Embed Size (px)
Citation preview

Alternative scenarios for health, life expectancy and social expenditure - AGIR WP4
Dr. Erika Schulz

Erika Schulz14.02.2003
Aims of WP4
– WP4 focuses on the implications of „living longer and in better health“ on health consumption, health and pension expenditure and sustainability of public finance.
– WP4 uses the data of WP1, WP2 and WP3 to make projections.
– The sensitivity of demographic projections for health consumption and expenditure as well as retirement benefits will be demonstrated using a scenario approach with alternative assumptions concerning life expectancy and health.

Erika Schulz14.02.2003
Two parts of WP4
– WP4 can be separated into two parts: Part A focuses on the impact of alternative assumptions of life expectancy on the demographic develop-ment and the use of health and long-term care services.
– Part B focuses on the development of health expenditure and public finances under alternativ scenarios.
– Both parts uses different models and methods and will be therefore presented separatly.

Erika Schulz14.02.2003
Life expectancy, morbidity and health expenditure
Population Health size, age-structure Use of insurance
Life health Health Prices, schemesexpectancy Morbidity/ care expenditure costs
Acut services Supply/health status access
Medical/ Socio-economic General frameworktechnological determinants/ conditionsprogress healthy behavior/ (policies, rules,
genetic conditions assets, economy)

Erika Schulz14.02.2003
WP4 Part A deals with following questions:
What impact have further improvements of life expectancy on the demographic development?
What impact has an increasing life expectancy on health care utilisation?
What impact has the ”near to death” on health care utilisation?
What impact has an increasing life expectancy on long-term care recipients in institutions and at home?
What impact have the increasing female labour force participation on the further potential of long-term care giving at home?

Erika Schulz14.02.2003
Tasks of WP 4 Part A– Building scenarios about further improvements in
life expectancy and computing the demographic development until 2050.
– Building scenarios about improvements in health and the impact on the use of health and long-term care services.
– Forecast the number of inpatients and people with LTC for selected EU countries.
– If data available forecasts of utilisation will be done consider the „near to death“.
– Estimation of the potential of informal care givers of long-term care at home.

Erika Schulz14.02.2003
Demographic scenarios– Most studies for EU countries uses the
EUROSTAT baseline scenario.– In this scenario an increase of the average
EU fertility rate from 1.5 (2000) to 1.7 in 2050 is projected.
– The average life expectancy at birth for men is projected to rise five years from 75 in 2000 to 80 by 2050; for women, it is also projected to rise from 81 years in 2000 to 85 by 2050.
– The migration will be nearly constant (660 to 630 million).

Erika Schulz14.02.2003
Demographic development in the EU
87 77 69
208 202169
80 107125
0
50
100
150
200
250
300
350
400
1998 2020 2050Year
in M
ill.
0 - 20 20 - 60 60 +
Source: Eurostat baseline scenario

Erika Schulz14.02.2003
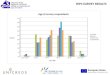
Changes in the number of persons aged 60+ between 1998 and 2050 in %
39
46
47
50
52
54
56
58
59
60
64
69
70
87
96
153
0 20 40 60 80 100 120 140 160
Ireland
Luxembourg
Netherlands
Austria
France
Portugal
Spain
United Kingdom
Finland
EU
Greece
Denmark
Sweden
Belgium
Germany
Italy
Source: Eurostat baseline scenario

Erika Schulz14.02.2003
Advantage and disadvantage of EUROSTAT – The advantage of using the baseline scenario is,
that this forecast is widely spread and that the assumptions are harmonised.
– The disadvantage is that • the assumptions seems to be not realistic for several EU
countries and were criticised at our Madrid meeting• the results are not separated by survivors and decedents• no scenario without further improvements in life
expectancy, but the same assumptions for the other variables as the baseline scenario exists.
– Mostly the further increase of life expectancy is underestimated.

Erika Schulz14.02.2003
Assumptions of the EU baseline scenarioBE DK DE GR ES FR IE IT LU NL AT PT FI SE UK
Total fertility rates1999 1,52 1,78 1,38 1,32 1,17 1,72 1,90 1,19 1,72 1,69 1,29 1,52 1,73 1,48 1,722000 1,54 1,77 1,40 1,34 1,19 1,73 1,89 1,22 1,72 1,71 1,31 1,53 1,73 1,50 1,722020 1,74 1,79 1,50 1,52 1,42 1,80 1,82 1,43 1,79 1,79 1,45 1,69 1,70 1,70 1,792050 1,80 1,80 1,50 1,60 1,50 1,80 1,80 1,50 1,80 1,80 1,50 1,70 1,70 1,80 1,80
Life expectancy of men1999 74,6 74,0 74,6 75,7 74,9 74,7 73,8 75,5 74,1 75,3 74,9 71,9 73,7 77,1 75,02000 74,8 74,2 74,7 75,9 74,9 74,8 74,0 75,5 74,4 75,5 75,0 72,0 73,9 77,3 75,22020 78,7 77,4 78,1 79,1 77,0 78,3 77,2 79,0 78,8 78,2 77,3 75,4 77,4 79,1 78,32050 80,0 79,0 80,0 81,0 79,0 80,0 79,0 81,0 80,0 80,0 81,0 78,0 80,0 82,0 80,0
Life expectancy of women1999 80,7 78,9 80,7 80,8 82,1 82,7 79,2 81,9 80,7 80,7 81,1 79,1 81,0 82,0 79,92000 80,9 79,0 80,8 81,0 82,1 82,8 79,4 82,0 80,8 80,9 81,2 79,2 81,1 82,0 80,02020 84,0 81,1 83,5 83,5 84,2 85,4 82,3 84,5 83,7 83,1 83,0 82,0 83,6 83,5 83,12050 85,0 83,0 85,0 85,0 85,0 87,0 84,0 86,0 85,0 85,0 86,0 84,0 85,0 86,0 85,0
Net-migration1999 10978 10876 192000 22483 30257 50230 18971 50000 3485 32594 9000 11000 5499 14881 1750002000 10204 11000 300000 21670 31054 50094 17477 50000 3072 33390 10000 12131 5604 15165 900002020 15000 10000 200000 25000 60000 50000 5000 80000 2000 35000 20000 25000 5000 20000 700002050 15000 10000 200000 25000 60000 50000 5000 80000 2000 35000 20000 25000 5000 20000 70000

Erika Schulz14.02.2003
Development of life expectancy
1960 1980 1999
EU 15 67,4 70,5 74,9min. (Portugal) 61,2 67,7 72,0max. (Sweden) 71,2 72,8 77,1
EU 15 72,9 77,2 81,2min. (Portugal) 66,8 75,2 79,1max. (Spain) 72,2 78,6 82,5
Source: EUROSTAT, 2001.
Men
Women
Life Expectancy at Birth

Erika Schulz14.02.2003
... for the Elderly
1960 1980 1998
EU 15 15,9 16,8 19,4min. (Ireland) 15,8 15,9 17,9max. (Greece) 16,9 18,2 20,2
EU 15 19,0 21,2 23,8min. (Ireland) 18,1 19,5 21,8max. (France) 19,5 22,4 25,2
Source: EUROSTAT, 2001.
Men
Women
Life Expectancy at Age 60

Erika Schulz14.02.2003
Life expectancy and health status
– Life expectancy is only a rough indicator for the global health status of a population.
– For the analysis of the impact of an increasing life expectancy on the use of health care services it will be better to distinguish between the number of years lived in full health and the number of years lived in bad health or the share of people with/without disability in each age-group.

Erika Schulz14.02.2003
WHO - Healthy life expectancy
Austria 7,0 8,8 9,3 10,7Belgium 7,1 9,4 9,5 11,6Denmark 5,5 8,7 7,3 10,9Finland 6,8 8,8 9,1 10,8France 6,6 9,5 8,7 11,4Germany 6,8 8,9 9,1 10,9Greece 6,5 8,9 8,6 11,0Ireland 6,1 8,9 8,3 11,2Italy 7,0 9,3 9,2 11,3Luxembourg 6,4 9,0 8,5 11,1Netherlandsb 7,1 9,6 9,4 11,9Portugal 8,5 10,7 11,7 13,4Spain 6,6 9,6 8,8 11,6Sweden 7,2 9,1 9,2 11,1United Kingdomb 6,6 9,0 8,8 11,3
USA 8,0 10,7 10,8 13,5
Expectation of lost healthy years at birth
in 2001 (years)
Percentage of total life expectancy lost in
2001
Member State Males FemalesMales Females

Erika Schulz14.02.2003
Scenarios of improvements in health
– Scenario with constant prevalence rates– Scenario with overall improvements in
health - decreasing share of sick or disabled people within all age-groups
– Scenario which uses the past trends or another scenario (to be discussed)

Erika Schulz14.02.2003
Three hypotheses
g e n era l re d uc tion o fm o rb id ity
"C o m pre ss ion -h yp o th e s is"ch a ng e s in sp e ctru m o f d isea ses
sh ift o f m orb id ityto h ig he r ag es
"D yn a m ic eq u ilib riu m "co n sta n t sp ec tru m o f d isea ses
in c re a sin g m o rb id ity"E xpa n s ion -h yp o the s is"
in c rea s ingd e ge n era tive a nd ch ro n ic d isea ses
In c rea s inglife exp e cta n cy
is con n ec tedw ith
Medical and technological progress
Socio-demographic and economic factors
Framework conditions: economic development, policies, assets

Erika Schulz14.02.2003
Changes in Healthy Life Expectancy (HLE) and Life Expectancy with Disability (LED)
69
73,6
72
75,2
6
6,4
8
4,8
62 64 66 68 70 72 74 76 78 80 82
2000
2050
2050
2050
Year
Age
HLE LED
Compression of Morbidity
Expansion of Morbidity
Dynamic Equilibrium
Men

Erika Schulz14.02.2003
Life expectancy and hospital utilisation in Germany
Changes to the year before in %Men
-15
-10
-5
0
5
10
15
1995 1996 1997 1998 1999
years
in %
hospital discharges per 1000 inhabitants
length of hospital stay
hospital days per 1000 inhabitants
life expectancy

Erika Schulz14.02.2003
Life expectancy and hospital utilisation in the Netherlands
Changes to the Year before in %Men
-5
-4
-3
-2
-1
0
1
2
1994 1995 1996 1997 1998 1999 2000
years
in %
life expectancy
hospitals discharges per 1000 inhabitants
length of hospital stay

Erika Schulz14.02.2003
Life expectancy and hospital utilisation in Belgium
Changes to the Year before in %Men
-20
-15
-10
-5
0
5
1992 1993 1995 1996 1997 1998
years
in %
life expectancy
length of hospital stay
hospital discharges per 1000 inhabitants

Erika Schulz14.02.2003
Use of health care services
Age Near to deathHealthy behavior Healthy behaviorGenetic conditions Genetic conditionsLiving conditions Living conditions
Health status
Use of health care services

Erika Schulz14.02.2003
Hospital days per capita - GermanyHospital days per capita
0
5
10
15
20
25
30
35
40
45
0-24 25-34 35-44 45-54 55-64 65-74 75+
age-groups
da
ys
sp
en
t in
a h
osp
ita
l
survivors
decedents in their last year of life
decedents in their second year before death
decedents in their third year before death average

Erika Schulz14.02.2003
Results for Germany - four scenarios
hospitalutilisation constant increasing
by age-groupand diagnosisby age-groupand near to death
Life expectancy
IA IIA
IB IIB

Erika Schulz14.02.2003
Development of days spent in a hospital in Germany (in Mill.) - constant LE
Age-groups 1998 2020 2050 1998 2020 2050
0-34 34,5 27,0 20,1 34,5 27,1 20,335-64 64,3 69,4 51,7 64,3 68,7 51,065-74 33,1 40,7 40,2 33,1 40,5 40,275+ 39,9 58,9 71,1 39,9 58,9 72,6total *) 171,9 195,9 183,2 171,9 195,2 184,1
*) Without "unknown age".1) Projection method A: Projection by age-groups, gender and diagnosis (ICD9).- 2) Projectionmethod B: Projection by age-groups, decomposed by survivors and decedents in their last, secondand third year before death.
Projection method A1) Projection method B2)

Erika Schulz14.02.2003
Development of days spent in a hospital in Germany (in Mill.) - increasing LE
Age-groups 1998 2020 2050 1998 2020 2050
0-34 35 27 20 35 27 2035-64 64 70 53 64 67 4965-74 33 43 45 33 39 3975+ 40 70 113 40 65 104total 172 210 231 172 198 212
1) Projection method A: Projection by age-groups, gender and diagnosis (ICD9).- 2) Projectionmethod B: Projection by age-groups, decomposed by survivors and decedents in their last, secondand third year before death.
Projection method A1) Projection method B2)

Erika Schulz14.02.2003
Development of days spent in a hospital in Germany (changes in %) - constant LE
Age-groups2020/98 2050/20 2050/98 2020/98 2050/20 2050/98
0-34 -21,95 -25,39 -41,76 -21,57 -25,16 -41,3035-64 7,82 -25,44 -19,62 6,71 -25,74 -20,7665-74 22,83 -1,20 21,36 22,35 -0,96 21,1775+ 47,58 20,80 78,28 47,58 23,34 82,03total 13,96 -6,50 6,55 13,53 -5,70 7,05
*) Without "unknown age".1) Projection method A: Projection by age-groups, gender and diagnosis (ICD9).- 2) Projectionmethod B: Projection by age-groups, decomposed by survivors and decedents in their last, secondand third year before death.
Projection method A1) Projection method B2)

Erika Schulz14.02.2003
Development of days spent in a hospital in Germany (changes in %) - increasing LE
Age-groups 2020/98 2050/20 2050/98 2020/98 2050/20 2050/98
0-34 -22 -25 -41 -22 -25 -4235-64 9 -24 -17 4 -26 -2365-74 29 5 35 18 0 1875+ 77 60 183 63 59 161total 22 10 34 15 7 24
1) Projection method A: Projection by age-groups, gender and diagnosis (ICD9).- 2) Projectionmethod B: Projection by age-groups, decomposed by survivors and decedents in their last, secondand third year before death.
Projection method A1) Projection method B2)

Erika Schulz14.02.2003
Number of persons with contact to a doctor in Germany
Age-group 1999 2010 2020 2030 2040 2050in 1000 in % in 1000 in %
0 - 5 198 162 159 140 123 118 - 79 -40,04 - 38 -19,325 - 10 153 127 119 112 97 90 - 63 -41,01 - 34 -22,3610 - 15 113 97 82 81 72 64 - 49 -43,10 - 31 -27,2015 - 20 127 117 101 96 90 79 - 47 -37,22 - 25 -19,9220 - 25 206 229 192 164 162 146 - 61 -29,41 - 14 -6,9225 - 30 251 237 215 184 175 167 - 85 -33,71 - 36 -14,4630 - 35 369 257 276 229 197 196 - 173 -46,87 - 93 -25,1335 - 40 373 264 265 239 206 198 - 176 -47,10 - 108 -29,0640 - 45 356 387 283 303 253 220 - 136 -38,13 - 72 -20,3745 - 50 363 461 329 331 300 262 - 100 -27,68 - 33 -9,2150 - 55 384 523 562 419 448 378 - 5 -1,35 179 46,6055 - 60 553 564 727 531 536 491 - 62 -11,26 174 31,4660 - 65 588 506 654 712 542 580 - 8 -1,34 67 11,3565 - 70 526 584 684 889 662 672 146 27,73 158 30,0870 - 75 554 763 664 873 961 742 187 33,83 109 19,7175 + 1 189 1 567 2 021 2 334 3 054 3 225 2 036 171,19 832 69,93Total 6 302 6 846 7 335 7 637 7 880 7 628 1 326 21,04 1 032 16,38
Source: Federal Statistical Office of Germany
in 1000
Changes2050/1999 2020/1999

Erika Schulz14.02.2003
People receiving LTC in GermanyDisability level 1999 2020 2050 2020 2050
constant LE increasing LE
Level I(substancial)home care 702 911 1 046 1 063 1 644institutional care 211 266 308 312 502total 913 1 177 1 354 1 374 2 147
Level II(severe)home care 499 643 734 752 1 189institutional care 241 326 409 396 718total 740 969 1 144 1 148 1 906
Level III(very severe)home care 150 184 203 213 322institutional care 126 167 205 201 353total 276 352 408 414 675
Allhome care 1 352 1 739 1 983 2 027 3 155institutional care 578 760 923 909 1 573total 1 929 2 498 2 906 2 936 4 728
Sources: German Federal Statistical Office; model estimates.
persons receiving long-term care in thousand

Erika Schulz14.02.2003
People in LTC - structure in %Disability level 1999 2020 2050 2020 2050
constant LE increasing LE
Level I(substancial)home care 36,4 36,5 36,0 36,2 34,8institutional care 10,9 10,6 10,6 10,6 10,6total 47,3 47,1 46,6 46,8 45,4
Level II(severe)home care 25,9 25,7 25,3 25,6 25,1institutional care 12,5 13,1 14,1 13,5 15,2total 38,4 38,8 39,4 39,1 40,3
Level III(very severe)home care 7,8 7,4 7,0 7,2 6,8institutional care 6,5 6,7 7,1 6,8 7,5total 14,3 14,1 14,0 14,1 14,3
Allhome care 70,1 69,6 68,2 69,0 66,7institutional care 29,9 30,4 31,8 31,0 33,3total 100,0 100,0 100,0 100,0 100,0
Sources: German Federal Statistical Office; model estimates.
structure of nursing level

Erika Schulz14.02.2003
Informal home care - care giving by groups of family caregivers in Germany
1999 2020 2050
women aged 40-65employed 3,2 4,2 9,3non-employed 8,1 12,2 24,9total 5,2 7,3 15,5
women aged 65-80 4,8 6,1 9,2
men aged 65-80 2,3 2,5 3,3
women aged 80 and over 4,8 3,9 3,8
men aged 80 and over*) 0,0 0,0 0,0
*) Current number of cases are very small but not zero.Sources: Federal statistical office of Germany; model estimates.
in %
share of caregivers required for informalhome care by population group

Erika Schulz14.02.2003
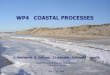
Share of caregivers required for informal home care by population group
0
5
10
15
20
25
30
1998 2020 2050Jahre
in %
employed women 40-65 non-employed women 40-65 total women 40-65
women 65-80 men 65-80 women 80 and over

Erika Schulz14.02.2003
Assumptions about life expectancy
Completed Mortality/ death rates Age male female
0 0,005179 0,004138 for the last three years1 0,000463 0,000397 as a basic information for 2 constant life expectancy34 for the forecasting period5 20106 20207 20308 20409 2050
10...highestpossibleage
100 1 1

Erika Schulz14.02.2003
Assumptions about fertility
Age of number of number of birth rateswomen female pop life births
15 if available for cohorts16 (same birth year)17 for all cohorts in the past18 else19 for periods in the past2021 forecast of birth rates for22 201023 202024 2030
... 204045 2050

Erika Schulz14.02.2003
Assumptions about migration (1)
Age orage-groups men women men women0-55-1010-15 for the last three years15-20 and so ontotal 100 100 100 100
Age-profile of gross migration flowsImmigration (flow in) Emigration (flow out)

Erika Schulz14.02.2003
Assumptions about migration (2)
yearmen women men women
19951996199719981999200020102020203020402050
Immigration EmigrationCount of gross migration flows

Erika Schulz14.02.2003
Utilisation rates separated for survivors and decedents
Age-groups survivorslast year 2 year 3 year of life before death before death
0-2425-3435-44 for male and for female if possible45-5455-6465-7475-7980-8485-8990+
decedentsfor example: hospital days of

Erika Schulz14.02.2003
Source: Mandeep Bains: Projection future needs. Presentation at the OECD workshop: Ageing related diseases, Paris 20/21 June 2002.

Erika Schulz14.02.2003
Health care expenditure separated for survivors and decedents
Age-groups survivorslast year 2 year 3 year of life before death before death
0-2425-3435-44 for male and for female if possible45-5455-64 for the most available years in the past65-7475-79 for single treatment categories (hospital, 80-84 doctor, medical and LTC)85-8990+
we are also interested in the age-profile of health expenditure of the total population
decedentsfor example: health expenditure for acut care