Embed Size (px)
DESCRIPTION
ADDICTION RECOVERY Where are we going? How do we get there? Lessons from the recovery experience for service development. Alexandre B. Laudet, Ph.D Institute for Research, Education, and Training in Addictions Tampa, FL ● August 2-4, 2010. All ears…. ACT ONE WHY ARE WE HERE TODAY?. - PowerPoint PPT Presentation
Citation preview

Alexandre B. Laudet, Ph.DAlexandre B. Laudet, Ph.DInstitute for Research, Education, and Training in AddictionsInstitute for Research, Education, and Training in Addictions
Tampa, FL ● August 2-4, 2010
ADDICTION RECOVERYADDICTION RECOVERY
Where are we going? How do we get there? Where are we going? How do we get there?
Lessons from the recovery experience for service developmentLessons from the recovery experience for service development

All ears…

ACT ONEACT ONEWHY ARE WE HERE TODAY?WHY ARE WE HERE TODAY?

Why are we here Why are we here today?today?
For many, substance use disorders are chronic (on par with diabetes, asthma etc…)
Addiction can not be cured but it can be arrested or managed
For some, it may require ongoing care of various intensities over time (e.g., intensive services, stepped down or after care, recovery checkups, 12-step)
HOW ARE WE TREATING ADDICTION?
Acute model of care (assess, treat, discharge)
Focused on symptoms, not on promoting wellness
Short-term episodes of intensive care are ill-suited to manage a chronic condition:
High attrition rate - e.g., 60% attrition from outpatient nationwide
Few achieve abstinence during treatment
High relapse rates after treatment –50– 60% within 6 months following treatment
Costly cycling through multiple episodes of care – e.g. in one study in NYC, 80% outpatient client report 1 or + previous episode, 50% >3
People don’t get better, some die, families and communities suffer

A wind of change…A wind of change…
Recovery is more than abstinence from alcohol and drugs; it is about building a full and productive life in the community. Our treatment systems must reflect and help people achieve this broader understanding of recovery. (Dr. W. Clark, 2007)
Recovery Oriented System of Care (ROSC)Recovery Oriented System of Care (ROSC)

Elements of Recovery-Elements of Recovery-Oriented Systems of CareOriented Systems of Care
A ROSC is a coordinated network of community-based services and supports that is person-centered and builds on the strengths and resilience of individuals, families, and communities to achieve abstinence and improved health, wellness, and quality of life for those with or at risk of alcohol and drug problems.
Person-centeredFamily and other ally involvementIndividualized and comprehensive servicesSystems anchored in the communityContinuity of carePartnershipsStrength-basedCulturally responsiveResponsive to personal belief systemsCommitment to peer servicesInclude recovering people and familiesIntegrated servicesSystem-wide educational and trainingOngoing monitoring and outreachOutcomes-driven Evidence-basedAdequately and flexibly funded
From W. Clark, CSAT, Generic ROSC talk

Paradigmatic shifts needed to Paradigmatic shifts needed to implement ROSCimplement ROSC
From intense episodes of acute specialty care to multi-systems, person-centered continuum of multi-systems, person-centered continuum of carecare
From addressing pathology to promoting globalpromoting global health, wellness, and recoveryhealth, wellness, and recovery

Recovery Oriented System Recovery Oriented System of Careof Care
THIS SOUNDS VERY GOOD
THIS MEANS BIG CHANGES (more PAPERWORK???)
HOW DO WE GET THERE?
NEED TO KNOW
1. What recovery means
2. What helps/hinders the process
3. How this can be translated into services and policy
At the patient level
At the program level
At the system level

How much do we know about How much do we know about recoveryrecovery??
Research has mirrored the service delivery paradigm
Focused on primary symptom as outcome
Focused on treatment populations
Short term studies mostly
As a result, we lack information on:
What ‘recovery’ means: abstinence + WHAT?
Long-term recovery paths, patterns and their predictors
Especially among persons who are not enrolled in treatment

How can we promote/support an outcome we have How can we promote/support an outcome we have
not examined and poorly understand?not examined and poorly understand?

We need a science of recoveryto inform Recovery Oriented
Systems of Care

WhatWhat will the science of will the science of recovery do?recovery do?
Support the development, monitoring and evaluation of ROSC at all 3 levels by answering:
1. Destination: Where are we going? Specifically what are we trying to promote (what is recovery? long-term recovery)?
2. Roadmap: How do we get there? What to put in our recovery-oriented services toolbox to best serve clients as their needs change?
3. Are we there yet? How can we measure recovery outcomes? (for service monitoring and quality improvement, accountability)

Summary of key datasetsSummary of key datasetsused in today’s used in today’s presentationpresentation
NIDA funded studies conducted in NYC 2002 - 2009

Pathways: Pathways: The community-based The community-based samplesample
Study funded to elucidate patterns and psychosocial predictors of stable abstinence from drugs and alcohol use
Media recruited sample (N = 354) re-interviewed yearly 3 times: one-, two- and three year follow-up (83% retention of surviving BL cohort of 342)
Self-reported abstinence at baseline from one month to 10+ years
Primarily members of inner-city ethnic, underserved minorities
Long & severe history of (primarily) crack and/or heroin use
Almost all are polysubstance users
30% HepC+ and 22% HIV+
Almost all have used formal addiction treatment services and 12-step fellowships

Pathways participants were classified Pathways participants were classified by baseline abstinence duration by baseline abstinence duration according to clinically meaningful according to clinically meaningful stagesstages
18 to 36 mo.20% 6 to 18 mos.
26%
Three+ yrs27%
< 6 mos. Drug abstinent
27%

Twelve-step as aftercare:Twelve-step as aftercare: The The outpatient treatment sampleoutpatient treatment sample
Study funded to identify predictors, patterns and outcomes of 12 step participation after outpatient
Recruited consecutive admissions at two publicly funded outpatient programs
250 clients re-interviewed at treatment end (90% re-contact) who constitute the prospective study cohort
Follow-up interviews 3-, 6- and 12-months post treatment end
Full dataset on 219 participants ( 87.6% retention) one year post discharge
Primarily members of inner-city ethnic, underserved minorities
Long & severe history of (primarily) crack and/or heroin use
Average of 5.8 previous treatment episodes

ACT TWOACT TWOWHERE DO WE NEED TO GO?WHERE DO WE NEED TO GO?
RecoveryRecovery

Substance users try to quit becauseSubstance users try to quit because they want a better lifethey want a better life
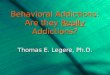
83
86
90
92
93
94%
50 75 100
Negative effects of drug use onothers
Weighing pros & cons ofcontinued use
Didn't like what I was becoming
Tired of the drug life
Desire for a better life
Didn't like where life wasgoing/feared consequences
To what extent was [item] a factor in your decision to stop using drugs this time?
“Not at all, a little, moderately, very much, extremely” (N = 354)(N = 354)
Laudet & White, 2004a

Does quitting use ‘lead’ to a Does quitting use ‘lead’ to a better life??? better life???

Benefits of recovery:Benefits of recovery: Open-endedOpen-endedaa
What, if anything, is/would be good about being in recovery?What, if anything, is/would be good about being in recovery?
RECOVERY = A BETTER LIFERECOVERY = A BETTER LIFE
11
13
16
17
18
16
23
33%
23
0 5 10 15 20 25 30 35
Having friendsBetter family lifeBetter physical/mental health
Better living conditionsBetter attitude
Having direction/goalsSelf-improvement
Clear headNew life/2nd chance
a Add to > 100% because up to 3 answers were coded

Stress and Quality of Life Satisfaction as a Stress and Quality of Life Satisfaction as a Function of abstinence duration Function of abstinence duration (N = 354)
RECOVERY STAGE
3+ years18 to 36 mos
Six to 18 mos>6 months
Mean
(sc
ale ran
ge =
0 to
10)
8.5
8.0
7.5
7.0
6.5
6.0
5.5
5.0
Overall life
satisfaction
Stress rating pst yr
Laudet, Morgen & White, Alc. Tx Q. 2006

Recovery definitionsRecovery definitions

Recovery definitionsRecovery definitions
Recovery from alcohol and drug problems is a process of change through which an individual achieves abstinence, improved abstinence, improved health, wellness, and health, wellness, and quality of lifequality of life. (CSAT, 2005 National Recovery Summit)
Recovery from substance dependence is a voluntarily maintained lifestyle characterized by sobriety, personal health, and sobriety, personal health, and citizenshipcitizenship. (Betty Ford Institute, 2007)

Let’s ask the REAL Let’s ask the REAL experts…people in experts…people in
recovery!recovery!
Let’s ask the REAL experts…Let’s ask the REAL experts…People in recovery!People in recovery!

Recovery definition: Recovery definition: Open-Open-endedendedaa
How would you define "recovery from drug and alcohol use"?
RECOVERY GOES BEYOND SUBSTANCE USERECOVERY GOES BEYOND SUBSTANCE USE
17%
21%
41%
44%
0 10 20 30 40 50
Dealing w/issues
Lifelong process
Total abstinence
Better life/new life
a Add to > 100% because up to 3 answers were coded; Laudet, JSAT, 2007

My definition of recovery is life… ‘Cause I didn’t have no life before I got into recovery
Laudet, JSAT, 2007
Pathways study participant H.W. 42 years old Af-Am male

Recovery is a Recovery is a processprocess, not an , not an endpointendpoint
“Recovery is a continuous process that never ends”
3.2%
96.8%
0 20 40 60 80 100
Disagree/Stronglydisagree
Agree/Stronglyagree
Laudet, JSAT, 2007

Relevance to ROSC Relevance to ROSC
Recovery is a realityRecovery is a reality
Recovery is a Process of Change and Growth Recovery is a Process of Change and Growth
Recovery is Sobriety + improved quality of Recovery is Sobriety + improved quality of lifelife

Destination Recovery: Destination Recovery: Few Direct flightsFew Direct flights

FOR TOO MANY PEOPLE, FOR TOO MANY PEOPLE, ADDICTIONADDICTION ISIS A CHRONIC A CHRONIC RELAPSING CONDITION…RELAPSING CONDITION…
That’s where ROSC comes That’s where ROSC comes in…in…

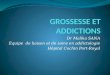
Addiction careerAddiction career Number of abstinent Number of abstinent periodsperiods one month or longer followed by return to one month or longer followed by return to drug use prior to current abstinencedrug use prior to current abstinence**
50% reported 4 or more abstinent periods followed by return to active addiction
*Outside of controlled environment, among those who report one or more such periods: 71% N=248Laudet & White 2004b
20 & over10%
Ten to 1917%
Six to nine7%
Four to five16%
Three11%
Two 22%
One17%

Relevance to ROSC Relevance to ROSC
Continuity of services and supportsContinuity of services and supports

ACT THREEACT THREEWhat’s wrong with the current What’s wrong with the current
model?model?

NYC Outpatient treatment NYC Outpatient treatment outcomeoutcome
Completed40%
Left before completion
60%
Laudet, Stanick, & Sands, JSAT 2009
Completion rate on par w/ national average of 36% for outpatient modalities

% Returned to substance use in the % Returned to substance use in the post-treatment year as a function of post-treatment year as a function of discharge statusdischarge status
57.8%
92.6%
0
10
20
30
40
50
60
70
80
90
100
Completed Left beforecompletion Chi. Sq. 35.5, p = .0000
Stanick, Laudet & Sands, 2008
Drop-outs were 2.8 times more likely to return to drug use in the year after services ended than were treatment completers (95%CI =1.86-4.23, p>.001)

Treatment Career:Treatment Career: Number of Number of prior episodesprior episodes
None21%
One15%
Two12%
Three-four17%
Five to nine21%
Ten +14%
Over half of outpatient clients have had 3 or more previous episodes
Laudet, Stanick & Sands, Eval Review, 2007

One third seek treatment One third seek treatment again in the 12 months after again in the 12 months after leaving the index episodeleaving the index episode
Laudet and Stanick, CPDD 2010
No additional treatment
69%
Additional treatment31%

Reasons for leaving treatment: Reasons for leaving treatment: Qualitative analysesQualitative analyses
What is the most important reason why you dropped out of the program?*
8.5
9.4
12
12
12
12
18.8
31.6%
0 5 10 15 20 25 30 35
Not helpful
Finances
Do not want help
Family/personal issues
Convenience (e.g.,transport)
Using
Tx interferes w/otheractivity (e.g., job)
Dislikeprogram/staff/clients
* Add to > 100% because up to 2 answers were coded; Laudet, Stanick, & Sands, JSAT 2009, 37:182-190

Minimizing attrition [1]Minimizing attrition [1]
Is there anything the program could have done differently so that you would have continued attending?
Yes33%
No67%
Laudet, Stanick, & Sands, JSAT 2009

Minimizing attrition [2]Minimizing attrition [2]
What could have been done differently so that you would have continued attending (among ‘yes’)
Practical assistance
11% Help with other areas of
functioning18%
Better, more caring staff
25%
Better individualized
services23%
Greater flexibility in scheduling
23%
Laudet, Stanick, & Sands, JSAT 2009

Substance use is but a Substance use is but a symptom, Promoting symptom, Promoting
abstinence is not enoughabstinence is not enough

Expectation of helpExpectation of helpOverall, how much do you think your coming to this treatment program will help you address your needs and priorities?
Quite a bit24%
Very much71%
Not at all1%
A little4%

Remember this? Remember this? 33% of drop outs may have
stayed longer if they had help in other life areas …Missed Missed opportunities?opportunities?
What could have been done differently so that you would have continued attending (among ‘yes’)
Practical assistance
11% Help with other areas of
functioning18%
Better individualized
services23%
Better/more caring staff
25%
Greater flexibility in scheduling
23%
Laudet, Stanick, & Sands, JSAT 2009

Quality of life Quality of life satisfaction sustains satisfaction sustains
abstinence…abstinence…

Quality of life satisfaction predicts Quality of life satisfaction predicts sustained abstinence: sustained abstinence: Community based sample
Stop drugs
SAY NO TO DRUGS
Want to stay happy
Controlling for other relevant variables, baseline QOL satisfaction predicts sustained abstinence one and two years later.
Association partially mediated by motivation for abstinence
HAPPIER
Laudet, Becker & White, 2009, 44
DIET Jeans fit better Want that feeling
Pass on Donut

“What worked for me is just the thought that I don’t wanna go through that madness
no more. … See, ‘cause if I was to use again, I probably would lose everything”.
Pathways participant
Behavioral economics: Demand lawBehavioral economics: Demand law

But what makes them But what makes them happy???happy???

Priorities @ outpatient Priorities @ outpatient admissionadmissionWhat are the priorities in your life right now? (N =
314)
0 10 20 30 40 50
Complete tx
Get life together
Relation w.family
Housing
Get kids back
Educ/Voc/Training
Get a job
Get/Stay clean
Abstinence is top goal Abstinence is top goal but not only goal!!!but not only goal!!!

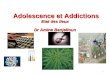
Life priorities in recoveryLife priorities in recovery by by abstinence duration abstinence duration
“What are the priorities your life right now?”“What are the priorities your life right now?” (N = 354)(N = 354)
0 10 20 30 40 50 60
Housing
Family reunification
Normal life
Educ/ training
Relationships
Employment
Recovery
< 6 mos.
6 - 18 mos.
18 - 36 mos.
> 3 years
Laudet & White, JSAT 2009

Relevance to ROSC Relevance to ROSC
Individualized and comprehensive Individualized and comprehensive services/supports services/supports
Multi-system Integrated servicesMulti-system Integrated services

ACT FOURACT FOURWith a little help from my With a little help from my
friends…friends…

Sources of support in long-term Sources of support in long-term recoveryrecovery PPathways pilot athways pilot (N = 52 CCAR members, median abstinence
duration 12 yrs)
7
11
17
18
43
53
53%
0 10 20 30 40 50 60Clinicians
FriendsSelf/inner strength SpouseRecovering peers FamilySpirituality/faith
Laudet, Savage & Mahmood, J. Psychoactive Drugs, 2002

Lessons learned from RelapseLessons learned from Relapse aa
Top answers (<10%)Top answers (<10%)
a Among those who report one or more such periods: N=253; Laudet & White, 2004b
10.3
11.5
15.1
18.3
18.7
21.8%
I'm an addict/can't use sociallyNeed to address issues/express fe...Cannot recover w/out supportLearn about/avoid from triggersClean =good/drugs = bad
Must want recovery/make it priorit...
What if anything have you learned from the relapse experience?

Strategies to deal with relapse Strategies to deal with relapse triggers:triggers:
Most cited = Seek support, stay focused on Most cited = Seek support, stay focused on recoveryrecovery
Meditate/pray8%
Stay focused42%
Seek help/support, Talk about pb
44%
Distraction6%
C Among those who report a challenge; Laudet & White 2004b

Example of source of support and Example of source of support and motivation: motivation:
Twelve-step fellowshipsTwelve-step fellowships

Role of Role of continuouscontinuous 12-step attendance 12-step attendance on on oddsodds of abstinence sustained for two of abstinence sustained for two years: years: Pathways studyPathways study
6.25
8
5.7
4.54.5
0
4
8
Totalsample
Under 6months
Six to 18months
18 to 36months
Threeyears +
Laudet & White 2006

Relevance to ROSC Relevance to ROSC
Draw on Support from peers, family members, significant
others, friends, and the community

ACT FIVEACT FIVE So what???So what???
Translating Research into Recovery Oriented Systems

Recovery Oriented System of Care Recovery Oriented System of Care makes Sense…makes Sense…
Based on the experience of people in treatment and in recovery, the core elements of ROSC ‘make sense’
The transition to ROSC will
Take time
Take full commitment from the ‘system’ including payors
Take place gradually
Experience and success of ‘leader states/cities’ (e.g., CT, Philly, ) will be invaluable
In the meantime, strive to ADOPT AS MANY ELEMENTS OF ROSC AS BUDGET ALLOWS

Recovery Oriented System of Care Recovery Oriented System of Care makes Cents…makes Cents…
60
Mathematical simulation of the costs of methadone treatment over the lifetime for an opiate dependent individual under the chronic vs. acute model of care: ‘We find that the benefit-cost ratio of treatment from our lifetime model (37.72) exceeds the benefit-cost ratio from a static model (4.86)’ (Zarkin et al., 2005, p. 1133).
NOT CONVINCED YET???
The Connecticut experience* (statewide ROSC)
24% decrease in expenses 46% increase in number of people served statewide62% decrease of acute care40% increase in outpatient care25% decrease in annual cost per client14% lower cost with recovery support
* 2008 statewide data from Kirk, in press in Kelly and White

Let’s get to work!Let’s get to work!

Questions? Comments?Questions? Comments?How can we help?How can we help?
http://www.attcnetwork.org/regcenters/index_northeast.asp www.ireta.org
Email: [email protected]