-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
1/7
2009;15:5609-5614. Published OnlineFirst September 8, 2009.Clin
Cancer ResYael P. Moss, Andrew Wood and John M. MarisInhibition of
ALK Signaling for Cancer Therapy
Updated Version10.1158/1078-0432.CCR-08-2762doi:
Access the most recent version of this article at:
Cited
Articleshttp://clincancerres.aacrjournals.org/content/15/18/5609.full.html#ref-list-1
This article cites 57 articles, 23 of which you can access for
free at:
Citing
Articleshttp://clincancerres.aacrjournals.org/content/15/18/5609.full.html#related-urls
This article has been cited by 4 HighWire-hosted articles.
Access the articles at:
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
SubscriptionsReprints and
[email protected] Department atTo order reprints of
this article or to subscribe to the journal, contact the AACR
[email protected] at
To request permission to re-use all or part of this article,
contact the AACR Publications
American Association for Cancer ResearchCopyright 2009on
February 27, 2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/lookup/doi/10.1158/1078-0432.CCR-08-2762http://clincancerres.aacrjournals.org/lookup/doi/10.1158/1078-0432.CCR-08-2762http://clincancerres.aacrjournals.org/lookup/doi/10.1158/1078-0432.CCR-08-2762http://clincancerres.aacrjournals.org/content/15/18/5609.full.html#ref-list-1http://clincancerres.aacrjournals.org/content/15/18/5609.full.html#ref-list-1http://clincancerres.aacrjournals.org/content/15/18/5609.full.html#related-urlshttp://clincancerres.aacrjournals.org/content/15/18/5609.full.html#related-urlshttp://clincancerres.aacrjournals.org/content/15/18/5609.full.html#related-urlshttp://clincancerres.aacrjournals.org/cgi/alertshttp://clincancerres.aacrjournals.org/cgi/alertsmailto:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/mailto:[email protected]:[email protected]://clincancerres.aacrjournals.org/cgi/alertshttp://clincancerres.aacrjournals.org/content/15/18/5609.full.html#related-urlshttp://clincancerres.aacrjournals.org/content/15/18/5609.full.html#ref-list-1http://clincancerres.aacrjournals.org/lookup/doi/10.1158/1078-0432.CCR-08-2762
-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
2/7
Molecular Pathways
Inhibition of ALK Signaling for Cancer Therapy
Yael P. Moss,1,2 Andrew Wood,1,2 and John M. Maris1,2,3
Abstract Paradigm shifting advances in cancer can occur after
discovering the key oncogenicdrivers of the malignant process,
understanding their detailed molecular mechanisms,
and exploiting this transdisciplinary knowledge therapeutically.
A variety of human
malignancies have anaplastic lymphoma kinase (ALK)
translocations, amplifications,
or oncogenic mutations, including anaplastic large cell
lymphoma, inflammatory myo-
fibroblastic tumors, nonsmall cell lung cancer, and
neuroblastoma. This finding has
focused intense interest in inhibiting ALK signaling as an
effective molecular therapy
against diseases with ALK-driven pathways. Recent progress in
the elucidation of the
major canonical signaling pathways postulated to be activated by
NPM-ALK signaling
has provided insight into which pathways may present a rational
therapeutic approach.
The identification of the downstream effector pathways
controlled by ALK should pave
the way for the rational design of ALK-inhibition therapies for
the treatment of a subset
of human cancers that harbor ALK aberrations. (Clin Cancer Res
2009;15(18):560914)
Background
Anaplastic lymphoma kinase (ALK) is an orphan receptor ty-rosine
kinase first identified as part of the t(2;5)
chromosomaltranslocation associated with most anaplastic large cell
lympho-mas (ALCL) and a subset of T-cell non-Hodgkins lymphomas(1).
It has recently become clear that many human cancers ac-tivate ALK
signaling by creating unique oncogenic fusions ofthe ALKgene at
chromosomal band 2p23 with a variety of part-ners through
chromosomal translocation events (2), resultingin the generation of
oncogenic ALK fusion genes and their en-coded proteins. These
oncogenic fusion proteins lead to consti-tutive activation of the
ALK kinase domain and have beenidentified in various solid tumors,
including inflammatorymyofibroblastic tumors (IMT; ref. 3),
squamous cell carcinomas(4), and non-small cell lung cancers
(NSCLC; ref. 5, 6). It hasalso recently been discovered that
germline mutations in ALKare the major cause of hereditary
neuroblastoma (7), and thatthese mutations can also be somatically
acquired (710).
The extracellular region of ALK shows significant homology tothe
leukocyte tyrosine kinase (11), which places ALK in the insu-lin
receptor superfamily of RTKs. The ALK gene encodes a 1,620-
amino acid protein that undergoes posttranslational
N-linkedglycosylation to a fully mature form weighing 220 kDa.
ALKex-pression is restricted to the developing central and
peripheralnervous system with a postulated role in participating in
the reg-ulation of neuronal differentiation (12). The absence of
pub-lished structural studies of ALK extracellular and
intracellulardomains, and the conflicting literature over whether
pleiotro-phin (13, 14) and/or midkine (15) are ALK ligands,
emphasizesthat much remains to be learned about ALK structure,
function,and signaling. Recently it has become clear thatALKisone
ofthe
few oncogenes activated in both hematopoietic and
nonhemato-poietic malignancies. Although constitutive ALK signaling
hasbeen shown in these contexts to induce cell transformation in
vi-tro and in vivo by controlling key cellular processes such as
cell-cycle progression, survival, cell migration, and cell shaping,
thecanonical signaling pathways and cell-type specificities of
signal-ing remain poorly defined. Regardless, it is now clear that
ALKrepresents a tractable target for innovative therapies on the
basisof selective inhibition of its tyrosine kinase activity. This
reviewfocuses on the normal and cancer-related biology of ALK and
thepreclinical proof-of-principle for ALK as a therapeutic
target.
Role of ALK in Cancer
A variety of mechanisms that lead to aberrant ALK signalingin a
variety of human cancers have been characterized, andthese include
translocations or structural rearrangements, ALKgene amplification,
mutations, and overexpression (Fig. 1). Im-portantly, missense
germ-line mutations in the tyrosine kinasedomain have been
described in patients with hereditary neuro-blastoma, with acquired
somatic mutations seen in the morecommon sporadic form of the
disease.
ALK Fusion Proteins-Translocations
Translocations are the most common known cause of ge-nomic ALK
aberration. Recent data suggest that deregulation
Authors' Affiliations:1Division of Oncology and Center for
ChildhoodCancer
Research, Children's Hospital of Philadelphia, 2Department of
Pediatrics,
University of Pennsylvania School of Medicine, and 3Abramson
Family
Cancer Research Institute, University of Pennsylvania School of
Medicine,
Philadelphia, Pennsylvania
Received 5/14/09; revised 5/22/09; accepted 5/28/09; published
OnlineFirst
9/8/09.
Grant support: National Institutes of Health (NIH) grants
K08-111733 (Y.P.
Moss), the Fulbright Foundation (A. Wood), R01-CA78454 (J.M.
Maris),
R01-CA124709 (J.M. Maris), and the Giulio D'Angio Endowed Chair
(J.M.
Maris).
Requests for reprints: John M. Maris, Children's Hospital,
Philadelphia, PA
19104-4318. Phone: 215-590-5242; Fax: 215-590-3770; E-mail:
[email protected].
F2009 American Association for Cancer Research.
doi:10.1158/1078-0432.CCR-08-2762
5609 Clin Cancer Res 2009;15(18) September 15,
2009www.aacrjournals.org
American Association for Cancer ResearchCopyright 2009on
February 27, 2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/
-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
3/7
of several genes (Fra 2 on 2p23, HLH protein Id2 on 2p25, andthe
CSF1 receptor on 5q33.1) located near the ALCL transloca-
tion breakpoint occurs before the formation of
translocationevents, and that aberrant transcriptional activity of
certain ge-nomic regions is linked to their propensity to undergo
chromo-somal translocations (16). In physiological ALK
signaling,ligand-induced homo-dimerization of the extracellular
do-mains is hypothesized to bring the tyrosine kinase domainsinto
sufficient proximity to enact trans-phosphorylation andkinase
activity. By contrast, translocations resulting in patho-genic
fusion partners provide dimerization domains that areligand
independent, leading to unregulated constitutive kinaseactivity and
malignant transformation.
Approximately 70 to 80% of ALK-positive ALCL express
thenucleophosmin-ALK (NPM-ALK) fusion protein derived from
the t(2;5)(p23;q35) translocation, and about the same fre-quency
of ALCLs stain positive for ALK by immunohistochem-
istry (17, 18). Within the truncated nucleophosmin protein
theessential domain required for transformation is a
coiled-coiloligomerization domain. Site-directed mutagenesis of the
di-merization domain abrogates NPM-ALK-transforming
activitysuggesting that proximity of the ALK kinase domains is a
pre-requisite to facilitate trans-phosphorylation of the
partnerkinase (19). The truncated NPM also encodes a nucleolar
local-ization domain that explains why in contrast to other ALK
fu-sions, NPM-ALK can be detected in the cytoplasm, nucleus,
andnucleolus (2), whereas most fusion products are largely
cyto-plasmic. The remaining 20% of translocations fuse ALKto
otherpartners that commonly encode coiled-coil oligomerization
do-mains such as Tyrosine Receptor Kinase-fused gene (TFG),
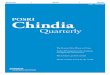
Fig. 1. A, representation of ALKaberrations in human cancers
and
major signaling pathways activatedthrough NPM-ALK. ALCL and
IMTshave unique and shared fusionpartners, but no overlap with
NSCLC.Mutations and amplification are uniqueto neuroblastoma but
rarely co-occur;translocations have not been detectedin
neuroblastoma specimens. Cancersdysregulate ALK via
multiplemechanisms. B, ligand-induceddimerization of the
extracellulardomain of ALK monomers leads totrans-phosphorylation
of the tyrosinekinase (TK) domain and physiologicalALK signaling.
C, ligand-independentsignaling is induced by activatingmutations
within the TK domain,or amplification of wild-type ALK
mediating overexpression,spontaneous dimerization,
andtransactivation of the TK domain.D, fusion partners
facilitateapproximation of truncated ALKcontaining the TK domain
throughcoiled-coil domains or subcellularlocalization. E,
constitutive ALKsignaling induces transformation viacanonical
signaling networks. SignalTransducers and Activation
ofTranscription protein 3 may couplecell growth to increased
oxidativephosphorylation, throughphosphorylation of tyrosine and
serineresidues, respectively. In ALCL, ALKsignaling cooperates with
othergenetic aberrations. AKT stabilizesthe GLI1 protein that is
upregulatedvia amplification of the SonicHedgehog locus.
5610Clin Cancer Res 2009;15(18) September 15, 2009
www.aacrjournals.org
Molecular Pathways
American Association for Cancer ResearchCopyright 2009on
February 27, 2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/
-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
4/7
Tropomyosin 3 (TPM3), and Tropomyosin 4 (TPM4). There arealso
several nonnuclear ALK fusion chimeras that induce transfor-mation
in vitro. The clathrin heavy chain-like gene (CLTCL), forexample,
encodes a clathrin family member that coalesces to pro-duce
cytoplasmic vesicles of CTLC-ALK bringing the ALK tyrosinekinase
domains into close proximity (20). Although almost all
ALK fusions retain the same portion of ALK because of
transloca-tion events that result in loss of the entire
extracellular portion
of normal ALK as well as the transmembrane segment, they
showslight differences in pathway activation, likely because of
differ-ences in their subcellular compartmentalization and/or
cell-type.NPM-ALK transgenic mouse models have shown T-cell
trans-formation as well as B-cell lymphomas (21) and may be
usefulin the evaluation of new therapeutic agents for these
diseases.
The deregulated expression of full length ALK and ALK fu-sions
has recently been observed in several nonlymphoid neo-plasms.
Interest in pharmacological inhibition of ALK has mostrecently been
spurred by the discovery of transforming echino-derm microtubule
associated protein like 4-anaplastic lympho-ma kinase (EML4-ALK)
fusions in a subset of NSCLCs (5), anda recent report of a novel
fusion transcript, kinesin family mem-
ber 5B-anaplastic lymphoma kinase (KIF5B-ALK), in this dis-ease
(22). Dimerization is enabled as the truncated EML4protein retains
a coiled-coil oligomerization domain in a man-ner similar to
NPM-ALK. Epidemiologic characterization ofEML4-ALK translocations
is ongoing but it seems to be a rareaberration, most common in
Asian nonsmokers or light-smokers
with the adenocarcinoma subtype of NSCLC, forming a
distinctsubgroup from patients harboring EGFR, KRAS, or NKX2-1
aber-rations (2326). The initial frequency of EML4-ALK fusion
tran-scripts was approximately 6.7% in Japanese NSCLC tumorsamples
(5), but subsequent studies showed lower frequenciesof 3% or less
(24, 25, 27). Direct demonstration of EML4-ALKas a dominant
oncogenic driver in NSCLC includes transforma-tion of mouse
3T3fibroblastic cells with forcedoverexpressionofhuman EML4-ALK and
de novo lung adenocarcinoma formationin mice engineered to express
EML4-ALK targeted to the lungalveolar epithelial compartment
(28).
IMT is a rare tumor of mesenchymal origin that arises in
mul-tiple tissues, possesses metastatic potential (29), and is
onlyminimally responsive to conventional chemotherapy or radia-tion
therapy. IMT is associated with various ALKtranslocationsthat
overlap with those found in ALCL, including TPM3 andTPM4 (30), CARS
(31), and CLTC (32), but not to date withfusion partners seen in
NSCLC. Immunohistochemical ALK re-activity occurs in 56% of cases
and is restricted to the cytoplasmconsistent with the observation
that NPM-ALK translocationsdo not occur in this disease. A subset
of esophageal cancers
show the TPM4-ALK fusion protein, but frequency and
signifi-cance of this has not been fully defined (33).
Mutations and Genomic Amplification
Expression of ALK has been reported in a large fraction
ofhuman-derived neuroblastoma cell lines (34), and our groupand
others had previously identified ALK as a candidate neuro-blastoma
oncogene through somatically acquired amplificationof the genomic
locus (35, 36). Recently, both germline (7) andsomatic (710)
mutations that activate ALK have been discov-ered in neuroblastoma,
an often lethal embryonal malignancythat contributes 15% to the
overall childhood cancer mortality
rate (37). Heritable gain-of-function mutations in ALKare
thecause of most hereditary neuroblastoma cases; one of the
fewpediatric tumors to be initiated by gain-of-function
mutations.
To date, heritable mutations have been restricted to the
kinasedomain of ALK, and it is presumed, but not yet proven,
thatthe second hit is somatic gain or amplification of the mutant
al-lele, similar to what is seen at the METlocus in hereditary
renalpapillary cancer (38). Although the number of families
studied
remains relatively small, it is apparent that theR1275Q
mutationis most common, and it seems that disease penetrance maybe
attributable to mutation type as rarer mutations, such asG1128A
seen in one large pedigree, was associated with verylow penetrance
compared with the near complete penetranceseen with the R1275Q
mutation. Both mutations fall withinthe kinase activation loop in a
region strongly associated withactivating mutations seen in other
oncogenic kinases (7). Thisfact compounds the already controversial
topic of the role forgenetic screening in this disease. Because
there are noninvasivemethods to screen for neuroblastoma (urinary
catecholaminemetabolites have relatively high sensitivity and
specificity fordetecting disease), we currently recommend genetic
testing
of the proband in any case in which there is a first or
seconddegree relative with neuroblastoma, or the proband has
multifo-cal disease consistent with hereditary predisposition.
Becauseneuroblastoma often occurs in families with other young
chil-dren or plans for future children, there is often parental
interestin testing even when there is no objective evidence for
hereditarypredisposition. As we define the frequency of occult
germlinemutations and further understand the role of ALK in the
initia-tion of neuroblastomas without a family history,
screeningrecommendations can be solidified.
ALKactivation by mutation and/or amplification is function-ally
relevant in models of high-risk neuroblastoma, and thusmight offer
a tractable therapeutic target. We and others haveshown thatALKis
expressedin themajorityof human neuroblas-toma-derived cell lines,
and thatALKexpression is significantlyhigher in neuroblastoma cells
harboring ALK mutations (39).
Analysis of protein lysates from these lines showed
constitutivephosphorylation in each of the cell lines harboring
mutations,
with weak phosphostaining in a smaller subset of wild-type
celllines, suggesting that ALK activation can occur by
mechanismsother than mutation within the kinase domain. Transient
siRNAknockdown directed against ALK in neuroblastoma cell
linesshowed significant inhibition of growth restricted to cells
withevidence for ALK activation. Baf3 cells expressing the two
mostcommon mutations showed cytotoxicity to NVP-TAE684, asmall
molecular competitive inhibitor of ATP binding inthe ALK kinase
domain (40). NVP-TAE684 has been shown
to block the growth of ALCL-derived and ALK-dependent celllines
with IC50 values between 2 and 10 nM; however, due toits toxicity
profile, it is now only used as a tool compound(40). More recently,
pharmacologic inhibition with a highly spe-cific small molecule
inhibitor of ALK currently in phase 1 clinicaltrials (PF-02341066,
see Clinical Translational Advances)showed potent antitumor
activity in preclinical models ofneuroblastoma both in vitro and in
vivo, in a mutation-specificmanner. Although these data are still
emerging, it is somewhatclear that ALK phosphorylation status is a
good biomarker forsensitivity to pharmacologic inhibition, but
there seem to bemutation-specific differences in sensitivity.
Solving the crystalstructure of the ALK kinase domain, and
cocrystallization with
5611 Clin Cancer Res 2009;15(18) September 15,
2009www.aacrjournals.org
ALK Inhibition Therapy
American Association for Cancer ResearchCopyright 2009on
February 27, 2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/
-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
5/7
pharmacologic inhibitors, will be necessary to understand ifsome
mutations confer resistance, and to understand how resis-tance
mutations may arise under selective pressure. In addition,defining
the downstream signaling pathways that mediate theef-fects of ALK
activity in the context of a neuroblastic cell will alsobe
critical, especially for the development of rational combina-tion
therapies. Work is ongoing to characterize the full spectrumof
germline and somatic DNA alterations leading to ALKactiva-
tion to develop strategies for future clinical trials on the
basis ofinhibiting ALK-mediated signaling in neuroblastoma.
Expression
ALK expression is of uncertain pathogenic significance inseveral
human cancers. The detection of ALK mRNA in diversehuman
tumor-derived cell lines (41), as well as the detection ofhigher
ALK expression in tumor compared with neighbor-ing normal tissue
(15), likely reflects physiological expressionrather than seminal
pathogenic events (41). ALK has previouslybeen shown to be
upregulated and functionally relevant in glio-blastoma, and recent
work has shown that ribozyme-mediated
knockdown of ALK results in abolishment of tumor growth in
axenograft model (42). This offers potentially novel
therapeuticoptions for an otherwise lethal brain tumor.
Immunohistochem-ical detection of ALK protein overexpression is
pathognomonicfor ALCL, and recent work suggests that ALK
immunohistochem-istry may have utility as a screening tool or
surrogate markerfor EML4-ALK fusion gene-positive NSCLC tumors
(43). Cur-rently work is focused on developing reliable techniques
forphospho-ALK staining in routine clinical specimens, and thismay
be critically important to properly evaluate future ALKinhibitor
clinical trials.
Differential Activation of Downstream Signaling
PathwaysThe critical pathways involved in transformation because
of
dysregulated ALK signaling are best characterized by
transloca-tions that juxtapose ALK to dimerization partners (Fig.
1; ref. 2).
The constitutive activation of ALK fusion proteins leads to
cel-lular transformation through a complex signaling network.
Among the potential combinations of proteins phosphorylatedby
ALK kinase activity, it has been postulated that the most
im-portant effects involve activation of STAT3 (44, 45),
AKT/PI3K(46), and RAS/ERK (47) pathways, which control cell
prolifer-ation, survival, and cell cycling. These pathways are
typicallyupregulated in transformed cell lines (48), and
pharmacologi-cal inhibition of ALK leading to apoptosis abrogates
phosphor-
ylation of these key signal-transducing proteins in ALCL
models(49, 50). Inhibition of downstream signal transduction
pro-teins, such as STAT3, has been shown to prevent NPM-ALK
in-duced transformation in vivo (45). Recent work has shown thatthe
sonic hedgehog signaling pathway (SHH/GLI1) is also acti-
vated in ALK-positive ALCLs (51). SHH/GLI1 activation is
theresult of SHH gene amplification and is further mediated
byNPM-ALK through activation of PI3K/AKT and stabilizationof GLI1
protein (51). Inhibition of this pathway induces apo-ptosis and
cell cycle arrest, suggesting that inhibition of SHH/GLI1 signaling
in combination with blocking NPM-ALK and/orthe PI3K/AKT pathway may
present a rational therapeutic ap-proach in ALK+ ALCL.
Different ALK aberrations produce diverse pathogenic signal-ing
anomalies through a combination of differentially activatingcommon
signal transduction pathways and unique pathogenicmechanisms.
Different ALK fusion proteins transfected intoNIH3T3 cells produced
clones with differential signaling andphenotypic differences beyond
those that could be explainedby the variable kinase activity of
each fusion. TPM3-ALK cellsshowed the most AKT phosphorylation and
migratory capacity
in vitro, but in vivo tumorigenicity was less than that
observedin NPM-ALK cells. In contrast, ATIC phosphorylation
enhancesenzymatic activity of NPM-ALK (52), and ATIC-ALK cells
causeSTAT3 phosphorylation with only modest invasion and in
vivotumorigenicity (48). TPM3-ALK invasive capacity may partly
bemediated by a unique pathogenic mechanism. TPM interacts
with endogenous tropomyosin in the cytoskeleton, which is
hy-pothesized to alter cytoskeletal organization and led to
greatermotility and metastatic potential (29). It has been
postulatedthat the STAT family is unlikely to play a key role of
the patho-genesis of EML4-ALK (53), even though STAT3
anti-senseoligonucleotides suppress the in vivo transforming
activity ofNPM-ALK (45). Tissue context and signaling differences
may
explain why some ALCL and IMT share some fusion partners,but
display no overlap with NSCLC. Additional signaling andphenotypic
variation will likely be discovered when the fullspectrum of
mutated ALK and pathogenically overexpressed
wild-type (via genomic amplification) prot eins are
studied.These signaling variations could arise because of multiple
me-chanisms including: variable subcellular localizations of
activated
ALK, altered sequences of tyrosine auto-phosphorylation,
alteredkinase substrate specificity, tissue context, autocrine or
paracrineligand effects, and by breakpoints disrupting the original
loci in
which truncated genes are translocated from.
Clinical Translational Advances
Small molecule tyrosine kinase inhibitors. Kinases are
criticalcomponents of cellular signal transduction cascades, and
arekey effectors of cell proliferation and differentiation.
Therenow exists clear precedent in clinical oncology that robust
anti-tumor activity can be obtained with inhibitors directed
towardoncogenic tyrosine kinases that are genetically dysregulated
(54,55), and these lessons are readily applicable to ALK kinase
in-hibition. Imatinib showed that off-target kinase inhibitioncould
be rationally exploited because of its efficacy in Kit+
gastro-intestinal stromal tumors (56). This is significant, as the
first ALKinhibitor to enter phase 1 clinical trials, PF-02341066,
was ini-tially designed to inhibit c-Met, but was also found to
have sig-nificant activity against ALK (50). This orally
bioavailable small
molecule inhibitor caused complete regression of
NPM-ALKxenografts at pharmacologically relevant doses, with a
strongcorrelation between antitumor response and abrogation of
phos-phorylation of ALK (50). PF-02341066 is currently the
onlyavailable ALK small-molecule inhibitor in clinical trials;
how-ever, recognition of the variety of malignancies in which
ALKplays a causative role has prompted broad developmental
effortsin this area. Point mutations in the kinase domain of other
tyro-sine kinases such as BCR-ABL, KIT, and EGFR impair drug
bind-ing as the major mechanism of acquired resistance to
kinaseinhibitors. To begin to address this, investigators have
generatedseveral ALK mutants in the kinase domain and evaluated
theirkinaseactivity andsensitivity to inhibition by two
ALKinhibitors
5612Clin Cancer Res 2009;15(18) September 15, 2009
www.aacrjournals.org
Molecular Pathways
American Association for Cancer ResearchCopyright 2009on
February 27, 2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/
-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
6/7
developed from different chemical series (57). Binding of
theseinhibitors to wild-type and mutant ALK was analyzed
usinghomology models, and showed that some of the mutants are
re-sistant to select small molecule inhibitors. It remains to be
seen
whether newer inhibitors designed with greater specificity
againstALK will eventually prove superior to multikinase
inhibitor.
Future Developments
ALK is one of the few examples of a receptor tyrosine
kinaseimplicated in the oncogenesis of both hematopoietic and
non-hematopoietic malignancies. Although the importance
ofautocrine-paracrine growth loops involving normal ALK in
tu-morigenesis is not yet fully elucidated, there are compelling
da-ta to support the hypothesis that tumors with ALK
aberrationsexhibit oncogene addiction, with inhibition of aberrant
ALKsignaling resulting in marked antitumor efficacy in
preclinicalmodels. Additional studies are required to determine
whether tu-mors that express full-length ALK that is activated by
its ligandexhibit the same or at least partial dependence upon
ALKgrowth signals.
There is strong rationale and significant enthusiasm towardALK
inhibition as a targeted therapy against tumors harboringoncogenic
fusions or activating mutations, and the results ofthe first
clinical trial testing the PF-02341066 dual c-Met/ALKinhibitor has
shown clinical activity in highly refractory patients
with tumors harboring ALK translocations, leading to
ongoingefforts to select patients for these trials based on ALK
transloca-tion status. Defining the epidemiology of ALK aberrations
ineach cancer that harbors ALK pathway activation seems
essential
to properly design and interpret clinical trials of ALK
inhibitors.Furthermore, as potency will likely be variable on the
basis of themechanism for pathway activation, and the emergence of
resis-tance mechanisms almost assured, co-development of small
mo-lecular and monoclonal antibody inhibitors of ALK
activationseems prudent. A pediatric trial of PF-02341066 will
begin en-rollment of subjects in 2009, and plans are currently
being madefor how to properly integrate ALK inhibition therapy into
front-
line chemotherapeutic regimens. If the preclinical models do
in-deed predict what will be observed in the clinic, it is clear
that forcancers that can usurp ALK signaling as a mechanism of
oncoge-nicity, ALK pathway status must be assayed for at the time
ofdiagnosis or relapse.
Cautious extrapolation from preclinical models and
inhibitor-kinase co-crystallization studies will help us to define
biomarkerspredictive of therapeutic response. Besides the use of
selective
ALK inhibitors, it may be crucial to develop strategies to
inhibitmultiple targets involved in the ALK-signaling pathway.
siRNAscreens of the druggable genome in combination with ALK
inhi-bitors, and preclinical testing for synergy and antagonism
withexisting chemotherapy backbones will be important to maxi-
mize efficacy. Lastly, the development of monoclonal
antibodiesagainst ALK should be pursued, a precedent set by the
develop-ment of monoclonal antibodies against members of the
EGFRfamily, and an approach that may prove to be particularly
usefulfor tumors with ALK gene amplification.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
References1. Morris SW, Kirstein MN, Valentine MB, et al.
Fu-
sion of a kinase gene, ALK, to a nucleolar proteingene, NPM, in
non-Hodgkin's lymphoma. Sci-
ence 1994;263:1281
4.2. Chiarle R, Voena C, Ambrogio C, Piva R, Inghirami
G. The anaplastic lymphoma kinase in thepathogenesis of cancer.
Nat Rev Cancer 2008;8:1123.
3. Griffin CA, Hawkins AL, Dvorak C, Henkle C,Ellingham T,
Perlman EJ. Recurrent involvementof 2p23 in inflammatory
myofibroblastic tumors.Cancer Res 1999;59:277680.
4. Jazii FR, Najafi Z, Malekzadeh R, et al. Identifi-cation of
squamous cell carcinoma associatedproteins by proteomics and loss
of beta tropo-myosin expression in esophageal cancer. WorldJ
Gastroenterol 2006;12:710412.
5. Soda M, Choi YL, Enomoto M, et al. Identifica-tion of the
transforming EML4-ALK fusion genein non-small-cell lung cancer.
Nature 2007;448:5616.
6. Rikova K, Guo A, Zeng Q, et al. Global survey
ofphosphotyrosine signaling identifies oncogenickinases in lung
cancer. Cell 2007;131:1190203.
7. Mosse YP, Laudenslager M, Longo L, et al. Iden-tificationof
ALKas a major familial neuroblastomapredisposition gene. Nature
2008;455:9305.
8. Janoueix-Lerosey I, Lequin D, Brugieres L, et al.Somatic and
germline activating mutationsof the ALK kinase receptor in
neuroblastoma.Nature 2008;455:96770.
9. George RE, Sanda T, Hanna M, et al. Activatingmutations in
ALK provide a therapeutic target inneuroblastoma. Nature
2008;455:9758.
10. Chen Y, Takita J, Choi YL, et al. Oncogenic mu-tations of
ALK kinase in neuroblastoma. Nature2008;455:9714.
11. Morris SW, Naeve C, Mathew P, et al. ALK, the
chromosome 2 gene locus altered by the t(2;5) innon-Hodgkin's
lymphoma, encodes a novel neu-ral receptor tyrosine kinase that is
highly related
to leukocyte tyrosine kinase (LTK). Oncogene1997;14:217588.
12. Iwahara T, Fujimoto J, Wen D, et al.
Molecularcharacterization of ALK, a receptor tyrosine ki-nase
expressed specifically in the nervous sys-tem. Oncogene
1997;14:43949.
13. Stoica GE, Kuo A, Aigner A, et al. Identificationof
anaplastic lymphoma kinase as a receptor forthe growth factor
pleiotrophin. J Biol Chem 2001;276:167729.
14. Mathivet T, Mazot P, Vigny M. In contrast toagonist
monoclonal antibodies, both C-terminaltruncated form and full
length form of Pleiotro-phin failed to activate vertebrate ALK
(anaplasticlymphoma kinase)? Cell Signal 2007;19:243443.
15. Stoica GE, Kuo A, Powers C, et al. Midkinebinds to
anaplastic lymphoma kinase (ALK) andacts as a growth factor for
different cell types.
J Biol Chem 2002;277:35990
8.16. Mathas S, Kreher S, Meaburn KJ, et al. Gene
deregulation and spatial genome reorganizationnear breakpoints
prior to formation of translo-cations in anaplastic large cell
lymphoma. ProcNatl Acad Sci U S A 2009;106:58316.
17. Stein H, Foss HD, Durkop Hu, et al. CD30(+) an-aplastic
large cell lymphoma: a review of its his-topathologic, genetic, and
clinical features.Blood 2000;96:368195.
18. Medeiros LJ, Elenitoba-Johnson KS. Anaplas-tic large cell
lymphoma. Am J Clin Pathol 2007;127:70722.
19. Ladanyi M, Cavalchire G. Detection of theNPM-ALK genomic
rearrangement of Ki-1 lym-phoma and isolation of the involved NPM
andALK introns. Diagn Mol Pathol 1996;5:1548.
20. Touriol C, Greenland C, Lamant L, et al.
Furtherdemonstration of the diversity of chromosomalchanges
involving 2p23 in ALK-positive lymphoma:
2 cases expressing ALK kinase fused to CLTCL(clathrin chain
polypeptide-like). Blood 2000;95:32047.
21. Chiarle R, Gong JZ, Guasparri I, et al. NPM-ALK transgenic
mice spontaneously developT-cell lymphomas and plasma cell tumors.
Blood2003;101:191927.
22. Takeuchi K, Choi YL, Togashi Y, et al. KIF5B-ALK, a Novel
Fusion Oncokinase Identified byan Immunohistochemistry-based
Diagnostic Sys-tem for ALK-positive Lung Cancer. Clin CancerRes
2009;15:31439.
23. Wong DW, Leung EL, So KK, et al. The EML4-ALK fusion gene is
involved in various histologictypes of lung cancers from nonsmokers
withwild-type EGFR and KRAS. Cancer 2009;115:172333.
24. Perner S, Wagner PL, Demichelis F, et al.
EML4-ALK fusion lung cancer: a rare acquiredevent. Neoplasia
2008;10:298302.
25. Koivunen JP, Mermel C, Zejnullahu K, et al.EML4-ALK fusion
gene and efficacy of an ALK ki-nase inhibitor in lung cancer. Clin
Cancer Res2008;14:427583.
26. Inamura K, Takeuchi K, Togashi Y, et al. EML4-ALK lung
cancers are characterized by rare othermutations, a TTF-1 cell
lineage, an acinar his-tology, and young onset. Mod Pathol
2009;22:50815.
27. Shinmura K, Kageyama S, Tao H, et al. EML4-ALK fusion
transcripts, but no NPM-, TPM3-,CLTC-, ATIC-, or TFG-ALK fusion
transcripts, innon-small cell lung carcinomas. Lung
Cancer2008;61:1639.
28. Soda M, Takada S, Takeuchi K, et al. A mouse
5613 Clin Cancer Res 2009;15(18) September 15,
2009www.aacrjournals.org
ALK Inhibition Therapy
American Association for Cancer ResearchCopyright 2009on
February 27, 2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/
-
7/29/2019 ALK_Clin Cancer Res-2009-Moss-5609-14
7/7
model for EML4-ALK-positive lung cancer. ProcNatl Acad Sci U S A
2008;105:198937.
29. Armstrong F, Lamant L, Hieblot C, Delsol G,Touri ol C. TPM3-
ALK expressi on i nduceschanges in cytoskeleton organisation and
con-fers higher metastatic capacities than otherALK fusion
proteins. Eur J Cancer 2007;43:6406.
30. Lawrence B, Perez-Atayde A, Hibbard MK,et al. TPM3-ALK and
TPM4-ALK oncogenes ininflammatory myofibroblastic tumors. Am
JPathol 2000;157:37784.
31. Cools J, Wlodarska I, Somers R, et al. Identifi-cation of
novel fusion partners of ALK, the ana-plastic lymphoma kinase, in
anaplastic large-celllymphoma and inflammatory
myofibroblastictumor. Genes Chromosomes Cancer 2002;34:35462.
32. Bridge JA, Kanamori M, Ma Z, et al. Fusion ofthe ALK gene to
the clathrin heavy chain gene,CLTC, in inflammatory myofibroblastic
tumor.Am J Pathol 2001;159:4115.
33. Du XL, Hu H, Lin DC, et al. Proteomic profilingof proteins
dysregulted in Chinese esophagealsquamous cell carcinoma. J Mol Med
2007;85:86375.
34. Lamant L, Pulford K, Bischof D, et al. Expres-sion of the
ALK tyrosine kinase gene in neuro-blastoma. Am J Pathol
2000;156:171121.
35 . Osajima-Hakomori Y, Miyake I, Ohira M,
Nakagawara A, Nakagawa A, Sakai R. Biologicalrole of anaplastic
lymphoma kinase in neuro-blastoma. Am J Pathol 2005;167:21322.
36. George R, Attiyeh E, Li S, et al. Genome-wideanalysis of
neuroblastomas using high-densitysingle nucleotide polymorphism
arrays. PLoSOne 2007;2:e255.
37. Maris JM, Hogarty MD, Bagatell R, Cohn SL.Neuroblastoma.
Lancet 2007;369:210620.
38. Jeffers M, Schmidt L, Nakaigawa N, et al. Ac-tivating
mutations for the met tyrosine kinasereceptor in human cancer. Proc
Natl Acad SciU S A 1997;94:1144550.
39. Wang Q, Diskin S, Rappaport E, et al. Inte-
grative genomics identifies distinct molecularclasses of
neuroblastoma and shows thatmultiple genes are targeted by regional
altera-tions in DNA copy number. Cancer Res 2006;66:605062.
40. Galkin AV, Melnick JS, Kim S, et al. Identifica-tion of
NVP-TAE684, a potent, selective, and effi-cacious inhibitor of
NPM-ALK. Proc Natl AcadSci U S A 2007;104:2705.
41 . Di rks W G, Fahnri ch S, Li s Y, Becker E,MacLeod RA,
Drexler HG. Expression and func-
tional analysis of the anaplastic lymphoma ki-nase (ALK) gene in
tumor cell lines. Int J Cancer2002;100:4956.
42. GrzelinskiM, Steinberg F, Martens T, CzubaykoF, Lamszus K,
Aigner A. Enhanced antitumori-genic effects in glioblastoma on
double targetingof pleiotrophin and its receptor ALK.
Neoplasia2009;11:14556.
43. Boland JM, Erdogan S, Vasmatzis G, et al.Anaplastic lymphoma
kinase immunoreactivitycorrelates with ALK gene rearrangement
andtranscriptional up-regulation in non-small celllung carcinomas.
Hum Pathol 2009;40:11528.
44. Kasprzycka M, Marzec M, Liu X, Zhang Q,Wasik MA.
Nucleophosmin/anaplastic lym-phoma kinase (NPM/ALK) oncoprotein
inducesthe T regulatory cell phenotype by activatingSTAT3. Proc
Natl Acad Sci U S A 2006;103:
9964
9.45. Chiarle R, Simmons WJ, Cai H, et al. Stat3 is
required for ALK-mediated lymphomagenesisand provides a possible
therapeutic target. NatMed 2005;11:6239.
46. Bai RY, Ouyang T, Miething C, Morris SW,Peschel C, Duyster
J. Nucleophosmin-anaplasticlymphoma kinase associated with
anaplasticlarge-cell lymphoma activates the phosphatidyli-nositol
3-kinase/Akt antiapoptotic signaling path-way. Blood
2000;96:431927.
47. Zou HY, Li Q, Lee JH, et al. An orally
availablesmall-molecule inhibitor of c-Met,
PF-2341066,exhibitscytoreductiveantitumor efficacy through
antiproliferative and antiangiogenic mechan-isms. Cancer Res
2007;67:440817.
48. Armstrong F, Duplantier MM, Trempat P, et al.Differential
effects of X-ALK fusion proteins onproliferation, transformation,
and invasionproperties of NIH3T3 cells. Oncogene
2004;23:607182.
49. McDermott U, Iafrate AJ, Gray NS, et al.Genomic alterations
of anaplastic lymphomakinase may sensitize tumors to anaplastic
lym-phoma kinase inhibitors. Cancer Res 2008;68:
3389
95.50. Christensen JG, Zou HY, Arango ME, et al.
Cytoreductive antitumor activity of PF-2341066,a novel inhibitor
of anaplastic lymphoma kinaseand c-Met, in experimental models of
anaplasticlarge-cell lymphoma. Mol Cancer Ther 2007;6:331422.
51. Singh RR, Cho-Vega JH, Davuluri Y, et al.Sonic hedgehog
signaling pathway is activatedin ALK-positive anaplastic large cell
lymphoma.Cancer Res 2009;69:25508.
52. Boccalatte FE, Voena C, Riganti C, et al. Theenzymatic
activity of 5-aminoimidazole-4-carboxamide ribonucleotide
formyltransferase/IMP cyclohydrolase is enhanced by NPM-ALK:new
insights in ALK-mediated pathogenesis andthe treatment of ALCL.
Blood 2009;113:277690.
53. Mano H. Non-solid oncogenes in solid tumors:
EML4-ALK fusion genes in lung cancer. CancerSci
2008;99:234955.
54. Schlessinger J. Cell signaling by receptor tyro-sine
kinases. Cell 2000;103:21125.
55. Blume-Jensen P, Hunter T. Oncogenic kinasesignalling. Nature
2001;411:35565.
56. Heinrich MC, Corless CL, Demetri GD, et al. Ki-nase
mutations and imatinibresponse in patientswith metastatic
gastrointestinal stromal tumor.J Clin Oncol 2003;21:43429.
57. Lu L, Ghose AK, Quail MR, et al. ALK mutantsin the kinase
domain exhibit altered kinase activ-ity and differential
sensitivity to small moleculeALK inhibitors. Biochemistry
2009;48:36009.
5614Clin Cancer Res 2009;15(18) September 15, 2009
www.aacrjournals.org
Molecular Pathways
Am i A i ti f C R hC i ht 2009on February 27,
2013clincancerres.aacrjournals.orgDownloaded from
Published OnlineFirst September 8, 2009;
DOI:10.1158/1078-0432.CCR-08-2762
http://clincancerres.aacrjournals.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/http://www.aacr.org/http://www.aacr.org/http://clincancerres.aacrjournals.org/