Embed Size (px)
Citation preview

Alcohol WithdrawalAnton Manasco, BS, Shannon Chang, MD, Joseph Larriviere, MD, L. Lee Hamm, MD,
and Marcia Glass, MD
Abstract: Alcohol withdrawal is a common clinical condition thathas a variety of complications and morbidities. The manifestations canrange from mild agitation to withdrawal seizures and delirium tre-mens. The treatments for alcoholwithdrawal include benzodiazepines,anticonvulsants, beta-blockers and antihypertensives. Although ben-zodiazepines are presently a first-line therapy, there is controversyregarding the efficacies of these medications compared with others.Treatment protocols often involve one of two contrasting approaches:symptom-triggered versus fixed-schedule dosing of benzodiazepines.We describe these protocols in our review and examine the datasupporting symptom-triggered dosing as the preferred method formost patients in withdrawal.The Clinical Institute Withdrawal Assessment for Alcohol scoringsystem for alcohol withdrawal streamlines care, optimizes patient man-agement, and is the best scale available for withdrawal assessment.Quality improvement implications for inpatient management of alco-hol withdrawal include increasing training for signs of withdrawaland symptom recognition, adding new hospital protocols to employeecurricula, and ensuring manageable patient-to-physician and patient-to-nurse ratios.
Key Words: alcohol withdrawal symptoms, alcohol withdrawal treat-ment, benzodiazepine, Clinical Institute Withdrawal Assessment forAlcohol, fixed-schedule dosing, symptom-triggered dosing
In the United States, alcohol is the most commonly abusedsubstance.1 Approximately one in four patients admitted to
general hospitals meets the criteria for alcohol dependence.2 In2009, approximately $185 billion were spent as a result ofexcessive alcohol consumption.3
The sequelae of alcohol abuse include loss of trust of friendsand family, inability to secure employment, legal consequences,physical debilitation, and permanent mental deterioration. Themanifestations of alcohol withdrawal range from mild symp-toms, such as tremors and malaise, to severe hemodynamicinstability or death.
Healthcare providers constantly encounter patients withalcohol-abuse problems. Physicians and nurses should identifysymptoms of alcohol withdrawal, including anxiety, diapho-resis, and seizures, to prevent patients’ further deterioration.
The treatment of alcohol withdrawal involves monitoringpatients, ruling out other causes, and symptom managementwith benzodiazepines. Failure to treat alcohol withdrawal canbe fatal, whereas overtreatment of symptoms with benzodiaze-pines can lead to sedation and respiratory depression. Quality-improvement ventures have produced a standardized method ofassessing patients with alcohol withdrawal. This protocol, theClinical Institute Withdrawal Assessment for Alcohol-revised(CIWA-Ar), expedites treatment and minimizes complications.
Withdrawal SymptomsAlcohol withdrawal usually begins 1 to 3 days after the
last drink and can last up to 1 week.2 Symptoms occur when thecentral nervous system, previously subjected to prolongedalcohol exposure, abruptly enters a state of decreased alcoholintake. Alcohol elicits central nervous system depression byexciting inhibitory F-aminobutyric acid (GABAA) A recep-tors, leading to a reduced level of GABA and GABA-receptorsensitivity. Alcohol also simultaneously inhibits the N-methyl-D-aspartate component of the excitatory glutamate receptor.4
In chronic alcoholism, the CNS increases excitatory tone to
Key Points& Alcohol withdrawal is a common clinical entity that should be
recognized by all physicians. Symptoms range from mildagitation to seizures, autonomic instability, and deliriumtremens.
& Long-acting benzodiazepines are a first-line treatment foralcohol withdrawal symptoms. Studies have shown thatsymptom-triggered dosing of benzodiazepines results insmaller benzodiazepine dosage, shorter treatment duration,fewer adverse reactions, and shorter hospitalizations.
& The Clinical Institute Withdrawal Assessment for Alcohol-Revised is the most validated scale for assessing alcoholwithdrawal severity. This scale can be used to determine theproper benzodiazepine dosage for individual patients basedon their withdrawal symptoms.
Review Article
Southern Medical Journal & Volume 105, Number 11, November 2012 607
From the Tulane University School of Medicine, New Orleans, Louisiana.
Reprint requests to Anton Manasco BS, Tulane University School of Medicine,1430 Tulane Ave, New Orleans, LA 70112. E-mail: [email protected]
The authors have no financial relationships to disclose and no conflicts ofinterest to report.
Accepted May 30, 2012.
Copyright * 2012 by The Southern Medical Association
0038-4348/0Y2000/105-607DOI: 10.1097/SMJ.0b013e31826efb2d
Copyright © 2012 The Southern Medical Association. Unauthorized reproduction of this article is prohibited.

maintain homeostasis. When alcohol cessation occurs abruptlyin these individuals, the inhibitory tone is withdrawn, but thecompensatory increase in excitatory neurotransmission remains.Furthering this excitatory tone is the role of homocysteine, anexcitatory amino acid that also acts as the N-methyl-D-aspartatereceptor.5 Its concentration increases during active drinking andremains elevated after the cessation of drinking. The combina-tion of homocysteine with unopposed glutaminergic neurotrans-mission in withdrawal yields an excitotoxic effect. This causesthe common withdrawal symptoms of tremulousness, anxiety,diaphoresis, headache, palpitations, insomnia, and gastrointes-tinal upset. Folate is a cofactor of homocysteinemetabolism andis deficient in most cases of chronic alcoholism. Lack of folatemay precipitate further withdrawal symptoms, making supple-mentation therapeutic.5
Withdrawal seizures are a complication occurringwithin thefirst 48 hours of cessation. They typically occur as a singlegeneralized tonic-clonic seizure or a brief episode of multipleseizures.5 Prolongation or recurrence of seizure activity neces-sitates an infectious disease workup (eg, complete blood count,lumbar puncture, blood cultures). Standard withdrawal therapyof long-acting benzodiazepines is indicated for the treatment ofwithdrawal seizures.
Delirium tremens (DT), also known as alcohol withdrawaldelirium, is the most severe manifestation of alcohol with-drawal, which occurs in approximately 5% to 20% of patientsexperiencing detoxification.7 Of the patients whose symptomshave progressed towithdrawal seizures, approximately 33% areexpected to progress to DT.8 The clinical features of DT aredisorientation, agitation, hallucinations, tremors, diaphoresis,and abnormalities in vital signs, including tachycardia, hy-pertension, and low-grade fever. The time of onset is 24 to72 hours after cessation of drinking, and the condition carries a5% mortality rate in uncomplicated patients and up to a 25%mortality rate in patients with concomitant complications.8 Acohort study conducted by Monte et al used a multivariatelogistic regression model to conclude that the following find-ings are independent variables for DT development: number ofseizures; 1 or 2 seizures (odds ratio [OR] 2.2), 3 seizures (OR2.6), systolic blood pressures 9150 mm Hg (OR 1.9), andaxillary temperature 938-C (OR 1.9).7
Wernicke syndrome, a potential complication of thiamindeficiency, is characterized by cognitive impairment, delirium,paralysis of eye muscles, and an abnormal gait. Incidencesof Wernicke encephalopathy can be as high as 12.5% in patientswith chronic alcoholism.9 Korsakoff syndrome, also known asamnestic-confabulation syndrome, is caused by thiamin defi-ciency.2 Thiamin, folic acid, and multivitamins are added tostandard benzodiazepine therapy to prevent progression to Wer-nicke encephalopathy. Thesemeasures, in addition to intravenousfluids, nutritional supplementation, and the repletion of potassi-um, magnesium, and phosphate, represent the full spectrum ofmanagement of the patient withdrawing from alcohol.
Pharmacological Treatment of WithdrawalIn the United States, the accepted practice for pharma-
cological treatment of alcohol withdrawal begins with theadministration of benzodiazepines (US Preventive ServicesTask Force grade A recommendation: consistent, high-qualityevidence).10 The most commonly administered benzodiaze-pines are chlordiazepoxide and diazepam. Other benzodiaze-pines may be administered based on desired duration of action,rapidity of onset, and cost. In a meta-analysis of the pharma-cological management of alcohol withdrawal, benzodiazepinessignificantly reduced seizures (P = 0.003) and reduced theincidence of delirium (P = 0.04).10 In a Cochrane review of 57randomized controlled trials on the efficacy of benzodiazepinesin alcohol withdrawal, benzodiazepines were found to be sig-nificantly superior to placebo in preventing alcohol-withdrawalseizures (P = 0.04Y0.69).11 Longer-acting benzodiazepines(eg, chlordiazepoxide, oxazepam) may be more effective inseizure prevention (US Preventive Services Task Force level II:randomized trials with high false-positive and/or high false-negative errors) and may result in a more uneventfulwithdrawalcoursewith less breakthrough of symptoms (level I: randomizedtrials with low false-positive and low false-negative errors).10
Longer-acting benzodiazepines also carry a greater risk of over-sedation (level III: nonrandomized, concurrent cohort compar-isons), especially in elderly adults and those with liver disease.10
Short-acting benzodiazepines (eg, diazepam, alprazolam, loraze-pam) are shown to have more addictive potential as comparedwith long-acting benzodiazepines (level I).10
Continuous infusions of short-acting benzodiazepines(eg, lorazepam, midazolam) have been tried. Studies havefound that costs were 910 times higher with continuous infu-sions versus intravenous or bolus therapy without significantchanges in outcomes or adverse effects.10
In comparing different benzodiazepines to prevent with-drawal seizures, chlordiazepoxide outperformed lorazepam,diazepam, and alprazolam, but results were not statisticallysignificant.11 To prevent withdrawal delirium, diazepam wasmore effective than alprazolam, chlordiazepoxide, abecamil, andlorazepam, but results were not statistically significant.11
In addition, other medications, including anticonvulsants,antipsychotics, beta-blockers, and antihypertensives, are used totreat alcoholwithdrawal.Ameta-analysis of the pharmacologicalmanagement of alcohol withdrawal by Mayo-Smith found thatbenzodiazepines are more effective than phenothiazines in re-ducing delirium (P = 0.002) and seizures (P G 0.001).10 In a2010 Cochrane review, Amato et al found that benzodiazepinesare not significantly superior to other drugs (anticonvulsants,including chlormethiazole, sodium valproate, phenobarbital,carbamazepine; antipsychotics, including chlorpromazine, hal-operidol, thioridazine; or clonidine, bromocriptine, thiamin, hy-droxyzine, baclofen, propranolol, and nitrous oxide) in preventingwithdrawal seizures (relative risk 0.21Y1.31) or delirium (RR0.21Y1.98).11 Antipsychotics are not recommended in alcohol
Manasco et al & Alcohol Withdrawal
608 * 2012 Southern Medical Association
Copyright © 2012 The Southern Medical Association. Unauthorized reproduction of this article is prohibited.

withdrawal syndrome because of their proconvulsant proper-ties.11 In a similar study, chlormethiazole, barbital, and tetra-bamate were found to be equal to benzodiazepines in thereduction of signs and symptoms of withdrawal.10 There wasno significant difference in adverse events when comparingdifferent benzodiazepines to one another or with other drugs.11
Certain types of drugs mentioned above provide specificbenefits for patients experiencing alcohol withdrawal. Beta-blockers, such as propranolol, decrease autonomic symptoms.10
Clonidine, a centrally acting >-adrenergic agonist, is shown torelieve withdrawal symptoms. These drugs, however, are noteffective for reducing delirium or seizures and may obscure theadrenergic symptoms of alcoholwithdrawal.10Carbamazepine isfrequently used in Europe to prevent withdrawal seizures and,when compared with benzodiazepines, does not bear the samerisks of sedation and respiratory depression.10
A 2006 case series described a patient cohort withbenzodiazepine-resistant alcohol withdrawal. These patientsrequired Q50 mg of diazepam in their first hour of admissionand large doses of benzodiazepines throughout their hospitalcourse. These patients also received supplemental intravenousbarbiturates, experienced vital sign abnormalities at 24 hoursdespite benzodiazepine treatment, and underwent a more com-plicated hospital course.19
Some medication supplementation is not shown to im-prove outcomes. Hypomagnesemia is common in alcoholwithdrawal. Neuromuscular excitability, refractory hypokale-mia, and electrocardiographic abnormalities such as a wid-ened QRS complex are seen in hypomagnesemia and requiresupplementation. A double-blind, placebo-controlled random-ized trial of magnesium supplementation to benzodiazepinesshowed no difference in incidence of seizures, delirium, andother symptoms of withdrawal.10 Thiamin administration doesnot change the incidence of withdrawal delirium or seizures.Clinicians should administer thiamine before carbohydrate in-fusion to prevent Wernicke-Korsakoff syndrome.10
Methods of Treatment: SymptomTriggered Versus Fixed Schedule
Two treatment modalities have been shown to have evidence-based efficacy: symptomatic treatment of alcohol withdrawalwith benzodiazepines and fixed-schedule dosing of long-acting benzodiazepines with additional symptomatic treat-ment. The advantage of symptom-triggered therapy is thatsignificantly smaller benzodiazepine doses are administeredyielding less sedation, shorter treatment, fewer adverse reac-tions, and a decreased risk of respiratory depression. In addi-tion, patients receiving symptomatic treatment were found torequire shorter hospitalizations.10,12Y16 Saitz et al showed thatthe median total administered dose of chlordiazepoxide was100 mg in a symptom-triggered group versus a median of425 mg of chlordiazepoxide in a fixed-schedule dosing group.16
In addition, the mean duration of treatment was significantly
shorter in the symptom-triggered group (9 vs 68 hours) whencompared with fixed-schedule dosing.16
The second treatment modality is fixed-schedule dosing ofbenzodiazepines regardless of the presence of symptoms. Theadvantage of a fixed schedule is that frequent reassessment ofsymptoms is not necessary. This is helpful in a setting with ahigh patient-to-clinician ratio. In addition, fewer protocolerrors are seen in comparison with symptom-triggered therapy.A meta-analysis of 64 studies performed by Amato et al foundlittle difference between the two therapies in terms of finaloutcomes.11 Fixed-schedule dosing is often the only way totreat patients withdrawing from alcohol with comorbid medi-cal illnesses or a postoperative status because of inability toassess withdrawal symptoms.12,17
Assessing for Withdrawal: CIWA-ArThe most popular and validated clinical assessment scale
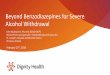
is the CIWA-Ar. Its predecessor, the CIWA-A, had been in usesince 1978 and has 15 items to consider.18 The CIWA-Ar is a10-item survey that assesses a patient’s symptoms and scores apatient’s severity of symptoms (Table 1).2 Scores on the CIWA-Ar range from 0 to 67 points. The CIWA-Ar evaluates thefollowing signs and symptoms: sweating; anxiety; tremors;agitation; disturbances of tactile, auditory, or visual nature;headache; and disorientation or clouding of sensorium.19
Clinicians used the CIWA-Ar in several clinical studiesto assess alcohol withdrawal and determine which patientsrequired benzodiazepines. To study symptom-triggered ther-apy, Riddle et al created a ‘‘standing order set’’ to administerwithdrawal medications based on a patient’s CIWA-Ar score.2
A CIWA-Ar score G8 is indicative of mild withdrawal symp-toms. No therapy is indicated at this score and the patientshould be reassessed in 4 hours. A CIWA-Ar score of 9 to 15represents moderate withdrawal and 25 to 50 mg of chlordi-azepoxide is given orally as needed every 4 hours for symp-toms (maximum 300 mg/24 hours). Patients should have theirscore reassessed after 2 hours. Severewithdrawal is representedby a score 915. In this case, chlordiazepoxide 50 to 100 mgis given hourly as needed for a maximum of 300 mg/24 hours,with lorazepam 2 to 4 mg given intravenously every 2 hours asneeded for a maximum of 24 mg/24 hours. This study foundthat the overall patients’ length of stay, days requiring medi-cation, and quantity of medication administered were less inthe symptom-triggered group as compared with the fixed-schedule group.
Prospective and retrospective trials have shown that incooperative patients experiencing alcohol withdrawal, theCIWA-Ar and its derivatives are associated with reductions inquantity of benzodiazepines administered and in length oftreatment.17
Discussion (Quality Improvement)Hospitals and healthcare institutions strive for optimum
medical management of patients. Given the current data,
Review Article
Southern Medical Journal & Volume 105, Number 11, November 2012 609
Copyright © 2012 The Southern Medical Association. Unauthorized reproduction of this article is prohibited.

benzodiazepines are recommended for first-line treatment ofalcohol withdrawal. Benzodiazepines are shown to be sig-nificantly better than placebo for treating withdrawal. Largerandomized controlled trials demonstrating benzodiazepinesuperiority to other medications in alcohol withdrawal arelacking.
Based on the few studies available, using symptom-triggered medication administration for patients with alcoholwithdrawal appears to be superior in patientswith uncomplicatedmedical histories. Daeppen et al found that the total dose ofoxazepam was less in the symptom-triggered group comparedwith the fixed-schedule group. The study also found that the
Table 1. Clinical Institute Withdrawal Assessment for Alcohol Scale
Patient: _______________________________________ Date: ___________ Time: ________Pulse: _________ BP: _______/_______
Nausea/vomiting. Ask ‘‘Do you feel sick to your stomach? Have you vomited?’’ Tactile disturbances. Ask ‘‘Doyou have any itching, pins-and-needles sensations,burning, or numbness, or doyou feel like bugs are crawling on or under your skin?’’0- No nausea and vomiting
0- None1-
1- Very mild itching, pins-and-needles sensation, burning, or numbness2-
2- Mild itching, pins-and-needles sensation, burning, or numbness3-
3- Moderate itching, pins-and-needles sensation, burning, or numbness4- Intermittent nausea with dry heaves
4- Moderately severe hallucinations5-
5- Severe hallucinations6-
6- Extremely severe hallucinations7- Constant nausea, frequent dry heaves, vomiting
7- Continuous hallucinationsTremor. Ask patient to extend arms and spread fingers apart.
Auditory disturbances. Ask ‘‘Are you more aware of sounds around you? Are theyharsh? Do they frighten you? Are you hearing anything that is disturbing to you?Are you hearing things you know are not there?’’
0- No tremor
0- Not present
1- Tremor not visible but can be felt, fingertip to fingertip
1- Very mild harshness or ability to frighten
2-
2- Mild harshness or ability to frighten
3-
3- Moderate harshness or ability to frighten
4- Moderate tremor with arms extended
4- Moderately severe hallucinations
5-
5- Severe hallucinations
6-
6- Extremely severe hallucination
7- Severe tremor, even with arms not extended
7- Continuous hallucinations
Paroxysmal sweats
Visual disturbances. Ask ‘‘Does the light appear to be too bright? Is its colordifferent? Does it hurt your eyes? Are you seeing anything that is disturbing toyou? Are you seeing things you know are not there?’’
0- No sweat visible
0- Not present
1- Barely perceptible sweating; palms moist
1- Very mild sensitivity
2-
2- Mild sensitivity
3-
3- Moderate sensitivity
4- Beads of sweat obvious on forehead
4- Moderately severe hallucinations
5-
5- Severe hallucinations
6-
6- Extremely severe hallucinations
7- Patient drenched in sweat
7- Continuous hallucinations
Anxiety. Ask ‘‘Do you feel nervous?’’
Headache, fullness in head. Ask ‘‘Does your head feel different? Do you feellike there is a band around your head?’’
0- No anxiety (at ease)
0- Not present
1- Mildly anxious
1- Very mild
2-
2- Mild
3-
3- Moderate
4- Moderately anxious or guarded, so anxiety is inferred
4- Moderately severe
5-
5- Severe
6-
6- Very severe
7- Equivalent to acute panic states as occur in severe delirium or acuteschizophrenic reactions
7- Extremely severe
(continued on next page)
Manasco et al & Alcohol Withdrawal
610 * 2012 Southern Medical Association
Copyright © 2012 The Southern Medical Association. Unauthorized reproduction of this article is prohibited.

symptom-triggered group had a shorter duration of treatment.15
Similarly, two studies demonstrated that symptom-triggered dos-ing reduces the duration of mechanical ventilation in the intensivecare unit with fewer nosocomial infections.20,21 A limitation ofthis method is that absolute staff numbers and inadequate stafftraining constrain hospitals and other healthcare institutions.
Another drawback is a higher proportion of protocol errors.12 Todecrease these errors, additional training to recognize signs andsymptoms of withdrawal and efficient, simple hospital protocolsshould be added to employee curricula. Fixed-schedule medica-tion dosing for alcohol withdrawal avoids protocol errors butbears the risk of oversedation and longer hospital stays.
Agitation Orientation and clouding of sensorium. Ask ‘‘What day is this?Where are you? Who am I?’’0- Normal activity
0- Oriented and can do serial additions1- Somewhat more than normal activity
1- Cannot do serial additions or is uncertain about date2-
2- Date disorientation by no more than 2 calendar days3-
3- Date disorientation by 92 calendar days4- Moderately fidgety and restless
4- Disoriented to place and/or person5-
6-
7- Paces back and forth during most of interview or constantly thrashes about
Total score: ____________________
Table 1. (Continued)
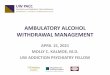
Table 2. Alcohol withdrawal scoring methods
Test Total points possible Point allocations
Clinical Institute Withdrawal Assessment for Alcohol - revised12 67 Nausea/vomiting (0Y7)
Tremor (0Y7)
Paroxysmal sweats (0Y7)
Anxiety (0Y7)
Agitation (0Y7)
Tactile disturbances (0Y7)
Auditory disturbances (0Y7)
Visual disturbances (0Y7)
Headache, fullness in head (0Y7)
Orientation and clouding of sensorium (0Y4)
Modified Severity Assessment Scale16 23 Nausea/vomiting (0Y3)
Tremor (0Y3)
Tachycardia (0Y3)
Diaphoresis (0Y3)
Fever (0Y3)
Agitation (0Y3)
Confusion, orientation, contact with reality (0Y3)
Hallucinations (0Y2)
Minnesota Detoxification Scale7 46 Pulse (0Y2)
Diastolic blood pressure (0Y2)
Tremor (0Y6)
Sweat (0Y6)
Hallucinations (0Y3)
Agitation (0Y9)
Orientation (0Y6)
Delusions (0Y6)
Seizures (0Y6)
Review Article
Southern Medical Journal & Volume 105, Number 11, November 2012 611
Copyright © 2012 The Southern Medical Association. Unauthorized reproduction of this article is prohibited.

Interestingly, a randomized controlled trial of outpatientswith alcohol withdrawal showed no difference in symptom-triggered versus fixed-schedule dosing of benzodiazepines.22
Direct extrapolation of these findings to the inpatient popula-tion is unclear. The results of this study illustrate the continueddebate between the two methods.
If hospitals are to move toward symptom-triggered med-ication administration, clinicians need an objective way tomeasure the severity of alcoholwithdrawal. CIWA-Ar (Table 1)has been used and reformulated into different scales, includingthe Severity Assessment Scale and the Minnesota Detoxifica-tion Scale (Table 2).1,13 Prospective and retrospective trialshave shown that in cooperative patients experiencing alcoholwithdrawal, the CIWA-Ar and its derivatives are associatedwith reductions in quantity of benzodiazepines administeredand length of treatment.17
One problem with these scales is that the patient mustrespond to questions and follow commands, limiting their usein certain patient populations. Withdrawal symptoms may bemisinterpreted as infection, pain, or other causes of delirium,and the diagnosis of alcohol withdrawal could be missed en-tirely. Conversely, a patient without a known history of alcoholabuse admitted for an unrelated condition could have with-drawal symptoms that are misattributed to his primary diag-nosis. A high level of clinical suspicion and accurate historytaking is required, even with the use of alcohol-withdrawalscales. In addition, continued vital sign and patient monitoringis critical when alcohol withdrawal is suspected.
ConclusionsSeveral studies validate the use of symptom-triggered
benzodiazepine therapy in inpatient and intensive care unitsettings for alcohol withdrawal.11,15,16,20 Benefits include adecrease in benzodiazepine dosage and associated adverseeffects, duration of treatment, and the use of a standardizedmethod to assess patients undergoing withdrawal.
Limitations to the CIWA-Ar include protocol errors, in-effectiveness in certain patient populations, and a consider-able time investment. Estimates of the length of time neededto conduct the CIWA-Ar range from 5 to 15 minutes.4,13
Although practical in inpatient detoxification units, the require-ments of the CIWA-Ar could overburden nurses and ancillarystaff in busy inpatient general hospitals.
Alcohol withdrawal is a common problem facing all clin-icians and must be treated appropriately. A staple in manage-ment is to use symptom-triggered medication administrationrather than fixed-dosed scheduling to tailor each patient’s treat-ment method to the actual condition. This innovation showspromise in terms of quality improvement and deserves focusedresearch.
References1. Phillips S, Haycock C, Boyle D. Development of an alcohol withdrawal
protocol. Clin Nurse Spec 2006;20:190Y198.
2. Riddle E, Bush J, Tittle M, et al. Alcohol withdrawal: development of astanding order set. Crit Care Nurse 2010;30:38Y47.
3. National Institute on Alcohol Abuse and Alcoholism five year strategicplan, FY07-11, alcohol across the lifespan. http://pubs.niaaa.nih.gov/publications/StrategicPlan/NIAAASTRATEGICPLAN.htm. AccessedMay 13, 2012.
4. Dodd PR, Beckmann AM, Davidson MS, et al. Glutamate-mediatedtransmission, alcohol, and alcoholism. Neurochem Int 2000;37:509Y533.
5. Hughes JR. Alcohol withdrawal seizures. Epilepsy Behav 2009;15:92Y97.
6. Deleted in proof.
7. Monte R, Rabunal R, Casariego E, et al. Risk factors for delirium tremensin patients with alcohol withdrawal syndrome in a hospital setting. Eur JIntern Med 2009;20:690Y694.
8. Stern TA. Alcohol-induced disorders. In: Stern TA, Rosenbaum JF, FavaM, et al, eds. Massachusetts General Hospital Comprehensive ClinicalPsychiatry. 1st ed. New York: Mosby/Elsevier; 2008:1059Y1060.
9. Zahr NM, Kaufman KL, Harper CG. Clinical and pathological features ofalcohol-related brain damage. Nat Rev Neurol 2011;7:284Y294.
10. Mayo-Smith MF. Pharmacological management of alcohol withdrawal.A meta-analysis and evidence-based practice guideline. JAMA 1997;278:144Y151.
11. Amato L, Minozzi S, Vecchi S, et al. Benzodiazepines for alcoholwithdrawal. Cochrane Database Syst Rev 2010;17:CD005064.
12. Weaver MF, Hoffman HK, Johnson RE, et al. Alcohol withdrawalpharmacotherapy for inpatients with medical comorbidity. J Addict Dis2006;25:17Y24.
13. DeCarolis DD, Rice KL, Ho L, et al. Symptom-driven lorazepam protocolfor treatment of severe alcohol withdrawal delirium in the intensive careunit. Pharmacotherapy 2007;27:510Y518.
14. Stanley KM, Worrall CI, Lunsford SI, et al. Experience with an adultalcohol withdrawal syndrome practice guideline in internal medicinepatients. Pharmacotherapy 2005;25:1073Y1083.
15. Daeppen JB, Gache P, Landry U, et al. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: a randomizedtreatment trial. Arch Intern Med 2002;162:1117Y1121.
16. Saitz R, Mayo-Smith MF, Roberts MS, et al. Individualized treatment foralcohol withdrawal. A randomized double-blind controlled trial. JAMA1994;272:519Y523.
17. Hecksel KA, Bostwick JM, Jaeger TM, et al. Inappropriate use ofsymptom-triggered therapy for alcohol withdrawal in the generalhospital. Mayo Clinic Proc 2008;83:274Y279.
18. Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability,and comorbidity of DSM-IValcohol abuse and dependence in the UnitedStates: results from the National Epidemiologic Survey on Alcohol andRelated Conditions. Arch Gen Psychiatry 2007;64:830Y842.
19. Hack J, Hoffman R, Nelson L. Resistant alcohol withdrawal: does anunexpectedly large sedative requirement identify these patients early?J Med Toxicol 2006;2:55Y60.
20. Gold JA, Rimal B, Nola A, et al. A strategy of escalating doses ofbenzodiazepines and phenobarbital administration reduces the need formechanical ventilation in delirium tremens. Crit Care Med 2007;35:724Y730.
21. Spies CD, Otter HE, Huske B, et al. Alcohol withdrawal severity isdecreased by symptom-orientated adjusted bolus therapy in the ICU.Intens Care Med 2003;29:2230Y2238.
22. Elholm B, Larsen K, Hornnes N, et al. Alcohol withdrawal syndrome:symptom-triggered versus fixed-schedule treatment in an outpatientsetting. Alcohol Alcohol 2011;46:318Y323.
Manasco et al & Alcohol Withdrawal
612 * 2012 Southern Medical Association
Copyright © 2012 The Southern Medical Association. Unauthorized reproduction of this article is prohibited.