Embed Size (px)
Citation preview

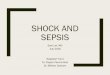
Acute Pulmonary Edema, Hypotension, & Shock Algorithm

Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Acute Pulmonary Edema
Acute Pulmonary Edema
Volume problemVolume problem Pump problemPump problem Rate problemRate problem
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/intubation if needed
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/intubation if needed
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
BradycardiaSee algorithm
BradycardiaSee algorithm
TachycardiaSee algorithm
TachycardiaSee algorithm
Blood Pressure?Blood Pressure?
Acute Pulmonary Edema, Hypotension, & Shock AlgorithmAcute Pulmonary Edema, Hypotension, & Shock Algorithm

Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Acute Pulmonary Edema
Acute Pulmonary Edema
Volume problemVolume problem Pump problemPump problem Rate problemRate problem
1st – Acute Pulmonary Edema•Furosemide•Iv 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
1st – Acute Pulmonary Edema•Furosemide•Iv 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
BradycardiaSee algorithm
BradycardiaSee algorithm
TachycardiaSee algorithm
TachycardiaSee algorithm
Blood Pressure?Blood Pressure?
Acute Pulmonary Edema, Hypotension, & Shock AlgorithmAcute Pulmonary Edema, Hypotension, & Shock Algorithm
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/intubation if needed
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/intubation if needed
Blood Pressure?Blood Pressure?

1st – Acute Pulmonary Edema
1st – Acute Pulmonary Edema
Blood Pressure?Blood Pressure?
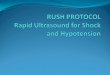
Acute Pulmonary Edema, Hypotension, & Shock AlgorithmAcute Pulmonary Edema, Hypotension, & Shock Algorithm
Systolic BPBP defines 2nd line of action
Systolic BPBP defines 2nd line of action
Systolic BP<70mm Hg
Signs & symptoms of
shock
Systolic BP<70mm Hg
Signs & symptoms of
shock
Systolic BP70 – 100mmHgSigns/symptoms of shock
Systolic BP70 – 100mmHgSigns/symptoms of shock
Systolic BP70 – 100mm HgNo signs/symptoms of shock
Systolic BP70 – 100mm HgNo signs/symptoms of shock
Systolic BP> 100mm Hg
Systolic BP> 100mm Hg
•Norepinephrine0.5 – 30 ug/min IV
•Dopamine5 – 15
ug/Kg/min IV
•Dobutamine2 – 20 ug/Kg/min IV
•Nitroglycerin10 – 20 ug/min IVConsider•Nitroprusside 0.1 – 5 ug/Kg/min
2nd-Acute Pulmonary edema•NTG/ nitroprusside if BP > 100mm Hg•Dopamine if BP= 70 – 100 mm Hg, Shock•Dobutamine if BP > 100mm Hg, No shock
Further diagnostic & therapeutic considerations•Pulmonary artery catheter•Intra-aortic balloon pump•Angiography for AMI/ ischemia

•28 Y/O, female, G2P1 in active labor•BP 160/100, CR=115/m•Sudden dyspnea after delivery of
placenta•(+) crackles both lung fields•Cold clammy extremity•Pulse oximeter: 60-70%
CASE # 1

• 12 lead EKG = ST, LAE, RAD; Tall R in V1, V2 Persistent S = V5,V6
• Chest X-Ray = Straightened LA border = Kerly B lines
• Blood-streaked, frothy sputum• Bluish nail beds• Heart: (+) opening snap;
irregularly irregular rhythm(+) diastolic rumble at the apex

1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
Acute Pulmonary EdemaAcute Pulmonary Edema
2nd-Acute Pulmonary edema•NTG/ nitroprusside if BP > 100mm Hg•Dopamine if BP= 70 – 100 mm Hg, Shock•Dobutamine if BP > 100mm Hg, No shock

• 60 Y/O, M, Smoker• Unconscious• Intubated/ambubagging• BP = 60 palpatory HR = 112/min
T=38 oC• C/L = (+) crackles BLF• Skin = cold, clammy
CASE #2

•BP = 70/40mmHg, CR = 110/min
•Still with crackles both MLF to Base
•Skin = cold, clammy•Elevated total CK, (+) troponin-T, CKMB 10X normal

•BP = 90/60mmHg, CR = 115/min
•EKG = ST elevation V1-V4•Skin/Lungs = Status Quo

•BP = 160/100mmHg•Still with crackles•Further ST segment elevation V1-V4
•Chest pain

Pump problemPump problem
Blood Pressure?Blood Pressure?
Systolic BP<70mm Hg
Signs & symptoms of
shock
Systolic BP<70mm Hg
Signs & symptoms of
shock
Systolic BP70 – 100mmHgSigns/symptoms of shock
Systolic BP70 – 100mmHgSigns/symptoms of shock
Systolic BP70 – 100mm HgNo signs/symptoms of shock
Systolic BP70 – 100mm HgNo signs/symptoms of shock
Systolic BP> 100mm Hg
Systolic BP> 100mm Hg
•Norepinephrine0.5 – 30 ug/min IV
•Dopamine5 – 15
ug/Kg/min IV
•Dobutamine2 – 20 ug/Kg/min IV
•Nitroglycerin10 – 20 ug/min IVConsider•Nitroprusside 0.1 – 5 ug/Kg/minFurther diagnostic &
therapeutic considerations•Pulmonary artery catheter•Intra-aortic balloon pump•Angiography for AMI/ ischemia

CASE # 3
• 35 Y/O, Male, Alcoholic• BP = 80 palpatory; CR = 120/min• Pale conjunctivae; pale nail beds• (+) Melena• (+) Hematamesis• Faint Pulse

• BP = 80 Palpatory• JVP = Angle of mandible• C/L = clear• Irritable; 5-pillow orthopnea• EKG: ST elevation II, III, AVF
ST elevation V4R, V3R Tall R in V1 2o AVB Mobitz I

Volume problemVolume problem
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors

Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Acute Pulmonary Edema
Acute Pulmonary Edema
Volume problemVolume problem Pump problemPump problem Rate problemRate problem
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/intubation if needed
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/intubation if needed
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
BradycardiaSee algorithm
BradycardiaSee algorithm
TachycardiaSee algorithm
TachycardiaSee algorithm
Blood Pressure?Blood Pressure?
Acute Pulmonary Edema, Hypotension, & Shock AlgorithmAcute Pulmonary Edema, Hypotension, & Shock Algorithm

Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Clinical Signs: shock, hypoperfusion, CHF, acute pulmonary edema
Most likely problem?
Acute Pulmonary Edema
Acute Pulmonary Edema
Volume problemVolume problem Pump problemPump problem Rate problemRate problem
1st – Acute Pulmonary Edema•Furosemide•Iv 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
1st – Acute Pulmonary Edema•Furosemide•Iv 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
Administer•Fluids•Blood transfusion•Cause specific interventionsConsider vasopressors
BradycardiaSee algorithm
BradycardiaSee algorithm
TachycardiaSee algorithm
TachycardiaSee algorithm
Blood Pressure?Blood Pressure?
Acute Pulmonary Edema, Hypotension, & Shock AlgorithmAcute Pulmonary Edema, Hypotension, & Shock Algorithm
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
1st – Acute Pulmonary Edema•Furosemide IV 0.5 – 1mg/kg•Morphine IV 2 – 4mg•NTG SL•Oxygen/ intubation if needed
Blood Pressure?Blood Pressure?

1st – Acute Pulmonary Edema
1st – Acute Pulmonary Edema
Blood Pressure?Blood Pressure?
Acute Pulmonary Edema, Hypotension, & Shock AlgorithmAcute Pulmonary Edema, Hypotension, & Shock Algorithm
Systolic BPBP defines 2nd line of action
Systolic BPBP defines 2nd line of action
Systolic BP<70mm Hg
Signs & symptoms of
shock
Systolic BP<70mm Hg
Signs & symptoms of
shock
Systolic BP70 – 100mmHgSigns/symptoms of shock
Systolic BP70 – 100mmHgSigns/symptoms of shock
Systolic BP70 – 100mm HgNo signs/symptoms of shock
Systolic BP70 – 100mm HgNo signs/symptoms of shock
Systolic BP> 100mm Hg
Systolic BP> 100mm Hg
•Norepinephrine0.5 – 30 ug/min IV
•Dopamine5 – 15
ug/Kg/min IV
•Dobutamine2 – 20 ug/Kg/min IV
•Nitroglycerin10 – 20 ug/min IVConsider•Nitroprusside 0.1 – 5 ug/Kg/min
2nd-Acute Pulmonary edema•NTG/ nitroprusside if BP > 100mm Hg•Dopamine if BP= 70 – 100 mm Hg, Shock•Dobutamine if BP > 100mm Hg, No shock
Further diagnostic & therapeutic considerations•Pulmonary artery catheter•Intra-aortic balloon pump•Angiography for AMI/ ischemia

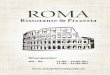
Acute Coronary Syndrome Algorithm

Acute Coronary Syndromes

Primary Goals of Therapy
• Reduce the amount of myocardial necrosis that occurs in patients with MI, preserving LV function and preventing heart failure.
• Prevent major adverse cardiac events (MACE): death, nonfatal MI, and need for urgent revascularization.
• Treat acute, life-threatening complications of ACS, such as ventricular fibrillation (VF)/pulseless ventricular tachycardia (VT),
symptomatic bradycardias, and unstable tachycardias.

Copyright ©2005 American Heart Association
Acute Coronary Syndromes Algorithm

Acute Coronary Syndromes Algorithm

Acute Coronary Syndromes Algorithm

Acute Coronary Syndromes Algorithm

Acute Coronary Syndromes Algorithm

Acute Coronary Syndromes Algorithm

Pulseless Cardiac Arrest Algorithm

Pulseless Cardiac Arrest
• Four rhythms produce pulseless cardiac arrest: - Ventricular fibrillation (VF)
- Rapid ventricular tachycardia (VT) - Pulseless electrical activity (PEA) - Asystole
• Survival from these arrest rhythms requires both basic life support (BLS) and advanced cardiovascular life support (ACLS).

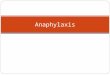
ACLS Pulseless Arrest AlgorithmACLS Pulseless Arrest Algorithm

Ventricular Fibrillation/ Pulseless Ventricular Tachycardia
• Deliver 1 shock then resume CPR immediately ( 5 cycles or 2 min)– 200 J (biphasic) for the first shock and an equal or
higher shock dose for the 2nd & subsequent shocks
• Check rhythm• Continue CPR while defibrillator is charging• Deliver shock

Providers should give 1 shock rather than 3 successive shocks which were previously recommended
First shock success rate is high
CPRCPRRHYTHM RHYTHM CHECKCHECK CPRCPR
SHOCKSHOCK

Copyright ©2005 American Heart Association
ACLS Pulseless Arrest Algorithm

Copyright ©2005 American Heart Association
ACLS Pulseless Arrest Algorithm

• If VF / pulseless VT persists after delivery of 1-2 shocks plus CPR– Give a vasopressor (epinephrine every 3-5 min) or one dose of
vasopressin
• When VF/ pulseless VT persists after 2-3 shocks plus CPR & vasopressor– Consider anti-arrhythmics such as amiodarone or lidocaine
Ventricular Fibrillation/ Pulseless Ventricular Tachycardia

Ventricular Fibrillation/ Pulseless Ventricular Tachycardia
• Minimize interruptions in chest compressions because they reduce coronary perfusion pressure.
• Establishing IV access should not interfere with CPR & delivery of shocks.
• Drugs should be administered ASAP before or after shock delivery.

• Drug doses should be prepared before the rhythm check.
• Rhythm checks should be very brief.
• Pulse checks should generally be performed if an organized rhythm is established. If there is any doubt, resume CPR.
Ventricular Fibrillation/ Pulseless Ventricular Tachycardia

Asystole & Pulseless Electrical Activity (PEA)• Pulseless electrical activity (PEA)
– Encompasses pseudo-electromechanical dissociation, idioventricular rhythm, ventricular escape rhythms, postdefibrillation idioventricular rhythms and bradyasystolic rhythms
– Often caused by reversible causes

• Does not benefit from defibrillation attempts• Perform high-quality CPR with minimal
interruptions• Continuous chest compressions 100/min• Two rescuers should change compression roles
every 2 minutes• Epinephrine can be administered every 3-5 min
Asystole & Pulseless Electrical Activity (PEA)

Medications for Arrest Rhythms
• Vasopressors
– No placebo-controlled trials have shown increased rate of neurologically intact survival to hospital discharge

Medications for Arrest Rhythms – VF/ Pulseless VT
• Epinephrine– Alpha-adrenergic effects can increase coronary &
cerebral perfusion pressure during CPR– Beta-adrenergic effects may increase myocardial work
& reduce subendocardial perfusion– No evidence to show that it improves survival– Dose: 1 mg every 3 -5 min (2-2.5 mg via endotracheal
route

• Vasopressin– Nonadrenergic peripheral vasoconstrictor that causes
coronary & renal vasoconstriction– No statistically significant differences between
vasopressin & epinephrine for return of spontaneous circulation (ROSC), 24-hour survival or survival to hospital discharge
– Dose: 40 U IV/IO
Medications for Arrest Rhythms – VF/ Pulseless VT

• Vasopressors– May consider giving vasopressin for asystole but insufficient
evidence in PEA
– Epinephrine 1mg every 3-5 min
• Atropine– Reverses cholinergic-mediated decreases in heart rate, systemic
vascular resistance & BP
– No prospective studies to support its use in asystole/ PEA
– Dose: 1 mg IV every 3 -5 min ( maximum of 3mg)
Medications for Arrest Rhythms – Asystole & PEA

• Amiodarone– Affects Na, K and Ca channels as well as alpha and
beta adrenergic blocking properties– May be administered for VF or pulseless VT
unresponsive to CPR, shock & vasopressor– Dose: 300 mg IV/IO followed by 150 mg IV/IO
Medications for Arrest Rhythms – Antiarrhythmics

• Lidocaine– Alternative anti-arrhythmic to Amiodarone– No proven short-term or long-term efficacy in cardiac
arrest– Initial dose: 1-1.5 mg/kg IV, then 0.5 – 0.75 mg/kg IV
push every 5 -10 minutes ( maximum dose of 3 mg/kg)
Medications for Arrest Rhythms – Antiarrhythmics

• Magnesium– Effectively terminates torsades de pointes– Not effective in irregular/ polymorphic VT in patients
with normal QT– Dose: 1-2 g in 10 ml D5W IV/IO push over 5-20min– When with pulse, 1-2 g in 50-100 ml D5W
Medications for Arrest Rhythms – Antiarrhythmics

Interventions not Supported by Outcome Evidence
• Pacing in arrest• Procainamide in VF and Pulseless VT• Norepinephrine• Precordial thump for VF/ pulseless VT• Electrolyte therapies in arrest rhythms (Magnesium)• Routine administration of IV fluids during arrest

Thank you for your attention !