Embed Size (px)
Citation preview
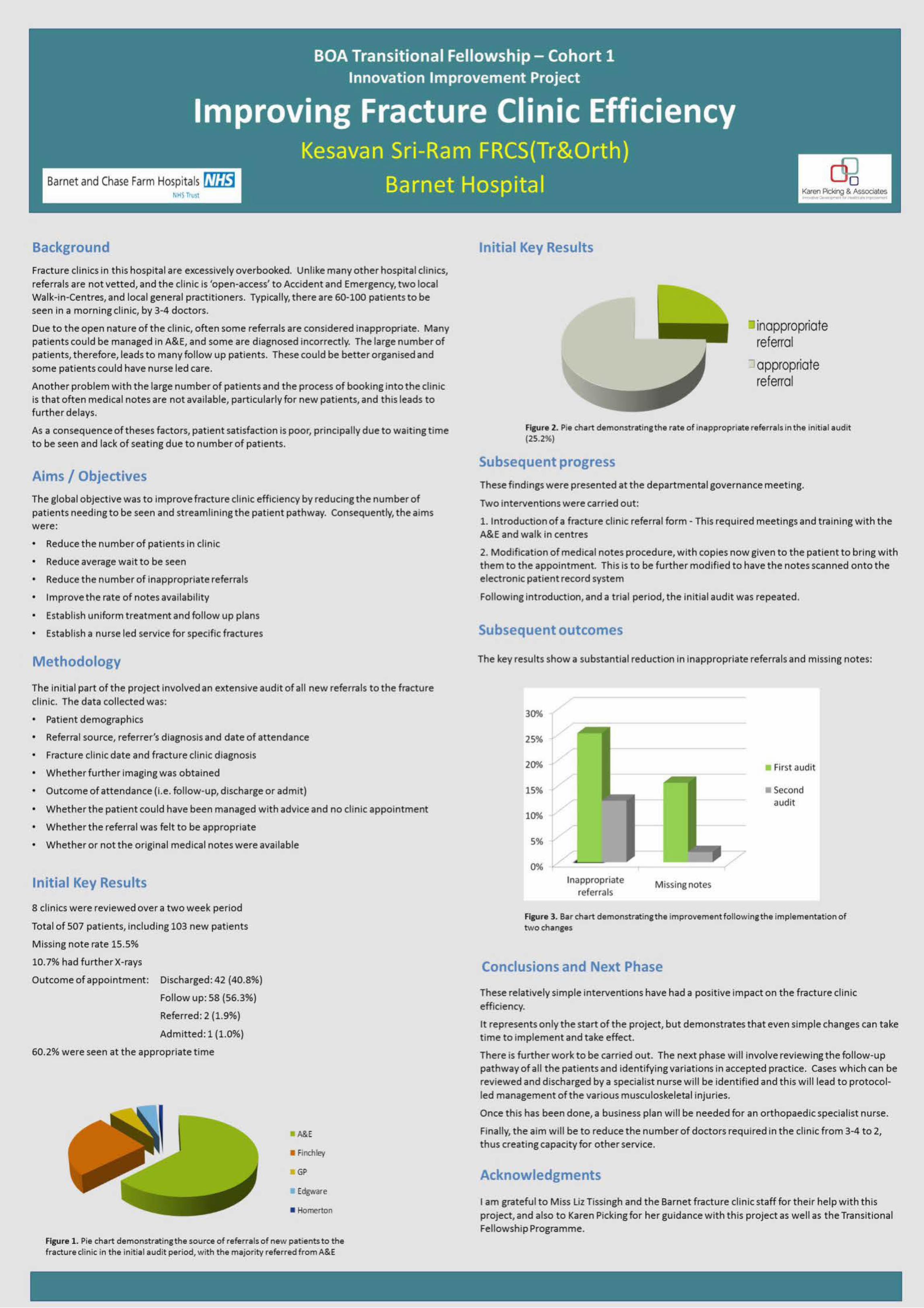
Progress to Date (Continued) • I audited my results of Ultrasound scans in theatre on the
morning of surgery with an aneasthetic ultrasound machine which they used for their nerve blocks with the intraoperative findings and found my results to be 76% accurate. The low result was probably because the Ultrasound probe was not specifically designed for musculoskeletal use and partly because of my learning curve.
Results • Place for ultrasound clinics has been finalised
• We have had a look at various machines and one has been finalised.
• Discussion has been done with the finance committee which has now accepted a need for such a clinic and we are awaiting funding for procurement of a machine.
Benefits • Patient satisfaction
• Reduce patient visits
• Reduce duration to treatment thereby reducing the waiting list times for both Orthopaedics and Radiology
• Reduce cost by reducing patient visits and using services of one department only
• Transfer skills by teaching trainees
Outcomes • Process mapping done.
• Place identified in community
• Learnt to do Ultrasound of shoulders
• Business plan written for Ultrasound machine
Next Phase • The new British Orthopaedic Association Fellow will be
learning to do the ultrasound scans and take it forward. • I will be writing a business plan to get an ultrasound
machine in the next hospital in my capacity as a consultant. Contact: [email protected]
Project Overview (Introduction) • Out patient journey from General Practise referral to
treatment can take 12-20 weeks. • The patient needs about three hospital visits, namely, initial
appointment with Orthopaedic specialist who may then send the patient for an Ultrasound scan and a review appointment to discuss the results and plan treatment.
• This process needs the services of an Orthopaedic specialist as well as a Radiologist.
Aims, Objectives & Outcomes • Aim of this project is to introduce a one stop clinic so that
the patient is seen in the Orthopaedic clinic, the Ultrasound scan is done by the Orthopaedic surgeon and the treatment is planned in One Visit.
• It can be done in the peripheral clinics or community centres with the help of a portable ultrasound.
Methodology • I mapped the patient pathway which showed that as per the
present arrangement the patients had to visit the hospital three times and wait for a total of anywhere between 12 -20 months to have a treatment plan.
• A discussion was done with the relevant stakeholders namely Orthopaedic Upper Limb consultants, musculoskeletal radiologist, nursing and auxillary staff.
• We were regularly conducting upper limb clinics in the peripheral and community hospitals and it was decided that the one stop clinics could be done in these locations.
• I attended a shoulder Ultrasound course at the beginning of my fellowship year and attended the shoulder ultrasound sessions with a musculoskeletal radiologist.
• I performed Ultrasound scans on patients on the morning of surgery in theatre
• We wrote a business plan in order to procure a portable ultrasound machine
Progress to Date • We did a survey of the outpatients in the clinic and most of
them agreed that a one stop shoulder clinic would be beneficial to them.
• We identified a place for the clinic in the periphery and discussed with the relevant stakeholders (Upper Limb Consultants, musculoskeletal radiologist and nursing staff in this case).
Amit B Putti, Department of Orthopedics,
North Tees and Hartlepool NHS Foundation Trust, Stockton-on-tees Orthopaedic Transitional Fellowship - Cohort 1

Implementation of British Spine Registry at Stoke Mandeville Hospital
Babur MAHMOOD MSc BM FRCS (T&O) BOA Transitional Fellow (2012-2013, Cohort 1) Spinal Surgery - Stoke Mandeville Hospital
Project Overview:
Outcome research is now an essential part of modern medical care.
Historically, outcomes of surgical treatment have been based on care providers’ criteria [e.g. fusion rate, deformity correction or clinician-based subjective data (“poor” to “excellent”)]
Outcome research is now increasingly focused on patient reported outcome measures [PROMs]. This typically involves patients self reporting their perception of the treatment received usually via a questionnaire.
The British Spine Registry [BSR] has been commissioned by the British Association of Spine Surgeons. It is a voluntary (both for patients and surgeons) web based permanently accessible and “easily” updatable database, managed by a private company. It allows patient details [diagnosis, treatment and complications] to be entered on to database along with PROMs [using validated spinal scoring systems (e.g. Visual Analogue Scale, Oswestry Disability Index, Neck Disability Index and Myelopathy Disability Index etc)].
Currently, the patient and treatment details have to be entered manually on the database. The PROMs can be entered manually [after patient has filled the scores on paper] or there are data entry kiosk PC being made available by the private company [at a considerable cost to the NHS]
Aim of the Quality Improvement Project: The aim of the project was to implement a system in the spinal outpatient clinics across the Buckinghamshire Healthcare NHS Trust, where the patients can enter their PROMs on to BSR database electronically using the tablet whilst sitting in the waiting room in the clinic.
This tablet based system of capturing the PROMs data would:
1. Save time that would otherwise be spent by the clinician or secretarial staff on entering the scores the BSR data base
2. Capture higher proportion of data by avoiding the loss of paper based scores
3. Be cheaper than the kiosk PC [due to its initial setting up and the “housing” costs]
Benefits of the Quality Improvement Project:
Information gathering:
1. BSR
2. Other Spinal Units using BSR
3. Hospital IT department
4. Caldicott Guardian
5. Cost
Progress to Date:
1. Hospital Caldicott Guardian approval obtained
2. Trust Estate department to install Wi-Fi units in spinal outpatient clinics
Results:
No results to report at this stage
Methodology:
Reasons for Delay: 1. My lack of knowledge regarding implementation of new “system” across an NHS trust
2. Slow response from the BSR
3. Cost implications [BSR kiosk PC, the company representative visiting fees]
4. Local IT / Caldicott Guardian reservations
5. Lack of Wi-Fi across the Trust
Next Stage:
New BOA fellow in post from November 2013
Awaiting Wi-Fi installation in spinal clinics
As Trust approval is in place – to commence usage of tablets in the spinal clinics
Training of medical and Nursing staff in smooth integration of the tablets in very busy spinal clinics [up to 150 patients per week]
www.spineregistry.co.uk
QUALITY IMPROVEMENT - A TOOL TO INTRODUCE A LUMBAR AND LUMBOSACRAL DAYCASE DISCECTOMY SERVICE
Ms Y Leung (Consultant Spinal Surgeon), Musgrove Park Hospital, Taunton, UK (Tel: 01823 344618) Orthopaedic Transitional Fellowship - Cohort 1
PROJECT OVERVIEW AND AIMS
METHODOLOGY
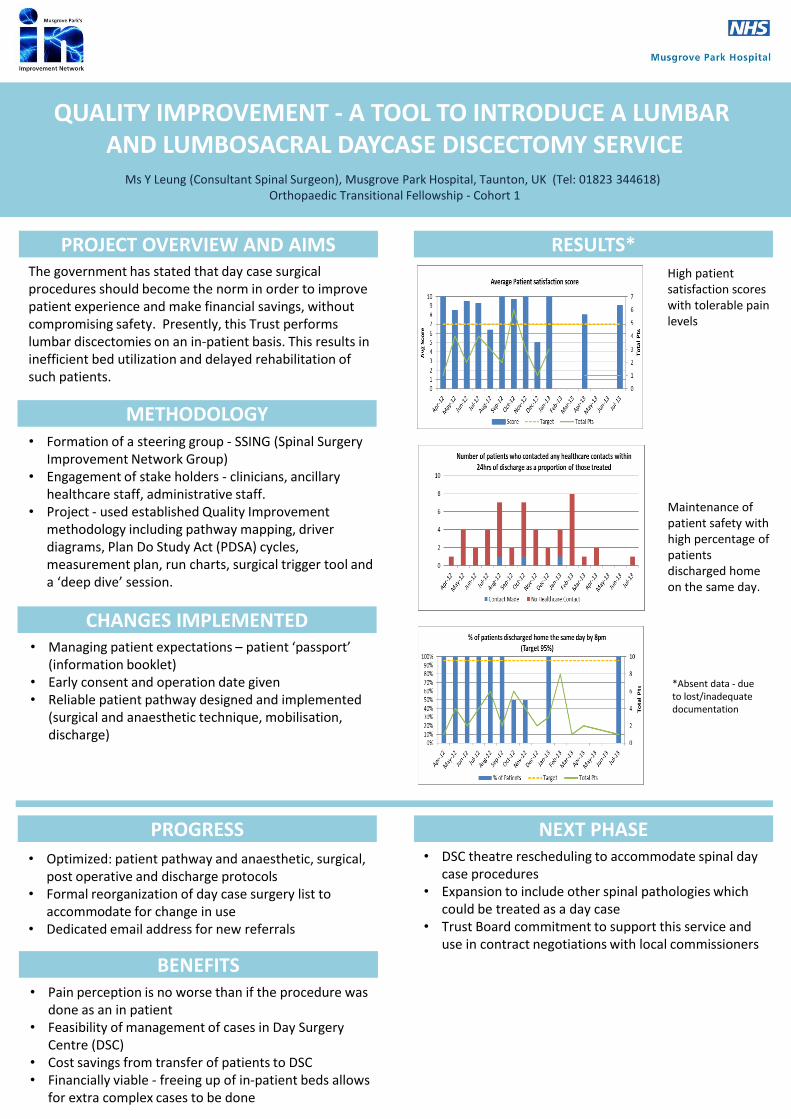
RESULTS*
CHANGES IMPLEMENTED
The government has stated that day case surgical procedures should become the norm in order to improve patient experience and make financial savings, without compromising safety. Presently, this Trust performs lumbar discectomies on an in-patient basis. This results in inefficient bed utilization and delayed rehabilitation of such patients.
• Formation of a steering group - SSING (Spinal Surgery Improvement Network Group)
• Engagement of stake holders - clinicians, ancillary healthcare staff, administrative staff.
• Project - used established Quality Improvement methodology including pathway mapping, driver diagrams, Plan Do Study Act (PDSA) cycles, measurement plan, run charts, surgical trigger tool and a ‘deep dive’ session.
• Managing patient expectations – patient ‘passport’ (information booklet)
• Early consent and operation date given • Reliable patient pathway designed and implemented
(surgical and anaesthetic technique, mobilisation, discharge)
PROGRESS
• Optimized: patient pathway and anaesthetic, surgical, post operative and discharge protocols
• Formal reorganization of day case surgery list to accommodate for change in use
• Dedicated email address for new referrals
BENEFITS • Pain perception is no worse than if the procedure was
done as an in patient • Feasibility of management of cases in Day Surgery
Centre (DSC) • Cost savings from transfer of patients to DSC • Financially viable - freeing up of in-patient beds allows
for extra complex cases to be done
NEXT PHASE • DSC theatre rescheduling to accommodate spinal day
case procedures • Expansion to include other spinal pathologies which
could be treated as a day case • Trust Board commitment to support this service and
use in contract negotiations with local commissioners
Maintenance of patient safety with high percentage of patients discharged home on the same day.
High patient satisfaction scores with tolerable pain levels
*Absent data - due to lost/inadequate documentation
• Anaesthesia
Prophylactic anti‐emetic
Tranexamic acid
Spinal anaesthesia (2‐3ml 0.5%
bupivacaine + 0.3‐0.5mg diamorphine)
Propofol ivi
Martin Goddard BOA Transitional Knee FellowLorraine Sanderson Orthopaedic Senior MatronJon Cort Consultant in Anaesthesia and Intensive Care MedicineFazal Ali Consultant Orthopaedic Surgeon.
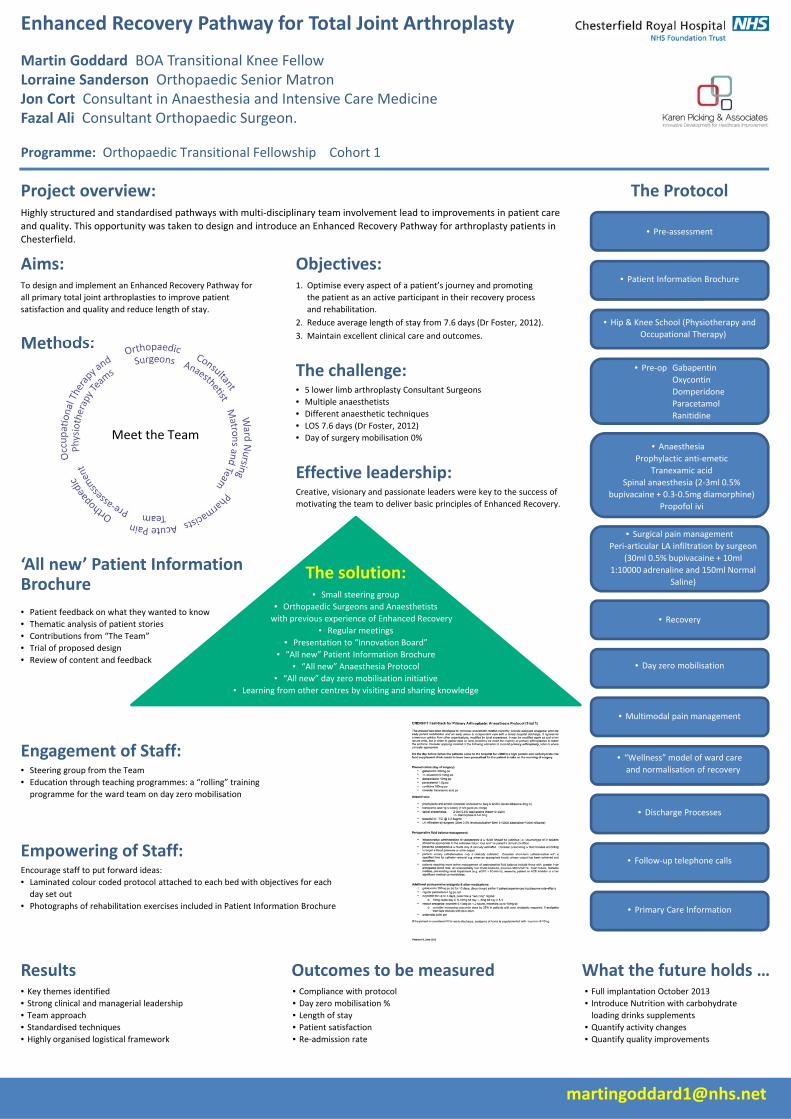
Enhanced Recovery Pathway for Total Joint Arthroplasty
Programme: Orthopaedic Transitional Fellowship Cohort 1
Project overview:Highly structured and standardised pathways with multi‐disciplinary team involvement lead to improvements in patient care
and quality. This opportunity was taken to design and introduce an Enhanced Recovery Pathway for arthroplasty patients in Chesterfield.
The Protocol
Aims:To design and implement an Enhanced Recovery Pathway for
all primary total joint arthroplasties to improve patient
satisfaction and quality and reduce length of stay.
Objectives:1. Optimise every aspect of a patient’s journey and promoting
the patient as an active participant in their recovery process
and rehabilitation.
2. Reduce average length of stay from 7.6 days (Dr Foster, 2012).
3. Maintain excellent clinical care and outcomes.
Results• Key themes identified
• Strong clinical and managerial leadership
• Team approach
• Standardised techniques• Highly organised logistical framework
Outcomes to be measured• Compliance with protocol
• Day zero mobilisation %
• Length of stay• Patient satisfaction• Re‐admission rate
What the future holds …
• Day zero mobilisation
• Primary Care Information
• Follow‐up telephone calls
• Discharge Processes
• “Wellness” model of ward care
and normalisation of recovery
• Multimodal pain management
• Recovery
• Surgical pain management
Peri‐articular LA infiltration by surgeon
(30ml 0.5% bupivacaine + 10ml
1:10000 adrenaline and 150ml Normal
Saline)
• Pre‐op Gabapentin
Oxycontin
Domperidone
Paracetamol
Ranitidine
• Patient Information Brochure
• Hip & Knee School (Physiotherapy and
Occupational Therapy)
• Pre‐assessment
Methods:
The challenge:• 5 lower limb arthroplasty Consultant Surgeons
• Multiple anaesthetists
• Different anaesthetic techniques
• LOS 7.6 days (Dr Foster, 2012)
• Day of surgery mobilisation 0%
Effective leadership:Creative, visionary and passionate leaders were key to the success of
motivating the team to deliver basic principles of Enhanced Recovery.
The solution:• Small steering group
• Orthopaedic Surgeons and Anaesthetists
with previous experience of Enhanced Recovery
• Regular meetings
• Presentation to “Innovation Board”
• “All new” Patient Information Brochure
• “All new” Anaesthesia Protocol
• “All new” day zero mobilisation initiative
• Learning from other centres by visiting and sharing knowledge
Engagement of Staff:• Steering group from the Team
• Education through teaching programmes: a “rolling” training
programme for the ward team on day zero mobilisation
Empowering of Staff:Encourage staff to put forward ideas:
• Laminated colour coded protocol attached to each bed with objectives for each
day set out
• Photographs of rehabilitation exercises included in Patient Information Brochure
• Full implantation October 2013
• Introduce Nutrition with carbohydrate loading drinks supplements
• Quantify activity changes• Quantify quality improvements
‘All new’ Patient Information Brochure
• Patient feedback on what they wanted to know
• Thematic analysis of patient stories
• Contributions from “The Team”
• Trial of proposed design
• Review of content and feedback
Meet the Team
Outcome score collection in upper limb surgery Orthopaedic transitional fellowship – Cohort 1
Mohan Pullagura
BOA Congress 2013. Birmingham [email protected]
Project Aims and Objectives: 1.Introduce a system of patient reported
outcome measures score collection in
clinics and theatres
2.Engage and involve the team to
implement change and in the process
develop my leadership skills
Project Methodology: 1.Collect background data on present
system and its effectiveness
2.Engaging the team – Consultants,
physiotherapists, OP staff, IT, business
manager
3.Equipment – Existing companies,
licensing, expenses, kiosks or tablets
4.Setting – OP clinics, theatre and expand
to other sub-specialities
Progress to date: 1.Audit on outcome score collection with
the existing system showing only 20% of
pre-op and 7% of post-op score collection.
2.Excellent engagement of consultants,
physiotherapists and staff
3.Meetings with a company detailing the
methods of data management and analysis,
expenses within reason and acceptable to
the trust
4.IT governance not agreeable to the
external company managing the data
despite the license agreement of data
protection and ownership of data after the
license expiry
Alternative strategies proposed
to progress the project: 1. Standalone application for a hospital
owned tablet involving external
professional
2. Include a patient satisfaction
questionnaire as a part of CQUIN target
3. Involve the same IT engineer who is
devising the PSQ to add the outcome
questionnaire
4. Start with one tablet with the fellow in
charge and demonstrate improvement
Results: 1. A tablet with PSQ has been approved
and a questionnaire designed enabling
analysis by importing data to excel
2. Improved negotiation skills and taking
people on board using a ‘build style’
technique.
Outcomes: Benefits for patients
and staff: 1. Patients can be informed the outcome of a
particular surgery and survival in years to
make an informed decision in the clinic
2. Performance indicator for the trust
3. Physiotherapists time is saved preventing
appointments just for scoring
4. Surgeons will have a good feedback of
their practice
Thrombo-Prophylaxis in Patients Undergoing Lower Limb Immobilisation. Introduction of a Patient Completed Risk Assessment Form.
BOA Transitional Fellowship (Cohort 1) Improvement Project.
Mr. R.P. Jeavons1*, Prof. A. Rangan1, Mr. S. Scott2, Mr. A. Gower2. 1. James Cook University Hospital, Middlesbrough. 2. University Hospital North Durham, Durham
Overview. The 2010 National Institute of Clinical Excellence (NICE), guidance on Venous Thrombo-Embolism (VTE) prophylaxis1 outlined the need for all patients prescribed immobilisation for lower limb injuries (non-operative) to be risk assessed for the development of a Thrombo-Embolic event. Then, if deemed to be high risk, and following discussion between the treating doctor and patient, prophylaxis commenced until immobilisation is stopped. This is a time consuming process especially in a busy Orthopaedic trauma clinic where in excess of 100 patients in 5 days can be seen. The challenges this posed were creating a simple screening tool that was quick and easy to use, identified the high risk patients and provided documentation of risk assessment, patient-doctor decision making and prescription of VTE prophylaxis.
Aims & Objectives. 1. Scoping review of literature on VTE related to lower limb
immobilisation. 2. Creation of Risk assessment form. 3. Introduce form into Orthopaedic clinics and overcome
associated problems. 4. Audit form effectiveness and make change where
appropriate.
Methods - Timeline.
Key Facts from Scoping Review. Incidence of VTE event whilst immobilised 5-6.3%.3,4 Cochrane Database review 20085 – VTE Prophylaxis significantly reduces incidence of VTE event when lower limb immobilisation used. No cost analysis in literature – Low Molecular Weight Heparin (LMWH) costs £161.28 for 6 weeks. Risks of LMWH: Heparin Induced Thrombocytopaenia (HIT) Major Bleed (0.3%) Allergy Wound problems (delayed healing, infection) Current Published Guidelines: NICE1 SIGN (Scottish Intercollegiate Guidelines Network)6 BOFAS (British Orthopaedic Foot & Ankle Society)7 American College of Chest Physicians8 All recommend risk assessment the if High risk consider VTE prophylaxis for period of immobilisation.
Benefits. Easy to use form with patient completed risk assessment. Saves time. Documents outcome & discussion between patient and Doctor, for incorporation into patient records. Fulfils risk assessment criteria set out by National Body Guidance.
Outcomes. The Introduction of the risk assessment form has taken 12 months to establish. It has been accepted well by patients and the improvements to the form have increased the acceptance by physicians. It is easy to use. Compliance amongst patients is excellent, but amongst Doctors is still poor. Only 50% of patients are aware of the risk of VTE events & even fewer would be willing to administer LMWH. Despite identifying the high risk patients, only 50% are being prescribed prophylaxis.
Next Phase. Continued reinforcement to Healthcare Professionals regarding the need for risk assessment & use of the form. A role for patient education regarding the risks and benefits VTE events & prophylaxis. Further adapt the form if required. Formal validation of the risk assessment score Grant application & MSc or PhD Project? A freely available validated VTE risk assessment form for use across the NHS. References. 1. National Institute for Health and Clinical Excellence. Venous Thomboembolism: Reducing the risk. 2010. 2. VTE Prevention England. http://www.vteprevention-nhsengland.org.uk/index.php/k2inv/item/222-plymouth-derriford-hospital 3. Patil S, Gandhi J, Curzon I, Hui ACW. Incidence of deep vein thrombosis in patients with fractures of the ankle treated in a plaster cast. J Bone Joint Surg Br. 2007;89:1340–1343 4. Riou B, Rothmann C, Lecoules N, Bouvat E, Bosson JL, Ravaud P, Samama CM, Hamadouche M. Incidence and risk factors for venous thromboembolism in patients with nonsurgical isolated lower limb injuries. Am J Emerg Med. 2007 Jun;25(5):502-8 5. Testroote M, Stigter W, de Visser DC, Janzing H. Low molecular weight heparin for prevention of venous thromboembolism in patients with lower-leg immobilization. Cochrane Database Syst Rev. 2008 Oct 8;(4) 6. Scottish Intercollegiate Guidelines Network. Prevention and management of venous thromboembolism: A national clinical guideline 2010. 7. http://www.bofas.org.uk/News/NewsDetails/tabid/187/ArticleId/1/Current-BOFAS-position-statement-on-VTE-prophylaxis-in-foot-and-ankle- surgery.aspx 8. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. February 2012; 141(2_suppl).
July 2013 onwards Plan to formally validate forms (? MSc/PhD
project) Share validated form for National NHS use
May 2013 Results presented James Cook University
Hospital Directorate Meeting Plan to introduce forms to New patient
Trauma Clinics
March 2013 Re-audit of new forms undertaken
December 2012 3 months audit of VTE forms performed &
presented Changes made & implemented (fig. 1)
September 2012 Forms introduced into all
New patient Trauma Clinics Senior Nurse &
Management briefings. Methods of supplying
prophylaxis determined
August 2012 Design of patient completed new risk assessment form and analysis tools
Demonstration of tool to senior departmental staff
July 2012 Scoping review of literature, current guidelines and available risk assessment tools
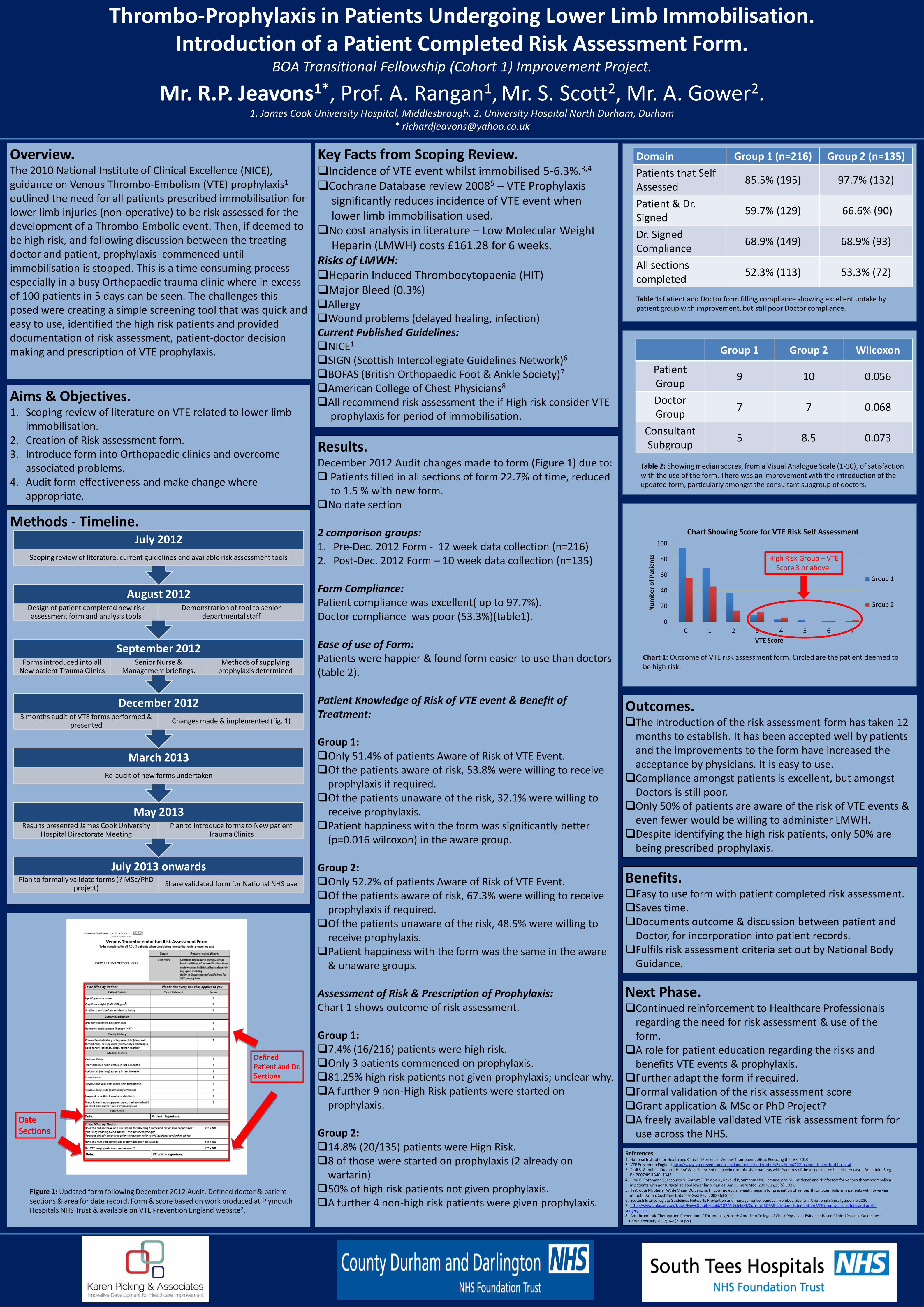
Figure 1: Updated form following December 2012 Audit. Defined doctor & patient sections & area for date record. Form & score based on work produced at Plymouth Hospitals NHS Trust & available on VTE Prevention England website2.
Results. December 2012 Audit changes made to form (Figure 1) due to: Patients filled in all sections of form 22.7% of time, reduced to 1.5 % with new form. No date section 2 comparison groups: 1. Pre-Dec. 2012 Form - 12 week data collection (n=216) 2. Post-Dec. 2012 Form – 10 week data collection (n=135) Form Compliance: Patient compliance was excellent( up to 97.7%). Doctor compliance was poor (53.3%)(table1). Ease of use of Form: Patients were happier & found form easier to use than doctors (table 2). Patient Knowledge of Risk of VTE event & Benefit of Treatment: Group 1: Only 51.4% of patients Aware of Risk of VTE Event. Of the patients aware of risk, 53.8% were willing to receive prophylaxis if required. Of the patients unaware of the risk, 32.1% were willing to receive prophylaxis. Patient happiness with the form was significantly better (p=0.016 wilcoxon) in the aware group. Group 2: Only 52.2% of patients Aware of Risk of VTE Event. Of the patients aware of risk, 67.3% were willing to receive prophylaxis if required. Of the patients unaware of the risk, 48.5% were willing to receive prophylaxis. Patient happiness with the form was the same in the aware & unaware groups. Assessment of Risk & Prescription of Prophylaxis: Chart 1 shows outcome of risk assessment. Group 1: 7.4% (16/216) patients were high risk. Only 3 patients commenced on prophylaxis. 81.25% high risk patients not given prophylaxis; unclear why. A further 9 non-High Risk patients were started on prophylaxis. Group 2: 14.8% (20/135) patients were High Risk. 8 of those were started on prophylaxis (2 already on warfarin) 50% of high risk patients not given prophylaxis. A further 4 non-high risk patients were given prophylaxis.
0
20
40
60
80
100
0 1 2 3 4 5 6 7
Num
ber o
f Pat
ient
s
VTE Score
Chart Showing Score for VTE Risk Self Assessment
Group 1
Group 2
High Risk Group – VTE Score 3 or above.
Domain Group 1 (n=216) Group 2 (n=135) Patients that Self Assessed 85.5% (195) 97.7% (132)
Patient & Dr. Signed 59.7% (129) 66.6% (90)
Dr. Signed Compliance 68.9% (149) 68.9% (93)
All sections completed 52.3% (113) 53.3% (72)
Group 1 Group 2 Wilcoxon
Patient Group 9 10 0.056
Doctor Group 7 7 0.068
Consultant Subgroup 5 8.5 0.073
Table 1: Patient and Doctor form filling compliance showing excellent uptake by patient group with improvement, but still poor Doctor compliance.
Chart 1: Outcome of VTE risk assessment form. Circled are the patient deemed to be high risk..
Table 2: Showing median scores, from a Visual Analogue Scale (1-10), of satisfaction with the use of the form. There was an improvement with the introduction of the updated form, particularly amongst the consultant subgroup of doctors.
Background
Patient Reported Outcome Measures (PROMS) are
increasingly being used to assess the functional outcome
following hip and knee replacement surgery. According to
North East Quality Observatory System (NEQOS), North
Tees and Hartlepool NHS Foundation Trust during
2011/2012 has been identified as Alert (probability of
significant difference 95% or more i.e. 95% chance that the
health gain is less than all organisations in England) on
EQ-5D generic health.
Aim
Stage 1: To undertake an audit and to identify the
demographic, surgical and implant related variables
associated with the poor functional outcome in terms of
generic health gain pertaining to hip replacement surgery in
our institution in 2011/2012.
Stage 2: To plan and evaluate service improvement if
needed by implementing a quality improvement project.
while understanding the principles of leadership techniques
learned from the numerous BOA training workshops.
Materials and Methods
Database from the clinical governance department was
made available to identify patients .The demographic,
surgical and implant related variables available from the
database were cross checked with the medical notes of the
patients who scored negative or revealed no change in
generic health gain(EQ-5D VAS).
We were able to identify a number of clinically important
operative variables (primary or revision arthroplasty
indication for revision particularly metal on metal( MoM)
revision, lead surgeon grade, consultant in charge, type of
prosthesis, from the database as well as the medical notes.
We also looked at the last orthopaedic clinic letter where
the patients reported satisfactory or non satisfactory
outcome following the index surgery.
Results
The results of the audit showed
•No single surgeon or prosthesis were outlier
•Six different primary total hip replacement prosthesis were
used
• Health gain ( post op – pre op EQ-VAS score) was low as
compared to National average.
• 82 % primary and revision patients satisfied
• Coding for four cases was inaccurate.
• Metal on metal revisions contributed to low gain.
Patient related outcome measures (PROMs)
in THR patients R Maheshwari, NJ Cooke
North Tees & Hartlepool NHS trust
Orthopaedic transitional fellowship : Cohort-1
Progress to date
Quality improvement project was implemented by
• By providing more education to patients regarding the
understanding of PROMs questionnaire and how to fill it in the
pre assessment clinics.
• Regular PROMs meeting with in the department
• Identifying Lead clinician and nurse for PROMs
• Improvement in Coding
• PROMs questionnaire copy to be kept in pt’s medical notes.
• Discussion in the departmental meeting regarding
procurement of the various hip prosthesis
Benefits
• Increased staff morale and satisfaction received through
feedback
• Enhanced patient experience and satisfaction
• Improved patient care
• Efficiency saving by reducing the number of type of primary
hip replacement prosthesis used.
Discussion & My leadership Journey
I undertook the task of performing this project by taking a
leadership role by taking initiation to create a team, delegating
tasks to the team members. During the project I had to act as a
team leader and manage the team of varied skills and
experience. My team comprised of junior doctor, nurse
practitioner, quality analyst, theatre coordinator, physiotherapist
and medical secretaries. I began the project with ‘end in mind’
and conveyed team members the importance of ‘think win-win’
(Covey, SR.1989).I explained to them that the project will lead
us to find improved ways of delivering patient care and will also
benefit our CV. Whilst conducting the project, I listened to
various ideas brought to my attention by different team
members. I regularly held team meetings in which I encouraged
and facilitated discussions and then helped to build consensus.
Throughout the project, I made sure that I was flexible; easy to
approach and open minded to my team suggestions. I
respected autonomy and provided regular feedback on the
strengths and weaknesses of the team members. This helped
me in strengthening my team playing leadership skills by
utilising resources effectively, developing a positive interaction
and cooperation between the team members.
During the project I took feedback from colleagues particularly
on team composition, team effectiveness, decision making,
communication, leadership capabilities, and development of the
innovative practice. The project has helped me enhance my
personal and professional attributes by allowing me to improve
my specific skills, particularly policy making, managing people,
negotiating and communication skills, improving trust, conflict
resolution and evaluation and also enabling trust in working
relationships.
References
1. North East Quality Observatory System 06 Aug 2012 v 1. ( April 2011-Dec 2011)
2. Covey, SR. (1989), The Seven habits of highly effective people, New York, Free Press

DISCUSSION: From the presented data, the
income could have potentially increased
significantly. An important finding in the coding
system is the number of codes for a given co-
morbidity. For example there are 12 different
codes for primary hypertension. This could
result in bias when recording the co-morbidity
code. Consultants should accurately record
allergy and co-morbidities when filling in waiting
list forms.
BOA Transitional Fellowship Leadership and Innovation Project
Service-Line Management (SLM)
Sherif M Isaac
University Hospitals Coventry and Warwickshire, Coventry, UK
Overview: SLM is a combination of trusted
management and business planning techniques
that can improve the way healthcare is delivered.
It was developed by Monitor to enable NHS
Trusts, to understand their performance and
organise their services in a way which benefits
patients and makes Trusts more efficient. One of
its tools is enabling clinicians to take the lead on
service development and drive improvements in
patient care. Monitor has set up seven steps
towards implementing SLM. Step three involves
ensuring sufficient quality of coding and data
collection. There was a wide variation in patients’
tariff undergoing primary hip/knee arthroplasty.
My role as a leader was to investigate the coding
process of these patients and create new
techniques or pathways to ensure quality in data
collection. This would increase income which
could be potentially used towards improving
department services and patient care.
WHAT IS NEXT: New pathways are being
developed to ensure all relevant patients’ data
is recorded. For example, the referring GPs are
currently encouraged to refer patients online
through the hospital website ensuring that all
relevant data is recorded. I am designing a
form with specific co-morbidities and allergy
conditions that have an impact on the coding
system. Patients will complete these forms
during their pre-assessment clinic visit.
METHODOLOGY: Initially, I initiated a meeting
with the Clinical Director and the department
service manger. We agreed on the project and
decided on who to involve as a team and a
schedule for the project. We discussed the
project benefits and potential obstacles and
solutions. An important obstacle was the financial
analysis. To support me with financial expertise a
private financial advisor was invited to undertake
the financial analysis. Then I arranged a meeting
with the hospital finance manager to go through
the project and what we need to achieve. A plan
was then designed allocating responsibilities for
different roles to the team members. A decision
was made to look at a two-months period (April
and May 2013). I familiarised myself with the
appropriate codes for NHS patients (ICD10,
OPCS, HRG).
Data extraction and analysis: I was presented
with all the patients that underwent hip/knee
arthroplasty with their codes. I extracted the
relevant information regarding population,
intervention, the caring consultant and co-
morbidities (recorded and unrecorded) by
reviewing the medical notes.
RESULTS: There were 139 patients recruited
during the reviewed period, 71 men and 68
women. Sixty-six and seventy-three patients
underwent total hip and knee arthroplasty
respectively. There was a wide variation in the
tariff received for the same procedure even with
the same co-morbidities. Table one shows the
inaccuracy in the coding of these patients.
There was a positive co-relation between the
patient age and sex and the recorded co-
morbidity code, the older the patient and being
a male, the more inaccuracy in the recorded co-
morbidity code. There was a co-relation
between the caring consultant and the recorded
codes. There was a deficiency recording allergy
By appropriately recoding the patients cases,
over £250,000 income could be have been
received by the hospital.
The data was analysed to check if the correct
tariff has been paid for these patients.
Number Correctly coded Incorrectly coded
THA 66 (47.5%) 9 (14%) 57 (86%)
TKA 73 (52.5%) 8 (11%) 65 (89%)
Experience of Enhanced recovery programme for hip
and knee replacement patients
S Krishnan, J Miles
Royal National Orthopaedic Hospital, Stanmore
Orthopaedic Transitional Fellowship – Cohort 1
Background
My assigned quality improvement project was to facilitate the
implementation of ‘Enhanced Recovery Programme’ (ERP) for patients
undergoing elective hip and knee replacements at the RNOH, Stanmore
and to use this as a learning experience to practice leadership skills learned
during the BOA transitional fellowship programme. The aim was to gain
experience in improving service quality in the NHS.
Aims
1. To identify deficiencies in the implementation of ERP and to implement
changes; thus obtaining a first hand experience in undertaking quality
improvement project.
2. To use this experience to understand the principles of leadership
techniques learned from the numerous BOA training workshops as well as
the online learning modules of Teeside University and the Chartered
Management Institute.
Project Methodology
Stage 1: Observe the practice of enhanced recovery programme and
assess it’s effectiveness in delivering reduced length of stay for patients
undergoing primary hip and knee replacements. This is done by comparing
the length of stay post-ERP (LOS Post-ERP) implementation with the LOS,
in a comparable group of patients, before the implementation of ERP (LOS
Pre-ERP). Patients with ASA Grades 1 and 2 were considered as the
comparable group.
Stage 2: Identify potential areas of service quality improvement and use the
acquired leadership and management skills to influence the system thereby
implementing the changes and produce a positive outcome.
Progress to date
An audit on the LOS for ERP patients was conducted and this was
compared with the historical data on LOS for comparable patients. A
comparison was also made with the LOS results reported by other centres
in the UK who have successfully implemented the ERP.
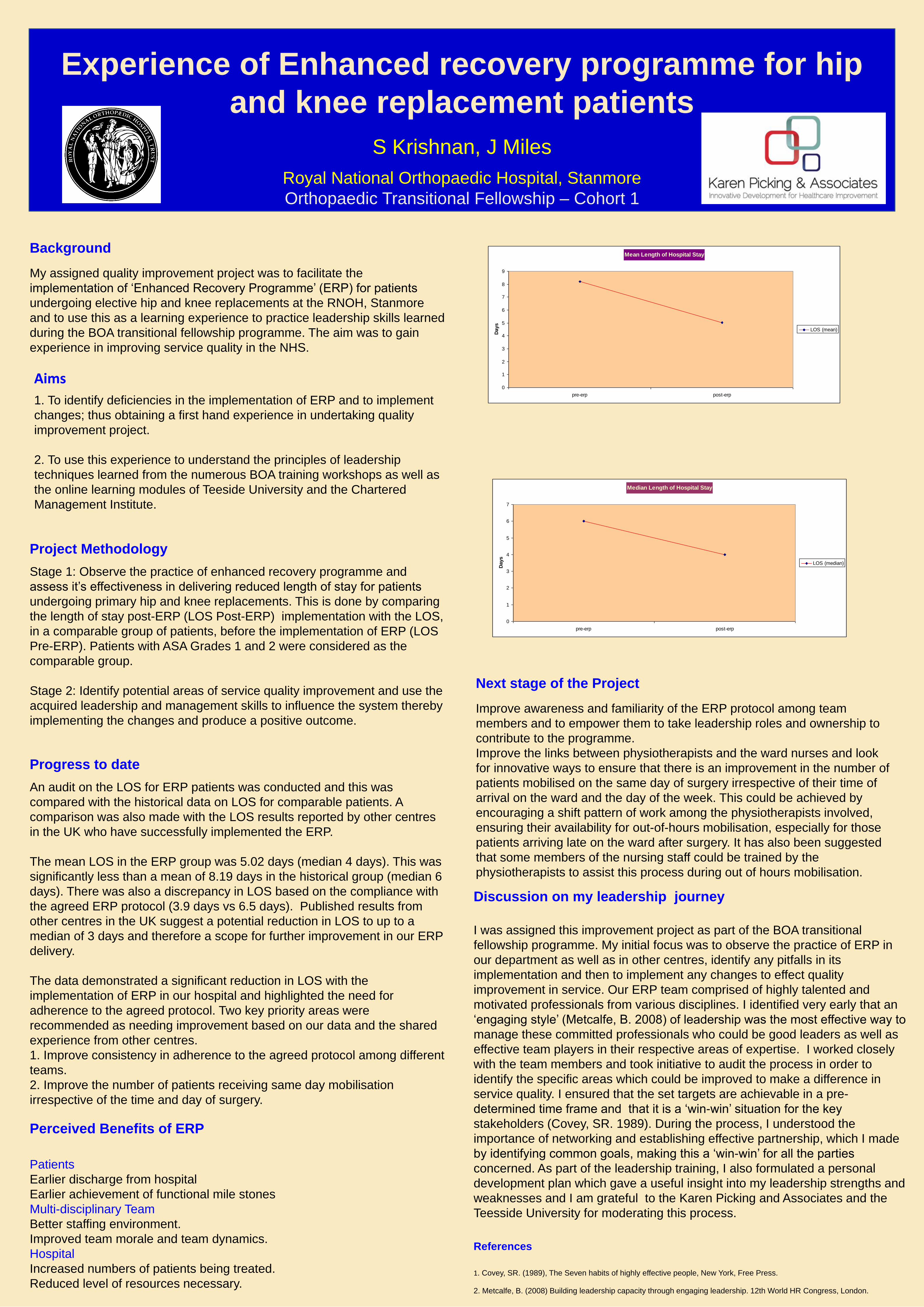
The mean LOS in the ERP group was 5.02 days (median 4 days). This was
significantly less than a mean of 8.19 days in the historical group (median 6
days). There was also a discrepancy in LOS based on the compliance with
the agreed ERP protocol (3.9 days vs 6.5 days). Published results from
other centres in the UK suggest a potential reduction in LOS to up to a
median of 3 days and therefore a scope for further improvement in our ERP
delivery.
The data demonstrated a significant reduction in LOS with the
implementation of ERP in our hospital and highlighted the need for
adherence to the agreed protocol. Two key priority areas were
recommended as needing improvement based on our data and the shared
experience from other centres.
1. Improve consistency in adherence to the agreed protocol among different
teams.
2. Improve the number of patients receiving same day mobilisation
irrespective of the time and day of surgery.
Next stage of the Project
Improve awareness and familiarity of the ERP protocol among team
members and to empower them to take leadership roles and ownership to
contribute to the programme.
Improve the links between physiotherapists and the ward nurses and look
for innovative ways to ensure that there is an improvement in the number of
patients mobilised on the same day of surgery irrespective of their time of
arrival on the ward and the day of the week. This could be achieved by
encouraging a shift pattern of work among the physiotherapists involved,
ensuring their availability for out-of-hours mobilisation, especially for those
patients arriving late on the ward after surgery. It has also been suggested
that some members of the nursing staff could be trained by the
physiotherapists to assist this process during out of hours mobilisation.
References
1. Covey, SR. (1989), The Seven habits of highly effective people, New York, Free Press.
2. Metcalfe, B. (2008) Building leadership capacity through engaging leadership. 12th World HR Congress, London.
Mean Length of Hospital Stay
0
1
2
3
4
5
6
7
8
9
pre-erp post-erp
Days
LOS (mean)
Median Length of Hospital Stay
0
1
2
3
4
5
6
7
pre-erp post-erp
Days
LOS (median)
Discussion on my leadership journey
I was assigned this improvement project as part of the BOA transitional
fellowship programme. My initial focus was to observe the practice of ERP in
our department as well as in other centres, identify any pitfalls in its
implementation and then to implement any changes to effect quality
improvement in service. Our ERP team comprised of highly talented and
motivated professionals from various disciplines. I identified very early that an
‘engaging style’ (Metcalfe, B. 2008) of leadership was the most effective way to
manage these committed professionals who could be good leaders as well as
effective team players in their respective areas of expertise. I worked closely
with the team members and took initiative to audit the process in order to
identify the specific areas which could be improved to make a difference in
service quality. I ensured that the set targets are achievable in a pre-
determined time frame and that it is a ‘win-win’ situation for the key
stakeholders (Covey, SR. 1989). During the process, I understood the
importance of networking and establishing effective partnership, which I made
by identifying common goals, making this a ‘win-win’ for all the parties
concerned. As part of the leadership training, I also formulated a personal
development plan which gave a useful insight into my leadership strengths and
weaknesses and I am grateful to the Karen Picking and Associates and the
Teesside University for moderating this process.
Perceived Benefits of ERP
Patients
Earlier discharge from hospital
Earlier achievement of functional mile stones
Multi-disciplinary Team
Better staffing environment.
Improved team morale and team dynamics.
Hospital
Increased numbers of patients being treated.
Reduced level of resources necessary.
Transitional Fellowship Quality Improvement ProjectImproving Multidisciplinary Care for Children with
Cerebral Palsy undergoing Botox Injections
Multidisciplinary Quality Improvement Team:T Nunn (BOA Transitional Fellow)D Lawniczak (Paediatric Fellow)J Whitaker (Surgical List Coordinator)D Smith (Specialist Children’s Physiotherapist)H Hughes (Specialist Children’s Physiotherapist)K Wardle (Specialist Children’s Physiotherapist)P Robins (Senior Orthotist)H Cain (Outpatient Clinic Manager)J Tansley (Outpatient Manager)E Smith (Quality Improvement Manager)Mr and Mrs Haslam (Patient/Parent representatives)Mr AG Davies (Paediatric Orthopaedic Surgeon)
Problems identified:
Children with CP were not receiving timely physiotherapy in a coordinated manner following Botox therapy.
This was due to :
1. Therapists were unaware that their patients were planned for Botox injection and were not informed of the
surgery date
2. Therapists were unaware which muscles were injected and what the treatment goals were
Background facts
• Botox injection is used in Cerebral Palsy (CP) to reduce abnormal muscle tone
• At Sheffield Children’s Hospital it is given as a guided injection performed under general anaesthesia
• Maximal effect is seen at 7-10 days post injection and effects wear off by 3 months
• Its use must be coordinated with a structured, targeted, goal focused physiotherapy and orthotic regime
• NICE guidance 2012 no.145 states ‘following Botulinum toxin type A administration an adapted physical
therapy programme is an essential component of management’
• In our Trust, failure to coordinate care potentially exposes children to a wasted procedure costing at least
£1,800/case
• We treat 115 patients per year with Botox from a wide geographical catchment area
Change Methods:
The multidisciplinary team met twice a month
over a 4 month period. Using the Trust’s
Microsystems Management tools we:
• Gathered baseline data
• Defined goals and specific aims
• Mapped out patient pathways
• Identified change ideas
• Formed an implementation strategy
Other benefits and future plans:• The identification of the relevant therapists and the Orthotic / Outpatient clinic coordination has been rolled out to include all Orthopaedic patients• In the long-term the use of the PAS system will store therapist details• The setting up of a dedicated Botox list allowing better scheduling for surgery is planned• Botox list will be run by an extended scope Physiotherapy practitioner with cost saving implications. A business case has been submitted to Trust Management
Further implementations:• A formal multidisciplinary departmental launch into the 2nd phase of the plan occurred on 25/09/2013, review of this is planned for January 2014.
Benefits:
1. Children have received treatment in a more coordinated, timely manner in accordance with NICE guidance
2. There has been an improved working relationship between members of the multidisciplinary team which we hope will successfully launch phase II
3. As Botox is ineffective without goal focussed physio, an uplift of the performance to pilot levels is expected to save approximately £59,000/yr in wasted procedures
Specific Aims:
• Ensure Therapists are informed of the planned Botox intervention (>90%)
• Therapists are informed of muscle groups injected (>90%)
• Therapists informed of the specific goals of the procedure (>90%)
• Patients receive their physiotherapy within 15 days of Botox (>90%)
• Targets will be reviewed every 6 months and increased accordingly
Authors: T.Nunn, J.Whitaker, D.Smith, P.Robins, H.Hughes, H.Cain, K.Wardle, D.Lawniczak, E.Smith, A.Davies Contact: [email protected]
Change initiatives + (progress to date):
• Outpatient reception clerks identify patients physiotherapist name & base, this information goes onto new theatre booking sheet and onto operation list (done)
• Patient receives a new Botox information leaflet (draft written)
• Copy of booking letter sent to Therapists. Orthopaedic Waiting List Coordinator sends out notification of surgery date to Physiotherapists using nhs.net email (done)
• Surgeon completes a standardised Botox proforma and discharge summary. Copies sent to Physio/OT as necessary (done)
• Orthotic outpatients if needed is arranged by Day Surgery and booked to coincide with clinical review by Outpatient Clinic Manager (done)
• Feedback process put in place from patients and Therapists to Surgical team (done)
Implementation Strategy:
• Phase I over 6 months (pilot of
one Consultant team’s practice)
• Phase II (Launch and rollout to
other Consultant Practitioners in
the department)
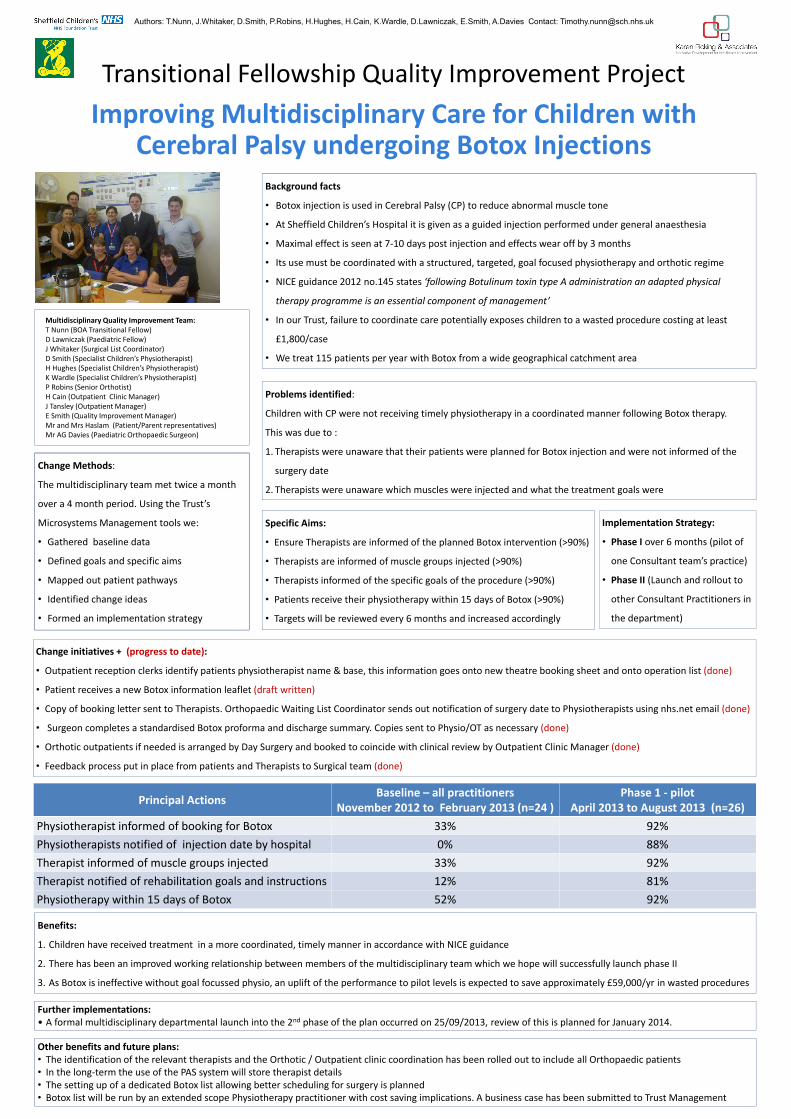
Principal Actions Baseline – all practitionersNovember 2012 to February 2013 (n=24 )
Phase 1 - pilotApril 2013 to August 2013 (n=26)
Physiotherapist informed of booking for Botox 33% 92%Physiotherapists notified of injection date by hospital 0% 88%Therapist informed of muscle groups injected 33% 92%Therapist notified of rehabilitation goals and instructions 12% 81%Physiotherapy within 15 days of Botox 52% 92%