Embed Size (px)
Citation preview

ONLINE ONLY
Alignment efficiency of Damon3 self-ligatingand conventional orthodontic bracket systems:A randomized clinical trialPaul Scott,a Andrew T. DiBiase,b Martyn Sherriff,c and Martyn T. Cobourned
London, United Kingdom
Introduction: The aim of this study was to compare the efficiency of mandibular tooth alignment and theclinical effectiveness of a self-ligating and a conventional preadjusted edgewise orthodontic bracket system.Methods: A multicenter randomized clinical trial was conducted in 2 orthodontic clinics. Sixty-two subjects(32 male, 30 female; mean age, 16.27 years) with mandibular incisor irregularities of 5 to 12 mm and aprescribed extraction pattern including the mandibular first premolars were randomly allocated to treatmentwith Damon3 self-ligating (Ormco, Glendora, Calif) or Synthesis (Ormco) conventionally ligated brackets.Fully ligated 0.014-in nickel-titanium archwires were used first in both groups, followed by a sequence of0.014 � 0.025-in and 0.018 � 0.025-in nickel-titanium, and 0.019 � 0.025-in stainless steel. Study castswere taken at the start of treatment (T1), the first archwire change (T2), and the placement of the final0.019 � 0.025-in archwire (T3). Cephalometric lateral skull and long-cone periapical radiographs of themandibular incisors were taken at T1 and T3. Results: No significant difference was noted (P �0.05) in initialrate of alignment for either bracket system. Initial irregularity influenced subsequent rate of movement, butsex, age, and appliance type were statistically insignificant. Alignment was associated with an increase inintercanine width, a reduction in arch length, and proclination of the mandibular incisors for both appliances,but the differences were not significant. Incisor root resorption was not clinically significant and did not differbetween systems. Conclusions: Damon3 self-ligating brackets are no more efficient than conventionalligated preadjusted brackets during tooth alignment. (Am J Orthod Dentofacial Orthop 2008;134:
470.e1-470.e8)The first phase of fixed appliance orthodontictreatment is concerned with tooth alignment, withthe effectiveness of this process dependent on
several variables. Clearly, the underlying tissue biologywill play a significant role; the response of the periodon-tium to the applied orthodontic force provides the funda-mental mechanism that allows tooth movement throughalveolar bone.1 Tissue vitality, cellular and connectivetissue response, and periodontal health all contribute tothe success of orthodontic tooth movement. Althoughthese biologic factors are largely outside the control of the
From King’s College London.aSpecialist registrar, Department of Orthodontics, East Kent Hospitals NHSTrust.bConsultant orthodontist, Department of Orthodontics, East Kent HospitalsNHS Trust.cReader in biomaterials, Department of Biomaterials, King’s College LondonDental Institute.dReader and honorary consultant in Orthodontics, Department of Orthodonticsand Craniofacial Development, King’s College London Dental Institute.Reprint requests to: Martyn Cobourne, King’s College Dental Institute,Floor 22, Guy’s Hospital, London, SE1 9RT, United Kingdom; e-mail,[email protected], January 2008; revised and accepted, April 2008.0889-5406/$34.00Copyright © 2008 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2008.04.018orthodontist, more direct influence can be achieved withthe choice of bracket system and archwire.
When using preadjusted edgewise brackets, importantfactors in determining the rate of tooth alignment includethe bracket slot dimension, the associated interbracketspan,2 and the choice of archwire.2-5 Frictional forcesgenerated between bracket and archwire also have asignificant effect on tooth movement.6 Friction is influ-enced by the physical characteristics of the archwire andbracket materials, and the method of attachment betweenarchwire and bracket.7,8 Conventional ligated edgewisebrackets incur increased levels of frictional resistance viathe elastomeric attachment between bracket and arch-wire.9-11 To reduce unwanted friction, various self-ligat-ing bracket systems have been developed. Self-ligationeliminates the requirement for an elastomeric attachmentand is associated with considerably reduced friction withdifferent archwires.12-15 Self-ligating brackets may alsooffer more certain archwire engagement, a requirementfor less chair-side assistance and faster archwire re-moval and ligation.16,17 Significantly, an overallreduction in treatment time has been associated withthese appliances16,18; however, this is not necessarily
associated with more rapid tooth alignment.19,20470.e1

American Journal of Orthodontics and Dentofacial OrthopedicsOctober 2008
470.e2 Scott et al
It is certainly desirable for fixed appliances to beplaced in a patient’s oral cavity for as short a time aspossible; these appliances increase plaque accumulation,make tooth brushing more difficult, and can promote bothcaries and periodontal disease. Therefore, any appliancesystem that can increase the rate of tooth alignment is apotential clinical advance. However, excessive forces andtoo-rapid tooth movement can also have undesirableside-effects. These include patient discomfort21,22 and lossof tooth root length due to resorption.23,24 It is importantto evaluate any new appliance system for its ability toalign teeth rapidly and predictably, but with minimaldeleterious effects to the oral tissues.
The Damon self-ligating bracket (Ormco, Glendora,Calif) was developed as an integral component of alow-friction appliance.25,26 It has been suggested that thelow-level friction associated with this bracket encouragesmore rapid levelling and alignment, allowing longerappointment intervals and reducing overall treatmenttime, although this evidence is largely anecdotal,26,27 andto date there is little robust clinical evidence to supportthese claims.20,28 The aim of this randomized clinical trialwas to compare the clinical efficiency of Damon3 self-ligating brackets with a conventional ligated bracketsystem during orthodontic tooth alignment. The primaryoutcome measure was rapidity of tooth alignment, al-though secondary outcome measures included changes inroot length and associated changes in arch dimension.
MATERIAL AND METHODS
The primary outcome in this investigation was rateof mandibular incisor alignment measured from serialdental casts by using Little’s irregularity index,29 andthis was used to calculate the sample size. Mean contactpoint movement by using a Titanol archwire waspreviously reported as 1.7 mm (SD, 0.79) over 34days4; this gives a mean alignment rate of 0.05 mm perday. Because the mean contact point displacement inthis sample was 3.12 mm, it would take about 62 days
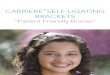
Fig 1. T1 occlusal views of the mandibularSynthesis (left) and the Damon (right) groups.
to align the teeth at this rate. We hypothesised that
reducing the alignment time by 20 days would producea clinically relevant difference, and therefore this ratewould have to be 0.073 mm per day, an increase of0.023 mm in the daily rate of movement. Therefore, thetotal alignment achieved after 34 days at the new ratewould be 2.48 mm, giving a clinically relevant differ-ence of 0.8 mm. The standardized difference would be0.98, and with a nomogram at a power of 95% and asignificance level of 0.05, this would require a totalsample size of 55 subjects.30
Ethical approval was obtained from the Guy’sHospital Research Ethics Committee (no. 04/Q0704/116), and written consent was received from all parentsor guardians and children. The subjects were recruitedfrom consecutive patients attending the orthodonticdepartments at the Guy’s campus of King’s CollegeLondon Dental Institute and the Kent and CanterburyHospital who satisfied the following criteria: (1) under30 years of age at the start of treatment; (2) no medicalcontraindications; (3) permanent dentition; (4) mandib-ular incisor irregularity of 5 to 12 mm; (5) extraction ofmandibular first premolars included in the treatmentplan; and (6) absence of a complete overbite. Repre-sentative samples are shown in Figure 1.
The subjects were randomly allocated for treatmentwith either Damon3 self-ligating brackets or Synthesis(Ormco) preadjusted edgewise brackets by using arestricted random number table to ensure equivalenceof numbers in each group. Both bracket systems use a
Table I. Bracket prescriptions used in the mandibulararch
Incisors Canine Second premolar
Damon tip �2° �5° �2°Synthesis (Roth) tip �2° �7° 1°Damon torque �1° 0° �17°Synthesis (Roth) torque �1° �11° �22°
l arches of representative subjects from the
denta0.22-in slot and either a Damon or a Roth prescription

American Journal of Orthodontics and Dentofacial OrthopedicsVolume 134, Number 4
Scott et al 470.e3
(Table I). A CONSORT diagram showing the flow ofsubjects through the trial is shown in Figure 2.31 A totalof 62 subjects were recruited, with 29 allocated to theSynthesis appliance and 33 to the Damon3. One subjectwas subsequently lost for each appliance—from theSynthesis group after declining treatment and from theDamon3 group after requesting appliance removal 2weeks after placement. This left 60 subjects—28 Syn-thesis and 32 Damon3—with the sample size thereforeachieving a power of 95% for this investigation.
The bonding method was standardized betweengroups, by using conventional etching and BluGloo(Ormco) bracket adhesive according to the manufactur-ers’ instructions. After bracket bonding, Damon arch-form 0.014-in copper-nickel-titanium (Ormco) arch-wires were placed and ligated to all teeth by using theself-ligation system for Damon3 or standard elasto-meric ligatures for Synthesis. The subjects were re-viewed approximately every 6 weeks, and a sequenceof 0.014 � 0.025-in and 0.018 � 0.025-in copper-nickel-titanium, followed by 0.019 � 0.025-in stainlesssteel archwires was used. Archwire progression occurredonly if full bracket engagement was achievable. Mandib-ular dental study casts were taken at appliance placement(T1), the first adjustment signified by placement of the
Fig 2. CONSORT flow diagram of p
0.014 � 0.025-inch copper-nickel-titanium archwire (T2),
and the end of alignment signified by placement of a0.019 � 0.025-in stainless steel archwire (T3).
The initial rate of alignment for each bracket systemwas measured from the difference in the irregularity indexof serial casts taken at T1 and T2, divided by the numberof days between the 2 measurements. The overall rate ofalignment was measured as the number of days from T1to T3.
Changes in arch dimensions were measured fromdental study casts taken at T1 and T3. Arch widthwas represented by the intercanine (distance betweenthe mandibular canine cusp tips) and intermolar(distance between the mandibular first molar’s cen-tral grooves) widths; arch length was represented bythe mean distance between the mesial first molarcontact point to the midpoint between the centralincisors. All dental cast measurements were takenwith digital calipers (ISO 9001, 150-mm electroniccaliper, Tesa Technology, Renens, Switzerland).Changes in arch length were represented by mandib-ular incisor inclination to the mandibular planemeasured from serial cephalograms at T1 and T3.Together, these measurements allowed determinationof differences in the method of alignment of the 2bracket systems between T1 and T3.
ants through each stage of the trial.
articipRoot length of the mandibular right first incisor was

American Journal of Orthodontics and Dentofacial OrthopedicsOctober 2008
470.e4 Scott et al
measured by using long-cone periapical radiographstaken at T1 and T3. Briefly, crown length was measuredas the distance from the cementoenamel junction to theincisal edge at T1 (CT1) and T3 (CT3). A correctionfactor (CT1/CT3) was calculated for enlargement dif-ferences between radiographs taken at T1 and T3.Apical root resorption was measured as root length (R)at T1 (RT1) minus root length at T3 (RT3) andmultiplied by the correction factor. Therefore, thecalculated apical root resorption � RT1 – RT3 �(CT1/CT3).32 Periapical radiographs were measuredwith the digital calipers.
All measurements were made blindly by the sameexaminer (P.S.). Reproducibility of the study cast,cephalometric, and periapical radiograph measure-ments was assessed by calculating Bland Altman limitsof agreement for 20 repeated measurements made 2weeks apart.33 For study cast measurements, the limitsof agreement were 1.101 to 1.440, with only 1 mea-surement outside these bounds. The limits of agreementranged from –1.576 to 1.426 for mandibular incisorinclination and from –0.175 to 0.217 for change in rootlength. In both cases, only 1 result was outside thisbound. All data were analyzed with Stata statisticalsoftware with significance predetermined at � � 0.05(version 10, StataCorp 2003, College Station, Tex).
RESULTS
The treated sample consisted of 31 males (52%) and29 females (48%), with male subjects making up 38%of the Damon3 group and 68% of the Synthesis group.The mean age at T1 for the whole sample was 16.27
Fig 3. Scattergram of alig
years (SD, 4.47 years); mean ages were 16.19 (SD,
3.68) and 16.38 (SD, 5.28) years for the Damon3 andSynthesis groups, respectively. The Synthesis grouphad a slightly higher mean irregularity at T1 of 12.44mm (SD, 3.72 mm) compared with the Damon3 group(11.23 mm; SD, 3.18 mm).
For the rate of initial incisor alignment between T1and T2, the Synthesis group had a slightly higher meanrate of initial incisor alignment of 0.135 mm per daycompared with 0.119 mm per day in the Damon3group. The gradient of the rate vs the irregularityscattergran at T1 suggested an effect of initial irregu-larity on the subsequent rate of tooth movement for bothappliances (Fig 3). As a consequence, the effects ofappliance, sex, and age (stratified as �16 and �16)were investigated by using analysis of covariance(ANCOVA), with start irregularity as the covariate.Interestingly, there was no significant effect of appli-ance (P � 0.79), sex (P � 0.268), or age (P � 0.121),or any of their interactions, on the rate of initial toothalignment. However, irregularity at T1 was significant(P � 0.001). Further analysis of the rate for eachappliance was undertaken by using analysis of variance(ANOVA), which gave linear prediction rates of 0.128mm per day for Synthesis and 0.125 mm per day for
Table II. Mean time to complete alignment (T3) bybracket system
Mean time to T3 in days (SD)
Synthesis 243 (82.5)Damon3 253 (63.6)
rate vs irregularity at T1.
nmentDamon3. Therefore, only incisor irregularity at T1 had

nd Da
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 134, Number 4
Scott et al 470.e5
any effect on initial incisor alignment; appliance typewas not significant.
The results for treatment time to final alignment at T3are shown in Table II. The mean time to final alignment(T1-T3) was slightly less for the Synthesis group com-pared with the Damon3 group. This gave mean rates of0.056 mm per day (SD, 0.022) for Synthesis and 0.047mm per day (SD, 0.047) for Damon3. Again, there was nosignificant effect of appliance, sex, or age on this overallrate to complete alignment. Figure 4 shows the minimaldifferences between treatment time and appliance for thewhole sample.
Table III shows the mean changes in arch width foreach appliance system as measured from dental casts
Fig 4. Variations in treatment duration to alignmof patients with crowded teeth in the mandibulano significant differences between Synthesis a
Table III. Mandibular intercanine, intermolar, and arch-
Model measurementTotal sample
meanTotal sample
SD
T1 (3-3) 25.73 2.63T3 (3-3) 28.34 1.93Change T1-T3 (3-3) �2.61 2.28T1 (6-6) 46.49 3.47T3 (6-6) 46.73 3.31Change T1-T3 (6-6) �0.24 2.28T1 (AL) 58.31 4.12T3 (AL) 56.47 3.88Change T1-T3 (AL) 1.84 3.03
3-3, Intercanine; 6-6, intermolar; AL, arch length.
taken at T1 and T3. Both appliance systems produced an
increase in intercanine width of approximately 2.5 mmduring tooth alignment. In contrast, changes in intermolarwidth were less; whereas Synthesis brackets increased thisdimension by approximately 0.5 mm, Damon3 bracketswere associated with a small decrease. Therefore, for bothsystems, the arch-width changes associated with correc-tion of crowding were primarily increased intercaninewidths, and these were not significantly different. Archlength decreased during the alignment phase for bothappliances (Table III); these reductions amounted to justover 1 and 2 mm for the Synthesis and Damon3 appli-ances, respectively. The differences were not statisticallysignificant between appliances.
Mean values for mandibular incisor inclination to
ith appliance. The y-axis shows the proportionat different times in days from T1. There weremon appliances.
changes (mm) induced by alignment from T1 to T3
thesisean
SynthesisSD
Damonmean
DamonSD P
6.10 2.74 25.41 2.548.76 2.11 27.96 1.712.66 2.33 �2.55 2.27 0.746.20 3.55 46.74 3.456.83 3.5 46.65 3.180.63 2.12 0.09 2.40 0.257.91 4.21 58.65 4.086.58 4.08 56.38 3.771.33 3.39 2.27 2.63 0.18
ent wr arch
length
Synm
22
�44
�55
the mandibular plane at T1 and T3 for the 2 appli-

6.0
American Journal of Orthodontics and Dentofacial OrthopedicsOctober 2008
470.e6 Scott et al
ance systems are shown in Table IV. Both appliancesproclined the mandibular incisors between T1 andT3, with Synthesis brackets producing a mean of2.34° (SD, 3.72°) and Damon3 achieving 1.73° (SD,4.06°). Therefore, treatment of crowding resulted insome proclination of the incisors, although thesechanges were not significant with respect to appli-ance type.
Mean root resorption values associated with themandibular right central incisor were 1.21 mm (SD,3.39) for Synthesis and 2.26 mm (SD, 2.63) forDamon3. There was no statistically significant differ-ence between bracket type and mandibular incisor rootresorption.
DISCUSSION
This investigation has shown that, in the sampleinvestigated, the Damon3 appliance system was nomore clinically effective than a conventional ligatedappliance during the alignment phase of orthodontictreatment. Clinical effectiveness was measured in termsof the initial rate of tooth alignment and overall rate toplacement of a 0.019 � 0.025-in stainless steel workingarchwire, and root resorption associated with the man-dibular incisors. In addition, the mechanism of toothalignment was studied in relation to changes in archwidth and arch length by using dental casts; mandibularincisor inclination was measured from cephalometriclateral skull radiographs.
Neither the Damon220,28 nor the Smartclip19 self-ligating bracket systems have previously been shown tobe more clinically effective than conventional ligatedbrackets during tooth alignment. However, for moder-ate crowding with an irregularity index of �5 mm,there is some evidence that Damon2 brackets canproduce faster correction, although this becomes mar-ginally insignificant for more severe crowding.28 Apossible explanation for this finding is that, as teethbecome more displaced, free sliding of the archwire inthe bracket slot, which is afforded by a self-ligatingbracket and theoretically potentiates tooth alignment, isnegated.28 This might explain the lack of a significantdifference between appliance systems in this study,where the mean initial irregularity index was about 12
Table IV. Changes in mandibular incisor inclination (deg
MeasurementTotal sample
mean
Mandibular incisor-mandibular plane T1 90.70Mandibular incisor-mandibular plane T3 92.71
mm, generally regarded as representing more severe
crowding. Significantly, the only factor in this investi-gation that influenced the rate of alignment was theamount of initial irregularity; this effect was seen forboth bracket types. Therefore, the proposed advantagesof reduced force levels and friction associated withDamon3 brackets do not appear to result in more rapidtooth alignment, either initially or at later stages tocompletion. Teeth only seem to align faster when theyare more displaced to start with, irrespective of theappliance placed on them.
It has also been suggested that the Damon systemmechanics rely less on the need for extraction if there iscrowding (www.ormco.com). As a preferred nonex-traction appliance, it can be speculated that Damonbrackets might have performed more effectively inpatients treated without the loss of premolars, regard-less of the amount of initial crowding. However, thechanges in arch dimension in our 2 groups did not differsignificantly; this is perhaps not surprising because thesame Damon arch form was used for both groups. Bothappliances expanded the intercanine width with essen-tially no change in the intermolar width. A tendency forthe canines to move distally into the first premolarextraction spaces during incisor alignment might ex-plain the changes in this dimension. Interestingly, theintermolar width increased in a previous study ofnonextraction alignment using Damon2 brackets andthe same prescribed Damon-system archwire se-quence.28 It is possible that, in this investigation,midarch premolar extractions might have allowed someforward movement of the first molars during alignment,negating any effects of archwire-induced expansion,even though the aligning archwires were not cincheddown. A further finding was that tooth alignment in themandibular arch was associated with some overallreduction in arch length that occurred despite proclina-tion of the mandibular incisors. Although wide individ-ual variation was seen in mandibular incisor proclina-tion in both samples, the overall arch-length reductionmight also reflect forward movement of the first molars.Although not significantly different, the arch-lengthreduction was greater with the Damon3 appliance; thiswas consistent with the reduced amount of mandibularincisor proclination in this group. However, despite
induced by alignment from T1 to T3 per bracket group
mple Synthesismean
SynthesisSD
Damonmean
DamonSD
90.98 4.93 90.41 5.184 93.32 5.01 92.11 7.07
rees)
Total saSD
5.0
this, the reduced friction associated with Damon3

American Journal of Orthodontics and Dentofacial OrthopedicsVolume 134, Number 4
Scott et al 470.e7
brackets might be expected to produce a significantdifference between appliances in how the teeth werealigned, but this did not happen. This suggests that thereduced friction levels allow more spontaneous toothmovement into extraction spaces during alignment.
A potential criticism regarding true equivalence ofour 2 groups is differences in bracket prescriptionvalues between the 2 appliances. Damon3 bracketshave a specific Damon prescription, but Synthesisbrackets have a Roth prescription (Table I). Theseprescription values were identical for mandibular inci-sors in both tip and torque; this might explain why theincisor proclination did not differ significantly betweenthe groups. There were some differences in tip valuesfor mandibular canines and second premolars, but thesewere not more than 3° for either tooth. The torquevalues varied more significantly between prescriptionsfor the canines and the second premolars, but datacollection for this investigation ended on placement ofthe 0.019 � 0.025-in stainless steel archwires beforefull torque expression; therefore, these differencesmight not be expected to have a major effect betweenappliance systems.
The mean root resorption in this investigation wasless than 2.5 mm for both appliances; this was notclinically significant.23 However, this change was mea-sured only during the alignment phase, and, as anextraction sample, some space closure would inevitablybe required that might precipitate further loss of rootlength. There were no significant differences in rootresorption between appliances, but the standard devia-tions were large; this finding was also seen in previousstudies evaluating treatment efficiency.32
We did not evaluate all the proposed advantages ofself-ligating bracket systems: in particular, those for theorthodontic operator, including less reliance on chair-side assistance and improved speed of archwire re-moval and ligation.16,17 In addition, it would be inter-esting to evaluate the rate of space closure andsubsequent torque expression in the maxillary incisorsbetween appliances.34 The impact of patient discomfortduring tooth alignment is the subject of another inves-tigation,35 and the psychological effect of the improvedesthetics of the Damon3 bracket was not investigated.On an anecdotal level, considerable difficulty wasexperienced with bracket failure in the Damon3 group.The metallic component often became detached fromthe composite base. This had a negative impact for bothpatient and operator in terms of additional appoint-ments for repairs and could have affected treatmenttime. However, we assume that this problem will beeliminated with appropriate modifications to the design
and manufacture of these brackets and should not affecttheir future use as an innovative ligature-free fixedorthodontic appliance.
CONCLUSIONS
The results of this randomized clinical trial suggestthe following conclusions.
1. There was no difference in the initial or the overallrate of mandibular incisor alignment between Syn-thesis conventional ligated and Damon3 self-ligatedbracket systems. The only significant influence oninitial rate of incisor alignment was the amount ofinitial irregularity; age, sex, and bracket type werenot statistically significant.
2. Incisor alignment was associated with an increasein intercanine width, maintenance of intermolarwidth, some reduction in arch length, and proclina-tion of the mandibular incisors for both appliances,but the differences were not significant.
3. There were no significant differences in the amountof mandibular incisor resorption associated withalignment with Synthesis and Damon3 brackets.
REFERENCES
1. Sandy JR, Farndale RW, Meikle MC. Recent advances inunderstanding mechanically induced bone remodeling and theirrelevance to orthodontic theory and practice. Am J OrthodDentofacial Orthop 1993;103:212-22.
2. Cobb NW 3rd, Kula KS, Phillips C, Proffit WR. Efficiency ofmulti-strand steel, superelastic Ni-Ti and ion-implanted Ni-Tiarchwires for initial alignment. Clin Orthod Res 1998;1:12-9.
3. Evans TJ, Jones ML, Newcombe RG. Clinical comparison andperformance perspective of three aligning arch wires. Am JOrthod Dentofacial Orthop 1998;114:32-9.
4. O’Brien K, Lewis D, Shaw W, Combe E. A clinical trial ofaligning archwires. Eur J Orthod 1990;12:380-4.
5. West AE, Jones ML, Newcombe RG. Multiflex versus super-elastic: a randomized clinical trial of the tooth alignment abilityof initial arch wires. Am J Orthod Dentofacial Orthop 1995;108:464-71.
6. Tidy DC. Frictional forces in fixed appliances. Am J OrthodDentofacial Orthop 1989;96:249-54.
7. Ireland AJ, Sherriff M, McDonald F. Effect of bracket and wirecomposition on frictional forces. Eur J Orthod 1991;13:322-8.
8. Taylor NG, Ison K. Frictional resistance between orthodonticbrackets and archwires in the buccal segments. Angle Orthod1996;66:215-22.
9. Michelberger DJ, Eadie RL, Faulkner MG, Glover KE, PrasadNG, Major PW. The friction and wear patterns of orthodonticbrackets and archwires in the dry state. Am J Orthod DentofacialOrthop 2000;118:662-74.
10. Pizzoni L, Ravnholt G, Melsen B. Frictional forces related toself-ligating brackets. Eur J Orthod 1998;20:283-91.
11. Schumacher HA, Bourauel C, Drescher D. The influence ofbracket design on frictional losses in the bracket/arch wiresystem. J Orofac Orthop 1999;60:335-47.
12. Henao SP, Kusy RP. Evaluation of the frictional resistance ofconventional and self-ligating bracket designs using standardized
archwires and dental typodonts. Angle Orthod 2004;74:202-11.
American Journal of Orthodontics and Dentofacial OrthopedicsOctober 2008
470.e8 Scott et al
13. Khambay B, Millett D, McHugh S. Evaluation of methods ofarchwire ligation on frictional resistance. Eur J Orthod 2004;26:327-32.
14. Read-Ward GE, Jones SP, Davies EH. A comparison of self-ligating and conventional orthodontic bracket systems. Br JOrthod 1997;24:309-17.
15. Thorstenson GA, Kusy RP. Resistance to sliding of self-ligatingbrackets versus conventional stainless steel twin brackets withsecond-order angulation in the dry and wet (saliva) states. Am JOrthod Dentofacial Orthop 2001;120:361-70.
16. Harradine NW. Self-ligating brackets and treatment efficiency.Clin Orthod Res 2001;4:220-7.
17. Turnbull NR, Birnie DJ. Treatment efficiency of conventional vsself-ligating brackets: effects of archwire size and material. Am JOrthod Dentofacial Orthop 2007;131:395-9.
18. Eberting JJ, Straja SR, Tuncay OC. Treatment time, outcome,and patient satisfaction comparisons of Damon and conventionalbrackets. Clin Orthod Res 2001;4:228-34.
19. Miles PG. SmartClip versus conventional twin brackets forinitial alignment: is there a difference? Aust Orthod J 2005;21:123-7.
20. Miles PG, Weyant RJ, Rustveld L. A clinical trial of Damon 2 vsconventional twin brackets during initial alignment. AngleOrthod 2006;76:480-5.
21. Ngan P, Kess B, Wilson S. Perception of discomfort by patientsundergoing orthodontic treatment. Am J Orthod DentofacialOrthop 1989;96:47-53.
22. Wilson S, Ngan P, Kess B. Time course of the discomfort inyoung patients undergoing orthodontic treatment. Pediatr Dent1989;11:107-10.
23. Linge L, Linge BO. Patient characteristics and treatment vari-ables associated with apical root resorption during orthodontic
treatment. Am J Orthod Dentofacial Orthop 1991;99:35-43.24. Remington DN, Joondeph DR, Årtun J, Riedel RA, Chapko MK.Long-term evaluation of root resorption occurring during orth-odontic treatment. Am J Orthod Dentofacial Orthop 1989;96:43-6.
25. Damon DH. The Damon low-friction bracket: a biologicallycompatible straight-wire system. J Clin Orthod 1998;32:670-80.
26. Damon DH. The rationale, evolution and clinical application ofthe self-ligating bracket. Clin Orthod Res 1998;1:52-61.
27. Loh KW. Rapid tooth movement with a low-force, low-frictionbracket system. J Clin Orthod 2007;41:451-7.
28. Pandis N, Polychronopoulou A, Eliades T. Self-ligating vsconventional brackets in the treatment of mandibular crowding:a prospective clinical trial of treatment duration and dentaleffects. Am J Orthod Dentofacial Orthop 2007;132:208-15.
29. Little RM. The irregularity index: a quantitative score of man-dibular anterior alignment. Am J Orthod 1975;68:554-63.
30. Altman DG. Statistics and ethics in medical research: III Howlarge a sample? Br Med J 1980;281:1336-8.
31. Moher D, Schulz KF, Altman D. The CONSORT statement:revised recommendations for improving the quality of reports ofparallel-group randomized trials. JAMA 2001;285:1987-91.
32. Mandall N, Lowe C, Worthington H, Sandler J, Derwent S,Abdi-Oskouei M, et al. Which orthodontic archwire sequence? Arandomized clinical trial. Eur J Orthod 2006;28:561-6.
33. Bland JM, Altman DG. Statistical methods for assessing agree-ment between two methods of clinical measurement. Lancet1986;1:307-10.
34. Pandis N, Strigou S, Eliades T. Maxillary incisor torque withconventional and self-ligating brackets: a prospective clinicaltrial. Orthod Craniofac Res 2006;9:193-8.
35. Scott P, Sherriff M, Dibiase AT, Cobourne MT. Perception ofdiscomfort during initial orthodontic tooth alignment using aself-ligating or conventional bracket system: a randomized clin-
ical trial. Eur J Orthod 2008;30:227-32.