Embed Size (px)
Citation preview

1
April 30, 2015
Mid-Year Convention
Alabama Nursing Home Association
Learning Objectives
2
Understand the re-organization of the Centers for Medicare & Medicaid Services (CMS) Quality Improvement Organization (QIO) program and the Three-Part Aim and its impact on the healthcare delivery system
Become familiar with the Six Priorities of the CMS Quality Strategy
Explore collaboration opportunities with community partners to improve the care transitions and coordination for reducing avoidable hospitalizations
Learn more about the National Nursing Home Quality Care Collaborative (NNHQCC) Aim, Goal, Task and the use of data and information analysis to track and trend admissions, benchmark performance, and monitor improvement
Deploy an effective strategy for improvement and make improvements stick through QAPI teams
National Partnership to Improve Dementia Care – new national goal of reducing the use of unnecessary antipsychotic medications
CMS-QIO Restructuring
3
Began exciting new, multi-state 5-year contract on Aug. 1, 2014
Beneficiary and Family Centered Care BFCC-QIOs
• #2 nationwide - Case Review and Monitoring
• www.keproqio.com
Quality Innovation Network QIN-QIOs
• #14 nationwide
• www.atomAlliance.org

2
KEPRO
4
KEPRO is the Beneficiary and Family Centered Care (BFCC) QIO in Areas 2, 3, and 4.
KEPRO Contact Information
5
Local Phone Number
Toll-free Phone Number Fax Number
Area 2 813-280-8256 844-455-8708 844-834-7129
Area 3 216-447-9604 844-430-9504 844-878-7921
Area 4 813-280-8256 855-408-8557 844-834-7130
What is a QIN-QIO?
6
Quality Innovation Network-Quality Improvement Organizations:
• Bring Medicare beneficiaries, providers, and communities together in data driven initiatives that increase patient safety, make communities healthier, better coordinate post-hospital care, and improve clinical quality.

3
QIN-QIOs Across the Country
7
atom Alliance Partners
8
Are you safe?
9

4
CMS Quality Strategy
10
Goals
Make care safer
Strengthen patient and family engagement
Promote effective communication and coordination of care
Promote effective prevention and treatment
Promote best practices for healthy living
Make care affordable
Make Care More Affordable
11
Make Care More Affordable
Quality Improvement Through Various Value-Based
CMS Reporting Programs:
Hospital Value-Based Purchasing (HVBP)
Various Quality Reporting Requirements Across Settings (ASC, IPF, OQR)
Physician Quality Reporting (PQRS)
Special Innovation Project Opportunities that Advance Efforts for Better Care at Lower Costs

5
Physician Feedback and Reporting
Promote Effective Prevention and Treatment of Chronic Disease
14
Improving Cardiac Health

6
Reducing Disparities in Diabetes
Improving Prevention Coordination through Meaningful Use of HIT
Reducing Hospital-Acquired Infections

7
Promote Effective
19
The Quality Chasm
20
Video
Continuing to Bridge the Quality Chasm
21
Forming a Community Partnership to:
• Improve Health Care Coordination, Delivery and Outcomes
• Improve the quality of care for those who transition across care settings through a comprehensive community effort

8
Catalyst CommunitiesA Powerful Force for Collective Impact
22
Coordination of Care
Coordination of Care

9
CMS Care Coordination Goals
25
Reduce Medicare hospital readmission rates in the Medicare program by 20% by 2019
Reduce hospital admission rates in the Medicare program by 20% by 2019
Increase community tenure, as evidenced by increased number of nights spent at home for Medicare beneficiaries by 10% by 2019
Reduce the prevalence of adverse drug events that contribute to significant patient harm, emergency department visits, observation stays, hospital admissions or readmissions occurring as a result of the care transitions process
QIN-QIO Working with Communities
26
Convene community providers and stakeholders to collaborate and share time and resources to meet the needs of the population of beneficiaries that they serve.
Provide mentorship to community leaders as they work within the community coalition to develop and achieve community wide goals.
Provide data and analytic support to communities to identify gaps in quality and develop strategies for improvement.
Assist communities in performing Root Cause Analysis to examine causes of poor care coordination.
Assist communities with implementing and measuring the impact of interventions and connecting those successes to community-wide goals.
Improve medication safety and aim to reduce or prevent adverse drug events by implementing evidence based and/or proven best practice strategies and tools in the communities
Be the Change You Want to See in Healthcare Safety and Quality
27
AAA/ ADRC
HEN
Trade Associations
Insurance
CBOs
Emergency Responders
Academic Institutions
ADPH
YOU! The Consumer!!
Hospitals
Physicians/PMC
Pharmacists
Nursing Facilities
Home Health
Hospice
Assisted Living
Faith-based Organizations
Family Caregivers

10
Healthy Gulf Coast Community
28
Make Care Safer by Reducing Harm Caused in the Delivery of Care
29
Reducing Healthcare-Acquired Conditions in Nursing Homes
30

11
National Nursing Home Quality Care Collaborative (NNHQCC)
31
The purpose of the NNHQCC is for it and its partners to seek to ensure that every nursing home resident receives the highest quality of care. Specifically, the QIN-QIO shall support the Collaborative objective to “instill quality and performance improvement practices, eliminate healthcare acquired conditions, improve resident satisfaction.”
Desired Outcomes
32
Attain a score of six or less on the Quality Measure Composite Score
Recruit sufficient nursing homes to meet or exceed NH total recruitment # by 2017
Increase the percentage of One-Star home participating in the Collaborative(s)
Improve the rate of mobility among long-stay residents
Reduction in the use of unnecessary antipsychotic medication in dementia residents
Recruited Nursing Homes
33
Recruitment Target Number = 170
Total Recruitment = 85 = 50%

12
Non-Recruited Nursing Homes
34
National Nursing Home Quality Care Collaborative (NNHQCC)
35
CMS’ MethodologyTargeted high performing nursing homes
Identified systems and processes that contribute to their overall quality
Focused on successful practices of high performers
Specific Focus On:Healthcare Acquired Infections (HAIs)
Healthcare Acquired Conditions (HACs)
Antipsychotics
National Nursing Home Quality Care Collaborative (NNHQCC)
36
Outcomes:Change PackageA living document to provide a menu of strategies, change concepts and actionable items
QAPI-At-A-Glance ToolkitA step-by-step guide to implementing a quality assurance and performance improvement (QAPI) plan

13
Leading and Sustaining Systemic Change Collaborative (LSSCC)
Leading and Sustaining Systemic Change Collaborative (LSSCC): Purpose
38
Effectively lead and develop self-directed, high functioning teams to drive and sustain systemic improvement using the IHI Model for Improvement and Quality Assurance / Quality Improvement (QAPI) in the nursing homes setting.
Leading and Developing High Performing Teams to Drive & Sustain Systemic Improvement Using QAPI Methodology
39

14
Affordable Care Act requires CMS to establish QAPI standards
CMS mandated nursing homes to use QAPI strategy
QAPI: A Transformative Approach to Quality in Nursing Homes
40
Sustainable
Standardized
Accountable
Supports Performance Improvement Processes (PIPs)
Proactive
Ongoing
Whole team/facility approach
QAPI: Something Different
41
Culture of QualityLeadership
Safety awareness
Responsiveness
Sharing and teamwork
Reporting, supporting and transparency
Avoiding blame
Accountability
42

15
QAPI Step 1: Leadership, Responsibility and Accountability
43
Leaders shouldDevelop a steering committee—a team that will provide QAPI leadershipProvide resources for QAPI, including equipment and trainingEstablish a climate of open communication and respect
John Kotter
Kotter’s 8 Stepsof Change
44
TeamSTEPPS PenguinsAlice: practical, reputation for being tough, gets things done, focused on the goal at hand, knows the colony, doesn't back down, smart but not arrogant
Fred: younger, open to all new ideas, overly curious, very observant, anxious to please, level-headed, thinker, creative, still wide-eyed, willing to volunteer for anything
Buddy: trusted and well-liked, happy to help, not an intellectual, always present, but not a big idea contributor
Louis: “Head Penguin in Charge” – very patient, wise from experience, overly conservative, calm, respected by most, open to new ideas only when supplied with ample evidence they’re needed
NoNo: negative, does not like change, closed to new ideas even when there is a need for them; favorite comment "we have never done that"
The Professor: scholarly intelligence, prefers working with data over coming up with solutions, happy to help, introverted personality
http://smarterteacher.blogspot.com/2011/07/our-iceberg-is-melting-collaboration.html45

16
Which Penguin are You1. Alice2. Fred3. Buddy4. Louis5. NoNo6. The Professor
46
Building a Peer Coaching Program
47
The network of Peer Coaches will represent diverse levels of nursing home staff, both administrative and direct care, as well as, residents and their families
Each state within the Alliance has identified nursing homes to serve as peer coaches within their region
The Purpose of a Peer Coaching Program
48
To serve as an integral part of the nursing home healthcare community to promote quality improvement and provide support among those participating and enrolled in the Leading and Sustaining Systemic Change Collaborative (LSSCC)

17
Composite Measure
49
What is the composite measure?A tool that can be used to help monitor NNHQCC progress from a systems perspective
Which measures are included in the composite measure?The 13 NQF-endorsed, publically reported long-stay quality measures
What is the data source?MDS 3.0
Quality Measure Composite Score
50
Example 1: Missed Opportunities vs. Composite Score
While this facility seems to be performing well on most measures, use of antipsychotic medications burdens overall composite score.

18
Example 2: Missed Opportunities vs. Composite Score
This facility has several opportunities for improvement; focusing on incon (incontinence) and ADL (ADL decline) measures may improve the overall composite score.
Composite Score Data
53

19
56
Partnership to Improve Dementia Care
AIMS of the National Partnership
57
Improve behavioral health using individualized & person-centered approaches to care
Safeguard against inappropriate antipsychotic drug use

20
Partnership to Improve Dementia Care Update
58
National Goal: Reduce the use of antipsychotic medications in long-stay nursing home residents by 25% by the end of 2015 and 30% by the end of 2016
Alabama’s Opportunity for Improvement
59
Reporting Period2011 Quarter 4 Baseline
Average for all reporting nursinghomes- AL
27.3%
Average for all reporting nursing homes- US
23.9%
Alabama’s Opportunity for Improvement
60
Reporting Period2014 Quarter 3
Average for all reporting nursinghomes- AL
21.97%
Average for all reporting nursing homes- US
19.2%

21
Meet Needs – Build on Strengths
61
Person-Centered CareHistory / Customary Routines (MDS) / Appropriate Interventions
Outdoor Activities
Organizational GoalsConsistent Assignment
Proper Care Approach (Bathing without a Battle)
Evidence-based ProgramsMusic & Memory
Art Therapy
Montessori-Based Dementia Programming
CMS Hand-in-Hand Toolkit
CMS Change Package
Kotter’s 8-Step Process for Leading Change
TeamSTEPPs
Quality Assurance Performance Improvement
QAPI Companion Guide
CMS Nursing Home Change Package
Advancing Excellence
Quality Improvement Tools
62
Learn More
http://www.atomalliance.org/lsscc
63

22
Questions?
AQAF Two Perimeter Park South
Suite 200 WestBirmingham, AL 35242
64
This material was prepared by atom Alliance, the Quality Innovation Network-Quality Improvement Program, coordinated byQsource for Tennessee, Kentucky, Indiana, Mississippi and Alabama under a contract with the Centers for Medicare & MedicaidServices (CMS), a federal agency of the U.S. Department of Health and Humans Services. Content does not necessarily reflectCMS policy. 15.ASC2.04.020
This material was prepared by AQAF, the Medicare Quality Improvement Organization (QIO), for the
state of Alabama, under a contract with the Centers for Medicare & Medicaid Services (CMS), a federal agency of the U.S. Department of Health and Human Services. Contents do not necessarily
represent CMS policy.
65
This material was prepared by atom Alliance, the Quality Innovation Network-Quality Improvement Program, coordinated byQsource for Tennessee, Kentucky, Indiana, Mississippi and Alabama under a contract with the Centers for Medicare & MedicaidServices (CMS), a federal agency of the U.S. Department of Health and Humans Services. Content does not necessarily reflectCMS policy. 15.ASC2.04.020

Source: CMS Quality Measure, based on MDS 3.0 data. For more information see the MDS 3.0 Quality Measures Users Manual
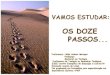
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Nursing Homes Trend Update
The National Partnership to Improve Dementia Care in Nursing Homes is committed to improving the quality of care for individualswith dementia living in nursing homes. The Partnership has a mission to deliver health care that is person-centered,comprehensive and interdisciplinary with a specific focus on protecting residents from being prescribed antipsychotic medicationsunless there is a valid, clinical indication and a systematic process to evaluate each individual’s need. The Centers forMedicare & Medicaid Services (CMS) promotes a multidimensional approach that includes; research, partnerships and state-basedcoalitions, revised surveyor guidance, training for providers and surveyors and public reporting.
CMS is tracking the progress of the Partnership by reviewing publicly reported measures. The official measure of the Partnership isthe percentage of long-stay nursing home residents who are receiving an antipsychotic medication, excluding those residentsdiagnosed with schizophrenia, Huntington's Disease or Tourette’s Syndrome. In 2011Q4 23.9% of long-stay nursing home residentswere receiving an antipsychotic medication; since then there has been a decrease of 19.4% to a national prevalence of 19.2% in2014Q3. Success has varied by state and CMS region, with some states and regions having seen a reduction of greater than 20%.
A three-quarter measure is posted to the Nursing Home Compare website at www.medicare.gov/nursinghomecompare. Thelong-stay measure on Nursing Home Compare, is the exact same measure as below, except each facility’s score is averaged overthe last three quarters in order to give consumers information on the past history of each facility.
For more information on this National Partnership, please send correspondence to [email protected].
23.6 23.7 23.9 23.823.2 23.0
22.321.7
21.1 20.820.3
19.8 19.4 19.2
2011Q2
2011Q3
2011Q4
2012Q1
2012Q2
2012Q3
2012Q4
2013Q1
2013Q2
2013Q3
2013Q4
2014Q1
2014Q2
2014Q3
Reported Quarter
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
An
tip
syc
ho
tic
Me
dic
ati
on
Pre
vale
nc
e
Start of Partnership
Quarterly Prevalence of Antipsychotic Use for Long-Stay Nursing Home Residents,2011Q2 to 2014Q3
Ba
selin
e Q
ua
rte
r

Source: CMS Quality Measure, based on MDS 3.0 data. For more information see the MDS 3.0 Quality Measures Users Manual
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Nursing Homes Trend Update
Quarterly Prevalence of Antipsychotic Use for Long-Stay Residents, CMS Regions 2011Q2 to2014Q3
Source: CMS Quality Measure, based on MDS 3.0 data. For more information see the MDS 3.0 Quality Measures Users Manual
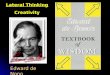
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Nursing Homes Trend Update
Quarterly Prevalence of Antipsychotic Use for Long-Stay Residents, CMS Regions 2011Q2 to2014Q3
CMS Region- and State-specific data are displayed below. These data show the change in the single-quarter prevalence ofantipsychotic medication use amongst long-stay residents since 2011Q2 and shows the change since the start of the Partnership
2011Q2
2011Q3
2011Q4
2012Q1
2012Q2
2012Q3
2012Q4
2013Q1
2013Q2
2013Q3
2013Q4
2014Q1
2014Q2
2014Q3
Reported Quarter
15.0%
17.5%
20.0%
22.5%
25.0%
27.5%
An
tip
syc
ho
tic
Me
dic
ati
on
Pre
vale
nc
e
Region 10Region 09Region 08Region 07Region 06Region 05Region 04Region 03Region 02Region 01
Start of Partnership
Region 2011Q4 2012Q1 2012Q2 2012Q3 2012Q4 2013Q1 2013Q2 2013Q3 2013Q4 2014Q1 2014Q2 2014Q3Percentage point
difference(2011Q4-2014Q3)
%Change
National 23.9% 23.8% 23.2% 23.0% 22.3% 21.7% 21.1% 20.8% 20.3% 19.8% 19.4% 19.2% -4.64 -19.4%
Region 01 26.2% 26.0% 25.1% 24.5% 23.7% 22.4% 21.6% 21.4% 20.5% 19.7% 19.4% 19.6% -6.65 -25.3%
Region 02 20.1% 20.0% 19.5% 19.4% 18.7% 18.4% 17.7% 17.4% 17.1% 16.8% 16.3% 16.2% -3.84 -19.2%
Region 03 21.8% 21.8% 21.1% 21.0% 20.6% 20.1% 19.1% 18.6% 18.1% 17.7% 17.4% 17.2% -4.62 -21.2%
Region 04 25.5% 25.4% 24.9% 24.2% 22.9% 21.7% 21.1% 20.9% 20.5% 20.2% 20.0% 19.9% -5.57 -21.8%
Region 05 22.7% 22.7% 22.1% 22.2% 21.8% 21.3% 20.9% 20.5% 19.9% 19.6% 19.1% 19.1% -3.63 -16.0%
Region 06 28.2% 28.3% 27.6% 27.6% 27.2% 26.6% 26.1% 25.6% 25.1% 24.4% 23.8% 23.2% -5.03 -17.9%
Region 07 24.5% 24.4% 23.8% 23.6% 23.4% 22.9% 22.7% 22.4% 22.1% 21.6% 21.2% 21.0% -3.49 -14.3%
Region 08 21.4% 21.5% 21.4% 20.9% 20.4% 19.8% 19.0% 18.5% 18.1% 17.8% 17.8% 17.9% -3.54 -16.5%
Region 09 21.3% 21.2% 20.4% 20.1% 19.2% 18.9% 18.4% 17.8% 17.4% 16.4% 15.9% 15.7% -5.60 -26.2%
Region 10 22.3% 22.1% 21.5% 21.3% 20.4% 20.1% 19.5% 19.1% 18.4% 18.0% 17.5% 17.4% -4.87 -21.8%

Source: CMS Quality Measure, based on MDS 3.0 data. For more information see the MDS 3.0 Quality Measures Users Manual
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Nursing Homes Trend Update
Quarterly Prevalence of Antipsychotic Use for Long-Stay Residents, States 2011Q2 to 2014Q3
Source: CMS Quality Measure, based on MDS 3.0 data. For more information see the MDS 3.0 Quality Measures Users Manual
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Nursing Homes Trend Update
Quarterly Prevalence of Antipsychotic Use for Long-Stay Residents, States 2011Q2 to 2014Q3
State 2011Q2 2011Q3 2011Q4 2012Q1 2012Q2 2012Q3 2012Q4 2013Q1 2013Q2 2013Q3 2013Q4 2014Q1 2014Q2 2014Q3Rank in2014Q3
(lower=better)
Percentage pointdifference
(2011Q4-2014Q3)
%Change
ALABAMA 27.0% 27.4% 27.3% 27.5% 26.5% 26.0% 24.0% 22.9% 22.2% 22.3% 22.2% 22.1% 22.39 21.97 44 -5.35 -19.6%
ALASKA 15.6% 15.1% 13.7% 13.4% 13.0% 13.6% 12.4% 12.5% 11.8% 15.0% 12.8% 12.7% 14.79 15.88 13 2.14 15.6%
ARIZONA 22.4% 22.5% 22.7% 22.7% 21.7% 21.6% 20.9% 20.4% 20.2% 19.9% 20.7% 18.5% 17.51 18.38 24 -4.37 -19.2%
ARKANSAS 25.7% 27.0% 26.1% 26.1% 25.3% 25.8% 25.5% 25.1% 24.4% 23.8% 22.8% 21.7% 19.91 18.78 28 -7.34 -28.1%
CALIFORNIA 21.7% 21.6% 21.6% 21.3% 20.4% 20.1% 19.2% 19.0% 18.4% 17.7% 17.1% 16.3% 15.85 15.52 12 -6.04 -28.0%
COLORADO 19.8% 19.7% 19.9% 19.9% 20.3% 19.6% 19.4% 18.5% 17.5% 17.0% 16.4% 16.4% 16.12 16.03 14 -3.87 -19.4%
CONNECTICUT 25.8% 26.1% 26.0% 25.8% 25.0% 24.3% 23.2% 22.4% 21.6% 22.0% 21.0% 20.4% 20.33 20.13 36 -5.91 -22.7%
DELAWARE 21.1% 21.0% 21.3% 21.8% 22.6% 21.9% 20.9% 18.0% 16.8% 16.8% 15.5% 15.5% 14.69 14.83 6 -6.47 -30.4%
DISTRICT OF COLUMBIA 21.4% 20.0% 20.0% 19.4% 18.8% 19.4% 18.2% 17.4% 17.6% 15.9% 14.5% 14.8% 15.04 14.72 5 -5.26 -26.3%
FLORIDA 24.2% 24.3% 24.5% 24.6% 23.8% 23.5% 23.3% 22.7% 22.1% 21.8% 21.2% 21.2% 20.63 20.60 38 -3.88 -15.9%
GEORGIA 28.4% 28.4% 28.7% 28.7% 28.0% 27.1% 24.2% 22.7% 21.8% 21.4% 21.1% 20.6% 20.33 20.11 35 -8.55 -29.8%
HAWAII 11.4% 12.2% 12.5% 13.5% 15.3% 13.2% 11.7% 11.0% 11.4% 12.1% 11.6% 8.5% 9.07 8.70 1 -3.75 -30.1%
IDAHO 26.4% 25.7% 25.3% 26.4% 25.1% 24.5% 23.9% 23.1% 21.9% 20.7% 19.3% 19.3% 18.85 18.40 25 -6.94 -27.4%
ILLINOIS 26.0% 25.8% 25.7% 25.6% 25.3% 25.7% 25.5% 25.0% 25.2% 24.8% 24.0% 24.1% 23.74 23.54 49 -2.16 -8.4%
INDIANA 23.0% 23.6% 24.0% 24.1% 22.9% 23.1% 22.2% 21.7% 20.9% 21.0% 20.2% 19.9% 19.24 19.02 30 -5.01 -20.8%
IOWA 22.2% 22.3% 22.3% 22.0% 21.7% 21.1% 20.6% 20.2% 20.2% 19.9% 20.0% 19.7% 19.31 19.19 33 -3.15 -14.1%
KANSAS 26.1% 26.5% 26.1% 26.1% 25.2% 25.3% 25.1% 24.2% 23.9% 23.5% 23.0% 23.1% 22.83 23.15 48 -2.96 -11.3%
KENTUCKY 25.5% 25.2% 26.0% 26.0% 25.2% 24.4% 23.1% 21.9% 22.0% 21.8% 21.6% 21.2% 20.90 21.15 41 -4.83 -18.6%
LOUISIANA 29.7% 29.9% 29.7% 29.7% 29.1% 28.9% 28.6% 27.8% 27.0% 26.6% 26.5% 25.5% 25.15 25.03 51 -4.69 -15.8%
MAINE 26.4% 26.7% 27.2% 26.9% 25.9% 25.1% 24.2% 22.6% 21.7% 21.3% 20.1% 18.5% 18.16 19.11 31 -8.14 -29.9%
MARYLAND 19.5% 19.8% 19.8% 19.6% 18.5% 17.8% 17.7% 17.3% 16.7% 15.6% 15.9% 15.9% 15.80 15.38 10 -4.41 -22.3%
MASSACHUSETTS 26.6% 26.7% 26.7% 26.6% 25.4% 25.1% 24.5% 22.9% 22.2% 21.8% 21.2% 20.6% 20.18 20.13 37 -6.59 -24.7%
MICHIGAN 16.2% 16.0% 16.4% 16.4% 15.8% 16.0% 15.5% 14.9% 14.4% 14.1% 13.9% 13.7% 13.35 13.33 2 -3.06 -18.7%
MINNESOTA 18.9% 19.0% 19.0% 18.8% 18.1% 18.0% 18.0% 17.9% 17.3% 16.7% 16.6% 16.0% 15.33 15.14 8 -3.89 -20.4%
MISSISSIPPI 26.6% 26.8% 26.6% 26.3% 26.6% 26.1% 25.3% 24.7% 24.4% 25.3% 24.3% 23.8% 23.00 23.04 47 -3.53 -13.3%
MISSOURI 25.5% 26.0% 26.1% 26.0% 25.3% 25.2% 24.9% 24.6% 24.4% 23.7% 23.1% 22.2% 21.62 20.78 40 -5.36 -20.5%
MONTANA 21.6% 22.0% 21.5% 21.5% 19.5% 19.7% 19.5% 19.7% 19.2% 18.1% 17.2% 16.9% 16.29 16.95 17 -4.53 -21.1%
NEBRASKA 22.7% 22.4% 22.3% 22.9% 22.6% 22.6% 22.9% 22.5% 22.2% 22.8% 22.7% 22.0% 21.36 21.68 42 -0.64 -2.9%
NEVADA 22.2% 20.7% 20.3% 20.5% 21.1% 19.7% 20.2% 20.1% 20.4% 19.9% 19.7% 19.1% 18.77 19.31 34 -0.96 -4.7%
NEW HAMPSHIRE 25.7% 25.4% 25.5% 25.1% 24.0% 23.8% 23.7% 22.7% 21.1% 21.2% 20.1% 18.8% 18.37 18.61 27 -6.92 -27.1%
NEW JERSEY 17.0% 18.2% 17.9% 17.8% 17.5% 17.4% 17.1% 16.6% 15.9% 15.4% 15.1% 14.5% 14.16 14.26 4 -3.65 -20.4%
NEW MEXICO 22.4% 22.3% 21.7% 22.0% 20.0% 20.4% 22.2% 20.3% 20.7% 17.7% 18.1% 19.5% 17.29 16.86 16 -4.81 -22.2%
NEW YORK 22.0% 21.6% 21.3% 21.4% 20.8% 20.6% 19.7% 19.5% 18.9% 18.7% 18.2% 18.0% 17.64 17.42 20 -3.89 -18.3%
NORTH CAROLINA 21.1% 20.8% 21.4% 21.3% 20.7% 19.9% 18.0% 16.5% 16.0% 15.8% 15.6% 15.0% 14.84 15.40 11 -6.05 -28.2%
NORTH DAKOTA 20.8% 21.4% 21.3% 21.2% 20.6% 20.4% 19.8% 19.1% 18.5% 18.3% 18.7% 18.0% 18.26 19.01 29 -2.30 -10.8%
OHIO 24.9% 25.0% 25.4% 25.4% 25.0% 24.8% 24.5% 24.1% 23.3% 22.7% 22.0% 21.6% 21.59 21.78 43 -3.66 -14.4%
OKLAHOMA 26.7% 26.8% 27.3% 27.5% 27.3% 26.6% 25.5% 23.0% 22.7% 22.3% 21.7% 21.5% 20.95 20.70 39 -6.63 -24.3%
OREGON 20.6% 21.0% 21.5% 21.3% 20.0% 19.9% 19.2% 19.1% 18.6% 18.8% 18.3% 18.4% 17.08 17.81 22 -3.67 -17.1%
PENNSYLVANIA 21.6% 22.1% 22.3% 22.2% 21.7% 21.7% 21.1% 20.5% 19.4% 19.2% 18.8% 18.3% 17.92 17.64 21 -4.66 -20.9%
RHODE ISLAND 23.0% 23.8% 24.0% 23.9% 23.1% 21.7% 20.2% 20.3% 19.3% 18.4% 17.5% 16.9% 16.54 16.99 19 -7.00 -29.2%
SOUTH CAROLINA 20.6% 20.5% 20.7% 20.6% 20.7% 20.2% 18.3% 17.2% 16.9% 15.9% 15.5% 15.3% 15.64 15.25 9 -5.45 -26.3%
SOUTH DAKOTA 21.8% 21.8% 21.5% 21.5% 21.3% 21.4% 20.5% 20.0% 18.8% 18.1% 18.6% 18.0% 18.06 18.17 23 -3.36 -15.6%
TENNESSEE 29.3% 29.5% 30.0% 29.3% 29.0% 27.7% 27.2% 25.0% 23.9% 24.0% 23.4% 23.1% 22.72 22.54 45 -7.42 -24.8%

Source: CMS Quality Measure, based on MDS 3.0 data. For more information see the MDS 3.0 Quality Measures Users Manual
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Nursing Homes Trend Update
Quarterly Prevalence of Antipsychotic Use for Long-Stay Residents, States 2011Q2 to 2014Q3
State 2011Q2 2011Q3 2011Q4 2012Q1 2012Q2 2012Q3 2012Q4 2013Q1 2013Q2 2013Q3 2013Q4 2014Q1 2014Q2 2014Q3Rank in2014Q3
(lower=better)
Percentage pointdifference
(2011Q4-2014Q3)
%Change
TEXAS 28.4% 28.5% 28.8% 28.9% 28.2% 28.3% 28.0% 27.9% 27.3% 27.0% 26.5% 25.7% 25.28 24.56 50 -4.29 -14.9%
UTAH 26.9% 24.7% 27.1% 26.9% 27.1% 26.3% 26.4% 25.0% 24.5% 23.6% 21.7% 21.7% 23.13 22.83 46 -4.28 -15.8%
VERMONT 25.5% 26.1% 25.4% 25.7% 26.2% 24.9% 23.4% 20.3% 20.2% 20.2% 18.8% 18.2% 18.00 19.18 32 -6.22 -24.5%
VIRGINIA 22.4% 22.8% 23.0% 22.9% 21.8% 21.9% 22.1% 22.1% 21.0% 20.5% 19.7% 19.0% 18.21 18.51 26 -4.53 -19.7%
WASHINGTON 22.8% 23.0% 22.3% 21.8% 21.7% 21.6% 20.6% 20.2% 19.7% 19.1% 18.6% 17.8% 17.45 16.99 18 -5.34 -23.9%
WEST VIRGINIA 20.1% 20.3% 20.5% 21.5% 20.4% 20.7% 20.4% 19.8% 19.0% 18.0% 16.5% 16.1% 16.55 16.20 15 -4.29 -20.9%
WISCONSIN 18.7% 18.7% 19.0% 18.9% 18.9% 19.0% 18.0% 17.7% 17.4% 16.8% 16.3% 15.4% 14.58 14.23 3 -4.82 -25.3%
WYOMING 17.8% 18.4% 16.8% 16.9% 19.4% 16.8% 17.5% 17.0% 16.5% 17.2% 17.9% 16.5% 15.56 15.09 7 -1.73 -10.3%

Frequently Asked Questions About the National Nursing Home Quality Care Collaborative (NNHQCC) Composite Measure July 2014 Q1: What is the NNHQCC Composite Measure? A: The NNHQCC composite measure is a tool that can be used to help monitor NNHQCC progress. Nursing homes participating in the NNHQCC focus on processes that improve their systems and measure individual tests of change. Specifically, they look at their Plan-Do-Study-Act (PDSA) improvement cycle results, clinical outcomes measures and composite scores. The composite measure is not intended to replace or supersede existing local or federal initiatives, including the 5-star rating system, but is offered as another way to look at quality from a systems perspective. Q2: Which quality measures are included in the composite measure? A: The composite is comprised of 13 NQF-endorsed, publically reported, long-stay quality measures that represent larger systems within the long term care setting:
Q3: What is the data source? A: Facility-level quality measure numerators, denominators and rates derived from the MDS 3.0 are extracted from the Quality Improvement and Evaluation System (QIES) Workbench for rolling six-month time periods on a monthly basis and used to calculate the composite score. There is a two-month delay from the last month of the time period. For example, the January through June time period would be extracted on the first business day after the first weekend in September; the February through July time period would be extracted on the first business day after the first weekend in October; the March through August time period would be extracted on the first business day after the first weekend in November, and so forth.
1. Percent of residents with one or more falls with major injury 2. Percent of residents with a urinary tract infection (UTI) 3. Percent of residents who self-report moderate to severe pain 4. Percent of high-risk residents with pressure ulcer 5. Percent of low-risk residents with loss of bowels or bladder 6. Percent of residents with catheter inserted or left in bladder 7. Percent of residents physically restrained 8. Percent of residents whose need for help with Activities of Daily
Living (ADL) has increased 9. Percent of residents who lose too much weight
10. Percent of residents who have depressive symptoms 11. Percent of residents who received antipsychotic medications 12. Percent of residents assessed and appropriately given the seasonal
influenza vaccine 13. Percent of residents assessed and appropriately given the
pneumococcal vaccine

Q4: How is the composite score calculated? A: The composite score is calculated based on the “opportunity model” concept. Numerators and denominators are summed across all 13 quality measures to determine the composite numerator and denominator. The composite numerator is then divided by the composite denominator and multiplied by 100 to obtain the composite score. (Please note that before the numerators and denominators can be summed, the direction of the two vaccine measures must be reversed because they are directionally opposite of the others. This can be done by subtracting the vaccine numerator from the vaccine denominator to obtain a “reversed” numerator. This “reversed” numerator is what should be counted in the composite numerator. By keeping all measure directions consistent, the composite score can be interpreted as the lower, the better.) Q5: Why are there fluctuations in the season influenza vaccine measure rates? A: Fluctuations in vaccine measure rates, across the six-month time periods, are expected. These are likely attributable to two factors: 1) the time period ends at the beginning or during the flu season, when many residents haven’t yet had the chance to be assessed and appropriately given the vaccine; and 2) the definition of “current” flu season may vary among healthcare providers and across states. Q6. How is the composite score evaluated? A: The NNHQCC seeks to rapidly spread the practices of high performing nursing homes with the aim of ensuring that every nursing home resident receives the highest quality of care. Specifically, the NNHQCC strives to instill quality and performance improvement practices, eliminate healthcare acquired conditions, and dramatically improve resident satisfaction through the achievement of a rate of 6 or less. Q7: How was the goal of “6 or less” established? A: Prior to the launch of the NNHQCC, nearly 10 percent of the nation’s nursing homes had achieved a composite score of 6 or less. Additionally, the 10 nursing homes identified for “best practices” site visits had an average composite score close to 6, and the national benchmark, using the Achievable Benchmarks of Care (ABC) method, was around 6. Q8: Will Quality Improvement Network-Quality Improvement Organizations (QIN-QIOs) be able to calculate their state and individual nursing homes scores? A: QIN-QIOs can calculate their state aggregate and individual nursing home composite scores using the facility-level data files provided by the National Coordinating Center (NCC) and following the method of composite score calculation as described earlier. The files provided by the NCC contain individual measure and composite measure numerators, denominators, and rates for every facility within their state. A second option is to download the individual measure data from CASPER (Certification and Survey Provider Enhanced Reports) and follow the same method for calculating the composite score. However, the two vaccination measures are not reported on CASPER and would have to be excluded 3 from the composite measure if using this data source to calculate state and individual nursing home composite scores. (See Attachment 1 “Information Regarding the Percent of Long-Stay Residents Assessed and Appropriately Given the Seasonal Influenza Vaccine Nursing Home Quality Measure”)

Q9: Some community-based nursing facilities are not Medicare or Medicaid certified. Are they included in the state composite score? A: Nursing homes without a CMS Certification Number (CCN) cannot be included when calculating a composite score. Q10: Can nursing homes calculate their own composite scores? A: Nursing homes can approximate their own composite scores using the publically available data on Nursing Home Compare, although the time frames reported there are different than the rolling six-month time periods used to monitor progress in the Collaborative. Nursing homes could also use CASPER data, although the two vaccination measure are not reported there and would have to be excluded from the composite measure if using this data source to calculate the composite score. Q11: Can QIN-QIOs share individual nursing home composite scores with corporations or other stakeholders? A: QIN-QIOs must follow provisions outlined in Part B of Title XI of the Social Security Act (the Act). Sections 1154, 1156, and 1160 provide the basis for the acquisition, protection, and disclosure of information. 42 CFR Part 480 implements the above referenced provisions of the Act. “Confidential information” includes information that explicitly or implicitly identifies an individual patient, practitioner, institution, or reviewer. Practitioner, reviewer and provider confidential information may only be disclosed to the identified practitioner, reviewer or provider, and this would include only information about them. Disclosure to others requires the written consent of the identified practitioner, reviewer or provider. QIN-QIOs should follow their organization’s QIN-QIO contractual confidentiality and disclosure policies. Q12: Are there significant differences in the composite scores across the nation? A: Composite scores vary across facilities and states.
This material was prepared by atom Alliance, the Quality Innovation Network-Quality Improvement Organization (QIN-QIO), coordinated by Qsource for Tennessee, Kentucky, Indiana, Mississippi and Alabama, under a contract with the Centers for Medicare & Medicaid Services (CMS), a federal agency of the U.S. Department of Health and Human Services. Content does not necessarily reflect CMS policy. 14.ASC2.11.032

Attachment 1
Information Regarding the “Percent of Long-Stay Residents Assessed and Appropriately Given the Seasonal Influenza
Vaccine” Nursing Home Quality Measure Background Seasonal fluctuations have been noted in the “percent of long-stay residents assessed and appropriately given the seasonal influenza vaccine” nursing home quality measure rates for rolling six-month time periods that are updated on a monthly basis (and, to a much lesser extent, also in the “percent of long-stay residents assessed and appropriately given the pneumococcal vaccine” nursing home quality measure rates for rolling six-month time periods which are updated on a monthly basis). The change appears to peak during the May through October time period before returning to normal at the November through April time period. The graph below illustrates the fluctuations. These fluctuations are likely attributable to two factors: 1) the time period ends at the beginning or during the flu season when many residents haven’t yet had the chance to be assessed and appropriately given the vaccine; and 2) the definition of “current” flu season may vary among healthcare providers and across states.
Flu and pneumonia vaccine opportunity rates (percent of residents not yet immunized): Dec. 2011-April 2014
Timing of Vaccination and Assessment Because the rolling six-month time periods are updated on a monthly basis (dropping the first month and adding the next month at each cycle), time periods that end with a month or two at the beginning or during the flu season are likely to include residents who have not yet been vaccinated for the current season that just started. Since all residents cannot be vaccinated simultaneously on Day 1 of the flu season, the six-month time periods that end on a month or two of the flu season are likely to include more residents who have not had a chance to be vaccinated or assessed. This explains the seasonal peak we consistently observe in the influenza measure rates as depicted in the graph above. Although the Pneumococcal vaccination is a year-around activity, the subtle fluctuation we also observe for the pneumococcal vaccination during the flu season may be due to the fact that some healthcare providers may tend to intensify pneumococcal vaccination assessment during the flu season as well.

Defining Flu Season The current MDS 3.0 Resident Assessment Instrument (RAI) Manual indicates that flu season varies annually and geographically, ending “when influenza is no longer active in your geographic area.” For more information, the manual suggests that healthcare providers visit the Centers for Disease Control and Prevention (CDC) website which states that the flu season can occur as early as October and advises them to “begin offering vaccination soon after vaccine becomes available and, if possible, before October.” Additionally, some states have their own definition of flu season that can begin earlier than October. The inconsistency in the timing of the flu season may explain why small changes in the measure rate begin during the six-month time periods before the biggest change in the measure rate during the May through October six-month time period. What Does This Mean? • We will likely continue to see fluctuations in the immunization measures that will affect the
overall Composite Measure used to assess progress in the National Nursing Home Quality Care Collaborative.
• The immunization measures will remain in the Composite Measure, given the important vaccine benefits to nursing home residents.
• This fluctuation does not necessarily mean that any nursing home is out of compliance with providing timely vaccinations.
• Nursing homes should be encouraged and supported to immunize all residents appropriately in a timely manner.
This material was prepared by atom Alliance, the Quality Innovation Network-Quality Improvement Organization (QIN-QIO), coordinated by Qsource for Tennessee, Kentucky, Indiana, Mississippi and Alabama, under a contract with the Centers for Medicare & Medicaid Services (CMS), a federal agency of the U.S. Department of Health and Human Services. Content does not necessarily reflect CMS policy. 14.ASC2.11.032