. Dreyfus & Dreyfus [89] described practitioners going through five different levels of experience, from novice to expert, before they master work-related skills. As a novice without previous experience, they make decisions using clear rules and instructions, which they follow strictly until they have gained experience, whereas an expert, who has developed a lot of clinical experi-ence over time, may see situations differently and identify and handle prob-lems more intuitively. Thus, skills such as face-mask ventilation and per-forming endotracheal intubation are mastered by working bedside on a daily basis (“learning by doing”) and by being exposed to patients with various individual anatomies and situations, especially in time-pressure emergency situations. Perhaps, after a couple years of clinical experience, you can cre-ate your own strategies for how to use airway algorithms, modified by your own clinical experiences to fit the patients and situations. Therefore, it seems evident that clinical experience is required, along with theoretical knowl-edge, to master skills such as handling a difficult airway in critical situations. The professional’s ability to communicate calmly and clearly is also impor-tant when acting in and handling critical situations [53]. Hands-on training is needed to improve procedural skills in critical airway situations [90]. Simu-lator training, together with education and reflection, contributes to improv-ing procedural skills and performance in critical situations [33,44]. However, the simulation training in anaesthesiology is still under development and it is not yet known how efficient such approach will be [91]. Part of the problem is that algorithms are developed for the "average" patient and do not account patient individual factors or the skill of the intubator. Simulation training for management of a difficult airway may well improve both knowledge and skills but perhaps not the professionals’ behaviour in critical situation.
The ability to maintain a free airway through face-mask ventilation and intubation is a craft that requires routine practice to master. Once a difficult airway appears, it is an emotionally stressful situation for the professionals [52]. In my experience, difficult intubation is less problematic than difficult mask ventilation because you can still ventilate and oxygenate the patient’s lungs. Problems may occur when it is difficult to ventilate the patient, espe-cially during time-pressure critical situations. Securing the patient's airway is

41
a team effort [92], and it is hard to work entirely on your own in a critical situation. When facing difficult mask ventilation, one may need to use a two-handed technique to oxygenate the patient’s lungs. However, study III re-vealed that the ASA algorithm is too descriptive, and it is hard to memorise all the steps and remember them in a critical situation:
“Algorithms are there in the back of your mind... so that you have a plan
to follow and know what to do next… but they´ve got to be simple and easy to follow - no more than 3-4 steps - to help avoid becoming blocked in critical situations… once you are in a difficult airway situation, you may not be able to think of every step in the algorithm…” (Study III)
In my opinion, more attention should be given to the development of an al-gorithm in the form of an illustrated picture showing, step by step, how to handle the situation when the airway fails. In a critical airway situation in which, the airway needs to be managed immediately, it is easier to look at an illustrated algorithm for instructions on what to do next than read a lot of text. The key is to make it easier when acting and handling difficult airways in critical situations. When an airway needs to be managed immediately, patients become extra vulnerable because there is no or little time to ade-quately prepare them.
Anaesthesia and intubation from a patient perspective Study IV revealed that careful emotional support before and during the an-aesthesia procedure is important when the intubation is performed in the awake state. Patients want tailored information about the procedure without technical details about the equipment used. Support, such as breathing in-structions, along with eye contact from the anaesthesia professional, helps patients cope and feel more safe and confident during the procedure. Ac-cording to Lazarus & Folkman [93], coping is a natural response when indi-viduals face a stressful situation, such as anaesthesia. How patients deal with stress depends on the situation and the patient´s own individual coping strategies. Patients can use several types of coping strategies [94]. Study IV revealed that patients use emotion-focused coping strategies, such as medi-tating and accepting the situation, when they feel that they have little control over their own situation. Also, patients use problem-focused coping before the procedure. Not knowing what should happen evoked feelings of being in a vulnerable situation. The patients expressed a need for tailored information about what to expect, which helped them master and control the situation. This finding is supported by the study by Mitchell [4], who highlighted that

42
patients undergoing general anaesthesia are more anxious and want more information than patients scheduled for local anaesthesia.
“It was just to realise that I must leave myself in other people’s hands. I
had full confidence, I meditated and calmed down... There is nothing I can do now, so I have to trust you and your colleagues, those who are going to do this, I must resign myself to it.” (Study IV)
Even if the study by Mitchell did not focus on awake intubation per se, the patients experienced greater feelings of emotional support when they felt informed. From the patients’ perspective, it is important to be well-informed [4] about what to expect and how the procedures could be experienced, as local anaesthetic is a common part of the anaesthetic procedure. Several patients in study IV described the most unpleasant experience during the whole procedure to be feelings of discomfort after the local anaesthetic solu-tion was sprayed into the throat and the injection was made in the back of the trachea, including pain, coughing, and feelings of suffocation.
“It felt like I could not swallow, like I would suffocate on the fluid, like as
I cough and throw up at the same time…” (Study IV)
This is a dilemma during an awake intubation, when patients need to be se-dated enough to make the procedure more tolerable and alleviate unpleas-antness, but still need to be able to follow instructions and commands. Patients experienced awake fiberoptic intubation as a feeling of being in a vulnerable situation but cared for in safe hands. Several of the patients de-scribed awake intubation as a quite acceptable experience, despite the emo-tional stress, and that they would not hesitate to undergo awake intubation again in the future if needed. Nevertheless, patients are vulnerable during the procedure because it is difficult to vocally communicate due to the local anaesthetic solution and when the tube is inserted. Therefore, it is important for the staff to be aware of how to communicate with the patients via eye contact during the procedures, as described by the patients in study IV. Simi-lar findings have been reported by others [95, 96].
Methodological considerations In studies I and II, quantitative study designs were chosen because of their usefulness in gaining valuable information about current anaesthesia practice and describing the presence of airway guidelines in our anaesthesia depart-ments. In studies III and IV, qualitative study designs were chosen in order to gain a deeper understanding of how algorithms can be understood and
43
how patients experience awake fiberoptic intubation. However, there are some methodological strengths and limitations in the presented studies that need to be taken into account [70]. In studies I and II, study-specific ques-tionnaires were used as a data collection method, which must be taken into consideration when assessing the validity and reliability [97]. Before the start of the studies, the questionnaires were pilot tested and reviewed by experienced researchers involved in the study and by RNAs and anaesthesi-ologists working in the field in order to ensure that the questions were clear and understandable and to establish face and content validity.
In addition, study I included relatively few patients, more women than men, and only healthy adult ASA I-II patients undergoing elective day sur-gery. Another limitation was that the study was conducted by RNAs who worked at the same anaesthesia clinic. The reliability may have differed if another group of RNAs with different experience or skills from different clinics or if anaesthesiologists had assessed and carried out the intubation. As in all quantitative research, the sample size is important for generalising the findings to a larger population [98]. A sample size calculation was not performed before starting study I. The findings cannot be generalised to other patients or be said to be representative of all anaesthesia departments. However, the result provided information that the Mallampati classification is a useful test for predicting easy intubation when the airway assessment is performed by RNAs in a standardised manner.
The main strength of Study II was that it was a nationwide survey with a high response rate (92%) and included a large number of anaesthesia de-partments. A limitation of study II was that the questions only addressed specific airway management issues and did not explore how often the de-partments evaluated their airway management guidelines. The generalisabil-ity of the results is questionable, as the data are not necessarily based on which guidelines really exist at these departments. Perhaps they had airway guidelines but use different terms for their documents, such as standards, protocols, checklists, algorithms, clinical pathways, and recommendations for clinical practice [41, 84, 99, 100]. This makes it difficult to draw firm conclusions when interpreting the results.
Individual interviews are a common data collection method in qualitative research. According to Lincoln & Guba [75], to ensure trustworthiness in qualitative research, the credibility, dependability, confirmability, and trans-ferability need to be taken into considerations. In studies III and IV, semi- structured face-to-face interviews were conducted by KK. An interview guide was developed and used to collect data and strengthen the credibility, minimising research bias (dependability). Pilot interviews were carried out with both anaesthesiologists and patients not included in the studies to test the interview guide and ensure that the questions that were asked closely reflect the aim of the study [67]. As Larsson & Holmström [73] suggested in a phenomenographic study, the data from 20 informants is usually enough to

44
discover variations in the ways people understand or perceive a specific phe-nomenon. The phenomenographic approach is based on the theory that peo-ple understand a specific phenomenon in a limited number of qualitatively different ways [101]. The data analysis in study III started when all inter-views had been conducted. In contrast to study IV, the data analysis was on-going until saturation was reached and no additional information was ob-tained [102]. To strengthen the confirmability, the data analyses began by reading the text repeatedly and breaking down the data into smaller units and codes, then grouping the coded material into categories and themes [73, 74]. In both studies, quotes from the interviews were extracted to exemplify the categories and themes that emerged. The research team had a pre-understanding of the phenomenon under study due to extensive experience in anaesthesiology and/or intensive care, which were actively reflected upon during the analysis to minimise interpretive bias [73]. During the whole analysis process, consensus was reached between the researchers concerning the emerging results through discussion to avoid influencing the authors’ pre-understanding of working in the field. The findings have been critically debated and discussed with others with experience in qualitative methods and different pre-understandings of the phenomenon during research semi-nars. As with all qualitative studies [70], the findings from these two studies cannot be generalised and the transferability of the results is up to the reader to decide. The results from study III are valuable as they can be used to de-velop a more applicable algorithm to follow in clinical practice. The results from study IV are useful as no available study has explored patient experi-ences with awake intubation. Such valuable information can improve the quality of care. Whether the results from these studies are transferable to other settings and patients requires further study.
45
Clinical implications
Preoperative airway assessment is important to identify patients who will be easy or difficult to intubate. Most of the published literature has mainly fo-cused on the prediction of difficult airways [25]. Mallampati classification III-IV is also a predictor of difficult mask ventilation combined with difficult laryngoscopy [103]. Therefore, it is important to use airway tests that can clearly define easy airways to provide guidance for when RNAs can main-tain and perform endotracheal intubation independently. In clinical practice, airway tests are more useful if they also predict an easy airway, as endotra-cheal intubations in Sweden are mostly performed by RNAs without the direct supervision of anaesthesiologists.
In order to promote patient safety in clinical practice, the development of evidence-based guidelines and algorithms for the management of difficult airways should be considered a higher priority. Study III revealed that algo-rithms are a valuable tool when presented with a difficult airway, but in clinical practice, more attention should be given to developing algorithms that are simple and easier to follow, as presented by the Difficult Airway Society (DAS) [36]. It will be interesting to follow when the DAS guidelines for the management of difficult airways become available in our anaesthesia departments. From the professional perspective, dealing with a difficult air-way is one of the most stressful events one will face, especially during an emergency, and the approach takes time to learn and master. Therefore, a well-designed algorithm that is easy to follow is essential. In critical situa-tions, a visual algorithm can be helpful for the practitioner to communicate effectively with the team, especially if one's own experience is governed.
Awake fiberoptic intubation is an alternative procedure for securing the patient’s airway when a difficult airway is expected. From the patients’ per-spective, tailored information about what to expect and how awake fiber-optic intubation could be experienced is important to increase their feelings of control and ability to cope during the procedure. To improve the quality of care, it is important to take patients’ needs, feelings, and thoughts into consideration. In addition, patients should be offered written and visual in-formation about how they should be cared for in the operating room to en-able patients to feel calm before the procedure is performed.
46
Conclusions
The overall aim of the present thesis was to study airway management in anaesthesia care from both the professional and patient perspective.
- Airway management is of central importance when performing anaesthesia. The Mallampati classification is a good screening test for predicting easy intubation when the airway assessment is performed in a structured manner by RNAs.
- In anaesthesia care, airway guidelines and algorithms have
been developed and recommended to achieve safer airway procedures, but airway guidelines are poorly implemented in Swedish anaesthesia departments.
- Algorithms have been recommended in clinical practice to aid in determining how to act and handle difficult airways. To be used in daily practice, algorithms need to be simple and easy to follow and based on the best available scientific evidence.
- From the patients’ perspective, the most unpleasant part of the procedures is discomfort following the application of local an-aesthetic. Tailored information about what to expect, ensuring eye contact, and giving breathing instructions during the pro-cedure may reduce patients’ feeling distress. Most of the pa-tients would not hesitate to undergo awake intubation again if needed, in the future.
47
Svensk sammanfattning (Swedish summary)
Preoperativ luftvägsbedömning är viktigt för att identifiera patienter som sannolikt kommer att bli lätta eller svåra att intubera. Trakeal intubation är i det flesta fall tekniskt okomplicerad och utförs vanligtvis efter en lyckad maskventilation, när patienten är nersövd. De flesta luftvägsproblem i sam-band med trakeal intubation har inträffat när adekvat luftvägsbedömning inte har gjorts. Olika rutiner och riktlinjer, nationellt som internationellt, för hur luftvägen ska bedömas har blivit beskrivna i syfte att öka patientsäkerheten vad gäller luftvägsproblem i samband med anestesi. Trots detta dokumente-ras viktiga förutsägande luftvägstester olika samt ibland inkonsekvent bland anestesipersonal. För att öka patientsäkerheten vid anestesi rekommenderas att evidensbaserade riktlinjer används och att en luftvägsalgoritm följs vid svår luftväg. Dock visar studier att förekomst och följsamhet till luftvägsrikt-linjer och algoritmer är bristfällig. Faktorer som personliga erfarenhet, ve-tenskaplig övertygelse och den enskildes attityd påverkar beslutet att följa eller frångå riktlinjerna.
Vakenintubation anses vara det säkraste sättet att erhålla fria luftvägar in-för generell anestesi och rekommenderas för patienter som identifierats med svår luftväg. En vakenintubation genomförs vanligtvis under lokalanestesi och lätt sedering. Samarbete och kommunikation mellan patienten och den som genomför vakenintubationen är av betydelse eftersom patientens möj-ligheter till verbala kommunikation begränsas genom trakealtubens placer-ing. För det flesta patienter är anestesi i samband med operation förknippat med varierande grad av oro och ångest. Generellt upplever kvinnor mer oro och ångest jämfört med män. Tidigare studier har kunnat påvisa ökad pati-enttillfredsställelse och minskad ångest och oro i samband med anestesi om patienten är välinformerad.
Det övergripande syftet med avhandlingen var att studera luftvägsbedöm-ning inom anestesisjukvård från både anestesiprofessionens och patientens perspektiv.
Syftet med studie I var att studera om Mallampatis klassifikation, thyromen-tal avstånd och Cormack och Lehanes gradering var användbara luftvägstes-ter för att predicera lätt intubation. Anestesisjuksköterskor vid en dagkirur-gisk operationsavdelning fick under en fyra månaders period preoperativt luftvägsbedöma 100 patienter inför planerad anestesi. Resultatet visade att
48
Mallampati klassifikation var ett användbart test för att predicera lätt luftväg om bedömningen genomförs på ett strukturerat sätt samt att intubationen kan genomföras självständigt och på ett patientsäkersätt av anestesisjuksköters-kan.
Syftet med studie II var att genom en nationell studie granska förekoms-ten av rutiner och riktlinjer för luftvägsbedömning. Ett strukturerat fråge-formulär skickades ut till samtliga chefer inom anestesiavdelningar i Sveri-ge. Resultatet visade att förekomst vad gäller riktlinjer för luftvägsbedöm-ning var bristfälligt. Riktlinjer för preoperativ luftvägsbedömning rapporte-rades tillgängliga hos 29 (43 %) av 68 anestesiavdelningar. Riktlinjer för hur man ska genomföra en vakenintubation rapporterades tillgängligt hos 18 (26 %) av anestesiavdelningarna. Endast 16 (24 %) av anestesiavdelningarna rapporterade riktlinjer för när anestesisjuksköterskans självständigt kunde intubera patienter.
Syftet med studie III var att beskriva hur strategiskt utvalda anestesiolo-ger tänker kring situationer med svår luftväg och vilka strategier de använder för att hantera och lösa situationen. Individuella intervjuer med 20 anestesio-loger spelades in och skrevs ut ordagrant och analyserades med hjälp av fenomenografisk metod. Resultatet visade att algoritmer (kan också kallas för riktlinjer, protokoll eller beslutsstöd) för att hantera svåra luftvägar kunde uppfattas som en enkel plan att följa vid svåra luftvägssituationer, ett be-slutsstöd, en handlingsplan anpassad efter patient och situation, en riktlinje utarbetad av experter for hur man handlägger svåra luftvägar baserad på evidens och expert kunnande.
Syftet med studie IV var att beskriva patienters upplevelser i samband med en vakenintubation. Under ett besök på den preoperativa mottagningen för sedvanlig anestesibedömning informeras patienten muntligt och skriftligt om studien. Därefter genomfördes individuella intervjuer med 13 patienter. Intervjuerna spelades in och analyserades med hjälp av kvalitativ innehålls-analys. Av resultatet framkom ett huvudtema; känna sig i en utsatt situation men vårdad i säkra händer och följande fem kategorier; behov av skräddar-sydd information, oro och rädsla inför intubation, tillit till personalens kom-petens, omtänksam och professionell vård och ingen tvekan att genomgå en vakenintubation igen.
Sammanfattningsvis visar avhandlingsarbetet att Mallampati klassifika-tion var ett användbart test för att predicera lätt luftväg när bedömningen genomfördes på ett strukturerat sätt av anestesisjuksköterskan. Vidare visade avhandlingen att nationella kliniska riktlinjer för luftvägshantering inför anestesi behöver förbättras för att öka patientsäkerheten. Trots att algoritmer för hur man ska hantera svåra luftvägar har utvecklats och publicerats, både nationell och internationell, framkom att algoritmer för hur man hantera svåra luftvägar är svåra att komma ihåg i en stressig luftvägssituation. Algo-ritmer bör vara enkla och innehålla få steg för att implementeras i det dagliga kliniska arbetet. Vakenintubation är en rekommenderad metod för att säk-

49
ra fria luftvägar hos patienter med misstänkt svår luftväg. Från patientens perspektiv, skräddarsydd information, ögonkontakt och andningsinstruk-tioner under själva förfarandet minskar oro och ångest inför anestesi. Patientens upplevelser av vakenintubation är av klinisk betydelse för hur den preoperativa informationen kan utformas samt hur patientens egen delaktighet kan optimeras i samband med vakenintubation.
50
Acknowledgements
First of all, I would like to thank my supervisor Ulrica Nilsson. Thank for guiding me over the past five years as this thesis would not have been possi-ble without your help. I would also like to thank Ulrika Pöder, my co-supervisor for your valuable assistance, encouragement, critical comments and editing of my numerous manuscripts. I would also like to thank Marieann Högman, my co-supervisor for your ideas and input when devel-oping my own algorithm and for your constructive comments and guidance during my research. I would also like to thank Anders Larsson, my co-supervisor for your constructive comments and valuable feedback and input into my work. I would also like to thank Dr. Jan Larsson for your expertise that contributed to this thesis.
Thanks to my friend and earlier colleagues, Ulla-Carin Blom-Ivarsson for introducing me to my supervisor. To Ann-Marie Broqvist & Tarja Lidberg for our many walking tours where you listened to my concerns, sharing my tears and holding me up during these years.
Thanks to my earlier colleagues working, at the anaesthesia departments in Gävle Hospital, Eva Åström & Miska Hibner for helping me when I needed support.
I would also like to thank all of my doctoral colleagues, too many to name, at the Department of Health and Caring Sciences at University of Gävle & at the Department of Public Health and Caring Science at Uppsala University who has helped me along my doctoral journey. Thank, especially for your support in reviewing, critiquing and feedback of my research during semi-nars and sharing my doctoral journey. Also, thanks to statistician Hans Högberg for your support with my statistics.
Thanks to my friends, too numerous to mention all by name, who have been there and supporting me. Thanks to my brother for your support with my tables.
To my family, Bent and lovely daughter Olivia for always being there, trust-ing and believing in me. I would not have been able to complete this thesis without your help. You are my all happiness and pleasure, love you.
51
References
1. Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, Nickinovich DG, et al. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult air-way: An updated report by the American Society of Anesthesiologists Task Force on management of the difficult airway. Anesthesiology 2013; 118: 251-270.
2. Benumof JL. Management of the difficult adult airway, with special emphasis on awake tracheal intubation. Anesthesiology 1991;75:1087-1110.
3. Schnack DT, Kristensen MS, Rasmussen LS. Patients' experience of awake versus anaesthetised orotracheal intubation: a controlled study. Eur J Anaesthe-siol 2011; 28: 438-442.
4. Mitchell M. Influence of gender and anaesthesia type on day surgery anxiety. J Adv Nurs 2012; 68: 1014-1025.
5. Mavridou P, Dimitriou V, Manataki A, Arnaoutoglou E, Papadopoulos G. Pa-tient's anxiety and fear of anesthesia: effect of gender, age, education, and pre-vious experience of anesthesia. A survey of 400 patients. J Anesth 2013; 27: 104-108.
6. Ramkumar V. Preparation of the patient and the airway for awake intubation. Indian J Anaesth 2011; 55: 442-447.
7. The National Board of Health and Welfare (Socialstyrelsen). Statistical Data-bases (Accessed 7 Mars 2016). Available from: http://www.socialstyrelsen.se/statistics
8. Vannucci A, Cavallone LF. Bedside predictors of difficult intubation: a system-atic review. Minerva Anestesiol 2016;82: 69-83.
9. Rose DK, Cohen MM. The incidence of airway problems depends on the defini-tion used. Can J Anaesth 1996; 43: 30-34.
10. Kheterpal S, Healy D, Aziz MF, Shanks AM, Freundlich RE, Linton F, et al. Incidence, predictors, and outcome of difficult mask ventilation combined with difficult laryngoscopy: a report from the multicenter perioperative outcomes group. Anesthesiology 2013; 119: 1360-1369.
11. Cook TM, MacDougall-Davis SR. Complications and failure of airway man-agement. Br J Anaesth 2012;109 1:i68-i85
12. Eberhart LH, Arndt C, Aust HJ, Kranke P, Zoremba M, Morin A. A simplified risk score to predict difficult intubation: Development and prospective evalua-tion in 3763 patients. Eur J Anaesthesiol 2010; 27:935-940.
13. Kheterpal S, Martin L, Shanks AM, Tremper KK. Prediction and outcomes of impossible mask ventilation: A review of 50,000 anesthetics. Anesthesiology 2009; 110:891-897.
14. Cook TM, Woodall N, Frerk C, Fourth National Audit Project. Major complica-tions of airway management in the UK: Results of the fourth national audit pro-ject of the royal college of anaesthetists and the difficult airway society. Part 1: Anaesthesia. Br J Anaesth 2011;106:617-631.
52
15. L'Hermite J, Nouvellon E, Cuvillon P, Fabbro-Peray P, Langeron O, Ripart J. The simplified predictive intubation difficulty score: A new weighted score for difficult airway assessment. Eur J Anaesthesiol 2009;26: 1003-1009.
16. Shiga T, Wajima Z, Inoue T, Sakamoto A. Predicting difficult intubation in apparently normal patients: A meta-analysis of bedside screening test perfor-mance. Anesthesiology 2005;103:429-437.
17. Mallampati SR. Clinical sign to predict difficult tracheal intubation (hy-pothesis). Can Anaesth Soc J 1983; 30:316-317.
18. Lee A, Fan LT, Gin T, Karmakar MK, Ngan Kee WD. A systematic review (meta-analysis) of the accuracy of the mallampati tests to predict the difficult airway. Anesth Analg 2006;102:1867-1878.
19. Khan ZH, Mohammadi M, Rasouli MR, Farrokhnia F, Khan RH. The diagnos-tic value of the upper lip bite test combined with sternomental distance, thyromental distance, and interincisor distance for prediction of easy laryngos-copy and intubation: A prospective study. Anesth Analg 2009;109:822-824.
20. Bindra A, Prabhakar H, Singh GP, Ali Z, Singhal V. Is the modified Mallampati test performed in supine position a reliable predictor of difficult tracheal intuba-tion? J Anesth 2010; 24:482-485.
21. Khan ZH, Eskandari S, Yekaninejad MS. A comparison of the Mallampati test in supine and upright positions with and without phonation in predicting diffi-cult laryngoscopy and intubation: A prospective study. J Anaesthesiol Clin Pharmacol 2015;31:207-211.
22. Frerk CM. Predicting difficult intubation. Anaesthesia. 1991; 46:1005-1008. 23. Baker P. Assessment before airway management. Anesthesiol Clin
2015;33:257-278. 24. Baker PA, Depuydt A, Thompson JM. Thyromental distance measurement--
fingers don't rule. Anaesthesia 2009; 64:878-882. 25. Shiga T, Wajima Z, Inoue T, Sakamoto A. Predicting difficult intubation in
apparently normal patients: A meta-analysis of bedside screening test perfor-mance. Anesthesiology 2005;103:429-437.
26. Rosenstock C, Hansen EG, Kristensen MS, Rasmussen LS, Skak C, Ostergaard D. Qualitative analysis of unanticipated difficult airway management. Acta Anaesthesiol Scand 2006; 50:290-297.
27. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984;39:1105 -1111.
28. Smith T, Pinnock C, Lin T, editors. Fundamentals of Anaesthesia. 3 rd ed. Cambridge Medicine: Lippincott Williams & Wilkins, 2009.
29. Corbanese U, Possamai C. Awake intubation with the Bonfils fibrescope in patients with difficult airway. Eur J Anaesthesiol 2009; 26:837-841.
30. Larsson J, Rosenqvist U, Holmström I. Enjoying work or burdened by it? How anaesthestists experience and handle difficulties at work: a qualitative study. Br J Anaesth 2007: 99; 493-499.
31. Law JA, Broemling N, Cooper RM, Drolet P, Duggan LV, Griesdale DE, et al. Canadian Airway Focus Group. The difficult airway with recommendations for management--part 1--difficult tracheal intubation encountered in an uncon-scious/induced patient. Can J Anaesth. 2013; 60:1089-1118.
32. Gjeraa K, Jepsen RM, Rewers M, Østergaard D, Dieckmann P. Exploring the relationship between anaesthesiologists' non-technical and technical skills. Acta Anaesthesiol Scand 2016; 60: 36-37.
33. Flin R, Patey R, Glavin R, Maran N. Anaesthetists’ non-technical skills. Br J Anaesth 2010; 105: 38-34.
53
34. American Society of Anesthesiologists. Practice guidelines for management of the difficult airway. A report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 1993; 78:597-602.
35. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. American Society of Anesthesiologists Task Force on Man-agement of the Difficult Airway. Anesthesiology 2003; 98:1269-1277.
36. Frerk CM, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for the management of unanticipated difficult intubation in adults (DAS). Br J Anaesth 2015; 115: 827-848.
37. Petrini F, Solca M, De Robertis E, Peduto VA, Pasetto A, Conti G, et al. SIAARTI-ESA Task Force. The Helsinki Declaration on Patient Safety in An-esthesiology: a way forward with the European Board and the European Society of Anesthesiology. Minerva Anestesiol 2010; 76:971-977.
38. Jensen AG, Callesen T, Hagemo JS, Hreinsson K, Lund V, Nordmark J. Scan-dinavian clinical practice guidelines on general anesthesia for emergency situa-tions. Acta Anasthesiol Scand 2010; 54: 922-950.
39. Crosby ET. An evidence-based approach to airway management: is there a role for clinical practice guidelines? Anaesthesia 2011; 66 2:112-118
40. World Health Organisation. Guideline for WHO Guidelines EIP/ GPE/EQC/2003.1 2003. (Accessed 7 Mars 2016). Available from: http://whqlibdoc.who.int/hq/2003/eip_gpe_eqc_2003_1.pdf
41. Smith A, Alderson P. Guidelines in anaesthesia: Support or constraint? Br J Anaesth 2012; 109:1-4.
42. Mehlman MJ. Medical practice guidelines as malpractice safe harbors: Illusion or deceit? J Law Med Ethics 2012; 40:286-300.
43. Marshall S. The use of Cognitive Aids During Emergencies in Anesthesia: A Review of the Literature. Anesth Analg 2013; 117:1162-1171.
44. Marshall SD, Mehra R. The effects of a displayed cognitive aid on non-technical skills in a simulated 'can't intubate, can't oxygenate' crisis. Anaesthesia 2014; 69: 669-677.
45. Heidegger T, Gerig HJ, Henderson JJ. Strategies and algorithms for manage-ment of the difficult airway. Best Pract Res Clin Anaesthesiol 2005; 19:661-674.
46. Petrini F. Airway management and guideline implementation: The gap from research to daily practice. Minerva Anestesiol 2008; 74:449-450.
47. Phipps DL, Beatty PC, Parker D, Nsoedo C, Meakin GH. Motivational influ-ences on anaesthetists' use of practice guidelines. Br J Anaesth 2009; 102: 768-774.
48. National Association for Anaesthesia and Intensive Care & Swedish Society of Nursing - SSF. Description of competence for Registered Nurse with Graduate Diploma in Specialist Nursing – Anaesthesia Care. Stockholm. (Accessed Mars 7 2016). Available from: http://www.swenurse.se/globalassets/publikationer-svensk-sjukskoterskeforening/kompetensbeskrivningar-publikationer/anestesi.eng.komp.pdf
49. Meeusen V, van Zundert A, Hoekman J, Kumar C, Rawal N, Knape H. Compo-sition of the anaesthesia team: A European survey. Eur J Anaesthesiol 2010; 27:773-779.
50. Matsusaki T, Sakai T. The role of certified registered nurse anesthetists in the United States. J Anesth 2011; 25:734-740.
54
51. Certification and regulation of advanced practice nurses. American association of colleges of nursing. J Prof Nurs 1999; 15:130-132.
52. Larsson J, Rosenqvist U, Holmström I. Enjoying work or burdened by it? How anaesthetists experience and handle difficulties at work: a qualitative study. Br J Anaesth 2007; 99:493-499.
53. Larsson J, Holmstrom IK. How excellent anaesthetists perform in the operating theatre: A qualitative study on non-technical skills. Br J Anaesth 2013; 110:115-121.
54. Sundqvist AS, Carlsson AA. Holding the patient's life in my hands: Swedish registered nurse anaesthetists' perspective of advocacy. Scand J Caring Sci 2013; 29: 281-288.
55. Matthias AT, Samarasekera DN. Preoperative anxiety in surgical patients - experience of a single unit. Acta Anaesthesiol Taiwan 2012; 50:3-6.
56. Mavridou P, Dimitriou V, Manataki A, Arnaoutoglou E, Papadopoulos G. Pa-tient's anxiety and fear of anesthesia: effect of gender, age, education, and pre-vious experience of anesthesia. A survey of 400 patients. J Anesth 2013; 27:104-108.
57. Burkle CM, Pasternak JJ, Armstrong MH, Keegan MT. Patient perspectives on informed consent for anaesthesia and surgery: American attitudes. Acta Anaesthesiol Scand 2013; 57:342-349.
58. Chan Z, Kan C, Lee P, Chan I, Lam J. A systematic review of qualitative stud-ies: patients' experiences of preoperative communication. J Clin Nurs 2012; 21:812-824.
59. Rudolfsson G, von Post I, Eriksson K. The expression of caring within the peri-operative dialogue: a hermeneutic study. Int J Nurs Stud. 2007;44: 905-915.
60. Lindwall L, von Post I, Bergbom I. Patients' and nurses' experiences of periop-erative dialogues. J Adv Nurs 2003; 43:246-253.
61. Rosén S, Svensson M, Nilsson U. Calm or not calm: the question of anxiety in the perianesthesia patient. J Perianesth Nurs 2008; 23:237-246.
62. Burkle CM, Mann CE, Steege JR, Stokke JS, Jacob AK, Pasternak JJ. Patient fear of anesthesia complications according to surgical type: potential impact on informed consent for anesthesia. Acta Anaesthesiol Scand. 2014; 58:1249-1257.
63. SFAI, Svensk Förening för Anestesi och Intensivvård. Den svåra luftvägen. Hallen K, Ullman J, Frykholm P, Nellgård P, Åkesson J. (Accessed 7 Mars 2016). Available from: http://sfai.se/riktlinje/medicinska-rad-och-riktlinjer/anestesi/den-svara-luftvagen/
64. Flin R, Patey R, Glavin R, Maran N. Anaesthetists' non-technical skills. Br J Anaesth 2010; 105:38-44.
65. Langeron O, Birenbaum A, Le Saché F, Raux M. Airway management in obese patient. Minerva Anestesiol 2014; 80:382-392.
66. Swedish Association of Local Authorities and Regions. Municipalities, county councils and regions. (Accessed 7 Mars 2016). Available from: http://english.skl.se/municipalities_county_councils_and_regions
67. Bowden, J A., Green, P. Doing developmental phenomenography. Melbourne, RMIT University Press. 2005.
68. Rosenstock C, Gillesberg I, Gatke MR, Levin D, Kristensen MS, Rasmussen LS. Inter-observer agreement of tests used for prediction of difficult laryngo-scopy/tracheal intubation. Acta Anaesthesiol Scand 2005; 49:1057-1062.
69. Naguib M, Scamman FL, O'Sullivan C, Aker J, Ross AF, Kosmach S, et al. Predictive performance of three multivariate difficult tracheal intubation mod-els: A double-blind, case-controlled study. Anesth Analg 2006; 102:818-824.
55
70. Polit, D.F. & Beck, C.T. Nursing research. Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Lippincott Williams & Wilkins, 2012.
71. Krippendorff K. Content Analysis: An Introduction to its Methodology. 2nd ed. Thousand Oaks, CA: Sage Publications, 2004.
72. Norman GR, Streiner DL. Biostatistic. The Bare Essentials, 3th ed. Canada: BC Decker Inc., 2008.
73. Larsson J, Holmström I. Phenomenographic or phenomenological analysis: does it matter? Examples from a study on anaesthesiologists’ work. Int J Qual Stud Health Well-being 2007; 2: 55-64.
74. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today 2004; 24: 105-112.
75. Lincoln YS, Guba EG. Naturalistic Inquiry. Thousand Oaks, CA: Sage Publica-tions Inc., 1985.
76. Swedish Codes of Statues (SFS). Law (2003:460). Ethical Review of Research Involving Humans. (Accessed 7 Mars 2016) Available from: http://www.riksdagen.se/sv/Dokument-Lagar/Lagar/Svenskforfattningssamling/Lag-2003460-om-etikprovning_sfs-2003-460/
77. Codex rules & guidelines for research. (Accessed 7 Mars 2016). Available from: http://www.codex.vr.se/en/index.shtml
78. CODEX rules and guidelines for research. [Accessed 4 Mars 2016]. Available from: http://www.wma.net/en/30publications/10policies/b3/
79. Lundstrøm LH, Møller AM, Rosenstock C, Astrup G, Gätke MR, Wetterslev J; Danish Anaesthesia Database. A documented previous difficult tracheal intuba-tion as a prognostic test for a subsequent difficult tracheal intubation in adults. Anaesthesia 2009; 64:1081-1088.
80. The National Board of Health and Welfare. Socialstyrelsen. (Accessed 7 Mars 2016). Available from: http://www.socialstyrelsen.se/english
81. Rosenstock C, Østergaard D, Kristensen MS, Lippert A, Ruhnau B, Rasmussen LS. Residents lack knowledge and practical skills in handling the difficult air-way. Acta Anaesthesiol Scand 2004; 48:1014-1018.
82. Goldmann K, Braun U. Airway management practices at German university and university-affiliated teaching hospitals-equipment, techniques and training: re-sults of a nationwide survey. Acta Anaesthesiol Scand. 2006; 50:298-305.
83. Borges BC, Boet S, Siu LW, Bruppacher HR, Naik VN, Riem N, Joo HS. In-complete adherence to the ASA difficult airway algorithm is unchanged after a high-fidelity simulation session. Can J Anaesth 2010; 57:644-649.
84. Ebben RH, Vloet LC, Verhofstad MH, Meijer S, Mintjes-de Groot JA, van Achterberg T. Adherence to guidelines and protocols in the prehospital and emergency care setting: a systematic review. Scand J Trauma Resusc Emerg Med. 2013 Feb 19; 21:9. doi: 10.1186/1757-7241-21-9.
85. Goldhaber-Fiebert SN, Howard SK. Implementing emergency manuals: can cognitive aids help translate best practices for patient care during acute events? Anesth Analg 2013; 117: 1149-1161.
86. Eldh AC, Vogel G, Söderberg A, Blomqvist H, Wengström Y. Use of evidence in clinical guidelines and everyday practice for mechanical ventilation in Swed-ish intensive care units. Worldviews Evid Based Nurs 2013; 10:198-207.
87. Polanyi M. The Tacit Dimension. London: Routledge & Kegan Paul, 1966
56
88. Buis ML, Maissan IM, Hoeks SE, Klimek M, Stolker RJ. Defining the learning curve for endotracheal intubation using direct laryngoscopy: A systematic re-view. Resuscitation 2016; 99: 63-71.
89. Dreyfus HL, Dreyfus SE. Mind over Machine: The Power of Human Intuition and Expertise in the Era of the Computer. New York. 1986.
90. Boet S, Borges BC, Naik VN, Siu LW, Riem N, Chandra D, et al. Complex procedural skills are retained for a minimum of 1 yr after a single high-fidelity simulation training session. Br J Anaesth 2011; 107: 533-539.
91. Green M, Tariq R, Green P. Improving Patient Safety through Simulation Train-ing in Anesthesiology: Where Are We? Anesthesiol Res Pract. 2016; doi: 10.1155/2016/4237523
92. Ford SR. Teamwork in anaesthetics and critical care is possible. Br J Anaesth 2015; 114:349.
93. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. Springer: New York, 1984.
94. Folkman S. Stress, coping and hope. Psychooncology 2010; 19:901-908. 95. Sundqvist AS, Carlsson AA. Holding the patient's life in my hands: Swedish
registered nurse anaesthetists' perspective of advocacy. Scand J Caring Sci 2014; 28: 281-288.
96. Karlsson AC, Ekebergh M, Mauléon AL, Almerud Österberg S."Is that my leg?" patients' experiences of being awake during regional anesthesia and sur-gery. J Perianesth Nurs 2012; 27:155-164.
97. Bolarinwa OA. Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger Postgrad Med J 2015; 22:195-201.
98. Tabachnick, B. G. & Fidell, L. S. Using multivariate statistics. 5th ed, Pearson Education, Inc., 2007.
99. Lawal AK, Rotter T, Kinsman L, Machotta A, Ronellenfitsch U, Scott SD et al. What is a clinical pathway? Refinement of an operational definition to identify clinical pathway studies for a Cochrane systematic review. BMC Med. 2016; doi: 10.1186/s12916-016-0580-z.
100. Kinsman L, Rotter T, James E, Snow P, Willis J. What is a clinical pathway? Development of a definition to inform the debate. BMC Med. 2010. doi: 10.1186/1741-7015-8-31.
101. Marton F. Phenomenography- Describing conceptions of the world around us. Instr Sci 1981; 10: 177-200.
102. Malterud K, Siersma VD, Guassora AD. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual Health Res 2015:27; 1-8.
103. Kheterpal S, Healy D, Aziz MF, Shanks AM, Freundlich RE, Linton F et al. Incidence, predictors, and outcome of difficult mask ventilation combined with difficult laryngoscopy: a report from the multicentre perioperative outcomes group. Anesthesiology 2013; 119:1360-1369.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1205
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-281905
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2016