Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=iimm20
Download by: [University of Toronto Libraries] Date: 17 March 2016, At: 20:52
Immunological InvestigationsA Journal of Molecular and Cellular Immunology
ISSN: 0882-0139 (Print) 1532-4311 (Online) Journal homepage: http://www.tandfonline.com/loi/iimm20
Alpha Interferon Treatment of Patients withChronic Fatigue Syndrome
Darryl M. See & Jeremiah G. Tilles
To cite this article: Darryl M. See & Jeremiah G. Tilles (1996) Alpha Interferon Treatment ofPatients with Chronic Fatigue Syndrome, Immunological Investigations, 25:1-2, 153-164, DOI:10.3109/08820139609059298
To link to this article: http://dx.doi.org/10.3109/08820139609059298
Published online: 07 Jul 2009.
Submit your article to this journal
Article views: 13
View related articles
Citing articles: 5 View citing articles

IMMUNOLOGICAL INVESTIGATIONS, 25(1&2), 153-164 (1996)
ALPHA INTERFERON TREATMENT OF PATIENTS WITH CHRONIC FATIGUE SYNDROME
Darryl M. See and Jeremiah G. Tilles Department of Medicine
School of Medicine, University of California at lrvine Orange, CA 92668
ABSTRACT
Thirty patients who fulfilled clinical criteria defined by the CDC for Chronic Fatigue Syndrome were treated with alfa 2a interferon or placebo in a double-blind crossover
of Life (QOL) survey. Although mean NK function rose from 87.8 +/- 19.6 to 129.3 +/- 20.7 lytic untis (LU; pc.05) with 12 weeks of interferon therapy, there was no significant change in the other immunologic parameters or QOL scores. When the 26 patients who completed the study were stratified according to their baseline NK function and lymphocyte proliferation, 4 groups were identified: 3 patients had normal NK cell function and lymphocyte proliferation when compared to normal, healthy controls, 9 had isolated deficiency in lymphocyte proliferation, 7 had diminished NK function only, and 7 had abnormalities for both parameters. QOL scores were not significantly different for the four groups at baseline. After 12 weeks of interferon therapy, QOL score significantly improved in each of the seven patients with isolated NK cell dysfunction (mean score, 16.3 +/- 7.9) compared to baseline (39.7 +/- 12.1 ; pc.05). In these patients the mean NK function increased from 35.1 +/- 11.7 to 91.5 +/- 22.7 LU (pc.01). Significant improvement was not recorded for QOL in the other three groups. Thus, therapy with alpha interferon has a si nificant effect on the QOL of that subgroup
. Outcome was evaluated by Natural Killer (N cell function, lymphocyte proli eration to mitogens and soluble antigens, CD4/ ? D8 counts and a 10 item Quality
of patients with CFS manifesting an isolate 1 decrease in NK function.
INTRODUCTION
Chronic Fatigue Syndrome is a protracted, debilitating illnes of unknown etiology. Affected patients suffer from fatigue and a variety of other constitutional signs and symptoms (1). Although no specific diagnostic tests are available, case criteria have been established by the Center for Disease Control (CDC) (2). A growing body of evidence suggests that the syndrome is associated with immune system dysregulation. Although many conflicting data have been presented, several studies have reported such findings as increased polyclonal antibody production (3),
153
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

154 SEE AND TILLES
decreased Immunoglobulin levels (4), elevated autoantibody titers (5), and circulating immune complexes (6) in affected patients. Other investigators have described patients with increased oligoadenylate synthetase levels (7), diminished natural killer cell and lymphocyte function (8), enhanced CD4 cell differentiation (9), and abnormalities in cytokine production (10). The pathogenesis of this immune system dysfunction is poorly characterized; a review of reported immunologic findings revealed an extremely wide variability in various studies for each parameter (1 1).
Several retrospective studies have attempted to define the underlying etiology of the illness. Many reports are either conflicting, or yield non-specific information. Some investigators feel that the Illness is primarily psychiatric in origin (12). Others have suggested that the illness may be due, in part, to abnormalities in the hypothalamic- pituitary-adrenal axis (1 3). Other reports suggest that limbic system dysfunction may be reponsible (1 4). Environmental agents have been implicated in several studies. Among these, viruses, Including retroviruses (1 5), enteroviruses (1 6), Epstein-Barr virus (17,18), and human herpesvirus-6 (19), have been championed. A definitive correlation of these viruses with CFS has been confounded, however, by the high prevelance of detectable organisms in normal controls. It has also been postulated that the disorder is caused by a post-Infectious autoallergic reaction to one or more viruses (20); thus, the responsible virus may no longer be detectable at the time the diagnosis of CFS is made.
Definitive therapy has not been established for the disorder. The immunopotentiator Ampligen was shown to be of benefit in one study (21). Therapy with intravenous immunoglobulin was beneficial in one study (22), but not in another (23). Others studies failed to document response to treatment with Acyclovir (24) or dialyzable leukocyte extract (25).
Alpha Interferon has potent lmmunomodulatory (26) and antiviral effects (27). It has been used successfully In the treatment of several tumors (28) and viral infections (29). Persistent viral infection and/or immune suppression have been postulated as playing a role in the pathophysiology of CFS. In an open label study of CFS patients, alpha interferon was beneficial in a subgroup of patients with increased IgM titers to one or more coxsackie group B viruses (30). The present report desribes a randomized, double-blind, placebo-controlled, crossover study of alpha interferon in patients with CFS.
PATIENTS AND METHODS
Thirty consecutive patients who fulfilled the diagnostic criteria for CFS per the CDC guidelines of 1988 (2) were enrolled in the study. The subjects were referred by local internists and faculty in the Department of Medicine at the University of California,
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

ALPHA INTERFERON A N D CHRONIC FATIGUE SYNDROME 155
Irvine. 24 women and 6 men with a mean age of 37.2 years (SD 7.4, range 22 to 58) were included. The thirty test patients had been symptomatic for CFS for a mean of 4.6 years (range 1 to 12 years). Patients who had received immunologic therapy during the previous year with intravenous immunoglobulin, interferon, cytokines or steroids were excluded. All other medications were allowed. Chronic infections (HIV, tuberculosis, Borrelia burgdorferi, Coccidioidomycose immitis and Toxoplasma gondii), rheumatologic disorders, multiple sclerosis, thyroid disease, IgG deficiency and primary psychiatric illness were excluded by appropriate clinical evaluation and diagnostic testing (2). Approval for the study was obtained from the local Institutional Review Board (IRB). Informed consent was obtained from each patient.
Studv desian: Alfa-2a Interferon was obtained from Roche Pharmaceuticals. Patients were randomized to receive either interferon (3 million units) or placebo (0.9% NaCl solution) subcutaneously three times per week for 12 weeks. At this time, each patient's medication was crossed over and the patient received the alternative placebo or interferon for an additional 12 weeks. All treatments were administered from sterile vials which were coded by study number to ensure blinding of both patients and investigators.
The study medication was administered in the early evening. Each patient drank at least 16 ounces of water with each dose and took 650 mg of acetominophen 2 hours following the dose in order to minimize side effects from interferon and to ensure blinding of the study. Patients were evaluated clinically biweekly for 2 visits initially, at the time of crossover, and then every four weeks for the remainder of the study. A final evaluation was performed 4 weeks after completion of the study medication. At each visit, blood was obtained for a complete blood count and liver function test. In addition, prior to the first dose and at 12 and 24 weeks, blood was obtained for immunologic studies.
lmmunoloaic assessment: Immunologic parameters were assessed at baseline, 12 weeks and 24 weeks. For each assay, peripheral blood mononuclear cells (PBMC) were separated from heparinized blood samples by standard Ficoll-Hypaque density gradient centrifugation (31). Blood was collected between 12:OO and 2:OO pm on each occasion.
Analysis of lymphocyte subsets: PBMC were incubated with fluorescein isothiocyanate-conjugated antibodies to CD3 (pan T cells), CD4 (T helper/inducer), CD8 (T suppressor/cytotoxic), CD20 (pan B cells) and CD16 and CD56 (natural killer cells) and analysed with a flow cytometer (Becton Dickenson) by standard methods (31).
Natural killer cell function: The K562 target cells were maintained in RPMl medium (Irvine Scientific, Santa Ana, CA) supplemented with 420 pg per ml of
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

156 SEE AND TILLES
glutamine, 400 U per ml of penicillin, 40 pg per ml of streptomycin and 10% fetal bovine serum (FBS). Fresh PBMC suspended in complete RPMl medium were used as effector cells. The target cells were labelled with 20 pC [51 Cr] sodium chromate (ICN, Costa Mesa CA)/0.3 cc for 1 hr. at 37 deg.C (5% C02), washed 4 times with medium, and seeded as an inoculum of 1 x 104 cells into each well of a 96-well U- bottom microtiter plate. Effectors cells were added to the wells in triplicate at an effector:target ratio of 20:l ,lO:l and 31. Control wells contained labelled target cells with plain medium for determination of spontaneous lysis, or 3% Triton X-100 for evaluation of total lysis. After incubation for 16 hours at 37 deg. C (5% Con), the cells were centrifuged, and 100 pl of the supernatant removed for determination of radioactivity by liquid scintillation counting in a Beckman LS-100. Cytotoxic activity in test wells was calculated in terms of % specific lysis by the following formula:
% specific lysis = [(test sample) - (spontaneous lysis)] x 100 [(total lysis) - (spontaneous lysis)]
(values in parentheses represent counts per minute [cpm])
The data were expressed in terms of lytic units (LU) by the method of Pross (32). One lytic unit was defined as the number of effector cells required to achieve 20% specific lysis of 5 x 103 targets. LU were calculated per 107 effector cells.
Lymphocyte proliferation: PBMC were suspended in complete RPMl medium with 10% FBS and dispensed in triplicate as 108 pl containing 1 x 1 O5 cells per well in 96-well U-bottom microtiter plates. The cells were stimulated with 12 HI alternatively of concanavalin A (con A, final concentration of 10 pg/ml), phytohemagglutinin (PHA, 10 ug/ml), pokeweed mitogen (PWM, 1 pg/ml), or candida albicans (0.4 colony forming unitdml), tetanus toxoid (0.01 Lf/ml) or mumps (4 colony forming units/ml) antigen. Cultures were incubated either for 3 days with mitogens or 6 days for antigens at 37 deg. C (5% C02), and pulsed with 1 pC of [3H] thymidine (ICN) per well for the final 24
hrs. of culture. Cells were harvested and [3H] thymidine incorporation measured with a Beckman LS-100 scintillation counter. Data were represented as net cpm after subtracting the background and then normalized to yield % normalized proliferation for each mitogen or antigen by the following formula:
net cpm test sample xl00 net cpm control sample
Selection of normal controls: NK function analysis was performed on three PBMC samples obtained from each of 20 normal, healthy adults on the staff at U.C. lrvine Medical Center between the ages of 23 and 44 (9 male, 11 female). The samples were drawn from 12:OO to 2:OO pm. Fresh blood from 1 of the consistently average
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

ALPHA INTERFERON AND CHRONIC FATIGUE SYNDROME 157
controls was obtained in parallel with test samples at each time interval during the course of the study in order to normalize lymphocyte proliferation for each run. Only control subjects that had been free of signs or symptoms of acute infection during the prior week were used on each occasion.
Clinical assessment: Clinical well-being was assessed using a 1 O-item set of symptoms (recording fatigue, objective fevers, sore throat, lymphadenopathy, muscle aches, headaches, joint pains, depression, concentration ability and insomnia). Each symptom was assessed on a scale of 0-6 and a cumulative Quality-of-Life score was calculated (range of 0-60, with 60 the worst score).
Statistics: Immunologic parameters and differences in QOL scores were compared before and after interferon therapy or placebo by analysis of variance for repeated measures.
RESULTS
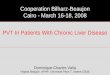
Immunologic assessment: The mean NK function for the 20 normal controls was 125.7 +/- 24.7 LU. 15 patients were on placebo prior to the crossover. Each of these patients completed 12 weeks of placebo therapy. At baseline, their mean NK function was 89.1 +I- 18.9 LU (Fig. I) and mean lymphocyte function (% normalized lymphocyte proliferation [% NLP]) was 62.3 +I- 23.1, 59.6 +I- 21.3, 78.5 +I- 22.7, 49.4 +/- 15.6, 71.5 +/- 19.8 and 54.8 +I- 22.6% for con A, PHA, PWM, candida, tetanus and mumps antigen, respectively. There was no significant change after 12 weeks of placebo therapy for either mean NK or mean % NLP for any of the mitogens or soluble antigens. At the time interferon therapy was initiated in those 26 patients who completed the trial (including 13 on interferon prior to the crossover and 13 on interferon after the crossover), mean NK function was 87.8 +I- 19.6 LU and mean % NLP was 61.3 +I- 18.7, 56.9 +I- 23.4, 80.3 +I-20.9, 46.8 +I- 15.9, 70.2 +/- 21.3 and 51.7 +I- 21 .O % for con A, PHA, PWM, candida, tetanus and mumps antigen, respectively. After 12 weeks of interferon therapy, mean NK function increased significantly to 129.3 +I- 20.7 LU (F= 3.51 ; p<.05), but the mean % NLP did not change for any of the mitogens or soluble antigens. In those 13 patients followed for an addition 12 weeks after completing interferon therapy, mean NK function had decreased to 101.5 +I- 24.8 LU. The 26 patients who completed the study were stratified into four groups based upon baseline NK and lymphocyte function. Thus, subjects in group 1 (n=3) had an NK function >50% of the mean for the 20 control patients and % NLP >50% for at least 4 of the 6 mitogens or soluble antigens tested; group 2 (n=7) had an NK function 40% of the mean for the 20 controls and % NLP 4 0 % for at least 4 of the 6 mitogens or antigens; group 3 (n=9) had reduced % NLP only; and group 4 (n=7) had reduced NK function only. The mean % NLP score was not significantly changed compared to baseline for any of the groups after 12 weeks of placebo or interferon therapy. The
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

158
180- 16C- 140- 120-
SEE AND TILLES
p < .os
k ;E; 1 40 20 0
8) 200 p = N S
p = N S
I I40 1n
PLACEBO INTERFERON lhenw
l Z 0 1 . I-+
PLACEBO INTXRFERON lbnpy
PLACEBO INlERFERON k-PY
PLACEBO lNl€RFERON therapy
FIGURE I
Mean Natural Killer cell function after 12 weeks of therapy with placebo or interferon. Placebo values are for those patients who began the trial on placebo. Interferon values are for those subjects who completed 12 weeks of drug therapy. A) All patients (placebo, n=15; interferon, n=26) B) Group 1: normal NKfunction and lymphocyte proliferation (placebo, n=2; interferon, n=3) C) Group 2: both NK function and lymphocyte proliferation decreased (placebo, n=3; interferon, n=7) D) Group 3: reduced lymphocyte proliferation only (placebo, n=7; interferon, n=9) E) Group 4: reduced NK function only (placebo, n=3; interferon, n=7).
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

ALPHA INTERFERON AND CHRONIC FATIGUE SYNDROME 159
mean NK function at baseline in those patients who began the trial on placebo was 124.5 +/- 22.1, 46.8 +/- 15.3, 103.1 +/- 23.9 and 37.5 +/- 13.1 LU for groups 1 to 4, respectively. After 12 weeks of placebo, the mean score was unchanged from baseline for all four groups. Conversely, after 12 weeks of interferon therapy, the score was increased significantly for groups 2, 3 and 4, with the most impressive significance for group 4 (F= 4.69; p<.Ol).
Four patients withdrew prematurely from the study (all from group 3). The baseline immunologic parameters for these patients were within 1 standard deviation of the mean for their respective group. When their values were included in the analysis, the means were not significantly altered.
The mean CD4 count was 836 +/- 31 6 cells/ mm3 (normal range 483-1 532); in 4/30 patients the value was below normal range. In one patient from group 4, the count rose from 422 to 673 after 12 weeks of interferon therapy. The score did not change significantly in any other patient. Mean CD8 count was 344 +I- 98 cells/mm3 (normal range 261 -876); in 9/30 patients the value was below normal range. The score did not change significantly during the trial in any subject. No patient had a CD4 or CD8 count that was above the normal range.
Clinical outcome: Each of the four patients that withdrew from the study was receiving interferon at the time of early withdrawal. Two patients were discontinued because of neutropenia (one patient after 10 weeks of interferon, and the other after 8 weeks). One patient withdrew after one week secondary to palpitations (she had a 30 year history of insulin-dependent diabetes mellitus and possible cardiac microvascular atherosclerotic occlusion) and the other patient because of worsened fatigue (after 6 weeks). Four patients complained of significant flu-like symptoms (fevers, muscle aches, headache) within 6 hours of the initial dose of new medication, either at the beginning of the study or at the time of crossover. Two patients complained of new- onset diarrhea. Each of these patients were receiving interferon at the time. Nine female patients complained of hair loss at some point during or after interferon therapy.
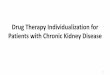
In the clinical evaluation of the entire study group, the mean QOL score at baseline was 35.7 +/- 10.9 and did not change significantly after 12 weeks of placebo (31.4 +/- 9.2; n=l3) or interferon (28.4. +I- 13.8; n=26) therapy. The patients were further evaluated clinically based upon their immunologic parameters. QOL score was not significantly different among the four groups at baseline. For groups 1, 2 and 3 the mean QOL score did not change significantly after 12 weeks of placebo or interferon therapy (Fig. 11). For the three group 4 patients who began the study on placebo, the QOL score was 38.6 4- 10.3 at baseline and did not change significantly after 12
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

160 SEE AND TILLES
B) 60
R
B 40
i ' O 20
10
0
0 2 4 8 time (weeks)
12 16
--t placebo
inmferon
1
0 2 4 8 12 16 time (weeks)
FIGURE II
Mean Qualii of Ufe score after therapy with placebo or interferon. Placebo plots represent those patients who began the trial on placebo. Interferon plots represent subjects who completed 12 weeks of drug therapy followed by 4 weeks of observation or placebo. 60 represents the most severe clinical status. A) All patients (placebo, n=l5; Interferon, n=26) B) Group 4: reduced NK function only (placebo, n=3; interferon, n=7).
weeks of placebo (35.9 +/- 8.5). When all seven patients from group 4 were considered, the mean QOL score at the time of initiation of interferon therapy was 39.7 +I- 12.1, The score improved significantly after 12 weeks of interferon (1 6.3 +/- 7.9, F= 3.87; pc.05) and was maintained after an additional four weeks of placebo or observation (1 4.6 +/- 6.3, F= 3.96; pe.05) but not after 16 weeks (36.1 +/- 10.6, n=4).
DISCUSSION
The results of the current study confirm recent observations of immunologic abnormalities associated with CFS. Diminished in vitro proliferation to mitogens and
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

ALPHA INTERFERON AND CHRONIC FATIGUE SYNDROME 161
soluble antigens was recorded at baseline in most patients. Similar findings have been reported in other studies (8,31), and suggest that in many CFS patients, lymphocytes are subject in vivo to a differentiation stimulus (9). Leading candidates include viruses (33), toxins (34) and hormones (13). Decreased NK function was observed for many patients in the current study, confirming other reports (8,35). One study reported a correlation between diminished NK function and severity of CFS symptomology (36). Finally, in the current study, mean CD4 and CD8 counts were within normal limits, again consistent with other studies (37,38).
Patients with CFS complain of a variety of constitutional symptoms, many of which overlap with the side effects of interferon such as low grade fevers, headaches, myalgias and nausea. Therefore, in the current study, it was felt by the investigators that the blind was adequately maintained although a minority of evaluable patients did report either an exacerbation of baseline symptoms or new symptoms at the onset of interferon therapy. There was suspicion by the investigators that these patients may have been receiving interferon. Hair loss was reported in some patients, but this was a delayed complication and could not easily be associated with interferon use itself.
Great care was used in the current study to control for experimental variables in the functional lymphocyte assays. In our experience, time of day is an important variable; NK function is higher in the morning and lower later in the day. Therefore, samples were obtained at the same time of day on each occasion.
Multiple immunologic (22), psychologic (24) and antiviral (23) therapies have failed to consistently demonstrate clinical efficacy in CFS patients. This would not be surprising if CFS should prove to be a heterogeneous illness with multiple etiologies and pathophysiologic mechanisms.
Because of the subjective nature of the symptoms and the potential for both placebo effect and observer bias, therapeutic trials for CFS must be double-blinded and placebo controlled. Ampligen has demonstrated efficacy for CFS patients in such a study (24). This drug is an immunopotentiator, with strong stimulation of interferon production in vivo. The results of the current double-blind, placebo-controlled trial with alpha interferon itsetf are consistent with the above study. In addition, a subgroup that benefits most has been characterized immunologically (decreased NK function and normal lymphocyte proliferation).
The mechanism leading to diminished NK function is not known. If the decrease is primary it could result in persistent infection once certain specific viruses are introduced. On the other hand, if the decrease in NK function is secondary to virus infection, the decreased NK function may serve as a marker for persistent infection. A recent study has reported tropism of HHV-6 for NK cells, and demonstrated in vitro
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

162 SEE AND TILLES
lysis of NK cells by the virus (39). One or more of several possible explanations may be responsible for the beneficial effects observed in the current study: 1) Interferon may have had its characteristic direct antiviral effects on persistent viral infections in the responders to treatment. 2) Stimulation of NK function by interferon may have secondarily enhanced the host resistance to one or more persistent, NK-sensitive viruses such as CMV, EBV, HHV-6, enteroviruses or retroviruses. 3) Since NK cells are important in the regulation of the immune system via the secretion of several cytokines (40) and abnormal immune function and cytokine production has been postulated as contributing to the symptomology of CFS (41), the beneficial effects observed in the current study may be due to enhancement of cytokine production by interferon-stimulated NK cells leading to a restoration of normal immune function.
In conclusion, alpha inteferon therapy was particularly effective in that subset of patients with CFS who had diminished NK function and normal lymphocyte proliferation. The specific mechanisms in CFS both for diminished NK function and for the clinical efficacy of interferon are still to be determined.
ACKNOWLEDGEMENTS
We greatfully acknowledge the nursing assistance of Thelma DuPre, the statistical advice provided by Robert Friis, and the data entry performed by Tuyet Bui.
REFERENCES
1. G. Holmes , J. Kaplan , J. Stewart, B. Hunt, P. Pinsky and L. Schonberger, JAMA,
2. G. Holmes, J. Kaplan , N. Gantz, A. Komaroff, L. Schonberger, S. Straus , J. 257, 2297-2302 (1 987).
Jones, R. Dubois, C. Cunningham-Rundles, S. Pahwa, G. Tosato, L. Zegans, D. Purtilo , N. Brown and R. Schooley, Annals Intern. Med., 108, 387-389 (1988).
3. J. Jones, Rev. Infect. Dis., 13 fSuppl 11, S26-S32 (1991). 4. A. Komaroff , A. Geiger and S. Wormsley, Lancet, 1, 1288-1289 (1988).
5. I. Salit, Can. Med. Assoc. J., 133, 659-663 (1985). 6. W. Gin, F. Christianson and J. Peter, Med. J. Aust., 151, 1 17-1 18 (1 989). 7. A. Morag, M. Tobi, 2. Ravid, M. Revel and A. Schattner, Lancet, 1, 744 (1982).
8. R. Kibler, D. Lucas, M. Hicks, B. Poulos and J. Jones, J. Clin. Immunol., 5, 46-54
9. S. Straus, S. Fritz, J. Dale, B. Gould and W. Strober, J. Clin. Imrnunol., B, 30-40 (1 985).
(1993).
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

163 ALPHA INTERFERON AND CHRONIC FATIGUE SYNDROME
10. C. Chao, E. Janoff, S. Hu, K. Thomas, M. Gallagher, M. Tsang and P. Peterson,
1 1 . D. Buchwald and A. Komaroff, Rev. Infect. Dis., 13 (Suppl 11, S12-Sl8 (1991). 12. M. Kruesi, J. Dale and S. Straus, J. Clin. Psychiatry, 50, 53-56 (1989).
13. M. Demitrack, J. Dale, S. Straus, L. Laue, S. Listwak, M. Kruesi, G. Chrousos and P. Gold, J. Clin. Endocrinol. Metab., 73, 1224-1234 (1991).
Medical Press, New York, (1993).
Wroblewski, M. Palladino, J. Woodward and H. Koprowski, Proc. Nat. Acad. Sci.
Cytokine, 3, 292-298 (1991).
14. J. Goldstein, Chronic Fatigue Syndrome: the Limbic Hypothesis, Haworth
15. E. DeFrietas, B. Hilliard, P. Cheney, D. Bell, E. Kiggundu, D. Sankey, Z.
USA, 88, 2922-2926 (1991). 16. G. Yousef, G. Mann, D. Smith, E. Bell, V. Murugesan, R. McCartney and J.
17. S. Straus, G. Tosato, G. Armstrong, T. Lawley, 0. Preble, W. Henle, R. Davey, G.
18. J. Jones, C. Ray, L. Minnich, M. Hicks, R. Kiblerand D. Lucas, Ann. Intern. Med.,
Mowbray, Lancet, 1, 146-1 50 (1 989).
Pearson, J. Epstein, I. Brus and M. Blaese, Annals Intern. Med., 102, 7-1 6 (1 985).
lQ2, 1-7 (1985). 19. D. Buchwald, A. Freedman, D. Ablashi, J. Sullivan, M. Caligiuri and D. Weinberg,
20. P. Behan and W. Behan, CRC Crit. Rev. Neurobiol., 4, 157-178 (1988). 21. A. Lloyd, I. Hickie, D. Wakefield, C. Boughton and J. Dwyer, Am. J. Med., 89, 561
568 (1 988). 22. P. Peterson, J. Shepard, M. Macres, C. Schenck, J. Crosson, D. Rechtman and N.
Lurie, Am. J. Med.,89, 554-560 (1990).
J. Clin. Immunol., 10, 335-344 (1990).
23. S. Straus, J. Dale, M. Tobi, T. Lawley, 0. Preble, R. Blaese, C. Hallahanand W.
24. A. Lloyd, I. Hickie, A. Brockman, C. Hickie, A. Wilson, J. Dwyerand D. Wakefield,
25. D. Strayer, W. Carter, 1. Brodsky, P. Cheney, D. Peterson, P. Salvato, C.
Henle, N. Engl. J. Med., 319, 1692-1698 (1988).
Am. J. Med., 94, 197-203 (1993).
Thompson, M. Loveless, D. Shapiro, W. Elsasserand D. Gillespie, Clin. Infect. Dis., 18 (supp l), S88-95 (1994).
26. A. Silva, B. Bonavida and S. Targan, J. Immunol., 125, 479-84 (1980). 27. H. Kikuta, A. Nikane, H. Lu, Y. Taguchi, T. Minagawa and S. Matsumoto, J. Infect.
28. R. Dorr, Drugs, 45, 177-21 1 (1993). Dis., 162, 35-38 (1990).
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016

164 SEE AND TILLES
29. S. Donohue, B. Wonke, A. Hoffbrand, J. Reittie, K. Ganeshaguru, P. Scheuer, D. Brown and G. Dusheiko, Br. J. Hematol., 83, 491-97 (1993).
30. M. Brook, B. Bannister and W. Weir, J. Infect. Dis., 168, 791 -2 (1 993).
31. S. Gupta and 8. Vayuvegula, Scand. J. Immunol., 33, 319-327 (1991). 32. H. Pross, M. Baines and P. Rubin, J. Clin. Immunol., 1, 51-63 (1981). 33. J. Gow, W. Behan, K. Simpson, F. McGarry, S. Keir, and P. Behan, Clin. Infect.
34. P. Behan and B. Haniffah, Clin. Infect. Dis., 18 (suppl l), S54 (1994).
35. M. Caligiuri, C. Murray, D. Buchwald, H. Levine, P. Cheney, D. Peterson, A.
36. A. Emmanuel, E. Ojo-Amaize, E. Conley and J. Peter, Clin. Infect. Dis., 18 (supp
37. P. Behan, W. Behan and E. Bell, J. Infect. Dis., 10, 21 1-222 (1985). 38. L. Borysiewicz, S. Haworth, J. Cohen, J. Mundin, A. Rickinson and J. Sissons,
39. P. Lusso, M. Malnati, A. Garzino-Demo, R. Crowley, E. Long and R. Gallo,
40. G. Trinchieri, Adv. Immunol., 47, 187-376 (1 989). 41. P. Cheney, S. Dorman and D. Bell, Ann. Intern. Med., 110, 321 (1989).
Dis., 18 (suppl 11, S126-129 (1994).
Komaroff and J. Rib, J. Immunol., 139, 3306-3313 (1987).
3, S157-159 (1994).
Q .J. Med., SS, 111-121 (1986).
Nature, 362, 458-462 (1993).
Dow
nloa
ded
by [U
nive
rsity
of T
oron
to L
ibra
ries]
at 2
0:52
17
Mar
ch 2
016