Embed Size (px)
Citation preview

8/10/2019 AKI POSTER
http://slidepdf.com/reader/full/aki-poster 1/1
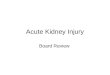
RIFLE
CLASS
RIFLE GFR Criteria UO Criteria AKIN GFR
CRITERIA
AKIN
CLASS
RISK Increase Cr × 1.5 Or
GFR decreases
>25%
UO < 0.5
ml/kg/hr
× 6 hr
Increase Cr ×
1.5 Or
≥ 0.3 mg/dl
STAGE 1
INJURY Increase Cr × 2 Or
GFR decreases
> 50%
UO < 0.5
ml/kg/hr
× 12 hr
Increase Cr ×
2
STAGE 2
FAILURE Increase Cr × 3 Or
GFR decreases
> 75% Or
Cr ≥ 4mg/dl ( with
acute rise of
≥ 0.5 mg/dl)
UO < 0.3
ml/kg/hr
× 24 hr Or
Anuria × 12
hr
Increase Cr ×
3 Or
Cr ≥ 4mg/dl (
with acute rise
of ≥ 0.5 mg/dl)
STAGE 3
LOSS Complete loss of renal function for >
4 weeks
ESRD END STAGE RENAL DISEASES
Table-4 : RIFLE v/s AKIN differences
ACUTE KIDNEY INJURY IN POST-OP NEUROSURGERY PATIENTS IN
CU: A COMPARISON BETWEEN RIFLE AND AKIN CLASSIFICATION
Dr. Vidit Joshi1 Col(Dr) R Ramprasad2, Brig (Dr)G S Ramesh3
1Resident Anesthesiology, AFMC Pune.2Associate Professor, Department of Anaesthesiology AFMC Pune
3Professor & HOD, Department of Anaesthesiology AFMC Pune
To study the incidence of AKI in post op
eurosurgery patients in ICU using RIFLE
AKIN criteria
To note whether there are differences in
entification of Acute Kidney injury in post-
p Neurosurgery patients in ICU using
IFLE and AKIN criteria
To study, associated risk factors in the
evelopment of AKI
Objectives
Acknowledgemen
References
Discussion
Introduction Observation
Sr No. Criteria AKIN RIFLE
1 Sr Creatinine
changes
Change
Within a 48-
hour
Over a one-week
period from
Baseline
3 Absolute S.Cr
increment in Stage 1
Rise of ≥0.3
mg/dL in 48
hrs
-
4 Renal replacement
therapy
Stage 3 No severity class
assigned
Acute kidney injury (AKI) is commonly
seen in the perioperative period and in
the intensive care unit (ICU). It is
associated with a prolonged hospital stay,
high morbidity and mortality.1
To date, there is no universally accepted
definition for acute kidney dysfunction.
The criteria for AKI was first published
with acronym RIFLE (Risk, Injury, Failure,
Loss of kidney function, and End-stage
renal failure), to overcome different
definitions for AKI2
More recently, a modified version was
proposed by the Acute Kidney injuryNetwork (AKIN)3
Neurosurgical patients are more prone to
kidney stress due to blood loss & major
fluid shift, water imbalance in peri-op
period and excessive use of diuretics.
Materials &
Methods
Results
Table-3 :RIFLE & AKIN criteria
Study Design: Prospective observational
study
Study Place: ICU CH(SC), AFMC, Pune
Study Population: All adult Neurosurgical
patients with ICU admission post-op for >
24 hrs
Study Period: DEC 2012 - SEPT 2013
Sample Size: 72 patient
All patients assessed daily for 7 post-op
day using both the RIFLE and AKIN
criteria
MALE43 (60%)
FEMALE29 (40%)
Figure-1: Distribution according to Sex
Non AKI48 (67%)
Stage 119 (26%)
Stage 21 (1%) Stage 3
4 (6%)
Figure-3: Incidence of AKIby AKIN
No AKI57 (79%)
RISK10 (14%)
Injury3 (4%)
Failure2 (3%)
Figure-4: Incidence of AKIby RIFLE criteria
15
23
10
19
54
0
5
10
15
20
25
RIFLE AKIN
Figure-7: PROGRESS OF STAGE 1 / RISK
S TA GE 1 RE COV ER Y H IGH ER GR ADI NG
3
5
0
1 1
0
5
9
4
21
10
2
4
6
8
10
IM DAY 1 DAY2 DAY3 DAY4 DAY5 DAY6 DAY7
Figure-6: Incidence of AKI ON
Post-op Day by AKIN/RIFLE
RIFLE AKIN
1. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. A
kidney injury, mortality, length of stay, and costs in hospitalizedpatients.J Am Soc Nephrol. 2005;16:3365-70.
2. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute
Dialysis Quality Initiative workgroup. Acute renal failure—definitoutcome measures, animal models, fluid therapy and informatio
technology needs:the Second International Consensus Conferen
the Acute Dialysis Quality Initiative (ADQI) .Crit Care. 2004;8:R212.
3. Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnoc
et al. Acute Kidney Injury Network: report of an initiative to impr
outcomes in acute kidney injury.Crit Care. 2007;11:R31
No AKI45 (62%)
AKINonly
12 (17%)
AKIN +RIFLE
12 (17%)
RIFLEonly
3 (4%)
Figure-5: Comparison ofAKIN & RIFLE
We are grateful to the Col (Dr) S Singh, Gp Capt.(Dr) R M Sh
Lt Col. (Dr) R Goyal and Department of Anaesthesiology and
critical care, AFMC Pune for their kind guidence and support.
16
911
9
4
3
911
0
5
10
15
20
25
< 30 yrs 31-45 yrs 46-60 yrs > 60 yrs
Figure-2: Distribution according to Age
No AKI AKI
Criteria AKI
Mean sd)
Non AKI
Mean sd)
p-
Value
Pre-op Cr (mg/dl) 0.83
(±0.24)
0.96
(±0.20)
0.018
Pre- Op Urea
(mg/dl)
29.11
(±10.25)
22.68
(±8.08)
0.795
Pre- Op K+ (mmol) 4.267
(± 0.38)
4.193
(±0.43)
0.470
Intra-Op Urine
output (ml)
1082.59
(±963)
956.89
(±418)
0.446
Intra-Op Blood loss
(ml)
653.33
(±256)
529.33
(±190)
0.022
Duration of Surgery(hr)
5.74(±1.14)
4.84(±1.84)
0.013
APACHE score 8.33
(±3.96)
6.04
(±4.95)
0.045
Criteria
ALL
cases 72)
AKI 27)
Non
AKI 45)
p-Value
Hypertension 16(22.2%) 8(29.6%) 8(17.8%) 0.258
Diabetes 15(20.8%) 10(37.0%) 5(11.1%) 0.015
Liver diseases 2(2.8%) 2(7.4%) 0(0%) 0.047
LVH/ CAD 3(4.2%) 3(11.1%) 0(0%) 0.049
Malignancy 12(16.7%) 4(14.8%) 8(17.8%) 1.000
Seizures 20(27.8%) 8(29.6%) 12(26.7%) 0.792
Immobilization 7(9.7%) 4(14.8%) 3(6.7%) 0.413
Chemotherapy 1(1.4%) 0(0%) 1(2.2%) 1.000
Contrast study 20(27.8%) 13(48.1%) 7(15.6%) 0.006
Transfusion
Reaction
2(2.8%) 1(3.7%) 1(2.2%) 1.000
Hypo
albuminemia
22(30.6%) 12(44.4%) 10(22.2%) 0.045
Conclusion Diagnosis of early AKI was found to
higher using the AKIN than RIFLE criter
Whether there is over-diagnosis by A
than RIFLE criteria cannot be interprete
this study.
All data analysed using SPSS Version
software
Patient’s age > 60 yr are more prone to
(Figure-2)
More patients were diagnosed as early
by AKIN (33.33%) than by RIFLE (20.8
criteria (P<0.0001). (Figure3-5)
The majority of patients had se
creatinine value increases of greater
50% or greater than 0.3 mg/Dl baseline within the first 48 h
postoperatively (Figure-6)
Association of Quantitative risk factor s
as Pre-op Sr Creatinine, Intra-op b
loss, Duration of surgery and APACH
score on ICU admission was fo
significant using un-paired test.
Association of Qualitative risk factor s
as Contrast, Diabetes, Hypo albumine
CAD/LVH and Liver diseases was fo
significant.
Diagnosis of early AKI was higher u
AKIN than RIFLE criteria.
Outcome prediction (recovery/failure)
comparable in both. (Figure-7)
Increased blood loss, increased opera
time, higher APACHE II score
admission & hypoalbumenemia were fo
to be associated with early AKI.
Limitations : Small sample size , si
center study and no sub group analysis
been done.
TABLE 1: Peri-op risk factors TABLE 2: Risk factors