Embed Size (px)
Citation preview
Review A rtic I es
Alcohol and diabetes-what should we tell our patients?
H Connor MD FRCP Consultant Physician, County Hospital, Hereford HR1 2ER
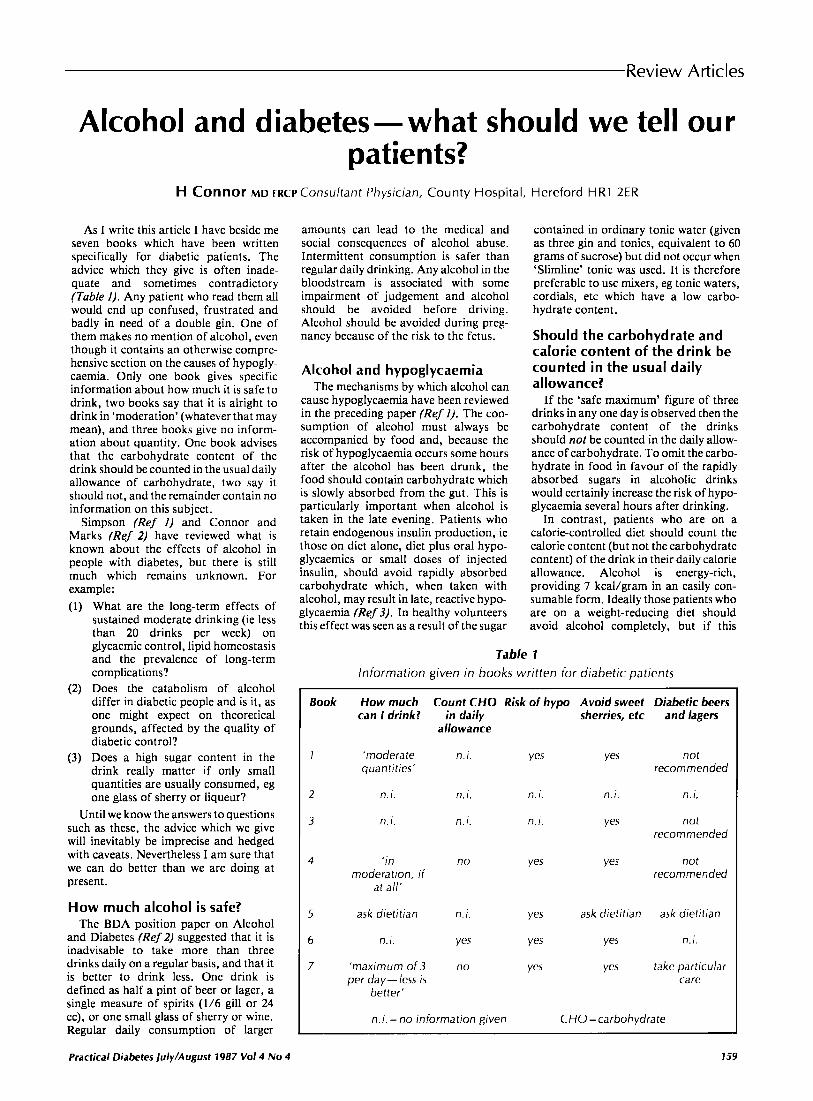
As I write this article I have beside me seven books which have been written specifically for diabetic patients. The advice which they give is often inade- quate and sometimes contradictory (Table I ) . Any patient who read them all would end up confused, frustrated and badly in need of a double gin. One of them makes no mention of alcohol, even though it contains an otherwise compre- hensive section on the causes of hypogly- caemia. Only one book gives specific information about how much it is safe to drink, two books say that it is alright to drink in ‘moderation’ (whatever that may mean), and three books give no inform- ation about quantity. One book advises that the carbohydrate content of the drink should be counted in the usual daily allowance of carbohydrate, two say it should not, and the remainder contain no information on this subject.
Simpson (Ref I) and Connor and Marks (Ref 2) have reviewed what is known about the effects of alcohol in people with diabetes, but there is still much which remains unknown. For example:
What are the long-term effects of sustained moderate drinking (ie less than 20 drinks per week) on glycaemic control, lipid homeostasis and the prevalence of long-term complications? Does the catabolism of alcohol differ in diabetic people and is it, as one might expect on theoretical grounds, affected by the quality of diabetic control? Does a high sugar content in the drink really matter if only small quantities are usually consumed, eg one glass of sherry or liqueur? ntil we know the answers to questions
such as these, the advice which we give will inevitably be imprecise and hedged with caveats. Nevertheless I am sure that we can d o better than we are doing at present.
How much alcohol is safe? The BDA position paper on Alcohol
and Diabetes (Ref 2) suggested that it is inadvisable to take more than three drinks daily on a regular basis, and that it is better to drink less. One drink is defined as half a pint of beer or lager, a single measure of spirits (1/6 gill or 24 cc), or one small glass of sherry or wine. Regular daily consumption of larger
Practical Diabetes july/August 1987 V o l 4 No 4
amounts can lead to the medical and social consequences of alcohol abuse. Intermittent consumption is safer than regular daily drinking. Any alcohol in the bloodstream is associated with some impairment of judgement and alcohol should be avoided before driving. Alcohol should be avoided during preg- nancy because of the risk to the fetus.
Alcohol and hypoglycaemia The mechanisms by which alcohol can
cause hypoglycaemia have been reviewed in the preceding paper (Ref I). The con- sumption of alcohol must always be accompanied by food and, because the risk of hypoglycaemia occurs some hours after the alcohol has been drunk, the food should contain carbohydrate which is slowly absorbed from the gut. This is particularly important when alcohol is taken in the late evening. Patients who retain endogenous insulin production, ie those on diet alone, diet plus oral hypo- glycaemics or small doses of injected insulin, should avoid rapidly absorbed carbohydrate which, when taken with alcohol, may result in late, reactive hypo- glycaemia (Ref 3). In healthy volunteers this effect was seen as a result of the sugar
contained in ordinary tonic water (given as three gin and tonics, equivalent to 60 grams of sucrose) but did not occur when ‘Slimline’ tonic was used. It is therefore preferable to use mixers, eg tonic waters, cordials, etc which have a low carbo- hydrate content.
Should the carbohydrate and calorie content of the drink be counted in the usual daily allowance?
If the ‘safe maximum’ figure of three drinks in any one day is observed then the carbohydrate content of the drinks should not be counted in the daily allow- ance of carbohydrate. To omit the carbo- hydrate in food in favour of the rapidly absorbed sugars in alcoholic drinks would certainly increase the risk of hypo- glycaemia several hours after drinking.
In contrast, patients who are on a calorie-controlled diet should count the calorie content (but not the carbohydrate content) of the drink in their daily calorie allowance. Alcohol is energy-rich, providing 7 kcal/gram in an easily con- sumable form. Ideally those patients who are on a weight-reducing diet should avoid alcohol completely, but if this
Table 1 ln format ion given in books wr i t ten for diabetic patients
Book
I
2
3
4
5
6
7
How much Count CHO Risk of hypo Avoid sweet Diabetic beers can I drink? in daily sherries, etc and lagers
allowance
’moderate n. i . yes yes not quantities’ recommended
n. i . f l . 1 . n. i . n. i . n.i.
n. i . n. i. f l . 1 . yes not recommended
‘ in n 0 Ye5 ves not moderation, if recommended
at all’
ask dietitian n. i . Yes ask dietitian ask dietitian
n. I . yes Yes Yes n. i .
‘maximum of 3 no yes yes take particular per day- less is care
better‘
n.i. =no information given C H O = carbohydrate
759

Review Articles Alcohol and diabetes- what should we fell our patients?
advice is not acceptable they should ensure that the calorie content obtained from alcohol does not exceed 10% of their daily calorie allowance, ie a maxi- mum of one drink daily on 1,OOO kcal diet.
Are some drinks better or worse than others?
Most of the books written for diabetic patients advise that sweet sherries and wines should be avoided (Table I), How- ever, I know of no clinical studies which support this advice. A glass of sweet sherry (95 gill or 50 cc) or of a sweet white wine (4 fluid oz or 113 cc) contains approximately 6 grams of carbohydrate which is no more than that found in half a pint (275 cc) of many beers (Ref 4), and considerably less than the quantity of sucrose which is needed to cause a late r e a c p hypoglycaemia (Ref 3). Even liquers, which patients are usually told to avo& contain only about 6 grams of carbohydrate per 1/6 gill (24 cc). A total embargo on sweet wines, sherries and liqueurs may not be justifiable.
Patients are usually advised to avoid low carbohydrate beers and lagers (Table I) on the grounds that, although they contain less carbohydrate, they often have a higher alcohol content than ordinary beers and lagers. This advice is supported by the results of Henderson et a1 (Ref 5) who compared the effects of four different beers (carbohydrate content 1.4-12.1 grams per 55 pint; alcohol concentration 3.5-5.5qo v/v) on short-term glycaemic control (12 hours) in seven insulin-dependent men. They found that the peak increment in blood glucose concentration was linearly related to the carbohydrate content of the beer and that low-carbohydrate beers were more likely to be associated with fasting hypoglycaemia the next morning. They concluded that patients who follow the BDA guidelines on alcohol consump- tion (Ref 2) should choose a beer or lager with a carbohydrate content of 3-7 grams per Yz pint and an alcohol concentration of <5%. About half the beers and lagers listed in Countdown (Ref 4) meet these criteria.
Alcohol and hypertriglyceridaemia
Alcohol abuse is associated with hyper- triglyceridaemia (Ref I) and even modest
amounts of alcohol may cause hypertri- glyceridaemia in some subjects. If alcohol is suspected as a cause of hyper- triglyceridaemia the blood test should be repeated after the patient has abstained for 2-3 weeks (Ref 2).
Alcohol and diabetic co m p I ica tio n s
There is some evidence that both neuropathy and retinopathy are com- moner in those who take more than 20 drinks per week. The BDA position paper (Ref 2) suggests that patients with neuropathy should limit their consump- tion to a maximum of one drink daily.
Alcohol and oral hypoglycaemic agents
Alcohol ingestion was an associated factor in some cases of phenformin- induced lactic acidosis, but clinical experience suggests that it is quite safe for patients treated with metformin to take small amounts of alcohol, eg one to two drinks in any one day (Ref 2).
Acute ingestion of alcohol can inhibit the metabolism of tolbutamide, but pro- longed heavy consumption induces hepatic enzyme induction and increases the metabolism of tolbutamide. Whether these effects are of clinical importance has not been investigated, though inhibi- tion to tolbutamide metabolism can occur with blood alcohol concentrations of about 80 mg per 100 ml (Ref 2).
A minority of patients who are treated with chlorpropamide will develop facial flushing when they drink alcohol, and some pharmacists now label all bottles of chlorpropamide with an instruction to ‘avoid alcohol’. I consider that this total embargo is unjustified, because only a very small number of patients are really bothered by this side effect.
It is the duty of the prescriber to warn patients of the possibility of facial flush- ing and to offer to try a different tablet if flushing does occur and the patient finds it uncomfortable or embarrassing.
Summary of recommendations of patients
The following recommendations are based on those given in the BDA position paper on Alcohol and Diabetes (Ref 2): (1) Three drinks in any one day is the
maximum acceptable consumption of
alcohol. It is better todrink less, and it is safer not to drink every day. One drink is taken to mean % pint (275 cc) of beer, lager or cider, or a single measure of spirits (1/6 gill, 24 cc), or a single glass of wine (4 fl oz, 113 cc) or a single glass of sherry (% gill, 50 cc).
(2) If recommendation one is observed the carbohydrate content of the drink should not be counted in the daily allowance of carbohydrate.
(3) Beers, lagers and ciders should have a carbohydrate content of 3-7 grams per Yz pint and an alcohol content of
(4) Food should accompany or follow soon after the ingestion of alcohol, but simultaneous absorption of rapidly absorbed carbohydrate is best avoided, and mixers such as tonic waters should have a low carbo- hydrate content to minimise the risk of late reactive hypoglycaemia in those who retain some endogenous insulin production.
( 5 ) Patients should be warned that hypo- glycaemia may occur several hours after they have drunk alcohol, and that the cerebral effects of alcohol may obscure or modify their usual hypoglycaemic symptoms.
(6) Patients on a weight-reducing diet should seek medical or dietetic advice before drinking alcohol. If they do drink, the calorie content of the alcohol should be counted in their daily calorie allowance and should not exceed 10% of total calorie consump- tion.
(7) Patients treated with chlorpropamide should be warned about the possibility of facial flushing.
<5% V/V.
References 1 . Simpson HCR. Metabolic effects of alcohol in
diabetes. Practical Diabetes, 1987; 4: ??-??. 2. Connor H, and Marks V. Alcohol and
Diabetes. Diabetic Medicine, 1985; 2: 413-6, and simultaneous publication in Human Nutrition: Applied Nutrition, 1985; 39A: 393-9.
3. O’Keefe SJD, and Marks V. Lunchtimegin and tonic, a cause of reactive hypoglycaernia. Lancet, 1977; 1: 1286-9.
4. Countdown. British Diabetic Association, 2nd edition, 1985; 237-62.
5. Henderson B. Atkin GE. Henderson E et al. The effect of difffrent beers on blood glucose concentration in insulin-dependent diabetes. Prac- tical Diabetes, 1987; in press.
Back copies of Practical Diabetes R x k c opies of Practical Diabetes are available to NUS health professionals at €1.50 each
Send your order and cheque/money order to the publishers:
The Newbourne Group, Greater London House Hampstead Road, London NW7 7QQ
160 Practical Diabetes /uly/Augusl 1987 Vol4 No 4















![RESEARCH Open Access Effects of body weight and alcohol ... · decreasing the risk of type-2 diabetes [2,8]. Alcohol con-sumption may decrease the risk of type-2 diabetes by promoting](https://img.pdfslide.net/doc/110x75/5f0acbaf7e708231d42d61df/research-open-access-effects-of-body-weight-and-alcohol-decreasing-the-risk.jpg)












