-
8/12/2019 Am. J. Epidemiol.-1999-Li-608-11
1/4
American Journal of Epidemiology
Copyright 1999 by The Johns Hopkins University School of Hygiene
and Public Health
All rights reserved
Vol.149,
N o.
7
Printed in U.S.A.
A BRIEF ORIGINAL CONTRIBUTION
Maternal Placental Abnormality and the Risk of Sudden Infant
Death
Syndrome
De-Kun Li and Soora Wi
To determine whether placental abnormality (placental abruption
or placental previa) during pregnancy
predisposes an infant to a high risk of sudden infant death
syndrome (SIDS), the authors conducted a
population-based case-control study using 1989-1 991 California
linked birth and death certificate data. They
identified 2,107 SIDS cases, 96 of whom were diagnosed through
autopsy. Ten controls were randomly
selected for each case from the same linked birth-death
certificate data, matched to the case on year of birth.
Abo ut 1.4 of mothe rs of case s and 0.7 of mothers of controls
had either placental abrup tion or placenta
previa during the index pregnancy. After adjustment for
potential confounders, placental abnormality during
pregnancy was ass ociated with a twofold increase in the risk of
SIDS in offspring (odds ratio = 2. 1, 95
confidence interval1.3-3.1 .The individual effects of placental
abruption and placenta previa on the risk of SIDS
did not differ significantly. An impaired fetal development due
to placental abnormality may predispose an infant
to a high risk of SIDS.
Am J Epidemiol 1999;
149:608-11.
abruptio, placentae; case-control studies; placenta praevia;
sudden infant death
Although changing sleeping position has resulted in
a reduction of sudden infant death syndrome (SIDS) in
many countries (1-6), the etiology for abnormal fetal
development that predisposes infants to a high risk of
SIDS remains elusive. Among the potential risk factors
during pregnancy, intrauterine hypoxia has been
hypothesized to be an important etiologic factor.
However, few studies have examined this hypothesis
(7). Maternal smoking during pregnancy, which,
among other potential toxicities, could result in chron-
ic intrauterine hypoxia, has been associated with an
increased risk of SIDS in offspring (7, 8). Other con-
ditions that may potentially be related to intrauterine
hypoxia, such as placental abnormality, cord prolapse,
and preeclampsia/eclampsia, were much less studied
(9).
The placenta is vital for delivering oxygen and
nutrients to the fetus. An abnormal placental condition
such as placenta previa (implantation of
the
placenta in
Received for publication March 2, 1998, and accepted for
publi-
cation August 5, 1998.
Abbreviation: SIDS, sudden infant death syndrome.
From the Division of Research, Kaiser Foundation Research
Institute, California Region, Kaiser Permanente Medical Care
Program, Oakland, CA.
Reprint requests to Dr. De-Kun Li, Division of Research,
Kaiser
Foundat ion Research Inst i tute, Cal i forn ia Region,
Kaiser
Permanente Medical Care Program, 3505 Broadway, Oakland, CA
94611.
the lower uterine segment) or placental abruption (pre-
mature separation of the normally implanted placenta
prior to birth) could result in an impaired delivery of
oxygen and nutrients to the fetus, thus leading to an
abnormal fetal development due to inadequate supply
of oxygen and essential nutrients (10-14). To examine
whether placental abnormality during pregnancy is
associated with an increased risk of SIDS in offspring,
we conducted a population-based case-control study
using the 1989-1991 California linked birth and death
certificate data.
MATERIALS AND METHODS
During the period of 1989-1991, 2,107 SIDS cases
with
International Classification of Diseases
Ninth
Revision, Clinical Modification, code 798.0 listed as
the underlying cause of death were identified from the
linked California birth and d eath certificate data. More
than 96 percent of the identified SIDS cases w ere diag-
nosed through autopsy. Controls were randomly
selected from infants who did not die from SIDS and
matched to cases on the year of birth with a 10/1 con-
trol/case ratio. The information on prenatal diagnoses
of placental abruption or placenta previa as well as
other conditions was listed under the category of
Com plications and P rocedures of Labor and
Delivery on the birth certificate. Any infant with a
60 8
b
yguestonMarch5,2012
http://aje.oxfordjournals.org/
Dow
nloadedfrom
http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/
-
8/12/2019 Am. J. Epidemiol.-1999-Li-608-11
2/4
Placental Abnormality and the Risk of SIDS 60 9
diagnosis of maternal placental abruption or placenta
previa on the birth certificate was considered to have a
maternal placental abnormality during pregnancy. The
information on potential confounders that were avail-
able from the birth certificate data included maternal
age,
race/ethnicity, educational level, parity, prior mis-
carriage and preterm delivery, maternal sm oking, pres-
ence of preeclampsia/eclampsia, gestational age at ini-
tial prenatal visit during the index pregnancy, infant
low birth weight, sex, and year of birth. The informa-
tion on paternal age, race/ethnicity, and educational
level was also available for adjustment.
An odds ratio w ith its 95 percent confidence interval
was used to estimate the relative risk of SIDS associated
with prenatal placental abnormality. Logistic regres-
sion was used to obtain the estimates after adjustment
for potential confounders (15).
RESULTS
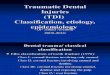
Table presents the characteristics of the study pop -
ulation. Compared with mothers of controls, mothers
of SIDS cases w ere more likely to be less than 18 years
old, to be black, to have had more prior live births and
more than two prior miscarriages, to have smoked, to
have had preeclampsia/eclampsia, or to have had inad-
equate prenatal care during the index pregnancy. In
addition, they were less likely to have any college ed u-
cation. SIDS cases were also more likely to have low
birth weight and to be male compared with controls.
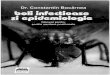
After adjustment for maternal age, educational level,
parity, prenatal smoking, prenatal care, and infant sex,
maternal placental abnormality (placental abruption or
placenta previa) was associated with a twofold
increase in the risk of SIDS in offspring (table 2).
Further adjustment for other potential confounders
including birth year of infants, maternal race/ethnicity,
birth interval, a history of miscarriage, preterm deliv-
ery, preeclampsia/eclampsia during pregnancy, pater-
nal age, and infant with low birth weight did not mate-
rially change the estimate. The individual effects of
abruptio placenta and placenta previa on the risk of
SIDS do not seem to differ significantly (table 2).
DISCUSSION
Limitations of this study need to be kept in mind
when one interprets the findings. Because the study
was based on the birth certificate data, the recorded
diagnosis of placental abruption and placenta previa
may not be complete. Although no recent quality con-
trol data are available for the California birth certifi-
cate data, it is generally expected that the incidence of
placental abruption and placenta previa is around
1-1.5 percent (10). Therefore, the incidence of 0.7 per-
TABLE 1. Characteristics of the study population California
1996-1997
Factors
Maternal age (years)
35
Maternal education (years)
1 2
Maternal race
White
Black
Asian
Hispanic
Pacific Islander
American Indian
Other
Parity (no.)
1
2
3
>4
Prior miscarriage (no.)
0
1
2
>3
Prior preterm delivery
Yes
No
Prior baby with low birth weight
Yes
No
Prenatal smoking
Yes
No
Gestational age at initial
prenatal visit (months)
-
8/12/2019 Am. J. Epidemiol.-1999-Li-608-11
3/4
610 LiandWi
underreporting had to be different between SIDS cases
and controls. Since the birth certificates were com-
pleted before the occurrence of SIDS, it is unlikely
that any differential recording was introduced because
of the SIDS status. In addition, because SIDS cases
had a relatively low socioeconomic status, a potential
differential recording bias, if it existed, would have
been more likely to result in underreporting of placen-
tal abnormality in the SIDS group than in the control
group, leading to attenuation of the observed associa-
tion between placental abnormality and SIDS risk.
Furthermore, when placental abnormality was rede-
fined to include excessive vaginal bleeding before
labor, the incidence of placental abnormality was
increased to 1 percent in the control group. How ever,
the risk of SIDS associated with the redefined placen-
tal abnormality remained elevated (odds ratio = 1.8, 95
percent confidence interval
1.2-2.6 .
The diagnosis of SIDS in the linked birth and death
certificate data should be reliable because more than
96 percent of cases were diagnosed through autopsy,
and all cases must be verified through a rigorous sys-
tem before the final diagnosis of SIDS could be
recorded on the California death certificate.
It is possible that some potential confounders such
as prenatal smoking exposure may be underreported
on the birth certificate, thus resulting in an incom-
plete control of the potential confounders. However,
any residual confounding, if it existed, was unlikely
to be strong enough to explain the observed twofold
increased risk of SIDS associated with placental
abruption or placenta previa during pregnancy, for
the current adjustment for those confounders,
though incomplete, resulted in essentially no change
between crude and adjusted odds ratios: 2.0 and 2.1,
respectively.
The findings from this study suggest that the placen-
tal problems during pregnancy may predispose an
infant to a higher risk of
SIDS.
The mechanism for this
observed association is not known at present. The pla-
centa provides a fetus with oxygen and essential n utri-
ents that are vital to normal fetal development.
Although the etiology of placenta previa is largely
unknown, it is believed that a need for increased pla-
cental surface area due to such factors as extensive
endometrial scarring is probably the driving force for
the formation of placenta previa (10). Therefore, pla-
centa previa not only results in the reduced supply of
oxygen and nutrients to the fetus due to decreased pla-
cental surface area, suboptimal uterine location, and
bleeding, but the presence of the condition also indi-
cates reduced uteroplacental oxygen and delivery of
nutrients (10). In the case of placental abruption, the
premature separation of the normally implanted pla-
centa will result in a decreased surface area for m aternal-
fetal blood exch ange, thus leading to a reduced supply
of oxygen and essential nutrients. It is obvious that
both placental abruption and placenta previa could
result in or indicate a reduced supply of oxygen and
essential nutrients to the fetus. Although placental
abruption may result in acute fetal hypoxia compared
with placenta previa which more likely leads to chronic
fetal hypoxia, the effect of fetal hypoxia on fetal devel-
opment, especially on the neurologic system, in terms
of duration and intensity is not well understood
(13,
16,
17). It is possible that both severe hypoxia for short
duration and chronic mild hypoxia can result in fetal
maldevelopment. Our separate analysis of the individ-
TABLE 2. Maternal placental abnormality and the risk of sudden
infant death syndrome California
1996-1997
Factors
Placental abnormality^
Yes
No
Abruptio placenta
Yes
No
Placental previa
Yes
No
Cases
(n = 2,028)
No .
28
2,000
16
2,000
13
2,000
1.4
98.6
0.8
99.2
0.7
99.3
Controls
(n = 21,037)
No .
146
20,891
80
20,891
69
20,891
*
0.7
99.3
0.4
99.6
0.3
99.7
Odds
ratiof
2.1
1.9
2.3
95
confidence
interval
1.3-3.1
1.1-3.3
1.3-4.3
* Subjects with m issing data on the adjusted variables were
excluded.
t Odd s ratio adjusted for m aternal age, educational level,
parity, prenatal sm oking, prenatal care, and infant's
sex. Further ad justme nt for birth year of infant, materna l
race, birth interval, a history of miscarriage, preterm deliv-
ery, preeclampsia during pregnancy, paternal age, and infant
with low birth weight did not materially alter the esti-
mate.
XIncluding abruptio placenta and placental previa. One case and
three controls had both conditions.
Am J Epidemiol
Vol. 149, No. 7, 1999
b
yguestonMarch5,2012
http://aje.oxfordjournals.org/
Downloadedfrom
http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/
-
8/12/2019 Am. J. Epidemiol.-1999-Li-608-11
4/4
Placental Abnormality and the Risk of SIDS 611
ual effects of placental abruption and placenta previa
on the risk ofSIDSdid not differ significantly (table 2).
Depending on the severity of the placental abnor-
malities, various damages to fetal development includ-
ing death may occur (12, 13 , 18, 19). Althoug h the
exact types of damages to live births by the placental
abnormalities during pregnancy are not well docu-
mented, the central nervous system is probably a
potential target because of the effect of fetal hypoxia
(13,
18). A defective cardiorespiratory con trol system
in the brainstem has been hypothesized to be involved
in the etiology of SIDS (20-25). Therefore, it is con-
ceivable that some of the neurologic damage could be
severe enough, though not detectable by autopsy, to
result in SIDS when extraneous risk factors such as
prone sleeping position are present. Although the inci-
dence of placental abruption and placenta previa is
low, understanding the association of placental abnor-
mality and the risk of SIDS may enhance our knowl-
edge of the role of the placenta in determining the risk
of SIDS as well as other adverse pregnancy outcomes.
ACKNOWLEDGMENTS
This study was supported in part by a grant from the
National Institute of Child Health and Human Development
(CRMC-94-01).
The authors thank the California Vital Statistics
Department for making the birth and death certificate data
available for research.
REFERENCES
1. Willinger M, Hoffman HJ, Hartford RB. Infant sleep
position
and risk for sudden infant death syndrome: report of meeting
held January 13 and 14, 1994, National Institutes of Health,
Bethesda, MD. Pediatrics 1994;93:814-19.
2. Dwyer T, Ponsonby ALB, Newman NM, et al. Prospective
cohort study of prone sleeping position and sudden infant
death syndrome. Lancet
99
;337:1244-7.
3. Gormally S, Matthews TG. Sleep position and SIDS in Irish
infants. Ir Med J 1994;87:58.
4. Wigfield RE, Fleming PJ, Berry PJ, et
al.
Can the fall in Avon's
sudden infant death rate be explained by changes in sleeping
position? (see comments). BMJ 1992;304:282-3.
5.
Engelberts AC, de Jonge GA, Kostense PJ. An analysis of
trends in the incidence of sudden infant death in the
Netherlands 1969-89. JPaediatr Child Health 1991;27:329-33.
6. Dwyer T, Ponsonby AL, Blizzard L, et al. The contribution
of
changes in the prevalence of prone sleeping position to the
decline in sudden infant death syndrome in Tasmania (see
comments). JAMA 1995;273:783-9.
7. Hoffman HJ, Hillman LS. Epidemiology of the sudden infant
death syndrome: maternal, neonatal, and postneonatal risk
fac-
tors.Clin Perinatol 1992; 19:717 -37.
8. Li DK, Daling JR. Maternal smoking, low birth weight, and
ethnicity in relation to sudden infant death syndrome. Am J
Epidemiol 1991;134:958-64.
9. Buck G M, Cookfair DL, Michalek AM, et al. Assessment of
in
utero hypoxia and risk of sudden infant death syndrome.
Paediatr Perinat Epidemiol 1989;3:157-73.
10.Scott JR. Placenta previa and placental abruption. In: Scott
JR,
Disaia PJ, Hamm ond C B, et al, eds. Danforth's obstetrics
and
gynecology. Philadelphia: JB Lippincott Company, 1994:
489-500.
11. Low J A. The relationship of asphyxia in the mature fetus
to
long-term neurologic function. Clin Obstet Gynecol
1993;36:82-90.
12.
Lam BC, Yeung CY. Perinatal features of birth asphyxia and
neurologic outcome. Acta Paediatr Jpn 1992;34:17-22.
13.
Perlman JM. Systemic abnormalities in term infants following
perinatal asphyxia: relevance to long-term neurologic out-
come. C lin Perinatol
1989;
16:475-84.
14.
Jiang ZD, Tierney
T S.
Long-term effect of perinatal and postna-
tal asphyxia on developing human auditory brainstem respons-
es : brainstem impairment. Int J Pediatr Otorhinolaryngol
1996;34: l l l -27.
15. Breslow N E, Day NE, eds. Statistical methods in cancer
research. Vol I. The analysis of case-control studies. Lyon:
International Agency for Research on Cancer, 1980. (IARC
scientific publication no. 32).
16. Low JA, Simpson LL, Tonni G, et al. Limitations in the
clini-
cal prediction of intrapartum fetal asphyxia. Am J Obstet
Gynecol 1995;172:801^t.
17. Low JA, Simpson LL, Ramsey DA. The clinical diagnosis of
asphyxia responsible for brain damage in the human fetus
(published erratum appears in Am J Obstet Gynecol
1992;167:1124). Am J Obstet Gynecol 1992,167:11-15.
18. Low JA. Relationship of fetal asphyxia to neuropathology
and
deficits in children. Clin Invest Med 1993;16:133^t0.
19. Williams LJ, Lucci AP. Placental examination can help
deter-
mine cause of brain damage in neonates. Tex Med 199O;86:
33-8 .
20 . Hunt CE. The cardiorespiratory control hypothesis for
sudden
infant death syndrome. Clin Perinatol 1992 ;19:757 -72.
21.
Schw artz PJ, Stram ba-Ba diale M , Segantini A , et al.
Prolongation of the QT interval and the sudden infant death
syndrome (see comments). N Engl J Med 1998;33 8:1709-14.
22 . Obonai T, Asanuma M, Mizuta R, et al. Evidence of brain
ischemia in early neonatal sudden death syndrome.
Neuropediatrics 1997;28:145-8.
23 .
Kinney HC, Filiano JJ. Brainstem research in sudden infant
death syndrome. Pediatrician
1988;
15:240-50.
24 . Willinger M. SID S: a challenge. J NIH Res
1989;1:73-80.
25 . Filiano JJ, Kinney HC. Sudden infant death syndrome and
brainstem research. Pediatr Ann 1995;24:379-83.
Am J Epidemiol
Vol. 149, No. 7, 1999
byguestonMarch5,2012
http://aje.oxfordjournals.org/
Do
wnloadedfrom
http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/http://aje.oxfordjournals.org/