Embed Size (px)
Citation preview
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
Alternative Budget for Health (“If health is wealth, then, we need to fund for the Filipinos’ wellness!”)
The Proposed Health Budget for CY 2007 The proposed health budget for CY 2007 is P11.66 Billion which accounts for only 1% of the Total Government Budget of P1.126 Trillion and ranks 8th in the budget allocation among National Government Agencies. An increase of P1.021 Billion from its 2006 budget is earmarked for adjustments in Personal Services (Php 397,483,000), the budget gap for the provision of Hepatitis B vaccines (Php 150,198,000), the budget gap for the provision of low-cost quality drugs and medicines including establishment of additional Botika sa Barangay (Php 120,000,000), and in the provision for backlog infrastructures of various retained hospitals (Php354,000,000). Table 22. Summary of Obligations and Proposed New Appropriations by Department (In thousand Pesos)
DEPARTMENTS OBLIGATIONS 2005
(ACTUAL) 2006
(ADJUSTED) 2007
(PROPOSED) 2007
(APPROPRIATION)Education 108,225,263 118,087,260 132,948,493 124,241,854 Public Works and Highways
50,669,829 62,328,189 73,567,928 65,286,040
Interior and Local Government
57,713,297 45,614,998 51,142,791 50,916,522
National Defense 75,615,818 46,642,803 49,462,695 49,326,721 Agriculture (inclusive of the Agricultural and fisheries modernization Program component)
3,263,530 3,197,774 3,292,618 18.5 Billion
3,099,353
State Universities and Colleges
17,508,494 16,666,627 17,815,117 16,645,252
Transportation and Communication
8,538,274 14,257,430 17,505,574 16,531,719
Health 10,5466,975 10,575,633 11,658,832 11,162,998 Commission on Elections 1,855,151 3,280,761 9,809,719 9,717,962 The Judiciary 8,286,882 8,534,736 9,675,485 9,180,831
Although there has been an increasing trend from 2004 to 2007, DOH budget remains lower than its 2002 level. Table 23. Total Distribution by Function, CY 2003 to 2007 (in billion Pesos)
An NGO-Legislators’ Initiative 34
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
2003 2004 2005 2006 2007 PARTICULARS
Amount % Share
Amount
% Share
Amount
% Share
Amount
% Share
Amount
% Share
Administration 1.39 14% 1.38 14% 1.39 14% 1.57 16% 1.8 16% Regulation 0.21 2% 0.21 2% 0.25 3% 0.49 5% 0.59 5% Public health 1.41 14% 1.4 15% 1.13 12% 1.16 12% 1.49 14% Hospital Services
6.89 70% 6.57 69% 6.95 71% 6.75 67% 7.11 65%
TOTAL 9.9 100% 9.56 100% 9.72 100% 9.97 100% 10.99 100% The pattern of DOH budget distribution does not change over the years. Hospital services gets more than 50% of the total DOH budget as depicted in the table. The passage and full implementation of the Local Government Code in 1991 resulted in the decentralization of health services and direct service provision by the Department of Health has been retained and limited only to the 72 DOH managed hospitals and sanitaria all over the country.
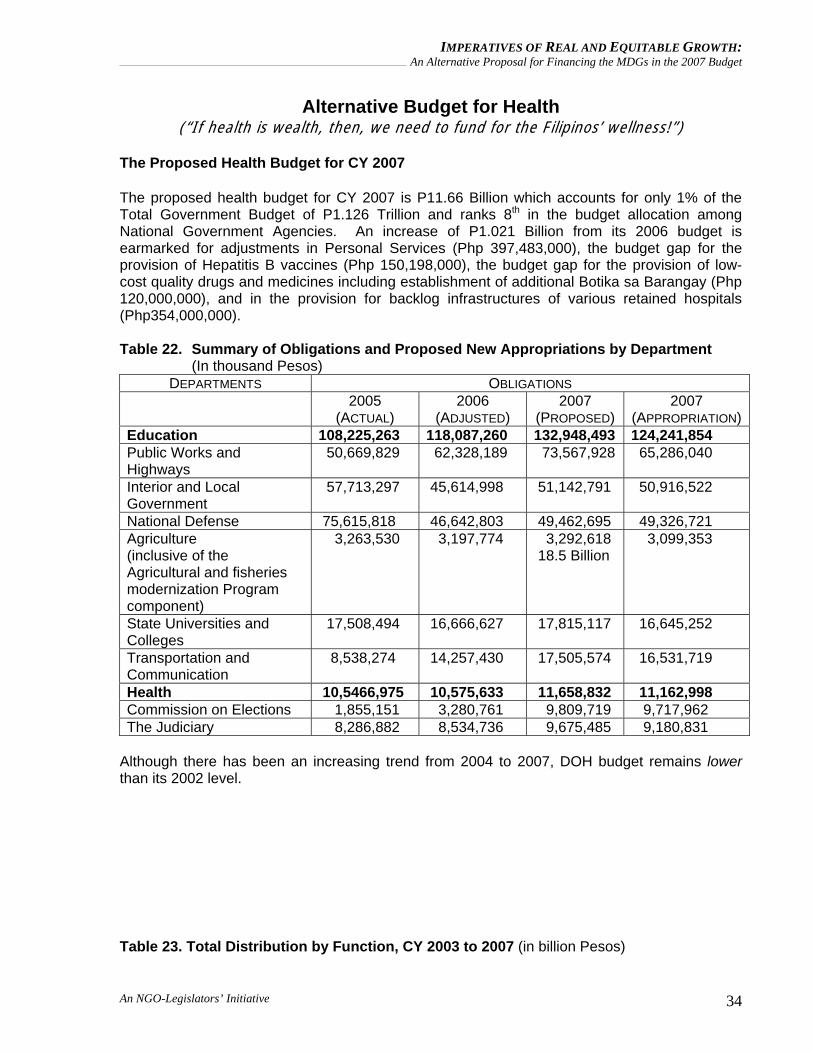
As proposed for CY 2007, hospital services amounting to P7.1 Billion or 65% of the total DOH Budget will be allotted while Public Health will only get a 14% share amounting to P1.49 Billion. (See Figure 7: Presentation of the DOH - Number and Percent Total Distribution by Function)
This figure shows that hospital services gets the biggest share amounting to 7.1 billion or 65% of the total DOH budget. Public health programs has a 14% share (P1.49Billion), general administration services with 16% (P1.80 Billion) and regulation gets 5% (P0.59 Billion).
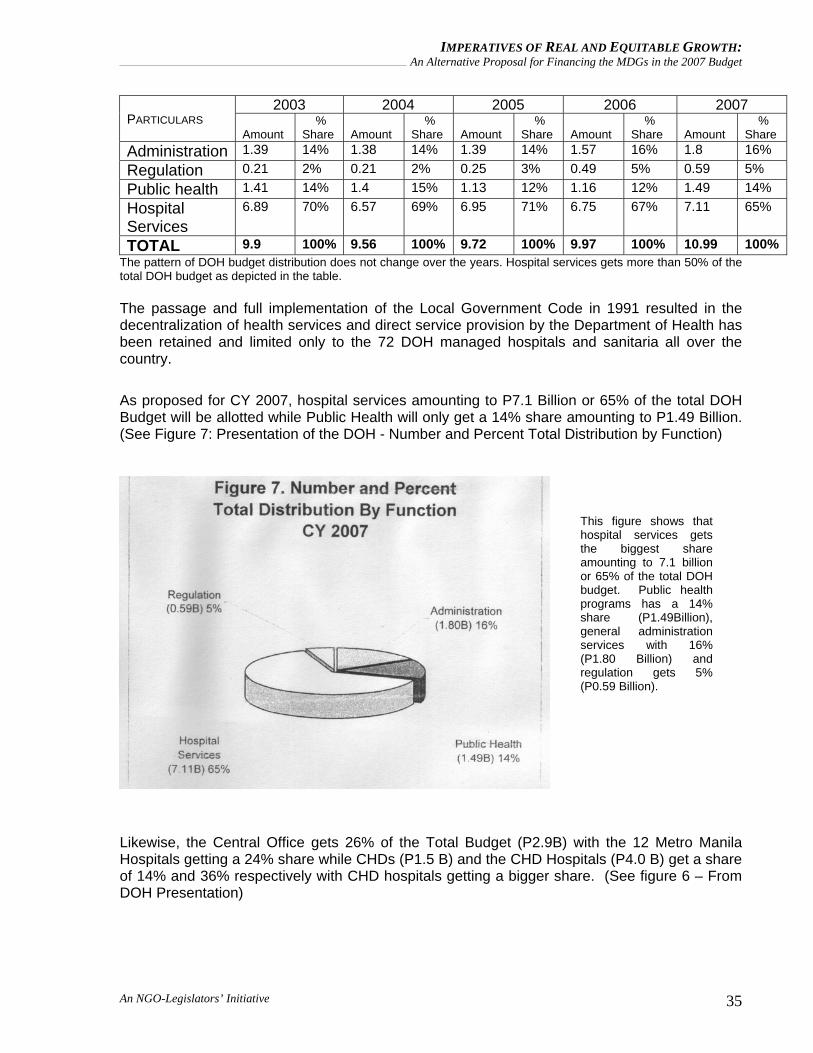
Likewise, the Central Office gets 26% of the Total Budget (P2.9B) with the 12 Metro Manila Hospitals getting a 24% share while CHDs (P1.5 B) and the CHD Hospitals (P4.0 B) get a share of 14% and 36% respectively with CHD hospitals getting a bigger share. (See figure 6 – From DOH Presentation)
An NGO-Legislators’ Initiative 35
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
Compared with the health expenditure of other Asian countries against the GDP, the Philippines registered 3.2% (2003 / National Statistical Board) which is way below the 5% norm set by the World Health Organization (WHO) for developing countries. Table 24. Health Expenditure in Asian Countries, 2001
COUNTRY % OF GDP China 5.5 Indonesia 2.4 Malaysia 3.8 Philippines 3.2 Singapore 3.9 Thailand 3.7 Vietnam 5.1
Source: 2003 PNHA, NSCB From the paper presented by the Congressional Planning and Budget Department entitled An Analysis of the President’s Budget for Fiscal Year 2006 The DOH admits that budget per person is just P95.96 for an average nationwide allocation with Luzon having the highest per person allocation of P109.87. Table 25. Department of Health Proper Budget Allocation Per Person, Per Region CY 2007
CENTER FOR HEALTH
DEVELOPMENT
POPULATION % POPULATION DISTRIBUTION
DOH BUDGET
ALLOCATION (IN ‘000 PESOS)
% BUDGET SHARE
BUDGET ALLOCATION
PER PERSON
Luzon 48,606,822 57.42 5,340,466 65.75 109.87Visayas 17,690,188 20.90 1157,424 14.25 65.43Mindanao 18,354,805 21.68 1,624,991 20.01 88.53Philippines 84,651,815 100.00 8,122,88 100.00 95.96
Note: Luzon budget allocation includes the 12 MM hospitals Source: 1995 Census Based City/Municipal Population Projections, National Statistics Office
An NGO-Legislators’ Initiative 36
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
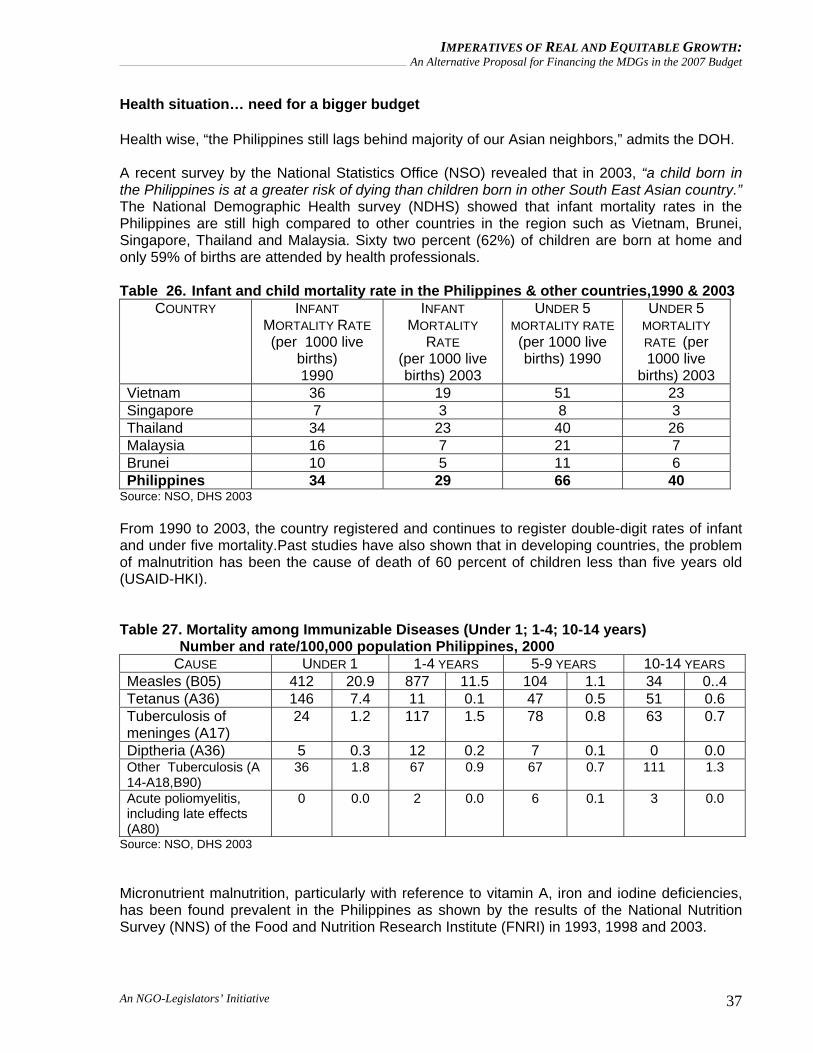
Health situation… need for a bigger budget Health wise, “the Philippines still lags behind majority of our Asian neighbors,” admits the DOH. A recent survey by the National Statistics Office (NSO) revealed that in 2003, “a child born in the Philippines is at a greater risk of dying than children born in other South East Asian country.” The National Demographic Health survey (NDHS) showed that infant mortality rates in the Philippines are still high compared to other countries in the region such as Vietnam, Brunei, Singapore, Thailand and Malaysia. Sixty two percent (62%) of children are born at home and only 59% of births are attended by health professionals. Table 26. Infant and child mortality rate in the Philippines & other countries,1990 & 2003
COUNTRY INFANT MORTALITY RATE (per 1000 live
births) 1990
INFANT MORTALITY
RATE (per 1000 live births) 2003
UNDER 5 MORTALITY RATE (per 1000 live births) 1990
UNDER 5 MORTALITY RATE (per 1000 live
births) 2003 Vietnam 36 19 51 23 Singapore 7 3 8 3 Thailand 34 23 40 26 Malaysia 16 7 21 7 Brunei 10 5 11 6 Philippines 34 29 66 40
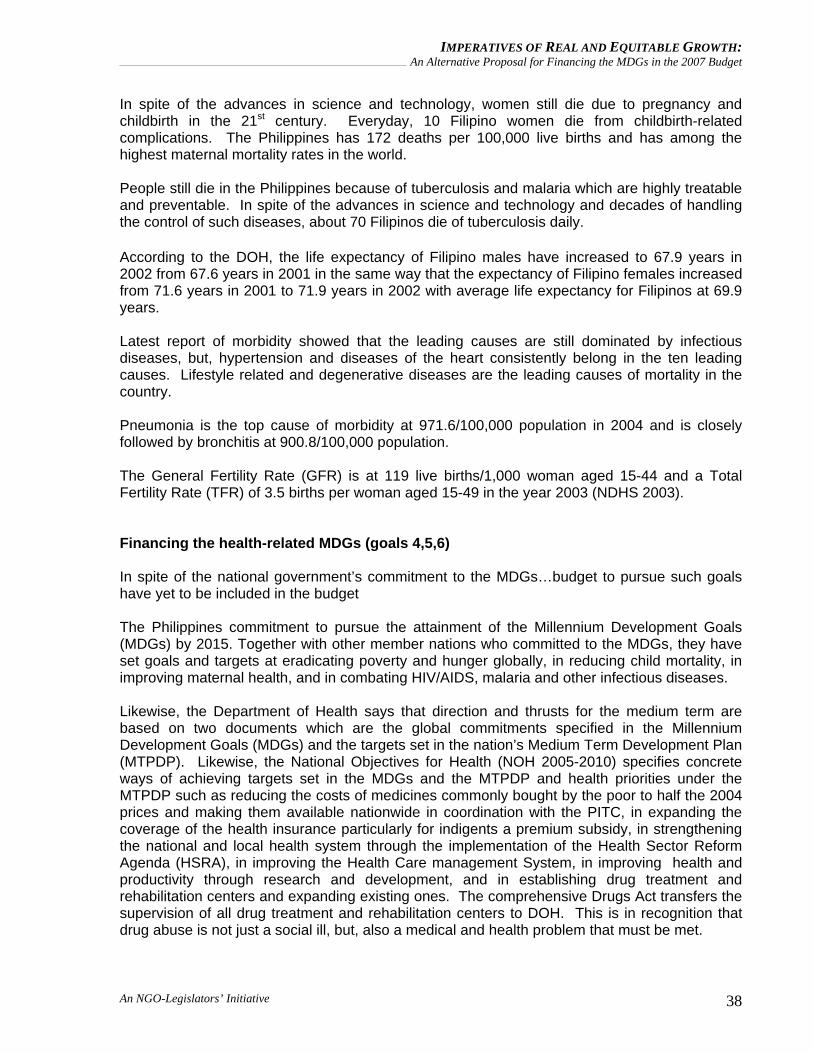
Source: NSO, DHS 2003 From 1990 to 2003, the country registered and continues to register double-digit rates of infant and under five mortality.Past studies have also shown that in developing countries, the problem of malnutrition has been the cause of death of 60 percent of children less than five years old (USAID-HKI). Table 27. Mortality among Immunizable Diseases (Under 1; 1-4; 10-14 years) Number and rate/100,000 population Philippines, 2000
CAUSE UNDER 1 1-4 YEARS 5-9 YEARS 10-14 YEARS Measles (B05) 412 20.9 877 11.5 104 1.1 34 0..4 Tetanus (A36) 146 7.4 11 0.1 47 0.5 51 0.6 Tuberculosis of meninges (A17)
24 1.2 117 1.5 78 0.8 63 0.7
Diptheria (A36) 5 0.3 12 0.2 7 0.1 0 0.0 Other Tuberculosis (A 14-A18,B90)
36 1.8 67 0.9 67 0.7 111 1.3
Acute poliomyelitis, including late effects (A80)
0 0.0 2 0.0 6 0.1 3 0.0
Source: NSO, DHS 2003 Micronutrient malnutrition, particularly with reference to vitamin A, iron and iodine deficiencies, has been found prevalent in the Philippines as shown by the results of the National Nutrition Survey (NNS) of the Food and Nutrition Research Institute (FNRI) in 1993, 1998 and 2003.
An NGO-Legislators’ Initiative 37
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
In spite of the advances in science and technology, women still die due to pregnancy and childbirth in the 21st century. Everyday, 10 Filipino women die from childbirth-related complications. The Philippines has 172 deaths per 100,000 live births and has among the highest maternal mortality rates in the world. People still die in the Philippines because of tuberculosis and malaria which are highly treatable and preventable. In spite of the advances in science and technology and decades of handling the control of such diseases, about 70 Filipinos die of tuberculosis daily. According to the DOH, the life expectancy of Filipino males have increased to 67.9 years in 2002 from 67.6 years in 2001 in the same way that the expectancy of Filipino females increased from 71.6 years in 2001 to 71.9 years in 2002 with average life expectancy for Filipinos at 69.9 years. Latest report of morbidity showed that the leading causes are still dominated by infectious diseases, but, hypertension and diseases of the heart consistently belong in the ten leading causes. Lifestyle related and degenerative diseases are the leading causes of mortality in the country. Pneumonia is the top cause of morbidity at 971.6/100,000 population in 2004 and is closely followed by bronchitis at 900.8/100,000 population. The General Fertility Rate (GFR) is at 119 live births/1,000 woman aged 15-44 and a Total Fertility Rate (TFR) of 3.5 births per woman aged 15-49 in the year 2003 (NDHS 2003). Financing the health-related MDGs (goals 4,5,6) In spite of the national government’s commitment to the MDGs…budget to pursue such goals have yet to be included in the budget The Philippines commitment to pursue the attainment of the Millennium Development Goals (MDGs) by 2015. Together with other member nations who committed to the MDGs, they have set goals and targets at eradicating poverty and hunger globally, in reducing child mortality, in improving maternal health, and in combating HIV/AIDS, malaria and other infectious diseases. Likewise, the Department of Health says that direction and thrusts for the medium term are based on two documents which are the global commitments specified in the Millennium Development Goals (MDGs) and the targets set in the nation’s Medium Term Development Plan (MTPDP). Likewise, the National Objectives for Health (NOH 2005-2010) specifies concrete ways of achieving targets set in the MDGs and the MTPDP and health priorities under the MTPDP such as reducing the costs of medicines commonly bought by the poor to half the 2004 prices and making them available nationwide in coordination with the PITC, in expanding the coverage of the health insurance particularly for indigents a premium subsidy, in strengthening the national and local health system through the implementation of the Health Sector Reform Agenda (HSRA), in improving the Health Care management System, in improving health and productivity through research and development, and in establishing drug treatment and rehabilitation centers and expanding existing ones. The comprehensive Drugs Act transfers the supervision of all drug treatment and rehabilitation centers to DOH. This is in recognition that drug abuse is not just a social ill, but, also a medical and health problem that must be met.
An NGO-Legislators’ Initiative 38
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
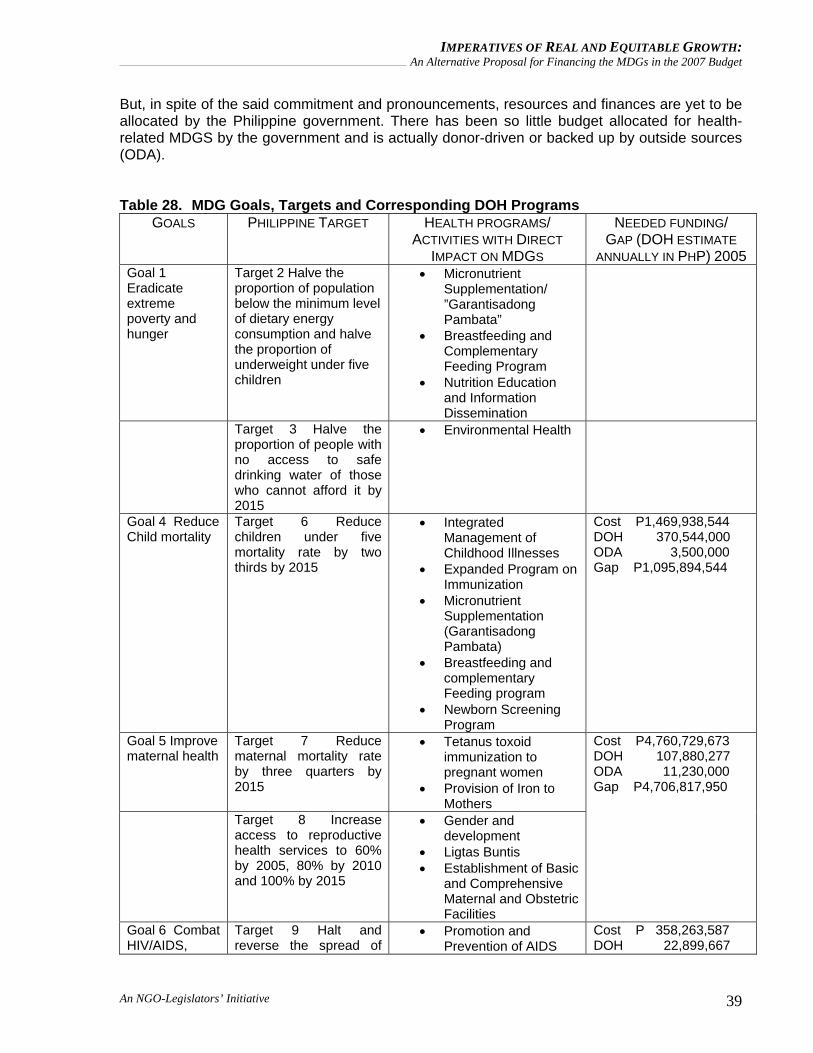
But, in spite of the said commitment and pronouncements, resources and finances are yet to be allocated by the Philippine government. There has been so little budget allocated for health-related MDGS by the government and is actually donor-driven or backed up by outside sources (ODA). Table 28. MDG Goals, Targets and Corresponding DOH Programs
GOALS PHILIPPINE TARGET HEALTH PROGRAMS/ ACTIVITIES WITH DIRECT
IMPACT ON MDGS
NEEDED FUNDING/ GAP (DOH ESTIMATE
ANNUALLY IN PHP) 2005 Goal 1 Eradicate extreme poverty and hunger
Target 2 Halve the proportion of population below the minimum level of dietary energy consumption and halve the proportion of underweight under five children
• Micronutrient Supplementation/ ”Garantisadong Pambata”
• Breastfeeding and Complementary Feeding Program
• Nutrition Education and Information Dissemination
Target 3 Halve the proportion of people with no access to safe drinking water of those who cannot afford it by 2015
• Environmental Health
Goal 4 Reduce Child mortality
Target 6 Reduce children under five mortality rate by two thirds by 2015
• Integrated Management of Childhood Illnesses
• Expanded Program on Immunization
• Micronutrient Supplementation (Garantisadong Pambata)
• Breastfeeding and complementary Feeding program
• Newborn Screening Program
Cost P1,469,938,544 DOH 370,544,000 ODA 3,500,000 Gap P1,095,894,544
Goal 5 Improve maternal health
Target 7 Reduce maternal mortality rate by three quarters by 2015
• Tetanus toxoid immunization to pregnant women
• Provision of Iron to Mothers
Target 8 Increase access to reproductive health services to 60% by 2005, 80% by 2010 and 100% by 2015
• Gender and development
• Ligtas Buntis • Establishment of Basic
and Comprehensive Maternal and Obstetric Facilities
Cost P4,760,729,673 DOH 107,880,277 ODA 11,230,000 Gap P4,706,817,950
Goal 6 Combat HIV/AIDS,
Target 9 Halt and reverse the spread of
• Promotion and Prevention of AIDS
Cost P 358,263,587 DOH 22,899,667
An NGO-Legislators’ Initiative 39
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
malaria and other diseases
HIV/AIDS by 2015 prevention services • Provision of Drugs and
Other Logistic Supplies
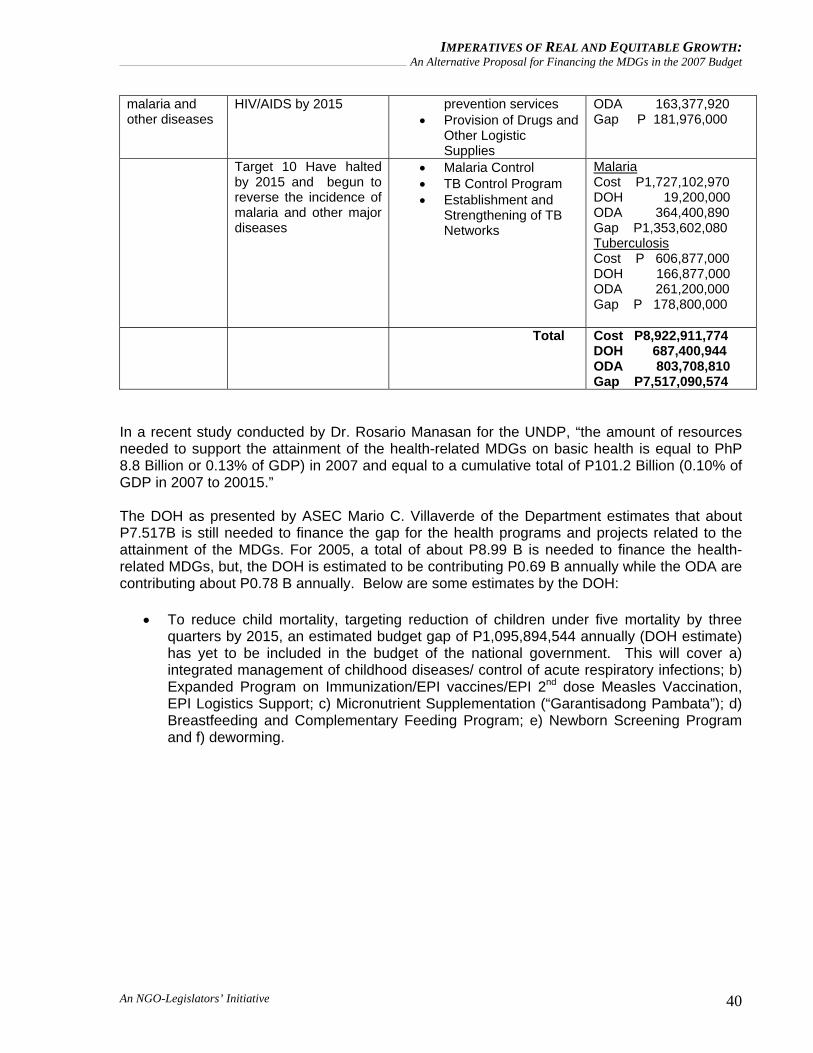
ODA 163,377,920 Gap P 181,976,000
Target 10 Have halted by 2015 and begun to reverse the incidence of malaria and other major diseases
• Malaria Control • TB Control Program • Establishment and
Strengthening of TB Networks
Malaria Cost P1,727,102,970 DOH 19,200,000 ODA 364,400,890 Gap P1,353,602,080 Tuberculosis Cost P 606,877,000 DOH 166,877,000 ODA 261,200,000 Gap P 178,800,000
Total Cost P8,922,911,774 DOH 687,400,944 ODA 803,708,810 Gap P7,517,090,574
In a recent study conducted by Dr. Rosario Manasan for the UNDP, “the amount of resources needed to support the attainment of the health-related MDGs on basic health is equal to PhP 8.8 Billion or 0.13% of GDP) in 2007 and equal to a cumulative total of P101.2 Billion (0.10% of GDP in 2007 to 20015.”
The DOH as presented by ASEC Mario C. Villaverde of the Department estimates that about P7.517B is still needed to finance the gap for the health programs and projects related to the attainment of the MDGs. For 2005, a total of about P8.99 B is needed to finance the health-related MDGs, but, the DOH is estimated to be contributing P0.69 B annually while the ODA are contributing about P0.78 B annually. Below are some estimates by the DOH:
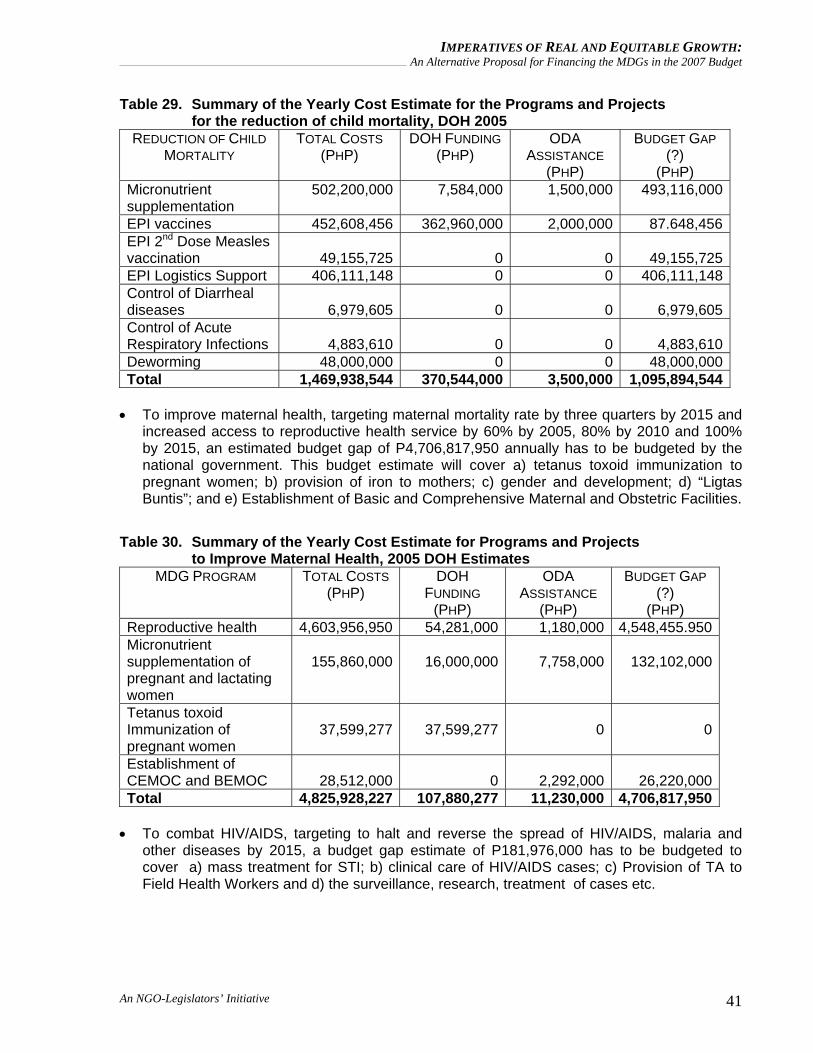
• To reduce child mortality, targeting reduction of children under five mortality by three quarters by 2015, an estimated budget gap of P1,095,894,544 annually (DOH estimate) has yet to be included in the budget of the national government. This will cover a) integrated management of childhood diseases/ control of acute respiratory infections; b) Expanded Program on Immunization/EPI vaccines/EPI 2nd dose Measles Vaccination, EPI Logistics Support; c) Micronutrient Supplementation (“Garantisadong Pambata”); d) Breastfeeding and Complementary Feeding Program; e) Newborn Screening Program and f) deworming.
An NGO-Legislators’ Initiative 40
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
Table 29. Summary of the Yearly Cost Estimate for the Programs and Projects for the reduction of child mortality, DOH 2005
REDUCTION OF CHILD MORTALITY
TOTAL COSTS (PHP)
DOH FUNDING (PHP)
ODA ASSISTANCE
(PHP)
BUDGET GAP (?)
(PHP) Micronutrient supplementation
502,200,000 7,584,000 1,500,000 493,116,000
EPI vaccines 452,608,456 362,960,000 2,000,000 87.648,456EPI 2nd Dose Measles vaccination 49,155,725 0
0 49,155,725
EPI Logistics Support 406,111,148 0 0 406,111,148Control of Diarrheal diseases 6,979,605 0
0 6,979,605
Control of Acute Respiratory Infections 4,883,610 0
0 4,883,610
Deworming 48,000,000 0 0 48,000,000Total 1,469,938,544 370,544,000 3,500,000 1,095,894,544
• To improve maternal health, targeting maternal mortality rate by three quarters by 2015 and
increased access to reproductive health service by 60% by 2005, 80% by 2010 and 100% by 2015, an estimated budget gap of P4,706,817,950 annually has to be budgeted by the national government. This budget estimate will cover a) tetanus toxoid immunization to pregnant women; b) provision of iron to mothers; c) gender and development; d) “Ligtas Buntis”; and e) Establishment of Basic and Comprehensive Maternal and Obstetric Facilities.
Table 30. Summary of the Yearly Cost Estimate for Programs and Projects to Improve Maternal Health, 2005 DOH Estimates
MDG PROGRAM TOTAL COSTS (PHP)
DOH FUNDING
(PHP)
ODA ASSISTANCE
(PHP)
BUDGET GAP (?)
(PHP) Reproductive health 4,603,956,950 54,281,000 1,180,000 4,548,455.950Micronutrient supplementation of pregnant and lactating women
155,860,000 16,000,000
7,758,000 132,102,000
Tetanus toxoid Immunization of pregnant women
37,599,277 37,599,277
0 0
Establishment of CEMOC and BEMOC 28,512,000 0
2,292,000 26,220,000
Total 4,825,928,227 107,880,277 11,230,000 4,706,817,950 • To combat HIV/AIDS, targeting to halt and reverse the spread of HIV/AIDS, malaria and
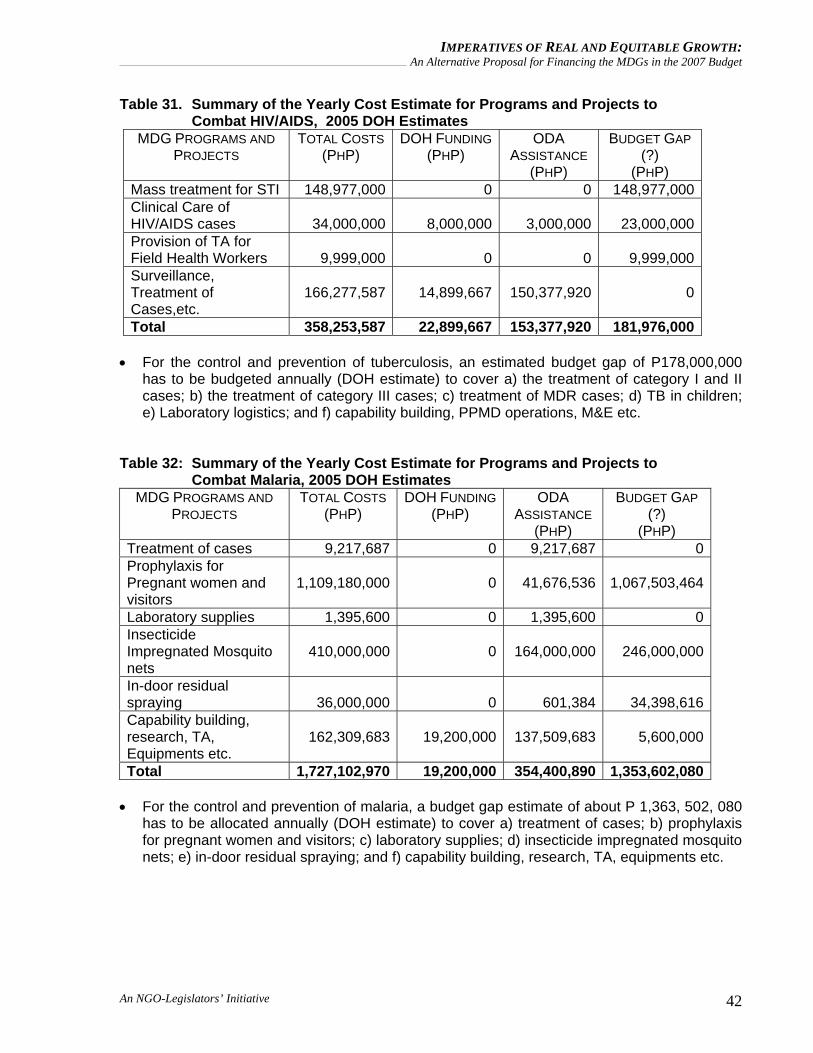
other diseases by 2015, a budget gap estimate of P181,976,000 has to be budgeted to cover a) mass treatment for STI; b) clinical care of HIV/AIDS cases; c) Provision of TA to Field Health Workers and d) the surveillance, research, treatment of cases etc.
An NGO-Legislators’ Initiative 41
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
Table 31. Summary of the Yearly Cost Estimate for Programs and Projects to Combat HIV/AIDS, 2005 DOH Estimates
MDG PROGRAMS AND PROJECTS
TOTAL COSTS (PHP)
DOH FUNDING(PHP)
ODA ASSISTANCE
(PHP)
BUDGET GAP (?)
(PHP) Mass treatment for STI 148,977,000 0 0 148,977,000Clinical Care of HIV/AIDS cases 34,000,000 8,000,000
3,000,000 23,000,000
Provision of TA for Field Health Workers 9,999,000 0
0 9,999,000
Surveillance, Treatment of Cases,etc.
166,277,587 14,899,667
150,377,920 0
Total 358,253,587 22,899,667 153,377,920 181,976,000 • For the control and prevention of tuberculosis, an estimated budget gap of P178,000,000
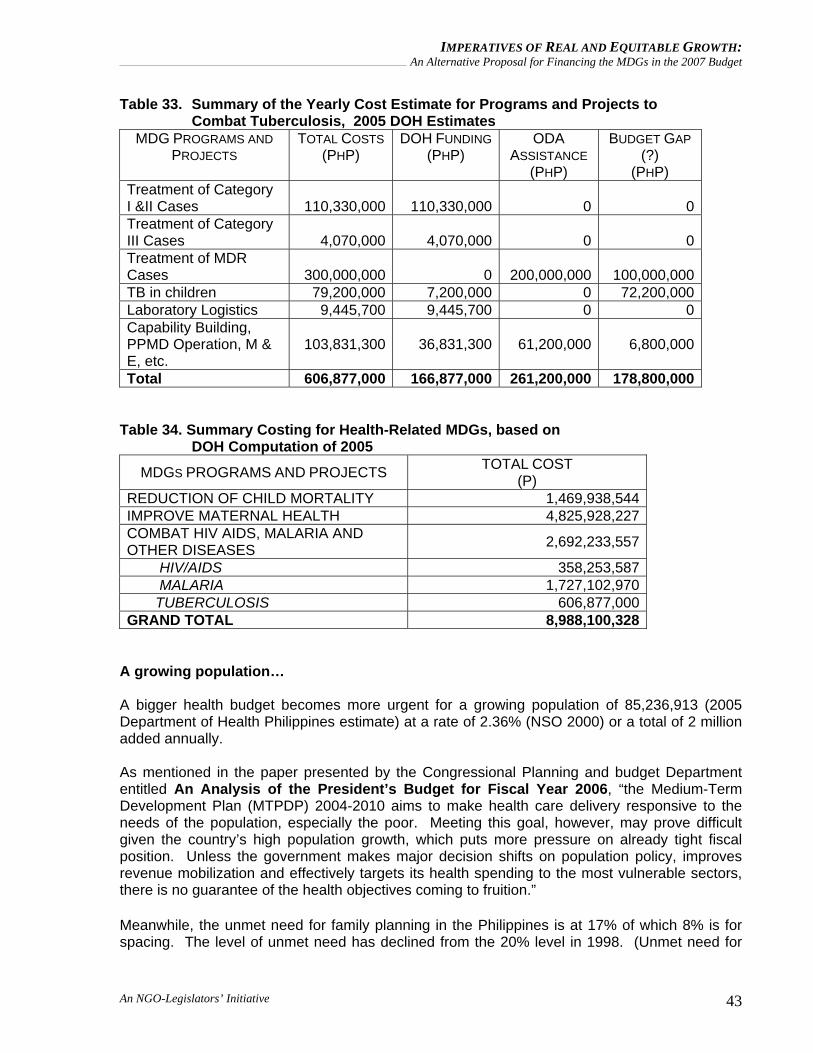
has to be budgeted annually (DOH estimate) to cover a) the treatment of category I and II cases; b) the treatment of category III cases; c) treatment of MDR cases; d) TB in children; e) Laboratory logistics; and f) capability building, PPMD operations, M&E etc.
Table 32: Summary of the Yearly Cost Estimate for Programs and Projects to Combat Malaria, 2005 DOH Estimates
MDG PROGRAMS AND PROJECTS
TOTAL COSTS (PHP)
DOH FUNDING(PHP)
ODA ASSISTANCE
(PHP)
BUDGET GAP (?)
(PHP) Treatment of cases 9,217,687 0 9,217,687 0Prophylaxis for Pregnant women and visitors
1,109,180,000 0
41,676,536 1,067,503,464
Laboratory supplies 1,395,600 0 1,395,600 0Insecticide Impregnated Mosquito nets
410,000,000 0
164,000,000 246,000,000
In-door residual spraying 36,000,000 0
601,384 34,398,616
Capability building, research, TA, Equipments etc.
162,309,683 19,200,000
137,509,683 5,600,000
Total 1,727,102,970 19,200,000 354,400,890 1,353,602,080 • For the control and prevention of malaria, a budget gap estimate of about P 1,363, 502, 080
has to be allocated annually (DOH estimate) to cover a) treatment of cases; b) prophylaxis for pregnant women and visitors; c) laboratory supplies; d) insecticide impregnated mosquito nets; e) in-door residual spraying; and f) capability building, research, TA, equipments etc.
An NGO-Legislators’ Initiative 42
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
Table 33. Summary of the Yearly Cost Estimate for Programs and Projects to Combat Tuberculosis, 2005 DOH Estimates
MDG PROGRAMS AND PROJECTS
TOTAL COSTS (PHP)
DOH FUNDING(PHP)
ODA ASSISTANCE
(PHP)
BUDGET GAP (?)
(PHP) Treatment of Category I &II Cases 110,330,000 110,330,000
0 0
Treatment of Category III Cases 4,070,000 4,070,000
0 0
Treatment of MDR Cases 300,000,000 0
200,000,000 100,000,000
TB in children 79,200,000 7,200,000 0 72,200,000Laboratory Logistics 9,445,700 9,445,700 0 0Capability Building, PPMD Operation, M & E, etc.
103,831,300 36,831,300
61,200,000 6,800,000
Total 606,877,000 166,877,000 261,200,000 178,800,000 Table 34. Summary Costing for Health-Related MDGs, based on DOH Computation of 2005
MDGS PROGRAMS AND PROJECTS TOTAL COST (P)
REDUCTION OF CHILD MORTALITY 1,469,938,544 IMPROVE MATERNAL HEALTH 4,825,928,227 COMBAT HIV AIDS, MALARIA AND OTHER DISEASES 2,692,233,557
HIV/AIDS 358,253,587 MALARIA 1,727,102,970 TUBERCULOSIS 606,877,000 GRAND TOTAL 8,988,100,328
A growing population… A bigger health budget becomes more urgent for a growing population of 85,236,913 (2005 Department of Health Philippines estimate) at a rate of 2.36% (NSO 2000) or a total of 2 million added annually.
As mentioned in the paper presented by the Congressional Planning and budget Department entitled An Analysis of the President’s Budget for Fiscal Year 2006, “the Medium-Term Development Plan (MTPDP) 2004-2010 aims to make health care delivery responsive to the needs of the population, especially the poor. Meeting this goal, however, may prove difficult given the country’s high population growth, which puts more pressure on already tight fiscal position. Unless the government makes major decision shifts on population policy, improves revenue mobilization and effectively targets its health spending to the most vulnerable sectors, there is no guarantee of the health objectives coming to fruition.” Meanwhile, the unmet need for family planning in the Philippines is at 17% of which 8% is for spacing. The level of unmet need has declined from the 20% level in 1998. (Unmet need for
An NGO-Legislators’ Initiative 43
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
family planning is defined as the percentage of currently married women who either do not want any more children or want to wait before having their next birth, but are not using any method of family planning). (Philippines National Demographic and health survey 2003)
From the same survey, more than half of women with at least a high school education are current users of contraception compared with less than one in five women with no formal education. The use of any method of family planning also increases with wealth status. However, over two–thirds of current users of modern methods obtain their contraceptive supplies from a public source (67 %), 29% from a private medical source and 3% from other sources. Compared with data from the 1998 NDHS, there has been a decrease in reliance to the public sector (from 72% and an increase in use from the private sector (from 26 %). Without the necessary intervention on the part of government to ensure the availability of modern contraceptives, where will the men and women get their family planning commodities and services? The Botika ng Barangays do not include in their list essential family planning commodities to be sold at affordable prices in their respective barangay. Other priority health concerns
The aggressive promotion of primary health care and breastfeeding has to be supported with resources and finances to improve mother and infant nutrition. Breastfeeding with all its healthful and economic advantages is the best form of feeding during the first six months of infancy. Although most Filipino babies (about 88%) are breastfed for some time, NDHS data indicate that supplementation with other liquids and foods occur too early. The first breast milk or colostrum, is particularly beneficial to newborn because it contains high concentration of antibodies that protect children against certain infectious diseases. In the Philippines today, among newborns, less than two months of age, one in seven is not breastfed, and 19 percent are receiving supplementary foods in addition to breast milk. The Botika ng Barangay when made use of and managed properly will address the poor’s access to safe, affordable and quality medicines that they need especially in far-flung communities. However, it has been noted that the corresponding support and backing up of Local Government Units is yet to be generated. We have to convince LGUs that it is both beneficial in terms of addressing their constituencies’ need for these safe and affordable medicines and as a sustainability measure at the same time. Moreover, herbal medicines and reproductive health commodities need to be included in the Botika ng Barangay. Some practices like storing medicines at the homes of the Barangay Chairperson have to be discarded right away and a clear plan has to be designed in the management and implementation of such health-related undertaking. Likewise, the LGUs which are expected to finance and deliver basic social services are performing below expectations. For fiscal year 2006, the LGUs were required to include in their budgets the implementation of basic social services responsive to the MDGs, which include nutrition services, maternal and child health services (DBM Policy, per LBM No. 47 (July 2005) (source: Paper on “The Gnawing Realities of poverty and State Negligence in the Lives of Children, Will We See an End?” by G,H.S. Ambat). For LGUs like Makati City, it is easy to
An NGO-Legislators’ Initiative 44
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
provide for the programs and projects for the attainment of the health-related MDGs. At the rate Makati is investing in health, especially in child and maternal health services, it is most likely that it will achieve and perhaps do better than just achieving the national target. However, for 4th class LGUs like Malinao in Aklan with a population of 23,000 in 2004 and dependent on the National Government for financing, it is a different story altogether. As admitted by the Secretary of Health last September 13, 2006 at the House of Representatives presentation of the Department of Health’s Accomplishments and the Proposed Budget for CY 2007, even syringes could not be supplied by some LGUs for the immunization program in some localities such that the proposed budget for 2007 had to include syringes to ensure its implementation. Meaning the national government can really provide such accommodations if they want to and really need to. The continuing exodus of trained, skilled and experienced health professionals ha had negative impact in the delivery of health services at the community level and in the retention of health service providers in hospitals and health units. A long term and short term solution to such exodus has to be addressed right away to save an already ailing health care system in the Philippines. Working abroad has to be career choice instead of a necessity. We have to accelerate training of health professionals like providing for scholarships to indigent but qualified students, but, have to work or render services in the Philippine Health Care Delivery System equivalent to the number of years of which they have trained. We also need to look into negotiating with recipient countries in terms of a per capita “training pay-back scheme” to support the program for acceleration and retention of health professionals in the Philippines. We also need to improve the working conditions and benefits of our health professionals and encourage LGUs to devise mechanisms on how to improve the benefits of their community health workers. Below are some hard realities:
o The Philippines is now the number one (1) exporter of nurses. “An estimated 85% of employed Filipino nurses (more than 150,000) are working internationally. (Alken et al 2000) About 70% of all Filipino nursing graduates are working overseas. “(Bach 2003)
o The Philippines also ranks number two (2) as exporter of doctors. About 68% of Filipino doctors work overseas, next to India.” (Mejia, WHO, 1979).
o Offers abroad are simply irresistible considering the a)higher compensation and benefit packages (US$180 a month vs. US$4,000 a month USA); b) more job opportunities abroad (more than 200,000 nursing positions available yearly in about 32 countries); c) more economic, social and political stability; d) better living conditions abroad; e) better career growth abroad; and f) better working conditions.
o Some of the reasons why they leave are a) low compensation and benefits; b) family obligations and security; c) political instability; d) poor working conditions; and e) graft and corruption
o The top five (5) countries of destinations are the United States of America (USA), the United Kingdom (UK), Saudi Arabia, Ireland and Singapore.
o Mushrooming of nursing schools because of the demand abroad. In a matter of ten months, an additional 109 schools were established in the country- from 251 in June 2003 to 370 in April 2004. There were only 40 nursing schools in the ‘70’s and about 170 in the ‘90’s.
o As a consequence of the rapid proliferation of nursing schools is the deteriorating performance in the National Nurse Licensure Examinations. The average
An NGO-Legislators’ Initiative 45
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
proportion of nursing graduates passing the Philippine Nurse licensure examinations in the 70’s to 80’s was 80-90%. With 1994 as a reference year, passing rate was 61.45% and succeeding years have all been below, even reaching a low of 45%. Current rate is at 49.4% and not even reaching 50%.
o The total number of licensed nurses have decreased to an average of 4,500 (1999-2002) compared to more than 15,000 in the early 1990s. It is now again increasing as not only original nursing graduates are taking, but also, second courses majority of whom are “nursing medics”
o Doctors are now shifting to nursing in order to work abroad. WHY? There is too much political instability, very poor working conditions, there is the threat of malpractice law, low salaries and benefits and the continuing peace and order problem.
o A decreasing enrollment of first year medical students (for the past two years ranging from 18% to 74% with an average of 30%), a decreasing number in applicants for the residency positions in training hospitals, the closing down of three (3) medical schools and a decreasing performance in the physician licensure exam.
o Three (3) hospitals in Mindanao and two (2) hospitals in Isabela have no more doctors and nurses; b) disparities and inequities are heightened; c) a decrease in health services coverage; d) hospitals across the country lament the loss of senior nurses and less ideal nurse:patient ratios and an increasing vacancies of MDs and RNs.
Source: The Brain Drain Phenomenon and Its Implications to Health by Jaime Galvez Tan, MD,MPH as presented in the 3rd Alfred J. Ganapin Advocacy Forum Series in September 30, 2005.
Research, production and distribution of herbal medicines should be accelerated and financially supported. The National Health Insurance of the Philippines or NHIP should be strengthened and supported to accommodate more indigents among its beneficiaries and should not allow itself to be used by government officials for their own benefits and selfish motives or for election purposes. A system has to be drafted in identifying who the real indigents are in each and every barangay in the Philippines and in the distribution of such PhilHealth cards. It has been noted that the number of indigent beneficiaries suddenly increase during election years. Our proposal for the year 2007 budget is to retain its P750 million premium subsidy to avoid its being manipulated for the elections, because 2007 is an election year.
Alternative Health Budget
The health budget for CY 2007 needs to be increased by P8.503 Billion, but, the allocation for premium subsidy for NHIP has to be slashed by P2.75 billion and maintained at its 2006 level which is at P750Million, until a thorough report is submitted on the evaluation/assessment of --
1. Previous distribution scheme and how program beneficiaries were identified, 2. Profiles of program beneficiaries and the Impact of the program on intended beneficiaries 3. The monitoring plan in place
Below are some budget items where additional budget is highly recommended:
An NGO-Legislators’ Initiative 46
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
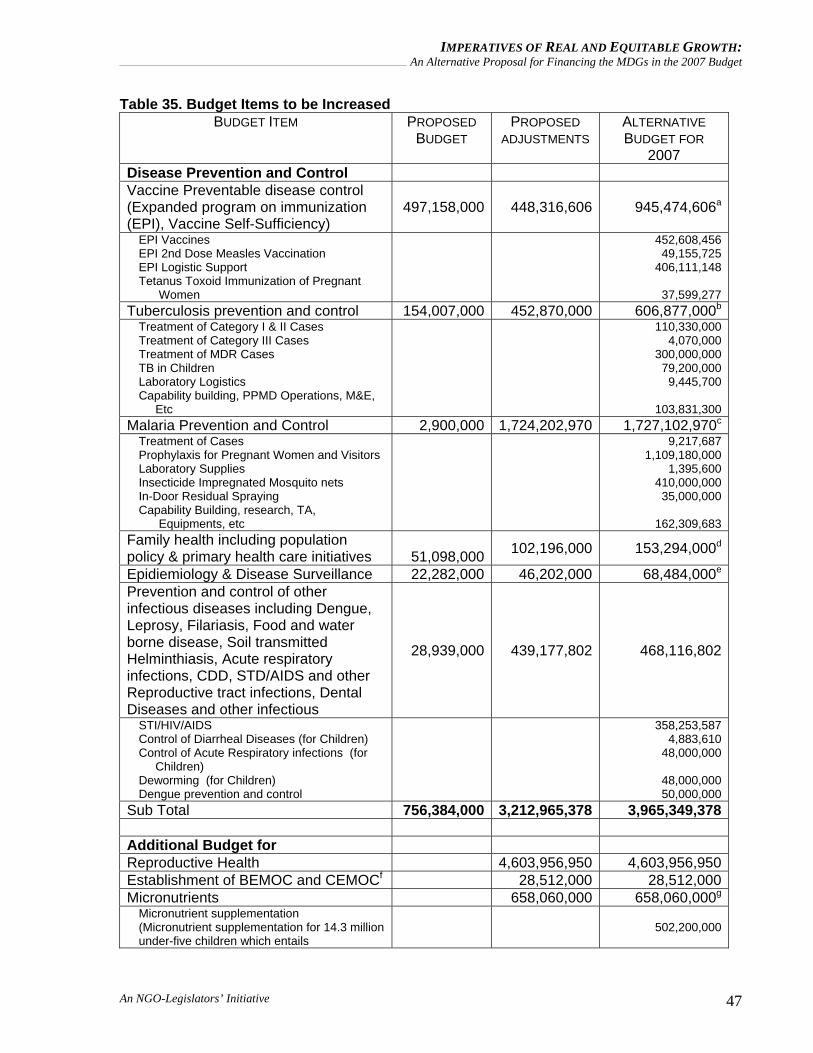
Table 35. Budget Items to be Increased BUDGET ITEM PROPOSED
BUDGET PROPOSED
ADJUSTMENTS
ALTERNATIVE BUDGET FOR
2007 Disease Prevention and Control Vaccine Preventable disease control (Expanded program on immunization (EPI), Vaccine Self-Sufficiency)
497,158,000 448,316,606 945,474,606a
EPI Vaccines EPI 2nd Dose Measles Vaccination EPI Logistic Support Tetanus Toxoid Immunization of Pregnant Women
452,608,456 49,155,725
406,111,148
37,599,277 Tuberculosis prevention and control 154,007,000 452,870,000 606,877,000b
Treatment of Category I & II Cases Treatment of Category III Cases Treatment of MDR Cases TB in Children Laboratory Logistics Capability building, PPMD Operations, M&E, Etc
110,330,000 4,070,000
300,000,000 79,200,000
9,445,700
103,831,300 Malaria Prevention and Control 2,900,000 1,724,202,970 1,727,102,970c
Treatment of Cases Prophylaxis for Pregnant Women and Visitors Laboratory Supplies Insecticide Impregnated Mosquito nets In-Door Residual Spraying Capability Building, research, TA, Equipments, etc
9,217,687 1,109,180,000
1,395,600 410,000,000 35,000,000
162,309,683
Family health including population policy & primary health care initiatives
51,098,000 102,196,000 153,294,000d
Epidiemiology & Disease Surveillance 22,282,000 46,202,000 68,484,000e
Prevention and control of other infectious diseases including Dengue, Leprosy, Filariasis, Food and water borne disease, Soil transmitted Helminthiasis, Acute respiratory infections, CDD, STD/AIDS and other Reproductive tract infections, Dental Diseases and other infectious
28,939,000 439,177,802 468,116,802
STI/HIV/AIDS Control of Diarrheal Diseases (for Children) Control of Acute Respiratory infections (for Children) Deworming (for Children) Dengue prevention and control
358,253,587 4,883,610
48,000,000
48,000,000 50,000,000
Sub Total 756,384,000 3,212,965,378 3,965,349,378 Additional Budget for Reproductive Health 4,603,956,950 4,603,956,950Establishment of BEMOC and CEMOCf 28,512,000 28,512,000Micronutrients 658,060,000 658,060,000g
Micronutrient supplementation (Micronutrient supplementation for 14.3 million under-five children which entails
502,200,000
An NGO-Legislators’ Initiative 47
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
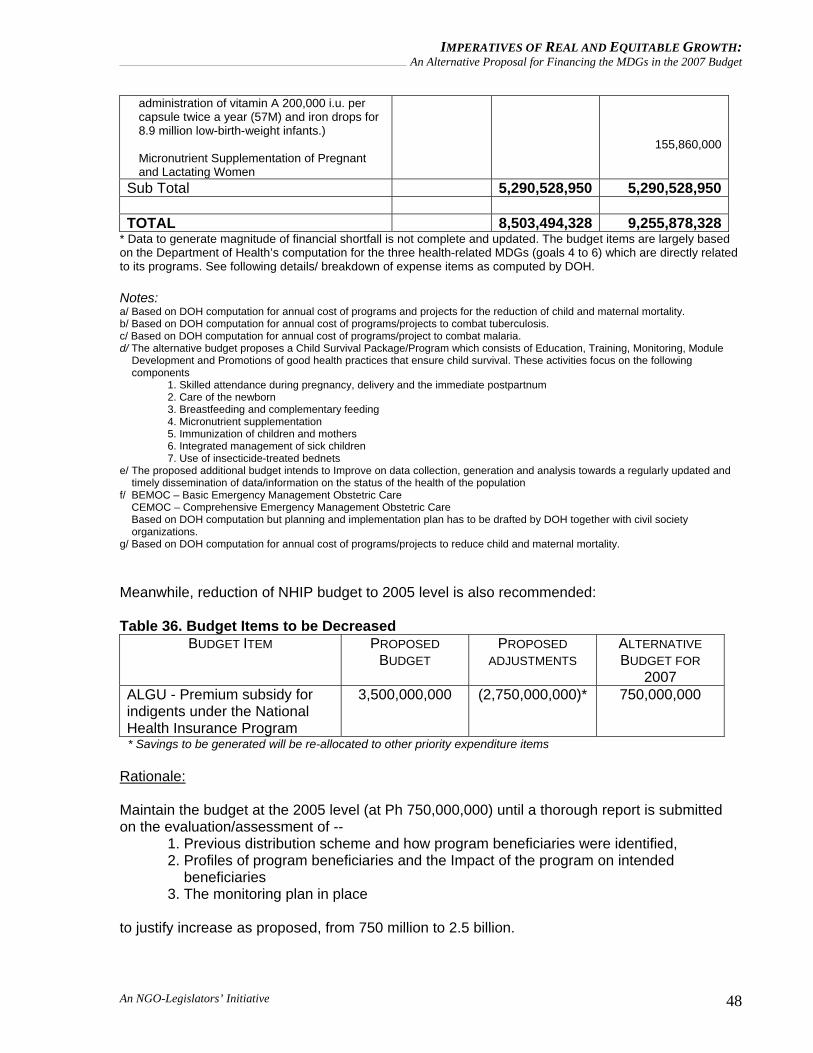
administration of vitamin A 200,000 i.u. per capsule twice a year (57M) and iron drops for 8.9 million low-birth-weight infants.) Micronutrient Supplementation of Pregnant and Lactating Women
155,860,000
Sub Total 5,290,528,950 5,290,528,950 TOTAL 8,503,494,328 9,255,878,328
* Data to generate magnitude of financial shortfall is not complete and updated. The budget items are largely based on the Department of Health’s computation for the three health-related MDGs (goals 4 to 6) which are directly related to its programs. See following details/ breakdown of expense items as computed by DOH. Notes: a/ Based on DOH computation for annual cost of programs and projects for the reduction of child and maternal mortality. b/ Based on DOH computation for annual cost of programs/projects to combat tuberculosis. c/ Based on DOH computation for annual cost of programs/project to combat malaria. d/ The alternative budget proposes a Child Survival Package/Program which consists of Education, Training, Monitoring, Module
Development and Promotions of good health practices that ensure child survival. These activities focus on the following components 1. Skilled attendance during pregnancy, delivery and the immediate postpartnum 2. Care of the newborn 3. Breastfeeding and complementary feeding 4. Micronutrient supplementation 5. Immunization of children and mothers 6. Integrated management of sick children 7. Use of insecticide-treated bednets
e/ The proposed additional budget intends to Improve on data collection, generation and analysis towards a regularly updated and timely dissemination of data/information on the status of the health of the population
f/ BEMOC – Basic Emergency Management Obstetric Care CEMOC – Comprehensive Emergency Management Obstetric Care Based on DOH computation but planning and implementation plan has to be drafted by DOH together with civil society
organizations. g/ Based on DOH computation for annual cost of programs/projects to reduce child and maternal mortality. Meanwhile, reduction of NHIP budget to 2005 level is also recommended: Table 36. Budget Items to be Decreased
BUDGET ITEM PROPOSED BUDGET
PROPOSED ADJUSTMENTS
ALTERNATIVE BUDGET FOR
2007 ALGU - Premium subsidy for indigents under the National Health Insurance Program
3,500,000,000
(2,750,000,000)*
750,000,000
* Savings to be generated will be re-allocated to other priority expenditure items Rationale: Maintain the budget at the 2005 level (at Ph 750,000,000) until a thorough report is submitted on the evaluation/assessment of --
1. Previous distribution scheme and how program beneficiaries were identified, 2. Profiles of program beneficiaries and the Impact of the program on intended beneficiaries 3. The monitoring plan in place
to justify increase as proposed, from 750 million to 2.5 billion.
An NGO-Legislators’ Initiative 48
IMPERATIVES OF REAL AND EQUITABLE GROWTH: An Alternative Proposal for Financing the MDGs in the 2007 Budget
The proposed alternative budget intends to address the following targets -- Reduction of child mortality and Improve maternal health • Fully immunized child coverage will increase from 84.5% in 2005 to 100% in 2015 • Coverage of tetanus toxoid vaccination will increase from 80% in 2005 to 100% in 2015 • Hepatitis B coverage will increase 45.6% in 2005 to 100% in 2015 • Proportion of children aged 0-5 years of age who are given Vitamin A will increase from 79%
in 2004 to 100% in 2015 • All under five children will be given micro-nutrient supplementation Combat HIV AIDS, Malaria and other Diseases • To reduce TB morbidity rate from 290 in 2006 per 100,000 population to 250 in 2010 and
190 in 2015; Includes treatment of TB cases among children • To reduce Malaria morbidity rate from 269 per 100,000 population in 2006 to 138 in 2010
and 1 in 2015 • To reduce STI prevalence rate from 5% of the general population in 2006 to 1% in 2010 and
0.5% in 2015
References: Congressional Planning and Budget Department (CPBD). “Analysis of the President's Budget for Fiscal Year 2006." January 2006.
Department of Health CY 2007 Proposed Budget, September 2006 Department of Health Proposed Budget for CY 2007, Presentation by Secretary of Health Francisco T. Duque III, MD, MSc, Committee Hearing , September 2006 Department of Health, Program of Work Fiscal Year 2007, distributed during Committee Hearing September 2006 Financing Health Related MDGs, Mario C. Villaverde, M.D., MPH, CESO III, Assistant Secretary of Health, Presentation during the May pera pa ba? forum, UP NCPAG, September 2005
Manasan, Rosario G. Financing the Millennium Development Goals: The Philippines (Paper presented during the validation meeting, Balay Kalinaw, UP Diliman Campus, Sept 26, 2006).
May pera pa ba? Moving Forward with the Millennium Development Goals, Social Watch Philippines, UNDP and UP NCPAG, June 2006 Philippine National Demographic Survey 2003 The Brain Drain Phenomenon and its Implications to Health, Jaime Z. Galvez Tan, M.D., MPH, (Paper presented at the Third Alfred J. Ganapin Advocacy Forum Series, September 30, 2005) The Philippine Phenomenon of Nursing Medics: Why Filipino Doctors are becoming nurses? A Primer, Medical Action Group, 2005 The President’s Budget Message FY 2007, “Budget: Strong Regions for a Strong Republic”, August 2006 WHO / UNICEF Regional Child Survival Strategy: Accelerated and Sustained Action Towards MDG 4, WHO – Western Pacific Region and UNICEF, 2006
An NGO-Legislators’ Initiative 49