Embed Size (px)
Citation preview

This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project – Clinical Interventions &
Staffing Guidelines.
Project Review and Closure Report – Phase 1
Version 1.b(6/02/06)
Project Manager and Author: Jenny Richardson

This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page ii
DOCUMENT ACCEPTANCE and RELEASE NOTICE
This is version 1.a of the Project Review and Closure Report for the GMCT / NSW Health Metropolitan Hospital Allied Health Project – Clinical Interventions and Staffing Guidelines.
The Project Review and Closure Report is a managed document. For identification of amendments each page contains a release number and a page number. Changes will only be issued as a complete replacement document. Recipients should remove superseded versions from circulation. This document is authorised for release once all signatures have been obtained.
PREPARED: DATE:___/___/___ (for acceptance) (Jenny Richardson, Project Manager) ACCEPTED: DATE:___/___/___ (for release) (Project Sponsor, Kerry Goulston – GMCT Chairman) 1. BUILD STATUS: The most recent amendment first.
Version Date Author Reason Sections
1.a January 2006 Jenny Richardson Initial Release All
2. DISTRIBUTION:
Copy No Version Issue Date Issued To
1 1.a February 06 Allied Health Project Steering Committee Members
1.b March 06 GMCT Executive
Final TBA Allied Health Clinicians and Representatives

Executive Summary
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is Appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
1. Executive Summary
1.1. Background
The challenges of providing equitable, accessible, sustainable, timely and safe health care are becoming more apparent given existing and pending workforce shortages, maldistribution of workforce1 and resources, higher complexity of clinical cases and higher expectations of service delivery. Workforce shortages across health care professions have been widely acknowledged and have become a high priority for State and Federal Health Ministers. 2 Workforce solutions are multi faceted. Recruitment and retention, education and training and maintenance of acquired skills all play an important role in addressing workforce shortages. The NSW Government’s Plan for Securing Our Health Workforce highlights positive initiatives specific to the medical and nursing fields and outlines longer term initiatives to address current supply and distribution issues including: - changes to traditional work practices that impede improved delivery of services; - exploring new models of care; - developing different skill mixes within and across professions; and - enhancing collaboration between health, education and training sectors.3
It is a widely held view that issues and/or solutions for allied health are sufficiently different to nursing or medicine to warrant appropriate inclusion in strategic and operational decision making.4 Clinicians from the GMCT Metropolitan Hospitals Program undertook a review of minimum Medical and Allied Health staffing and skill levels required in a number of clinical areas. Nursing was not addressed by this group given the project currently under way by NSW Health relating to nursing workload. Allied health participants from the Metropolitan Hospitals Program emphasised that in order to explore new models of care and define skill mixes within the Allied Health professions careful review of current work practices by skilled Allied Health Professionals needed to occur. Identifying how many clinicians are required for a particular clinical population and definition of the clinical interventions attached to these positions needs to be considered. The need for additional resources in order to begin to address these issues was recognised and a proposal put forward for project management support. A project manager was appointed and an Allied Health Steering Committee established with work commencing September 12, 2005. (Steering Committee Terms of Reference attached).
1 National Health Workforce Strategic Framework (April 2004) 2 ibid. 3 The NSW Government’s Plan for Securing Our Health Workforce 4 Allied Health Presentation Metropolitan Hospitals Forum GMCT March 2005

Executive Summary
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 2
1.2. Aim
The aim of this project was to develop staffing guidelines for Allied Health working in metropolitan hospitals. It is felt that the development of such guidelines will: - Assist in planning a service based on the requirements of the patient. - Promote consistency in staffing mix across metropolitan hospitals - Provide a baseline for allocation of staff rather than relying on an individual’s subjective
interpretation of a particular role. - Enhance retention assuming that appropriately staffed services will be more attractive from a
recruitment perspective - Assist professional groups in the development of competency standards for Allied Health
professions by defining core clinical interventions. - Further assist clinical service planning and design by clearly delineating core interventions for
technical and support staff. It is further hoped that such information will: - Assist others to better understand the contribution that allied health makes to quality health care. - Assist administrators to make informed decisions regarding staffing mix in metropolitan
hospitals. - Assist Allied Health management to present staffing requirements with clarity and credibility - Enable Allied Health Professions to further develop & implement appropriate staffing models. Project methodology has been based on the premise that clinical expertise plays a vital role in the determination of staffing requirements. Scope For this particular project the following clinical areas were targeted: - General Medicine - Orthopaedics - Outpatients (Hospital based) - Paediatrics (Inpatient) - Emergency - ICU / HDU - Aged Care Allied Health Disciplines encompassed those professions currently identified by NSW Health including: - Audiology - Dietetics - Occupational Therapy - Orthoptics - Pharmacy – hospital based. It is acknowledged that Hospital based Pharmacy have begun work in this area with the Society of Hospital Pharmacists of Australia (SHPA) Clinical Pharmacy Practice Standards 2004 due to be published shortly. - Physiotherapy - Podiatry

Executive Summary
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 3
- Psychology - Radiation Therapy - Radiography –A project is being prepared for GMCT Medical Imaging investigating recruitment
and retention in Radiography. Given that this report does not touch on guidelines for appropriate staffing levels it is felt this proposal will complement this work
- Speech Pathology - Social Work Given very limited time constraints this project was only able to focus on metropolitan hospitals. The following metropolitan hospitals were identified in order to include as many Area Health Services and Allied Health disciplines as practically possible in the four-month period. Teaching hospitals and those with a large rural component will be consulted for feedback as the project progresses. It is anticipated that outcomes may be applied to these settings in the future.
AREA HEALTH SERVICE METROPOLITAN HOSPITALS NORTHERN SYDNEY / CENTRAL WYONG COAST HORNSBY RYDE MONA VALE MANLY SOUTH EASTERN SYDNEY / SYDNEY HOSPITAL ILLAWARRA SUTHERLAND BULLI SHELLHARBOUR SHOALHAVEN SYDNEY WEST MT DRUIT AUBURN BLUE MOUNTAINS HAWKESBURY SYDNEY SOUTH WEST BLACKTOWN FAIRFIELD BANKSTOWN CAMDEN CAMBELLTOWN HUNTER / NEW ENGLAND NEWCASTLE MATER BELMONT DISTRICT MAITLAND
Process A series of area wide workshops were held at selected facilities to ensure broader representation from as many Allied Health disciplines as possible. Experienced Clinicians were asked to consider what it is that they uniquely provide in each clinical area and on average, how long it takes to provide such a service. Department Managers were also encouraged to attend. Data collated was used to develop a staffing template or ‘ Matrix’ for each discipline. Where time permitted drafts were sent out to all participants and the project steering committee for comment and adjustment prior to data analysis.

Executive Summary
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 4
1.3. Phase 1 closure
Funding for 16 weeks of a project officer has been exhausted.
It is acknowledged that the development of staffing guidelines for Allied Health is in its infancy. It is hoped that the information generated from this project will be utilised as a baseline for future projects.
Significantly more work needs to be done in order to further develop and validate the data collated during Phase 1 for each Allied Health Profession.
1.4. Highlights and Innovations
• Despite enormous differences between services, sites and infrastructures in Metropolitan hospitals the clinical interventions provided by Allied Health disciplines remain quite consistent.
• Separate to Clinical Expertise and Client complexity, the time taken to provide specific
interventions is affected by such things as staffing ratios and resources, system processes, access to other allied health disciplines, access to community services, access to and interrelationships with other essential services eg. Nutrition and food services, Speech Pathology and Radiography, access to technology.
• Whilst researchers may question the validity of the data collated, experienced staff do appear to
have some notion of how long it takes to complete a task under normal and extraneous circumstances. In the examples produced the majority of therapy hours calculated were very close if not equal to those produced using retrospective statistical data.
• There is a common misconception that many Allied Health professions duplicate each other’s roles or interventions. There was no evidence of duplication of interventions or roles between the disciplines represented here.

Executive Summary
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 5
1.5. Summary of Recommendations
This is considered to be Phase 1 of the project. It should be noted the draft templates included in this report may assist future development of staffing guidelines once verified. In their current form the templates are not a complete tool and require further work for verification. The templates should not be used as guidelines to determine indicative staffing numbers. Phase 1 involved template development only. Additional funding needs to be sought for Phase 2 of the project. Recommendations to progress further development of Clinical Intervention and Staff Guideline Tool include: • Co-ordination of an Allied Health Forum related to workforce issues.
This would be utilised as a communication strategy for presenting the outcomes of the project thus far to Allied Health representatives and clinicians, particularly those who participated in the project. Such an event would also provide a forum for allied health clinicians to openly discuss current workforce issues and to hear from other disciplines about the work that is currently being conducted.
• Further liaison with participant groups in order to refine draft matrix templates. • Presentation of Matrix templates to appropriate professional bodies for review and professional
validation ie. NSW Health / Directors and Chairs / Advisor groups, professional associations, The Allied Health Alliance.
• Possible Application of the matrix methodology to Allied Health Professions who were not
represented at Area workshops. Future • Significantly more work needs to be done to evaluate and define the role of technical assistant for
each allied health profession. • Application of the matrix methodology to tertiary hospitals and rural settings.
It should be noted that allied health professionals form a significant proportion of the health workforce in rural and remote Australia5 Given the recent restructure of health administration in NSW five out of the eight new Area Health Services include a rural component. In establishing ideal staffing templates consideration will need to be given to service composition of clinical areas in rural settings and the mechanisms for access to specialist allied health services.
• Area Health Services to be invited to trial the staffing guidelines in a particular service area and
provide suggestions for future trials across the areas with opportunities for each Area Health Service to customise according to need.
• Development of computer software for the matrix template to be used as a tool for determining
Allied Health staffing levels and professional mix.
5 A Study of Allied Health Professionals in Rural and Remote Australia S.A.R.R.A.H 2000

Project Performance
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 6
2. Project Performance
The project was completed with only minor alterations to the project plan. Workshops/ focus groups were conducted at the following hospital sites: AREA HEALTH SERVICE
Hospital Site Clinical Representation
Wollongong Bulli Shellharbour
Shoalhaven Shoalhaven
SESIAHS
Sutherland Sutherland Wyong Wyong NSCCAHS Manly Manly
Mona Vale Hornsby Ryde
WESTERN SYDNEY Blacktown Blacktown Mt Druit Auburn Blue Mountains Hawkesbury
SOUTH WESTERN SYDNEY
Campbelltown Camden Campbelltown
Bankstown Bankstown Fairfield
HUNTER Wallsend Maitland Belmont Newcastle Mater
16 workshop sessions were conducted with a total of 143 clinicians providing input Workshop numbers have varied considerably from 8 to 20 with discipline specific numbers varying from 1 to 7. Clinicians have approached the task with varying degrees of ease and understanding. Clinicians often grappled with the concept of average intervention time, quick to relate the best and worst case scenarios. Several groups quoted ranges of times eg. from 1 to 12 hours. Similarly, when asked to list the clinical interventions provided to a particular client group some clinicians had difficulty relating actual versus ideal interventions, several indicating that current services were under resourced. There were varying levels of engagement in the project. Many clinicians and managers were uncertain re the future use of such information. Annual leave over the Christmas / New Year period also limited communication during the final weeks of the project. Other factors affecting the completion of project tasks included concerns with the demands of: - The recent NSW Health Restructure - EquIP 2005 - Numerical Profile 2005

Project Performance
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 7
Area Health Service amalgamation created difficulties re changes in allied health structures, roles and responsibilities as well as unforseen problems with e-mail and telephone communications. A significant amount of data was generated from each workshop. Data quality varied between clinical groups and appeared to be impacted positively and negatively by larger group numbers ie. Group dynamics Not all Allied Health disciplines were represented. No information was collated for Audiology, Radiography, Radiation Therapy or Orthoptics as these groups were not represented at the workshops conducted. Allied Health structures and definitions varied between area health services. Insufficient data was obtained to produce a matrix example for Pharmacy. The practise of utilising assistant staff to perform interventions which do not require direct contact with a qualified health professional is not as developed in Australia compared to the UK and the United States. Many clinicians involved in this project reported little involvement or experience in working with assistant staff. This was reflected in the limited data collated re Technical Assistant interventions and the conditions under which their use would be appropriate. Some clinicians were very clear about interventions that would not be suitable for an assistant to perform. Others referred only to clerical assistant roles rather than incorporating clinical assistants. Significantly more work needs to be done to evaluate and define the role of technical assistant for each Allied Health profession.
2.1. Performance Against Outputs
The Allied Health Staffing Matrix was developed as a template for determining staffing numbers and professional mix. Guidelines have been developed around the use and application of the matrix and examples provided for each Allied Health Discipline in particular clinical units (see APPENDIX A) Tables demonstrating intervention and intervention time comparisons between different services have been included in APPENDIX B.
2.2. Performance Against Schedule
16 weeks was not sufficient time to produce validated data for each profession in each targeted clinical area. This would need to be addressed during the next phase of the project.

Lessons Learnt
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 8
2.3. Performance Against Budget
Funding was sought for a HSM 3 Project Manager for a period of 4 months
Cost Item / Element Dedicated Project Resources required EFT No's
2004/05$000's
Salary & Wages (see note 1)
Project Manager HSM3 (4months)
1 28.0
Good & Services (example of major consumables required)
Stationery
.4
Other (including equipment by item and quantity)
Meeting costs, teleconference, telephone calls, travel and accommodation
2.6
Total Expenses 31.0
Note 1: Salary and Wages includes 10.09% on costs The majority of the budget provided salary and wages for one project officer for a 16-week period. Goods and Services including travel and accommodation costs were kept to a minimum by running area wide workshops with clinicians.
3. Lessons Learnt
3.1. What Worked Well?
• Area wide 1 – 2 day workshops enabled cost effective participation of each area health service. • Provision of background materials and workshop outlines prior to session dates prepared
participants for workshop sessions and tended to improve participant understanding and flow of information.
• Personal contact with prospective participants proved more successful in fostering engagement than relying upon the dissemination of e-mail material.
• Presentations to the GMCT Forum and Allied Health Representatives and Chairs appeared to improve acceptance of the project.
3.2. What Could Be Improved?
• Additional preparation time for participants. A number of participants indicated that they would have liked more time to prepare for the workshop session. Some areas did not receive information in sufficient time to prepare for the workshop session due to a reliance on e-mail for the dissemination of information.
• Earlier contact with Allied Health representatives to facilitate engagement in the process. • An additional group facilitator for larger group workshops to maintain focus and ensure quality
of data
Closure Activities
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 9
• Additional time allocation for the collation and entry of workshop data. • Additional time for correspondence with participants post workshop for review and feedback of
data. • Additional time for the project to look at validation of the information obtained not only
statistically but also through engaging the appropriate professional bodies for each discipline.
4. Closure Activities
• Project Staff: - The details of the project will be disseminated to the Project Steering Committee and GMCT Executive for review February / March, 2006.
• Dissemination of Project outcomes to Allied Health participants, clinicians and representatives.
• Proposal submitted to GMCT Executive regarding the co-ordination of an Allied Health Forum re workforce challenges. Project outcomes to be presented at this forum as a communication strategy, should such an event take place.
• Steering committee to discuss opportunities for further project funding with GMCT Executive, February, 2006.
• Record Management – Copies of all documents to be electronically stored within GMCT databases.
Appendices
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is Appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
5. Appendices
Appendix A Allied Health Clinical Interventions and Staffing Guidelines
Appendix B Comparative Tables
Appendix A
2
Allied Health Clinical Interventions and Staffing Guidelines. Allied Health is not a homogenous group but a collective of unique professions, which provide core specialist services to Metropolitan Hospitals. As a group they have often battled with the view that Allied Health services are not essential to the running of a hospital. A view which ignores the enormous role that Allied Health plays in the diagnosis, treatment and discharge planning of acute inpatients, and the long term management of health clients in the community. Allied Health professions are united by the fact that they are not part of the larger medical and nursing groups. They are united by their predicament. Early involvement of key professions in the care plan/ management plan enhances clinical effectiveness, impacts on length of stay, enhances therapeutic interventions and avoidance of complications1 Identifying exactly which professions should be present in order to provide optimal health care has often defaulted to the divisibility of limited resources, the ability of those representing a profession to put forward a reasonable argument, often in direct competition with other Allied Health professions, and the subjective views of the financier. Few guidelines have been developed to address staffing levels and skill – mix for Allied Health professions. Those that have been attempted highlight the enormity of such a task given the complex, moveable feast, that is Public Health. Staffing Ratios To date there have been a number of attempts to develop staffing ratios for particular service areas eg. Acute Stroke and Aged Care. As a result managers have utilised these figures to argue for additional enhancement funding. Whilst based on expert consensus adopting a ‘one size fits all’ approach does not reflect the complex changing needs of our clients and the health system. Previous staffing ratios were based upon round table discussion. Whilst not without credibility they remained very subjective. Ratios do not define what level of service is actually being prescribed nor do they account for the enormous variability, which exists between sites, services, and populations. The level of staffing required by one particular service may fall above or below that required by another service provided within the same clinical area. In addition Bed numbers are used to define staffing ratios. This is ironic given that the vast majority of allied health interventions are not driven by bed numbers but the complexity of the client that lies within. In November 2004 the clinical Sub – Committee of the metropolitan Hospital Program – GMCT put together a draft document outlining recommended Allied Health staffing ratios for Metropolitan Hospitals. It was from the early work of this group that the concept of this project was born.
1 Allied Health Professionals and Healthcare Scientists Critical Care Staffing Guidance – A Guideline for AHP and HCS Staffing Levels, July 2003.
Appendix A
3
Issues impacting on staffing levels There are a number of variables, which must be taken into account when defining appropriate staffing levels and skills-mix. These include: - Casemix - Client complexity - Bed occupancy and Length of stay - Seasonal fluctuations in admission and incident rates. - Models of care - Treatment complexity - Clinical Governance and Infrastructure requirements - Local service infrastructure and processes - Departmental and Organisational structures - Local demographics impacting on the health needs of the population - Access to appropriate resources both within the hospital system and out in the community - Local Geography including site and service locations - Financial resources - Clinical Interventions driven by best practice and client needs. - Level of preparation and experience (ie. Competency) of those providing care2 - Quality of life and optimal health outcomes for metropolitan hospital clients3 - Duty of care responsibilities3 - Responsibilities under OH&S legislation and the promotion of a safe and healthy workplace3 - Recruitment issues - Leave coverage - Service Hours of operation including the need / availability of overtime and On- Call - Inter-relationships between services ie. Speech Pathology and Radiology, Nutrition and Food Services, Occupational Therapy and Physiotherapy. Casemix Casemix data is very useful for establishing the number and mix of diagnoses which may flow through a clinical area however many Allied Health interventions are driven by client need, rather than the diagnosis allotted to a client, particularly when there are other significant co-morbidities impacting on a patients recovery. Aged care clients for example are notoriously complex.
2 Safe Staffing Guidelines, Alabama State Nurses’ Association Reporter.2000 Mar-May; 27(2): 13. 3 National Aged Care Alliance – Principles for Staffing Levels and Skills Mix in Aged Care Settings, December 2004.

Appendix A
4
The presence of dementia, for example on top of surgery, say for a fractured neck of femur, may exponentially increase the amount of time and resources required to see such a patient through to discharge. The level of Allied Health involvement in this instance may vary. For a discipline such as Social Work there may be additional time spent with the clients family due to emotional, legal and financial implications of the clients cognitive function. Physiotherapy on the other hand may spend less time with a client who is confused or restrained. Social Work intervention is perhaps least concerned about the diagnosis of a patient and more concerned with the psychosocial impact of trauma or illness on the client and his or her family or carers. It is possible in fact for a social worker to spend a significant amount of time with someone who has no immediate medical need in the case of a homeless person presenting to the ED. Client Complexity The following are examples of issues which can significantly impact upon the amount of intervention time spent with a client - Co-morbidities as in the aged care example mentioned above. - Family dynamics - NESB clients requiring interpreters - The absence of supports in the community E.g. living alone, conflicts with family, limited access to community services. - Specialised equipment needs eg. palliative care clients – hospital beds, pressure care mattresses, wheelchairs etc. - Obesity - Access to bariatric equipment, OH&S issues, staff numbers for mobility etc The true complexities of a case are often not revealed until after assessment and treatment has commenced. Bed occupancy and Length of stay Bed occupancy and Length of Stay may or may not impact on the amount of intervention time required from Allied Health disciplines. Clients who require daily interventions throughout their stay eg. daily mobilisation by a Physiotherapist, will naturally increase intervention hours should they stay longer in hospital. Decreasing length of stay can dramatically increase allied health workload particularly if clients are being sent home ‘sicker’ than previously. For example if LOS for hip surgery is decreased then more patients are likely to require equipment for discharge than if they remained in hospital until they were more ambulant. There is of course an increase in the number of initial assessments required to be completed by allied health staff as patient turnover increases. In the majority of cases Length of Stay appears to drive the prioritisation process ie. Clients going home sooner will often be seen first.

Appendix A
5
Models of care Allied Health Disciplines work across all areas of the health service continuum. Eg. Primary health care
Early intervention Acute care Post acute care Chronic Care Health education/disease prevention
Models of care will impact significantly on a particular disciplines approach, where intervention is focused, and the time spent providing particular interventions. For Example: The treatment focus for an Occupational Therapist in an Acute Medical Ward may be assessment, safe discharge and referral to other services for further treatment. In a Rehab setting treatment will be more intensive and aim at assisting the client towards safety and independence in the home. In a Community Outreach therapy service the OT may be treating the client in the context of the home and community environment, maintaining function and addressing long term goals. Therapist hours will vary considerably in each context. Treatment complexity Advances in treatment technology, evidence based practise, and the increasing acuity of clients entering and moving within the Health System impact significantly on staffing requirements. Clinical Governance and Infrastructure requirements No Clinical workforce can be suitably trained and maintained without appropriate professional leadership, supervision and support. Suitably structured services not only allow for the development and maintenance of a competent workforce but allow for capacity building of a service with the availability of temporary coverage, access to senior and specialist staff for mentoring and supervision, and a greater depth of knowledge and experience. It must be acknowledged that a significant amount of clinical and management resources are required for the development of competent, professional clinicians. Appropriate management structures provide an environment of professional support and Clinical Governance throughout the professional learning continuum.

Appendix A
6
The Allied Health Staffing Matrix. The Allied Health Staffing Matrix has been developed as a template or guide for determining staffing requirements in a particular clinical area based upon client profile, the unique clinical interventions a discipline provides, the Clinical Governance and Infrastructure requirements of the service and the average amount of time required to perform the interventions / duties outlined. In addition it is a tool for defining levels of service achievable for dollar values and determining staff mix based upon client needs and the clinical interventions provided by each discipline. The matrix is to be used in conjunction with relevant statistical data. Whether this includes casemix data re Diagnostic categories, Average number of cases per year, Length of Stay etc, prospective Population Planning unit data or clinician generated statistics recorded on paper or through databases such as AHMIS (Allied Health Management Information System). The Matrix is designed to be flexible in order to: - meet the changing needs of clients and the health system - allow information to be customised to suit each locality - allow application to any clinical area, not just acute inpatients or hospital based outpatients. Skill –mix can be determined by identifying what interventions clients will be expected to require and which disciplines are best able to provide these interventions. The use of technical and support staff can also be mapped out for each clinical area. The Matrix does not address competency levels of staff nor levels of seniority. These things need to be determined by the person designing the service in the context of departmental and organisational structures. It must be clearly stated that any statement of staffing level, therapist hours or FTE requirement can only truly be applied to the specific site that is described. It is not appropriate to generalise numbers across all sites/ settings/ services as this ignores the unique nature of each locality and the variables described earlier. Each of the parameters included in the matrix may vary between localities. Numbers appropriate for one setting will not necessarily be appropriate for another. Matrix data presented to date makes no statement of what is Best Practise nor any determination of expected clinical outcomes. These things will need to be addressed by each particular Allied Health profession.

Appendix A
7
Understanding the Matrix template From the Top Initial headings identify the discipline to be described, clinical area to be serviced and the number of beds this incorporates. Diagnostic / Target Groups The first column describes the Diagnostic or target client groups for the service These are the main diagnoses or client groups that the particular discipline targets or sees as a priority in this clinical area. In addition it includes types of clients or intervention needs that tend to demand more of the service ie-additional therapist hours. Average Number of Cases per year / Average Length of Stay Columns 2 and 3 relate to relevant statistical information obtained via casemix, allied health or relevant local population projections. Intervention Requirements per client This column outlines all of the unique interventions provided by the particular discipline for each diagnostic / targeted client group. It includes all client-related activities not just face to face contact. It is also a description of the level of service, which can be provided given appropriate staffing. For many of the Allied Health disciplines interviewed there were number of interventions which are conducted with all clients. For this reason many of the templates have been divided horizontally into ‘Interventions attributable to most clients’ (top section) and ‘Additional intervention hours specific to client group’ (sections below). Average Intervention time (mins/ hours) Obviously the amount of time it takes to complete an intervention will fluctuate depending upon client complexity and the clinical expertise of the health professional involved. This figure is an estimated average. It is assumed that this figure should represent the majority of interventions and therefore allow for the extreme cases, which tend to occur less frequently ie. Time spent with a particular group of clients may vary from 5 minutes to 3 hours however the majority of clients would fall somewhere between these two figures. Where possible local statistical information should be entered into this field to improve accuracy / validity. This may be done retrospectively, where existing data is available or estimated, using sound clinical judgement and expertise, in the case of a new service.

Appendix A
8
Clinical Governance and Infrastructure This includes all Departmental and Infrastructure activities necessary for efficient and safe operation of a quality allied health service Including: - Supervision and Professional Development - Clinical Training of Staff and Students - Administration / statistics - Departmental meetings and In-services - Continuing Education including Evidence Based Practise - Mandatory training requirements eg. OH&S, Manual Handling, Infection control, Child Protection - Non – Clinical travel where staff are required to travel to other sites to complete the above Consideration also needs to be given to the level of seniority of the position being developed / described as this will alter time requirements for Clinical Governance and Infrastructure activities. Some areas may already stipulate clinical vs non clinical workload ratios for staff. Figures are calculated as hours per Full Time Equivalent (40 hours per week). Obviously if therapy hours were to equate to a part time figure then Clinical Governance and infrastructure figures would need to be adjusted accordingly. Leave Coverage The absence of Leave Coverage is a long-standing issue for Allied Health disciplines. This has not been the case for Nursing and Junior Medical staff. Few examples exist where Allied Health have successfully included leave coverage into staffing establishment. In the majority of instances limited coverage is provided by existing staff establishment, often on an urgent only basis and to the detriment of other clinical areas and services. For the purpose of this exercise only Annual Leave, Sick Leave and FACS leave have been included. It must be noted that whilst 4 weeks Annual Leave is considered a mandatory entitlement, Sick Leave and FACS leave are left to the discretion of the staff member and may accrue over several years. For this reason no additional leave entitlements have been factored into coverage hours. Further refining of coverage hours would be possible if there was a means of determining a figure for Average Leave of Absence within a service. Coverage for ADOs (Allocated Days Off) has not been included in this instance as staff work additional hours for this entitlement. If coverage for ADOs was considered necessary in a particular area than this could either be built into the framework or provided by existing establishment as deemed appropriate.

Appendix A
9
*Caseload Specific hours This represents all caseload-related activities, which form a significant part of therapist hours and cannot be specifically attributed to an individual patient Eg. Case Conferences, other clinical team meetings, clinical travel. Therapy Assistant (Y/N) The purpose of this column is to assist Allied Health managers to clearly delineate clinical interventions that could be completed by a Technical Assistant and under what circumstances this should occur eg. Direct / Indirect Supervision from a suitably qualified health professional, Only after specific training etc. Assumptions In order to accommodate both full time and part time staffing calculations it is assumed that * 1 FTE represents approximately 2080 hours of available service per year PROVIDED there is full coverage for annual leave, sick leave and ADO’s. In reality there are fewer hours available for 1 FTE when we consider that coverage may not be available for leave entitlements or Allocated Days Off and that there are 11 NSW Public Holidays in one calendar year. 40 hours per week x 52 = 2080 hours 12 Allocated Days Off per year = 96hours (Assuming no coverage provided) 11 NSW Public Holidays = 88hours In the absence of annual, sick and FACS leave coverage service hours for 1 FTE could potentially be reduced to 1644 hrs per year (4 weeks annual leave entitlement + 2 weeks sick leave + 3 days FACS leave = 252hours) Generally part time positions would not be entitled to ADO’s and may or may not be impacted upon by public holidays.

Appendix A
10
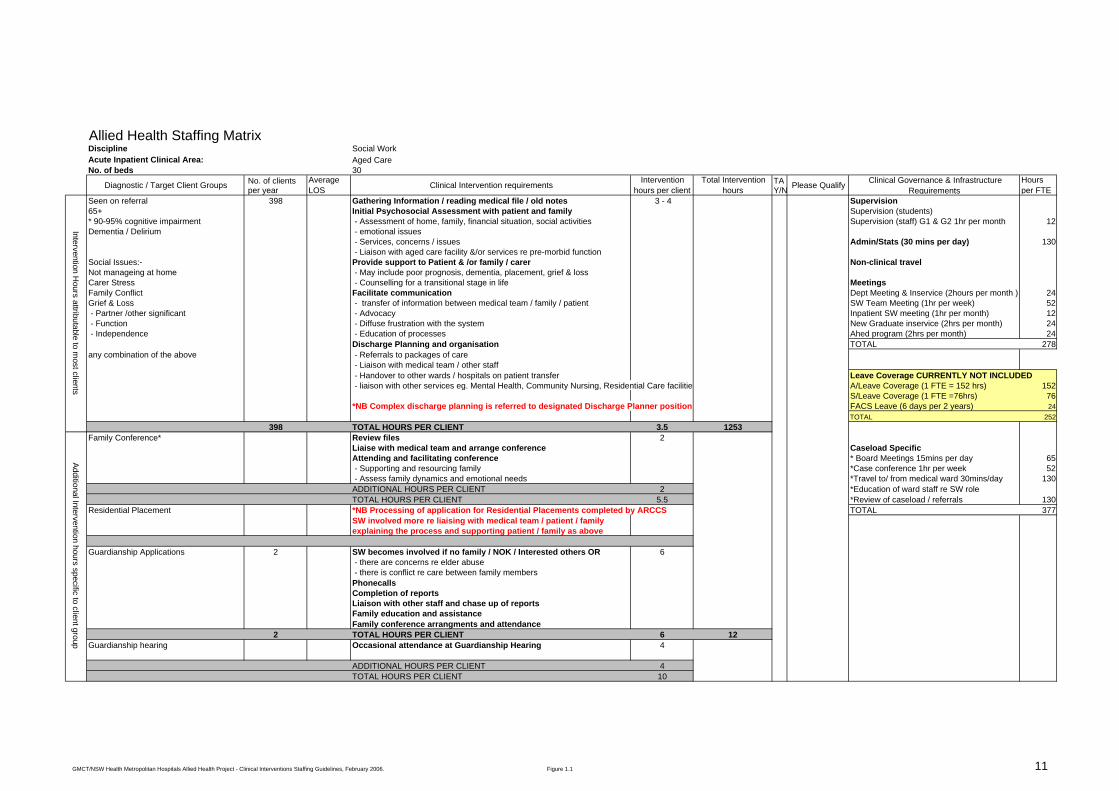
Allied Health Staffing Matrix Example 1 Social Work – Aged Care Figure 1.1 is one example of a staffing matrix completed for Social Work in an Acute Aged Care unit. Clinical Area Description: This particular unit is a 30 bed Acute Aged Care ward situated within a 274 bed Metropolitan Hospital in an area which has a significant and increasing elderly population (approximately 18% over the age of 65).4 It has access to Geriatrician services as well as other Allied Health professionals including Physiotherapy, Occupational Therapy, Nutrition and Speech Pathology. Psychology services are available on a consultancy basis. Clients are seen on referral from ward staff. Social Work staff are not required to complete applications for residential placements as this is performed by ARCCS (Aged and Residential Continuing Care Service) Complex Discharge planning is referred to a designated Discharge Planner Position Area Department structure enables sufficient coverage for limited periods of absence. Staff work 8 hours per day in order to accrue one ADO per month. In addition Clinicians reported the following: - Generally Social Work intervention is not diagnosis driven. - Social Work staff felt that 90 – 95% of clients seen present with cognitive impairment. - Staff reported that it takes between 3 to 4 hours to provide the listed interventions to the majority of clients
Having said this an extremely straightforward case may take 20 to 30 minutes to attend to. eg. → Patient requiring Nursing Home placement and accepting of this.
→ Family accepting of need for nursing home placement → Medical team involved
→ Patient previously assessed as suitable for placement - Additional intervention hours are required for clients requiring family conferences, residential placement, Guardianship applications, Respite care or
where there is family conflict or carer stress. - Death viewings with families and Destitute funerals were also identified as placing significant demands on Social Worker time. - Intervention time will increase with an increase in psychosocial issues / complexity - The need for a family conference is determined on a case by case assessment - Length of stay will also affect levels of Social Work intervention and the amount of ongoing support offered. 4Basic Community Profile completed by the Australian Bureau of statistics August 7, 2001 Census.
Allied Health Staffing MatrixSocial WorkAged Care 30
No. of clients TA per year Y/N
Seen on referral 398 Gathering Information / reading medical file / old notes 3 - 4 Supervision65+ Initial Psychosocial Assessment with patient and family Supervision (students) * 90-95% cognitive impairment - Assessment of home, family, financial situation, social activities Supervision (staff) G1 & G2 1hr per month 12Dementia / Delirium - emotional issues
- Services, concerns / issues Admin/Stats (30 mins per day) 130 - Liaison with aged care facility &/or services re pre-morbid function
Social Issues:- Provide support to Patient & /or family / carer Non-clinical travel Not manageing at home - May include poor prognosis, dementia, placement, grief & lossCarer Stress - Counselling for a transitional stage in life MeetingsFamily Conflict Facilitate communication Dept Meeting & Inservice (2hours per month ) 24Grief & Loss - transfer of information between medical team / family / patient SW Team Meeting (1hr per week) 52 - Partner /other significant - Advocacy Inpatient SW meeting (1hr per month) 12 - Function - Diffuse frustration with the system New Graduate inservice (2hrs per month) 24 - Independence - Education of processes Ahed program (2hrs per month) 24
Discharge Planning and organisation TOTAL 278any combination of the above - Referrals to packages of care
- Liaison with medical team / other staff - Handover to other wards / hospitals on patient transfer Leave Coverage CURRENTLY NOT INCLUDED- liaison with other services eg. Mental Health, Community Nursing, Residential Care facilities A/Leave Coverage (1 FTE = 152 hrs) 152
S/Leave Coverage (1 FTE =76hrs) 76*NB Complex discharge planning is referred to designated Discharge Planner position FACS Leave (6 days per 2 years) 24
TOTAL 252398 TOTAL HOURS PER CLIENT 3.5 1253
Family Conference* Review files 2Liaise with medical team and arrange conference Caseload SpecificAttending and facilitating conference * Board Meetings 15mins per day 65 - Supporting and resourcing family *Case conference 1hr per week 52 - Assess family dynamics and emotional needs *Travel to/ from medical ward 30mins/day 130ADDITIONAL HOURS PER CLIENT 2 *Education of ward staff re SW roleTOTAL HOURS PER CLIENT 5.5 *Review of caseload / referrals 130
Residential Placement *NB Processing of application for Residential Placements completed by ARCCS TOTAL 377SW involved more re liaising with medical team / patient / familyexplaining the process and supporting patient / family as above
Guardianship Applications 2 SW becomes involved if no family / NOK / Interested others OR 6 - there are concerns re elder abuse - there is conflict re care between family membersPhonecallsCompletion of reportsLiaison with other staff and chase up of reportsFamily education and assistanceFamily conference arrangments and attendance
2 TOTAL HOURS PER CLIENT 6 12Guardianship hearing Occasional attendance at Guardianship Hearing 4
ADDITIONAL HOURS PER CLIENT 4TOTAL HOURS PER CLIENT 10
Additional Intervention hours specific to client groupIntervention H
ours attributable to most clients
No. of bedsAverage LOSDiagnostic / Target Client Groups
DisciplineAcute Inpatient Clinical Area:
Intervention hours per client
Hours per FTE
Total Intervention hours
Clinical Governance & Infrastructure RequirementsPlease QualifyClinical Intervention requirements
GMCT/NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions Staffing Guidelines, February 2006. Figure 1.1 11

Allied Health Staffing MatrixSocial WorkAged Care
Target Groups Average No. of Intervention requirements per client TA Please Qualify Clinical Governance & Infrastructure cases per year Y/N Hours per FTE
Respite Care Liaising with services and finding appropriate respite 1
TOTAL HOURS PER CLIENT 1Carer stress Conflict resolution / Family Conference 2Family Conflict Counselling
Organising support networksTOTAL HOURS PER CLIENT 2
Death 40 Arrange time with mortuary 0.5 - 2Viewings if requested by nursing / family Meet with the family re: process
View body before family & explain what the deceased will look likeStay and provide support after viewingProvide written information about Grief and when Someone Dies in Hospital
40 TOTAL HOURS PER CLIENT 1.25 50Destitute Funeral Co-ordinate Funeral and paperwork for DOH payment 3
TOTAL HOURS PER CLIENT 3 TOTAL 655TOTAL CLINICAL INTERVENTION HOURS 1315TOTAL INFRASTRUCTURE HOURS 655TOTAL CLINICIAN HOURS 1970
Intervention time (hrs)
Hours per FTE
Additional Intervention hours specific to client group
DisciplineAcute Inpatient Clinical Area:No. of beds
Average LOS
Total Intervention hours
Figures tabled are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT/NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions Staffing Guidelines, February 2006. Figure 1.1 11

Appendix A
12
Data Analysis In this particular Aged Care Ward 400 clients were seen by Social Work staff over a 12 month period (Data obtained via paper and newly established AHMIS data entries). It was deemed important to utilise a full Calendar year in order to capture seasonal fluctuations in admission and incident rates. Of these 400, 2 were identified as requiring Guardianship interventions and another 40 involved viewings of deceased clients. No figures were available for any other targeted groups listed however it was felt that what remained would more than likely be covered within the intervention hours for the larger group. Based on the figures provided: The majority of clients required 3-4 hours of Social Work intervention (assume 3.5 hours for the purpose of estimation) Two clients required approximately 6 hours of intervention for Guardianship applications. No attendance at a hearing was required during the 12 month snapshot so in this instance the additional 4 hours for this intervention has been disregarded. Social Work attended 40 deceased viewings. Clinicians estimated that these interventions take between 30mins to 2 hours. Given the range of time an average of 1.25 hours or 75 mins was assumed. Number of clients seen by Social Work in Aged Care per year x Estimated hours per client = Clinical Intervention hours per year Ie. 358 x 3.5 = 1253 2 x 6 = 12 40 x 1.25 = 50 TOTALS 400 CLIENTS 1315 CLINICAL INTERVENTION HOURS Clinical Governance and Infrastructure hours total 907 hours with full leave coverage (655 hours in the absence of leave coverage).

Appendix A
13
TOTAL CLINICAL INTERVENTION HOURS + TOTAL INFRASTRUCTURE HOURS = TOTAL CLINICIAN HOURS Ie. 1315 + 907 = 2222 CLINICIAN HOURS Given that the data provided is retrospective and representative of an existing service we must take into account that there is currently no leave coverage other than that provided from within the Social Work department as able Ie. 1315 + 655 = 1970 CLINICIAN HOURS FTE conversion 1970 divided by 2080 = 0.94 RESULTS The methodology used to develop this matrix would appear to substantiate the need for 1 FTE of social work services in this particular clinical unit. Staff interviewed believed that 1 FTE provided sufficient clinician time to attend to the needs of the clients entering the service as well as the needs of staff and administration. Management and clinical staff agreed that this level of staffing resulted in a productive, manageable workload for Social Work clinicians. Leave coverage is currently not built in to the Social Work establishment and should perhaps be considered for future staffing enhancements.

Appendix A
14
Allied Health Staffing Matrix Example 2 Occupational Therapy – General Medical Figure 2.1 is one example of a staffing matrix completed for Occupational Therapy in an Acute General Medical Ward Definitions: General Medical Ward For the purpose of this project a ‘General Medical Ward’ is defined as an acute medical ward which may provide limited specialist services but generally will expect to see any number and combination of medical diagnoses subject to local demographics and disease prevalence. Initial Assessment An assessment of: - Social Situation (Family /other supports, services) - Home Environment (equipment needs, Access, Safety Issues) - Previous and current level of function re: Self Maintenance, Productivity - Paid and unpaid work, Leisure, rest - Brief Assessment of Physical, Cognitive, Perceptual and emotional function. Self care Assessment - An assessment tool used to identify functional deficits which may impact on safety and independence - Cognitive and perceptual function - Functional mobility, transfers, Equipment, dressing / showering / drying / toileting / grooming - Provides an insight into the ability of the patient to perform daily maintenance tasks at home - Provides a baseline measurement for self care re-training if appropriate Kitchen Assessment - Assessment of the client’s ability to plan, sequence and physically prepare a meal / light snack - Addresses Physical, Cognitive and Perceptual function - Safety in operating appliances, the use of electricity and heat. - Provides insight into the ability of the patient to safely attend to nutritional needs once home - Provides a baseline for retraining if appropriate

Allied Health Staffing Matrix Occupational TherapyGeneral Medicine 26
TA Please QualifyY/N
General Medical 105 Review of medical file 10 Supervision (students) Patients Initial assessment - including return to work and driving 30 - average of 3 weeks per year
Functional Review 20 - approx imately 2 hours per dayequipment prescription / ordering 10 Supervision (staff) provision and explanation of equipt use 10 Y Guided by OT - G1 2 hours per week 104Family / carer education 15 - Formal Performance Appraisal 2 hours per year 2report writing 40 Admin/stats 130gathering resources 5 Y Guided by OT - 30 mins per dayreferral out 5 Non-clinical travel 9liaison with other staff 10 - 45mins per month
105 TOTAL HOURS PER CLIENT 2.58 271.25 Dept Inservice 12Family Liaison with medical team 10 - 1hr per monthConferences Attendance at family conference 30 Department Business Meeting 12
ADDITIONAL HOURS PER CLIENT 0.67 - 1 hour per monthCVA Self Care Assessment 45 New Graduate inservice 24Neurological event Self care re-training- showering, dressing, toileting, oral hygiene 20 Y Training and supervision - 2 hours per month
report writing 15 Ahed program 24ADDITIONAL HOURS PER CLIENT 1.33 - 2 hours per monthCognitive screen 30 TOTAL 317Perceptual screen 30report writing 15ADDITIONAL HOURS PER CLIENT 1.25Upper Limb assessment 30Positioning 10 Leave Coverage CURRENTLY NOT INCLUDEDSplinting 60 Y To assist OT only A/Leave Coverage (1 FTE = 152 hrs) 152Upper limb ranging / retraining 30 Y Training and supervision S/Leave Coverage (1 FTE =76hrs) 76report writing 15 FACS Leave (6 days per 2 years) 24ADDITIONAL HOURS PER CLIENT 2.42 TOTAL 252Staff education re: management of patient on ward 10Family / carer education 15report writing 10ADDITIONAL HOURS PER CLIENT 0.58Kitchen assessment 45report writing 15ADDITIONAL HOURS PER CLIENT 1
Cognitive impairment cognitive screen 30Dementia Kitchen assessment 45
liaison with other staff - Med.,SW, CCN, PT 30 * Caseload specific infrastructurefamily /carer education 30 case conference - once per week 52
Delerium eg. Post anaesthesia, UTI, wound infection Daily review of cognitive status 30 board meetings - 15 mins daily 65report writing 30 TOTAL 117ADDITIONAL HOURS PER CLIENT 3.25
COPD 19 Self Care assessment 45Functional assessment 30Education / Retraining using Pulse Oximetry 60Liaison with medical team re Oxygen needs 15
19 ADDITIONAL HOURS PER CLIENT 2.5 47.5AMI Education on safe activities post AMI 20 N
Education on energy conservation techniques 20 NEducation on return to work 20 NEducation on driving 10 NReview of education 15 Y Guided by OTReferal out to Cardiac Rehab, CRS, Community OT 20 NADDITIONAL HOURS PER CLIENT 1.75
Additional interventions / hours specific to client groupInterventions/hours
attributable to most clients
DisciplineAcute Inpatient Clinical Area:No. of beds
Average LOSDiagnostic / Target
client groups Hours per FTE
No. of clients seen by OT Sept to Dec Intervention requirements Total Intervention
HoursClinical Governance & Infrastructure
RequirementsIntervention time (mins)
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 2.1 15

Allied Health Staffing Matrix Occupational TherapyGeneral Medicine (Continued)30Intervention requirements TA Please Qualify Clinical Governance & Infrastructure Including non face to face Y/N Hours per FTE
Cancer 21 Functional Review 10Paliative Care & going home equipment prescription / ordering 15
sourcing specialist equipment 30Family / carer education / training in client management 20referral out 5
21 ADDITIONAL HOURS PER CLIENT 1.33 28.00MVA Screening for Post Traumatic Amnesia 15
report writing 100.42
Daily review of Westmead PTA Scale 15report writing 10
Hand / UL Splinting 60 Y To assist OT onlyMisc # Outpatient referral 5nerve injuries report writing 10
ADDITIONAL HOURS PER CLIENT 1.25Communtiy Home Assessment Team Home assessment - preparation 30
Home assessment 60Travel - Home assessment 60report writing 90Liaison with inpatient staff 15Liaison with trades people 60ADDITIONAL HOURS PER CLIENT 5.25 TOTAL 434
TOTAL CLINICAL INTERVENTION HOURS 346.75TOTAL CLINICAL INTERVENTION HOURS FOR 12 MONTHS 1040.25TOTAL INFRASTRUCTURE HOURS 434TOTAL THERAPIST HOURS
Additional interventions / hours specific to client group
DisciplineAcute Inpatient Clinical Area:
Com
munity
Interventions
Hours per FTE
No. of beds
Average LOSIntervention time (mins)
Total Intervention Hours
No. of clients seen by OT Sept to Dec
Diagnostic / Target client groups
Figures tabled are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 2.1 15

Appendix A
16
Clinical Area Description:
This particular Medical ward (X) is a relatively new unit situated within a recently redeveloped 274 bed metropolitan hospital. 4 of the 30 beds have been separately funded as Acute Stroke beds and have therefore not been included in the statistical data presented. The Hospital services a significant and increasing elderly population (approximately 18% over the age of 65).4 Other Allied Health professionals provide a service to this ward including Physiotherapy, Social Work, Nutrition and Speech Pathology. Psychology services are available on a consultancy basis. Referrals are received via ward staff or through bed list screening for blanket referral diagnoses. Blanket referral status exists for the following diagnoses: CVA, Fractured Neck of Femur, Total Hip Replacement / Hemi arthroplasty, Total Knee Replacement, Chronic Obstructive Pulmonary Disease, Acute Myocardial Infarct & under 65years of age. Occupational Therapy services are not funded for specific hours in this medical ward but provide a service across two medical wards, 2 surgical wards and outpatients. Time spent in one particular ward location is determined by referral rates and professional prioritisation. This service is operated 5 days per week excluding public holidays, 8am to 4.30pm. Community Home Assessments are not conducted by inpatient staff. Inpatient staff liaise closely with the Community Home Assessment Team to determine home environment needs prior to or immediately post discharge. Equipment may be provided for discharge as a temporary measure for those clients requiring home modifications. Length of Stay tends to drive the prioritisation process. This service has only recently adopted AHMIS as its Statistical database. Staff enter statistics into this database on a daily basis. Data Analysis This particular OT department had only been inputting statistics into AHMIS for 6 months prior to this project. Data for the first 2 months of this period was inadequate due to the fact that staff were still familiarising themselves with the database. For this reason only 4 months worth of AHMIS data was reviewed and the figures extrapolated over a 12 month period. 129 referrals were received by Occupational Therapy in this medical ward from September to December. Only 105 clients were entered into the AHMIS database. Of those reported, 21 were listed with a diagnosis of Neoplasm – Cancer, 19 with COPD, 15 with CVA and 8 with FALLS 4 Basic Community Profile completed by the Australian Bureau of statistics August 7, 2001 Census.

Appendix A
17
The remaining clients were reported under other diagnoses with client numbers of 5 or less. (See table 2.2). Diagnosis No. of Patients Time Units (minutes) Average Intervention time (hrs) 020 Neoplasms - Cancer 21 3606 2.86 082 Chronic Obstructive Airways Limitation 19 1595 1.39 074 CVA - TIA 15 2045 2.27 125 FALLS 8 610 1.27 Other diagnoses 42 4815 1.91 TOTALS 105 12671 2.01 Table 2.2 AHMIS Data for Medical ward X, September 2005 to December 2005 RESULTS With client numbers entered into the matrix the Total Clinician reported intervention time equals 346.75.25 hours. This result was multiplied by 3 to obtain a figure for 12 months ie. 1040.25 Caseload specific infrastructure hours must be added to this to determine total therapy hours required on the ward. Ie. 1040.25 + 117 = 1057.25 hours or approximately 0.5FTE of specific clinical caseload hours. NB. Clinical Governance and Infrastructure hours have not been factored into this figure due to the fact that staff provide coverage to a number of clinical areas based upon demand. If a Full Time staff member is providing services to the medical ward in question as well as other areas then the clinical governance and infrastructure requirements (0.2 FTE in this instance) must be factored in. If a part time staff member is providing service to this area then Clinical Governance and infrastructure hours may look quite different depending upon hours of work and availability to attend departmental meetings etc. Leave coverage hours would also proportional to hours of work.
Generally there tends to be a high turn over of therapy staff on the acute medical wards therefore staff are often less experienced or new graduates. For this reason additional hours have been factored in to include new graduate education and hours for student supervision have been omitted (New graduates do not take on student supervision until they have at least 12 months clinical experience). Clinician reported intervention times Whilst each individual intervention time may demonstrate some accuracy, the number and combination of interventions may vary considerably. It may not be worthwhile to separate out intervention times to such a degree but rather to identify total average times for each client group. Clinicians indicated that total time for most clients would be approximately 2.58 hours. AHMIS data indicated a total average intervention time of 2.01 hours however this figure was obtained from only 4 months worth of data from staff using a new system of reporting.

Appendix A
18
Allied Health Staffing Matrix Example 3 Physiotherapy - Figure 3.1 is one example of a staffing matrix completed for Physiotherapy in Outpatients Clinical Area Description: This particular Outpatient service is part of a Metropolitan Hospital in an area which has a significant NESB population as well as large numbers of clients with chronic and complex conditions. During the 2001 Census 48.4% of the local population reported speaking only English at home5. The three most common languages spoken at home other than English were Arabic (including Lebanese): 26719 (16.2%), Vietnamese: 11811 (7.2%) and Chinese languages: 8143 (4.9%). Interpreter services are engaged daily by at least one clinician in the service. Clients are seen on referral Staff work 8 hours per day in order to accrue one ADO per month. Treatment sessions must comply with allocated timeslots of 60mins initial assessment and 30 mins follow up treatment . On average clients receive 6-8 follow up treatment sessions Elderly clients and those requiring interpreter services generally take longer to see Previous service reviews identified that clients requiring interpreters tended to wait %80 longer for treatment than English speaking clients. In order to address this the service instituted set days / times for clients with specific interpreter needs. For example an ‘Arabic morning’ where the team of therapists arranges bookings with an interpreter for clients who speak Arabic. Groups vary from site to site and are dependent on staffing and client need Technical Assistant availability is dependent job description with duties/ responsibilities shared across clinical areas. Until recently there was no clerical support available and therapists were required to arrange all appointment and interpreter bookings
5 Basic Community Profile completed by the Australian Bureau of statistics August 7, 2001 Census

Allied Health Staffing Matrix PhysiotherapyOutpatient
TAY/N
Initial assessment / treatment session Referral received All StaffInitial assessment Y Receiving referrals,taking details , Mandatory training courses
Chronic / complex issues - Investigations eg. CT, Xray , MRI making booking - 1-5 days per year 40Low back pain - Subjective assessment N Stats New patient - Objective assessment N - 15 mins per day 65
- Treatment planning / goal setting N Dept inservice 60 minutes allocated per session Treatment N - 1 hour per fortnight 25
- eg. Traction, mobilisation, exercises, Y Assistance with supervision of exercises Staff meetings - Advice, education , handouts - 1 hour per fortnight 25
Evidence Based Practise Interpreter required Use of interpreter to complete above 10 - 15 - 1 hour per week 52
Bookings dependent upon availability Site unit meetings TOTAL HOURS PER CLIENT 1 422 - including admin / education / EBP
Follow up Assessment / Treatment Review assessment - 1 hour per week 52Lower back pain Subjective assessment Admin tasks
Objective assessment - 1 hour per day 260Treatment planning - Answering phones / clerical activities in the absence of clerical Treatment support
30 minutes allocated per session - eg. Traction, mobilisation, exercises, OH&S - Advice, education , handouts - monthly inspectionsNotes - 2 hours per month for each area 24
NESB Use of interpreter to complete above 10 - 15 Grade 2 / 3Interpreter required Bookings dependent upon availability Admin tasks
TOTAL HOURS PER CLIENT 0.5 1477 - 3 hours per dayNew patient Referral received(Post surgical) Investigations / Check Protoco OrientationOrthopaedics Subjective assessment - new staff and staff on rotation# Humerus Treatment - 8hours 4-6 times per year
- planning / Goal setting45 minutes allocated per session - exercise prescription, sling provision
- Advice, printing / drawing exercises
TOTAL HOURS PER CLIENT 0.75 270Follow up Review assessment( Post Surgical) Subjective assessment
Objective assessmentTreatment - planning
30 minutes allocated per session - eg. Traction, mobilisation, exercises, - Advice, education , handouts Leave Coverage CURRENTLY NOT INCLUDEDNotes A/Leave Coverage (1 FTE = 152 hrs) 152TOTAL HOURS PER CLIENT 0.5 1260 S/Leave Coverage (1 FTE =76hrs) 76
NESB Use of interpreter to complete above 5 - 10 FACS Leave (6 days per 2 years) 24Interpreter required Bookings dependent upon availability TOTAL 252
NESB Additional time may be required if patient of NESB 5 - 10in absence of interpreter and interpreter not present
Aging clients Additional time required 5 - 10ie. getting dressed / undressed, mobility
Total Intervention Hours
7
360 1
360 7
60
30
45
30
Additional interventions / hours specific to client group
422
Diagnostic / Target Group
Clinical Area:
Average No. treatment sessions
422 1
Discipline
Additional interventions / hours specific to client groupIntervention / hours attributable to m
ost clientsIntervention / hours
attributable to most clients
Average No. of cases per year Please Qualify
Hours per FTEClinical Governance & Infrastructure RequirementsIntervention time (mins)Clinical Intervention requirements
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 3.1 19

Allied Health Staffing Matrix
Discipline PhysiotherapyClinical Area: Outpatient (Continued)
TAY/N
POP Application Referral received Yor Splinting Preparation of materials & room Y
Application of splint or POP Y Only to assist PTAdvice on skin care / precautionsRebook for removal and reviewDocumentationTOTAL HOURS PER CLIENT 0.75 150
Removal Remove POP - provide advice, exit app. / notes 15 Y Only to assist PT
TOTAL HOURS PER CLIENT 0.25 50Group Work Contacting patients 60 Y
Assessment for group see below NPreparation / Organising equipment etc 15 YRunning group session see below Y With supervisionRecording group activities in records 15Post group assessment 20 mins per patient see below Y With PhysiotherapistTOTAL HOURS PER GROUP SESSION 1.5 72
Able & Stable' Falls prevention x8 1 hour sessions + 4 hours of education + interventions above Y With training & supervisionTOTAL HOURS PER GROUP
Back 90mins per week for 6 weeks + 1hour initial assessment + interventions above Y With training & supervisionTOTAL HOURS PER GROUP
Neck 90mins per week for 6 weeks + 1hour initial assessment + interventions above Y With training & supervisionTOTAL HOURS PER GROUP
Knee 90mins per week for 6 weeks + interventions above Y With training & supervisionno. sessions TOTAL HOURS PER CLIENT
Open Gym Assessment for group (per client ) 20 NAssessment for Discharge (per client) 20 Y With PhysiotherapistTOTAL HOURS PER CLIENT 0.67 293.31 hour per week for 12 weeks + interventions above 60 Y With training & supervisionTOTAL HOURS PER GROUP SESSION 1 48 TOTAL 795
TOTAL CLINICAL INTERVENTION HOURS 3994.3TOTAL INFRASTRUCTURE HOURS 1590TOTAL THERAPIST HOURS 5584.3
Total Intervention Hours
440 48
45
Additional interventions specific to client group
Intervention / hours attributable to m
ost clients
200
200
Please Qualify
Groupw
ork interventions
Diagnostic / Target Group Average No. of cases per year Clinical Governance & Infrastructure Requirements
Hours per FTE
Average No. treatment sessions Clinical Intervention requirements Intervention time (mins)
Figures tabled are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 3.1 19
Appendix A
20
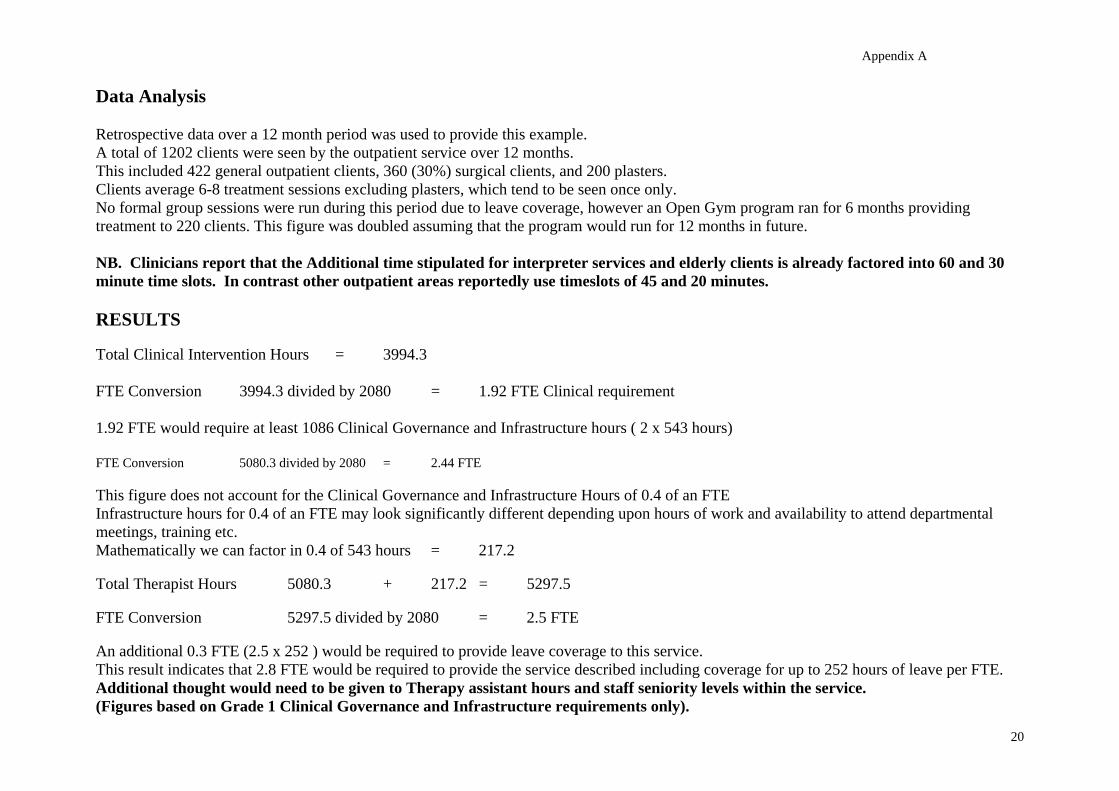
Data Analysis Retrospective data over a 12 month period was used to provide this example. A total of 1202 clients were seen by the outpatient service over 12 months. This included 422 general outpatient clients, 360 (30%) surgical clients, and 200 plasters. Clients average 6-8 treatment sessions excluding plasters, which tend to be seen once only. No formal group sessions were run during this period due to leave coverage, however an Open Gym program ran for 6 months providing treatment to 220 clients. This figure was doubled assuming that the program would run for 12 months in future. NB. Clinicians report that the Additional time stipulated for interpreter services and elderly clients is already factored into 60 and 30 minute time slots. In contrast other outpatient areas reportedly use timeslots of 45 and 20 minutes. RESULTS Total Clinical Intervention Hours = 3994.3 FTE Conversion 3994.3 divided by 2080 = 1.92 FTE Clinical requirement 1.92 FTE would require at least 1086 Clinical Governance and Infrastructure hours ( 2 x 543 hours) FTE Conversion 5080.3 divided by 2080 = 2.44 FTE This figure does not account for the Clinical Governance and Infrastructure Hours of 0.4 of an FTE Infrastructure hours for 0.4 of an FTE may look significantly different depending upon hours of work and availability to attend departmental meetings, training etc. Mathematically we can factor in 0.4 of 543 hours = 217.2 Total Therapist Hours 5080.3 + 217.2 = 5297.5 FTE Conversion 5297.5 divided by 2080 = 2.5 FTE An additional 0.3 FTE (2.5 x 252 ) would be required to provide leave coverage to this service. This result indicates that 2.8 FTE would be required to provide the service described including coverage for up to 252 hours of leave per FTE. Additional thought would need to be given to Therapy assistant hours and staff seniority levels within the service. (Figures based on Grade 1 Clinical Governance and Infrastructure requirements only).

Appendix A
21
Allied Health Staffing Matrix Example 4 Speech Pathology - Aged Care Figure 4.1 is one example of a staffing matrix completed for Speech Pathology in Aged Care. Clinical Area Description: Medical Ward Y is an Acute Aged Care ward situated within a 274 bed Metropolitan Hospital in an area which has a significant and increasing elderly population (approximately 18% over the age of 65).6 It has access to Geriatrician services as well as other allied health professionals including Physiotherapy, Occupational Therapy, Nutrition and Social Work. Psychology services are available on a consultancy basis. Clients are seen on referral from ward staff. Staff work 8 hours per day in order to accrue one ADO per month. 3.3 FTE across all inpatient and outpatient services including 0.5 FTE stroke unit . This establishment includes senior positions ie a grade 2 with supervisor responsibilities and a grade 3 clinical educator position. An additional consultation service is provided to a neighbouring Hospital as able with swallowing problems given priority Modified Barium Swallow (MBS) Clinics operate twice per week with Inpatients given priority. Local policy states that 2 staff are required to attend MBS procedures at all times. Data Analysis During a six month period this particular Speech Pathology service had seen a total of 52 clients on Medical ward Y (AHMIS reporting) Of these 13 had a diagnosis of Stroke, 7 were diagnosed with Dementia and 4 required Modified Barium Swallow assessment. Current AHMIS data collecting makes it difficult to determine how many patients required daily therapy interventions however clinicians felt that the majority of stroke patients would receive daily interventions. Local casemix data reported an Average Length of Stay in Medical Ward Y of 11.3 days. Given that Speech Pathologists do not work on weekends this figure was adjusted to 8 days (Approximately 3.3 therapy free days per admission).
6Basic Community Profile completed by the Australian Bureau of statistics August 7, 2001 Census.

Allied Health Staffing Matrix Discipline Speech PathologyAcute Inpatient Clinical Area: Aged CareNo. of beds 30
TAY/N
Clients presenting with Dysphagi Review of medical file 10or Communication difficultie Initial assessment 30 Supervision (G1 staff) G2 only
- Orientation - Formal once per month 12Dementia / Delirium - Receptive / Expressive language - informal guidance and review of complex cases 10mins per week 8.6
- speech Admin/stats - Voice - 30 mins per day 130
CVA - oromuscular motor assessment (cranial nerves) 'Adults' Meeting once per mont 24 - Airway protection AHED (new graduate) program - Oral trials for swallowing / swallowing techniques - 2hrs per month 24
Other Neuro eg. Parkinsons' Disease Report writing 20 Bi-monthly professional development meetinMND Liaison with staff 5 - 2 hour Inservice 12
Liaison with family 10 Quality ImprovementLiaison with kitchen / nutrition re; diet changes based on swallowing functi 5 - 1-2 hours per month 18Liaison with other agencies eg Nursing Hom 10Family / carer education re: Feeding strategies & safe swallowin 20 Monthly OH& S repor 24
COPD Liaison with medical team re: Quality of life issues / clie 5 Non-clinical travel 90mins per meetingPnuemonia Gathering resources 10 - AHED X6 9
Referral to other disciplines eg. Nutrition, OT, PT, SW 10 - 'Adults' meetings x8 12Meal time review 5 - Professional Development meeting x6 9 - observation of eating, preferable with cognitive impaired &/or geriatric clientsReferral out 5 TOTAL 282.6TOTAL HOURS PER CLIENT 2.42 125.67Family Conference 45TOTAL HOURS PER CLIENT
CVA Standardised assessments of Speech & Languag 90Other Neuro Analysis & report writing 30 Additional requirements senior staff
ADDITIONAL HOURS PER CLIENT 2 26 - Writing agendasTOTAL HOURS PER CLIENT 4.42 - ordering stock / stationery
Severe speech / language difficulties Resource Development 30 - policy development - communication boards, cue cards, individualised, laminat - Portfolio Management ie. QI, PD, OH&S, Health Promotion, PR
in the absence of significant cognitive impairment Education of client / staff / family re use 20 - submissionsReport writing 10 - Business planningADDITIONAL HOURS PER CLIENT 1 - memosTOTAL HOURS PER CLIENT 3.42 - seniors meeting
Dementia Delirium 7 Additional time taken to R/V patient at meal time 20 - project co-ordinationADDITIONAL HOURS PER CLIENT 0.33 2.33TOTAL HOURS PER CLIENT 2.75
Clients requiring therapy Average LOS Daily review and treatmen 45is 11.3 days - preparation for session
- review of medical file8 assumed as - conduct treatment session Leave Coverage CURRENTLY NOT INCLUDED
No weekend speech - liaise with staff / carer A/Leave Coverage (1 FTE = 152 hrs) 152 - report writing S/Leave Coverage (1 FTE =76hrs) 76ADDITIONAL HOURS PER CLIENT 0.75 78 FACS Leave (6 days per 2 years) 24TOTAL HOURS PER CLIENT 3.17
Palliative Care Strategies for swallowing / feeding optionsComfort care / Quality of Life issues / Patient WishesLiaison with family / clientLiaison with medical teamADDITIONAL HOURS PER CLIENT **Caseload specificTOTAL HOURS PER CLIENT Caseload planning (10mins per day ) 43.3
Modified Barium Swallows Liaison with medical imagin 10 Case Conferences 3 per week, 30mins ea 782 Clinics per week preparation of food / fluid 15 Travel to ward - 30mins per day 130
Oromuscular examination and explanation of procedu 52 staff required at all time Procedure conducted - one therapist feeding the other observing & recordin 30 TOTAL 251.3
Discussion re findings 15feedback & recommendations given to clien 15Report dictated for typis 15Written summary entered in medical fi 15
ADDITIONAL HOURS PER CLIENT 2 8 TOTAL CLINICAL GOVERNANCE AND INFRASTRUCTURE HOUR 533.9TOTAL CLINICAL INTERVENTION HOURS 240.00TOTAL CLINICAL INTERVENTION HOURS FOR 12 MONTHS 480TOTAL CASELOAD SPECIFIC INFRASTRUCTURE HOURS 251.3TOTAL CLINICAL INTERVENTION AND CASELOAD SPECIFIC INFRASTRUCTURE HOURS 731.3TOTAL THERAPIST HOURS
Intervention / hours attributable to most clients
Additional interventions / hours specific to client group
Clinical Governance & Infrastructure Requirements Hours per FTE
Please Qualify
Total Interventionhours
52
13
13
4
Intervention time (mins)Diagnostic / Target Group No. of cases
June to Dec Average LOS Clinical Intervention Requirements
Figures tabled are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 4.1 22

Appendix A
23
RESULTS TOTAL CLINICAL INTERVENTION AND CASELOAD SPECIFIC INFRASTRUCTURE HOURS = 731.3 For the service described at its current referral rate this represents a clinical requirement for Medical Ward Y of 0.35 FTE Clinical Governance and Infrastructure requirements would need to be considered and built into each therapists position in the context of full time or part time hours and the division of workload across clinical areas. In this instance the remaining infrastructure hours represent approximately 0.13 of an FTE Once again Leave coverage is not currently built into establishment positions but should be considered for any future enhancement funding.

Appendix A
24
Allied Health Staffing Matrix Example 5 Nutrition & Dietetics - General Medicine Figure 5.1 is one example of a staffing matrix completed for Nutrition & Dietetics in General Medicine Definitions: General Medical Ward For the purpose of this project a ‘General Medical Ward’ is defined as an acute medical ward which may provide limited specialist services but generally will expect to see any number and combination of medical diagnoses subject to local demographics and disease prevalence. Clinical Area Description: This particular Nutrition Department provides a service across inpatients and outpatients within a 274 bed metropolitan hospital. There are no designated clinician hours for this 30 bed medical ward. Referral rates and professional prioritisation determine time spent in one particular ward location. Nutrition assistants work 5am to 6pm 7 days per week and are responsible for the following:- - Screening all inpatients for malnutrition during menu collection. A validated screening tool is used and clients are prioritized based on a total score between 1 and 6. Dietician intervention is indicated if the score is greater than 3. - Monitoring and review of basis diet needs - Monitoring and review as requested by a Dietician - Data entry Prioritization of referrals occurs through liaison with assistant and ward staff. In addition Dieticians will check diagnoses etc during Board round meetings.

Allied Health Staffing Matrix Discipline NutritionAcute Inpatient Clinical Area: General MedicalNo. of beds 30
All inpatients Screening for malnutrition Y Currently screen all inpatients during menu collectionReview of Medical file 15 validated screening toolReview of Pathology 5 prioritisation based on scoreInitial Assessment 20 - Talking to patient / family Monitoring and review of basic diet needs - diet history, intake, weight history, medical history Monitoring & review as requested by Dietician
Oral nutrition Support - factors effecting intake Data entry - Biochemistry - nausea & vomitting / bowels Admin/stats 130
Enteral & - energy & protein requirements - 30 mins per dayParenteral Nutrition Suppo Case Planning / Management 10 Non Clinical Travel 104
- discussion with nursing staff, team, nutrition assistant - 2 hours per weekDocumentation Dept Inservice 12 - Medical notes & inpatient card 20 - 1 hour per month - Hard copy 5 Clinical Team Meetings 52Monitoring / review 10 Y - weeklyEducation for Discharge 15 New Graduate Inservice program 'AHED' - May include Patient / carer / Nursing Home / Institution - 2 hours per month 24Handover / Referral out 5 Inservices / Education
- 2 hours per month 2412 TOTAL HOURS PER CLIENT 1.75 21.00 OH&S safety audits
Oral nutrition Support Initial Assessment 10 - 30 mins per month 130Documentation 10 Quality Improvement Projectsmonitoring / review 20mins x2 per week 40 - 2 hours per week 104Education for Discharge 5 TOTAL 580ADDITIONAL HOURS PER CLIENT 1.08
100 TOTAL HOURS PER CLIENT 2.83 283.33Enteral & Case Planning / Management 10 *Caseload Specific InfrastructureParenteral Nutrition Suppo - discussion with nursing staff, team, nutrition assistant Board round meetings / case conferences
Equipment prescription / ordering 5 - 1.5 to 2 hours per week 91Monitoring & review 20mins daily 158 TOTAL 91Education for Discharge - May include Patient / carer / Nursing Home / Institution 30Handover to HENS, Nusing Home 20ADDITIONAL HOURS PER CLIENT 3.72
10 TOTAL HOURS PER CLIENT 5.47 54.67Renal Disease Initial assessment 10
monitoring /review 10Education for Discharge 5ADDITIONAL HOURS PER CLIENT 0.42TOTAL HOURS PER CLIENT 2.17
Newly Diagnosed IDDM o Review of Pathology 5commencing insulin
ADDITIONAL HOURS PER CLIENT 0.08TOTAL HOURS PER CLIENT 1.83 Leave Coverage CURRENTLY NOT INCLUDED
Eating Disorders Review of Medical file -5 A/Leave Coverage (1 FTE = 152 hrs) 152Handover/ referral out eg. eating disorder units 15 S/Leave Coverage (1 FTE =76hrs) 76ADDITIONAL HOURS PER CLIENT 0.17 FACS Leave (6 days per 2 years) 24TOTAL HOURS PER CLIENT 1.92 TOTAL 252
Coeliac Disease Initial Assessment -5Education for discharge 5Documentation -5ADDITIONAL HOURS PER CLIENT -0.08TOTAL HOURS PER CLIENT 1.67 24.67
Interventions / hours attributable to most clients
Hours per FTEAverage
LOS
Additional interventions / hours specific to client group
10 7.9
100
Diagnostic / Target client groups
No. of cases per year
12 7.9
7.9
Clinical Governance & Infrastructure RequirementsPlease QualifyTA (Y/N)
13
Average therapeutic intervention time =
1.8975
Clinical Intervention requirements Intervention time (mins)
Total Intervention time
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 5.1 25

Allied Health Staffing Matrix Discipline NutritionAcute Inpatient Clinical Area: General Medical (Continued)No. of beds 30
Diagnostic Average No. of Intervention requirements TA Please Qualify Clinical Governance & Infrastructure Group cases per year Including non face to face Y/N Hours per FTENewly diagnosed NIDDM / High cholesterol review of medical file 10
Interview / education / provision of resources 10Documentation 15TOTAL HOURS PER CLIENT 0.58
Allergies Review medical file 10Interview 10Documentation 10(Medical notes +/- inpatient cardHardcopy 5TOTAL HOURS PER CLIENT 0.58
Weight reduction Interview / Provision of written resources 10Documentation 5
TOTAL HOURS PER CLIENT 0.25 TOTAL 580TOTAL CLINICAL INTERVENTION HOURS 383.67TOTAL CLINICAL INTERVENTION HOURS FOR 12 MONTHS INCLUDING CASELOAD SPECIFIC INFRASTRUCTURE HOURS 858.34TOTAL GOVERNANCE AND INFRASTRUCTURE HOURS PER FTE EXCLUDING CASELOAD SPECIFIC 580TOTAL CLINICAL GOVERNANCE AND INFRASTRUCTURE HOURS FOR MEDICAL WARD X 232
Hours per FTE
Other brief interventions
Average LOS
Intervention time (mins)
Figures presented are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 5.1 25

Appendix A
26
Data Review 135 clients were seen by Nutrition in this particular medical ward over a 6 month period. Of these 12 required assessment only, 100 were seen for Oral Nutrition support, 10 for Total Parenteral Nutrition Support and 13 for Therapeutic Interventions ie. Renal Disease, Newly Diagnosed IDDM / NIDDM, Eating Disorders, Coeliac Disease. No data was available for the Other Brief Interventions listed however these were thought to have been included in the assessment only group. According to local Casemix data the mean Length of Stay for the unit was 7.9 days. Intervention times were multiplied by this figure where daily interventions were indicated. Intervention hours were averaged for the 4 target groups included in the Therapeutic intervention category. Total clinical Intervention Hours for the 6 month period = 383.67 hours This figure was multiplied by 2 in order to estimate hours for a 12 month period ie. 767.34 hours. Caseload specific intervention hours were also added to this figure in order to include all intervention hours specific to the medical ward caseload. RESULTS: Total Clinical Intervention Hours for 12 months including Caseload Specific Infrastructure hours = 858.34. This represents approximately 0.4 FTE (858.34 divided by 2080) Clinical Governance and Infrastructure Hours would need to be reviewed by the service manager with regard to full time or part time staffing needs. The figures presented represent requirements for one Full Time Equivalent. In reality these hours are shared across a number of clinical units. If Total therapist hours were to be calculated for this ward (assuming that the staff member works full time) we could mathematically assume that this staff member would require at least 0.4 times the clinical governance and infrastructure hours listed ie. 232 hours or 0.1 FTE. In this instance the estimated FTE requirement for this medical ward independent of any others would be 0.5FTE

Appendix A
27
Allied Health Staffing Matrix Example 6 Psychology – General Medicine, Aged Care, Orthopaedics and Outpatients Figure 6.1 is one example of a staffing matrix completed for Psychology for General Medicine, Aged Care and Orthopaedic Inpatients as well as Outpatients. Definitions: Clinical Neuropsychological assessments - Assessments performed by Clinical Neuropsychologists (minimum of 6 year degree plus additional post graduate supervision) - Involve interviewing, the formulation of diagnostic hypotheses and the administration of standardised tests of cognitive, behavioural and
emotional function. - Additional information about the patients function is obtained from external sources and from skilled (trained) observation of the patients
presentation. - Neuropsychological assessments assist the diagnostic process and, where appropriate, the formulation and execution of appropriate
treatments, including psychological treatment and behavioural management and cognitive rehabilitation. Clinical Area Description: At this particular site Neuropsychology services are provided to a 274 bed Metropolitan Hospital in an area which has a significant and increasing elderly population (approximately 18% over the age of 65).7 A Consultancy based service is provided across all clinical areas and divisions. Patients over 60 constitute the majority of referrals Staff attend to the inpatient areas of General Medicine, Aged Care and Orthopaedics on a referral basis. Outpatient services are provided by the same inpatient staff. Leave coverage is provided as able by existing staff within the Psychology department. Inpatients are generally given priority over outpatient clients Waiting lists exist for both inpatient and outpatient clients with numbers tending to fluctuate from month to month. At the time of this report there were 12 outpatient clients awaiting assessment and the waiting period for assessment on the acute wards was 2 weeks. Length of Stay does not impact on clinical intervention hours but does drive the prioritisation process. Statistical recording for this service is paper generated and relates primarily to number of referrals and OOS.
7Basic Community Profile completed by the Australian Bureau of statistics August 7, 2001 Census.

Allied Health Staffing Matrix Discipline Psychology - NeuropsychologyAcute Inpatient Clinical Area Acute Inpatient wards including General Medicine, Aged Care and Orthopaedi
TA Please QualifyY/N
Patients with known or suspected Review of medical records 0.5 -1hr 0.75 NB. No part of the neuropsychological Undergo professionaCognitive Disorder 50 Discussion / Liaison with treating team member 0.5 - 2hrs 1.25 assessment proper (file review, interview, supervision, includingdue to neurological, other medical re their observations / impressions of the patients hypothesis formulation, test selection, test supervision of complianceor psychiatric disorder cognitive, behavioural and emotional status administration, results interpretation, or with evidence-based practice
**Neuro psychological examinatio 2 - 5 hours 3.5 report writing) can be done by a technica - 2 hours per month 24Priority is given to cases that require Scoring of test data 1 hour 1 assistant. Provide cover for twoneuropsychological evaluation to assist Report Writing 1 - 3 hours 2 neuropsychologists based awith immediate medical management Clerical tasks 1-2 hours 1.5 Y Clerical assistant another hospital sitedecisions, such as diagnosis. - report typing - 5 hours per month 60Second priority given to those - filing Supervision of Internrequiring assessment for non-immediate - mailing Neuropsychologistscare, e.g. discharge planning and Interview of significant others, when availabl 0.5 - 1 hour 0.75 - 10 hours per month 120Guardianship Tribunal Applications - re patients premorbid and current cognitive , behavioural and emotional status Attendance at departmenta
Post assessment liaison with treating team meetings and professiona - re treatment management recommendations development activities,eg.Advice regarding behavioural management including travel time Advice about Guardianship - 6 hours per month 72 Recommendation for other consultant involvement eg. neurology , psychology
50 TOTAL HOURS PER CLIENT 10.75 537.5Guardianship Tribunal Hearings 0 Phone interview or attendance at Guardianship Tribunal Hearings 0.25 - 1.5 ho 0.88
re applications for a Guardian &/or Financial Manager
ADDITIONAL HOURS PER CLIENT 0.88TOTAL HOURS PER CLIENT 11.63 0
Intervention time (hrs) Hours per yearAssumed
Average (hours) Total Intervention
HoursClinical Governance & Infrastructure
RequirementsTargeted Client Group No. of clients seen over 12 month period Clinical Intervention requirementsAverage
LOS
Intervention / hours attributable to most clients
Additional
interventions / hours specific to client group
Figures presented are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 6.1 28

Allied Health Staffing Matrix Psychology - NeuropsychologyOutpatients - Hospital Based
TA Please Qualify
Y/NArrangement of appointment by phone 0.5 hours 0.5 Y Could be done by a clerical assistan No additional hours are typing and sending of formal appointment letter required on top of those
Patients with known or suspected 50 Review of medical records 0.5 -1hr 0.75 NB. No part of the neuropsychological listed on the previousCognitive Disorder Discussion / Liaison with treating team member 0.5 - 2hrs 1.25 assessment proper (file review, interview, page - for inpatient workdue to neurological, other medical re their observations / impressions of the patients hypothesis formulation, test selection, or psychiatric disorder cognitive, behavioural and emotional status test administration, results interpretation
**Neuro psychological examinatio 2 - 5 hours 3.5 or report writing)can be done by a technicaPriority given to cases that require Scoring of test data 1 hour 1 assistantneuropsychological evaluation to assist Report Writing 1 - 3 hours 2with immediate medical management Clerical tasks 1-2 hours 1.5 Y Could be done by a Clerical assistandecisions, such as diagnosis. - report typingSecond priority given to those - filingrequiring assessment for non-immediate - mailingcare ie. Discharge planning and Interview of significant others, when availabl 0.5 - 1 hour 0.75Guardianship Tribunal Applications - re patients premorbid and current cognitive , behavioural and emotional status
Post assessment liaison with treating team - re treatment management recommendationseg.Advice regarding behavioural management Leave Coverage CURRENTLY NOT INCLUDED Advice about Guardianship A/Leave Coverage (1 FTE = 152 hrs) 152 Recommendation for other consultant involvement eg. neurology , psychology S/Leave Coverage (1 FTE =76hrs) 76
FACS Leave (6 days per 2 years) 24TOTAL HOURS PER CLIENT 11.25 562.5 TOTAL 252
Guardianship Tribunal Hearings 5 Phone interview or attendance at Guardianship Tribunal Hearings 0.25 - 1.5 ho 0.88re applications for a Guardian &/or Financial Manager
ADDITIONAL HOURS PER CLIENT 0.88TOTAL HOURS PER CLIENT 12.13 60.65
Cardiac Rehabilitation Group Education 1 hour Lecture provided on the psychological consequences of heart disease 4 43-4 times per year and infarction
Number of sessions 4 TOTAL SESSION HOURS 4 4 TOTAL 276TOTAL CLINICAL INTERVENTION HOURS 1164.65TOTAL INFRASTRUCTURE HOURS 276TOTAL CLINICIAN HOURS 1440.65
DisciplineAcute Inpatient Clinical Area
Average LOS
Intervention time (hrs) Hours per yearAssumed
Average (hours)
No. of clients seen over 12 month period
Total Intervention HoursTargeted Client Group Clinical Governance & Infrastructure
RequirementsClinical Intervention requirements
Other
interventionsIntevention / hours attributable to m
ost clientsA
dditional interventions specific to client group
Figures presented are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 6.1 28

Appendix A
29
RESULTS The results would appear to indicate that approximately 0.69 FTE of a Neuropsychologist would be sufficient to provide the service described to 50 inpatients / 50 outpatients and 4 group education sessions per year ( FTE conversion: 1440.65 divided by 2080 = 0.69). Ironically this service is currently staffed by 0.6FTE Neuropsychologist. Waiting lists and referral rates would need to be monitored to determine additional staffing needs. Staff interviewed report that actual clinical governance and infrastructure hours may decrease with increasing clinical workload. Meetings will tend to be given lower priority than acute inpatient needs. Leave coverage is again not factored into current staffing establishment but should be considered for any enhancement positions. The hours described do not allow for additional professional development / research activities required to attain seniority within the Psychology profession.

Appendix A
30
Allied Health Staffing Matrix Example 7 Podiatry - Outpatients Figure 7.1 is one example of a staffing matrix completed for Podiatry Outpatients Clinical Area Description: The Podiatry service in this example is predominantly Outpatient based. Currently 5.6 FTE provide an Area wide service which incorporates 4 hospital sites and 2 health centres. The Podiatry office and equipment is centralised at one Hospital site. Staff travel 4 times per week to this Metropolitan Hospital to attend Outpatient Clinics which operate from 9am to 3pm. Staff enter statistical information into AHMIS on a daily basis. The recruitment of Podiatry staff has been a long-term problem. Data Analysis This particular Podiatry department had only been inputting statistics into AHMIS for 6 months prior to this project. Data for the first 2 months of this period was inadequate due to the fact that staff were still familiarising themselves with the database. For this reason only 4 months worth of AHMIS data was reviewed and the figures extrapolated over a 12 month period. From September to December 467 clients were seen for Initial Assessment and general palliative care, 269 for diabetic Review, 76 for Ulcer Care, 21 for Diabetic acute injuries. 38 clients attended 2 Diabetic Education sessions. Based upon clinician estimated figures for the interventions described Total Clinical Intervention Hours = 621.45. This figure was multiplied by 3 to obtain Estimated Clinical Intervention Hours for 12 months = 1864.35 Total Clinical Governance and Infrastructure hours = 468.66. NB. 242.66 of these hours are required for travel to the site to provide the service described. Student supervision hours have not been stipulated and the AHED program is only applicable to new graduates. RESULTS Total Podiatrist Hours = 2333.01 hours FTE Conversion: 2333.01 divided by 2080 = 1.1 FTE These figures would appear to indicate that 1.1 FTE of a Podiatrist would be sufficient to provide the service described. Note: Leave coverage has not been factored into the Clinical Governance and Infrastructure total as currently there is no financial
arrangement for leave coverage.

Allied Health Staffing Matrix Discipline PodiatryClinical Area Outpatients
TA Please QualifyY/N
Diabetic clients with Pensioner or Initial Assessment including Departmental meetings 1.5 hours per mont 60Health Care Card entitlements General Palliative care 20 N Inservice 1 hour per month 12Paediatric Diabetes - Nailcare, corn and calllous debriding Student 4-5 weeks per yearAny person with a foot ulcer Biomechanical assessment ( quick review 10 N Ahed programme 2 hours per month (new grads 24
Further referral 10 NGeneral Paliative Care - eg. booking for possible orthotic therapy or nail surgery
report writing 5 NY Training and supervision Stats 30mins per day 130
TOTAL HOURS PER CLIENT 0.75 350.25Diabetic Reviews Sensation testing 10 N
Circulation testing 10 NDiabetic foot education 10 Y Training approved by Diabetes centreReply letters to GP's etc 10 NADDITIONAL HOURS PER CLIENT 0.67 179.33
Ulcer Care Assessment and treatment plan 15 N- Assess wound causes ** Caseload specific - Determine suitable dressing Clinical trave - Pressure 'off loading' requirements - 70mins 4 times per week 242.66digital photography 2 Yredressing 5 NProvide pressure off - loading device 30 Y Training approved by Diabetes centrereport writing 5 NReply letters to GP's etc 10 NADDITIONAL HOURS PER CLIENT 1.12 84.87 Leave Coverage
Foot in crisis' care Assess and Phone Registrar for review re: hospitalisatio 60 N A/Leave Coverage (1 FTE = 152 hrs) 152for infected foot wound S/Leave Coverage (1 FTE =76hrs) 76ADDITIONAL HOURS PER CLIENT 1 FACS Leave (6 days per 2 years) 24
Paediatric Diabetes Full biomechanical assessmen 25 NPaediatric sensation / circulation testin 25 NADDITIONAL HOURS PER CLIENT 0.83
Diabetic acute injury 21 Debridement and dressing 20 NADDITIONAL HOURS PER CLIENT 0.33 7
Injury sports strapping for injur 10 NADDITIONAL HOURS PER CLIENT 0.17
Outpatient Groups Attendances No. of sessionsDiabetes Education Groups Group education session 60for newly diagnosed - 60 minutes per session
Travel to Health centres / hospitals
TOTAL GROUP SESSION HOURS 1 2 TOTAL 468.66TOTAL CLINICAL INTERVENTION HOURS 621.45TOTAL CLINICAL INTERVENTION HOURS FOR 12 MONTHS 1864.35TOTAL CLINICAL GOVERNANCE AND INFRASTRUCTURE HOURS 468.66TOTAL PODIATRIST HOURS 2333.01
Hours per FTEClinical Intervention requirements
Intervention / hours atributable to m
ost clients
No. of Cases Sept to DecDiagnostic / Target Client Groups Clinical Governance & Infrastructure RequirementsIntervention
time (mins)total Intervention
hours
Other
outpatient in terventions
38 2
467
269
76
Additional interventions / hours specific to client
group
Figures presented are representative ONLY of current practise, in each Metropolitan Hospital locality, as reported by clinicians at the time of data collection.This project does not attempt to make any statement of what is adequate or appropriate with regard to staffing levels nor suggest that the intervention requirements listed represent Best Practise.
Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise.
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. Figure 7.1 31

Appendix A
32
CONCLUSION It must be emphasized again that the staffing figures produced should not be generalised across all areas due to the enormous variability between clinical units and the populations they service. Apart from site specific statistical data all clinical intervention hours are estimates only based on the experience of the staff currently working within these services. Validation of the data collated can only occur through the management and application of accurate statistical databases, a commitment to Evidence Based Practise, and an acknowledgement of the variety of practice models within disciplines. There can never be an exact number for total clinician hours. - In reality staff may take more or less leave depending on individual leave balances. (Additional leave entitlements such as Long Service and
Study leave have not been accounted for). - In practice Clinical interventions generally take priority over Clinical Governance and Infrastructure requirements. In the presence of a
heavy clinical workload meetings/ supervision / statistical reporting etc will often be placed on hold. - Not all clients referred to Allied Health clinicians will receive the recommended or expected interventions. In the context of a hospital
system patients may be transferred, deteriorate medically, die, or be discharged before the clinician gets to see them. Clients may also decline to receive any interventions.
Our estimations can be improved upon. We have the ability to not only be more accurate with our estimations but also to be better able to define what level of service we can provide for a dollar value and at what point a service is no longer safe nor viable. Significantly more work needs to be done to truly analyse data obtained during this project to validate interventions and time estimates with each individual profession. The concept of Best Practise is in itself provocative. To date Best Practise has represented the ideal, that which we must all strive to provide. As the current workforce crisis looms it may increasingly mean that we do the very best with the resources available to us. A significant Paradigm shift will need to occur if we are to openly address workforce issues and investigate all options. The business of accountancy may win over best practise ideals but this is a choice that administrators must make. Allied Health can only strive to better educate and inform those who make these decisions and to be creative in their approach to staffing mix and role delineation. Let us define what is feasible; what is safe for our clients and our staff; what is sustainable.

Appendix B
Appendix B Intervention Comparisons
Nutrition Occupational Therapy Physiotherapy Podiatry Psychology Social Work Speech Pathology

Intervention ComparisonsDiscipline NutritionAcute Inpatient Clinical Area: General Medical / Aged Care / Orthopaedics
All inpatients Screening for malnutrition T/A 5 Y Currently screen all inpatients during menu collectionReview of Medical file 15 15 15 15 15 validated screening toolReview of Pathology 5 5 5 prioritisation based on scoreInitial Assessment 20 20 20 20 25 45 - Talking to patient / family Monitoring and review of basic diet needs - diet history, intake, weight history, medical history Monitoring & review as requested by Dietician
Oral nutrition Support - factors effecting intake Data entry - Biochemistry 5 - nausea & vomitting / bowels
Enteral & - energy & protein requirementsParenteral Nutrition Support Case Planning / Management 10 10 10 15 15 15
- discussion with nursing staff, team, nutrition assistantDocumentation - Medical notes & inpatient card 20 20 - Medical notes 20 10 - Hard copy / department files 5 - Including CBORD ordering Y - Multidisciplinary patient management plan 5 - Medical notes and CBORD 15Monitoring / review 10 10 Y Information Management - 1 -2 per admission 10 - Frequency depends on diagnosis / intervention - 20mins 1-2 times per week 20Monitoring / review plus documentation 15 Unsupervised , after specific trainingMonitoring / review may be daily initially 5 Ythen (2-3 per week ) after nutrition support established5 minutes dailyCheck Biochem on computer 5Adjust CBORD entries, manipulate data to ensure adequate nutrition 15 5Calculate nutrition intake 30 Y With appropriate training
& computer useEducation for Discharge 15 15 15 20 40 30 - May include Patient / carer / Nursing Home / Institution - Follow up 20Handover / Referral out 5 5 5 10
TOTAL HOURS PER CLIENTInterpreter required Use of interpreter to complete above 40
ADDITIONAL HOURS PER CLIENTOral nutrition Support Initial Assessment 10 10 10
Documentation 10 10 10monitoring / review x2 per week 20 20 20Education for Discharge 5 5 5Med Pass programme 5 - Liaise with medical team to have 'TwoCalHN 60mls qid written into medical chart'ADDITIONAL HOURS PER CLIENT
Dysphagia Liaison with Speech Pathologist re: texture and consistency of food & fluids 5Daily monitoring of intake including food charts 5ADDITIONAL HOURS PER CLIENT
Please Qualify
25
F A B C D
Intervention time (mins) Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements A B C* D
Interventions / hours attributable to most clients
E**
15
Additional interventions / hours
specific to client group
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1
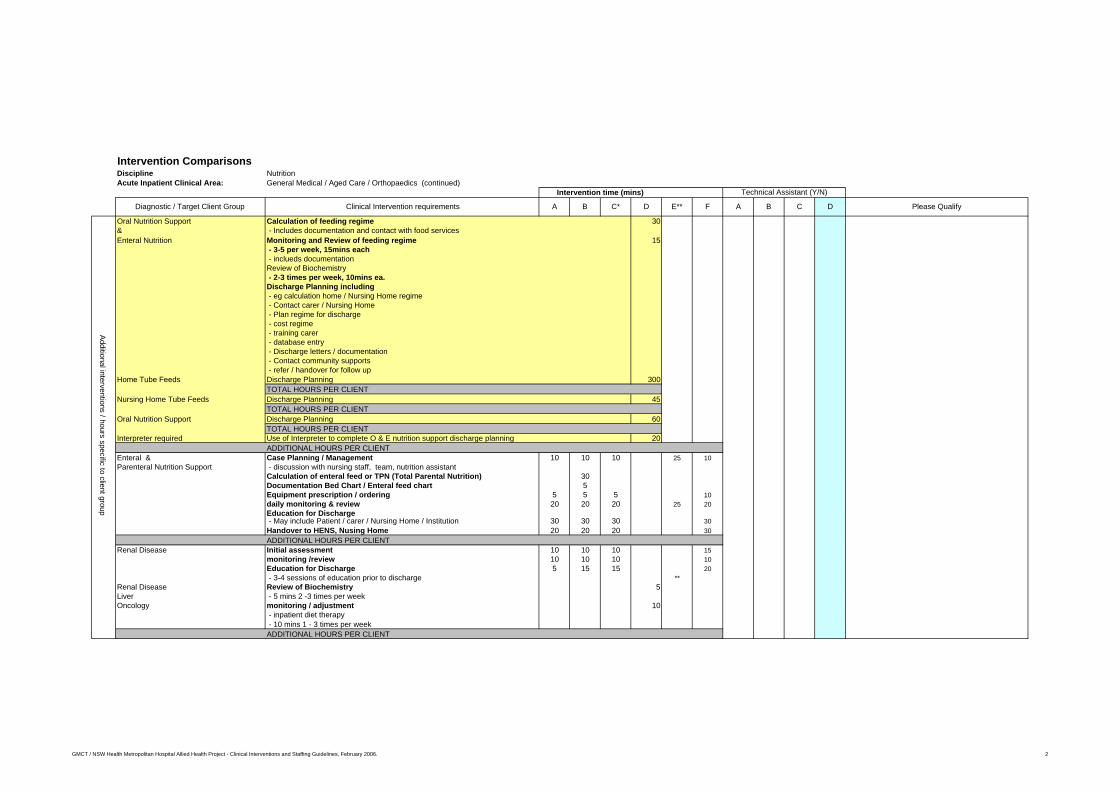
Intervention ComparisonsDiscipline NutritionAcute Inpatient Clinical Area: General Medical / Aged Care / Orthopaedics (continued)
Oral Nutrition Support Calculation of feeding regime 30& - Includes documentation and contact with food servicesEnteral Nutrition Monitoring and Review of feeding regime 15
- 3-5 per week, 15mins each - inclueds documentationReview of Biochemistry - 2-3 times per week, 10mins ea.Discharge Planning including - eg calculation home / Nursing Home regime - Contact carer / Nursing Home - Plan regime for discharge - cost regime - training carer - database entry - Discharge letters / documentation - Contact community supports - refer / handover for follow up
Home Tube Feeds Discharge Planning 300TOTAL HOURS PER CLIENT
Nursing Home Tube Feeds Discharge Planning 45TOTAL HOURS PER CLIENT
Oral Nutrition Support Discharge Planning 60TOTAL HOURS PER CLIENT
Interpreter required Use of Interpreter to complete O & E nutrition support discharge planning 20ADDITIONAL HOURS PER CLIENT
Enteral & Case Planning / Management 10 10 10 25 10Parenteral Nutrition Support - discussion with nursing staff, team, nutrition assistant
Calculation of enteral feed or TPN (Total Parental Nutrition) 30Documentation Bed Chart / Enteral feed chart 5Equipment prescription / ordering 5 5 5 10daily monitoring & review 20 20 20 25 20Education for Discharge - May include Patient / carer / Nursing Home / Institution 30 30 30 30Handover to HENS, Nusing Home 20 20 20 30ADDITIONAL HOURS PER CLIENT
Renal Disease Initial assessment 10 10 10 15monitoring /review 10 10 10 10Education for Discharge 5 15 15 20 - 3-4 sessions of education prior to discharge **
Renal Disease Review of Biochemistry 5Liver - 5 mins 2 -3 times per weekOncology monitoring / adjustment 10
- inpatient diet therapy - 10 mins 1 - 3 times per weekADDITIONAL HOURS PER CLIENT
A
Technical Assistant (Y/N)
Additional interventions / hours specific to client group
E**
Intervention time (mins)
Diagnostic / Target Client Group Clinical Intervention requirements A B C* D F B C D Please Qualify
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline NutritionAcute Inpatient Clinical Area: General Medical / Aged Care / Orthopaedics (continued)
Newly Diagnosed IDDM or NIDDM Review of Pathology 5 5 5Education of patient &/or relatives 60 5 10 NUse of interpreter to complete Education 20Referral to diabetes education programme 5 - 3-4 sessions of education prior to discharge** **Additional education over 2-3 sessions 20mins each 60Documentation 10 - 15 mins per session 10
ADDITIONAL HOURS PER CLIENTEating Disorders Review of Medical file -5 -5 -5
Handover/ referral out eg. eating disorder units 15 15 15ADDITIONAL HOURS PER CLIENT
Coeliac Disease Initial Assessment -5 -5 -5Education for discharge 5 5 15Documentation -5 -5 -5ADDITIONAL HOURS PER CLIENT
Newly diagnosed NIDDM / High cholesterol review of medical file 10 10 10Interview / education / provision of resources 10 10 20Documentation 15 15 15TOTAL HOURS PER CLIENT
Allergies Review medical file 10 10 10Interview 10 10 10 10
*Few seen, usually Documentation 10 10 10 10food intolerances (Medical notes +/- inpatient card
Hardcopy 5 5 5TOTAL HOURS PER CLIENT
Weight reduction Interview / Provision of written resources 10 10 10 10Documentation 5 5 5 5TOTAL HOURS PER CLIENT
Pancreatitis Education 15Cholecystitis Documentation 10Bowel resections +/- Formation of Stomas
TOTAL HOURS PER CLIENT
Interventions omitted from template or not performed by a service
Interventions reported by only one particular service
Other brief interventions
15
Intervention time (mins)
Please Qualify
Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements A B C* D E** F
Additional interventions / hours specific to
client group
B C DA
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 3
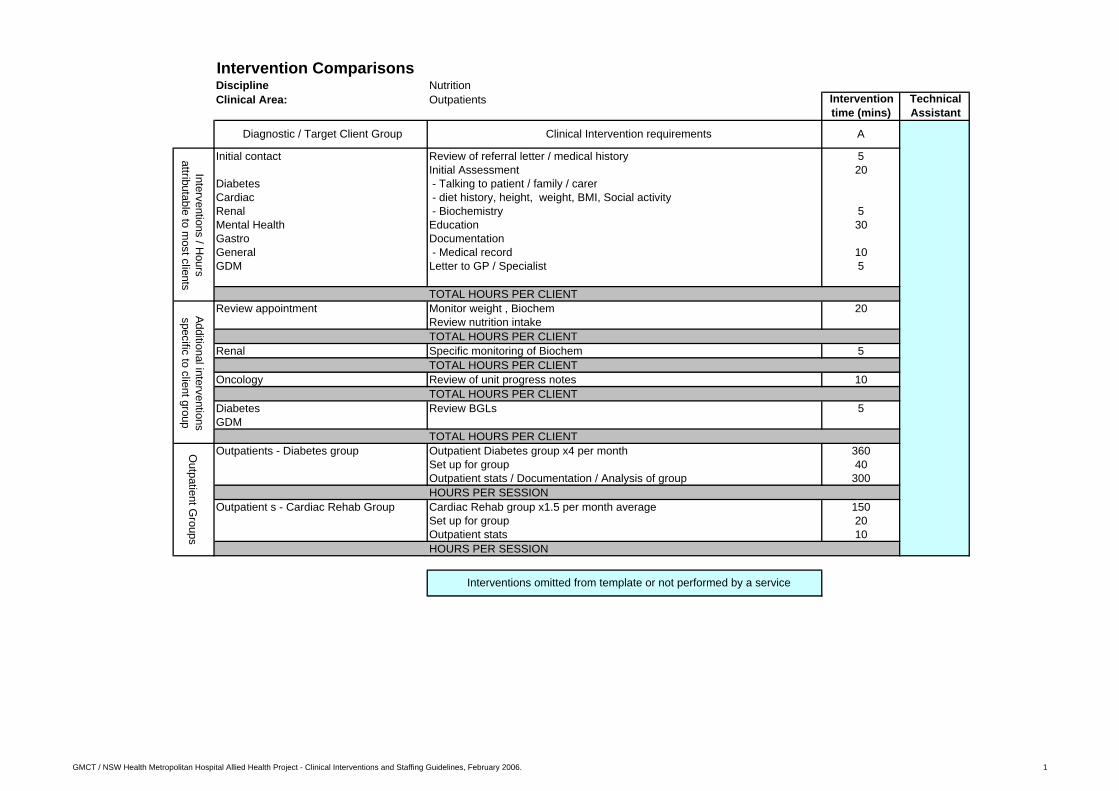
Intervention ComparisonsDiscipline NutritionClinical Area: Outpatients
Initial contact Review of referral letter / medical history 5Initial Assessment 20
Diabetes - Talking to patient / family / carerCardiac - diet history, height, weight, BMI, Social activityRenal - Biochemistry 5Mental Health Education 30Gastro DocumentationGeneral - Medical record 10GDM Letter to GP / Specialist 5
TOTAL HOURS PER CLIENTReview appointment Monitor weight , Biochem 20
Review nutrition intakeTOTAL HOURS PER CLIENT
Renal Specific monitoring of Biochem 5TOTAL HOURS PER CLIENT
Oncology Review of unit progress notes 10TOTAL HOURS PER CLIENT
Diabetes Review BGLs 5GDM
TOTAL HOURS PER CLIENTOutpatients - Diabetes group Outpatient Diabetes group x4 per month 360
Set up for group 40Outpatient stats / Documentation / Analysis of group 300HOURS PER SESSION
Outpatient s - Cardiac Rehab Group Cardiac Rehab group x1.5 per month average 150Set up for group 20Outpatient stats 10HOURS PER SESSION
Technical Assistant
Diagnostic / Target Client Group Clinical Intervention requirements A
Intervention time (mins)
Outpatient G
roupsAdditional interventions specific to client group
Interventions / Hours
attributable to most clients
Interventions omitted from template or not performed by a service
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline NutritionAcute Inpatient Clinical Area ICU
Referral driven Review of Medical file 20 15Nil by mouth patients Review of Pathology 5 - ventilated Initial Assessmen 25 20 - post operative - Talking to patient / family Enteral nutrition mostly TPN - diet history, intake, weight history, medical history
- factors effecting intake - Biochemistry 5
Oral nutrition Support - nausea & vomitting / bowelsEnteral & - energy & protein requirementsParenteral Nutrition Support Documentation of initial assessmen 30
- Medical notes 10 - CBORD ordering 5 Y Information Management - Department files UnsupervisedCalculation of Regimen 15 Following specific trainingDocumentation 5Case Planning / Management 10 15 - discussion with nursing staff, team, nutrition assistantDaily Monitoring / review 20mins + 10 mins documentatio 30 - May require more time if recalculation of needs requiredEducation for Discharge 15 20 - May include Patient / carer / Nursing Home / InstitutionHandover / Referral out 5TOTAL HOURS PER CLIENT
Oral nutrition Support Initial Assessmen 5Documentation 10monitoring / review x2 per week 20Education for Discharge 5TOTAL HOURS PER CLIENT
Enteral & Case Planning / Management 10 10Parenteral Nutrition Support - discussion with nursing staff, team, nutrition assistant
Calculation of enteral feed or Total Parental Nutritio 30Documentation Bed Chart / Enteral feed char 5Equipment prescription / orderin 5 5Daily Monitoring / review 20Education for Discharge 30 30 - May include Patient / carer / Nursing Home / InstitutionHandover to HENS, Nusing Home 20 20TOTAL HOURS PER CLIENT
Oral Nutrition Support Calculation of feeding regim 30& - Includes documentation and contact with food servicesEnteral Nutrition Monitoring and Review of feeding regim 15
- 3-5 per week, 15mins each - inclueds documentationReview of Biochemistry- 2-3 times per week, 10mins eaDischarge Planning includin - eg calculation home / Nursing Home regime - Contact carer / Nursing Home - Plan regime for discharge - cost regime - training carer - database entry - Discharge letters / documentation - Contact community supports - refer / handover for follow up
Home Tube Feeds Discharge Planning 300TOTAL HOURS PER CLIENT
Nursing Home Tube Feeds Discharge Planning 45TOTAL HOURS PER CLIENT
Oral Nutrition Support Discharge Planning 60TOTAL HOURS PER CLIENT
Interpreter required Use of Interpreter to complete O & E nutrition support discharge planning 20TOTAL HOURS PER CLIENT
Renal Disease Review of Biochemistry 5Liver - 5 mins 2 -3 times per weekOncology monitoring / adjustmen 10
- inpatient diet therapy - 10 mins 1 - 3 times per weekTOTAL HOURS PER CLIENT
Newly Diagnosed IDDM or NIDDM Education for discharge 5Interpreter required Use of interpreter to complete education 20
TOTAL HOURS PER CLIENT
Diagnostic / Target Client Group Clinical Intervention requirements B B
Additional interventions / hours specific to client group
Intervention hours attributable to most clients
Interventions reported by only oneparticular service
Interventions omitted from template or not performed by a service
Please Qualify
Technical Assistant(Y/N)
CC
Intervention time (mins)
AA
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline NutritionAcute Inpatient Clinical Area: Paediatrics
Referral drivenPriorities: Review of Medical file 15 15 - Newly diagnosed IDDM Review of Pathology 5 - food allergy Initial Assessment 20 20 - Failure to thrive - Talking to patient / family - eating disorders - diet history, intake, weight history, medical history
- factors effecting intake - Biochemistry 5 - nausea & vomitting / bowels - energy & protein requirementsCase Planning / Management 10 15
Oral nutrition Support - discussion with nursing staff, team, nutrition assistantDocumentation of initial assessment 25 - Medical notes 10 - CBORD ordering 5 Y Information Management
Enteral & - Department files unsupervisedParenteral Nutrition Support Monitoring / review + 5 mins documentation 15 Following specific training
Education for Discharge 15 20 - May include Patient / carer / Nursing Home / InstitutionHandover / Referral out 5
TOTAL HOURS PER CLIENTOral nutrition Support Initial Assessment 10
Documentation 10monitoring / review x2 per week 20Education for Discharge 5ADDITIONAL HOURS PER CLIENT
Enteral & Case Planning / Management 10Parenteral Nutrition Support - discussion with nursing staff, team, nutrition assistant
Equipment prescription / ordering 5daily monitoring & review 20Education for Discharge - May include Patient / carer / Nursing Home / Institution 30Handover to HENS, Nusing Home 20ADDITIONAL HOURS PER CLIENT
Oral Nutrition Support Calculation of feeding regime 30& - Includes documentation and contact with food servicesEnteral Nutrition Monitoring and Review of feeding regime 15
- 3-5 per week, 15mins each - inclueds documentationReview of Biochemistry - 2-3 times per week, 10mins ea.Discharge Planning including - eg calculation home / Nursing Home regime - Contact carer / Nursing Home - Plan regime for discharge - cost regime - training carer - database entry - Discharge letters / documentation - Contact community supports - refer / handover for follow up
Home Tube Feeds Discharge Planning 300TOTAL HOURS PER CLIENT
Nursing Home Tube Feeds Discharge Planning 45TOTAL HOURS PER CLIENT
Oral Nutrition Support Discharge Planning 60TOTAL HOURS PER CLIENT
Interpreter required Use of Interpreter to complete O & E nutrition support discharge planning 20ADDITIONAL HOURS PER CLIENT
B Please QualifyDiagnostic / Target Client Group Clinical Intervention requirements A B A
Additional interventions / hours specific to client group
Intervention time (mins)
Technical Assistant (Y/N)
Interventions / hours attributable to most clients
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline NutritionAcute Inpatient Clinical Area: Paediatrics (continued)
Renal Disease Initial assessment 10Review of Biochemistry 5monitoring /review 10 10Education for Discharge 5ADDITIONAL HOURS PER CLIENT
Newly Diagnosed IDDM or NIDDM Review of Pathology 5commencing insulin Up to 4 reviews with education provided - per session 30
Documentation - per session 10Education for Discharge 5Use of interpreter to complete education 20ADDITIONAL HOURS PER CLIENT
Eating Disorders Review of Medical file -5Usually only encountered on kids ward Handover/ referral out eg. eating disorder units 15
ADDITIONAL HOURS PER CLIENTCoeliac Disease Initial Assessment -5
Education for discharge 15Documentation -5Outpatient review (30 minute appointment )ADDITIONAL HOURS PER CLIENT
Newly diagnosed NIDDM / High cholesterol review of medical file 10Interview / education / provision of resources 20Documentation 15ADDITIONAL HOURS PER CLIENT
Allergies Review medical file 10few seen Interview 10usually food intolerances Documentation 10
(Medical notes +/- inpatient cardHardcopy 5ADDITIONAL HOURS PER CLIENT
Weight reduction Interview / Provision of written resources 10Documentation 5May require additional outpatient appointmentADDITIONAL HOURS PER CLIENT
Other brief interventions
Intervention time (mins)
Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements Please Qualify
Additional interventions / hours specific to client
group
A B A B
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2
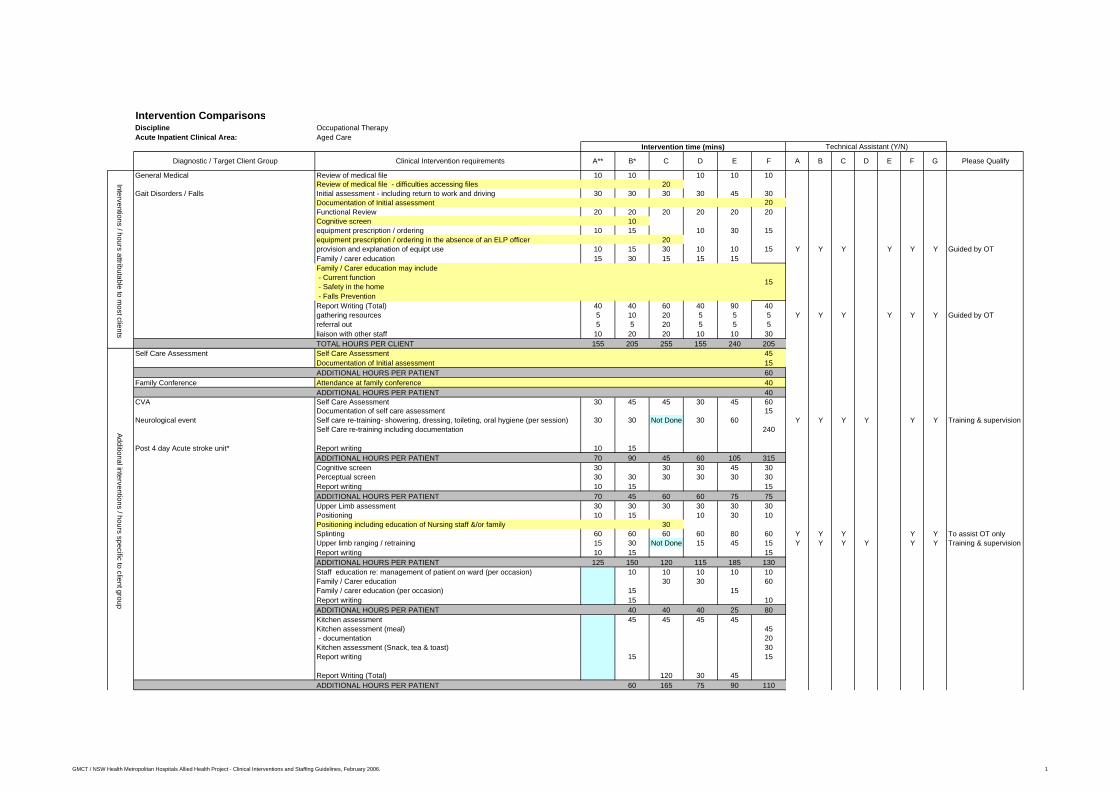
Intervention ComparisonsDiscipline Occupational TherapyAcute Inpatient Clinical Area: Aged Care
General Medical Review of medical file 10 10 10 10 10Review of medical file - difficulties accessing files 20
Gait Disorders / Falls Initial assessment - including return to work and driving 30 30 30 30 45 30Documentation of Initial assessment 20Functional Review 20 20 20 20 20 20Cognitive screen 10equipment prescription / ordering 10 15 10 30 15equipment prescription / ordering in the absence of an ELP officer 20provision and explanation of equipt use 10 15 30 10 10 15 Y Y Y Y Y Y Guided by OTFamily / carer education 15 30 15 15 15Family / Carer education may include - Current function - Safety in the home - Falls PreventionReport Writing (Total) 40 40 60 40 90 40gathering resources 5 10 20 5 5 5 Y Y Y Y Y Y Guided by OTreferral out 5 5 20 5 5 5liaison with other staff 10 20 20 10 10 30TOTAL HOURS PER CLIENT 155 205 255 155 240 205
Self Care Assessment Self Care Assessment 45Documentation of Initial assessment 15ADDITIONAL HOURS PER PATIENT 60
Family Conference Attendance at family conference 40ADDITIONAL HOURS PER PATIENT 40
CVA Self Care Assessment 30 45 45 30 45 60Documentation of self care assessment 15
Neurological event Self care re-training- showering, dressing, toileting, oral hygiene (per session) 30 30 Not Done 30 60 Y Y Y Y Y Y Training & supervisionSelf Care re-training including documentation 240
Post 4 day Acute stroke unit* Report writing 10 15ADDITIONAL HOURS PER PATIENT 70 90 45 60 105 315Cognitive screen 30 30 30 45 30Perceptual screen 30 30 30 30 30 30Report writing 10 15 15ADDITIONAL HOURS PER PATIENT 70 45 60 60 75 75Upper Limb assessment 30 30 30 30 30 30Positioning 10 15 10 30 10Positioning including education of Nursing staff &/or family 30Splinting 60 60 60 60 80 60 Y Y Y Y Y To assist OT onlyUpper limb ranging / retraining 15 30 Not Done 15 45 15 Y Y Y Y Y Y Training & supervisionReport writing 10 15 15ADDITIONAL HOURS PER PATIENT 125 150 120 115 185 130Staff education re: management of patient on ward (per occasion) 10 10 10 10 10Family / Carer education 30 30 60Family / carer education (per occasion) 15 15Report writing 15 10ADDITIONAL HOURS PER PATIENT 40 40 40 25 80Kitchen assessment 45 45 45 45Kitchen assessment (meal) 45 - documentation 20Kitchen assessment (Snack, tea & toast) 30Report writing 15 15
Report Writing (Total) 120 30 45ADDITIONAL HOURS PER PATIENT 60 165 75 90 110
Additional interventions / hours specific to client group
Please Qualify
Technical Assistant (Y/N)Intervention time (mins)
C E FB GC DD E F AA**Diagnostic / Target Client Group B*
Interventions / hours attributable to most clients
Clinical Intervention requirements
15
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Occupational TherapyAcute Inpatient Clinical Area: Aged Care (continued)
Mini Mental Scale Examination 15 30Initial contact with family / carer re pre-morbid function 15 15 15 45Functional assessment 20 20 20
Cognitive impairment cognitive screen 30 30 30 30Dementia Kitchen assessment 35 45 45 45 35 35
liaison with other staff - Med.,SW, CCN, PT 30 30 30 30 30liaison with other staff - Med.,SW, CCN, PT including - current function - Discharge planning eg. Medication management, services, transport homefamily /carer education 30 45 30 30 30 30
Delerium eg. Post anaesthesia, UTI, wound infection Daily review of cognitive status 30 10 Not done 30 30 30report writing 30 30 60 30 30 30Liaison with other institutions re: packages of care 20 20 20 20Guardianship application 180 180 180Participation in Family Conference 60ADDITIONAL HOURS PER PATIENT 420 175 255 410 420 360
COPD Self Care assessment 30 45 45 30 45 60Functional assessment 30 45 30 30 30 30Education eg energy conservation techniques without Pulse Oximetry 30Education / Retraining using Pulse Oximetry 60 60 Not done 60 60Liaison with medical team re Oxygen needs 15 10 15 15 15
ADDITIONAL HOURS PER PATIENT 135 160 75 135 120 165AMI Education on safe activities post AMI, Stent , CABG 20 20 30 30 20 20post Stent Education on energy conservation techniques 10 20 20 30 10 10post CABG Education on return to work 20 20 20 20 20 20
Education on driving 10 10 10 10 10 10Review of education 15 15 15 15 15 15 Y Y Y Y Y Y Guided by OTReferal out eg. Cardiac Rehab, Commonwealth Rehab Service, Community OT 20 5 20 20 20 20ADDITIONAL HOURS PER PATIENT 95 90 115 125 95 95
Palliative Care & going home Functional Review 30 40 30 30 30 30equipment prescription / ordering 10 30 30 60 30equipment prescription / ordering in the absence of an ELP officer 40sourcing specialist equipment 30 30 80 45 30 30provision and explanation of equipt use 10 30 10 30 10 Y Y N Y Y Y Y Guided by OT - including specialist equipment eg. Training of hoist use 30Family / carer education / training in client management 15 30 20 15 15 15referral out 10 20 10 10 10 10liaison with other staff re: discharge 10 20 10 10 20 10ADDITIONAL HOURS PER PATIENT 115 200 220 150 195 135
MVA Screening for Post Traumatic Amnesia 15 15 15 15 15Daily review of cognitive status 30report writing per session 10 10 10 10 10ADDITIONAL HOURS PER PATIENT 25 25 55 25 25 0
Hand / UL Splinting 60 60 60 60 60 Y Y Y Y Y Y To Assist OT OnlyMisc # Outpatient referral 5 5 5 5 5nerve injuries report writing 10 10 30 10 10
ADDITIONAL HOURS PER PATIENT 75 75 95 75 0 75Home Environment Assessment Home assessment - preparation 15 30 30 15Conducted by separate Community team** or Home assessment 90 60 80 90by Acute Care OT's Travel - Home assessment 60 60 100 60
report writing 30 90 90 120 30Liaison with inpatient staff 10 15 10Liaison with trades people including referral / drawings 15 60 60 30 60ADDITIONAL HOURS PER PATIENT 220 315 360 325 120 240
Additional interventions / hours specific to client group
Interventions reported by only one particular service
Interventions omitted from template or not performed by a service
F G Please QualifyB C D E
Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements A** B* C D E F A
120
150
120
Intervention time (mins)
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline Occupational TherapyAcute Inpatient Clinical Area: General Medical
General Medical Review of medical file 10 10 10 10Review of medical file - difficulties accessing files 20
Gait Disorders / Falls Initial assessment - including return to work and driving 30 30 30 30 45Initial assessment - Read and understand medical file - Liaise with other releent health professional (s) - Functional Review eg. Mobility Transfers, self care, range of motion - Clarify information with family / carer if required - Identify issues - Plan intervention / treatment plan - Document in medical fileFunctional Review 20 20 20 30 20Cognitive screen 10equipment prescription / ordering 10 15 10 60 10equipment prescription / ordering in the absence of an ELP officer 20provision and explanation of equipt use 10 15 30 10 10 10 Y Y Y Y Y Y Guided by OTFamily / carer education 15 30 15 15 15 15Report Writing (Total) 40 40 60 40 90 40gathering resources 5 10 20 5 5 5 Y Y Y Y Y Y Guided by OTreferral out 5 5 20 5 20 5liaison with other staff 10 20 20 10 10 10TOTAL HOURS PER CLIENT 155 205 255 165 285 145
Family Conference Participation in Family Conference 60TOTAL HOURS PER CLIENT 60
Complex Family Issues Additional Family Carer Education 45Development / collation and Provision of Education resources 60TOTAL HOURS PER CLIENT 105
CVA Self Care Assessment 30 45 45 45 60 60Neurological event Self care re-training- showering, dressing, toileting, oral hygiene (per session) 30 30 Not Done 20 20 20 Y Y Y Y Y Y Training & supervisionPost 4 day Acute stroke unit* Report writing 10 15
TOTAL HOURS PER CLIENT 70 90 45 65 80 80Cognitive screen 30 30 30 45 30Perceptual screen 30 30 30 30 30 30Report writing 10 15TOTAL HOURS PER CLIENT 70 45 60 60 75 60Feeding assessment 30TOTAL HOURS PER CLIENT 30Upper Limb assessment 30 30 30 30 45 30Positioning 10 15 10 30 10Positioning including education of Nursing staff &/or family 30Splinting 60 60 60 60 80 60 Y Y Y Y Y To assist OT onlyUpper limb ranging / retraining 15 30 Not Done 30 30 30 Y Y Y Y Y Y Training & supervisionReport writing 10 15TOTAL HOURS PER CLIENT 125 150 120 130 185 130Staff education re: management of patient on ward (per occasion) 10 10 10 10 10 10Family / Carer education 30 15Family / carer education (per occasion) 15 15 15 15Report writing 10 15TOTAL HOURS PER CLIENT 35 40 40 25 25 25Kitchen assessment 45 45 45 45 30 60Report writing 10 15Report Writing (Total) 120 30 80 30TOTAL HOURS PER CLIENT 55 60 165 75 110 90
Please Qualify
Technical Assistant (Y/N)Intervention time (mins)
50
C E FBD E F A GC DA**Diagnostic / Target Client Group B*
Interventions / hours attributable to most clients
Clinical Intervention requirements
Additional interventions / hours specific to client group
GMCT / NSW Health Metopolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Occupational TherapyAcute Inpatient Clinical Area: General Medical
Mini Mental Scale Examination 15Initial contact with family / carer re pre-morbid function 15Functional assessment 20
Cognitive impairment cognitive screen 30 30 30 30 30Dementia Kitchen assessment 35 45 45 45 45 45
liaison with other staff - Med.,SW, CCN, PT 30 30 30 30 30 30family /carer education 30 45 30 30 30 30
Delerium eg. Post anaesthesia, UTI, wound infection Daily review of cognitive status 30 10 Not Done 30 30 30report writing 30 30 60 30 30 30Liaison with other institutions re: packages of care 20Guardianship application 180TOTAL HOURS PER CLIENT 420 175 195 195 195 195
COPD Self Care assessment 30 45 45 45 60 45Functional assessment 30 45 30 30 30 30Education eg energy conservation techniques without Pulse Oximetry 40Education / Retraining using Pulse Oximetry 60 60 Not Done 60 60Liaison with medical team re Oxygen needs 15 10 Not Done 15 15 15TOTAL HOURS PER CLIENT 135 160 75 150 145 150
AMI Education on safe activities post AMI, Stent , CABG 20 20 30 30 30 20post Stent Education on energy conservation techniques 10 20 20 30 20post CABG Education on return to work 20 20 20 20 5 20
Education on driving 10 10 10 10 5 10Review of education 15 15 15 15 15 15 Y Y Y Y Y Y Guided by OTReferal out eg. Cardiac Rehab, Commonwealth Rehab Service, Community OT 20 5 20 20 20 20TOTAL HOURS PER CLIENT 95 90 115 125 75 105
Palliative Care & going home Functional Review 30 40 30 30 30 30equipment prescription / ordering 10 30 30 60 15equipment prescription / ordering in the absence of an ELP officer 40sourcing specialist equipment 30 30 80 50 30 30provision and explanation of equipt use 10 30 10 30 10 Y Y N Y Y Y Y Guided by OT - including specialist equipment eg. Training of hoist use 30Family / carer education / training in client management 15 30 20 20 20 20referral out 10 20 10 10 10 10liaison with other staff re: discharge 10 20 10 10 45 10TOTAL HOURS PER CLIENT 115 200 220 160 225 125
MVA Screening for Post Traumatic Amnesia 15 15 15 15 15Daily review of cognitive status 30report writing per session 10 10 10 10 10TOTAL HOURS PER CLIENT 25 25 55 25 0 25
Hand / UL Splinting 60 60 60 60 60 60 Y Y Y Y Y Y To Assist OT OnlyMisc # Outpatient referral 5 5 5 5 5 5nerve injuries report writing 10 10 30 10 10 10
TOTAL HOURS PER CLIENT 75 75 95 75 75 75Home Environment Assessment Home assessment - preparation 15 30 30 30Conducted by separate Community team** or Home assessment 90 60 80 60by Acute Care OT's Travel - Home assessment 60 60 100 60
report writing 30 90 90 120Liaison with inpatient staff 10 15 15Liaison with trades people including referral / drawings 15 60 60 60 120TOTAL HOURS PER CLIENT 220 315 360 345 120 240
120
Technical Assistant (Y/N)
F G
Interventions reported by only one particular service
Interventions omitted from template or not performed by a service
Intervention time (mins)
120
Diagnostic / Target Client Group Clinical Intervention requirements A** B* C Please Qualify
Additional interventions / hours specific to client group
B C D ED E F A
GMCT / NSW Health Metopolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline Occupational TherapyAcute Inpatient Clinical Area: Orthopaedics No. of beds
Please Qualify
Review of medical file 10 10 10 10 10Review of medical file - difficulties accessing files 20Initial assessment 30 30 30 30 30 30
#NOF Functional Review 20 20 20 20 20Functional Review including documentation 20equipment prescription / ordering in the absence of an ELP Officer 20
General Orthopaedic equipment prescription / ordering 10 15 30 30 Y Ordering onlyprovision and explanation of equipt use 10 15 30 10 10 Y Y Y Guided by OTFamily / carer education 15 30 15 15 15 15report writing 40 40 60 40 40gathering resources 5 10 15 20 5 5 Y Y Y Guided by OTreferral out 5 5 5 20 5 5 - all hips and knees referred to a Post Acute Community Therapist #liaison with other staff 10 20 10 20 10 10TOTAL HOURS PER CLIENT
Self Care Assessment deemed necessary Self Care Assessment / retraining 30 45 30 30#NOF** report writing 10 10 10 10Total and Partial Knee Replacements** Limited self care intervention #Total Hip Replacement / hemiarthroplasty**
TOTAL HOURS PER CLIENTCognitive impairment cognitive screen 15 15 15 15 15
Initial Mini Mental Scale Examination 20Functional Assessment 60 - self care and instrumental
Dementia liaison with other staff - Med.,SW, CCN, PT 30 30 30 30 30 30family /carer education 30 30 30 30 30 30Formal Cognitive assessment 60
Delerium eg. Post anaesthesia, UTI, wound infection **Daily review of cognitive status 30 30 30report writing 30 30 30 60 30 30TOTAL HOURS PER CLIENT
Total and Partial Knee Replacements Knee precaution education 10 10 10 10 10report writing 5 5 5 5 5Education re: Work simplification and documentation 15TOTAL HOURS PER CLIENT
THR/ Hemiarthroplasty Hip precaution education 15 15 15 15 15Review of hip precautions 10 10 10 10 Y Y Y Training and supervisionreport writing 10 10 10 10 10TOTAL HOURS PER CLIENT
MVA Initial Screening for Post Traumatic Amnesia 15 15 15 30Daily completion of Westmead PTA scale (mins per day) 15 15Daily review of cognitive status 30report writing (per day) 10 10 20 10TOTAL HOURS PER CLIENT
Hand / UL Splinting 60 60 60 60 60Functional Education 30 - e.g One handed techniques
Misc # Outpatient referral 5 5 5 5 5nerve injuries report writing 10 10 10 20 10
Outpatient follow up at 45 mins per session #TOTAL HOURS PER CLIENT
Home Assessment Home assessment - preparation 30 30 30 30 30 Y Gided by OTConducted by separate Community team* or Home assessment 60 60 60 80 60by Acute Care OT's Travel - Home assessment 60 60 60 100 60
report writing (Dept of Housing, PADP, Home Mods) 90 90 90 90 120Liaison with inpatient staff 15 15 15 15Liaison with trades people including referral / drawings 60 60 60 60 60TOTAL HOURS PER CLIENT
Pre-admission Orthopaedics Home Assessment prior to THR 60Travel - Home assessment 100TOTAL HOURS PER CLIENT
120
E F
60
25
A B C DDiagnostic / Target Client Groups Clinical Intervention requirements
Intervention time (mins) Technical Assistant (Y/N)
A* B* C** D E F
Intervention / hours attributable to most
clientsA
dditional interventions/ hours specific to client group
Interventions reported by only one particular service
Interventions omitted from template or not performed by a service
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1
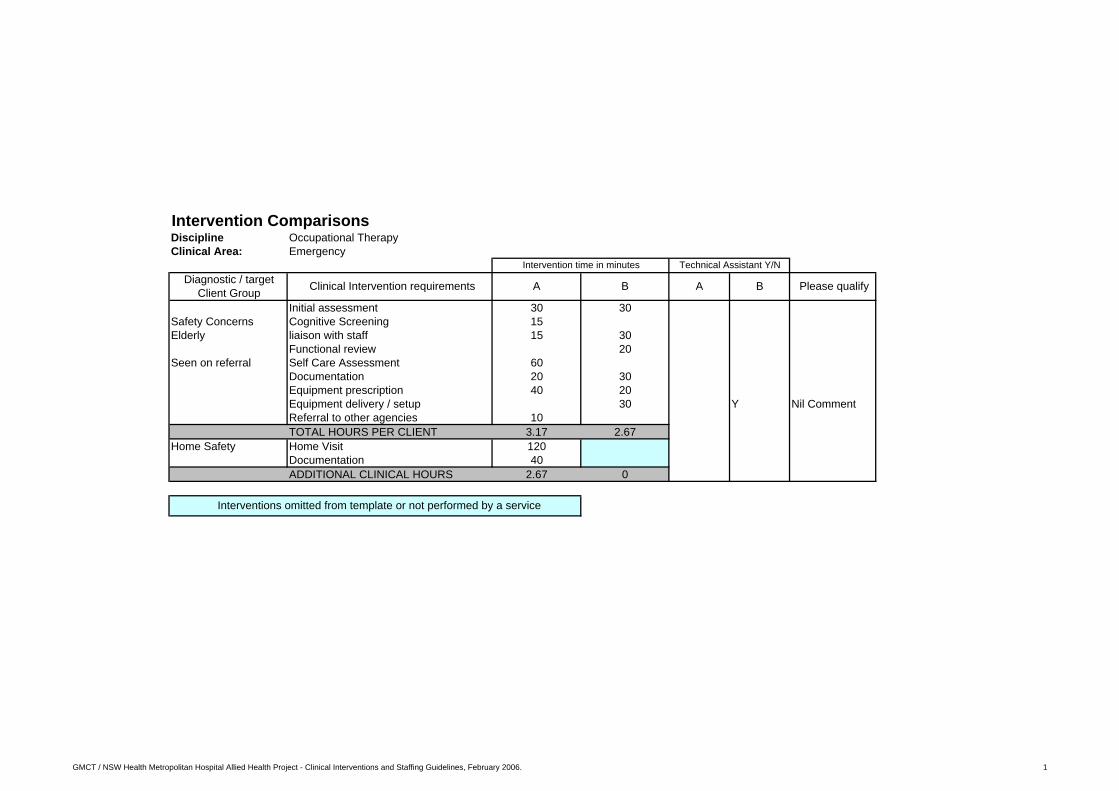
Intervention ComparisonsDiscipline Occupational TherapyClinical Area: Emergency
Initial assessment 30 30Safety Concerns Cognitive Screening 15Elderly liaison with staff 15 30
Functional review 20Seen on referral Self Care Assessment 60
Documentation 20 30Equipment prescription 40 20Equipment delivery / setup 30 Y Nil CommentReferral to other agencies 10TOTAL HOURS PER CLIENT 3.17 2.67
Home Safety Home Visit 120Documentation 40ADDITIONAL CLINICAL HOURS 2.67 0
Interventions omitted from template or not performed by a service
Please qualifyDiagnostic / target Client Group
Intervention time in minutes
BClinical Intervention requirements
Technical Assistant Y/N
A BA
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Occupational TherapyClinical Area: Paediatrics
Orthopaedics Initial Assessment 30Equipment prescription 60Education 20Documentation 15
Neuro Initial Assessment 30Equipment prescription 60Education to patient 20Self care assessment 40Upper limb assessment 40Upper limb retraining 45 per daySplinting 60Home Visit 120School Visit 120Education to School 40Report writing 90
MVA Cognitive Assessment - PTA 60Initial Assessment 30Equipment prescription 30Referral to other agencies 20
Substance abuse Initial Assessment 10babies / neglect Developmental assessment 60
Documentation 20Education 30Developmental Treatment 60
Intervention time (mins)
Diagnostic / Target Client Groups Clinical Intervention requirements
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Occupational TherapyClinical Area: ICU / HDU
Intervention time (mins)
Discharge Planning Initial Assessment 40 30 N/A N/A Nil CommentsFunctional Review 20Equipment prescription 30Education 20Cognitive Screening 30Documentation 30TOTAL HOURS PER CLIENT 2 1Home Visit 120
2 0Self care Assessment 60
1 0Upper Limb Assessment 30
Positioning 20Splinting 60Documentation 30ADDITIONAL INTERVENTION HOURS 2.33 0
Technical Assistant (Y/N)
BAA
Interventions omitted from template or not performed by a service
Please qualifyClinical Intervention requirementsDiagnostic / Target Client Groups B
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Occupational TherapyClinical Area Outpatients
General Rehab: Initial assessmen 30 - Arthritis Functional Review 15 - CVA's Explanation of the condition 10 - Carpel Tunnel Syndrome Education /training re ongoing managemen 10
referral out 10liaison with other staf 15equipment prescription 15provision and explanation of equipt us 15report writing 20Splint fabrication 60Splint - review of fit, wearing regime, maintenance exercise 40
CVA's cognitive / perceptual assessmen 60 60ABI Splint fabrication 60 60
Balance work 30Upper Limb therapy 60Prescription of upper limb support system 15cognitive therapy 45perceptual therapy 45functional assessments & retrainin 60community access 60Review home environment and function 60Family Conferences 45Liaison with referrees 20Eg. CRS, SEDS, workplacereport writing 20 15TOTAL HOURS PER CLIENT
Acute Hands Initial assessment 60 45 60tendon repairs Splinting 60 608 - 12 weeks management Therapy sessions 50
- Oedema Management - Scar Management
Rarely seen* - ROM / Strengthening - Review / winding down 20 30 30
Wrist #s - Functional review / retraining / ADL 30 30Liaison with specialists 40Documentation 30
Pre-admission Clinic Initial assessment 20 30Orthopaedics Functional Review / Home environment 20
Education re post op requirements for home 30 - Equipment provided after admissionEquipment prescription 20Ordering equipment if client unable to source themselves 30Documentation 5 60
Complicated joint replacement Functional review and home assessment if need identified in 60pre-admission clinic
Falls Clinic 1 session per weekIncluding home assessment
Group Initial assessment 45Cancer Therapy Lymphoedema assessment 90Centre Energy conservation & fatigue management education 60
Lymphoedema treatment 90mins per dayHome visit 120Equipment prescription 30Report writing 60
EA*
Intervention time (mins
Diagnostic / Target Groups Clinical Intervention requirements DB
50
120
C
10
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Discipline Occupational TherapyClinical Area Outpatients (continued)
Palliative Care Initial Assessment 45Home Visit 120Equipment prescription 60Education to patient and carer 30Liaison with team 30Report writing 60
Supported Discharge Initial Assessment 45Home Visit 120Equipment prescription 20Report writing 90Education 30
Cardiac Outpatients Home Visits 120Education 20Equipment prescription 30
Cardiac Relaxation Group Relaxation Group 60Preparation for group 20
Weekly sessionsie. 52 per year
Cardiac Rehab Group Travel from another hospital site 30Rehab education and exercise session 60
Handwriting Assessments Handwriting assessment 60Report writing 150
Cardiac Review Case 10Respiratory Arrange appointment 10
Prepare treatment area 10Assessment of functional capacity 60education 20 - 30Home assessment 90 - Home mods / equipmentTravel 30Report writing 60 - PADP / Home Modification applicationsFamily liaison
Wheelchair Prescription File Review 10Arranging Appointment 5Treatment preparation 10Mat evaluation 90Home assessment 60Telephone call to wheelchair supplier re wheelchair requirements 15Trial of wheelchair 120Re-assessment on supply of wheelchair 60Report writing 90? Involvement in the financial aspect of wheelchair purchaseeg. PADP applications
Splinting File review 10Arranging appointment 5Treatment preparation 10Assessment of the hand 15Splint fabrication 60 60Report writing 15Education 15 - 20 - Review of fit, wearing regime, maintenance exercises 40Equipment prescription 10 - 15
Intervention time (mins
Diagnostic / Target Groups Clinical Intervention requirements A* B C D E
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: General Medical
* Respiratory Review of medical file 10 5 5 NInitial assessment 10
* Mobility - talk to patient (family if present) re: past history, medical , social , level of function - current physical status 5 5 N
* Pain relief Mobility assessment ie sitting out of bed, standing, walking - assessment of gait & balance disorders - determining safety for dischargePrescription & provision of appropriate mobility aid 15 N - including standing aid 15 - including gathering equipment and ELP 30Daily assessment & mobilisation - 30mins per day Y Y Y Under supervision of physio - gait retraining Often require assistance x2 - range of motion and strengthening exercises May be a TA or another PT - progression of mobility / walking aids / terrain - safety for dischargeStairs - 20mins per session 20 N - includes transport of patient to and from staircase plus practise session* sreps are 210m from ward and patients often require wheelchair transportationEducation - per day 10Gathering equipment eg. walking aids, splints, braces 10 10 YLiaison with medical / nursing staff re condition and pain relief 5 5 10 NDischarge Planning 25 N N - Ordering equipment through the Equipment loan pool 30 30 - Advice to patient/ family re purchase/ hire of equipment 10 10 - Referral Out ie Outpatients, Hydrotherapy, community therapy teams - Report writingliaison with staff - per day 10Liaison with family - per day 10Report writing - per day 10 10 10Documentation per session 10 5 Y For specific treatment sessions TOTAL HOURS PER CLIENT Under supervision of physioDaily Upper limb retraining - 20 mins per day 20TOTAL HOURS PER CLIENT
Respiratory Assessment 10 20 N - Auscultation (stethoscope) 10 - Assessment & observation of respiratory pattern - Oxygen sats - Assessment of cough effectiveness ( moist, dry , productive)Review X-Rays for abnormality 10 10Treatment 30 30 20 N - patient education re: self clearance of secretions, breathing technique - Positive Expiratory Pressure exercises - Mobilisation to improve breathing function / exercise tolerance report writing 10 10 5Spirometry D/C 15Pre & Post 30Baseline 15TOTAL HOURS PER CLIENT
Acute respiratory infection Postural drainage 20 20PercussionVibrationSaline Nebulisers 5 5Positioning to improve ventilation 10 10Suctioning if ineffective cough & bed bound 30 30Induced sputum samples requested by DrTOTAL HOURS PER CLIENT
Technical Assistant (Y/N)
B D
Intervention time (mins)
Diagnostic / Target Client Group Clinical Intervention requirements A B C D Please Qualify
30
30 25
20 20
A C
45
Intervention / hours attributable to most clients
30 30
20 40
Additional intervention hours specific to client group
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: General Medical (Continued)
Pain relief Monitoring of drug effects / blood pressure changes 20 5 - musculoskeletal treatment modalities eg. Hot packs, cryotherapy (ice), TENs 20 - #'s Close liaison with medical team 10 10 - neurological Daily review of symptoms, effects of treatment 10 10
report writing 5TOTAL HOURS PER CLIENT
# Cervical spine If ASPEN Brace requested by neurosurgeon - Ordering 30 - fitting 60 - Review and show and tell with relatives 30 - education of nursing staff re management of ASPEN BraceTOTAL HOURS PER CLIENT
CVA Initial assessment 20 Y May require asssit of 2 staffother Neuroological - MAS Mobility Assessment Score Often specific training needed
- Respiratory assessment - General informationProvision of Shoulder sling / AFO 20Prescription and application of: - foot splints / AFOs 40 - Shoulder slings , FES 20Ongoing Stroke rehabilitation - per session 30Education to family 10Tilt Table - 30 mins per session 30TOTAL HOURS PER CLIENT
Please Qualify
Additional intervention hours specific to client group
B C D
Intervention time (mins) Technical Assistant (Y/N)
Interventions omitted from template or not performed by a service
C D A
Interventions reported by only one particular service
Diagnostic / Target Client Group Clinical Intervention requirements A B
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2
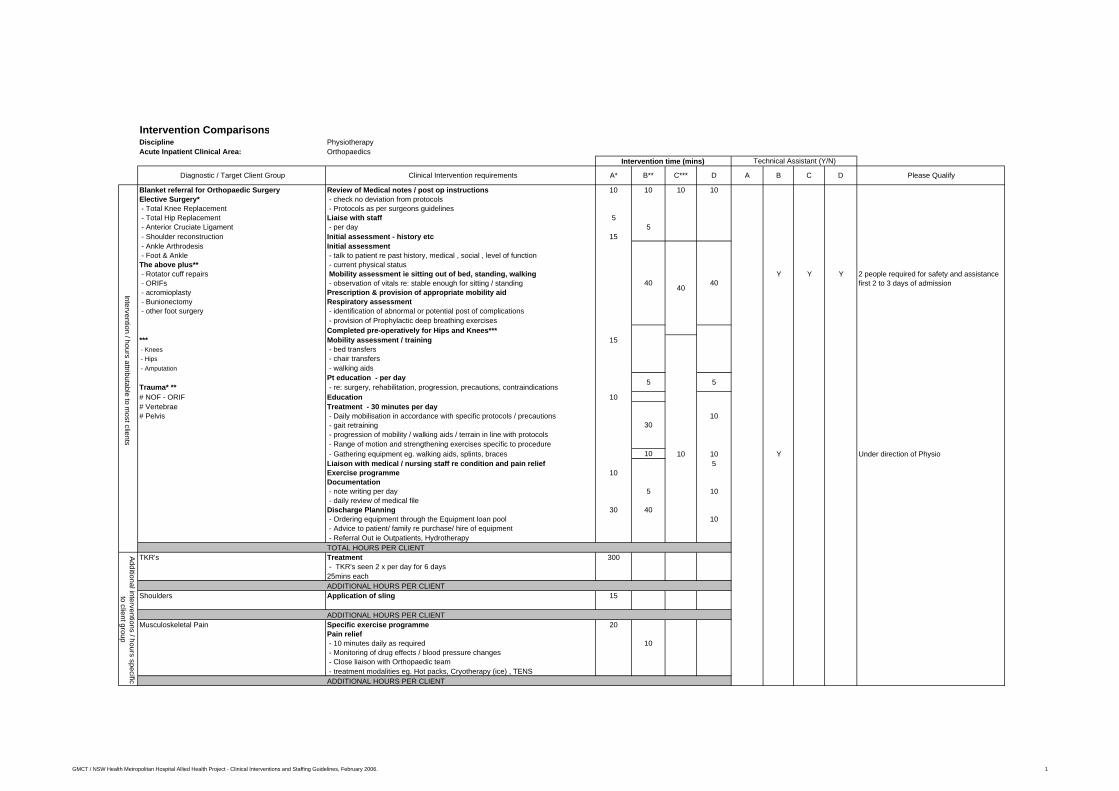
Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: Orthopaedics
Blanket referral for Orthopaedic Surgery Review of Medical notes / post op instructions 10 10 10 10Elective Surgery* - check no deviation from protocols - Total Knee Replacement - Protocols as per surgeons guidelines - Total Hip Replacement Liaise with staff 5 - Anterior Cruciate Ligament - per day 5 - Shoulder reconstruction Initial assessment - history etc 15 - Ankle Arthrodesis Initial assessment - Foot & Ankle - talk to patient re past history, medical , social , level of functionThe above plus** - current physical status - Rotator cuff repairs Mobility assessment ie sitting out of bed, standing, walking Y Y Y 2 people required for safety and assistance - ORIFs - observation of vitals re: stable enough for sitting / standing first 2 to 3 days of admission - acromioplasty Prescription & provision of appropriate mobility aid - Bunionectomy Respiratory assessment - other foot surgery - identification of abnormal or potential post of complications
- provision of Prophylactic deep breathing exercisesCompleted pre-operatively for Hips and Knees***
*** Mobility assessment / training 15 - Knees - bed transfers - Hips - chair transfers - Amputation - walking aids
Pt education - per dayTrauma* ** - re: surgery, rehabilitation, progression, precautions, contraindications# NOF - ORIF Education 10# Vertebrae Treatment - 30 minutes per day# Pelvis - Daily mobilisation in accordance with specific protocols / precautions 10
- gait retraining - progression of mobility / walking aids / terrain in line with protocols - Range of motion and strengthening exercises specific to procedure - Gathering equipment eg. walking aids, splints, braces 10 10 10 Y Under direction of PhysioLiaison with medical / nursing staff re condition and pain relief 5Exercise programme 10Documentation - note writing per day 5 10 - daily review of medical fileDischarge Planning 30 40 - Ordering equipment through the Equipment loan pool 10 - Advice to patient/ family re purchase/ hire of equipment - Referral Out ie Outpatients, HydrotherapyTOTAL HOURS PER CLIENT
TKR's Treatment 300 - TKR's seen 2 x per day for 6 days25mins eachADDITIONAL HOURS PER CLIENT
Shoulders Application of sling 15
ADDITIONAL HOURS PER CLIENTMusculoskeletal Pain Specific exercise programme 20
Pain relief - 10 minutes daily as required 10 - Monitoring of drug effects / blood pressure changes - Close liaison with Orthopaedic team - treatment modalities eg. Hot packs, Cryotherapy (ice) , TENSADDITIONAL HOURS PER CLIENT
B
4040
5
Intervention / hours attributable to most clients
A*
30
5
Intervention time (mins) Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements B** C*** D A C D Please Qualify
40
Additional interventions / hours specific to client group
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: Orthopaedics (Continued)
Secondary Respiratory problems Respiratory assessment & breathing exercises 20 10Daily treatment 20ADDITIONAL HOURS PER CLIENT
ACL Repairs Application of Range Of Motion Brace 30Roy Brace fitting 15ADDITIONAL HOURS PER CLIENT
# ankles Application of plasters 20Gathering materials 10 YADDITIONAL HOURS PER CLIENT
Change of Plaster Gathering equipment 10 10 10for # Removal / appliction of plaster 30 30 30 Y Requires 2 people for lower limb plasters
ADDITIONAL HOURS PER CLIENTUpper Limb # Application of slings / collar and cuff 15 15 15
ADDITIONAL HOURS PER CLIENT# NOF complicated by social factors / cognitive issues Discharge Planning re accommodation and safety issues 30 30 30
ADDITIONAL HOURS PER CLIENTTrauma whilst an inpatient Daily Skin traction until day of surgery 20 20awaiting assessment / surgeryeg. fall and # whilst on ward or missed #
ADDITIONAL HOURS PER CLIENTPain relief Daily intervention as necessary 10 15Deciding factor in speed of recovery - Monitoring of drug effects / blood pressure changes
- Close liaison with Orthopaedic team - treatment modalities eg. Hot packs, cryotherapy (ice), TENs ADDITIONAL HOURS PER CLIENT
Orthopaedic Clinics Plaster application & removal 20 Y Y Y To Assist Physiox2 therapists - short leg 30 Requires 2 people for lower limb plasters
- long leg 60 - removal 25Caseload specific:
3 hours Total Set up of orthopaedic clinic Y Under instruction from Physio - 30mins once per weekTOTAL HOURS PER CLIENT
Pre-admission Clinic Initial assessment 20 NBreathing educationTOTAL HOURS PER CLIENT
Pre admission clinic group session 30 mins per week 30 N NTKR's and THR's Pre-op assessment 60
TOTAL HOURS PER CLIENT
Other O
utpatient Interventions
B
Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements A* B** C*** D A Please Qualify
Additional interventions / hours specific to client group
Intervention time (mins)
C D
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2
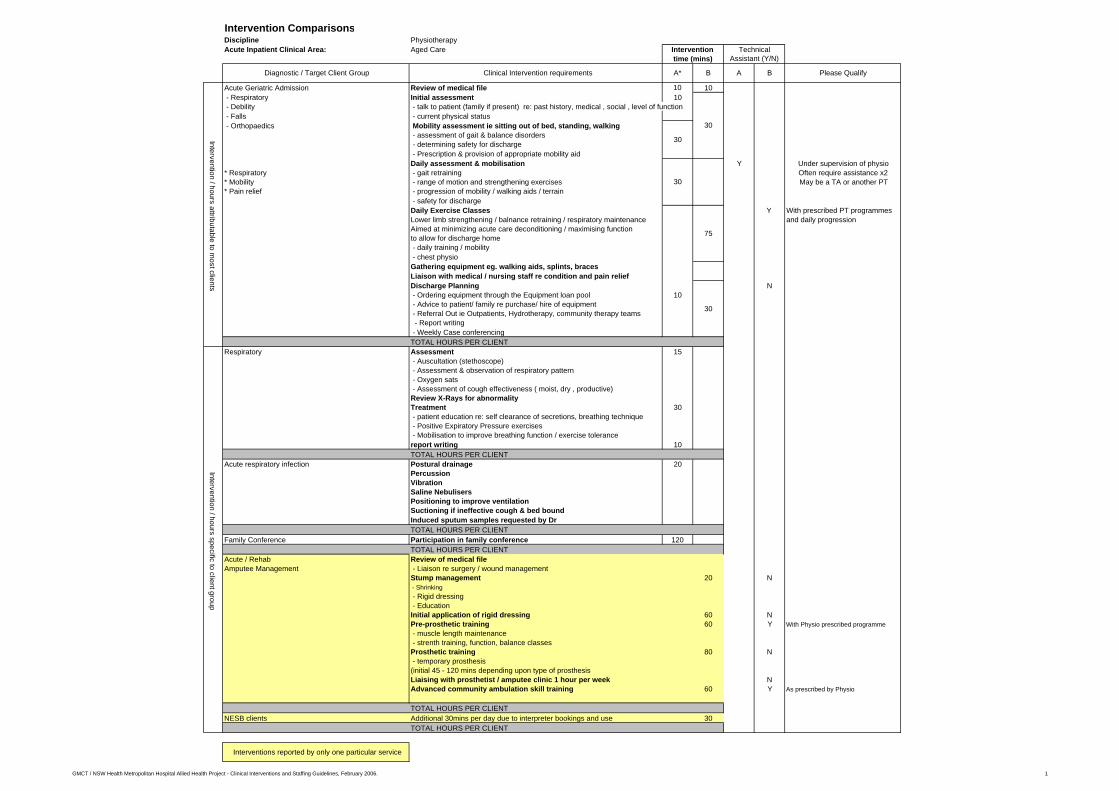
Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: Aged Care
Acute Geriatric Admission Review of medical file 10 10 - Respiratory Initial assessment 10 - Debility - talk to patient (family if present) re: past history, medical , social , level of function - Falls - current physical status - Orthopaedics Mobility assessment ie sitting out of bed, standing, walking
- assessment of gait & balance disorders - determining safety for discharge - Prescription & provision of appropriate mobility aidDaily assessment & mobilisation Y Under supervision of physio
* Respiratory - gait retraining Often require assistance x2* Mobility - range of motion and strengthening exercises May be a TA or another PT* Pain relief - progression of mobility / walking aids / terrain
- safety for dischargeDaily Exercise Classes Y With prescribed PT programmes Lower limb strengthening / balnance retraining / respiratory maintenance and daily progressionAimed at minimizing acute care deconditioning / maximising functionto allow for discharge home - daily training / mobility - chest physioGathering equipment eg. walking aids, splints, bracesLiaison with medical / nursing staff re condition and pain reliefDischarge Planning N - Ordering equipment through the Equipment loan pool 10 - Advice to patient/ family re purchase/ hire of equipment - Referral Out ie Outpatients, Hydrotherapy, community therapy teams - Report writing - Weekly Case conferencingTOTAL HOURS PER CLIENT
Respiratory Assessment 15 - Auscultation (stethoscope) - Assessment & observation of respiratory pattern - Oxygen sats - Assessment of cough effectiveness ( moist, dry , productive)Review X-Rays for abnormalityTreatment 30 - patient education re: self clearance of secretions, breathing technique - Positive Expiratory Pressure exercises - Mobilisation to improve breathing function / exercise tolerance report writing 10TOTAL HOURS PER CLIENT
Acute respiratory infection Postural drainage 20PercussionVibrationSaline NebulisersPositioning to improve ventilationSuctioning if ineffective cough & bed boundInduced sputum samples requested by DrTOTAL HOURS PER CLIENT
Family Conference Participation in family conference 120TOTAL HOURS PER CLIENT
Acute / Rehab Review of medical fileAmputee Management - Liaison re surgery / wound management
Stump management 20 N - Shrinking - Rigid dressing - EducationInitial application of rigid dressing 60 NPre-prosthetic training 60 Y With Physio prescribed programme - muscle length maintenance - strenth training, function, balance classesProsthetic training 80 N - temporary prosthesis (initial 45 - 120 mins depending upon type of prosthesisLiaising with prosthetist / amputee clinic 1 hour per week NAdvanced community ambulation skill training 60 Y As prescribed by Physio
TOTAL HOURS PER CLIENTNESB clients Additional 30mins per day due to interpreter bookings and use 30
TOTAL HOURS PER CLIENT
Interventions reported by only one particular service
B Please QualifyADiagnostic / Target Client Group Clinical Intervention requirements A* B
Technical Assistant (Y/N)
75
30
Intervention / hours specific to client groupIntervention / hours attributable to m
ost clients
30
30
30
Intervention time (mins)
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1
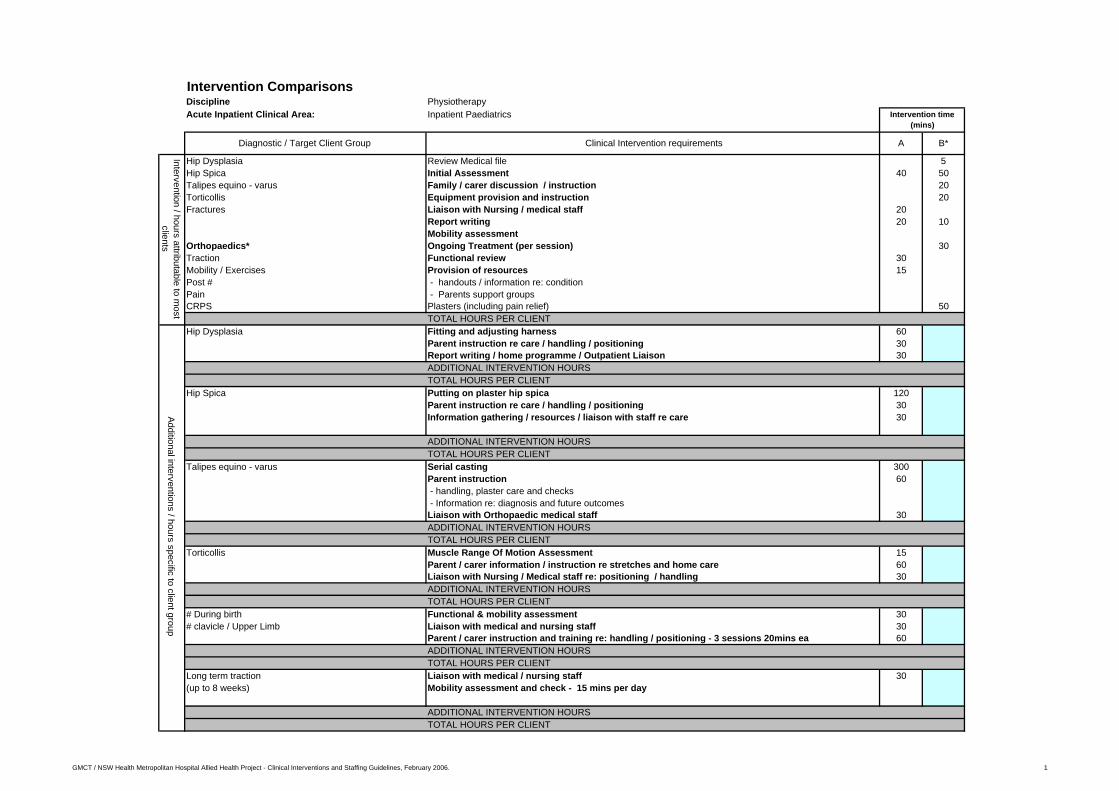
Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: Inpatient Paediatrics
Hip Dysplasia Review Medical file 5Hip Spica Initial Assessment 40 50Talipes equino - varus Family / carer discussion / instruction 20Torticollis Equipment provision and instruction 20Fractures Liaison with Nursing / medical staff 20
Report writing 20 10Mobility assessment
Orthopaedics* Ongoing Treatment (per session) 30Traction Functional review 30Mobility / Exercises Provision of resources 15Post # - handouts / information re: conditionPain - Parents support groupsCRPS Plasters (including pain relief) 50
TOTAL HOURS PER CLIENTHip Dysplasia Fitting and adjusting harness 60
Parent instruction re care / handling / positioning 30Report writing / home programme / Outpatient Liaison 30ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Hip Spica Putting on plaster hip spica 120Parent instruction re care / handling / positioning 30Information gathering / resources / liaison with staff re care 30
ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Talipes equino - varus Serial casting 300Parent instruction 60 - handling, plaster care and checks - Information re: diagnosis and future outcomesLiaison with Orthopaedic medical staff 30ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Torticollis Muscle Range Of Motion Assessment 15Parent / carer information / instruction re stretches and home care 60Liaison with Nursing / Medical staff re: positioning / handling 30ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
# During birth Functional & mobility assessment 30# clavicle / Upper Limb Liaison with medical and nursing staff 30
Parent / carer instruction and training re: handling / positioning - 3 sessions 20mins ea 60ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Long term traction Liaison with medical / nursing staff 30(up to 8 weeks) Mobility assessment and check - 15 mins per day
ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Intervention time (mins)
Diagnostic / Target Client Group Clinical Intervention requirements B*A
Intervention / hours attributable to most
clientsAdditional interventions / hours specific to client group
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Discipline PhysiotherapyAcute Inpatient Clinical Area: Inpatient Paediatrics (continued)
Respiratory Review medical file 15 5Cystic Fibrosis Initial Assessment 40 20
Daily Treatment 60 - Postural drainage / P & V / PEP / Exercises / education - x2 30min sessions per day
Asthma Liaison wih medical staff 20Education to parents / Nursing Staff 15
Pnuemonias report writing 20 5functional review 30Written Programsresource gathering 15TOTAL HOURS PER CLIENT
Cystic Fibrosis Postural drainage & chest Physio - 2x per day for 30minsExercise assessment 30Exercise programme outline / Instruction - once per day for 15minutesParent / carer instructions 60Patient instruction / p.d. Breathing techniques - 2x per day for 15minsLiaison with community health / support services 30Report writing - 2x per day for 5 minutesADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Asthma Postural drainage & chest Physio - 2x per day for 30mins 60Exercise assessment 30parent / carer instruction / demonstration of techniques 60patient instruction re equipment 30report writing 30liaison with medical / nuring staff 60ADDITIONAL INTERVENTION HOURSTOTAL HOURS PER CLIENT
Pnuemonias Postural drainage & chest Physio - 2x per day for 20mins 40Instruction re breathing techniques 30Parent / carer instructons 30TOTAL HOURS PER CLIENT
Developmental Review of medical file and initial assessment 30Review of medical file 5Initial Assessment 50
Neglect / Abuse Developmental assessment 60Liaison with medical / nursing staff 120
With associated conditions admitted for Case conferences 1 hour x 2 - clinical & review / discharge 120medical surgical reasons Patient intervention 20mins daily
Ongoing Treatment (per session) 30Education to parents / nursing staff 20Parent / carer instructionGathering and provision of equipment / play resources 30Instruction re: use of equipment to parent / carer / menidcal / nursing staff 30Report writing 60Written programmes 20Daily file review - 10mins per dayDaily report writing - 5 minutes per dayReferral / Liaison with community resources 60TOTAL HOURS PER CLIENT
A B*
Intervention / hours attributable to m
ost clients
Intervention time (mins)
Clinical Intervention requirements
Additional interventions / hours specific to client groupIntervention / hours attributable to m
ost clients
Diagnostic / Target Client Group
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2
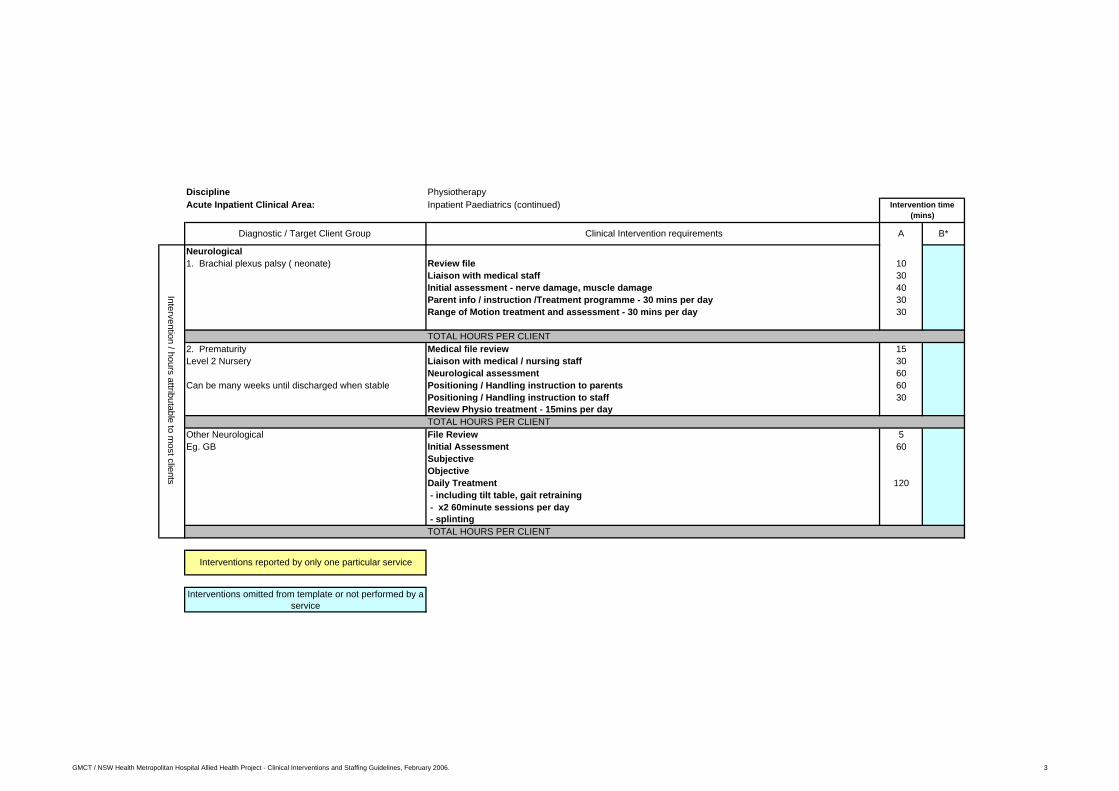
Discipline PhysiotherapyAcute Inpatient Clinical Area: Inpatient Paediatrics (continued)
Neurological1. Brachial plexus palsy ( neonate) Review file 10
Liaison with medical staff 30Initial assessment - nerve damage, muscle damage 40Parent info / instruction /Treatment programme - 30 mins per day 30Range of Motion treatment and assessment - 30 mins per day 30
TOTAL HOURS PER CLIENT2. Prematurity Medical file review 15Level 2 Nursery Liaison with medical / nursing staff 30
Neurological assessment 60Can be many weeks until discharged when stable Positioning / Handling instruction to parents 60
Positioning / Handling instruction to staff 30Review Physio treatment - 15mins per dayTOTAL HOURS PER CLIENT
Other Neurological File Review 5Eg. GB Initial Assessment 60
SubjectiveObjectiveDaily Treatment 120 - including tilt table, gait retraining - x2 60minute sessions per day - splintingTOTAL HOURS PER CLIENT
Interventions omitted from template or not performed by a service
Intervention / hours attributable to most clients
Interventions reported by only one particular service
Intervention time (mins)
Diagnostic / Target Client Group Clinical Intervention requirements A B*
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 3

Intervention ComparisonsDiscipline PhysiotherapyClinical Area: Outpatients
Initial assessment / treatment session Referral received Y Receiving referrals,taking details , New patient Initial assessment 20 N making bookingChronic / complex issues - Investigations eg. CT, Xray , MRI NLower back pain - Subjective assessment N
- Objective assessment N*Musculoskeletal conditions - Treatment planning / goal setting N*Arthritis Treatment Y Assistance with supervision of exercises*Pain - eg. Traction, mobilisation, exercises, respiratory techniques Under instruction from Physio*Maternity Problems - Advice, education , handouts*Respiratory - Manual therapy 10 - COPD - Exercise programme 15 - CF - Scar management 10 - pnuemonia - post treatment measurement 5
Liaising with medical team 10 NReports / Discharge letters 10 N
Interpreter required Use of interpreter to complete above 10 - 15Bookings dependent upon availabilityTOTAL HOURS PER CLIENT
New patient Referral received(Post surgical) Investigations / Check Protocol NOrthopaedics Subjective assessment N# Humerus Treatment
- planning / Goal setting - exercise prescription, sling provision - Advice, printing / drawing exercises
TOTAL HOURS PER CLIENTFollow up Assessment / Treatment Review assessment 30 5 30 NLower back pain Subjective assessment 30
Objective assessmentTreatment planningTreatment - eg. Traction, mobilisation, exercises, - Advice, education , handouts - Electrotherapy - Manual therapy - Exercise programmePost treatment measurement 5Correspondence with referring Doctors re progress at Discharge 15 - letter / phoneNotes 10
NESB Use of interpreter to complete above 15Interpreter required Bookings dependent upon availability
TOTAL HOURS PER CLIENTFollow up Review assessment N( Post Surgical) Subjective assessment
Objective assessmentTreatment - planning - eg. Traction, mobilisation, exercises, - Advice, education , handoutsNotes
30
E
Additional interventions / hours specific to client group
35
Clinical Intervention requirements
6060
Diagnostic / Target Client Group
Intervention / hours attributable to most clients
Intervention / hours attributable to m
ost clients
Intervention time (mins)
C D
60 60
B*A
60
30
45
30
Please QualifyDC
Technical Assistant (Y/N)
BA
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 1

Intervention Comparisons
Discipline PhysiotherapyClinical Area: Outpatients (Continued)
Respiratory Respiratory techniques 10 - CAL - deep breathing exercises 10 - asthma - postural drainage 15
- Bubble PEP 10 - bronchiectasis - percussion - pnuemonia - vibration
- Forced Expiratory technique - education including carer 10
Neurological Initial assessment 60CVA Treatment per session 30 30 60 30Gait & balance disorder
Poor balanceCo-ordinationDe-conditioned
Amputees
Applying splints eg. ROM Brace, corsets,belts,collars,slings 10 30 N
Hands Initial assessment 60 NSplinting 50Treatment per session 30Hands - splint adjustment 20 20
NESB Use of interpreter to complete above 10Interpreter required Bookings dependent upon availability
NESB Additional time may be required if patient of NESB 10in absence of interpreter and interpreter not present
Aging clients Additional time required 10ie. getting dressed / undressed, mobility
POP Application Referral received Yor Splinting Preparation of materials & room Y
Application of splint or POP Y Only to assist PTAdvice on skin care / precautionsRebook for removal and reviewDocumentationTOTAL HOURS PER CLIENT 0.75
Removal Remove POP - provide advice, exit app. / notes 15 15 Y Only to assist PTTOTAL HOURS PER CLIENT 0.25
E
Additional Intervention hours specific to client group
30
Clinical Intervention requirements A BA*
45
Diagnostic / Target Client Group Please Qualify
Intervention time (mins) Technical Assistant (Y/N)
C*** D C DB**
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 2

Intervention Comparisons
Discipline PhysiotherapyClinical Area: Outpatients (Continued)
Group Work Contacting patients 60 YAssessment for group see below NPreparation / Organising equipment etc 15 YRunning group session see below Y With supervisionRecording group activities in records 15Post group assessment 20 mins per patient see below Y With PhysiotherapistTOTAL HOURS PER GROUP SESSION 1.5
Able & Stable' Falls prevention x8 1 hour sessions + 4 hours of education + interventions above Y With training & supervisionTOTAL HOURS PER GROUP
Back 90mins per week for 6 weeks + 1hour initial assessment Y With training & supervision + interventions aboveInitial assessment 60 NWeekly exercise programme 2 x per week 60 YTOTAL HOURS PER GROUP
Neck 90mins per week for 6 weeks + 1hour initial assessment Y With training & supervision + interventions aboveTOTAL HOURS PER GROUP
Knee 90mins per week for 6 weeks + interventions above Y With training & supervisionTOTAL HOURS PER CLIENT
Open Gym Assessment for group (per client ) 20 NAssessment for Discharge (per client) 20 Y With PhysiotherapistTOTAL HOURS PER CLIENT1 hour per week for 12 weeks + interventions above 60 Y With training & supervisionTOTAL HOURS PER GROUP SESSION
Pulmonary Rehab Initial assessment 60 NExercise Programme 2 x per week 90 YTOTAL HOURS PER CLIENT
Cardiac Rehabilitation Initial assessment 30 Nfor post MI / Stent / Bypass / VR Exercise programme 2 x per week 120 Y
Initial assessment 20Exercise Programme - 1.5 hours 2 times per week 180 Y T/A assists under supervision of PT and CNCCardiac walk - 1.5 hours per week 90 Y 2 staff required for safetyTOTAL HOURS PER CLIENT
Falls Group Initial assessment 60 NWeekly exercise programme 90 YTOTAL HOURS PER CLIENT
Lower Limb group Initial assessment 60 NExercise programme once per week 60 YTOTAL HOURS PER CLIENT
EMU and ED referral Gait retraining / mobility assessment and management 10 Y Could assist with practise under superv ision Pain / Trauma involving musculoskeletal conditions - re: increasing weight bearing status of PhysioOncologyPain / Mobility management
TOTAL HOURS PER CLIENTHydrotherapy Initial assessment 20for musculoskeletal conditions Exercise Programme - 1 hour 2 times per week Y T/A has qualifications in aquafitness
Operates under supervision of PTTOTAL HOURS PER CLIENT
Respiratory Group class twice per week for 7 weeks, 4 hours per session - pnuemonia per session 240 - emphysema - COPD
TOTAL HOURS PER CLIENT 56Pre-admission Clinic Pre- op assessment 60Pre-op joint replacementsBilateral Mastectomies
TOTAL HOURS PER CLIENTPlaster Clinic Initial assessment and treatment 30 N
TOTAL HOURS PER CLIENT
Interventions omitted from template or not performed by a service
Please Qualify
Groupw
ork interventions
Interventions reported by only one particular service
Clinics
Intervention time (mins)
Diagnostic / Target Client Group
Technical Assistant (Y/N)
Clinical Intervention requirements A* B** C*** D E A DB C
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 3

Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: ICU / HDU
Ventilated Patients Initial Assessment (once only) 30 30 N N - Review medical file 15
Non-ventilated patients - Reviewing X-Rays and Pathology resultsPost Surgical - Reason for admission & previous level of function
Liaise with staff 10 10Respiratory assessment 10 10 10 N NMusculoskeletal Assessment 10Musculoskeletal Treatment 10 20 N - prevention of contractures - prevention of pressure sores - exercise programme 10 NEducation 15Documentation 10 5 5 N NDaily Review / Assessment 10Provision of equipment 15 YTOTAL HOURS PER CLIENT
Non-ventilated patients Mobility Assessments 15 20 15 N - bed transfers - chair transfers - mobility aidsIntervention to improve exercise tolerance 10 NReport writing 10TOTAL HOURS PER CLIENT
Post Surgical Huffing & coughing techniques 10 NTOTAL HOURS PER CLIENT
Long Term patients Tilt Table 60 Y Can assist Physio to transport to dept and treatUsually performed 2-3 x per week
TOTAL HOURS PER CLIENTAcute Respiratory Intervention Spirometry
- pre / post 30 - baseline 15Bubble PEP 5
Acute Respiratory Intervention Sputum Collection 10 NMobilising to improve lung function 15Report writing 10Respiratory Treatments - per day 20 30 20 25 - positioning - Percussion - Vibration - sputum removal - suctioning - Deep Breathing exercisesTOTAL HOURS PER CLIENT
Prevention of musculoskeletal deterioration Musculoskeletal Treatment 10 5 - prevention of contractures - prevention of pressure sores - exercise programmeTOTAL HOURS PER CLIENT
Mobility assessment and training Mobility assessment and training 30 - Sitting out of bed - Standing - AmbulateTilt Table 45TOTAL HOURS PER CLIENT
Splinting 60 Y To assist Physio onlyTOTAL HOURS PER CLIENT
No identified Technical Assistant interventions
Please Qualify
Intervention / hours attributable to most
clients
B D B D
Additional interventions / hours specific to client group
A CA C
Intervention time (mins) Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2005. 1

Intervention ComparisonsDiscipline PhysiotherapyAcute Inpatient Clinical Area: Emergency
Musculoskeletal Review medical file 10#'s requiring crutches / stick Initial assessment 20 nil nil#'s requiring plasters Talk to patient / family 5Acopia Liaison with medical / nursing staff 5Respiratory problems Advice to patient and family 10Falls Referral to ward or outpatient physio 10Seizures Documentation 10CVA's - notes
- Care Plan - PathwayReferral to other disciplines if required 5
On Referral from Emergency staff 4-5 interventions per month each lasting 20 - 120 minutes* 70**Average**Includes - Mobility Review - Equipment Loaning - Arranging follow up outpatient review - Plastering - Occasional Respiratory assessmentsTOTAL HOURS PER CLIENT 75 70
Muskuloskeletal Treatment 15TOTAL HOURS PER CLIENT 90
#'s requiring crutches / stick Gather equipment 5 YFalls Adjust height of equipment 5 YAcopia Teach correct techniqueSeizures stairs 10
Equipment hire policy / paperwork 5ADDITIONAL HOURS PER CLIENT 25TOTAL HOURS PER CLIENT 100
#'s requiring plasters Transport to plaster room 5 YApplication of cast and provision of warnings 20 + / - crutches if applicable 25ADDITIONAL HOURS PER CLIENT 50TOTAL HOURS PER CLIENT 125
Respiratory problems Treatment 20CVA's
ADDITIONAL HOURS PER CLIENT 20TOTAL HOURS PER CLIENT 95
Intervention / hours attributable to most clients
Please Qualify
Additional interventions / hours specific to client group
Interventions omitted from template or not performed by a service
Intervention time (mins) Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements B* A BA
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline PodiatryAcute Inpatient Clinical Area: General Medicine (Diabetes)
T1 T2 Diabetes Myelitis Review file 5 Nwith foot pathology Initiial Assessment / History 10 N
Foot Assessment 10 NFoot Education 10 NReport writing 5 NLetter writing 10 NTreatment (debridement, nail care) 10 N
** Caseload specific InfrastructureStats 2 hours per week YTOTAL HOURS PER CLIENT
Foot Ulcer / Acute Assess wound 20 N Urgent ReviewHigh risk foot Debride wound and apply dressings 10 N
'Off load' wound 10 N
ADDITIONAL HOURS PER CLIENTTOTAL HOURS PER CLIENT
Amputee Assess remaining limb 10 N Outpatient Rehab amputee clinicEducation 5 NADDITIONAL HOURS PER CLIENTTOTAL HOURS PER CLIENT
Intervention / hours atributable to m
ost clientsA
dditional interventions / hours specific to client group
Diagnostic / Target Client Group Clinical Intervention requirements A Please QualifyA
Intervention time (mins)
Technical Assistant (Y/N)
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline PodiatryAcute Inpatient Clinical Area: Aged Care
Frail Aged Review file 5 NInitiial Assessment / History 10 NFoot Assessment 10 NFoot Education 10 NNail care 5 Y After Podiatrist assessment and Corn / Callous debridement 5 N TA staff trainingAppointment booking 5 Y
** Caseload specific InfrastructureStats 2 hours per week Y
TOTAL HOURS PER CLIENT
Intervention / hours atributable to most
clients
A
Intervention time (mins)
Diagnostic / Target Client Group Clinical Intervention requirements Please Qualify
Technical Assistant (Y/N)
A
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline PodiatryAcute Inpatient Clinical Area: Outpatients
Diabetic clients with Pensioner or Initial Assessment including:-Health Care Card entitlements General Palliative care 20 NPaediatric Diabetes - Nailcare, corn and calllous debridingAny person with a foot ulcer Biomechanical assessment ( quick review) 10 N
Further referral 10 NGeneral Paliative Care - eg. booking for possible orthotic therapy or nail surgery
report writing 5 NDatabase stats entry 5 Y Training and supervisionTOTAL HOURS PER CLIENT 0.83
Diabetic Reviews Sensation testing 10 NCirculation testing 10 NDiabetic foot education 10 Y Training approved by Diabetes centreReply letters to GP's etc 10 NADDITIONAL HOURS PER CLIENT 0.67
Ulcer Care Assessment and treatment plan 15 N - Assess wound causes - Determine suitable dressing - Pressure 'off loading' requirementsdigital photography 2 Yredressing 5 NProvide pressure off - loading devices 30 Y Training approved by Diabetes centrereport writing 5 NReply letters to GP's etc 10 NADDITIONAL HOURS PER CLIENT 1.12
Foot in crisis' care Assess and Phone Registrar for review re: hospitalisation 60 Nfor infected foot woundADDITIONAL HOURS PER CLIENT 1
Paediatric Diabetes Full biomechanical assessment 25 NPaediatric sensation / circulation testing 25 NADDITIONAL HOURS PER CLIENT 0.83
Diabetic acute injury Debridement and dressing 20 NADDITIONAL HOURS PER CLIENT 0.33
Injury sports strapping for injury 10 NADDITIONAL HOURS PER CLIENT 0.17
Diabetes Education Groups Group education session 60for newly diagnosed - 60 minutes per session
Travel to Health centres / hospitals
TOTAL GROUP SESSION HOURS 1
Intervention time (mins)
Technical Assistant (Y/N)
Diagnostic / Target Client Group Clinical Intervention requirements A A
Intervention / hours atributable to most
clientsAdditional interventions / hours specific to client group
Please Qualify
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Psychology - NeuropsychologyAcute Inpatient Clinical Area: General Medicine / Aged care / Orthopaedics
Patients with known or suspected Review of medical records 45 NB. No part of the neuropsychological Cognitive Disorder Discussion / Liaison with treating team members 75 assessment proper (file review, interview, due to neurological, other medical re their observations / impressions of the patients hypothesis formulation, test selection, test or psychiatric disorder cognitive, behavioural and emotional status administration, results interpretation, or
**Neuro psychological examination 210 report writing) can be done by a technical Priority is given to cases that require Scoring of test data 60 assistant.neuropsychological evaluation to assist Report Writing 120with immediate medical management Clerical tasks: 90 Y Clerical assistantdecisions, such as diagnosis. - report typingSecond priority given to those - filingrequiring assessment for non-immediate - mailingcare, e.g. discharge planning and Interview of significant others, when available 45Guardianship Tribunal Applications - re patients premorbid and current cognitive , behavioural and emotional status
Post assessment liaison with treating team - re treatment management recommendationseg.Advice regarding behavioural management Advice about Guardianship
** Recommendation for other consultant involvement eg. neurology , psychologyGeneral medicine Assessment of coping styles / self esteem / grief & loss 75 Y *Clinical intern psychologist under supervisionAdjustment / Cognitive / Psychological intervention 225 Y Pain Management - aimed at facilitating adjustmentBehaviour Management Report / file note writing 105 Y Drug & alcohol issues Liaison with other staff 35 Y
-Feedback on results provided re identified deficits - Implications for treatment
Patients suspected of having Cognitive / Perceptual impairment - capacity to return to work - ability to drive - ability to manage finances - Adcvice re medicolegal issues re Power of attorney, testimetric capacityor guardianshipReferral out 20 Y TOTAL HOURS PER CLIENT 10.75 7.67
Stroke / Aged Care / Rehab Cognitive assessment (ADASCOG) 60Adjustment / - required for authority to prescribe anti - dementia drugsMood & anxiety disorder Assessment specific to presenting problem 60Pain Management - ie. mood / anxiety disorderBehaviour Management - This will include file review and gathering information from other staff
Liaison with other staff 35 -Feedback on results provided re identified deficits
Grief & Loss - Implications for treatmentDrug & Alcohol issues - capacity to return to workPatients suspected of having Cognitive / Perceptual impairment - ability to drive
- ability to manage finances - Adcvice re medicolegal issues re Power of attorney, testimetric capacityor guardianshipDesign treatment program 45Carrying out treatment program 145 Y Once the program is designed it can be Educate families / carers re management strategies carried out by other disciplinesTOTAL HOURS PER CLIENT 5.75Differential diagnosis 115 - Assessment of depression and dementiaTOTAL HOURS PER CLIENT 1.92Formal psychological assessment 90 - includes formal report and / or case reviewTOTAL HOURS PER CLIENT 1.5
Guardianship Tribunal Hearings Phone interview or attendance at Guardianship Tribunal Hearings 53re applications for a Guardian &/or Financial ManagerADDITIONAL HOURS PER CLIENT 0.88TOTAL HOURS PER CLIENT 11.63
Intervention time (hrs) Technical Assistant (Y/N)
Intervention / hours attributable to most clients
AA
Additional interventions / hours specific to client group
Interventions reported by only one particular service
Please QualifyB**Targeted Client Group Clinical Intervention requirements B
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006 1

Intervention Comparisons
Discipline Psychology - NeuropsychologyAcute Inpatient Clinical Area: Outpatients - Hospital Based
Arrangement of appointment by phone, 30 Y Could be done by a clerical assistanttyping and sending of formal appointment letter
Patients with known or suspected Review of medical records 45 N NB. No part of the neuropsychological Cognitive Disorder Discussion / Liaison with treating team members 75 assessment proper (file review, interview, due to neurological, other medical re their observations / impressions of the patients hypothesis formulation, test selection, or psychiatric disorder cognitive, behavioural and emotional status test administration, results interpretation
**Neuro psychological examination 210 N or report writing)can be done by a technical Priority given to cases that require Scoring of test data 60 N assistant***neuropsychological evaluation to assist Report Writing 120 Nwith immediate medical management Clerical tasks: 90 Y Could be done by a Clerical assistantdecisions, such as diagnosis. - report typingSecond priority given to those - filingrequiring assessment for non-immediate - mailingcare ie. Discharge planning and Interview of significant others, when available 45 NGuardianship Tribunal Applications - re patients premorbid and current cognitive , behavioural and emotional status
Post assessment liaison with treating team N - re treatment management recommendationseg.Advice regarding behavioural management Advice about Guardianship
** Recommendation for other consultant involvement eg. neurology , psychologyPost Natal Depression Assessment - Diagnosis 120 Y *Clinical Intern psychologist under supervisionPain Management Brief treatment intervention 75 YVarious Psychiatric Diagnoses Referral - liaison including report 35
TOTAL HOURS PER CLIENT 11.25 3.83Guardianship Tribunal Hearings Phone interview or attendance at Guardianship Tribunal Hearings 50 N
re applications for a Guardian &/or Financial Manager
ADDITIONAL HOURS PER CLIENT 0.83TOTAL HOURS PER CLIENT 12.08
Cardiac Rehabilitation Group Education 1 hour Lecture provided on the psychological consequences of heart disease 4 N3-4 times per year and infarction
Number of sessions TOTAL SESSION HOURS 4
Targeted Client Group Clinical Intervention requirements
Other
interventions
Additional interventions
specific to client group
Intevention / hours attributable to most clients
B**A
Intervention time (hrs)
B*
Technical Assistant (Y/N)
Interventions reported by only one particular service
A*** Please Qualify
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006 2

Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: Aged Care
Technical assistant
Seen on referral Gathering Information / reading medical file / old notes 2065+ Initial Psychosocial Assessment with patient and family 120
- Assessment of home, family, financial situation, social activitiesDementia / Delirium - emotional issues
- Services, concerns / issues - Liaison with aged care facility &/or services re pre-morbid function 60 20
Social Issues:- Provide support to Patient & /or family / carer 120Not manageing at home - May include poor prognosis, dementia, placement, grief & lossCarer Stress - Counselling for a transitional stage in life 60Family Conflict Facilitate communication Grief & Loss - transfer of information between medical team / family / patient - Partner /other significant - Advocacy - Function - Diffuse frustration with the system - Independence - Education of processes 35
Complex discharge planning referrals 60 210Living alone with other risk factors Discharge Planning and organisation 60
- Referrals to packages of care 60 - Liaison with medical team / other staff 30 - Handover to other wards / hospitals on patient transfer 30
any combination of the above - liaison with other services eg. Mental Health, Community Nursing, Residential Care facilities 60*NB Complex discharge planning is referred to designated Discharge Planner positionTOTAL HOURS PER CLIENT 4 13 8 3 3 6
Family Conference* Review filesLiaise with medical team and arrange conferenceAttending and facilitating conference - Supporting and resourcing family - Assess family dynamics and emotional needsADDITIONAL HOURS PER CLIENT 2 3
Residential Placement
Liaise with family and Aged Care facility to secure placement 120Liaise with staff re Discharge 30Review of client / ACCR / Assessment / Liaison with team 180 180Family conference arrangements and attendance 60 60Family and client support as able 60 60Phonecalls to locate vacancy 30 30Discussion with patient / family re decision in liaison with medical teamCheck re financial situationReferral to Aged Care Residential Consultancy ServiceFurther liaison if necessaryInformation re new Asset testADDITIONAL HOURS PER CLIENT 3 5.5 3.75 3.75 5.5
60
210
9090 180
60
90 - 360
180180
225
NB. Processing of application for residential placement completed by ARCCS Social Work involved more re liaising with patient / family/ medical team. Explaining the process and supporting patient and family as above.
240
180120
Clinical Intervention requirements
Intervention time (mins)
A* B C D E FTarget Client Groups
Intervention Hours attributable to m
ost clientsAdditional Intervention hours specific to client group
GMCT/NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions Staffing Guidelines, February 2006. 1
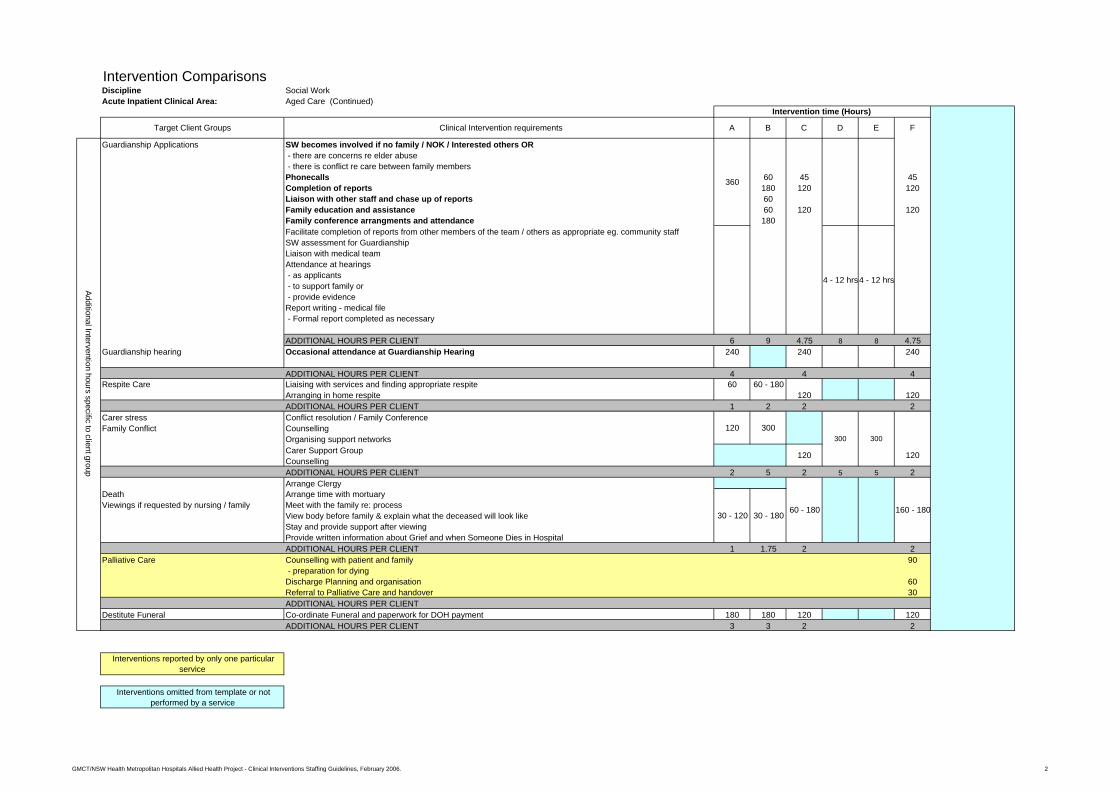
Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: Aged Care (Continued)
Guardianship Applications SW becomes involved if no family / NOK / Interested others OR - there are concerns re elder abuse - there is conflict re care between family membersPhonecalls 60 45 45Completion of reports 180 120 120Liaison with other staff and chase up of reports 60Family education and assistance 60 120 120Family conference arrangments and attendance 180Facilitate completion of reports from other members of the team / others as appropriate eg. community staffSW assessment for GuardianshipLiaison with medical teamAttendance at hearings - as applicants - to support family or - provide evidenceReport writing - medical file - Formal report completed as necessary
ADDITIONAL HOURS PER CLIENT 6 9 4.75 8 8 4.75Guardianship hearing Occasional attendance at Guardianship Hearing 240 240 240
ADDITIONAL HOURS PER CLIENT 4 4 4Respite Care Liaising with services and finding appropriate respite 60 60 - 180
Arranging in home respite 120 120ADDITIONAL HOURS PER CLIENT 1 2 2 2
Carer stress Conflict resolution / Family ConferenceFamily Conflict Counselling
Organising support networksCarer Support GroupCounsellingADDITIONAL HOURS PER CLIENT 2 5 2 5 5 2Arrange Clergy
Death Arrange time with mortuaryViewings if requested by nursing / family Meet with the family re: process
View body before family & explain what the deceased will look likeStay and provide support after viewingProvide written information about Grief and when Someone Dies in HospitalADDITIONAL HOURS PER CLIENT 1 1.75 2 2
Palliative Care Counselling with patient and family 90 - preparation for dyingDischarge Planning and organisation 60Referral to Palliative Care and handover 30ADDITIONAL HOURS PER CLIENT
Destitute Funeral Co-ordinate Funeral and paperwork for DOH payment 180 180 120 120ADDITIONAL HOURS PER CLIENT 3 3 2 2
Interventions omitted from template or not performed by a service
120 300
60 - 18030 - 120 30 - 180
120
160 - 180
300
120
360
FC
4 - 12 hrs
300
4 - 12 hrs
E
Intervention time (Hours)
A B D Clinical Intervention requirements
Interventions reported by only one particular service
Additional Intervention hours specific to client group
Target Client Groups
GMCT/NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: General Medical
CVA (Blanket referral) Gathering information / reading medical file 20 15 15 15Psychosocial assessment - Patient 60 60 60 60Liaison with existing support network 60
General Medical clients Liaison with ward staff eg. OT, PT, Dietician, Nursing, Medical staff 30with emotional issues, Care Planning 20 30 30social isolation or other Supportive Counselling eg. loss 60support needs Education / information re: impact of illness, emotional issues 60
Family support 315 - assessment - counselling - Liaison between family and medical teamFollow up with patient/ client / family 30Referral to community support services 45Writing in medical file 20 20Referral and Discharge planning 60Report writing / letters 60TOTAL HOURS PER CLIENT
Family Conference Review files 180Liaise with medical team and arrange conferenceAttending and facilitating conference - Supporting and resourcing family - Assess family dynamics and emotional needsTOTAL HOURS PER CLIENT
Guardianship issues / applications Phonecalls 45 45completion of reports 120 120liaison with other staff and chase up of reportsFamily education and assistance 120 120Family conference arrangements and attendanceoccasional attendance at Guardianship Hearings 240 240TOTAL HOURS PER CLIENT
Nursing Home Placement Review of client / Complete 3020 ( Aged Care Client Record ) 60Hostel Placement - As above + assessment and liaison with team 180 180
Family conference arrangements and attendance 90 60 60Education of junior medical staff of processes 30Education / Counselling of client and family 120Referral to ACAT for 3020 approval 10Liaise with family and Aged Care Facility to secure placement 120Liaise with staff re: Discharge 30Family and client support as able 60 60Phonecalls to locate vacancy 30 30Hostels-take patient for hostel assessments 120TOTAL HOURS PER CLIENT
Technical assistant
480
180
60
600
180
480
225
Intervention time (mins)
Target Client Groups Clinical Intervention requirements A B C D E F
Intervention Hours attributable to m
ost clientsIntervention H
ours attributable to client group
60
480
225
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Discipline Social WorkAcute Inpatient Clinical Area: General Medical (Continued)
Palliative Care Bereavement issues 120 120New Diagnosis Counselling re: coming to terms with diagnosis, impact, emotional issues
Family supportliaison with ward staffSupport for NFR ordersReferral OutDischarge Planning - Transport to private hospital - Arranging services - Referral to Palliative care team - Provision of information re: funerals - Liaison with ward , medical staffTOTAL HOURS PER CLIENT
Destitute Funeral Psychosocial / Financial assessment 120 120Co-ordinate Funeral and paperwork for DOH paymentTOTAL HOURS PER CLIENT
Oxygen Arrange through PADP 60 60
TOTAL HOURS PER CLIENTYoung Disabled Assessment 45
Accommodation 40Practical assistance 45counselling 45Case Management 40Liaison with services 40Support for family 30TOTAL HOURS PER CLIENT
270
Intervention time (mins)
A B C
270
E
120120
270
D
Interventions reported by only one particular service
Intervention Hours attributable to client group
Target Client Groups Clinical Intervention requirements
Interventions omitted from template or not performed by a service
F Technical assistant
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: Orthopaedics
Aged Care Family support 90 No identified role - particularly for out of area clients
Dementia / Delirium with Liaison between family and medical team Family meetings 45 45broken bones Psychosocial assessment 60
Discharge planning , referral to servicesTraumas via ED Accommodation for relatives
Assistance through IPTAASFinancial assistance
*electives tend not to be seen issues identified at preadmission -accommodation prior to booked procedure for country patientsliaison with ward staffreport writingTOTAL HOURS PER CLIENT
Family Conference 75TOTAL HOURS PER CLIENT
Fiancial issues / Centrelink Fiancial issues / Centrelink 45 45TOTAL HOURS PER CLIENT
Accommodation issues / Homeless Initial interview with client re: social situation 90 90Locating accommodation - liaison with Department of Housing - Contacting the Homeless persons lineLiaison with Mental HealthDrug & Alcohol issuesreport writingTOTAL HOURS PER CLIENT
Workers Compensation Liaison with employer, insurance company 40 40Inform patient of rights and processesTOTAL HOURS PER CLIENT
Need for Community services Arranging services / packages eg. COMPACKS 45 45TOTAL HOURS PER CLIENT
Patient with private health insurance Liaison with private hospital for transfer to Respite / Rehab 60requiring Rehab
TOTAL HOURS PER CLIENTYoung person intervention Psychosocial assessment 120 120
TOTAL HOURS PER CLIENTChronic Pain Psychosocial assessment 60 60
TOTAL HOURS PER CLIENTAged Care Residential Placement Review of client / ACCR / Assessment / Liaison with team 180Nursing Home Placement Family conference arrangements and attendance 60Hostel Placement Family and client support as able 60
Phonecalls to locate vacancy 30Hostels-take patient for hostel assessments 120
Intervention hours specific to client group
Interventions reported by only one particular service
Interventions omitted from template or not performed by a service
Technical assistant
Intervention / hours attributable to most clients
Intervention time (mins)
Target Client Groups Clinical Intervention requirements A B
90
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: Paediatrics
Technical assistant
Child / Family Gathering information / reading medical file 45 No identified rolewith emotional issues, Psychosocial assessment 75social isolation or other Provide support to Patient & /or family / carersupport needs - May include poor prognosis, grief & loss
Supportive Counselling eg. loss - as above per day 45
Social Issues:- Care PlanningNot manageing at home Education / information re: impact of illness, emotional issueCarer Stress Discharge Planning and organisationFamily Conflict Liaison with medical team / other staff eg. OT, PT, Dietician, N
- as above per day 15Grief & Loss Handover to other wards / hospitals on patient transfer - Partner /other significant liaison between family and medical team - Function Follow up with patient/ client / family - Independence Referral outany combination of the above report writing
Liaison with other agencies (per day) 45 - eg. Mental Health, Drug and Alcohol, DOCS - Support letters and advocacyTOTAL HOURS PER CLIENT
Child protection Child at risk assessments 180DOCS reportLiaison with doctor and nursing staffreport writingLiaison with DOCS & JIRT*Case ManagementCommunity Follow Up 45TOTAL HOURS PER CLIENT
Child with disability Psychosocial assessment 330 180or chronic medical Supportive counsellingcondition Liaison with community resources/ supports
Liaison with medical team / doctorInformation re: Centrelink entitlementsLiaison work with multidisciplinary teamAdvocacy for patients / familiesTOTAL HOURS PER CLIENT
150
Intervention time (mins)
Target Client Groups Clinical Intervention requirements A B C D
Intervention Hours attributable to client group
Intervention Hours attributable to m
ost clients
180
450
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Discipline Social WorkAcute Inpatient Clinical Area: Paediatrics (Continued)
Long term hospitalisations Psychosocial assessment 210 No identified roleSupportive counsellingPractical assistanceTOTAL HOURS PER CLIENT
Families needing Psychosocial assessmentPractical assistance Liaison with community servicesSupport - accommodation, child care 90
TOTAL HOURS PER CLIENTNew Diagnosis Psychosocial assessment
Supportive CounsellingLinks to servicesTOTAL HOURS PER CLIENT
NET transfers to other Support for family / parents 300hospitals (Paediatric) Liaise with Doctors
Liaise with Social Worker at receiving hospitalTOTAL HOURS PER CLIENT
Parental AssessmentRelationship Issues Counselling
TOTAL HOURS PER CLIENTYoung person AssessmentDrug & Alcohol Issues Counselling
ReferralTOTAL HOURS PER CLIENT
NAS Babies Ongoing Assessment of parenting skills 360+Child Protection as aboveDischarge Planning
TOTAL HOURS PER CLIENTEating Disorders 300
TOTAL HOURS PER CLIENTSelf Harming Behaviour 300
TOTAL HOURS PER CLIENT
Interventions omitted from template or not performed by a service
Technical assistant
Intervention Hours attributable to client group
150
120
Target Client Groups Clinical Intervention requirements A B
90300
150
Intervention time (mins)
C D
Interventions reported by only one particular service
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: ICU
Withdrawal of life support Family conference with Intensivist 45 No identified role Counselling post conference 75TOTAL HOURS PER CLIENT
Extended stay in ICU Assessment with patient and family 90 Staff working in ED - work issues must be highly skilled - practical issues - Income / financial issues - counselling / support - sourcing practical needs
Follow up of identified issues variable
TOTAL HOURS PER CLIENTBereavement Family support 90
Assistance with funeral arrangements
TOTAL HOURS PER CLIENTPost Surgical Information gathering for family + advocacy 150Complications
TOTAL HOURS PER CLIENTUnidentified Patient Liaison with Police 120
Follow up contacts on Medical record if anyTOTAL HOURS PER CLIENT
TRAUMA Review medical file 15Mental Health Psychosocial assessment 50Drug & Alcohol Speak to family / significant other 30Child at Risk Liaison with medical team 20Domestic Violence Supportive Counselling 35Assault Providing information / education 20Death Explaining hospital process 10Homeless Making Appropriate referrals / handover 30New Diagnosis - ward staffAcute Illness - community agenciesGeriatrics - Allied HealthVictims of Crime Report / Note writing 20Womens Health Gathering resources 10Chronic Illness - not copingCarer StressPalliative Care
TOTAL HOURS PER CLIENTFamily Conference Review files 10
Liaise with medical team and arrange conference 40Attending and facilitating conference 60 - Supporting and resourcing family- Assess family dynamics and emotional needsTOTAL HOURS PER CLIENT
Homeless Assessment re social situation 30Investigation of possible alternatives for accommodation 30 - ie. Family / friendsLiaison with Homeless Persons Helpline 30Liaison with Dept of Housing 20Locating assistance with finances 30Locating assistance with transport 20Report writing 20Liaison with Mental HealthDrug and Alcohol issuesTOTAL HOURS PER CLIENT
Technical assistant
Intervention hours attributable to most clients
Target Client Groups BA Clinical Intervention requirements
Interventionl hours specific to client groupIntervention hours specific to client group
Intervention time (mins)
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Discipline Social WorkAcute Inpatient Clinical Area: ICU (continued)
Domestic Violence Assessment 30 No identified role Assualt Counselling and debriefing 30Victims of Crime Providing information 30
Liaison and referral to appropriate services 60 Staff working in ED - Police, Family support, Court, DOCS, Victims of Crime Bureau, Domestic Violence services etc. must be highly skilledReport writing 30TOTAL HOURS PER CLIENT
Geriatric Comprehensive assessment 60Chronic Illness - Ascertain supports, service involved (family & community)Carer Stress Cognitive assessments / GDS 20
Liaison with team and referral 30 - ACAT, GPs, CNs, Homecare etc - Allied HealthCare Planning / Discharge Planning 20Report writing 30Respite Care for aged partner or childreferral to community Carers Support GroupTOTAL HOURS PER CLIENT
Mental Health Review files 10& Liaise with Medical, &/or Mental Health & Drug & Alcohol teams 20Drug & Alcohol Follow up if social work assistance required
- Accommodation (see homeless) - Family support 35Referral to other agencies eg DOCS 60Report writing 20TOTAL HOURS PER CLIENT
Crisis Aspect Review file 10TRAUMA Crisis Intervention 120 - MVA - Liaise with family - Drowning - Supportive Counselling - Heart Attack Liaise with medical staff 30 - Sick Young People Provision of information 30 - Burns Handover to staff - including ward or other hospital 10 - OD's Report writing 20
TOTAL HOURS PER CLIENTDeath Review file 10including SIDS Liaise with family 30Miscarriage Provide Supportive Counselling 60
Facilitate viewing 90Provision of information 20 - procedures, funeralsReport writing 20TOTAL HOURS PER CLIENT
If Coroner involvement Liaison with Police, Medical staff, family 30Provision of resources 10Report writing 20TOTAL HOURS PER CLIENT
Interventions reported by only one particular service
Interventions omitted from template or notperformed by a service
Technical assistantTarget Client Groups BA Clinical Intervention requirements
Intervention Hours specific to client group
Intervention time (mins)
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Intervention ComparisonsDiscipline Social WorkAcute Inpatient Clinical Area: Emergency
TRAUMA Review medical file 15 No identified role Mental Health Psychosocial assessment 50Drug & Alcohol Speak to family / significant other 30Child at Risk Liaison with medical team 20 Staff working in ED Domestic Violence Supportive Counselling 35 must be highly skilledAssault Providing information / education 20Death Explaining hospital process 10Homeless Making Appropriate referrals / handover 30New Diagnosis - ward staffAcute Illness - community agenciesGeriatrics - Allied HealthVictims of Crime Report / Note writing 20Womens Health Gathering resources 10Chronic Illness - not copingCarer StressPalliative Care
TOTAL HOURS PER CLIENTFamily Conference Review files 10
Liaise with medical team and arrange conference 40Attending and facilitating conference 60 - Supporting and resourcing family - Assess family dynamics and emotional needsTOTAL HOURS PER CLIENT
Suspected child abuse Liaison with doctorChild at risk assessmentsDOC's reports - via telephoneLocating accommmodation as appropriate
& discharge prior to SW assessment Completion of DOCs report for inclusion on file 10 10 10 10Case Management with DOCSLiaison with policeTOTAL HOURS PER CLIENT
Homeless Assessment re social situation 30 90 60 60 90 90 90Investigation of possible alternatives for accommodation 30 - ie. Family / friendsLiaison with Homeless Persons Helpline 30 25 25Liaison with Dept of Housing 20Locating assistance with finances 30Locating assistance with transport 20Report writing 20 20 20 20 20 20 20Liaison with Mental HealthDrug and Alcohol issuesTOTAL HOURS PER CLIENT
Domestic Violence Assessment 30Assualt Counselling and debriefing 30Victims of Crime Providing information 30
Liaison and referral to appropriate services 60 - Police, Family support, Court, DOCS, Victims of Crime Bureau, Domestic Violence services etc.Report writing 30
Domestic Violence CounsellingAccommodation / refugePolice liaisonChild protectionfamily liaisonreport writingSupport for clientLiaison with Doctor / PoliceLiaison with local Domestic Violence Community ServicesPossible DOCS notificationAssistance with crisis accommodation / Dept of HousingTOTAL HOURS PER CLIENT
Interventionl hours specific to client group
150
30
210
45
Intervention time (mins)
G
240
240
150
30
180 150 150
45
240
Technical assistantC D E F
Intervention hours attributable to most clients
Target Client Groups BA Clinical Intervention requirements
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 1

Discipline Social WorkAcute Inpatient Clinical Area: Emergency (continued)
Geriatric Comprehensive assessment 60 No identified role Chronic Illness - Ascertain supports, service involved (family & community)Carer Stress Cognitive assessments / GDS 20
Liaison with team and referral 30 Staff working in ED - ACAT, GPs, CNs, Homecare etc must be highly skilled - Allied HealthCare Planning / Discharge Planning 20Report writing 30Respite Care for aged partner or child 90referral to community Carers Support Group
Aged Care Psychosocial assessment - Mental health / cognitive assessment - Case management - Liaisaon with ACAT re: placement - Liaising with family / Providing support - CounsellingTOTAL HOURS PER CLIENT
Mental Health Review files 10& Liaise with Medical, &/or Mental Health & Drug & Alcohol teams 20Drug & Alcohol Follow up if social work assistance required
- Accommodation (see homeless) - Family support 30 - 40Referral to other agencies eg DOCS 60Report writing 20
Drug & Alcohol AssessmentLinking / referring to D & A servicesCounsellingTOTAL HOURS PER CLIENT
Suicide Attempt Assessment - Risk and PsychosocialCounsellingFollow - UpReferral TOTAL HOURS PER CLIENTReview file 10
Crisis Aspect Crisis Intervention 120TRAUMA - Liaise with family - MVA - Supportive Counselling - Drowning Liaise with medical staff 30 - Heart Attack Provision of information 30 - Sick Young People Handover to staff - including ward or other hospital 10 - Burns Report writing 20 - OD's Family support particularly for out of area clients
Locating significant othersLiason between the treating staff and family membersCrisis arrangements eg child care, dependents, respiteArrangement of ongoing supportLiaison with Tertiary referral hospitalLiaison with Police and ambulanceTOTAL HOURS PER CLIENT
Technical assistant
Intervention hours specific to client group
15
150
120
180
90
90
G
Intervention time (mins)
150150 150
15
150
15
150
20 20
FTarget Client Groups B C D EA Clinical Intervention requirements
90
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 2

Discipline Social WorkAcute Inpatient Clinical Area: Emergency (continued)
Death Review file 10including SIDS Liaise with family 30Miscarriage Provide Supportive Counselling 60
Facilitate viewing 90Provision of information 20 - procedures, funeralsReport writing 20Family support particularly for out of area clientsViewings of deceased (increased time for larger families/no.s)Support parents/ children re viewing with child death - mortuary (increased time to arrange appointments)Police identification , explain role of the CoronerLocate clergy - otherLiason with the Coroners Office CounsellorsCounselling- Grief and LossProvision of information and arrangement of follow-upTOTAL HOURS PER CLIENT
If Coroner involvement Liaison with Police, Medical staff, family 30Provision of resources 10Report writing 20TOTAL HOURS PER CLIENT
New diagnosis Counselling 45 60 90 90 90eg. tumours, Cancer Handover to ward staff 15 15
TOTAL HOURS PER CLIENTASET Team Psychosocial assessment 30(Aged Services Emergency Team) Follow up services 90
TOTAL HOURS PER CLIENT**NET transfers to other Support for family / parentshospitals (Paediatric) Liaise with Doctors
Liaise with Social Worker at receiving hospitalTOTAL HOURS PER CLIENT
Sexual Assault Assessment(child and adult) Laison with Police
DOCS report and liaisonAdvocacyReferral to sexual assault servicesAccommodation / refugeTOTAL HOURS PER CLIENT
Interventions omitted from template ornot performed by a service
Intervention time (mins)C D E F G Technical assistant
Intervention Hours specific to client group
300
180150150150
240
Interventions reported by only one particular service
180
150
Target Client Groups Clinical Intervention requirements A B
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February 2006. 3

Intervention ComparisonsDiscipline Speech Pathology Acute Inpatient Clinical Area: Outpatients
Intake 30 30 - Liaison wih GP / Referral 10 Y
Clients referred with Dysphagia - Receiving referrals, booking transport, liaison with client/ significant othersor Communication difficulties Initial assessment 30 30 30 50 30
- OrientationOrder of Priority - Receptive / Expressive languageReferred for MBS - speechLaryngectomy - VoiceRecent Neurological event effecting speech language - oromuscular motor assessment (cranial nerves)
- Airway protectionVoice problems - Oral trials for swallowing / swallowing techniques
Clinical Intervention requirements 75Resource / Research for assessment and treatment material 75 YTherapy preparation 20 YTherapy sessions 65Liaison with referring agent 10Result analysis and documentation 75
- ENT assessment required prior to acceptance into service report writing & file organisation 40 20 20 20Liaison with family 10 10 10 10
Stuttering Family / carer education re: Feeding strategies & safe swallowing 20 20 20 20 20MBS/ FEES 65gathering resources 10 10 10 10
Rehabilitation outpatients Referral out 5 5 5 5Liaison with other agencies eg Nursing Home, Hostel, Nutrition 10 10 10 10 - CRS, Medicare, DADHC 40TOTAL HOURS PER CLIENTCase Conference 20
Ongoing Review and Follow up 65
Recent Neurological event effecting speech / language Preparation / planning for therapy sessions 20Standardised assessments of Speech & Language 90 90 45 90Analysis & report writing 60 30 20 30Therapy sessions - weekly for minimum of 6 weeks (per session) 45 30 45Daily review and treatment 45 - preparation for session - review of medical file - conduct treatment session - liaise with staff / carer - report writingLiaison with family / significant others 10 minutes per week 10Liaison with multidisciplinary team (per week) 10report writing / medical file 30 10 10 15ADDITIONAL HOURS PER SESSION
Severe speech / language difficulties Resource Development - communication boards, cue cards, individualised, laminated 30 60 30 30in the absence of significant cognitive impairment Education of client / staff / family re use. 45 30 20 45
Report writing 10 10 10 10ADDITIONAL HOURS PER CLIENT
Clients requiring review Preparation / planning for therapy sessions 20eg. Progressive neurological diseases Liaison with multidisciplinary team / specialist clinics 20mins per visit 20
Liaison with family / significant others 10 minutes per visit 10ADDITIONAL HOURS PER SESSION
B** EC
Intervention Time (mins) Techical Assistant (Y/N)
Please qualifyDA* CA* B**
Additional interventions / hours specific to client groupIntervention / hours attributable to m
ost clients
Diagnostic / Target Client Group Clinical Intervention requirements
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 1

Intervention ComparisonsDiscipline Speech Pathology Acute Inpatient Clinical Area: Outpatients (continued)
Modified Barium Swallows Liaison with medical imaging (includes booking procedure) 30 10 10 101 patient per week* preparation of food / fluid 15 15 15 15
Obtaining case history if client not known to service 152 clinics per week** Oromuscular examination and explanation of procedure 5 5 5 5
Procuedure conducted - one therapist feeding the other observing & recording 15 30 30 30Discussion re findings 15 15 15 15feedback & recommendations given to client 15 15 15 15Report written by Speech Pathologist including summary for GP 30 15report dictated for typist 15 15Written summary completed for GP 5 5 5 5Report writing in community file 5 5 5 5Editing of typists document 15 15Final report sent out to GP, Specialist etc. 10 10 10 10ADDITIONAL HOURS PER CLIENT
Clients suitable for Group therapy Group organisation / scheduling 60Session preparation 30mins per week 180
6 week programs held 4-6 times per year Group sessions 60 mins per week 360 2 speech therapists Documentation of group outcomes 30mins per week 180
Referral / Discharge Planning reports for each client, 2hours 120ADDITIONAL HOURS PER CLIENT
Voice problems Initial Assessment 45 - ENT assessment required prior to acceptance - History into service - ENT diagnosis
- Voice AssessmentExplanation of findings 5Patient education 15Documentation 10Therapy sessions as required - 6 weeks to 3 months (per session) 30Documentation 10Home Program 20ADDITIONAL HOURS PER CLIENT
Stuttering / Articulation / Language Initial Assessment 30(Blacktown Mt Druit Hospital Only ) Explanation of findings 5
Patient education 15Documentation 10Therapy sessions 30Documentation 10Home Program 20ADDITIONAL HOURS PER CLIENT
Interventions omitted from template or not performed by a service
A*A* B** C Clinical Intervention requirements C Please qualify
Interventions reported by only one particular service
B**D E
Intervention Time (mins) Techical Assistant (Y/N)
Intervention / hours attributable to most clients
Additional interventions / hours specific to client group
Diagnostic / Target Client Group
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 2

Intervention ComparisonsDiscipline Speech PathologyAcute Inpatient Clinical Area: ICU / HDU
Technical assistant
Seen on referral Review of medical file 10 20 30Clients presenting with Dysphagia Initial assessment 60 30or Communication difficulties - Orientation
- Receptive / Expressive languageRespiratory - speechTrache - VoiceNeurology - oromuscular motor assessment (cranial nerves)Other Surgical - Airway protection
- Cuff deflation trials - Oral trials for swallowing / swallowing techniquesReport writing 20 20 20Liaison with Nursing staff / Medical team 10 20 20Liaison with family 10 10Liaison with kitchen / nutrition re; diet changes based on swallowing function 5 5Liaison with other agencies eg Nursing Home 10 10Family / carer education re: Feeding strategies & safe swallowing 20 20 20Liaison with medical team re: Quality of life issues / client 5 5Gathering resources 10 10 25Referral to other disciplines eg. Nutrition, OT, PT, SW 10 10Meal time review - observation of eating, preferable with cognitive impaired &/or geriatric clients 5 5Referral out 5 5TOTAL HOURS PER CLIENTFamily Conference 45 45ADDITIONAL HOURS PER CLIENT
Review assessment Review assessment sessions as required 45Daily or regular review / assessment 40 30 - includes conduction of assessment, review and documentation in medical file, liaison with kitchenADDITIONAL HOURS PER SESSION
speech / language difficulties Screening assessments of Speech & Language 30in the absence of significant cognitive impairment Analysis & report writing 15
Resource Development - communication boards, cue cards, individualised, laminated 30Education of client / staff / family re use. 20ADDITIONAL HOURS PER CLIENT
Clients requiring alternative Resource Development - communication boards, cue cards, individualised, laminated 30commmunication systems Education of client / staff / family re use. 45
Report writing 10ADDITIONAL HOURS PER CLIENT
Clients with Tracheostomy Liaison with staff 10Seen Daily Set up of patient eg. Suctioning by RN 15
Gathering resources 5Preparation 15 - Trachy Cuff deflation - O2 support modalityBlue Dye test 25Intervention / Review eg. Cuff deflation trial, food trial etc. 30Education of patient / family 10Documentation in medical file 10ADDITIONAL HOURS PER CLIENTFEES test 25ADDITIONAL HOURS PER CLIENTMBS if possible 45ADDITIONAL HOURS PER CLIENT
Interventions omitted from template or not performed by a service
Interventions reported by only one particular service
A*
Intervention / hours attributable to most clients
Target Client Groups Clinical Intervention requirements
Intervention time (mins)
B C
Additional intervention hours specific to client group
GMCT / NSW Health Metropolitan Hositals Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 1

Intervention ComparisonsDiscipline Speech PathologyAcute Inpatient Clinical Area: General Medical, Aged care and Orthopaedics
Referral Documentation 15Clients presenting with Dysphagia Review of medical file 10 10 10 15 10 20or Communication difficulties Initial assessment 30 30 30 60 30
- OrientationDementia / Delirium - Receptive / Expressive languageCVA - speechOther Neuro eg. Parkinsons' Disease - VoiceMND - oromuscular motor assessment (cranial nerves)COPD - Airway protectionPnuemonia - Oral trials for swallowing / swallowing techniques
Initial Screeniing 45Formal analysis 90Patient Education 10 Nwriting in progress notes 30
palliative care report writing 20 20 20 60 20Liaison with staff 5 5 5 15 5
Oesophageal Dysphagia Liaison with family 10 10 10 15 10 20Liaison with kitchen / nutrition re; diet changes based on swallowing function 5 5 5 15 5Diet entries 15
Dysphonia Liaison with other agencies eg Nursing Home 10 10 10 10Family / carer education re: Feeding strategies & safe swallowing 20 20 20 30 20Counselling 30
Oncology Liaison with medical team re: Quality of life issues / client 5 5 5 10gathering resources 10 10 10 10referral to other disciplines eg. Nutrition, OT, PT, SW, specialist consult 10 10 10 15 10Meal time review - observation of eating, preferable with cognitive impaired &/or geriatric clients 5 5 5 10 30Referral out 5 5 5 15 5Discharge Docmentation 30TOTAL HOURS PER CLIENTFamily Conference 45 45 45 45 45ADDITIONAL HOURS PER CLIENTSwallowing review 30Swallowing therapy / compensatory 45Swallowing therapy rehabilitation 60Modified Barium Swallow 30ADDITIONAL HOURS PER CLIENTcommunication screen 45Communication intervention 60MOT Intervention 45Therapy Planning (programs etc) / Gathering resources 30 45 Y With training and supervisionADDITIONAL HOURS PER CLIENTInterpreter services 15ADDITIONAL HOURS PER CLIENTTracheostomy Management 60ADDITIONAL HOURS PER CLIENT
CVA Standardised assessments of Speech & Language 90 90 90 NOther Neuro Analysis & report writing 30 30 30
Therapy sessions as needed - per session 35report writingADDITIONAL HOURS PER CLIENT
Additional interventions / hours specific to client group
BA*Target Client Groups Clinical Intervention requirements B** C A
Intervention time (mins)
G
15
Intervention / hours attributable to most clients
Technical assistant
C D E FF2E F Please Qualify
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 1

Intervention ComparisonsDiscipline Speech PathologyAcute Inpatient Clinical Area: General Medical, Aged care and Orthopaedics (Continued)
Severe speech / language difficulties Resource Development - communication boards, cue cards, individualised, laminated 30 30 60 Yin the absence of significant cognitive impairment Education of client / staff / family re use. 20 20 30
Report writing 10 10 10ADDITIONAL HOURS PER CLIENT
Dementia Delirium Additional time taken to R/V patient at meal times 20 20 20 20ADDITIONAL HOURS PER CLIENT
Palliative Care Strategies for swallowing / feeding options 20 60 20 15 N( NB. These clients tend to be transferred out of Orthopaedic Comfort care / Quality of Life issues / Patient Wishes 15 15 10units to other medical wards ) Liaison with family / client 5 5 10F2 represents figures for Orthopaedics only Liaison with medical team 5 5 5 N
ADDITIONAL HOURS PER CLIENTClients requiring therapy Daily review and treatment 45 60 45 N
- preparation for session - review of medical file - conduct treatment session - liaise with staff / carer - report writingADDITIONAL HOURS PER CLIENT
Clients requiring review Daily/ regular review / assessment 45 N - includes review of medical file, conduction of review / assessment, liaison and report writing - liaison with kitchen / client etcADDITIONAL HOURS PER CLIENT
Clients with persisting dysphagia or communication problems Discharge Planning 45 N - report, referral, further patient educationADDITIONAL HOURS PER CLIENT
Modified Barium Swallows Liaison with medical imaging (includes booking procedure) 10 30 10 N Ypreparation of food / fluid 15 15 15 Y
2 Clinics per week* Oromuscular examination and explanation of procedure 5 5 52 staff required* Procedure conducted - one therapist feeding the other observing & recording 30 15 30
Discussion re findings 15 15 15Analysis / Interpretation / Discussion re findings
1 patient per week** feedback & recommendations given to client 15 15 15Report dictated for typist 15Report written by Speech Pathologist 30 15Written summary entered in medical file 15 15 15MBS 50MBS preparation / report / entry 60ADDITIONAL HOURS PER CLIENT
Interventions reported by only one particular service
Please Qualify
Additional interventions / hours specific to client group
D E FCTarget Client Groups Clinical Intervention requirements F
Intervention time (mins) Technical assistant
A* B** C E
Interventions omitted from template or not performed by a service
F2
Resource Development under supervision
G A B
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 2

Intervention ComparisonsDiscipline Speech PathologyAcute Inpatient Clinical Area: Emergency
Referral Documentation 15Seen on referral Review of medical file 10 10 10 10 20 10Clients presenting with Dysphagia Initial assessment or Communication difficulties - Orientation
- Receptive / Expressive languageDementia / Delirium - speechCVA - VoiceOther Neuro eg. Parkinsons' Disease - oromuscular motor assessment (cranial nerves)MND - Airway protectionCOPD - Oral trials for swallowing / swallowing techniquesPnuemonia Report writing 20 20 20 15 20 20palliative care Liaison with staff 5 5 5 5 10 5
Liaison with family 10 10 10 10 15 10Oesophageal Dysphagia Liaison with kitchen / nutrition re; diet changes based on swallowing function 5 5 5 5 5
Liaison with other agencies eg Nursing Home 10 10 10 10 10Dysphonia Family / carer education re: Feeding strategies & safe swallowing 20 20 20 20 20
Liaison with medical team re: Quality of life issues / client 5 5 10 5 5Oncology Gathering resources 10 10 10 10 10
Referral to other disciplines eg. Nutrition, OT, PT, SW 10 10 10 10Meal time review - observation of eating, preferable with cognitive impaired &/or geriatric clients 5 10 5Referral out 5 15 5 5 5Referral / Discharge Summary if Discharged 15TOTAL HOURS PER CLIENT 2.42 2.33 2.58 2.50 1.50 2.42Family Conference 45 45 45TOTAL HOURS PER CLIENT 0.75 0.75 0.75MBS 50TOTAL HOURS PER CLIENT
Speech / language difficulties in the absence of Screening assessments of speech and language 15significant cognitive impairment Analysis and report writing 10
TOTAL HOURS PER CLIENT 25
Interventions reported by only one particular service
Interventions omitted from template or not performed by a service
Intervention / hours attributable to most clients
Technical Assistant (Y/N)B E
25
CADiagnostic / Target Client Group Clinical Intervention requirements F
30 30 30 45 30
D
GMCT / NSW Health Metropolitan Hospital Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 1

Intervention ComparisonsDiscipline Speech PathologyAcute Inpatient Clinical Area: Paediatric Inpatients
Receive Referral / Documentation 15Review of medical file 10 20
Feeding Difficulties Initial assessment Premature Infants - OrientationNeurological difficulties - Receptive / Expressive language
- speech - Voice - oromuscular motor assessment (cranial nerves)
Language Development issues - Airway protection - Oral trials for swallowing / swallowing techniquesReport writing 20 20Liaison with staff 10Liaison with family 15 25Liaison with medical / nursing team 10 15Liaison with other services 25Liaison with kitchen / nutrition re; diet changes based on swallowing function 5Liaison / referral to other agencies 10 15Family / carer education re: Feeding strategies & safe swallowing 20Gathering resources 10 15Referral to other disciplines eg. Nutrition, OT, PT, SW 10Meal time review - observation of eating 20 30Follow up contact phonecall 15TOTAL HOURS PER CLIENT 2.83 4.08MBS / FEES 45TOTAL HOURS PER CLIENT 45Case Conference 25TOTAL HOURS PER CLIENT 25
50
B Technical Assistant (Y/N)ADiagnostic / Target Client Group Clinical Intervention requirements
Intervention / hours attributable to most clients
30
GMCT / NSW Health Metropolitan Hospitals Allied Health Project - Clinical Interventions and Staffing Guidelines, February, 2006. 1

References
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 2
6. References
1. Australian Bureau of statistics, Basic Community Profile, August 7, 2001 Census. 2. National Aged Care Alliance, December 2004. Principles for Staffing Levels and Skills Mix in Aged Care Settings. 3. National AHP and HCS Critical Care Advisory Group, July 2003. Allied Health Professionals and HealthCare Scientists Critical Care Staffing
Guidance – A Guideline for AHP and HCS Staffing Levels. Critical Care Program Modernisation Agency, United Kingdom. 4. NSW Health, April 2004. National Health Workforce Strategic Framework. 5. NSW Health, April 2005. Securing Our Health Workforce. 6. Safe Staffing Guidelines, Alabama State Nurses’ Association Reporter.2000 Mar-May; 27(2): 13. 7. Services for Australian Rural and Remote Allied Health (S.A.R.R.A.H), 2002. A Study of Allied Health Professionals in Rural and Remote
Australia. 8. Stevenson, K. March 2005. Allied Health Services in Metropolitan Hospitals. GMCT Metropolitan Hospitals Forum.

Acknowledgments
This is a draft discussion document and is considered to be Phase 1 of the GMCT/ NSW Health Metropolitan Hospital Allied Health Project. This project does not attempt to make any statement of what is appropriate with regard to staffing levels. Further work needs to be done with each specific Allied Health Profession in order to determine what would be considered minimum requirement and Best Practise. Page 3
7. Acknowledgments
The author would like to acknowledge:
The Greater Metropolitan Clinical Taskforce and NSW Health for providing the opportunity for this project to occur.
The members of the Allied Health Steering Committee and
All Allied Health Clinicians who participated in the data collection and analysis process.





























