Embed Size (px)
Citation preview

Alice Guh, MD, MPH
Division of Healthcare Quality PromotionCenters for Disease Control and Prevention
CSTE CRE Panel Session – June 14, 2011
Public Health Response to Carbapenem-Resistant Enterobacteriaceae:
The Role of Health Departments
National Center for Emerging and Zoonotic Infectious Diseases
Division of Healthcare Quality Promotion

Carbapenem-resistant Enterobacteriaceae (CRE)
Common cause of HAIs Found in both acute care hospitals and long-term
care settings Since 2004, reports of CRE cases from LTACH and
LTCF
Similar to the spread of other MDROs Movement of colonized patients across the
continuum of care contributes to regional transmission
Supported by mathematical modeling
Urban C et al. Clin Infect Dis 2008;46:e127030Endimiani A et al. J Antimicrob Chemother 2009;64:1102-1110.Smith DL et al. PNAS 2004;101:3709-14.

Inter-Facility Transmission of MDROs (Including CRE)
Munoz-Price SL. Clin Infect Dis 2009;49:438-43.
Regional Approach to MDRO Prevention is Essential
Rationale for regional approach What happens in one facility will impact
surrounding facilities Individual facilities can reduce MDRO prevalence
only to a certain point
Successful regional coordination by public health VRE control in Siouxland region CRE containment in Israel
Sohn AH et al. Am J Infect Control 2001;29:53-7.Schwaber MJ et al. Clin Infect Dis 2011;52:848-55.

How to Operationalize Public Health Response to Emerging MDROs
Opportunity to apply regional approach to CRE prevention
HDs in unique position to coordinate local and regional response to CRE Assess CRE prevalence/incidence within their
jurisdiction in order to provide situational awareness to facilities
Serve as resource to facilities about prevention options
Informs public health response to other emerging MDROs

DEVELOPMENT OF CRE TOOLKIT

Outline of CRE Toolkit
Facility-level prevention strategy for facilities and HDs
Regional prevention strategy specifically for HDs Aggressive approach to contain or prevent CRE
emergence • Regions with no CRE identified• Regions with few CRE identified
Regional Prevention Strategy
Regional Surveillance for CRE
Determine CRE prevalence within a given jurisdiction Make CRE laboratory reportable (in regions with
no known or few CRE) Survey IPs or lab directors
Feedback of surveillance results Provide specific enough data for facilities to act
upon • Facility name, if possible
or• Stratify results by geographic area and/or by facility
type

Regional Prevention Strategy
Regions With No CRE Identified
Aggressive efforts at detection: Perform periodic surveillance and feedback
Frequency may depend on CRE prevalence in neighboring regions (establish mechanism for communication)
Educate facility staff to increase awareness Epidemiologic importance of CRE Recommended surveillance and prevention
measures*
* http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5810a4.htm

Regional Prevention Strategy
Regions With Few CRE Identified
Aggressive efforts at containment, may target select areas:
Implement infection prevention measures Reinforce core prevention measures in all facilities Facilities with CRE: use supplemental measures Facilities without CRE: targeted surveillance testing,
preemptive CP
Use inter-facility patient transfer forms Indicate CRE status, open wounds/devices,
antimicrobial therapy
Educate facility staff to increase awareness
Perform periodic surveillance and feedback
REGIONAL CRE SURVEILLANCE BY SELECT HEALTH DEPARTMENTS
Development of CRE Survey
Fall 2010 – CRE conference calls with interested HDs to identify actionable steps to take HDs notified through CSTE HAI listserve
CRE survey template designed to be used by HDs to assess CRE prevalence within their jurisdiction 7 questions to administer to IPs of acute care
facilities Estimate frequency of CRE colonized- or infected-
patients Assess facility-level surveillance activities for CRE
and related prevention measures** http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5810a4.htm

State HDs Conducting CRE Survey (n=7)
Utah Illinois
Virginia Idaho
South Carolina West Virginia
Wisconsin

Administration of CRE Survey
Targeted acute care hospitals, but included: Long-term acute care hospitals (≥3 states) Critical access hospitals (≥2 states)
Survey methods by HDs Email /online survey (e.g., Survey Monkey) to IPs Paper survey at APIC meetings
Date of survey: ranged Sep 2010-Mar 2011 Survey lasted one day to 2-3 months Sent reminder emails, phone calls to non-
respondents

Survey Respondents
Aggregated state-level data across all 7 states: Median response rate – 67% (range: 26% to 100%)
Breakdown by bed size (n=6 states): Total 360 facilities ≤50 beds – 30% 51-200 beds – 39% 201-500 beds – 27% >500 beds – 4%
Fairly representative of national data (2008 AHA data) Except greater % of facilities with ≤50 beds
captured in survey

CRE Prevalence in Past 12 Months (n=7 states)
Percentage of Facilities Per State
CRE Prevalence Median Range
Identified CRE 30 10-46
Daily or weekly 0 0-16
Monthly or greater 100 84-100
≤48 hrs of admission 92 74-100
>48 hrs of admission 59 25-75
Do not know if have CRE 12 10-18
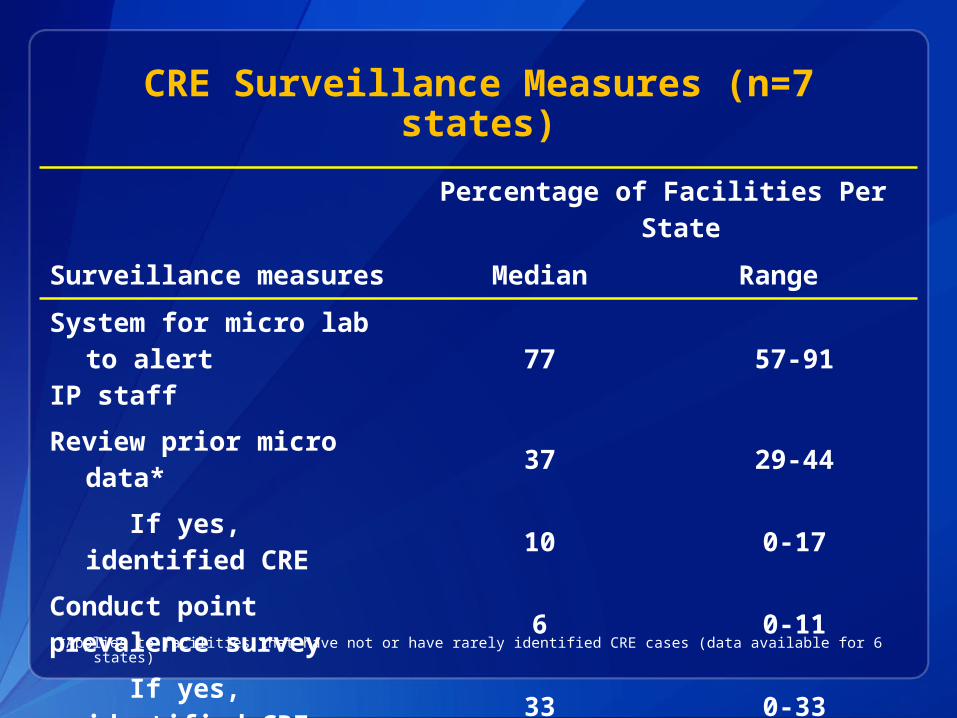
CRE Surveillance Measures (n=7 states)
Percentage of Facilities Per State
Surveillance measures Median Range
System for micro lab to alert
IP staff77 57-91
Review prior micro data* 37 29-44
If yes, identified CRE 10 0-17
Conduct pointprevalence survey 6 0-11
If yes, identified CRE 33 0-33
Conduct AST of epi-linked
patients12 10-18
*Applies to facilities that have not or have rarely identified CRE cases (data available for 6 states)
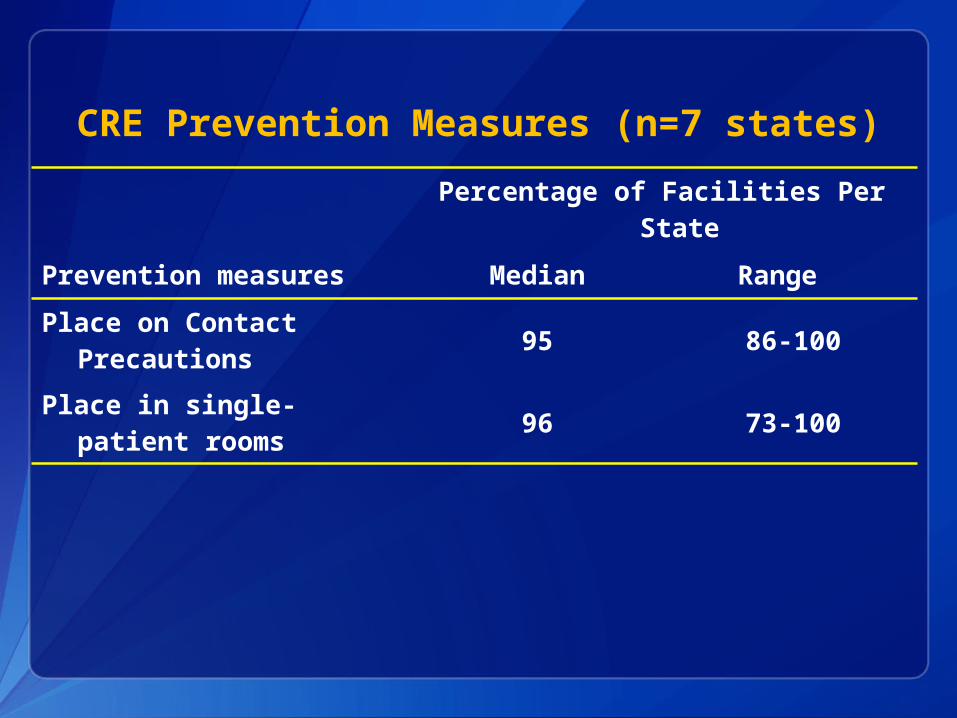
CRE Prevention Measures (n=7 states)
Percentage of Facilities Per State
Prevention measures Median Range
Place on Contact Precautions 95 86-100
Place in single-patient rooms 96 73-100

Summary of CRE Survey Results
CRE identified in <50% of all responding facilities, still have opportunity to prevent full emergence
Although there is intra-facility transmission, majority of identified cases are imported Important role of inter-facility patient sharing Supports the need for regional approach to
prevention
Low facility adherence to recommended surveillance practices and need for increased education / awareness Potential under-reporting of CRE

Feedback of Survey Results by HDs
At least 5 states provided feedback to IPs / facilities Email (memo, monthly HAI newsletter) Presentation at APIC meeting
Feedback content Only shared aggregated results
• Some stratified by geographical region (n=2), facility type (n=1)
Some provided streamlined 2009 MMWR guidance* (n=3)
* http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5810a4.htm

INTERVIEWS WITH STATE HEALTH DEPARTMENTS

Key Informant Interviews
Primary objective: to understand why some HDs decided to conduct CRE survey and others did not
Participants All 7 states that conducted CRE survey 4 additional states that did not conduct CRE
survey (participants of initial CRE calls via CSTE HAI listserve)
Standardized script with trained interviewer

Key Interview Findings (n=11 states)
All HDs communicated regularly with IPs about HAI topics in previous 12 months (prior to CRE survey)
No difference between states in competing priorities and concerns about CRE survey Main concern – perception of overburdening IPs
Yet perspectives differed regarding conducting survey: opportunity to learn vs concerns about survey intent and logistics and other data source Assess for other confounders and contextual
factors Evaluate alternative sources to IPs for information

CASTING A VISION FOR PUBLIC HEALTH ACTION

Anywhere County, USAStatus Report: Emerging MDRO X
St. Joseph’s Hosp
St. Vincent’s Hosp
St. Mary’s LTACH Orangetown
LTACHSmallville Hosp
Peachtree Hosp Smithville
LTACH
Magnolia LTCF
Appletree Hosp
St. Peter’s Hosp
Jamesville Hosp
Greensville LTCF
St. Claire’s LTACH
Thomasville Hosp
Franklin Hosp
For more information please contact Centers for Disease Control and Prevention1600 Clifton Road NE, Atlanta, GA 30333Telephone, 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348E-mail: [email protected] Web: www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
National Center for Emerging and Zoonotic Infectious Diseases
Division of Healthcare Quality Promotion
Thank you





























