Embed Size (px)
Citation preview

ORIGINAL ARTICLE
An assessment of iron overload in children treated for cancerand nonmalignant hematologic disorders
Jelena Rascon & Lina Rageliene & Sigita Stankeviciene &
Darius Palionis & Algirdas Edvardas Tamosiunas &
Nomeda Valeviciene & Tadas Zvirblis
Received: 29 November 2013 /Revised: 17 February 2014 /Accepted: 3 March 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Our goal was to assess the natural fate of ironoverload (IO) following transfusions of packed red blood cells(PRBCs) in children treated for cancer and nonmalignantdisorders according to the intensity level of their treatment.Sixty-six children were followed up from February 2010 toMarch 2013. The transfusion burden was compared betweenthree treatment intensity groups assigned according to theIntensity of Treatment Rating Scale 3.0 (ITR-3). IO wasassessed by serial measurements of serum ferritin (SF) (n=
66) and quantification of tissue iron by magnetic resonanceimaging (MRI) (n=12). Of the children studied, 36 % (24/66)received moderately intensive treatment (level 2), 21 % (14/66) received very intensive treatment (level 3), and 42 % (28/66) received the most intensive treatment (level 4). The num-ber of PRBC (p=0.016), the total transfused volume (p=0.026), and transfused volume adjusted to body weight (p=0.004) were significantly higher in the level 4 group. By themedian follow-up time of 35.5 months (range 8–133), 21–29 % of patients (including level 2 and level 3 children) hadSF >1,000 μg/l 1 year after cessation of transfusions. Theslowest decrease of SF was observed in the level 4 group.Initial MRI examination demonstrated either mild or moderateIO in the liver and spleen. Repetitive MRI showed significantimprovement in relaxation time between the initial andfollow-up MRI performances in the liver (5.9 vs. 8.6 ms, p=0.03) and the spleen (4.3 vs. 8.8 ms, p=0.03). Conclusion: IOdiminished over time, but in the level 4 patients, it wasdetectable for years after cessation of transfusions.
Keywords Cancer survivors . Iron overload . Treatmentintensity groups . Ferritin .MRI
AbbreviationsIO Iron overloadMRI Magnetic resonance imagingPRBC Packed red blood cellsSF Serum ferritinUIBC Unsaturated iron-binding capacity
Introduction
The current long-term survival rate of children suffering frommalignant disorders is approximately 80 % [11]. Significant
Communicated by David Nadal
J. Rascon (*) : L. Rageliene : S. StankevicieneCenter of Pediatric Oncology and Hematology, Children’s Hospital,Affiliate of Vilnius University Hospital Santariskiu Klinikos, Vilnius,Lithuaniae-mail: [email protected]
L. Ragelienee-mail: [email protected]
S. Stankevicienee-mail: [email protected]
J. Rascon : L. Rageliene :D. Palionis :A. E. Tamosiunas :N. ValevicieneFaculty of Medicine, Vilnius University, Vilnius, Lithuania
D. Palionise-mail: [email protected]
A. E. Tamosiunase-mail: [email protected]
N. Valevicienee-mail: [email protected]
D. Palionis :A. E. Tamosiunas :N. ValevicieneCenter of Radiology and Nuclear Medicine, Vilnius UniversityHospital Santariskiu Klinikos, Vilnius, Lithuania
T. ZvirblisHematology, Oncology and Transfusion Medicine Center, VilniusUniversity Hospital Santariskiu Klinikos, Vilnius, Lithuaniae-mail: [email protected]
Eur J PediatrDOI 10.1007/s00431-014-2295-5

progress in pediatric cancer survival rates is largely attribut-able to the intensification of chemotherapy and the appropriateuse of hematopoietic stem cell transplantation (HSCT). Anadequate transfusional support with packed red blood cells(PRBCs) is necessary in order to overcome anemic complica-tions during chemotherapy and transplant procedure. In clin-ical practice, the transfusional burden is rarely being traced.However, in view of the increasing cure rates, an awareness oflong-term sequelae of iatrogenic iron deposits in various or-gans and their potential impact on the quality of life is becom-ing more important.
The adverse effect of iron overload (IO) caused by chronictransfusions has been well recognized in thalassemia [27, 6,17] and myelodysplastic syndrome [20], but the number ofstudies exploring this issue in children treated for cancer orother nonmalignant disorders is still limited. Recently, Engand Fish assessed the iron accumulation in children treated foracute lymphoblastic leukemia and demonstrated greater trans-fusion demand in high-risk patients compared to the standardrisk [10]. Subsequent studies, which included a broad spec-trum of pediatric malignancies, revealed a correlation betweenthe intensity of treatment and the need for PRBC as well as thelevel of accumulated iron [25, 21]. A consensus opinion arosefrom the aforementioned analyses that there is a need toquantify the number of transfused PRBC and to monitoriatrogenic iron deposition.
Studies that followed the accumulated IO over time foundserum ferritin (SF) to remain elevated for years after thecompletion of chemotherapy [13, 12]. Along with the abnor-mal ferritin level, excessive iron deposition in the liver wasobserved by Halonen et al. who inspected liver biopsy spec-imens for intrahepatic iron [12]. Jastaniah et al. [13] usedsuperconducting quantum interference devices (SQUID) forthe same purposes. Both methods appeared to be reliable toprove iron accumulation in the liver. However, these tech-niques have limitations to quantifying intrahepatic iron rou-tinely: a liver biopsy is an invasive procedure, while SQUIDdevices are available only in a very limited number of centers.Recently, magnetic resonance imaging (MRI) was demon-strated to be sensitive, noninvasive, and widely available toassess iron stores in the liver and myocardium [18, 23, 8].
In our study, we aimed to assess the natural fate of IO inchildren treated for cancer and nonmalignant disorders otherthan thalassemia according to the intensity level of treatment.Changes in the excess level of iron were assessed by serialmeasurements of serum iron parameters and parallel quantifica-tion of liver and cardiac iron deposits by means of MRI testing.
Patients and methods
The longitudinal observational study was initiated onFebruary 1, 2010. The included patients were followed up
prospectively until March 1, 2013. The research project wasconducted in accordance with Good Clinical Practice. Thestudy design was approved by the Institutional Review Boardand Ethics Committee. Written informed consent was obtain-ed from parents or legal guardians of all the children prior totheir enrollment in the study.
During the study period, 66 children up to the age of 18,who had completed their treatment and were available forassessment on an outpatient basis, were recruited. At leastone PRBC transfusion was required to be included in thestudy. Previous chelation therapy was assumed as exclusioncriteria. No iron removal attempt was undertaken by patientsduring the study period.
Demographic data (i.e., age, gender) and clinical charac-teristics (i.e., diagnosis, type of treatment, body weight, num-ber of PRBC, the total transfused volume) as well as values ofSF, serum iron, and unsaturated iron-binding capacity (UIBC)were retrieved from laboratory databases and patient records.A treatment intensity level was assigned according to theIntensity of Treatment Rating Scale version 3.0 (ITR-3) [14].
In order to monitor the kinetics of iron deposits, SF, serumiron, and UIBC were initially assessed at the time of recruit-ment. Subsequently, only ferritin was measured during regularpatient visits. According to the study design, venous blood forresearch purposes was obtained only if the patient had centralvenous access. If not, the study variables could be measuredonly in case other clinically relevant analytics had to beobtained from the venous blood at the day of visit.
SF level was measured using an “electrochemiluminescenceimmunoassay” (ECLIA) (Cobas E 411 Elecsys 1010; RocheDiagnostics GmbH, Manheim, Germany). The level of serumiron was analyzed by a colorimetric assay with FerroZine(Cobas Integra 700; Roche Diagnostics GmbH, Manheim,Germany). UIBC was analyzed using colorimetric assay directdetermination with FerroZine (Cobas Integra 700; RocheDiagnostics GmbH, Manheim, Germany).
The blood center of our institution manufacturedleukodepleted PRBC using apheresis and an automated wholeblood processing system pursuant to local requirements thatdefined target hematocrit level as 50–70 %. The total ironburden was calculated using the formulation described byCohen et al. [7]: Iron transfused (mg)=Volume transfused×Hematocrit (Hct)×1.08, assumingmean empiric hematocrit tobe 60 %. Projected transfused iron was adjusted to the recip-ient body weight measured at the time of the last PRBCtransfusion.
MRI methodology
Patients were prospectively evaluated using a 1.5-T MRI(Avanto, Siemens) during 2011–2013. Tissue IOwas assessedin a cohort of 12 randomly selected patients who could un-dergo MRI procedure without need for general anesthesia
Eur J Pediatr

(respiration and motion artifacts were not significant). TotalMRI procedure time ranged from 20 to 30 min.
Liver image acquisition for T2* evaluation was done with asingle 10-mm slice through the central part of the liver (in-cluding both lobes) at 12 different echo times (TE 0.99–16.5ms) in transversal plane. Each image was acquired duringan 11–13-s single breath hold using a dedicated gradient echosequence (repetition time 200 ms, flip angle 20, matrix 128×128 pixels, field of view 40 cm). The same sequence was usedfor the spleen in transversal plane. For evaluation of myocar-dial T2*, a short-axis mid-ventricular slice was acquired ateight separate echo times (TE 2.59–18.2 ms) with dedicatedgradient echo sequence (flip angle 20, matrix 256×128 pixels,field of view 40 cm).
T2* time was calculated from gradient echo images usingCMRtools 2010 (©Cardiovascular Imaging Solutions). Car-diac T2* was evaluated from the intraventricular septumregion (represents both ventricles) in short-axis view [5].The left ventricle ejection fraction was evaluated from short-axis images using Argus software (Siemens).
Statistical analysis
Descriptive statistics were used to describe demographic char-acteristics. A Mann-Whitney-Wilcoxon test was performed toevaluate differences between two independent groups. A com-parison between more than two groups was performed usinganalysis of variance (ANOVA). Differences between indepen-dent two qualitative data groups were evaluated by means ofchi-square test. Pearson correlation analysis was performed toevaluate relation between two variables. A two-sided p valueless than 0.05 was considered to be significant. Statisticalanalysis was performed using the Statistical Analysis System(SAS) package version 9.2.
Results
Sixty-six patients in total were evaluated. Within this group,56 % represented different types of leukemia (37/66), 36 % ofsolid tumors (24/66), and 8 % (5/66) of nonmalignant disor-ders following HSCT (during the study period there was notransfusion-free patients with nonmalignant disorders withoutHSCT) (Table 1). Thirty-six percent of children (24/66) re-ceived moderately intensive treatment (level 2), 21 % (14/66)received very intensive treatment (level 3), and 42 % (28/66)received the most intensive treatment (level 4). Twenty-onepatients (32 %) were grafted with either autologous or alloge-neic hematopoietic stem cells. These children were assignedto the most intensive treatment level according to the defini-tion [14].
There was no significant difference between treatmentintensity groups in terms of the patients’ ages (p=0.058), the
time elapsed from the last PRBC transfusion, and the first SFmeasurement (p=0.333) and the follow-up period (p=0.275).
An assessment of the transfusion burden revealed that thechildren treated in the most intensive way had the highestPRBC demand. Comparative analysis of the included vari-ables between three treatment intensity groups (level 4 to level3 to level 2, Table 1) showed that the number of transfusedPRBC units (median 21.5 vs. 16 vs. 8, respectively, p=0.016),the total transfused volume (median 4,606.5 vs. 3,501 vs.1,691, respectively, p=0.026), and the transfused PRBC vol-ume adjusted to recipient body weight (median 159.6 vs. 117vs. 87.3, respectively, p=0.004) were significantly superiorfor level 4. This was translated into the highest projected ironburden (median 3,233.8 vs. 2,453.7 vs. 1,187.1, respectively,p=0.026) and iron load adjusted for body weight (median105.7 vs. 79.6 vs. 61.3, respectively, p=0.005).
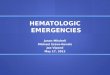
An initial evaluation of iron parameters at the time ofenrollment into the study demonstrated SF to be highly ele-vated in all three groups. The ferritin level was significantlyhigher in the level 4 group as compared to the level 3 and level2 groups (median 1,071.8 vs. 810 vs. 401.5, respectively, p=0.008). Measurements of serum iron and UIBC at the sametime point showed that both of the markers exceeded thenormal range only in the level 4 group (Table 1). The differ-ence between the three treatment intensity groups was notsignificant for either serum iron (p=0.363) or for UIBC (p=0.402). Nevertheless, a higher number of PRBC transfusionscorrelated with a higher level of SF and serum iron (r=0.3944,p=0.0009, and r=0.3280, p=0.0244, respectively) and lowerUIBC level (r=−0.3723, p=0.0009) (Fig. 1).
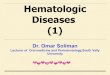
Serial measurements of SF showed a gradual decrease ofhyperferritinemia over time. Median ferritin value becamelower than 1,000 μg/l approximately after 1 year of follow-up (Fig. 2). Twenty-nine percent of children (8/28) in the level4 group had SF level over 1,000 μg/l following 1 year aftercessation of PRBC transfusions as compared to 21% (3/14) inthe level 3 and 21% (5/24) in the level 2 groups. After 2 yearsof follow-up, hyperferritinemia over 1,000 μg/l was found in4 of 28 children (14 %) in the level 4 group and in 1 of 14children (7%) in the level 3 group. In one adolescent treated inthe most intensive way sustained, hyperferritinemia>1,000 μg/l was still detectable 3 years after the lasttransfusion.
Tissue iron evaluation using MRI
Evaluation of tissue iron deposits using MRI T2* was per-formed in 12 patients. The median time from the last PRBCtransfusion to the first MRI was 11.7 months (ranging from 1to 44 months). In six children, an MRI scan was repeatedapproximately 1 year after the primary assessment with amedian time of 13.5 months (ranging from 12 to 23 months).MRI evaluation was performed in older children. Compared
Eur J Pediatr

Table 1 Clinical characteristics, transfusion burden, and iron status parameters
Total (n=66) Treatment intensity level
Level 2 (n=24) Level 3 (n=14) Level 4 (n=28) p value
Diagnoses
ALLa (total) 30 17 8 5
SR 10 10
IR 14 7 7
HR 4 1 3
Relapse 2 2
AML 6 6
JMML 1 1
Non-Hodgkin lymphoma 7 6 1
Hodgkin lymphoma 3 3
Wilms’ tumor 2 1 1
Neuroblastoma 3 3
Osteosarcoma 2 2
Ewing sarcoma 4 4
Rhabdomyosarcoma 1 1
Adrenocortical carcinoma 1 1
Germ cell tumor 1 1
Nonmalignant disordersb 5 5
HSCT (total) 22 21
Autologous 11 11
Allogeneic 11 11
Age at diagnosis (years)
Median 7.6 4.0 11.5 7.9 0.058Range 0.1–16.8 0.7–15.0 2.6–15.2 0.1–16.8
Number of PRBC (units)
Median 13 8 16 21.5 0.016Range 1–144 1–22 2–48 1–144
Total volume of PRBC (ml)
Median 2,404 1,691 3,501 4,606.5 0.026Range 163–37,795 163–5,449 720–11,827 260–37,795
Transfused volume of PRBC per kg (ml/kg)
Median 110.7 87.3 117.0 159.6 0.004Range 4.1–899.9 4.1–181.3 42.4–394.2 7.4–899.9
Projected iron burden (mg)
Median 1,687.3 1,187.1 2,457.7 3,233.8 0.026Range 114.4–26,532.1 114.4–3,825.2 505.4–8,302.6 182.5–26,532.1
Adjusted iron burden per kg (mg/kg)
Median 76.7 61.3 79.6 105.7 0.005Range 2.9–631.7 2.9–127.2 31.6–276.8 5.2–631.7
Ferritin (normal range 4–327 μg/l)
Median 701.2 401.5 810.0 1,071.8 0.008Range 23.3–5,723.0 31.2–2,404.0 98.0–5,723.0 23.3–5,657.1
Serum iron (normal range 4.5–22.7 μmol/l)
Median 19.3 17.8 16.0 24.2 0.363Range 4.4–42.2 4.4–37.7 11.1–36.0 5.2–42.2
UIBC (normal range 20–66 μmol/l)
Median 25.7 30.4 26.7 15.2 0.402Range 02.–58.7 3.7–58.7 3.4–35.1 0.2–53.6
Eur J Pediatr

to the remaining non-MRI cohort, the age at diagnosis of theMRI cohort was 10.3 versus 5.4 years, although the differencewas not significant (Table 2). The median age at the first MRIexamination was 12.9 years (ranging from 3.8 to 17 years).There was no significant difference in treatment intensitybetween MRI and non-MRI cohorts. However, transfusionintensity and subsequent iron burden differed significantlywhen comparing all included variables (Table 2).
Clinically significant myocardial IO was excluded in all 12patients validating T2* against cardiac function [3, 15]; in 11patients, myocardial T2* was >20 ms (17–52.2) with an ejec-tion fraction (EF) of >50 %, and one patient had mild myocar-dial iron overload (T2* value of 17 ms) with an EF of 54 %.Liver T2* values ranged from 1.9 to 22.9 ms, and according toDi Tucci et al. [9], two patients were suspected to have mod-erate (5–10 mg iron/g (dry liver)) and four patients mild (2–5 mg iron/g (dry liver)) IO in the liver. According to IronHealth Alliance T2* validation versus biopsies [26, 29], threepatients hadmoderate and sixmild (due to upper T2* thresholdat 11.4 ms) IO in the liver. Spleen initial T2* values rangedfrom 2.1 to 6.6 ms (no thresholds are available to determine IOdegree). Preliminary data suggest that spleen iron depositiondoes not directly correlate to liver overload: five patients hadlower initial spleen T2* and five higher compared to the liver.
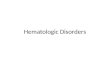
A follow-up MRI performed in six children revealed thatIO decreased both in the liver and the spleen (Fig. 3a). Medianrelaxation time compared between the initial MRI and follow-upMRI improved significantly in the liver (5.9 vs. 8.6 ms, p=0.03) and spleen (4.3 vs. 8.8 ms, p=0.03) (Fig. 3b). Myocar-dial tissue iron remained within normal range at initial andfollow-up imaging (29.0 vs. 31.6 ms, p=0.81).
Discussion
Our single-center study aimed to explore the natural fate ofiatrogenic IO in children treated for the most common types of
pediatric cancer and nonmalignant disorders. The main pointof interest was to evaluate whether the amount of accumulatediron differs depending on treatment intensity and what thenatural course of iron deposits is. Sixty-six children followedup through the study period were available for the evaluation.Of note, no patients suffering from brain tumors (most of themassignable to the level 3 or 4) were represented. Likewise, nopatients who received the least intensive treatment (level 1)were included in the study as none of them needed a PRBCtransfusion.
The largest group in our study was the one with the mostintensive level of treatment (i.e., level 4). Level 4 accountedfor 32 % (21/66) of the transplanted children. Along withcancer survivors, this group included the five recipients whounderwent an allogeneic transplant for nonmalignant disor-ders. On the other hand, the abovementioned absence ofneuro-oncology patients could also potentially contribute tothe predominance of the most intensively treated children.
As anticipated, the level 4 patients had the highest transfu-sion requirements. All evaluated variables of transfusion in-tensity and iron burden were significantly higher in the level 4group (Table 1). Our findings are consistent with previouslypublished data. Three retrospective studies reported that trans-fusion demand was associated with treatment intensity, andthe highest projected iron burdenwas found in children treatedin the most intensive way [21, 10, 25]. Evaluation of serumiron parameters showed significantly higher SF in the groupreceiving the most intensive treatment, though the values ofserum iron and UIBC did not differ significantly between thethree treatment groups. This could be explained by the meth-odology of quantification of serum iron and UIBC that isbased on the measurement of transferrin-bound iron [24].Some studies showed that UIBC is a sensitive marker forcalculation of empty iron stores [4] and could be consideredas an alternative to transferrin saturation [19]. We speculatedthat UIBC evaluation along with SF could be useful to provehyperferritinemia due to IO, but not due to an underlying
Table 1 (continued)
Total (n=66) Treatment intensity level
Level 2 (n=24) Level 3 (n=14) Level 4 (n=28) p value
Time from the last PRBC transfusion until the first ferritin assessment (months)
Median 9.6 13.9 9.95 3.2 0.333Range 0.2–84.2 2.7–77.8 0.2–27.9 0.5–84.2
Follow-up (months)
Median 35.5 37.5 35.5 36.5 0.275Range 8–133 8–94 15–60 8–133
a Twenty-one from 30 patients with ALLwere treated according to NOPHOALL-2008 protocol, six children were treated according to BFMALL-2000protocol, one child had Ph-positive ALL, and one patient was treated according to NHL protocol because of mature B cell leukemiabNonmalignant disorders consisted of SAA (n=2), DBA (n=1), Fanconi anemia (n=1), and MDS-RC (n=1). All five patients received allogeneicHSCT
Eur J Pediatr

inflammation or malignancy. Although we could not demon-strate the difference between serum iron and UIBC depending
on the treatment intensity level, a correlation between thenumber of transfused PRBC and all evaluated iron parameterswas found (Fig. 1).
Serial SF measurements over time showed thathyperferritinemia was decreasing gradually. The average lev-el of ferritin fell below 1,000 μg/l approximately 1 year afterthe cessation of transfusions. Interestingly, we found thatapproximately one fifth of patients who received less inten-sive treatment (21 % of children in each level 2 and level 3groups) was also heavily transfused and had severehyperferritinemia detectable 1 year after cessation of transfu-sions. This finding suggests that the transfusion historyshould be carefully traced in all children to define a cohortfor close monitoring of IO. In our study, the level 4 patientsshowed the slowest pattern of resolution of the accumulatediron; in one adolescent, an SF level over 1,000 μg/l wasdetected more than 3 years after the last PRBC transfusion.Slow resolution of hyperferritinemia could be related to thehigh initial SF (reflecting the degree of accumulated iron). Arecent study by Amid et al. demonstrated that the age atdiagnosis might affect the resolution of hyperferritinemia;greater change in body surface area was protective for thelong-lasting hyperferritinemia [2]. In other words, smallerchildren utilize the accumulated iron for their needs to grow.In our study, there was no age difference between the threecompared treatment groups, although some observations notreflected in this study also suggested that adolescents had aslower release of accumulated iron. The monitoring of tissueiron using MRI T2* showed a similar pattern of decrease ofiatrogenic iron deposits expressed as a significant improve-ment in the liver and splenic relaxation time 1 year after theinitial MRI T2* (Fig. 3).
In our study, tissue iron evaluation using MRI T2* wasperformed only in older children who could undergo the
Fig. 1 Relationship between iron parameters (a serum ferritin, b serumiron, c UIBC) and the number of transfused PRBC
Fig. 2 Kinetics of SF by serial assessment in the entire patient group (n=66). One cross represents one serum sample. One patient had several SFmeasurements
Eur J Pediatr

procedure without general anesthesia. The major reason forthis was our decision not to sedate small children solely forresearch purposes. This is the major limitation of our study aspatient selection for MRI evaluation was biased with regard toage. The second limitation is the small number of childrenassessed by MRI, especially for the second time. Despite agedifferences (although not statistically significant), there wasno difference in the treatment intensity level betweenMRI andnon-MRI cohorts. Surprisingly, the MRI cohort was moreintensively transfused and had a significantly greater ironburden and SF level (Table 2). The data published thus farhave explored the influence of age at the time of diagnosis onIO only retrospectively and are in dispute. In the analysis of amixed patient population, Ruccione et al. found that youngerage at diagnosis was significant for projected iron burden [25].
Eng and Fish analyzed only ALL patients and reported noinfluence of age on the amount of blood received [10]. Amidet al. found that age, weight, and body surface area correlatedwith the level of SF at the end of treatment, though only thetotal transfused volume was independently significant forhyperferritinemia [2]. In addition, this study demonstrated thatyounger patients who had a more pronounced change in bodysurface area were less likely to have high SF after the com-pletion of chemotherapy than older children. From clinicalobservations, it is well known that smaller children have amuch higher tolerance to low hemoglobin levels and thuscould require lesser transfusions than adolescents.
Depending on the validation system, between six and ninechildren from the MRI cohort had measurements of the liverT2* that indicated mild or moderate IO. Liver MRI results canbe compared to the liver biopsy. Three studies have confirmedthat the use of a relaxometry liver MRI and biopsy values wasstrongly correlated [3, 1, 28]. Myocardial T2* values of<20 ms are generally considered below the lower normalthreshold and are associated with a progressive and significantdecline in left ventricle ejection fraction (LVEF) and arrhyth-mias [15, 3]. We have detected mild myocardial IO in onepatient (with T2* value of 17 ms) and one had borderline T2*value of 20.6 ms, with EF >50 % for both patients. Data fromβ-thalassemia suggested that myocardial IO detectable byMRI was to be expected after at least 35 g of transfusionaliron that corresponded to nearly 200 PRBC units [30]. Thedegree of liver IO and SF seem did not correlate with myo-cardial IO [30, 8]. A lower transfusion burden in our studypopulation could justify normal myocardial T2* relaxationtime in 11 of 12 patients. In contrast to our results, othergroups did find excessive iron accumulation in cancer survi-vors. De Ville de Goyet et al. recently reported myocardial IOin 14 % of patients prospectively evaluated by MRI 1 yearafter treatment [8]. Interestingly, this study failed to find anassociation between myocardial T2* and transfused bloodvolume and SF, although such association could be provenfor the liver T2*. Lutz et al. [18] also found myocardial IO intwo of three cancer survivors who were heavily transfused.
In our study, we could demonstrate iron accumulation inthe spleen. Follow-up MRI examinations of both the liver andspleen after 1 year showed significant improvement in T2*relaxation indicating a reduction of iron stores (Fig. 3). How-ever, sustained IOwas still detectable in some patients. Recentstudies evaluated spleen IO importance along with liver mea-surements. Kolnagou et al. [16] presented a comparison ofiron load using MRI T2* and iron grading of stained biopsies,indicating that substantial but variable amounts of excessiveiron are stored in the spleen (0–40 %) in addition to those inthe liver. Spleen iron seems to be cleared faster than liver ironusing effective chelation protocols. Normalization of the bodyiron stores at an early age could maintain the spleen in near-normal capacity, and secondary effects such as cardiac and
Table 2 Characteristics of children who underwent tissue iron overloadevaluation usingMRI T2* technique (MRI cohort) and those who did not(non-MRI cohort)
MRI cohort Non-MRI cohort p valuen=12 n=54
Treatment intensity, n (%)
Level 2 3 (25) 21 (39) 0.157Level 3 1(8) 13 (24)
Level 4 8 (67) 20 (37)
Age at diagnosis (years)
Median 10.3 5.4 0.1249Range 2.0–16.0 0.1–16.8
Number of PRBC (units)
Median 28 12 0.0002Range 8–144 1–56
Total volume of PRBC (ml)
Median 6,623 2,926 0.0004Range 1,984–37,795 163–13,696
Transfused volume of PRBC per kg (ml/kg)
Median 200.6 106.1 0.0061Range 31.6–899.9 4.1–326.1
Projected iron burden (mg)
Median 4,649 1,442.6 0.0004Range 1,392.8–26,532.1 114.4–9,614.6
Adjusted iron burden per kg (mg/kg)
Median 142.5 74.2 0.0061Range 25.3–631.7 2.9–228.9
Ferritin (normal range 4–327 μg/l)
Median 2,021.5 586.9 0.0006Range 285.0–5,723.0 23.3–5,657.1
Serum iron (normal range 4.5–22.7 μmol/l)
Median 26.3 18.4 0.0034Range 21.1–42.2 4.4–34.1
UIBC (normal range 20–66 μmol/l)
Median 6.9 28.5 0.0014Range 2.5–35.1 02.–58.7
Eur J Pediatr

other complications could be avoided. Oshtrakh and col-leagues [22] reported preliminary data from a comparativestudy of human liver ferritin and spleen tissues from healthyindividuals and a patient with primary myelofibrosis usingMössbauer spectroscopy. The results obtained demonstratedthat the iron content in a patient’s spleen in the form of ironstorage proteins was about ten times higher than that in normaltissue. They reported that IO in the case of patient withprimary myelofibrosis may be related mainly to an increasein the ferritin content. Our initial data showed that spleen irondeposition does not correlate directly to liver overload, al-though more studies are needed to evaluate spleen IO corre-lation with ferritin and functional impact on the spleen. To ourknowledge, no threshold data are available at the moment todetermine normal and overloaded spleen parenchyma usingMRI scanning. More comparable studies are needed to estab-lish a reliable technique for IO diagnosis and its grade
evaluation as well as for the exact measurement of ironconcentration.
In summary, iatrogenic IO is most prominent in childrenwho received the most intensive level of treatment (i.e., thelevel 4 patients). However, up to one fifth of patients treatedless intensively is also exposed to numerous transfusions andexcessive iron accumulation. Sustained IO detectable as per-sistent hyperferritinemia and intraorganic MRI changes de-crease over time; though in heavily transfused children, ittakes years until SF decreases below 1,000 μg/l. These find-ings are important for future studies that should clarify if afinal clearance of the accumulated iron occurs or not. In caseof irreversible IO, there is a need to assess the contribution ofIO on late organ damage following cancer treatment. Thelong-term nature of iron deposits requires a special follow-up program of heavily transfused patients to prove the finalclearance or persistence of IO.
Fig. 3 Noninvasive evaluation ofiron overload using MRI T2*technique in the liver,myocardium, and spleen. MRI 1indicates initial MRI performed in12 patients andMRI 2 repetitiveimaging performed in six patientsafter 1 year. a Level of tissue irondeposits measured as relaxationtime in 12 patients. b Differencein median relaxation timebetween MRI 1 and MRI 2calculated for the six patients withpaired MRI (Wilcoxon test)
Eur J Pediatr

Acknowledgments The study was supported by a research grant fromNovartis. The grant was used to purchase biochemical diagnostics. Thefinancial support had no influence on study design, data collection,analysis, and interpretation on the writing of the report and on the decisionto submit the report for publication.
Conflict of interest The authors declare that the study does not containany potential conflicts of interest and financial and personal relationshipsthat might bias this work.
References
1. Alexopoulou E, Stripeli F, Baras P, Seimenis I, Kattamis A, Ladis V,Efstathopoulos E, Brountzos EN, Kelekis AD, Kelekis NL (2006) R2relaxometry withMRI for the quantification of tissue iron overload inbeta-thalassemic patients. J Magn Reson Imaging 23(2):163–170.doi:10.1002/jmri.20489
2. Amid A, Barrowman N, Vijenthira A, Lesser P, Mandel K, RamphalR (2013) Risk factors for hyperferritinemia secondary to red bloodcell transfusions in pediatric cancer patients. Pediatr Blood Cancer60(10):1671–1675. doi:10.1002/pbc.24629
3. Anderson LJ, Holden S, Davis B, Prescott E, Charrier CC, BunceNH, Firmin DN, Wonke B, Porter J, Walker JM, Pennell DJ (2001)Cardiovascular T2-star (T2*) magnetic resonance for the earlydiagnosis of myocardial iron overload. Eur Heart J 22(23):2171–2179
4. Asberg A, Thorstensen K, Mikkelsen G, Asberg AE (2013) Thediagnostic accuracy of unbound iron binding capacity (UIBC) as atest for empty iron stores. Scand J Clin Lab Invest 73(3):208–213.doi:10.3109/00365513.2013.765029
5. Carpenter JP, He T, Kirk P, Roughton M, Anderson LJ, de NoronhaSV, Sheppard MN, Porter JB, Walker JM, Wood JC, Galanello R,Forni G, Catani G, Matta G, Fucharoen S, Fleming A, House MJ,Black G, Firmin DN, St Pierre TG, Pennell DJ (2011) On T2*magnetic resonance and cardiac iron. Circulation 123(14):1519–1528. doi:10.1161/CIRCULATIONAHA.110.007641
6. Cianciulli P (2008) Treatment of iron overload in thalassemia. PediatrEndocrinol Rev 6(Suppl 1):208–213
7. Cohen AR, Glimm E, Porter JB (2008) Effect of transfusional ironintake on response to chelation therapy in beta-thalassemia major.Blood 111(2):583–587. doi:10.1182/blood-2007-08-109306
8. de Ville de Goyet M, Moniotte S, Robert A, Dupont S, Vermylen C,Veyckemans F, Brichard B (2013) Iron overload in children under-going cancer treatments. Pediatr Blood Cancer 60(12):1982–1987.doi:10.1002/pbc.24705
9. Di Tucci AA, Matta G, Deplano S, Gabbas A, Depau C, Derudas D,Caocci G, Agus A, Angelucci E (2008) Myocardial iron overloadassessment by T2* magnetic resonance imaging in adult transfusiondependent patients with acquired anemias. Haematologica 93(9):1385–1388. doi:10.3324/haematol.12759
10. Eng J, Fish JD (2011) Insidious iron burden in pediatric patients withacute lymphoblastic leukemia. Pediatr Blood Cancer 56(3):368–371.doi:10.1002/pbc.22851
11. Gatta G, Zigon G, Capocaccia R, Coebergh JW, Desandes E, KaatschP, Pastore G, Peris-Bonet R, Stiller CA (2009) Survival of Europeanchildren and young adults with cancer diagnosed 1995-2002. Eur JCancer 45(6):992–1005. doi:10.1016/j.ejca.2008.11.042
12. Halonen P, Mattila J, Suominen P, Ruuska T, Salo MK, MakipernaaA (2003) Iron overload in children who are treated for acute lympho-blastic leukemia estimated by liver siderosis and serum iron param-eters. Pediatrics 111(1):91–96
13. Jastaniah W, Harmatz P, Pakbaz Z, Fischer R, Vichinsky E, WaltersMC (2008) Transfusional iron burden and liver toxicity after bone
marrow transplantation for acute myelogenous leukemia and hemo-globinopathies. Pediatr Blood Cancer 50(2):319–324. doi:10.1002/pbc.21260
14. Kazak AE, Hocking MC, Ittenbach RF, Meadows AT, Hobbie W,DeRosa BW, Leahey A, Kersun L, Reilly A (2012) A revision of theintensity of treatment rating scale: classifying the intensity of pediat-ric cancer treatment. Pediatr BloodCancer 59(1):96–99. doi:10.1002/pbc.23320
15. Kirk P, Roughton M, Porter JB, Walker JM, Tanner MA, Patel J, WuD, Taylor J,WestwoodMA, Anderson LJ, Pennell DJ (2009) CardiacT2* magnetic resonance for prediction of cardiac complications inthalassemia major. Circulation 120(20):1961–1968. doi:10.1161/CIRCULATIONAHA.109.874487
16. Kolnagou A,Michaelides Y, Kontoghiorghe CN, Kontoghiorghes GJ(2013) The importance of spleen, spleen iron, and splenectomy fordetermining total body iron load, ferrikinetics, and iron toxicity inthalassemia major patients. Toxicol MechMethods 23(1):34–41. doi:10.3109/15376516.2012.735278
17. Kwiatkowski JL, Kim HY, Thompson AA, Quinn CT, Mueller BU,Odame I, Giardina PJ, Vichinsky EP, Boudreaux JM, Cohen AR,Porter JB, Coates T, Olivieri NF, Neufeld EJ (2012) Chelation useand iron burden inNorthAmerican andBritish thalassemia patients: areport from the Thalassemia Longitudinal Cohort. Blood 119(12):2746–2753. doi:10.1182/blood-2011-04-344507
18. Lutz K, von Komorowski G, Durken M, Engelhardt R, Dinter DJ(2008) Myocardial iron overload in transfusion-dependent pediatricpatients with acute leukemia. Pediatr Blood Cancer 51(5):691–693.doi:10.1002/pbc.21663
19. Murtagh LJ, Whiley M, Wilson S, Tran H, Bassett ML (2002)Unsaturated iron binding capacity and transferrin saturation areequally reliable in detection of HFE hemochromatosis. Am JGastroenterol 97(8):2093–2099. doi:10.1111/j.1572-0241.2002.05927.x
20. Neukirchen J, Fox F, Kundgen A, Nachtkamp K, Strupp C, Haas R,Germing U, Gattermann N (2012) Improved survival in MDS pa-tients receiving iron chelation therapy—a matched pair analysis of188 patients from the Dusseldorf MDS registry. Leuk Res 36(8):1067–1070. doi:10.1016/j.leukres.2012.04.006
21. Nottage K, Gurney JG, Smeltzer M, Castellanos M, Hudson MM,Hankins JS (2013) Trends in transfusion burden among long-termsurvivors of childhood hematological malignancies. LeukLymphoma 54(8):1719–1723. doi:10.3109/10428194.2012.750724
22. Oshtrakh MI, Alenkina IV, Vinogradov AV, Konstantinova TS,Kuzmann E, Semionkin VA (2013) Mossbauer spectroscopy of theiron cores in human liver ferritin, ferritin in normal human spleen andferritin in spleen from patient with primary myelofibrosis: prelimi-nary results of comparative analysis. Biometals 26(2):229–239. doi:10.1007/s10534-012-9602-2
23. Reddy KS, Eng J, Carlson C, Ginsberg J, Fish J (2011) Impact oftransfusional support for childhood cancer—peering behind the ironcurtain. Pediatr Blood Cancer 56:908
24. Roche DIA customer self-service portal. https://cssportal.roche.com/eld/lt/lt/DocumentResult/ResultList. Accessed 10 Aug 2013
25. Ruccione KS, Mudambi K, Sposto R, Fridey J, Ghazarossian S,Freyer DR (2012) Association of projected transfusional iron burdenwith treatment intensity in childhood cancer survivors. Pediatr BloodCancer 59(4):697–702. doi:10.1002/pbc.24046
26. St Pierre TG, Clark PR, Chua-anusorn W, Fleming AJ, Jeffrey GP,Olynyk JK, Pootrakul P, Robins E, Lindeman R (2005) Noninvasivemeasurement and imaging of liver iron concentrations using protonmagnetic resonance. Blood 105(2):855–861. doi:10.1182/blood-2004-01-0177
27. Taher AT, Musallam KM, Karimi M, Cappellini MD (2012)Contemporary approaches to treatment of beta-thalassemiaintermedia. Blood Rev 26(Suppl 1):S24–27. doi:10.1016/S0268-960X(12)70008-5
Eur J Pediatr

28. Voskaridou E, DouskouM, Terpos E, Papassotiriou I, StamoulakatouA, Ourailidis A, Loutradi A, Loukopoulos D (2004) Magnetic reso-nance imaging in the evaluation of iron overload in patients with betathalassaemia and sickle cell disease. Br J Haematol 126(5):736–742.doi:10.1111/j.1365-2141.2004.05104.x
29. Wood JC, Enriquez C, Ghugre N, Tyzka JM, Carson S, Nelson MD,Coates TD (2005) MRI R2 and R2* mapping accurately estimates
hepatic iron concentration in transfusion-dependent thalassemia andsickle cell disease patients. Blood 106(4):1460–1465. doi:10.1182/blood-2004-10-3982
30. Wood JC, Origa R, Agus A, Matta G, Coates TD, Galanello R(2008) Onset of cardiac iron loading in pediatric patients withthalassemia major. Haematologica 93(6):917–920. doi:10.3324/haematol.12513
Eur J Pediatr