Embed Size (px)
Citation preview

Journal of Research in Medical Sciences | February 2013 |89
Or
igin
al a
rt
icl
e An association of hyperglycemia with plasma malondialdehyde and atherogenic lipid risk factors in newly diagnosed Type 2 diabetic patients
Suchitra Mustur Manohar, Seshadri Reddy Vaikasuvu, Deepthi K, Alok Sachan1, Srinivasa Rao Pemmaraju Venkata Lakshmi NarasimhaDepartments of Biochemistry, 1Endocrinology, SV Institute of Medical Sciences, SVIMS University, Tirupati, Andra Pradesh, India
Background: Oxidative stress (OS) generated by hyperglycemia, is one of the major focuses of recent research related to diabetes mellitus. Studying associations between hyperglycemia, OS and atherogenic dyslipidemia (AD) is therefore important. Materials and Methods: Plasma was obtained form a total of 52 subjects with newly diagnosed Type 2 diabetes mellitus (T2DM) and 52 healthy controls to study associations between hyperglycemia, lipid risk factors for atherogenicity and malondialdehyde (MDA), a lipid peroxidation product. Ferric reducing ability of plasma (FRAP) was evaluated as a measure of total antioxidant capacity (TAC). Results: Diabetic patients had significantly higher (P < 0.05) plasma triglycerides (TG)), very‑low‑density lipoprotein cholesterol (VLDL‑C), TG to high‑density lipoprotein cholesterol ratio (TG/HDL‑C), atherogenic index (AI), and MDA. Whereas FRAP levels were depleted significantly in the patients compared to that of controls (P = 0.000). Pearson correlation analyses showed MDA correlates significantly with Fasting blood sugar (r = 0.39, P = 0.004), TG/HDL‑C (r = 0.45, P = 0.001), and AI (r = 0.40, P = 0.003), and a significant negative correlation with LDL‑C (r = ‑0.33, P = 0.019) which was lost upon nullifying the effect of FBS by partial correlation analysis (r = ‑0.28, P = 0.050). Receiver operating curve (ROC) analysis showed high Area under curve for TG/HDL‑C and AI (0.62; P = 0.03). Conclusion: Hyperglycemia of diabetes is associated with elevated levels of plasma MDA. This study suggests that TG/HDL‑C and AI may be particularly useful as atherogenic risk predictors in newly diagnosed patients with T2DM.
Key words: Atherogenic index, dyslipidemia, hyperglycemia, malondialdehyde, oxidative stress
Address for correspondence: Dr. Suchitra MM, Department of Biochemistry, SVIMS, Tirupati, Aandra Pradesh, India. E‑mail: [email protected]: 02‑12‑2011; Revised: 06‑01‑2013; Accepted: 23‑01‑2013
predictor than LDL.[10,11] Hermans et al., proposed atherogenic index of plasma (AIP) as a simple means to estimate atherogenic dyslipidemia and the residual cardiovascular risk in T2DM.[12]
Diabetes is usually accompanied by increased production of free radicals or impaired antioxidant defenses resulting in increased oxidative stress (OS) contributing to the development and progression of diabetes and its complications.[13] OS induced by Reactive Oxygen Species (ROS), generated by hyperglycemia, is one of the major focuses of recent research related to DM,[14] there are studies reporting increased levels of plasma malondialdehyde (MDA) as an indicator of elevated lipid damage.[15-17] In addition, dyslipidemia may also contribute to increase in OS.[18] Despite the occurrence of atherogenic dyslipidemia and OS in diabetes, to the best of our knowledge no study has compared the association among lipid risk factors of atherosclerosis, hyperglycemia, and OS in newly diagnosed T2DM. Therefore, the present study was taken up to address this issue. In this study, total antioxidant capacity (TAC) as ferric reducing ability of plasma (FRAP) has been assessed as an antioxidant marker. Smoking status, alcohol consumption, abnormal Body mass index (BMI),
INTRODUCTION
Being the prime cause of morbidity and mortality, cardiovascular disease (CVD) risk is great in diabetic patients,[1,2] with more than a 200% greater risk of CVDs than non-diabetic individuals.[3] India has a high prevalence of Type 2 diabetes mellitus (T2DM) and CVD risk associated with urbanization.[4] Dyslipidemia characterized by the elevation of plasma total cholesterol (TC), triglycerides (TG) and TG-rich very-low-density lipoprotein cholesterol (VLDL-C), reduced high-density lipoprotein cholesterol (HDL-C), and increased low-density lipoprotein cholesterol (LDL-C) contributes significantly to the excess risk of CVD.[5] Several studies have reported the possibility that newly addressed lipid profiles may be more useful than the traditional ones such as TC/HDL-C, TG/HDL-C and LDL-C/HDL-C ratio,[6-8] which are independently associated with insulin resistance and CVD risk prediction.[6] Furthermore, the Adult Treatment Panel (ATP-III) of the National Cholesterol Education Program has recommended using non-HDL-C (nHDL-C) in assessing CVD risk,[9] and was better explored in a diabetic cohort as a stronger
www.mui.ac.ir

Suchitra, et al.: Association of MDA with hyperglycemia in diabetes
Journal of Research in Medical Sciences| February 2013 | 90
and hypertension which may influence lipid status and OS are confounding factors, and their effect was nullified by conducting the study in newly diagnosed T2DM patients who were non-smokers, non-alcoholics, and normotensives with normal BMI, with the aim of studying whether increased OS is related to lipid risk factors of atherosclerosis.
MATERIALS AND METHODS
Patients and assessmentsThe present study recruited 52 (33 males and 19 females) newly diagnosed patients with T2DM from the outpatient clinic of the Endocrinology and Metabolism division of Sri Venkateswara Institute of Medical Sciences (SVIMS) from August 2009 to March 2010. Inclusion criteria were patients with fasting blood sugar (FBS) >126 mg/dl, and who were not receiving any treatment for the hyperglycemia. The criteria for exclusion were patients on antioxidant supplements and/or hypolipidemic agents, end-stage renal disease, active infection, pregnant and post-menopausal females, chronic or acute illnesses and patients suffering from endocrine disorders other than T2DM. Smokers, alcoholics, patients with abnormal BMI and hypertension were excluded to remove their confounding effect on dyslipidemia and OS. Fifty-two gender- and age-matched, healthy participants (38 males and 14 females) were enrolled as control group. The study was approved by the institutional ethical committee and informed consent was taken from the participants.
Overnight fasting venous blood samples were drawn from each participant in fluoride-containing anticoagulant tubes for blood glucose estimation and in heparinized tubes for the remaining parameters. The samples were processed by centrifugation at 3000 rpm to obtain plasma for immediate analysis or stored at ‑80°C until further analysis. Plasma levels of fasting glucose, uric acid, total cholesterol (TC), triacylglycerol (TG), and high-density lipoprotein (HDL-C) were determined by enzymatic colorimetric methods on Beckman Synchron CX9 Autoanalyzer using commercial kits. Since the TG level in all participants was lower than 400 mg/dl, VLDL was calculated as TG/5 and LDL as TC-HDL-C-TG/5 using Friedwald formula.[19] Various lipid risk factors of atherosclerosis, such as non-HDL-C (TC-HDL-C), molar ratios of TG/HDL-C, TC/HDL-C, LDL/HDL-C, and non-HDL-C/HDL-C were calculated from the lipid profile. Atherogenic index (AI) was calculated as the logarithm of the ratio of molar concentrations of TG and HDL-C [AI = log (TG/HDL-C)]. Plasma MDA, the end product of lipid peroxidation was estimated spectrophotometrically as thiobarbituric acid reactive substances (TBARS),[20] and TAC was determined by FRAP method in which a colorless ferric tripyridyltriazine complex is reduced to
a blue ferrous complex by the antioxidants in the plasma. The change in absorbance at 593 nm is directly related to the total reducing power of electron-donating antioxidants present in the plasma.[21]
Statistical analysisBetween-group differences for all normal distributed variables were tested by unpaired student t-test and expressed as mean ± SEM. The correlations were assessed by the Pearson and partial correlation. Receiver operating curve (ROC) analysis was done to statistically predict the variables with higher area under curve (AUC) values. A statistical significance was reported at a two-tailed P value of <0.05. All the statistical analyses were done using MedCalc software Version 12.1.0 (MedCalc®, Mariakerke, Belgium) and the SPSS software Version 11.5 (SPSS Inc, Chicago, IL, USA).
RESULTS
Mean and SEM of age, lipid profile, lipid risk factors and parameters of OS in patient and control groups are shown in Table 1. There was no significant difference in BMI between the groups. Diabetic patients had significantly high levels of FBS, TG (P < 0.01) and VLDL (P < 0.01) whereas there was no significant change in the TC, LDL, and HDL-C levels in the patients when compared to controls. Among various atherogenic lipid risk factors, TG/HDL-C (P < 0.01), and AI (P < 0.05) were found to be significantly elevated in diabetic patients compared to controls. There was a significant increase in the level of plasma MDA, a lipid peroxidation marker among diabetic patients versus controls (P < 0.01). FRAP levels
Table 1: Demographic and biochemical characteristics of the study populationVariable Cases (n=52)
mean±SDControls (n=52)
mean±SDP value
Age 50.2±1.13 52.3±0.95 0.16
BMI (kg/m[2]) 24.87±0.70 23.92±0.47 0.26
FBS (mg/dL) 135.43±0.48 92.09±1.13 0.000**
TC (mg/dL) 160.37±5.05 153.67±4.70 0.33TG (mg/dL) 156.08±10.83 126.13±4.95 0.01*HDL‑C (mg/dL) 43.73±1.29 44.37±0.49 0.64VLDL (mg/dL) 31.22±2.16 25.23±0.99 0.01*LDL (mg/dL) 87.38±5.18 84.08±4.48 0.63Non‑HDL‑C (mg/dL) 116.63±4.93 109.31±4.66 0.28TG/HDL‑C 3.78±0.30 2.87±0.12 0.006**
TC/HDL‑C 3.74±0.10 3.48±0.10 0.09LDL/HDL‑C 1.99±0.11 1.90±0.10 0.55Non‑HDL‑C/HDL‑C 2.74±0.10 2.48±0.10 0.09AI 0.16±0.03 0.08±0.01 0.02*UA (mg/dL) 4.52±0.07 4.62±0.14 0.54MDA (µmol/L) 3.42±0.09 0.80±0.05 0.000**FRAP (mmol/L) 0.33±0.01 1.41±0.05 0.000***P<0.05, **P<0.01; when significance was checked by the student t-test
www.mui.ac.ir

Suchitra, et al.: Association of MDA with hyperglycemia in diabetes
Journal of Research in Medical Sciences | February 2013 |91
were decreased significantly in the patient group when compared with the control group (P < 0.01).
The bivariate Pearson correlations between FBS, lipids, lipid risk factors and MDA are depicted in Table 2. The MDA levels correlated positively with FBS [Figure 1], TG, non-HDL-C, TG/HDL-C and with AI (P < 0.01), and negatively with LDL (P < 0.05). The partial correlation analysis of MDA with lipids and lipid risk factors after nullifying the effect of FBS in the patient group is shown in Table 2. The partial correlation analysis found a similar significant positive correlation of MDA with TG, TG/HDL-C and AI and a significant positive correlation was also observed with VLDL. The significant negative correlation observed with LDL was lost by partial correlation analysis. Partial correlation of MDA with FBS after nullifying the effects of each of the lipid variables among diabetic patients is depicted in Table 2, wherein the significant positive correlation of MDA with FBS did not change. ROC curve analysis showed high AUC for TG/HDL-C and AI respectively as shown in Table 3 and Figure 2.
DISCUSSION
Previous studies have also demonstrated hyperlipidemia and an increase in OS among Type 2 DM patients as compared to control counterparts.[15-17] The present study is novel in its approach of addressing the association of various lipid risk factors with diabetes and OS.
OS results when there is increased production of free radicals or decreased activity of counter-actors, antioxidants or both in a combination.[22] In the present study we found a significant increase in the levels of MDA, the major marker of lipid peroxidation and OS, which is in agreement with a similar observation reported in newly diagnosed
Type 2 DM patients.[23] We found a depletion of TAC in the diabetic group, represented by significantly reduced FRAP level indicating antioxidant imbalance in favor of OS. MDA levels correlated positively with FBS indicating
Table 2: Pearson and partial correlations of MDA with variablesVariable MDA with
variablesMDA with
lipids (nullified by FBS)
MDA with FBS (nullified by each
lipid variable)Pearson
correlation r value
Partial correlation
r value
Partial correlation r value
FBS (mg/dL) 0.39** ‑TC (mg/dL) −0.22NS −0.17NS 0.37**TG (mg/dL) 0.38** 0.41** 0.34*HDL‑C (mg/dL) −0.21NS −0.18NS 0.38**VLDL (mg/dL) −0.17NS 0.41** 0.34*LDL (mg/dL) −0.33* −0.28NS 0.36*Non‑HDL‑C (mg/dL)
0.38** −0.12NS 0.38**
TG/HDL‑C 0.45** 0.45** 0.32*TC/HDL‑C 0.01NS 0.03NS 0.39**LDL/HDL‑C −0.24NS −0.21NS 0.36**Non‑HDL‑C/HDL‑C
0.01NS 0.03NS 0.39**
AI 0.40** 0.38** 0.34*r(Correlation coefficient); P(two‑tailed significance); *P<0.05, **P<0.01; NS‑Not significant; MDA=Malondialdehyde; TG=Triglycerides; LDL=Low‑density lipoprotein; HDL‑C=High‑density lipoprotein cholesterol
Table 3: Receiver operating characteristics’ curve for atherogenic lipid risk factorsVariable AUC 95% CI P value
Non‑HDL 0.53 0.45‑0.65 0.32TG/HDL 0.62# 0.52‑0.74 0.03*TC/HDL 0.57 0.50‑0.69 0.07LDL/HDL 0.51 0.43‑0.63 0.56Non‑HDL/HDL 0.58 0.50‑0.69 0.07AI 0.62# 0.50‑0.74 0.03*CI=Confidence interval; AUC=Area under curve; #(high AUC); *(P<0.05)
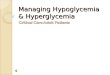
Figure 1: Correlation analysis of plasma MDA with FBS in diabetic patients (n = 52). r = 0.39, p = 0.004 by Pearson’s correlation and y = 11.23x + 90.12 and R2 = 0.16 for the graph
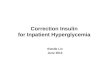
Figure 2: Receiver operating curve analysis showing high Area under curve values for atherogenic lipid risk factors; TG/HDL‑C (AUC = 0.62, p = 0.03) and AI (AUC = 0.62, p = 0.03).
www.mui.ac.ir

Suchitra, et al.: Association of MDA with hyperglycemia in diabetes
Journal of Research in Medical Sciences| February 2013 | 92
the association of hyperglycemia with OS. The source of OS in DM includes non-enzymatic, enzymatic and mitochondrial pathways.[15] It has been demonstrated that higher concentrations of glucose lead to excess free radical generation. Recently, Whiting et al., observed that chronic hyperglycemia can influence the generation of free radicals, which may eventually lead to increased lipid peroxidation and depletion of antioxidants, and thereby enhanced OS in subjects with T2DM.[24]
In the present study we observed significant lipid peroxidation, higher levels of lipids (TG and VLDL) and lipid risk factors (such as TG/HDL-C and AI) indicating atherogenic changes. Hypertriglyceridemia may lead to an increased production of the small, dense form of LDL cholesterol and to decreased HDL transport of cholesterol back to the liver. It has been proposed that TC/HDL-C and LDL/HDL-C ratios could be better predictors of atherosclerosis than the individual lipid parameters.[25] TG levels and TG–HDL-C ratio have been reported to be sensitive markers of insulin resistance, where the cutoff values that were most predictive of insulin resistance were TG level of 130 mg/dL or more and/or TG–HDL-C ratio of 3 or more.[8] In the present study the patient group had a significantly higher TG/HDL-C ratio when compared to controls. TG/HDL-C ratio has been proposed as an easily measurable predictor of LDL size and is best suggested as a surrogate marker of small dense LDL particles.[26] AI, which correlated inversely with LDL particle size was proposed as a marker of plasma atherogenicity that has better predictive value than lipids individually and ratios of individual lipids to HDL-C.[27] Hermans et al., proposed AI as a simple means to estimate atherogenic dyslipidemia and the residual cardiovascular risk in Type 2 DM.[12] A recent study by Rao et al.,[28] emphasizes the importance of AI in predicting CVD risk associated with newly diagnosed diabetes. The current study’s observation of significantly raised TG/HDL-C and AI is in accordance with the above observations, indicating the presence of atherogenic risk in newly diagnosed Type 2 DM patients.
OS is known to be associated with dyslipidemia.[18] Chronic OS in diabetic subjects may be related to the metabolism of excess substrates available such as glucose and fatty acids present in the hyperglycemic state. DM is a condition where hyperlipidemia is very common. Moreover, lipid peroxidation increases with hyperlipidemia.[18] In the present study, there were significant positive correlations of FBS, lipids and lipid risk factors with MDA, indicating the coexistence of atherogenic risk factors and OS. However, there was a negative correlation between MDA and LDL which may indicate excess LDL lipid peroxidation and thereby the increase in MDA. We statistically nullified the effect of hyperglycemia on the significant associations between MDA and lipid variables. In this case, the significance of the
association of MDA was lost only for LDL after statistical nullification. This indicates that hyperglycemia might play a significant role in the elevation of oxidative stress by increased oxidizability of LDL. Similarly, we nullified the effect of each of the lipid variables on the association between MDA and FBS, wherein the significance of positive correlation of MDA with FBS was retained even after nullifying the effect of lipid parameters. Therefore, lipid parameters cannot be the only main cause of OS in DM. Importantly, these correlation analyses also suggest that hyperglycemia per se is greatly involved in OS resulting in increased lipid peroxidation which is mainly associated with high blood sugar. It is clear from these observations that hyperglycemia in Type 2 DM results in increased lipid peroxidation and thereby elevated plasma MDA levels, which in turn are responsible for increase in coronary lipid risk factors. Furthermore, among all lipid risk factors, high AUC values were observed for TG/HDL-C and AI indicating the importance of these ratios as predictors of cardiovascular risk even in the early stages of T2DM. Our study has certain limitations, such as lack of data on insulin resistance. Nevertheless, as has been well documented previously, increased TG/HDL-C and AI, which we have also observed in the present study, may serve as sensitive markers for insulin resistance.
To conclude, our study suggests that hyperglycemia in newly diagnosed patients with Type 2 DM is associated with elevated OS through increased lipid peroxidation and depleted antioxidant capacity. The elevated plasma MDA levels are in turn associated with increased atherogenic lipid risk factors such as TG/HDL-C and AI in particular.
These findings point towards the need for early diagnosis and management of Type 2 DM patients in order to prevent the development of OS-associated diabetic complications. It may also be inferred that even in the early stages diabetic patients are exposed to OS due to hyperglycemia and OS is known to be the unifying factor in the development of diabetes complications. Hence supplementation of antioxidants may also be considered in the management of newly diagnosed Type 2 DM.
ACKNOWLEDGMENT
The authors wish to acknowledge the support and cooperation received from Prof. B Vengamma, Director, SVIMS University and wish to thank all the persons who helped us in this work.
REFERENCES
1. Howard BV, Robbins DC, Cowan LD, Lee ET, Go OT, Welty TK. Adverse effects of diabetes on multiple cardiovascular disease risk factors in women: The Strong Heart Study. Diabetes Care 1998;21:1258-65.
2. Fox CS, Coady S, Sorlie PD, D’Agostino RB Sr, Pencina MJ,
www.mui.ac.ir

Suchitra, et al.: Association of MDA with hyperglycemia in diabetes
Journal of Research in Medical Sciences | February 2013 |93
Vasan RS, et al. Increasing cardiovascular disease burden due to diabetes mellitus: The Framingham Heart Study. Circulation 2007;115:1544-50.
3. Grundy SM, Howard B, Smith S Jr, Eckel R, Redberg R, Bonow RO. Prevention Conference VI: Diabetes and Cardiovascular Disease: Executive summary: Conference proceeding for healthcare professionals from a special writing group of the American Heart Association. Circulation 2002;105:2231-9.
4. Ramachandran A, Mary S, Yamuna A, Murugesan N, Snehalatha C. High Prevalence of Diabetes and Cardiovascular Risk Factors Associated With Urbanization in India. Diabetes Care 2008;31:893-8.
5. Garg A, Grundy SM. Management of dyslipidemia in NIDDM. Diabetes Care 1990;13:153-69.
6. Kimm H, Lee SW, Lee HS, Shim KW, Cho CY, Yun JE, et al. Associations between lipid measures and metabolic syndrome, insulin resistance and adiponectin-Usefulness of lipid ratios in Korean men and women. Circ J 2010;74:931-7.
7. McLaughlin T, Reaven G, Abbasi F, Lamendola C, Saad M, Waters D, et al. Is there a simple way to identify insulin-resistant individuals at increased risk of cardiovascular disease? Am J Cardiol 2005;96:399-404.
8. McLaughlin T, Abbasi F, Cheal K, Chu J, Lamendola C, Reaven G. Use of metabolic markers to identify overweight individuals who are insulin resistant. Ann Intern Med 2003;139:802-9.
9. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adult (Adult Treatment Panel III). JAMA 2001;285:2486-97.
10. Cui Y, Blumenthal RS, Flaws JA, Whiteman MK, Langenberg P, Bachorik PS, et al. Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med 2001;161:1413-9.
11. Liu J, Sempos C, Donahue RP, Dorn J, Trevisan M, Grundy SM. Joint Distribution of Non-HDL-C and LDL Cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care 2005;28:1916-21.
12. Hermans MP, Ahn SA, Rousseau MF. Log (TG)/HDL-C is related to both residual cardiometabolic risk and β-cell function loss in type 2 diabetes males. Cardiovasc Diabetol 2010;9:88.
13. Ceriello A. Oxidative stress and glycemic regulation. Metabolism 2000;49:27-9.
14. Pfaffly JR. Review on diabetic complications. Free Radic Biol Med 2001;77:222.
15. Hong-zhi P, Zhang L, Mei-yi G, Hong Sui, Hui Li, Wei-hua Wu, et al. The oxidative stress status in diabetes mellitus and diabetic nephropathy. Acta Diabetol 2010;47:S71-6.
16. Bonfanti G, Ceolin RB, Valcorte T, De Bona KS, Leidiane de Lucca, Gonçalves TL, et al. δ-Aminolevulinate dehydratase activity in type 2 diabetic patients and its association with lipid profile and
oxidative stress. Clin Biochem 2011;44:1105-1109.17. Narasimhan S, Gokulakrishnan K, Sampathkumar R, Farooq S,
Ravikumar R, Mohan V, et al. Oxidative stress is independently associated with non-alcoholic fatty liver disease (NAFLD) in subjects with and without type 2 diabetes. Clin Biochem 2010;43:815-21.
18. Moriel P, Plavnik FL, Zanella MT, Bertolami MC, Abdalla DS. Lipid peroxidation and antioxidants in hyperlipidemia and hypertension. Biol Res 2000;33:105-12.
19. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972;18:499-502.
20. Sangeetha P, Das U, Koratkar R, Suryaprabha P. Increase in free radical generation and lipid peroxidation following chemotherapy in patients with cancer. Free Radic Biol Med 1990;8:15-9.
21. Benzie IF, Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: The FRAP assay. Anal Biochem 1996;239:70-6.
22. Baynes JW. Role of oxidative stress in development of complications in diabetes. Diabetes 1991;40:405-12.
23. Pasaoglu H, Sancak B, Bukan N. Lipid peroxidation and resistance to oxidation in patients with type 2 diabetes mellitus. Tohoku J Exp Med 2004;203:211-8.
24. Whiting PH, Kalansooriya A, Holbrook I, Haddad F, Jennings PE. The relationship between chronic glycaemic control and oxidative stress in type 2 diabetes mellitus. Br J Biomed Sci 2008;65:71-4.
25. Temelkova-Kurktschiev T, Hanefeld M. The lipid triad in type 2 diabetes-prevalence and relevance of hypertriglyceridaemia/low high-density lipoprotein syndrome in type 2 diabetes. Exp Clin Endocrinol Diabetes 2004;112:75-9.
26. Hanak V, Munoz J, Teague J, Stanley A, Bittner V. Accuracy of the triglyceride to high-density lipoprotein cholesterol ratio for prediction of the low-density lipoprotein phenotype B. Am J Cardiol 2004;94:219-22.
27. Dobiasova M. Atherogenic Index of Plasma [Log (Triglycerides/HDL-C Cholesterol)]: Theoretical and Practical Implications. Clin Chem 2004;50:1113-5.
28. Rao BR, Parineetha PB, Raman VV. Study on Correlations Between Glycated Haemoglobin, Lipid Profi les and Blood Glucose Levels in Type 2 Diabetics Living at Moderate High Altitude. International Medical journal Malaysia 2010;9:39-44.
How to cite this article: Manohar SM, Vaikasuvu SR, Deepthi K, Sachan A, Narasimha SRPVL. An association of hyperglycemia with plasma malondialdehyde and atherogenic lipid risk factors in newly diagnosed Type 2 diabetic patients. J Res Med Sci 2013;18:89‑93.
Source of Support: Nil, Conflict of Interest: None declared.
www.mui.ac.ir