Embed Size (px)
Citation preview
Also known nationally as the Chronic Disease Self-Management Program
- Developed by Stanford University -
Living Well with Chronic Conditions
Introductory Note
• The Utah Approach to CDSMP and Diabetes Care: In no way is CDSMP to take the place of Diabetes Self-Management Education (DSME)
• DSME comes first and foremost for a patient with diabetes
• We would like to view CDSMP as complementary/supportive to the DSME process

Utah Arthritis Program
• Leads the administration of the Chronic Disease Self-Management Program in Utah
• Funding sources are the Centers for Disease Control and Prevention (CDC) and the Administration on Aging (AoA)
• Work in partnership with the CDC and AoA to address the burden of arthritis, and other chronic diseases, in Utah
• Primary objective is to develop partnerships around the state to increase access to and use of evidence-based programs
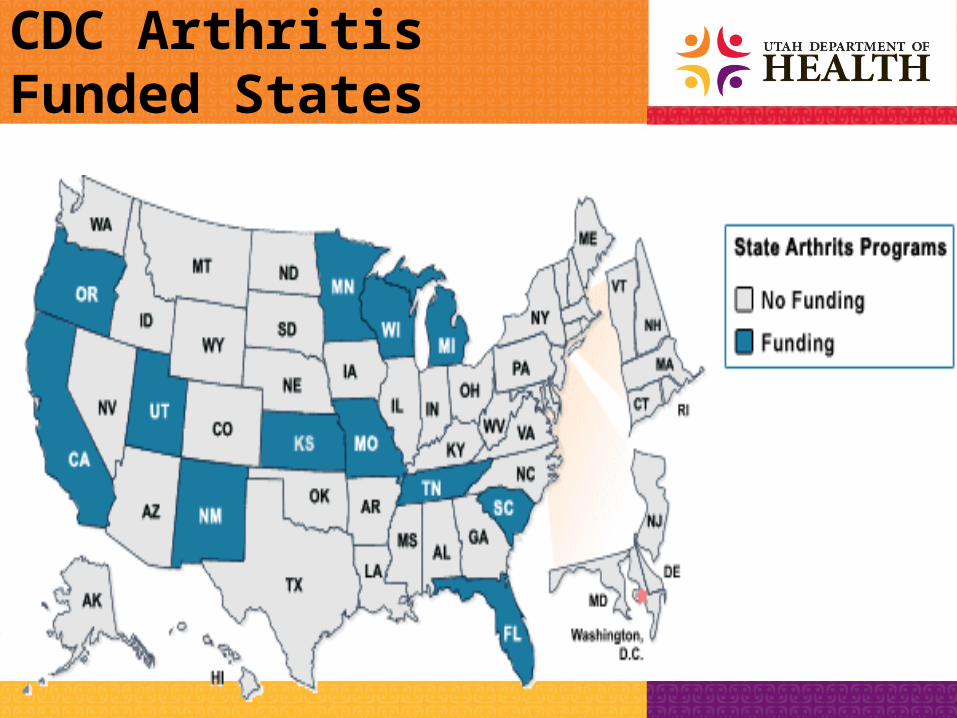
CDC Arthritis Funded States
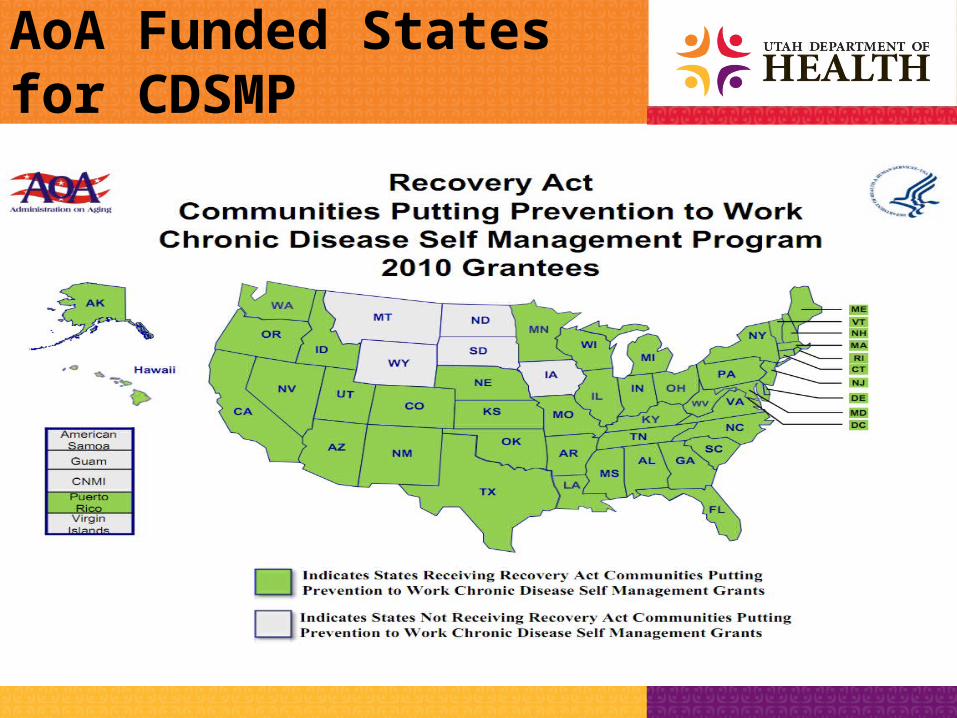
AoA Funded States for CDSMP
Our Broad Goal
To improve the quality of life for people affected by arthritis and other chronic conditions.
I love CDSMP
and ADEU!
The Chronic Disease Problem
Research has shown that an increasing number of U.S. families are experiencing high financial burdens from medical care expenses, as rapidly rising health care costs are passed on to families in the form of higher premiums, deductibles, co-payments, and even reduced benefits. For people with chronic health conditions, such burdens can be a long-term problem that threatens their families' financial well-being.
Commonwealth Fund (July 23, 2009)
The Chronic Disease Problem
• Approximately 30% of Utahns have at least one chronic condition (similar number for U.S.)
• Chronic diseases are the most prevalent and costly healthcare problems in the U.S.
• More than two-thirds of all deaths are caused by one or more of five chronic conditions: heart disease, cancer, stroke, COPD, and diabetes
Sources: BRFSS, 2007; Centers of Disease Control and Prevention (CDC)

The Chronic Disease Problem
• Chronic disease not only affects health and quality of life, but is also a major driver of healthcare costs…
• Chronic disease accounts for about 75% of the Nation’s aggregate healthcare spending, or about $5,300 per person in the U.S. each year
• In taxpayer-funded programs, treatment of chronic disease constitutes an even larger proportion of spending:
• 96 cents per dollar for Medicare
• 83 cents per dollar for Medicaid
Source: Centers of Disease Control and Prevention (CDC)

Chronic Disease Rates
Age-adjusted Rates:Utah Data: Utah BRFSS 2009U.S. Data: National Center for Chronic Disease Prevention and Health Promotion, BRFSS Survey
Utah
High Cholesterol 25.9%
Hypertension 25.4%
Arthritis: 24.0%
Asthma: 7.9%
Diabetes: 6.9%
U.S.
High Cholesterol 37.6%
Hypertension 26.7%
Arthritis: 26.1%
Asthma: 8.5%
Diabetes: 8.5%
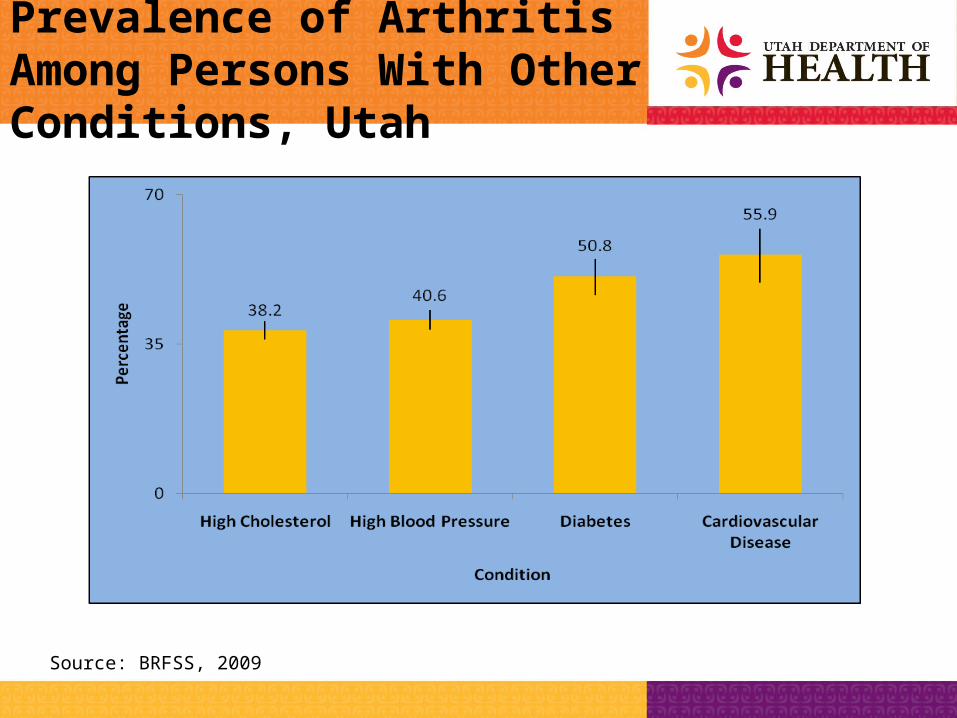
Prevalence of Arthritis Among Persons With Other Conditions, Utah
Source: BRFSS, 2009
Stanford’s CDSMP
• In the past 20 years or so, the Stanford University, Patient Education Research Center has developed, tested, and evaluated self-management programs for people with chronic health problems
• All programs are designed to help people gain self-confidence in their ability to control their symptoms and how their health problems affect their lives
• Workshops are highly interactive, focusing on building skills, sharing experiences and support
Stanford’s CDSMP
• Once a program is developed, it is evaluated for effectiveness through a randomized, controlled trial, which is 2-4 years in length
• It is ONLY after a program has been shown to be safe and effective through these trials that it is released for dissemination
• This was the procedure for the Chronic Disease Self-Management Program (CDSMP)
Chronic Conditions Represented in CDSMP Workshops
• 52.7% Arthritis• 41.0% High Blood Pressure• 36.6% Chronic Joint Pain• 34.8% Diabetes• 33.2% High Cholesterol• 27.4% Chronic Pain • 23.5% Depression
• 17.2% Heart Disease• 14.3% Asthma• 13.2% Lung Disease• 12.8% Fibromyalgia• 8.0% Cancer• 7.6% Kidney Disease
Source: Utah Arthritis Program, 2010
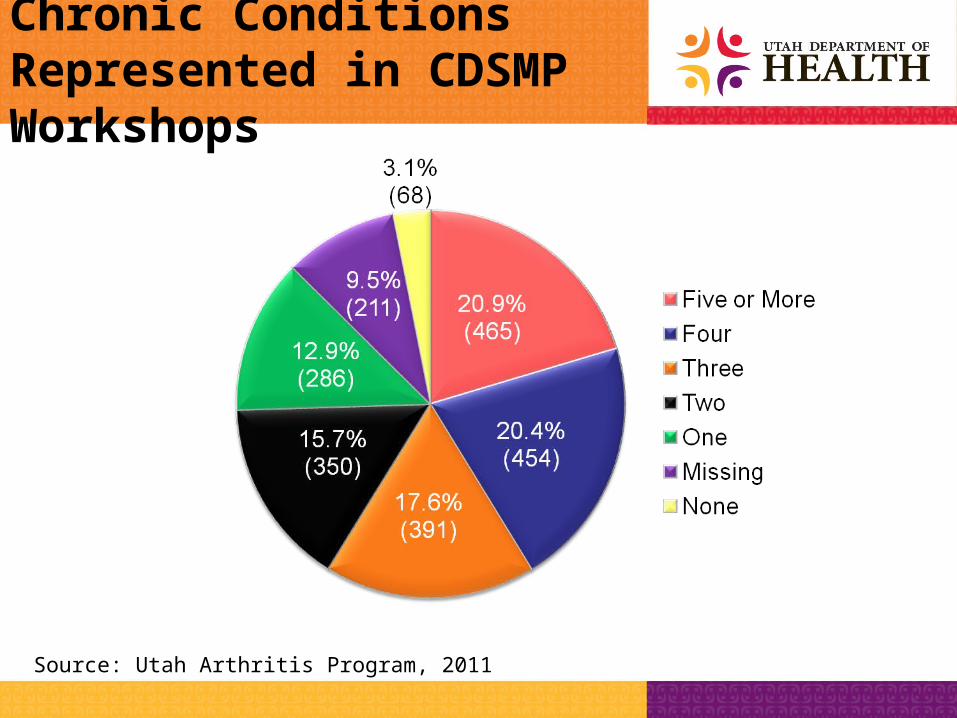
Chronic Conditions Represented in CDSMP Workshops
Source: Utah Arthritis Program, 2011

Living Well with Chronic ConditionsStanford Model of CDSMP
Living Well with Chronic ConditionsStanford Model of CDSMP
Program Description– Designed for people who live with any chronic
condition– Based on the symptoms of chronic conditions– Participants learn tools that enable them to
self-manage their symptoms– Community or healthcare-based settings
Living Well with Chronic ConditionsStanford Model of CDSMP
Patient Engagement Activities
– Participants learn how to identify problems
– Participants learn how to act on problems
– Participants learn how to generate short-term action plans
– Participants learn problem-solving skills related to chronic conditions in general

Living Well with Chronic ConditionsStanford Model of CDSMP
Program Subject Matter:– Dealing with frustration, fatigue, pain and
isolation– Exercise for maintaining and improving
strength, flexibility and endurance– Appropriate use of medication and proper
nutrition– Communicating effectively with family, friends
and health professionals– Evaluating new treatments
Living Well with Chronic ConditionsStanford Model of CDSMP
Program Structure
• Series of 6 sessions, 1 session per week, 2 hours per session
• Held in community settings (including healthcare)
• Highly scripted curriculum
Living Well with Chronic ConditionsStanford Model of CDSMP
Program Structure
• Designed to be lay-led; 2 leaders facilitate each class; at least 1 facilitator also has a chronic condition
• Workshops offered at no charge (free!)
• Available in Utah in English, Spanish, Tongan
Living Well with Chronic ConditionsStanford Model of CDSMP
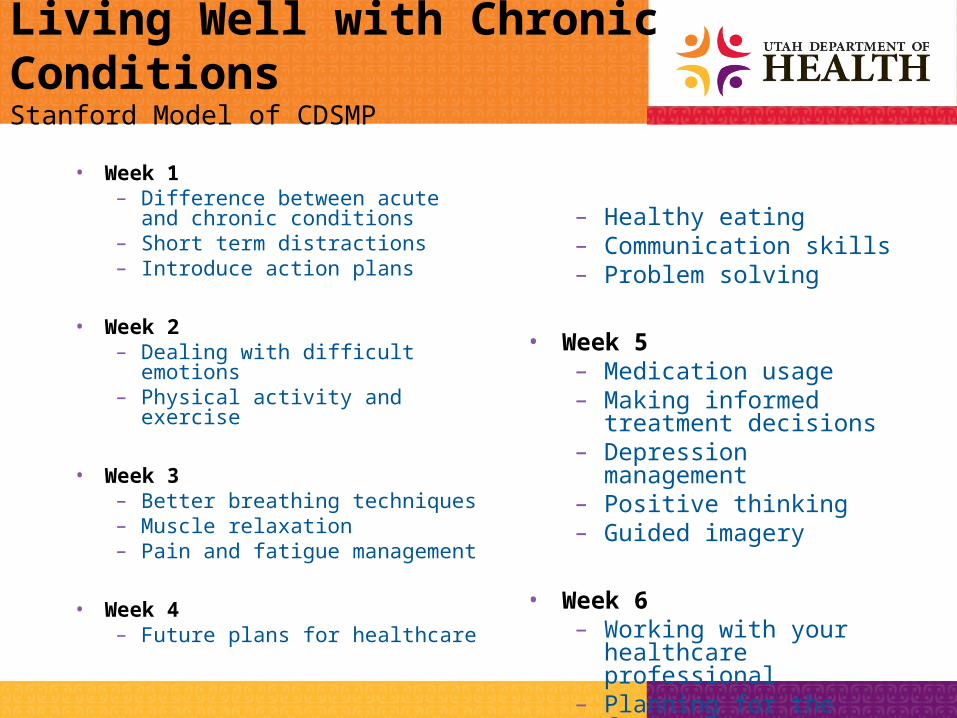
• Week 1– Difference between acute and
chronic conditions– Short term distractions– Introduce action plans
• Week 2– Dealing with difficult emotions– Physical activity and exercise
• Week 3– Better breathing techniques– Muscle relaxation– Pain and fatigue management
• Week 4– Future plans for healthcare
– Healthy eating– Communication skills– Problem solving
• Week 5– Medication usage– Making informed treatment
decisions– Depression management– Positive thinking– Guided imagery
• Week 6– Working with your
healthcare professional– Planning for the future
Living Well with Chronic ConditionsStanford Model of CDSMP
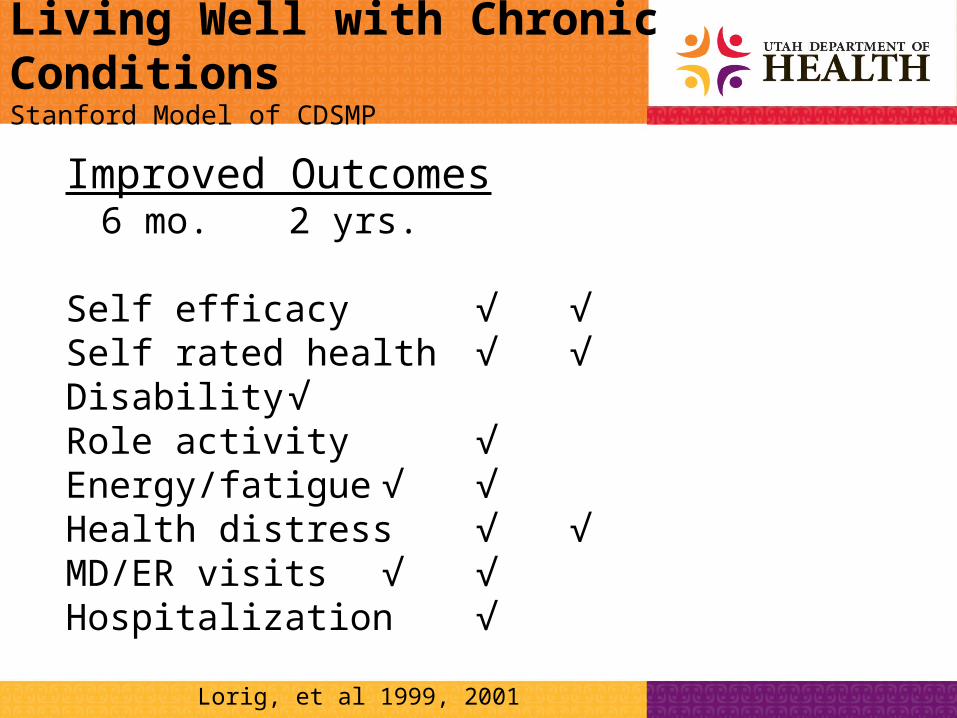
Improved Outcomes6 mo. 2 yrs.
Self efficacy √ √Self rated health √ √Disability √Role activity √Energy/fatigue √ √Health distress √ √MD/ER visits √ √Hospitalization √
Lorig, et al 1999, 2001
Living Well with Chronic ConditionsStanford Model of CDSMP
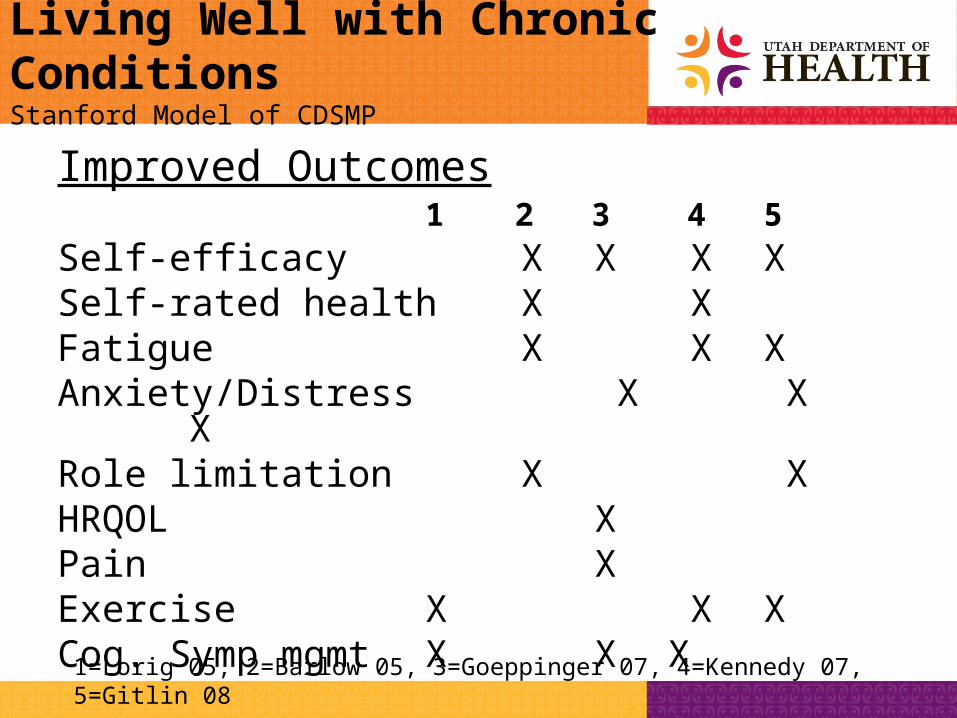
Improved Outcomes 1 2 3 4 5
Self-efficacy X X X XSelf-rated health X XFatigue X X XAnxiety/Distress X X XRole limitation X XHRQOL XPain XExercise X X XCog. Symp mgmt X X X
1=Lorig 05, 2=Barlow 05, 3=Goeppinger 07, 4=Kennedy 07, 5=Gitlin 08
Living Well with Chronic ConditionsStanford Model of CDSMP
Action Plans
– Something they want to do
– Achievable
– Confidence Level
– Problem Solving
– Action Specific
– What
– How much
– When
– How often

Living Well with Chronic ConditionsStanford Model of CDSMP
Workshop Resources
• Resource book: Living a Healthy Life with Chronic Conditions
• CD: Time for Healing
• Weekly action plans and feedback
• Groups are small: 10-15 people
– Share information, interactive learning activities, problem-solving, decision-making, social support for change
Living Well with Chronic ConditionsStanford Model of CDSMP
Infrastructure• Master Trainers – 11 in state of Utah as of
October 2011 (8 English, 2 Spanish)– Attend 4 ½ day training at Stanford University– Teach classes and train leaders
• Peer Leaders / Instructors– Complete 4-day training taught by 2 Master Trainers in order to
teach classes
• Stanford License – Each organization teaching this program must purchase a
license from Stanford
• Training Material– Resource books and CDs for participants and leaders
Living Well with Chronic ConditionsStanford Model of CDSMP
What participants are saying. . . .
– “I know I can self-manage a few problems and make life better for me and my husband.”
– “It gave me some important coping mechanisms.”
– “This class has helped me get my life in order.”
– “I recommend this course and handbook to all seniors.”
– “We have set goals, accomplished them and will continue to manage our lives better due to this class.”
Source: Class participants of Wasatch and Summit County courses
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Spanish Program Development
• Not a translation but an independent development in Spanish
• Developed to be culturally appropriate
• Focus groups conducted in Spanish
• Health care professionals working with persons with chronic conditions
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Spanish Program Development
• Participants incorporate healthy habits into their lives:– Healthy eating habits
– Exercise (physical activity)
– Cognitive management of symptoms
– Better communication with health care providers
– Overall perception of better health

Tomando Control de Su SaludStanford Model of Spanish CDSMP
Overview/
responsibilities Acute/chronicUsing
mind/symptoms Action plans
English
Overview/Responsibilities Acute/chronic Proactive in
management, Importance of food &
exercise Healthy food
Spanish
Week One
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Action plan rpt/problem solve
Difficult emotions Intro to physical
activity/exercise Action plan
English
Share diaries/problem solve
Formula for a healthy menu
Action plans
Intro to physical activity/exercise
Exercise practice
Spanish
Week Two
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Week ThreeAction plan
report/problem solve Better breathing Muscle relaxation Pain/fatigue
management Endurance activities Action plan
English
Action plan rpt/problem solve
Prepare a low fat menu
Managing symptoms Muscle relaxation Better breathingAction plan
Spanish
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Week FourAction plan
report/problem solve Future plans for health
careHealthy eating Communication skills Problem solvingAction plan
English
Action plan rpt/problem solve
Reading nutrition labels
Finding health care
Managing depression
Positive thinking
Action plan
Spanish
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Week FiveAction plan
report/problem solve Medication usage Informed treatment
decisions Depression managementPositive thinking Guided
imagery Action plan
English
Action planreport/problem solve
Communication skillsFuture plans for healthcare Increasing physical activity
intensityMedication usageWorking with healthcare
professional Action plan
Spanish
Tomando Control de Su SaludStanford Model of Spanish CDSMP
Week Six
Action plan rpt/problem solve
Working with health care Professional/health care system
Looking back and plan future
English
Action plan rpt/problem solve
Evaluating home remedies
Guided imagerySharing
successes/plan future
Celebration
Spanish
Ideas for Linking CDSMP with Diabetes Education
• The Utah Approach to CDSMP and Diabetes Care: In no way is CDSMP to take the place of Diabetes Self-Management Education (DSME)
• DSME comes first and foremost for a patient with diabetes
• That said, we would like to encourage referrals from Diabetes Programs into local CDSMP classes for some of the following reasons….

Ideas for Linking CDSMP with Diabetes Education
• Self-management support option for post-DSME (National DSME Standard #7)
• Great option for follow up work with patients with diabetes (National DSME Standard #8)
• Supports and complements self-management efforts of diabetes educators/healthcare providers
• Continuous quality improvement opportunity??
Ideas for Linking CDSMP with Diabetes Education
• Powerful evidence-based program for patients with co-morbid conditions– CDSMP is successful at addressing mental health
issues as well
• Excellent self-management option for uninsured patients; if you have to turn away uninsured patients, please send them to a free CDSMP workshop
• Addresses income issues by offering classes at no charge
Ideas for Linking CDSMP with Diabetes Education
• Opportunity to connect to community resources (perhaps as part of a planned care model)
• Reinforces lifestyle behaviors so that patients continue implementing healthy choices such as regular physical activity and nutrition
• Other ideas?
Living Well with Chronic ConditionsStanford Model of CDSMP
General Patient and Provider Benefits
• An evidence-based program such as Living Well/CDSMP can capture many chronic diseases through this one channel
• Self-management support option
• Can improve self-rated health and energy levels
• Reduced healthcare utilization (ED visits)
• As the New Jersey program puts it: Feel Better!

Living Well with Chronic ConditionsStanford Model of CDSMP
Program Partnerships
• University of Utah Community Clinics
• Arthritis Foundation, Utah/Idaho Chapter
• Area Agencies on Aging/Senior Centers:– Weber-Morgan
– Davis County
– Salt Lake County
– Mountainlands (Summit/Wasatch/Utah Counties)
– Five County (Southwest Utah)
– Tooele County
– San Juan County
Living Well with Chronic ConditionsStanford Model of CDSMP
Program Partnerships
• Community-based Organizations:– National Tongan American Society
– Alliance Community Services (Spanish)
• Local Health Departments:– Bear River
– Central Utah
– Davis County
– Salt Lake Valley
– Southwest– Tri County– Utah County– Weber-Morgan
Living Well with Chronic ConditionsStanford Model of CDSMP
Program Partnerships
• Dixie Regional Medical Center in St. George
• Valley View Medical Center in Cedar City
• Salt Lake VA Medical Center
• Valley Mental Health– SL County, Park City, Tooele
• Utah Partnership for Healthy Weight– Healthy weight project in Magna
Living Well with Chronic ConditionsStanford Model of CDSMP
Resources– Stanford University’s site on CDSMP
http://patienteducation.stanford.edu
– Utah Arthritis Program (class schedules) http://health.utah.gov/arthritis
– Administration on Aging: www.aoa.gov
– National Council on Aging: http://healthyagingprograms.org
Living Well with Chronic ConditionsStanford Model of CDSMP
Contact Information
• Utah Arthritis Program: www.health.utah.gov/arthritis (for class schedules)
• Rebecca Castleton: [email protected];
801-538-9340
• Christine Weiss: [email protected];
801-538-9458
Help Your Clients Help Your Clients Quit Tobacco Quit Tobacco
Marci Nelson, B.S., CHESMarci Nelson, B.S., CHES
Tobacco Prevention and Control ProgramTobacco Prevention and Control Program
Utah Department of HealthUtah Department of Health
[email protected]@utah.govhttp://www.tobaccofreeutah.org/healthcare.htmlhttp://www.tobaccofreeutah.org/healthcare.html
(801) 538-7002(801) 538-7002
ObjectivesObjectives Discuss the risks of tobacco use especially the Discuss the risks of tobacco use especially the
effects of smoking on diabeteseffects of smoking on diabetes
Present Present a brief interventiona brief intervention to quit to quit
Discuss procedures for implementationDiscuss procedures for implementation
Supply information on free tobacco cessation Supply information on free tobacco cessation servicesservices
Tobacco Use in Utah:Tobacco Use in Utah:The ProblemThe Problem
More than 200,000 Utahns use tobaccoMore than 200,000 Utahns use tobacco More than 1,330 die annually from their smokingMore than 1,330 die annually from their smoking Nearly 17,150 children exposed to secondhand Nearly 17,150 children exposed to secondhand
smoke in their homessmoke in their homes $663 million each year in smoking-attributable $663 million each year in smoking-attributable
medical and lost productivity costsmedical and lost productivity costs
Source: Tobacco Prevention and Control in Utah Tenth Annual Report - August 2010Source: Tobacco Prevention and Control in Utah Tenth Annual Report - August 2010
Tobacco Health Effects
Long-term Heart disease Stroke Lung function Cancers Ulcer Infertility
Short-term Respiratory illness Decreased lung capacity High blood pressure &
cholesterol Nervousness Mouth problems Reduced taste & smell
Responsible for more than 400,000 premature deaths each year in the U.S.
Health Effects of Secondhand Smoke Stillbirth; miscarriage Premature Birth Cleft palates and lips Sudden Infant Death Infertility Tooth Decay
Cancer Bronchitis;
pneumonia Asthma Upper Respiratory
Tract Disease Ear Infections Coughs
Secondhand smoke affects loved ones & is a Secondhand smoke affects loved ones & is a powerful motivator to quit!powerful motivator to quit!

Effect of Smoking on Diabetes
Tobacco raises blood sugar levelsTobacco raises blood sugar levels Tobacco use increases the risk of heart attack Tobacco use increases the risk of heart attack
or stroke or stroke Increased chance of getting gum disease and Increased chance of getting gum disease and
may suffer tooth lossmay suffer tooth loss Tobacco use can make foot ulcers, foot Tobacco use can make foot ulcers, foot
infections, and blood vessel disease in the legs infections, and blood vessel disease in the legs worseworse

WHY SHOULD CLINICIANS ADDRESS TOBACCO?
Tobacco users expect to be encouraged to quit by health professionals.
• 72% of Utahns saw a healthcare provider in the last year
Screening for tobacco use and providing tobacco cessation counseling are positively associated with patient satisfaction (Barzilai et al., 2001).
Advice from a healthcare provider can double the chances of successful quitting.
Clinical Practice Guideline for Treating Clinical Practice Guideline for Treating Tobacco Use and DependenceTobacco Use and Dependence
Update released May 2008Update released May 2008 Sponsored by the Agency for Healthcare Sponsored by the Agency for Healthcare
Research and Quality of the U.S. Public Research and Quality of the U.S. Public Heath Service withHeath Service with Centers for Disease Control and Centers for Disease Control and
PreventionPrevention National Cancer InstituteNational Cancer Institute National Institute for Drug AddictionNational Institute for Drug Addiction National Heart, Lung, & Blood National Heart, Lung, & Blood
InstituteInstitute Robert Wood Johnson FoundationRobert Wood Johnson Foundation
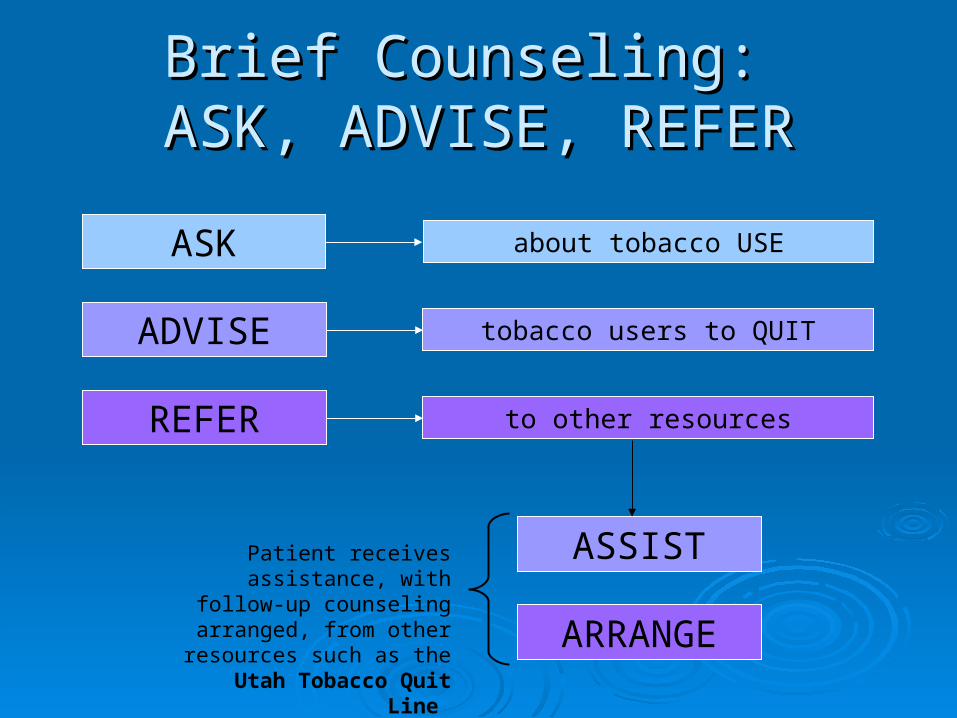
Brief Counseling: Brief Counseling: ASK, ADVISE, REFERASK, ADVISE, REFER
ASK about tobacco USE
ADVISE tobacco users to QUIT
REFER to other resources
ASSIST
ARRANGE
Patient receives assistance, with follow-up counseling arranged,
from other resources such as the Utah Tobacco Quit Line
Step 1: Step 1: ASK ASK 1 min1 min
Ask EVERY patient about tobacco use status at Ask EVERY patient about tobacco use status at EVERY visit. EVERY visit.
• Current Current • Former Former • NeverNever
This occurs most consistently when there are systems This occurs most consistently when there are systems in place, such as question on intake form, chart in place, such as question on intake form, chart stickers, or electronic prompts on electronic medical stickers, or electronic prompts on electronic medical records. Chart stickers are available.records. Chart stickers are available.

Step 2: Step 2: AdviseAdvise 1 min1 min
Clinicians should urge all tobacco users to quit.Clinicians should urge all tobacco users to quit.
Even brief advice to quit by a clinician results in greater Even brief advice to quit by a clinician results in greater quit rates. Smokers cite a clinician's advice to quit as an quit rates. Smokers cite a clinician's advice to quit as an important motivator for attempting to stop smoking.important motivator for attempting to stop smoking.
Advice should be:Advice should be:• clearclear• strongstrong• personalizedpersonalized
Specific to the individual 's own situation Specific to the individual 's own situation (e.g. oral health condition, family status, costs of tobacco). (e.g. oral health condition, family status, costs of tobacco).
Offer a motivational intervention, the “5 R's”
RelevanceRisks
RewardsRoadblocksRepetition
What if they are not willing?
The “5 R’s”The “5 R’s”Relevance:Relevance: Why is quitting important to Why is quitting important to
their own personal situation?their own personal situation?
Risks:Risks: Outline the risks of continued Outline the risks of continued tobacco use.tobacco use.
Rewards:Rewards: Outline the benefits of quitting.Outline the benefits of quitting.
Roadblocks:Roadblocks: What are the barriers What are the barriers preventing this person from quitting? preventing this person from quitting? What are some solutions to these barriers?What are some solutions to these barriers?
Repetition:Repetition: Repeat this discussion Repeat this discussion frequently, until the person is ready to frequently, until the person is ready to quit.quit.
Step 3: Step 3: ReferRefer 1 min1 min
Referral options:Referral options: A doctor, nurse, pharmacist, or other clinician, for A doctor, nurse, pharmacist, or other clinician, for
additional counselingadditional counseling The Utah Tobacco Quit LineThe Utah Tobacco Quit Line Utah QuitNetUtah QuitNet Text to QuitText to Quit Local ServicesLocal Services
- Ending Nicotine Dependence (youth)- Ending Nicotine Dependence (youth)
- First Step (pregnant women)- First Step (pregnant women)

Utah Tobacco Quit LineUtah Tobacco Quit Line
Toll free: Toll free: 1.800.QUIT.NOW1.800.QUIT.NOW
- Spanish: 1.877.629.1585- Spanish: 1.877.629.1585
- TTY: 1-877-777-6534- TTY: 1-877-777-6534 Monday-Sunday, 6:00 am to 11:00 pmMonday-Sunday, 6:00 am to 11:00 pm FREEFREE For adults and youthFor adults and youth Services available in English, Spanish and Services available in English, Spanish and
translation in 140 other languagestranslation in 140 other languages
Utah Tobacco Quit Line
• Professional counseling sessions by telephone – up to five 40-minute sessions
• Individualized Quit Plan
• NRT upon qualification (patch, gum or lozenge)
• Tailored resources for Utah residents
1.800.QUIT.NOW
Fax Referral System
“Would you like the Utah TobaccoQuit Line to help
you quit?”
3 Simple Steps
1. Personalize your forms online at: www.tobaccofreeutah.org/utqlprofax.html
2. 2 A’s and R with client. For those ready to quit give them the form to fill out. Verify signature!
3. Fax form in to the Utah Tobacco Quit Line: 1-800-483-3076
*The Quit Line will fax you to inform you of services your patient received.
http://utahquitnet.comhttp://utahquitnet.com
Quitting guide
Medication guide
Expert counseling
Personalized quit plan
24 hour community support
Online NRT purchase
Lifetime membership!Lifetime membership!
Text messaging service that offers Utahns daily Text messaging service that offers Utahns daily quit tips to help them get through the quitting quit tips to help them get through the quitting processprocess Users text READY to 53535 to receive two quit tips Users text READY to 53535 to receive two quit tips
per day via cell phone for 21 days. per day via cell phone for 21 days. • Users will be asked to answer simple questions regarding Users will be asked to answer simple questions regarding
age, gender and zip code. age, gender and zip code. New research suggests that motivational text New research suggests that motivational text
messages more than double the odds that messages more than double the odds that smokers will be able to kick the habit.smokers will be able to kick the habit.
Source: The Lancet, news release, June 29, 2011
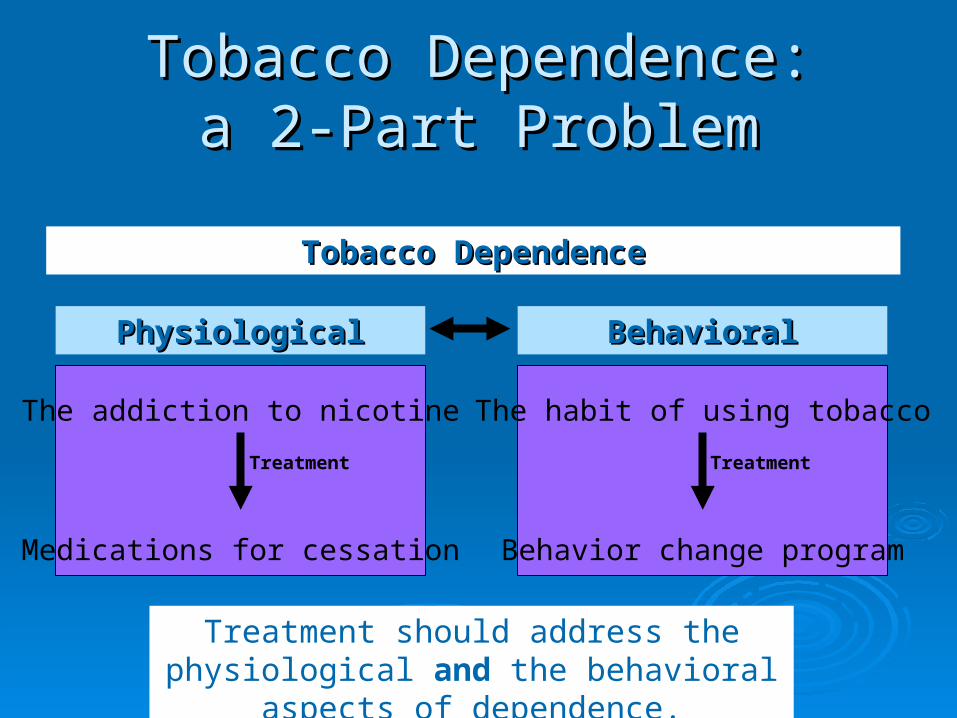
Tobacco Dependence:Tobacco Dependence:a 2-Part Problema 2-Part Problem
Tobacco DependenceTobacco Dependence
Treatment should address the physiological and the behavioral
aspects of dependence.
PhysiologicalPhysiological BehavioralBehavioral
Treatment Treatment
The addiction to nicotine
Medications for cessation
The habit of using tobacco
Behavior change program

Nicotine polacrilex gum Nicorette (OTC) Generic nicotine gum (OTC)
Nicotine lozenge Commit (OTC) Generic nicotine lozenge (OTC)
Nicotine transdermal patch Nicoderm CQ (OTC) Nicotrol (OTC) Generic nicotine patches (OTC, Rx)
Nicotine nasal spray Nicotrol NS (Rx)
Nicotine inhaler Nicotrol (Rx)
Bupropion SR (Zyban)
Varenicline (Chantix)
These are the only medications that are These are the only medications that are FDA-approved for smoking cessation.FDA-approved for smoking cessation.
Smoking Cessation MedicationsSmoking Cessation Medications
What About A Relapse?
Viewed as a learning experience Not a sign of personal or clinician failure Continue to provide encouragement
It takes an average of 7 quit attempts to successfully quit using tobacco!
Make a Commitment
Address tobacco use Address tobacco use with all patients. with all patients.
At a minimum, At a minimum, make a commitment to incorporate brief tobacco make a commitment to incorporate brief tobacco interventions interventions as part of routine patient care.as part of routine patient care.
Ask, Advise, and Refer.Ask, Advise, and Refer.
For more information, contact:Tobacco Free Resource Line: 1-877-220-
3466 orhttp://www.tobaccofreeutah.org/
healthcare1.html





























