Embed Size (px)
Citation preview

Amanda Smart, Director of Practice and Member Services,
Ontario Physiotherapy Association,
Emily Stevenson, Physiotherapist, East End Community Health
Centre
Tariq Asmi, CEO, The Four Villages Community Health Centre
1

After attending this session participants will:
1. Understand the opportunities for integrating physiotherapists in primary health care (PHC) organizations
2. Understand how integration of new physiotherapist positions will support clinical best practices and enhance the inter-professional team
3. Be aware of opportunities to strengthen their own services through the integration of physiotherapists
4. Understand some of the current models of collaborative practice involving physiotherapy services
5. Be aware of the role of Ontario Physiotherapy Association in supporting organizations and PTs in these roles
2

3
Presenter Disclosure Presenters: Amanda Smart, Emily Stevenson, Tariq Asmi Relationships with commercial interests: • Grants/Research Support: None • Speakers Bureau/Honoraria: None • Consulting Fees: None • Other: None

5500 members
Largest provincial branch of the Canadian Physiotherapy Association
What we do: ◦ advocacy
◦ professional development
◦ career support
4
5
• Self regulated • Direct access health care professional • Inter-professional • Prevent and address illness, injury or disability resulting from a variety of conditions

6
• Comprehensive care approach (assessment, treatment, consultation, education) • Present in all parts of the health care system from acute to ambulatory/primary care

“The assessment of neuromuscular, musculoskeletal and cardio respiratory systems, the diagnosis of diseases or disorders associated with physical dysfunction, injury or pain and the treatment, rehabilitation and prevention or relief of physical dysfunction, injury or pain to develop, maintain, rehabilitate or augment function and promote mobility” Physiotherapy Act, 2009, c. 26, s. 22 (1)
7

Additional Authorities 1. Communicating a diagnosis identifying a disease, a physical
disorder or dysfunction as the cause of a person’s symptoms. 2. Moving the joints of the spine beyond a person’s usual
physiological range of motion using a fast, low amplitude thrust.
3. Tracheal suctioning. 4. Treating a wound below the dermis using any of the following
procedures: cleansing, soaking, irrigating, probing, debriding, packing, dressing.
5. For the purpose of assessing or rehabilitating pelvic musculature relating to incontinence or pain disorders, putting an instrument, hand or finger, beyond the labia majora, or beyond the anal verge.
6. Administering a substance by inhalation. 2009, c. 26, s. 22 (2) http://www.ontario.ca/laws/statute/91p37
8

9

10

11
• Assessment, diagnosis , treatment including self-management programs for people with: -low back pain
• Assessment and treatment
for those with neurological conditions - stroke - Parkinson’s
• Falls prevention programs
including outreach programs in community

12
• Self-management programs and counseling for increased activity for those with -obesity -diabetes -arthritis and -chronic diseases
• Pain management
programs

13
14
Dufour SP, Lucy SD, Belle Brown J. Understanding Physiotherapists' Roles in Ontario Primary Health Care Teams. Physiotherapy Can. 2014;66(3);234-242

Positive outcomes related to:
High levels of client satisfaction
Decreased wait times
Increased cost-effectiveness relative to hospital-based services
Reduced rates of referral to specialists and improved
Patient-related outcomes such as quality of life, exercise tolerance, and health status
Cott CA, Mandoda S, Landry MD. Models of integrating
physiotherapists into family health teams in Ontario, Canada: challenges and opportunities. Physiotherapy Can. 2011; 63(3):265-
75.
15
Limited number of PTs practicing in CHCs
The FHT story: ◦ PT were initially on the list of team members for
the MOHLTC initiative announced in 2005.
◦ No requests for PT were approved because of a policy barrier
16
17
Minister Matthews announcement on April 18th, 2013 ◦ $156M per year for physiotherapy and
reactivation/exercise programs for seniors ◦ Implementation date August 1st, 2013 ◦ home care, community clinics, LTC, primary care,
retirement homes ◦ Primary care= Community Health Centres, Family
Health Teams, Aboriginal Health Access Centres, NP led clinics program based funding (cardiovascular health, lung
health, diabetes, healthy aging)
18

19

20
www.opa.on.ca

TCLHIN CHCs Expanding Access to Community-Based Rehabilitation
21

22
23

24

25
CHC Funding: $2.2 Million (52%) Ontario: $4.2 Million

1) Flemingdon Health Centre 2) Davenport-Perth Neighbourhood CHC 3) LAMP CHC 4) Stonegate CHC 5) The Four Villages CHC 6) Parkdale CHC 7) Central Toronto CHC 8) Anne Johnston Health Station 9) Regent Park CHC 10) South Riverdale CHC 11) Anishnawbe Health Toronto 12) East End CHC
26

27

28
Site Assessments
Renovations
Supplies and Equipment
29
Comprehensive Report assessing the state of physiotherapy care in CHCs across Toronto AND great potential to build on success to:
Expand Access to Rehabilitation
Drive a Population Health Model
Foster a system/network of care
Create a community of practice
Demonstrate new and effective process for coordinated investment in community sector
30
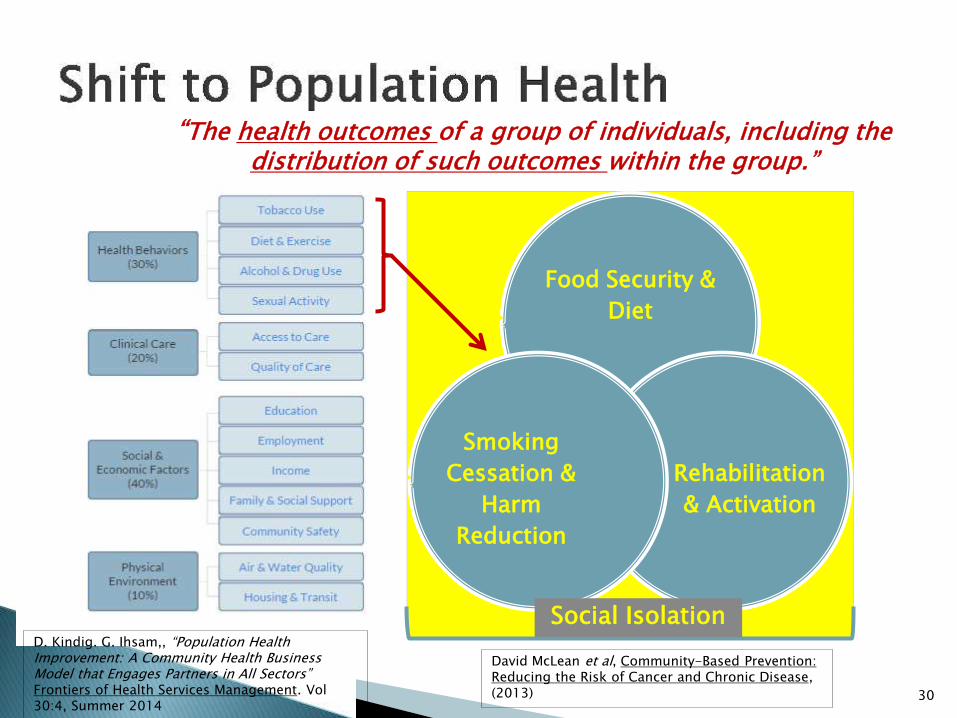
“The health outcomes of a group of individuals, including the distribution of such outcomes within the group.”
Food Security &
Diet
Rehabilitation
& Activation
Smoking
Cessation &
Harm
Reduction
Social Isolation D. Kindig. G. Ihsam,, “Population Health Improvement: A Community Health Business Model that Engages Partners in All Sectors” Frontiers of Health Services Management. Vol 30:4, Summer 2014
David McLean et al, Community-Based Prevention: Reducing the Risk of Cancer and Chronic Disease, (2013)
1. Report Completed a) Report is fully accepted by CHCs as a
comprehensive overview with key recommendations for strengthening community-based rehab across TCLHIN
b) View report as being applicable to new and existing PT resources at CHCs
2. PTs are being hired
3. Equipment ordered and arriving
4. Renovations underway
31

CLINIC CARE OUTREACH CASE
MANAGEMENT
SHARED CARE INTEGRATED
CARE PROGRAMMING CONSULTATION
32
Delivering on Features: 1. All partnerships offer all six features with new and possibly existing PTs 2. Each CHC’s clients can access all six features ACROSS THE
“PARTNERSHIPS” (provider back-up within partnerships)
3. Full client mobility across the entire CHC Community Rehab Network

1. Clinic care: (1 on 1 AND group) Provides clients with individual goal-oriented care in a one to one or group care delivery format.
2. Outreach: Targeted outreach services for marginalized populations who would not otherwise access services but who may be at risk
3. Case management: Where the PT holds accountability for referral to other required services (internal and external)
4. Shared care: Collaborative service delivery for coordinated care within the CHC.
5. Integrated care: External partnerships for collaborative service delivery for coordinated care across the continuum of care with at least one other non-CHC provider
6. Programming Consultation: Internal and external partnerships for programming development support to wellness services for preventative, maintenance care and health promotion
33

Item Timeline CHC Feedback
Changes
1. Create collaborative oversight governance structure to oversee implementation
By April 15 In agreement
Establish by end of May 2015
2. Establish a PT Network of CHC PTs that is enabled by a “Lead PT”
ToR by April 15th . Network by May 15th . Lead appointed by June 30th.
Support All to be done by June 30, 2105
3. Engage and Educate Internal Staff about PT Primary Health Care Model and Implementation Plan
Start April 1st Underway Start June 1, 2015
4. Engage and Educate External Partners about PT Primary Health Care Model and Implementation Plan
(consistent info and messages)
Plan by April 30th; execute by May 1st
Start Mid- June 2015
34
CONT’D....

Item Timeline CHC Feedback
Changes
5. Establish programming integration principles for the CHC PT Primary Health Care Model
Programming integration principles related to model Implementation are drafted by 30 April 2015 and Disseminated for review CHC leads adopt/approve by 15 May 2015 A minimum of 2 of the 6 service delivery features of the CHC PT Primary Health Care model are implemented at each CHC by 30 June 2015 A minimum of 4 of the 6 service delivery features of the CHC PT Primary Health Care model are implemented at each CHC by 30 September 2015 All 6 service delivery features of the CHC PT Primary Care Model are implemented at all CHCs by Dec 31, 2016
Support
35

CURRENT POPULATIONS: Seniors, Infants, Individuals with Physical Disabilities, Adults Family specific programs, Racialized populations, Youth, Underinsured, Women/Men specific programs, Children, Housing Challenged, Newcomers/Immigrants/Refugees, People living with mental health and/or addictions, People with limited English proficiency.
CURRENT CONDITIONS/INDICATIONS ( listed alphabetically):
- -
-
36
Current conditions/indications
Abuse Impaired mobility
Arthritis/Rheumatism Low Back Pain
Asthma Musculoskeletal Injury
Cancer Neurological disorders
Chronic Obstructive Pulmonary Disease (COPD) Obesity
Chronic Pain - Chronic Fatigue Pre/Post Natal
Diabetes Pre/Post-Surgical
Fetal Alcohol Spectrum Disorder Repetitive Strain Work Related Injuries
Hepatitis C Stress and stress-related disorders
HIV Trauma
Hypertension Wound Care

37
a) Need to measure: access/activities; client/staff satisfaction; client outcomes (i.e., Triple Aim)
b) Need to get measures right and in place.
c) Phased Approach to collecting data
d) Priority indicators for TCLHIN
e) Via NOD

38
LHIN Liaison & Oversight
Group
Clinical Directors PT Implementation Working
Group Chaired by Clinical Director Enabled by Part-time “PT
Project Lead”
( Clinical Directors or other)
Participating CHCs’/FHT
Primary Care PT Network (new and existing PTs)

Clinical Directors Working Group to:
1) Develop Evaluation Framework (with Project Lead) with input from Liaison/Oversight and TCLHIN
2) Select Evaluator (not PT lead but “PT lead” helps to oversee)
3) Report back both on outcomes/successes & collaborative process
4) Oversee Evaluation Process and report generation
5) Report back to Liaison/Oversight
6) Share report with TCLHIN for input and feedback
7) Draft Final Report
39

PTs hired
Renovations done
PT Lead being hired (competition closes June 5th)
Services being offered
Inter-CHC service collaboration & coordination being strengthened
40
Emily Stevenson
Registered Physiotherapist
41
1.8 FTEs physiotherapists
3700 clinical (registered) clients
1200 group clients
Individual care, group programming, and consultation
42
Self-referrals, or referrals from clinical/allied health team
Interventions: **education, **self-management, manual (“hands on” therapy), posture and movement retraining, exercise, acupuncture/dry needling
Frequency of visits: maximum 1x/week
Average # of visits: 4-5
43
Initiatives to manage demand ◦ Referral prioritization
◦ Urgent care appointments
◦ Full scope of practice (direct access, medical directives)
44

Chronic Pain Management (physiotherapist, psychotherapist, pharmacist, MD, community health worker)
Bone Health (physiotherapist, community health worker)
Weight Management (physiotherapist, dietitian)
45

Gentle Fit (kinesiologist)
Building Better Backs (kinesiologist)
Walking program (kinesiologist)
Exercise is Medicine (kinesiologist)
Yoga (yoga instructor)
Aquafitness program (community health worker)
Consultation/joint assessment/intervention with NPs/MDs and chiropodist
Referral to community programs/services
Education for staff for re: client care (ie. interpretation of diagnostic imaging)
Ergonomics/health promotion for centre staff
47

Identify physiotherapists with skills/interests in both individual care and program development/delivery/evaluation
Identify client populations, and gaps in service, where
physiotherapy can improve care Identifying appropriate ratio of components of the Model
for effective service delivery (ie. Clinic Care, Outreach, Case Mgt, Consultation)
Providing support/resources for physiotherapists in
new/emerging primary care roles Measuring outcomes
48

Questions?
49





























