Embed Size (px)
Citation preview

Alcohol Policy
Thomas K. Greenfield, Ph.D.
Alcohol Research Group Public Health Institute
Emeryville, California;
Department of Psychiatry, UCSF
Editor: Jűrgen Rehm, Ph.D. University of Toronto and CAMH
(Supported in part by Center Grant P30 AA05595)

Alcohol Policies: Overall Approach Will consider first the underlying epidemiology
– Alcohol consumption; overall trends and drinking patterns– health and social consequences – clues for policy levers?
Give an overview of the range of types of policies– First identify historical and cultural backdrop for US policies – Types of alcohol policies – jurisdictional level; role of
enforcement. Emphasis will be on evidentiary basis – Treatment policies are not addressed – other than costs
Other issues– Touch on several other issues like policy development,
optimal policy mix, pragmatic versus ‘ideal’ policies

Alcohol Policies: Levels, Types, IssuesJurisdictional Level
– Federal, state, county, municipal; as well as – institutional
Type– Legislatively Based (e.g., taxation/pricing, access,
advertising regulation, transportation rules, etc.) – Law Enforcement (e.g., policing, random breath testing,
and justice system)– Institutional/Organizational policies (e.g., server
intervention, schools, workplace, military)– International Policies (e.g., trade agreements, treaties)
Issues– Cutting edge issue: what is the appropriate policy mix?– The role of science in policy development/implementation

Prevention Policies
“[Prevention policies] are all policies that operate in a non- personalized way to alter the set of contingencies affecting individuals as they drink or engage in activities that (when combined with intoxication) are considered risky.”1
“Alcohol policy is defined broadly as any purposeful effort or authoritative decision on the part of government or non-government groups to minimize or prevent alcohol-related consequences.” 2
1Moore & Gerstein (1981), p 53 Beyond the Shadow of Prohibition2Babor et al. (2003), p 95 Alcohol: No Ordinary Commodity

Reductions in Problems During Prohibition
Measure Dates Change
Cirrhosis mortality 1911–1929 29.5 to 10.7 per 100,000
Admissions for alcoholic psychosis
1919–1928 10.1 to 4.7 per 100,000
Arrests for drunk & disorderly
1916–1922 50% decline
Source: Moore & Gerstein, 1981
Prohibition took effect January 1920, lasted to December 1933Impact had two stages—first years: changed drinking patterns;second period: lawlessness, crime and loss of legitimacy.
Source: Berridge, 2003, citing Burnham, 1968-69

Repeal: Alcohol Control• 1932: Roosevelt campaigns for repeal of 18th Amendment• December 1933: 21st Amendment (Repeal) ratified by 35 states • Alcohol Control becomes “a pivotal idea” in post-Repeal era
– Federal• regulate production of spirits, wine & beer (curb illegal production)• manage product purity and labeling; impose excise taxes• Authority with Department of Justice (ATF since 1972; now ATFE)
– State• Devolved Powers including dry option, retail monopolies, taxation• Alcoholic Beverage Control (ABC Laws); outlet licensing, density, etc.
– Local• Dry Counties; Zoning regulation, policing outlets, etc.
Sources: Levine 1980; Moore & Gerstein, 1981

Sources: Lakins, Williams, Yi, & Smothers (2004); Kerr, Greenfield, Tujague, & Brown (2005)
U.S. Per Capita Consumption of Pure Alcohol from Beer, Wine and Spirits
0.00
0.25
0.50
0.75
1.00
1.25
1.50
1.75
2.00
2.25
2.50
2.75
3.00
1950
1952
1954
1956
1958
1960
1962
1964
1966
1968
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
Ga
llon
s o
f Alc
oh
ol
SpiritsWineBeerTotal AlcoholAEDS SpiritsAEDS WineAEDS BeerAEDS Total

Optimal Policy Approaches: A Controversy Resolved?
• Single Distribution Theory (Skog improving Ledermann).Argues that a substantial decrease in a population’s mean (or per capita) consumption will be accompanied by a decrease in the prevalence of heavy drinkers; supports policy measures like taxation aimed at achieving overall reduction
• Harm Reduction: Abates Hazardous Drinking Patterns. Attention is less on trying to modify everyone’s drinking, be it light or heavy, and more on policy measures targeting heavy quantity per occasion drinking patterns; high quantity contexts
Sources: Skog, 1985; Edwards et al, 1994;Rehm et al, 1996; Stockwell et al, 1997; 1Babor et al, 2003
“Per capita alcohol consumption is … related to the prevalence of heavy use, which in turn is associated with … negative effects”1

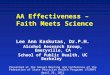
Concentration of U.S. Alcohol Consumption
0
20
40
60
80
100
2.5 5 10 20 30 40 50 60 70 80 90 100
Highest Volume Percentile of Drinkers Lowest Volume
% T
otal
V
olum
e (g
/day
)Cumulative Percent Volume (g/day)
Source: adapted from Greenfield & Rogers, JSA,1999
Top 10% drinking > 3 drinks/day: 58% of Total
Top 5% drinking > 4 drinks/day: 40% of Total

Hazardous Drinking: U.S. Percentage
81%
4%
15%
Beer
Wine
Spirits
OF TOTAL OF BEVERAGE
Source: adapted from Rogers & Greenfield, JSA,1999
63%
86%
41%59%
14%
37%
0% 20% 40% 60% 80% 100%
Hazardous Nonhazardous Share
58.4%
26.7%
14.9%
(Hazardous drinking occurs more in bars, other people’s parties, and public places)

Alcohol-attributable Mortality 2002 (number of deaths) –Epidemiological Model for Americas and World
Americas
2002 best estimates
% of all alcohol-
attributable
World % of all alcohol-
attributable
Maternal perinatal condit. 203 0.1% 3,057 0.2%
Cancer 47920 16.7% 377,968 21.2%
Neuro-psychriatric condit. 28733 10.0% 113,603 6.4%
Vascular conditions -5154 -1.8% 196,646 11.0%
Oth. noncommun diseases 52557 18.4% 237,985 13.3%
Unintentional injury 92661 32.4% 585,553 32.8%
Intentional Injury 69430 24.3% 269,155 15.1%
All alcohol-related deaths 286346 100.0% 1,783,567 100.0%
% alcohol-attributable of all deaths 4.8% 3.1%
Sources: Adapted from Rehm, Room, Monteiro, et al., 2003; Rehm & Monteiro, 2005

Economic costs of alcohol abuse by type, 1998
14%
48%
20%
18%Direct Costs
Morbidity Costs
Mortality Costs
Other Costs
U.S. Data
Source: Harwood, Fountain & Livermore, 1998;NIAAA, 2000http://pubs.niaaa.nih.gov/publications/economic-2000/printing.htm
(e.g., crime, crashes)
(e.g., medical)
(lost productivity)
(lost future earnings)
•Total: $184.6 Billion
$26.3 Billion
$88.1 Billion
$36.0 Billion
$34.2 Billion

Jurisdictional Levels: Example Policies
Federal • Excise taxes• Transportation (e.g., Minimum Drinking Age, aviation)• Commercial regulation, production, advertising, marketing• Warning Labels, Dietary Guidelines, etc.
State• State alcohol taxes• Access: alcohol distribution systems, State ABCs, retail
monopolies, local options, regulating outlets, labeling, etc. • Server licensing, training, dram shop or server liability• Drinking driver laws: mandatory license actions, treatment,etc.

Price and Taxation Policies
Studies at both federal and state levels show:
• generally, significant price effect on consumption owing to taxation
• quality substitution, market, etc., may partially neutralize price effects • effects seen for heavier drinkers as well as lighter ones• Well-designed studies have found effects on population-level problem
indicators: cirrhosis mortality, vehicular crashes• not particularly regressive tax measure compared to other commodity
taxes—there is a lower burden on the poor; youth are affected
• supported by public health experts, anathema to industry
Sources: Coate & Grossman, 1988; Babor et al, 1978; Cook & Tauchen, 1982; Edwards et al, 1994; Gruenewald & Treno, 2000; Chaloupka et al, 2002

Relative Price of Alcoholic Beverages, 1970-2005
1.00
2.00
3.00
4.00
5.00
6.00
1970
1975
1980
1985
1990
1995
2000
2005
AlcoholicBeverages
Consumer PriceIndex
Non-AlcoholicBeverages
Sources: Mosher, 1997; Mosher & Cowan, 1985;Bureau of Labor Statistics, 2006 (www.bls.gov)
Relative Price, 1970 $

U.S. Drinking Driving Legislative PoliciesMinimum Drinking Age (MDA)
• Federal law required 21 year old MDA for states to receive national highway funds (incentive to comply)
• By mid 1980’s all states adopted uniform MDA of 21• Changes before and after federal law provide natural
experiments: most studies found reductions in crashes
Evidence• Crashes of drinking drivers under 21: mean decrease 16%1
• NHTSA estimates MDA of 21 prevented 21,000 traffic deaths since 1976; saves 700-1000 deaths annually 2
• 30 states with <21 zero-tolerance laws: 19% less drunk driving3
—yet low enforcement Sources: Edwards et al, 1994; Babor et al, 2003; 1Schultz et al, 2001; 2NHTSA, 2003; 3Wagenaar, 2001

Alcohol Warning Label (PL100-690, 1988)
Federal law required health warning on container labels• Government warning from credible source: Surgeon General
• Pregnant women should not drink : risk of birth defects
• Impairs ability to drive a car or operate machinery and may cause health problems; political compromises—warnings often obscure
Major Results of national study commissioned by NIAAA • By 1994, 60% of drinkers saw the label–asymptotic exposure
• Messages reach > 50% males 18-20 (drunk driving); > 65% drinkers 18-29 (pregnancy); reach heavy drinkers but may miss less educated and ethnic minority groups
• Modest associations with precautionary behavior, conversations Sources: Giesbrecht & Greenfield, 2003;Greenfield et al, 1999; Hankin et al, 1993

Sliding Public Support for Stronger Alcohol Policies
20
30
40
50
60
70
80
90
100
1989 1990 1991 1993 1994 2000
Warning Labels
More Prevention
Host Liability
Counter Ads
Increase Taxes
Store Hours
Drinking Age
Souce: Greenfield, Johnson & Giesbrecht, CDP, 2004
%

Alcohol Access Regulation
Access primarily regulated at state and local levels• Responsibility of State Alcoholic Beverage Control agency• Limiting Outlet Density: Possible benefits—lower crashes, less
violence
Monopoly States• By 2 years after Repeal, 15 states enacted retail monopolies• Deregulation and privatization have led to increased wine sales in
several states and a Canadian province (Quebec)
• Iowa and West Virginia increased wine and overall consumption
Sources: Babor et al, 2003; Friestheler et al, 2004; Gruenewald et al, 1993; Gruenewald et al, 1996; Gorman et al, 2001; Lipton & Gruenewald, 2002; Scribner et al, 2000; Treno et al, 2003; Trolldal, 2005; Wagenaar & Holder, 1991;1995; Weitzman et al, 2003

Case Study: Underage Drinking Enforcement
Age-of-sale Compliance Checks (e.g. underage decoys)• Can significantly reduce number of outlets selling alcohol to a minor
• Have also been shown to reduce youth’s reported ease of acquisition • In California, law enforcement conducted 291 minor decoy operations
in 1997-98, lowering violation rate to 21% from 29% in 1993-94; ABC supported effort: Grant Assistance to Law Enforcement (GALE)
“Cops in Shops” detects and cites youth purchasers—developed by Century Council, an industry group • Funding also from NHTSA, Office of Juvenile Justice;• Less often implemented by police agencies than compliance checks,
but more common in communities with large college dorm populations • Prior year: 55-74% used compliance check; 23-41% Cops in Shops
Sources: Montgomery, Foley & Wolfson, 2006; Ryan & Mosher, 2000; Grube, 1997

Server Intervention, RBS Programs
Steps servers can take to reduce chance of intoxication• One third to one half alcohol-impaired drivers drank last at
public places—bars or restaurants
• 1980-2005: RBS studies tend to show modest efficacy
• Factors enhancing effectiveness include management incentives, “house rules,” enforcement of laws banning service to intoxicated patrons; community involvement
• State mandated server training (Oregon): time series study demonstrated 23% reduction in crashes
• Training programs focused on aggressive patrons have also shown promise
Sources: Saltz, 1997; Holder, 1994; Hommel et al, 2001; Graham & Wells, 2001; Babor et al 2003;

Policies in Colleges and Schools
Colleges and Universities• Much focus on Greek system: highest volumes and amounts• Importance of clear articulation of comprehensive campus-
wide policies with consistent enforcement; community buy in• Importance of student participation in policy making
Meta-analyses of School (K–12) Programs• Programs more effective when based on sound behavioral
theory and knowledge of risk and protective factors• Importance of community and parental involvement and
consistent enforcement of school policies & access controls Sources: Weschler et al, 1995; 1998; Cohen & Rogers, 1997; Whitcomb, 1999; Pentz et al. 1996; Tobler et al, 2000; Komro & Toomey, 2002

Workplace PoliciesDrinking on the job
• Examples: Management styles in manufacturing plants predict norms & availability; barriers to policies/enforcement
Drinking off the job• Examples: Civil Aviation requirements—aircrew cannot drink
before flying; new attention to hangovers & problems on job
Policies on employee testing• Examples: Considerable variation in civil aviation; bus drivers
Policies affecting employee assistance• Examples: EAPs and parity for addictions in health plans
Sources: Ames, Grube, & Moore, 1997; 2000; Cook, 1997; Sturm et al, 1998; ASAM, 1997; Roman & Blum, 2002

Ratings of policy-relevant strategies and interventions
Policy - strategyEffectiveness Breadth of
research
support
Cross-cultural Testing
Cost to implement
Retail monopoly +++ +++ ++ Low
Restrict outlet density ++ +++ ++ Low
Increase alcohol taxes +++ +++ +++ Low
No service to intoxicated + +++ ++ Moderate
Server liability +++ + + Low
School programs 0 +++ ++ High
Warning labels 0 + + Low
Min. legal purchase age +++ +++ ++ Low
Drivers <21 ‘zero tolerance’
+++ +++ ++ Low
Brief intervention-at risk ++ +++ +++ Moderate
Source: Adapted from Babor et al, Alcohol: No ordinary commodity (Table 16.1), 2003

Summary and Conclusions• A wide range of legislative policies at various jurisdictional
levels is currently being used to regulate alcohol commerce and people’s drinking in the U.S.
• In the last 25 years, policy analyses and evaluations have demonstrated efficacy of certain model programs; implementation, effectiveness and sustainability studies needed
• We need both policies that affect all drinkers and targeted harm reduction measures aimed at heavy drinkers and settings in which drinking large quantities is promoted
• Policy development studies reveal opportunities and may improve strategies for enacting evidence-based policies
• Global burden of disease studies plus new surveys are leading to policy work for choosing practical interventions