Embed Size (px)
Citation preview

SELF-MANAGEMENT IN PARKINSON’S DISEASE FOR HEALTH QUALITY OF LIFE
Linda Tickle-Degnen, PhD, OTR/L, FAOTA
ALLIED TEAM TRAINING FOR
PARKINSON 2014 –San Diego

Disclosures for Linda Tickle-Degnen, PhD, OTR/L, FAOTA
None
I will not be discussing the off-label use of various medications.

Objectives
• Identify gaps in current self-management approaches for Parkinson’s, particularly the role of social life and supports.
• Learn models that can be used by interdisciplinary or inter-professional team members in self-management interventions.
• Understand how to support people with Parkinson’s disease and their care partners in self-management.
3

National Council on Aging United States of Aging Survey 2014
(Downloaded/revised from www.ncoa.org/UnitedStatesofaging)
4
What is the most important key to keeping a positive outlook on life? (Ranked by Seniors 60+)

WHO International Classification of Functioning, Disability and Health - ICF
Body Functions & Structure
Participation
Personal Factors
Environmental Factors
Health Condition
Activity
Where is the category for “taking care of one’s health”?
www.who.int/classifications/icf/en/
5

ICF category related to the self-management of health:
A focus on physical management
Component d = Activities & Participation Domain 5 = Self-Care Category d570 = Looking after one's health
Ensuring physical comfort, health and physical and mental well-being, such as by maintaining a balanced diet, and an appropriate level of physical activity, keeping warm or cool, avoiding harms to health, following safe sex practices, including using condoms, getting immunizations and regular physical examinations.
6

7
ICF category related to the self-management of health:
A focus on social management
Component d = Activities & Participation Domain 5 = Self-Care Category d578 = Looking after one's health, other specified
Our wording: Ensuring social comfort and physical and mental well-being, such as by maintaining socially supportive interpersonal relationships, and engaging in a level of social activity that supports personal flourishing and prevents loneliness, including seeking help for supporting health.

How we got to d578 from d570
1. Interdisciplinary self-management rehabilitation for Parkinson’s: A randomized controlled trial (RCT)
2. Follow-up videotape/transcript studies from the RCT
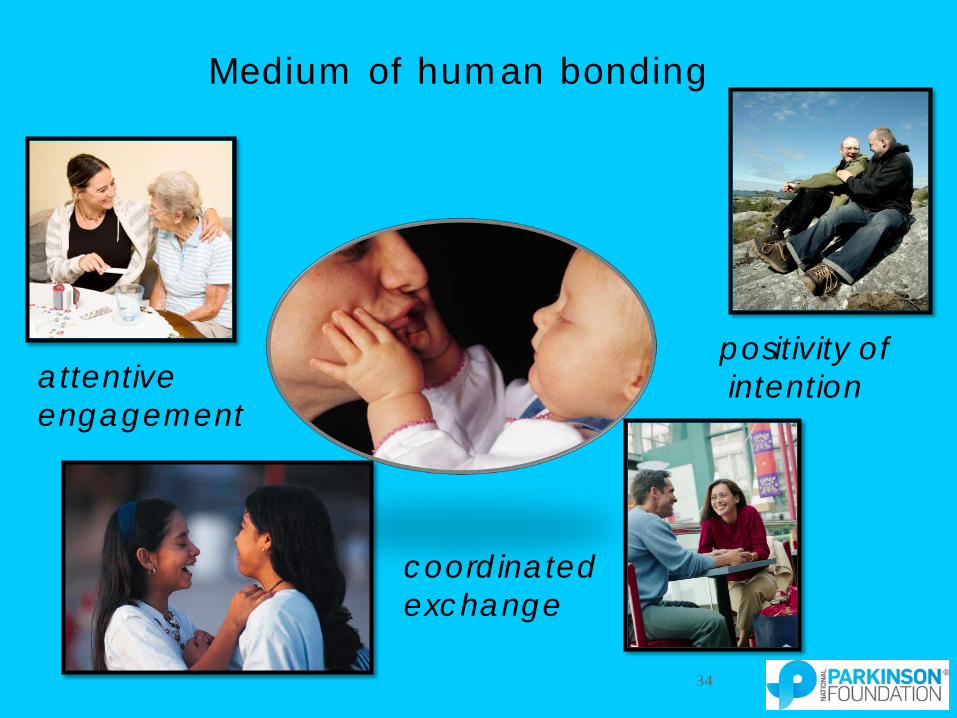
3. Health care stigma in Parkinson’s: A cross-cultural field experiment on effect of symptom of reduced facial expression (masked facies/hypomimia) on practitioner diagnostic impressions
4. Development of a longitudinal study on the social self-management of PD
8

Challenges to Maintaining Valued Life Activities:
The Case of Parkinson’s Disease Pusswald et al. (2012) People with Parkinson’s had lower sense of feeling of control and consistency in their lives, fewer active coping strategies and lower well-being compared to people with chronic non-neurological disease. McCabe et al. (2008) People with neurological disease and their care partners had highly compromised work and leisure lives due to the disease. McNamara et al. (2006) People with Parkinson’s felt that their life goals – work, leisure, social life, religious and financial – were significantly “off track” compared to age-matched peers without Parkinson's.
9

Building Personal Control & Competency:
The Case of Parkinson’s Disease Holman & Lorig (1992)
Self-efficacy to cope with consequences of chronic disease contributes to self-management capabilities.
McQuillen, Licht, & Licht (2003)
Perceived control over life in general (primary) and perceived control over adaptation to PD (secondary) positively relates to life satisfaction and negatively relates to depression.
Morgan, Hunter, & Todaro (2010)
Teaching people with PD how to be advocates for research in PD increased confidence as a PD advocate, inclination to join a support group, feeling of ability to effect changes, plan to seek disease management information, ability to cope with the disease and plans and interests in engaging in more outside and social activities.
10

Attitude toward
Behavior
Subjective Norm
Perceived behavioral
control
Intention (Goal)
Self- observa-
tion
Judg- mental process
Self- reaction
(Self-efficacy)
Ajzen’s Theory of Planned Behavior Bandura’s Social Cognitive Theory of Self-Regulation
THEORETICAL MODELS BEHIND SELF-MANAGEMENT INTERVENTION
Behavior
11

RANDOMIZED CONTROLLED TRIAL Tickle-Degnen, L., Ellis, T., Saint-
Hilaire, M. H., Thomas, C. T., & Wagenaar, R. C. (2010). Self-management rehabilitation and health related quality of life in Parkinson’s disease. Movement Disorders, 25, 194-204.
12

N = 116 community living, non-depressed, normal mental status: I. 0 hrs: Medication only II. 18 hrs: Clinic group rehab18 hrs + 9 hrs placebo social group III. 27 hrs: Clinic group rehab 18 hrs + 9 hrs home transfer of training
-6
-4
-2
0
I. Medication onlyII. Clinic plus social groupIII. Clinic plus home visit
Impr
ovem
ent i
n Q
ualit
y of
Life
baseline post 2 months 6 months
-----6 wks----- ---------------------------follow-up period-------------------------
13

Content of Group Rehabilitation Sessions 1.5 hr session 2 times/week
1. Motion, flexibility, and strength exercises (25 min.) •Active ranging/stretching to increase trunk extension/rotation •Stretching hip flexors, hamstrings and gastrocnemius, •Strengthening trunk/hip postural muscles, knee, ankle extensors
2. Speech exercises (10 min.) •Active ranging/stretching facial muscles •Strengthening muscles of vocal folds •Vocal rate control and intensity
3. Daily function training examples (15 min.) •Moving in bed, rising from chair, from floor •Dressing, handwriting •Swallowing, social communication
4. Gait training (10 min.) •Walking with external auditory cues to optimize gait pattern and speed
14

Content of Group Rehabilitation Sessions (cont’d)
5. Group discussion (30 min.) “Be your own therapist”
•Barriers to exercise, communication, mobility •Benefits of exercise •Enhancing social communication •Strategies to improve walking •Coping with tremor, stiffness •Self-management for life: moving forward •Preventing falls •Talking on the phone •Strategies to improve dressing •Relaxation, stress management •Self-management for life: staying on track
15

Environment Occupation
Person
“Self-Manage” Be your own therapist
Law, Cooper, Strong, Stewart, Rigby, & Letts (1996)
16

is for PERSON: How Can I Use or Develop My Strengths?
Listen Read Imagine
17

is for ENVIRONMENT: How Can My Environment or Objects Be Selected
or Adapted To Match My Ability?
18

is for OCCUPATION: How Can the Occupation/Task Be Modified
To Make it More Complex or Simpler?
19

Content of Social “Placebo” or in-Home 1.5 hr session 1 time/week
PLACEBO (II): “Get to know one another aside from Parkinson’s”
• Ice breaker activity
• Discuss a topic of mutual interest: e.g., travels, work, interests, family, cars, sports
• Share photo’s, poetry, literature, music, art
• Show or teach others a personal hobby
• Share food together and chat
HOME (III):
• Individualized transfer of training from group rehab sessions
20

Change from baseline to post, beyond medication only
.00
.05
.10
.15
.20
.25
.30
.35
.40
.45
.50
Communication
Bodily Discomfort
Mobility ADL
Social S
upportStigma
Emotional Well-b
eing
Cognition
Effec
t size
d
---- Physical ---- ---- Psycho-social ----
Condition III (rehab + home) & Condition II (rehab + social “placebo”) M
ore
bene
ficia
l
21

National Council on Aging United States of Aging Survey 2014
(Downloaded/revised from www.ncoa.org/UnitedStatesofaging)
22
What is the most important key to keeping a positive outlook on life? (Ranked by Seniors 60+)

There is nothing better than “social enjoyment."
W. Godwin 23

The world around…
24

25
Human activities and pursuits occur within a socio-cultural context

Personal and social projects are among the
most meaningful life activities.
They promote personal & social flourishing.
People who actively participate: 1. experience happiness & well-being 2. affirm their unique skills, values, identity 3. have enhanced relationships 4. protect against motor decline and mortality
(Buchman, 2009; Christiansen et al., 1999; Holt-Lundstad, 2010; Little, 2007)
26

“My grandson is in his third year … of Little League. So I go, I always go, to every one of his practices plus the games.”
27
>450 taped interviews

“We’ve been taking dance lessons for around thirteen years now…We have a lot of nice friends.”
28

“Each time it’s someone’s birthday, we get the men together and go out for lunch or a couple of beers.”
29

Tell me about an enjoyable event… a frustrating event in the past week
Methods: 40 people with PD (meds only arm of RCT): 4 times over 7 months. 320 events transcribed (Tickle-Degnen et al., 2012; Yur et al., 2013).
• Quantitative: Social and health/symptom words were counted with Pennebaker’s Linguistic Inquiry Word Count
• Qualitative: Content analysis
Results: 1. 3.5 times more social than health/symptom words (p <.0001). 2. Especially for enjoyable than frustrating events (p <.0001). 3. Symptoms described most frequently for social participation events
(social, leisure, IADL) than basic self-care 4. Symptoms described as creating stigma, reducing social competency. 5. Social relations described as reducing or exacerbating symptoms.
30

Parkinson’s disease involves the loss of power to give physical and social action to one’s
intentions, thoughts, and feelings. 31
http://www.humboldt.edu/~osprey/fall00/living.html
A disorder of movement or of social connection?

HAPPY SMILE ANGRY SMILE
(Pentland et al., 1987) 32
The Face Fast, salient, potent channel of communication
mood
character
intention
gender
33
Medium of human bonding
attentive engagement
coordinated exchange
positivity of intention
34
Depression
Sociability
Social supportiveness
Cognitive competence
35

Depression Sociability Social Supportiveness
Cognitive Competence
(N = 285 practitioners, 50% PD experts, 50% training students;
patients were 12 Taiwanese Asians, 12 American Whites)
Deg
ree
of
Judg
ed A
ttrib
ute
36
(all differences p < .0001)

all differences p < .05
Higher bar = more negative bias towards patients with reduced facial expression
37

How does the Health Care Interview Contribute to Facial Expression in PD?
RCT: Describe a recent frustrating / enjoyable event
(Takahashi et al., 2010), N=106; all differences p < .01)
Higher bar = More expressive face
38
39
ICF category related to the self-management of health:
A focus on social management
Component d = Activities & Participation Domain 5 = Self-Care Category d578 = Looking after one's health, other specified
Our wording: Ensuring social comfort and physical and mental well-being, such as by maintaining socially supportive interpersonal relationships, and engaging in a level of social activity that supports personal flourishing and prevents loneliness, including seeking help for supporting health.
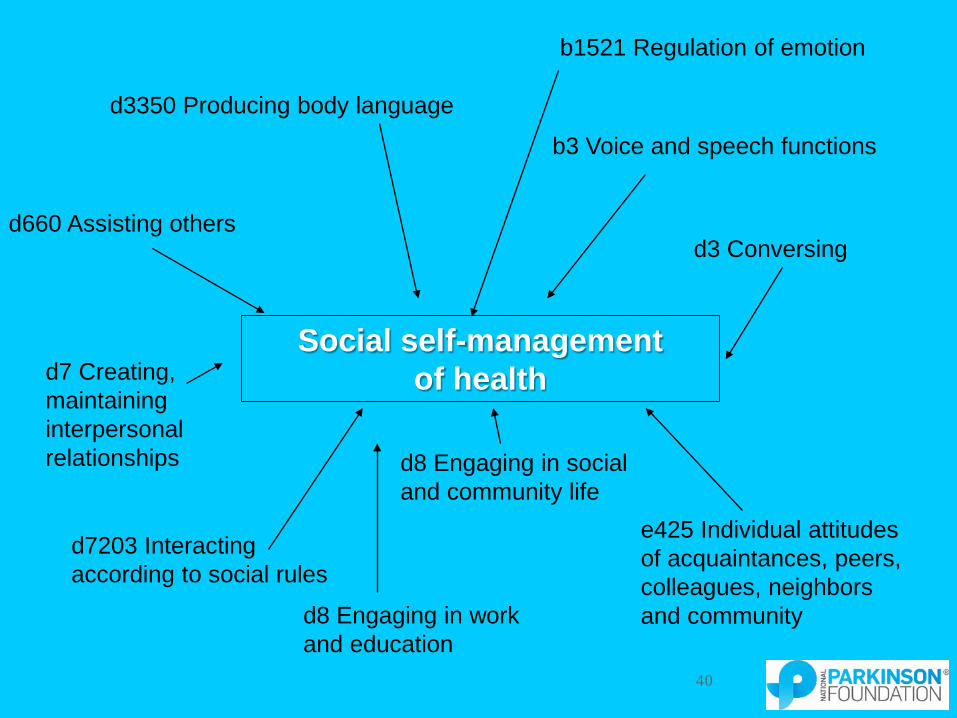
e425 Individual attitudes of acquaintances, peers, colleagues, neighbors and community
d7203 Interacting according to social rules
d7 Creating, maintaining interpersonal relationships
d3 Conversing d660 Assisting others
b3 Voice and speech functions
d3350 Producing body language
Social self-management of health
b1521 Regulation of emotion
d8 Engaging in work and education
d8 Engaging in social and community life
40

LONGITUDINAL STUDY PROTOCOL Tickle-Degnen, L., Saint-Hilaire, M.,
Thomas, C. A., Habermann, B., Martinez, L. S., Terrin, N., Noubary, F. & Naumova, E. N. (2014). Emergence and evolution of social self-management of Parkinson's disease: study protocol for a 3-year prospective cohort study. BMC neurology, 14(1), 95.
41

Aim 1: Characterize social self-management trajectories of PD over 3-yr period by assessing: a) social participation and management of social activities, b) informal and formal social networks, and c) social comfort and overall health and well-being. Aim 2: Estimate degree to which expressive nonverbal capacity predicts social self-management trajectory. Aim 3: Determine moderating effect of gender on association between expressive capacity and change in social self-management.
42
Emergence & Evolution of Social Self-Management Of Parkinson’s Disease

Study Design 120 individuals with PD and their care partners (CP)
• PD: English speaking, community living, idiopathic PD, H&Y 1-4, non-disoriented at baseline, > 18 yo
• CP: Consent of person with PD, English speaking, non-disoriented at baseline
Over 3 yr period, 14 assessments per participant
• 7 in-person assessments (1 in home): baseline plus every 6 mo
• 7 shorter telephone assessments in-between
Rationale for design: • Time series power to capture linear and non-linear trajectories of individuals
and dyads (cholera research paradigm)
• Idiographic (variability of lives) and nomothetic (central tendencies) information
43

Mixed Method
Quantitative
Facial Expression Task Facial Action Coding System
Interpersonal Communication Rating Scales
MOCA (Cognition) GDS (Depression)
SF-12 (Self-reported health) MDS – UPDRS (Disease symptoms)
PDQ-39 (PDQ-8) (PD Quality of life)
Activity Card Sort
Social Network Composition, Contact, & Exchange
Chronic Illness Resource Survey Home Visit Assessment (TBD)
Isolation/loneliness
MOS Social Support Stigma Scale for Chronic Illness
Qualitative
Individual: Frustrating/Satisfying activities
Strategies for social self-management
Dyad: Frustrating/Satisfying activities together
Managing as a couple
Qualitative Content Analysis Linguistic Inquiry Word Count
44

BUILDING SELF-MANAGEMENT IN PARKINSON’S DISEASE
AWARENESS & EDUCATION
45

Enhancing Self-Management for Living with Parkinson’s: A Health System Approach
While building and implementing client-based evidence, conduct awareness and education campaigns 46

Grassroots Recruitment and Awareness Building Campaign
Objective: Reach older adults not connected to traditional services.
1. Listservs focused on minority health and health disparities
2. Local newspapers and TV media targeting minority communities
3. Present to 26 local community health centers that serve primarily minority populations;
4. Present to elder services; adult daycare programs; churches; senior housing facilities.
300 outreaches 20+ partnerships
47

To be Resilient…
1. Take the time to identify an important problem.
2. Determine why it is a problem to you and your quality of life.
3. Make a plan to address the problem to be able to:
– function to your satisfaction in daily life, and
– keep being the person who defines who you are.
(Informed by Almedom, 2009) 48
Healthy Aging Talks: Problem-solving for engagement in
valued daily activities

1. Select a project (goal) 2. Optimize social resources and medical self-management
to accomplish the project 3. Adapt project to make the right fit between
• Person skills and interests • Environment and objects • Occupations/Tasks involved (Baltes & Baltes,1990; Lowenstein & Tickle-Degnen, 2008)
49
PD Support Group Talks: Building Resilience
by Planning Social Projects

Use multiple channels of connection
family or friend
creative expression
clothing
nonverbal behavior
words
shared interests
social projects
robot
HOW TO IMPROVE YOUR SOCIAL CONNECTIONS
50

Practitioner Self-Improvement:
Everyday bias Clinical bias
CHANGE HEALTH-CARE INTERACTION
1.Reduce confidence about one’s quickly formed impressions. Test out “alternative” clinical hypotheses about participant capacities, social vitality, interests.
2.Identify and use valid cues of attributes in people with reduced facial movement (self-report, partner report).
3.Enrich the assessment and environmental stimuli to promote active patient communication and practitioner accuracy of observation. Support autonomy. (Kahneman & Klein, 2009; Schwab, 2008)
51

Acknowledgements Tufts Health Quality of Life Lab
BMC Neurology, Movement Disorders Clinic Marie Saint-Hilaire, MD; Cathi Thomas, RN
Boston University Social Work Linda Sprague-Martinez, PhD
Tufts Civil & Environmental Engineering Elena Naumova, PhD
Tufts School of Medicine, CTSI Farzad Noubary, PhD
University of Delaware Nursing Barbara Habermann, PhD, RN
Tufts Human Robot Interaction Lab Matthias Scheutz, PhD
52