Embed Size (px)
Citation preview

AN APPROACH TO THE ANEMIC PATIENT
Martin H. Ellis MD
Meir Hospital
2007

CASE PRESENTATION
• 67 y.o.male
• Chronic Lymphocytic leukemia for 4 years
• 1 week of weakness and dyspnea
6 mo agoNow
Wbc60 00072 000
Hb14.2 g/dL6.8 g/dL
Platelets192 K178 K
LAB DATA

Classification of anemia
• Etiologic– Decreased production– Increased destruction– Blood loss
• Morphologic– Microcytic hypochromic– Normocytic normochromic– Macrocytic

Approaching the diagnosis:First impressions
• Obvious clinical problems– Serious illness, overt bleeding
• Remainder of CBC– wbc, platelets
• MCV

Approaching the diagnosis:Isolated anemia, MCV low
• Iron deficiency– Elevated red cell distribution width
• Thalassemia– Normal red cell distribution width
• Anemia of chronic disease
• Lead poisoning

Approaching the diagnosis:Isolated anemia, MCV high
• B12, folate levels
• TSH
• Liver function tests
• Hemolytic parameters
• Consider bone marrow disorders

Approaching the diagnosis:Isolated anemia, MCV normal
• Mixed nutritional deficiencies– Dimorphic picture on smear
• Hemolysis
• Bone marrow disorders
• Anemia of chronic disease
• Chronic renal failure
• Acute bleeding

Approaching the diagnosis:Anemia with other cytopenias
• BM failure– Severe B12/FA deficiency– Aplastic anemia
• BM infiltration– Malignancies– Infections– Storage diseases
• Hypersplenism

BACK TO THE PATIENT…
• Background of CLL
• “Sudden” decrease in hemoglobin– Differential diagnosis
• Hemorrhage• Decreased production• Hemolysis

Aplastic anemia
• Pancytopenia with bone marrow hypocellularity
• Etiology:– Idiopathic – immune - T cell mediated– Constitutional (Fanconi anemia)– Radiation– Chemicals (benzene)– Drugs (cytotoxics, chloramphenicol, etc)– Infections (seronegative hepatitis, EBV)– Transfusion associated graft versus host disease

Aplastic anemia: diagnosis
• Clinical features– Abrupt or slow onset– Bleeding and anemia symptoms & signs
• Laboratory features– Pancytopenia (neutrophils < 500/µL, retic count <1%
& platelets , 20 000 /µL = severe AA)– Hypocellular/acellular bone marrow biopsy

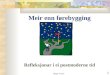
BONE MARROW BIOPSIES
NORMOCELLULARAPLASTIC

Aplastic anemia: treatment
• Bone marrow transplant– For young patients– Sibling donors preferred– 80% cure rate
• Immunosuppression– Antithymocyte globulin + cyclosporine ± steroids– 70-80% response rate

Pure red cell aplasia (PRCA)
• Anemia, reticulocytopenia, absent red cell precursors in bone marrow
• Congenital– Diamond Blackfan anemia
• Acquired– Transient (parvovirus B19 in patients with hemolytic
anemia)– Paraneoplasatic (thymoma, CLL)– SLE, rheumatoid arthritis– Pregnancy– Drugs – new entity: anti EPO antibodies PRCA!

Paroxysmal nocturnal hemoglobinuria (PNH)
• Acquired mutation in PIG-A gene occurs at the stem cell level
• Results in reduced/absent GPI-linked cell surface membrane proteins (CD 55, CD 59)
• Red cells have enhanced sensitivity to circulating complement
• Bone marrow failure, hemolysis and thrombosis occur

HEMOLYTIC ANEMIA:DEFINITION
• Anemia caused by premature destruction of red blood cells
• Lifespan of erythrocyte reduced from its normal 120 days
NOTE: hemolysis = hemolytic anemia

CLASSIFICATION
SITE OF DESTRUCTION
• Extravascular vs Intravascular
SITE OF ERYTHROCYTE ABNORMALITY
• Membrane
• Cytoplasm
• Hemoglobin
• Extracorpuscular

EXTRACORPUSCULAR CAUSES
Immune hemolytic anemia• Autoantibodies of IgG or IgM subtype
• IgG reacts best at 37 C = “warm” antibody
• Ig M reacts below body temperature
= “cold” antibody

WARM AUTOIMMUNE HEMOLYTIC ANEMIA
CLINICAL FEATURES
• Females > males
• Pallor
• Jaundice
• Splenomegaly
• Occasional fulminant hemolysis-cardiovascular collapse

WARM AUTOIMMUNE HEMOLYTIC ANEMIA
• Causes:– Idiopathic
- Malignancies (lymphoma, CLL, other)
- Drugs (alpha methyl dopa, penicillin, quinidine)
- Collagen-vascular diseases (SLE)
• Laboratory features– Extravascular hemolysis
– Smear shows microspherocytes, polychromatophilia, basophilic stippling

WARM AUTOIMMUNE HEMOLYTIC ANEMIA
DIAGNOSTIC TEST
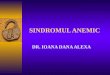
• Direct Coombs test
presence of antibody (or complement) on
RED CELLS
• Indirect Coombs test
presence of antibody in SERUM

DIRECT COOMBS TEST
Anti Human Globulin

Making the diagnosis in our patient
• Reticulocyte count– Beware… sometimes AIHA can occur without
reticulocytosis!!
• Biochemical parameters– LDH, indirect bilirubin, haptoglobin
• Direct Coombs test– Indirect Coombs less informative
• Bone marrow biopsy– Presence or absence of red cell precursors