Embed Size (px)
Citation preview

Alternating Penalization in the Prevention of AmblyopiaRecurrence
Gunter K. von Noorden, M.D., and Fadia Attiah
Improved or normalized visual acuity in aformerly amblyopic eye has a tendency todeteriorate unless all amblyopiogenic factorsare eliminated. As this can only be rarelyaccomplished, continued therapy to maintainoptimal acuity in the formerly amblyopic eyeis essential. Optic penalization of each eye bytwo pairs of spectacles, overcorrecting eacheye on alternate days, has been effective inpreserving visual acuity in 16 patients whohad been successfully treated for strabismic oranisometropic amblyopia. This maintenancetherapy is continued until the patient is nolonger susceptible to a recurrence of amblyopia.
The goal in treating amblyopia is to restorenormal visual acuity in the affected eye. Occlusion of the sound eye with an adhesive patch isunequivocally effective in enforcing visualstimulation of the amblyopic eye; complete recovery of visual acuity occurs in most instances, provided treatment is begun early inlife. However, once visual acuity has been normalized, the problem arises of how to preventrecurrence of amblyopia. Among the differentstrategies used to avoid such a relapse is alternating penalization. Since, to our knowledge,no data have been presented that show theeffectiveness of this method in an age group inwhich recurrence of amblyopia is common, wepresent the results of alternating penalization
Accepted for publication July 21, 1986. .From the Cullen Eye Institute, Baylor College of Medi
cine, Houston, and the Ophthalmology Service, TexasChildren's Hospital, Houston, Texas. Supported in partby grants EY 01120, EY 07001 and EY 02520 from theNational Institutes of Health, and the Houston DeltaGamma Foundation, Houston. This study was presented in part at the American Association of CertifiedOrthoptists, Southern Region Meeting, New Orleans,April 22, 1986.
Reprint requests to Gunter K. von Noorden, M.D.,Ophthalmology Service, Texas Children's Hospital, Box20269, Houston, Texas 77225.
in formerly amblyopic patients whose visualacuity had been brought back to normal ornear-normal by previous occlusion therapy.
Material and Methods
Sixteen patients with strabismic (n = 14) andanisometropic (n = 2) amblyopia whose visualacuity at the end of occlusion therapy was 20/50or better, and who were then treated withalternating penalization, were selected fromthe clinical material of the OphthalmologyService, Texas Children's Hospital, Houston.The single criterion for selection was thetion of alternating penalization; all patientswho received alternating penalization for 12months or longer were included in this study.The mean duration of treatment was 19.9months with a range of 12 to 48 months. Thepatients' ages at the end of the ambly~pia
therapy and beginning of alternatingtion therapy ranged from 2.5 to 8 years, WIth amean of 5.1 years.
The patients received a prescription fortwo pairs of eyeglasses to be used o~ alternatedays. One pair had a hypermetropic overcorrection of +3.00 diopters sphere incorporatedin the lens of the right eye, and the other pairhad the same overcorrection in the lens for theleft eye. If a significant refractive error w~spresent, this was prescribed for both eyes In
addition to the overcorrection. By varyingthese prescriptions, distance and near visionwere blurred in each eye every other day.Compliance with this treatment was withoutexception excellent, and in many instances better than during the preceding occlusion therapy.
Results
The results are shown in the Figure. Thecolumns present the visual acuity of the ambly-
©AMERICAN JOURNAL OF OPHTHALMOLOGY 102:473-475, OCTOBER, 1986 473

474 AMERICAN JOURNAL OF OPHTHALMOLOGY October, 1986
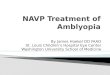
Age (y) 5 8 6 3.5 6 4.5 2.5 3.5 5.5 3.5 7 8 5 4.5 4 5.5Tx (m) 17 20 24 12 15 48 33 24 14 24 12 14 13 16 18 15
20/2020/2520/3220/4020/5020/6320/80
20/10020/12520/15020/20020/25020/30020/400
Figure (von Noorden and Attiah). Results of alternating penalization after completion of amblyopia therapy.
opic eye before and after occlusion treatment,and after alternating penalization. The age atwhich amblyopia therapy stopped and alternating penalization began and the duration ofalternating penalization are listed at the top ofthe Figure. With the exception of the patientwho was 2.5 years old at the end of occlusiontreatment and whose visual acuity was determined with Allen cards, the visual acuity in allother patients was measured with illiterate Esor, age permitting, the Snellen chart at 20 feet.The broken bottom in the first, seventh, ninth,tenth and 15th columns of the Figure indicatesthat amblyopia therapy began at an age atwhich visual acuity could not be measured.Since none of these patients were able to maintain fixation with the amblyopic eye at thebeginning of therapy, it is reasonable to assume that their visual acuity was less than20/200.
The Figure shows that even though all patients in this study belonged to an age group inwhich recurrences of amblyopia are common,such recurrences were prevented by alternatingpenalization. The patients had unchanged visual acuity or an insignificant increase or decrease of visual acuity (Figure, arrows) at theend of penalization treatment.
Discussion
Weiss! first suggested alternating overcorrection of each eye with a +4.00-diopter sphericallens to prevent amblyopia in children between
the ages of 2 and 5 years, or to encourage analternating fixation pattern in those with strabismus but without amblyopia. Other authorshave alluded to the use of alternating penalization,2-4 and we have mentioned the possibilitythat this method may be effective in maintaining a good visual result after amblyopia therapy.5 The present study shows that a recurrenceof amblyopia can indeed be prevented by alternating penalization. Whereas the same effectcan be achieved by alternating occlusion withan adhesive patch, it has been our experiencethat alternating penalization is infinitely moreeasily accepted by the child and the parent.This is especially so in patients who receivedocclusion treatment for many months or evenyears and who consider the opportunity tocontinue therapy with eyeglasses to be a greatrelief.
The question arises when it is safe to discontinue all treatment, including alternating penalization. Complete elimination of the amblyopiogenic factors" in strabismic patients bysurgical or prismatic orthotropization or in anisometropic patients by the appropriate opticalcorrection is rarely accomplished. After surgery the patient is left, as a rule, with a smallangle esotropia or a microtropia. There is nocorrelation between the size of the deviationand the prevalence of strabismic amblyopia,"and the amblyopiogenic mechanisms continueto remain active as long as there is any residualmanifest strabismus. The susceptibility to thedevelopment of amblyopia ends, as a rule, withthe completion of the eighth year of life." butrecurrences of amblyopia are possible as late as

Vol. 102, No.4 Alternating Penalization to Prevent Amblyopia 475
during the early teens," and thus occur longafter the visual system has reached a state ofmaturity.
As the tendency for a recurrence of amblyopia varies greatly from patient to patient, itbecomes necessary to determine the timing ofcessation of therapy individually. We proceedin the following manner: After the best possiblevisual acuity has been obtained by occlusiontherapy, we continue alternating penalizationuntil the age of 6 years. At that time, wediscontinue alternating penalization for sixweeks and remeasure visual acuity. If amblyopia has not recurred, the periods without treatment are extended until it can be shown thatvisual acuity in the formerly amblyopic eye ismaintained. If amblyopia recurs, we immediately resort to conventional occlusion treatment until a previous level of optimal visualacuity has been restored in the amblyopic eye.This is followed by an additional six months ofalternating penalization before the next trial ismade to reduce treatment. Good rapport withthe patient, and, especially with the parents, isessential to gain full cooperation with this rather complicated but ultimately successful therapeutic regimen to maintain a good visual resultin a formerly amblyopic eye.
References
1. Weiss, J.: La surcorrection de 4 dioptries dans Ietraitement du strabisme convergent avec ou sansamblyopie. Bull. Soc. Ophtal. Fr. 12:228, 1968.
2. Quere, M.: Les penalisations optiques dans Ietraitement des amblyopies strabiques. Arch. OphtaImol. 31:877, 1971.
3. Gregersen, E., Pontoppidan, M., and Rindziunski, 0.: Optic and drug penalization and favoringin the treatment of squint amblyopia. Acta Ophthalmol. 52:60, 1974.
4. Berard, P., and Layec-Arnal, M.: Penalization instrabismus. Int. Ophthalmol. 6:13, 1983.
5. von Noorden, G., and Milam, J.: Penalization inthe treatment of amblyopia. Am. J. Ophthalmol.88:511, 1979.
6. von Noorden, G.: Amblyopia. A multidisciplinary approach. Invest. Ophthal. Vis. Sci. 26:52,1985.
7. von Noorden, G., and Frank, J.: Relationshipbetween amblyopia and the angle of strabismus. Am.Orthopt. J. 26:31, 1976.
8. von Noorden, G.: New clinical aspects of stimulus deprivation amblyopia. Am. J. Ophthalmol.92:410, 1981.
9. Gregersen, E., and Rindziunski, 0.: "Conventional" occlusion in the treatment of squint amblyopia. A Itl-year follow-up. Acta Ophthalmol. 43:462,1963.