Embed Size (px)
Citation preview
An Atlas of Investigation and Management
HYPERTENSION
Edward D FrohlichAlton Ochsner Medical Foundation
New Orleans, USA
Hector O VenturaAlton Ochsner Medical Foundation
New Orleans, USA
CLINICAL PUBLISHINGOXFORD
Hypertension prelims 16/10/08 16:25 Página iii
Clinical Publishing an imprint of Atlas Medical Publishing LtdOxford Centre for InnovationMill Street, Oxford OX2 0JX, UK
Tel: +44 1865 811116Fax: +44 1865 251550E mail: [email protected]: www.clinicalpublishing.co.uk
Distributed in USA and Canada by:Clinical Publishing30 Amberwood ParkwayAshland OH 44805 USA
tel: 800-247-6553 (toll free within U.S. and Canada)fax: 419-281-6883email: [email protected]
Distributed in UK and Rest of World by:Marston Book Services LtdPO Box 269AbingdonOxon OX14 4YN UK
tel: +44 1235 465500fax: +44 1235 465555e mail: [email protected]
© Atlas Medical Publishing Ltd 2009
First published 2009
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted,in any form or by any means, without the prior permission in writing of Clinical Publishing or Atlas MedicalPublishing Ltd
Although every effort has been made to ensure that all owners of copyright material have been acknowledgedin this publication, we would be glad to acknowledge in subsequent reprints or editions any omissions broughtto our attention
A catalogue record for this book is available from the British Library
ISBN-13 978 1 904392 15 6ISBN-10 1 904392 15 6ISBN e-book 978 1 84692 524 5
The publisher makes no representation, express or implied, that the dosages in this book are correct.Readers must therefore always check the product information and clinical procedures with the mostup-to-date published product information and data sheets provided by the manufacturers and the mostrecent codes of conduct and safety regulations. The authors and the publisher do not accept anyliability for any errors in the text or for the misuse or misapplication of material in this work
Project managed by Prepress Projects Ltd, Perth, UKTypeset by Initial Typesetting Services, Edinburgh, UKPrinted by T G Hostench, s.a.
Hypertension prelims 16/10/08 16:25 Página iv
Contents
Preface and a brief apologia vi
Abbreviations vii
Dedication viii
Introduction ix
1. Pathophysiology: disease mechanisms 1
2. Evaluation of the patient 15
3. Clinical pharmacology of antihypertensive agents 37
4. Uncomplicated essential hypertension 55
5. The heart in hypertension 73
6. The kidney in hypertension 89
7. Renal arterial disease 113
8. Concluding comments 123
Epilogue 125
Index 127
Hypertension prelims 16/10/08 16:25 Página v

Preface and a brief apologia
In a textbook of this nature, it is in order to provide theprospective reader and potential reviewer with a briefoverview of the goals, limits and editorial guidelines that weset for ourselves in preparing the material for this atlas. Inthe Introduction we provide some personal remarks relatedto our agreement to organize and present our repertoire ofvisual material, but, perhaps, a few words might be in orderhere to explain our selection.
First, a number of friends and colleagues encouraged us topublish the material for many of our lectures over the years.Our publisher further supported these comments althoughhe raised the concern that some material and referencesmight seem to be dated. We agreed and exerted particulareffort to select only that pictorial and diagrammatic materialwhich we strongly believed was currently pertinent forpresentation and for pedagogic purposes.
Another concern (as a past Editor-in-Chief of two majorjournals and the author of several textbooks and manypapers) was related to our selection of reference material.The purpose of this text was to present neither a literaturereview nor a current state of the art. We therefore chose toprovide ‘suggested reading’ so that the reader can consult inthe peer-reviewed literature the primary references for theclinical and experimental material we use to support ourpictorial, tabular and diagrammatic material.
With these comments, we sincerely hope that the atlasmaterial, the accompanying discussion and suggestedreading are of value to the reader. We hope that this bookwill be of value to readers who are clinicians and students ofhypertension and who are interested in the pathophysiologyof hypertensive disease.
vi
Hypertension prelims 16/10/08 16:25 Página vi
vii
Abbreviations
ACE angiotensin-converting enzymeACEI angiotensin-converting enzyme inhibitorARB angiotensin receptor blockerAT angiotensinogenAV arteriolar–venularBB beta blockerCBC complete blood countCCB calcium channel blockerCHD coronary heart diseaseCHF congestive heart failureCOPD chronic obstructive pulmonary diseaseCPV cardiopulmonary volumeDBP diastolic blood pressureECG electrocardiogramERBF estimated renal blood flowESRD end-stage renal diseaseFF filtration fractionGFR glomerular filtration rateHCTZ hydrochlorothiazideHCVD hypertensive cardiovascular diseaseHHD hypertensive heart diseaseIP3 inositol triphosphateISA intrinsic sympathomimetic activityIVU intravenous urography
LV left ventricleLVH left ventricular hypertrophyLVS left ventricular strainMAP mean arterial pressureMI myocardial infarctionL-NAME nitro-L-arginine methyl ester hydrochlorideNSAID non-steroidal anti-inflammatory drugPKD polycystic kidney diseasePRA plasma renin activityPSA prostate-specific antigenPV plasma volumePWT pulmonary wall thicknessRA renal afferentRE renal efferentRHD rheumatic heart diseaseSHR spontaneously hypertensive ratSBP systolic blood pressureSNFF single-nephron filtration fractionSNGFR single-nephron glomerular filtration rateSNPF single-nephron plasma flowSMA smooth muscle actinTPR total peripheral resistanceTSH thyroid-stimulating hormoneUPE urinary protein excretionWKY Wistar–Kyoto rat
Hypertension prelims 16/10/08 16:25 Página vii

viii
Dedication
We dedicate this textbook to our wives, Sherry Frohlich andLaurie Ventura, and to our children, who share with us thevery honest and warm thirst for knowledge, whether in themedical or in other academic environments. It is thisunderstanding of the need to impart one’s personal orprofessional knowledge and experience which provides an
added dimension to nurture family as well as our pro-fessional colleagues. This is the long-standing commitmentof the well-rounded physician, and it is the obligation of allteachers and professionals to impart a better life to manwithin our professional careers.
Hypertension prelims 16/10/08 16:25 Página viii

Introduction
Producing an atlas on hypertension was not at the forefrontof my thinking until I was approached by Jonathan Gregory,commissioning editor at Clinical Publishing, who wasinterested in publishing such a textbook. Indeed, in recentyears, I have questioned the importance of hypertension asa discipline. Institutions such as mine no longer maintain aseparate hospital service for admitting patients with thediagnosis of hypertension; and the numbers of patients withprimary problems relating to hypertension have diminishedconsiderably. This is in striking contrast to the early days ofmy academic career, when a large majority of hospitalizedpatients were admitted with hypertensive emergencies orhypertension associated with myocardial infarction,congestive heart failure, angina pectoris, stroke or renalinvolvement. Today, a patient with hypertension who ishospitalized because of myocardial infarction, acutecoronary syndrome or renal failure is immediately sent to aspecialized unit. Yes, we have certainly come a long way overthe past five decades.
On the other hand, the number of patients withhypertension continues to increase all over the world.Clearly, this is partly the result of what I have termed the‘numbers game’ of disease. That is to say, the limits ofnormal – whether of blood pressure, blood sugarconcentration or body weight – continue to converge, and sothe number of potential patients with hypertension ordiabetes mellitus or obesity continues to rise. And as aconsequence, the increasing attention demanded by thesediseases falls on the shoulders of the primary care physician,and with this responsibility comes a greater need for a clearunderstanding of the pathophysiology of these diseases andtheir management. Related to the increased attention thesediseases receive, and the increase in the number of suchpatients seen in any physician’s day-to-day practice, areremarkable innovations in diagnosis and management. Andso the subject arose of yet another textbook about hyper-tension. I was won over by the need to confine the text tojust these subjects: classification of the disease; a clearinsight into the pathophysiology and initial evaluation of the
hypertensive patient; an elucidation of the mechanisms ofaction of the varied modes of therapy including non-drug aswell as pharmacological entities; and my personal overviewand investigative and clinical experience with two vital areas,the heart and kidney in hypertension.
Most national and international guidelines present astraightforward concept for the evaluation and treatment ofpatients with hypertension; and they presently suggest aclear-cut course of action with respect to treatment unlessthere are complicating considerations. For the most part, weagree with this presentation; but, of course, as is the casewith most consultants, consideration must be focused on thepatient in whom complicating factors suggest specificproblems. To my way of thinking, the major areas thatrequire more specific attention relate to the hypertensivepatient with cardiac or renal involvement. Indeed, cardiacand renal failure continue to increase in frequency despitethe reduction in deaths from stroke or coronary heartdisease and the fact that hypertensive emergencies are todayrather rare. Patients with hypertension who are hospitalizedwith myocardial infarction or with end-stage renal disease,as well as patients with an acute stroke, require veryspecialized hospital services. And so we are left with theneed to consider in detail the heart in hypertension and thekidney in hypertension. Both deserve very specificdiscussions in a textbook for the primary care physician orinternist, cardiologist or nephrologist, all of whom deal witha large number of such patients who are not coveredadequately by current clinical guidelines. Moreover, over thepast few years I have on several occasions been invited topresent my thoughts on this matter to such physicians, andso I was convinced that now might be an appropriate timeto share my personal thoughts in an ‘atlas’ format. It becameapparent to me that in such a book I would be able to impartnot only my personal clinical experience, but also theongoing work in my laboratories, which focuses primarily onthe heart and kidney. At this point in my thinking about thesubject, I discussed the merits of the task with my long-timefriend and colleague, Hector Ventura. Hector convinced me
ix
Hypertension prelims 16/10/08 16:25 Página ix

of the potential ‘need’ for such an undertaking, and when he‘volunteered’ to assist me I readily agreed. Thus, theconcept and the format for this atlas of hypertensiondeveloped and we thereupon began this job.
Not infrequently, we are invited to write a book review.Often, one of the major pitfalls for an author is to clearlyidentify what the book is trying to achieve; and so we werevery careful to ensure that we express our thinking clearly.We did not want to write a textbook that deals with thehypertensive patient who presents with problems that con-stitute an emergency or those who require hospitalization ina special care unit. Nor did we want to discuss the patientwhose demographic characteristics are such that specificchapters need be dedicated to a discussion of the role of thepatient’s age, race or gender, or the patient who suffers froma new popular syndrome. In the final analysis, when thephysician is confronted by a particular patient, the relation-ship is one-on-one, and the decision about diagnosis andtherapy for that person is very specific and unique for thatclinical situation.
Thus, we accepted Jonathan Gregory’s invitation andpresented to him our revised thinking. We proposed atextbook that would present our personal opinions abouthypertensive disease and its cardiac and renal complicationsas it relates to everyday pathophysiological assessment andabout the choice of therapy not only for the relativelyuncomplicated patient but also for the frequentlyencountered patient with complications affecting the heartand kidneys. This material would, we believe, best bepresented as tables or figures that would hopefully clarifyour thinking on patient management as suggested by ourclinical as well as laboratory experience.
To complete our task we want to express our appreciationto Jonathan Gregory for stimulating our thinking about howto present the very common problem of hypertension in thepractice setting. We also want to express our warm andheartfelt appreciation to our wives and children, first andforemost, for their abiding understanding of our need tospend more time away from home and family in order tomeet yet another deeply personal commitment. It is to them,our dear families, that we dedicate this endeavour. Inaddition, we want to express our appreciation to our officestaff (Lillian Buffa, Caramia Fairchild and PamellaTadesco), whose continuous support of our dailyprofessional activities permitted us to pursue yet anotherjob.
It would be totally remiss of me not to mention a fewstumbling blocks that I encountered along the way duringthe preparation of this book: the sudden striking ofHurricanes Katrina and Rita; the associated flooding andloss of my home and long-to-be remembered library(including ‘saved’ copies of completed chapters on harddrives and disks), records and recollections; an enforcedevacuation from New Orleans to our daughter’s home inChicago; and conversation and support from my son in NewJersey whereby personal refocusing was made possible. And,finally, I want to express my (our) appreciation to ourcolleagues and institution, who continue to provide theambience and culture required to pursue an academicdimension to the overall healthcare effort (especially in thepast difficult times).
Edward D. Frohlich, MDNew Orleans, LA
May 2008
Introductionx
Hypertension prelims 16/10/08 16:25 Página x
Pathophysiology:disease mechanisms
Chapter 1
Introduction
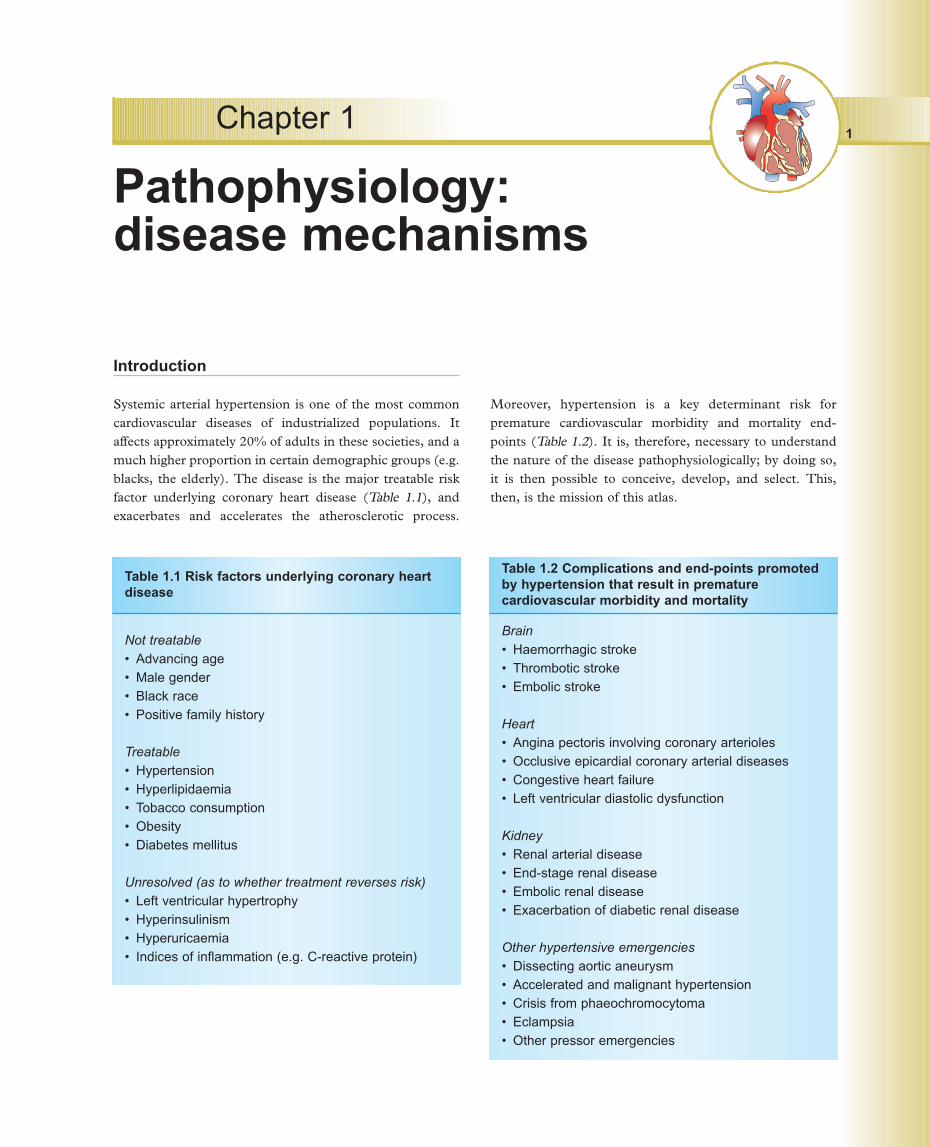
Systemic arterial hypertension is one of the most commoncardiovascular diseases of industrialized populations. Itaffects approximately 20% of adults in these societies, and amuch higher proportion in certain demographic groups (e.g.blacks, the elderly). The disease is the major treatable riskfactor underlying coronary heart disease (Table 1.1), andexacerbates and accelerates the atherosclerotic process.
Moreover, hypertension is a key determinant risk forpremature cardiovascular morbidity and mortality end-points (Table 1.2). It is, therefore, necessary to understandthe nature of the disease pathophysiologically; by doing so,it is then possible to conceive, develop, and select. This,then, is the mission of this atlas.
1
Not treatable• Advancing age• Male gender• Black race• Positive family history
Treatable• Hypertension• Hyperlipidaemia• Tobacco consumption• Obesity• Diabetes mellitus
Unresolved (as to whether treatment reverses risk)• Left ventricular hypertrophy• Hyperinsulinism• Hyperuricaemia• Indices of inflammation (e.g. C-reactive protein)
Table 1.1 Risk factors underlying coronary heartdisease
Brain• Haemorrhagic stroke• Thrombotic stroke• Embolic stroke
Heart• Angina pectoris involving coronary arterioles• Occlusive epicardial coronary arterial diseases• Congestive heart failure• Left ventricular diastolic dysfunction
Kidney• Renal arterial disease• End-stage renal disease• Embolic renal disease• Exacerbation of diabetic renal disease
Other hypertensive emergencies• Dissecting aortic aneurysm• Accelerated and malignant hypertension• Crisis from phaeochromocytoma• Eclampsia• Other pressor emergencies
Table 1.2 Complications and end-points promotedby hypertension that result in prematurecardiovascular morbidity and mortality
Hypertension ch1 16/10/08 14:51 Página 1
The mosaic
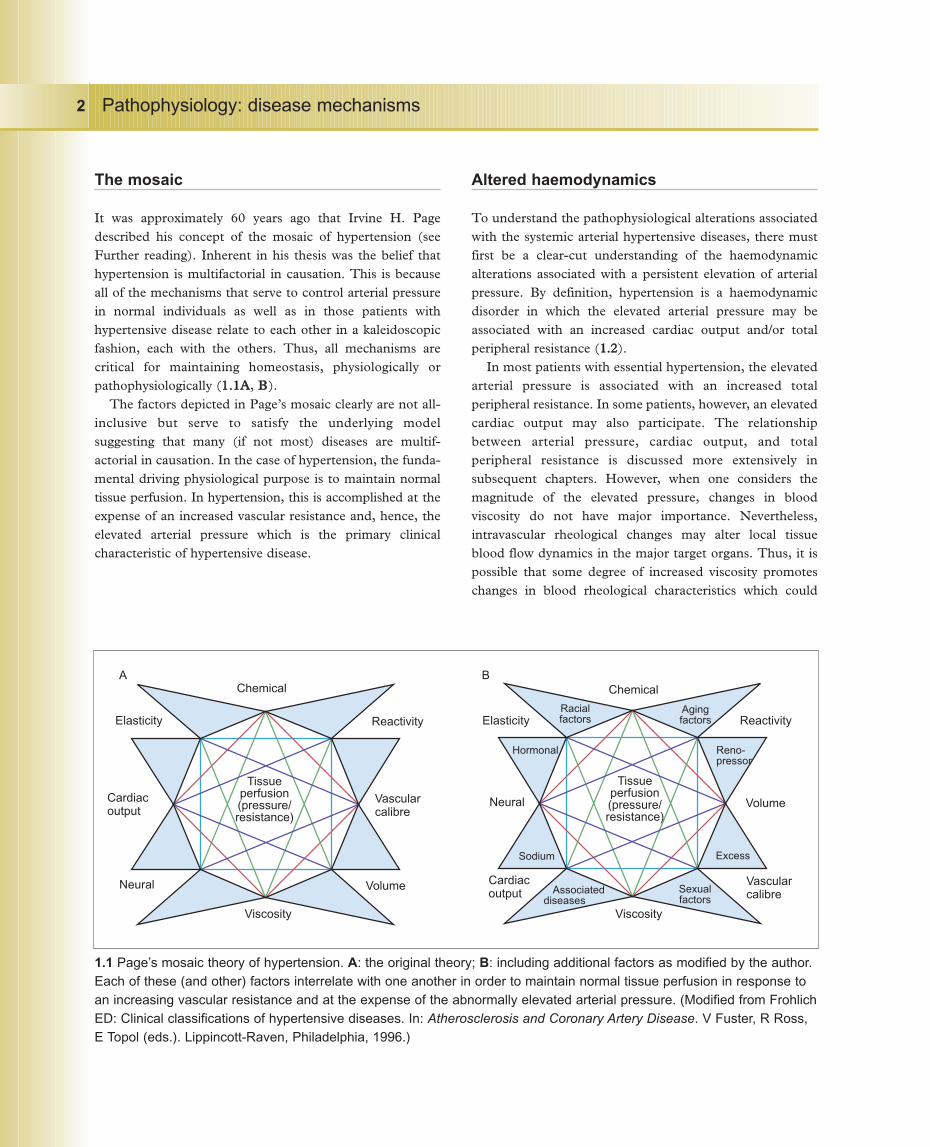
It was approximately 60 years ago that Irvine H. Pagedescribed his concept of the mosaic of hypertension (seeFurther reading). Inherent in his thesis was the belief thathypertension is multifactorial in causation. This is becauseall of the mechanisms that serve to control arterial pressurein normal individuals as well as in those patients withhypertensive disease relate to each other in a kaleidoscopicfashion, each with the others. Thus, all mechanisms arecritical for maintaining homeostasis, physiologically orpathophysiologically (11..11AA, BB).
The factors depicted in Page’s mosaic clearly are not all-inclusive but serve to satisfy the underlying modelsuggesting that many (if not most) diseases are multif-actorial in causation. In the case of hypertension, the funda-mental driving physiological purpose is to maintain normaltissue perfusion. In hypertension, this is accomplished at theexpense of an increased vascular resistance and, hence, theelevated arterial pressure which is the primary clinicalcharacteristic of hypertensive disease.
Altered haemodynamics
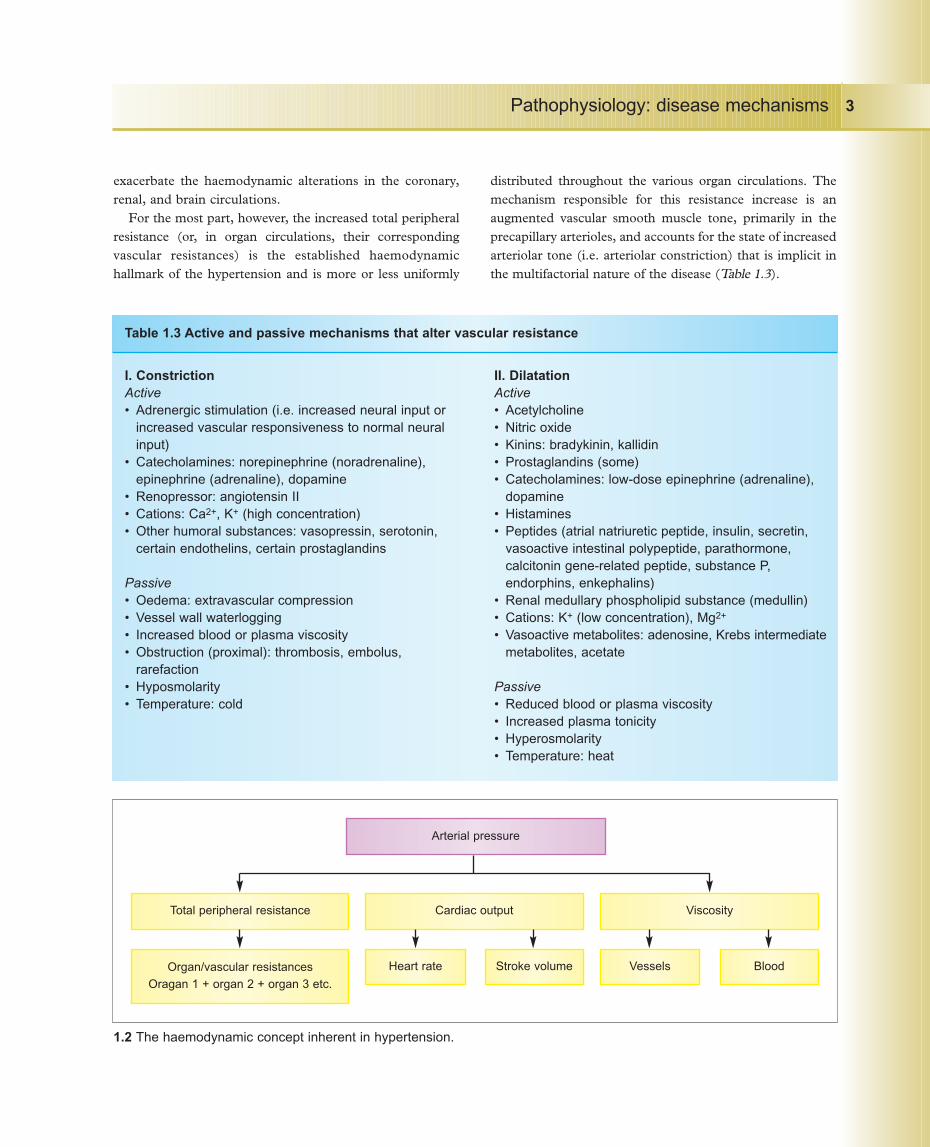
To understand the pathophysiological alterations associatedwith the systemic arterial hypertensive diseases, there mustfirst be a clear-cut understanding of the haemodynamicalterations associated with a persistent elevation of arterialpressure. By definition, hypertension is a haemodynamicdisorder in which the elevated arterial pressure may beassociated with an increased cardiac output and/or totalperipheral resistance (11..22).
In most patients with essential hypertension, the elevatedarterial pressure is associated with an increased totalperipheral resistance. In some patients, however, an elevatedcardiac output may also participate. The relationshipbetween arterial pressure, cardiac output, and totalperipheral resistance is discussed more extensively insubsequent chapters. However, when one considers themagnitude of the elevated pressure, changes in bloodviscosity do not have major importance. Nevertheless,intravascular rheological changes may alter local tissueblood flow dynamics in the major target organs. Thus, it ispossible that some degree of increased viscosity promoteschanges in blood rheological characteristics which could
Pathophysiology: disease mechanisms2
1.1 Page’s mosaic theory of hypertension. A: the original theory; B: including additional factors as modified by the author.Each of these (and other) factors interrelate with one another in order to maintain normal tissue perfusion in response toan increasing vascular resistance and at the expense of the abnormally elevated arterial pressure. (Modified from FrohlichED: Clinical classifications of hypertensive diseases. In: Atherosclerosis and Coronary Artery Disease. V Fuster, R Ross,E Topol (eds.). Lippincott-Raven, Philadelphia, 1996.)
ChemicalChemical
Reactivity Reactivity
Volume
Volume
Vascularcalibre
Vascularcalibre
ViscosityViscosity
Cardiacoutput
Neural
Cardiacoutput
Neural
ElasticityElasticity
Tissueperfusion(pressure/resistance)
Tissueperfusion(pressure/resistance)
Racialfactors
Agingfactors
Hormonal Reno-pressor
Sodium Excess
Associateddiseases
Sexualfactors
A B
Hypertension ch1 16/10/08 14:51 Página 2
exacerbate the haemodynamic alterations in the coronary,renal, and brain circulations.
For the most part, however, the increased total peripheralresistance (or, in organ circulations, their correspondingvascular resistances) is the established haemodynamichallmark of the hypertension and is more or less uniformly
distributed throughout the various organ circulations. Themechanism responsible for this resistance increase is anaugmented vascular smooth muscle tone, primarily in theprecapillary arterioles, and accounts for the state of increasedarteriolar tone (i.e. arteriolar constriction) that is implicit inthe multifactorial nature of the disease (Table 1.3).
Pathophysiology: disease mechanisms 3
1.2 The haemodynamic concept inherent in hypertension.
Arterial pressure
Total peripheral resistance Cardiac output Viscosity
Organ/vascular resistances
Oragan 1 + organ 2 + organ 3 etc.
Heart rate Stroke volume Vessels Blood
I. ConstrictionActive• Adrenergic stimulation (i.e. increased neural input or
increased vascular responsiveness to normal neuralinput)
• Catecholamines: norepinephrine (noradrenaline),epinephrine (adrenaline), dopamine
• Renopressor: angiotensin II• Cations: Ca2+, K+ (high concentration)• Other humoral substances: vasopressin, serotonin,
certain endothelins, certain prostaglandins
Passive• Oedema: extravascular compression• Vessel wall waterlogging• Increased blood or plasma viscosity• Obstruction (proximal): thrombosis, embolus,
rarefaction• Hyposmolarity• Temperature: cold
II. DilatationActive• Acetylcholine• Nitric oxide• Kinins: bradykinin, kallidin• Prostaglandins (some)• Catecholamines: low-dose epinephrine (adrenaline),
dopamine• Histamines• Peptides (atrial natriuretic peptide, insulin, secretin,
vasoactive intestinal polypeptide, parathormone,calcitonin gene-related peptide, substance P,endorphins, enkephalins)
• Renal medullary phospholipid substance (medullin)• Cations: K+ (low concentration), Mg2+
• Vasoactive metabolites: adenosine, Krebs intermediatemetabolites, acetate
Passive• Reduced blood or plasma viscosity• Increased plasma tonicity• Hyperosmolarity• Temperature: heat
Table 1.3 Active and passive mechanisms that alter vascular resistance
Hypertension ch1 16/10/08 14:51 Página 3
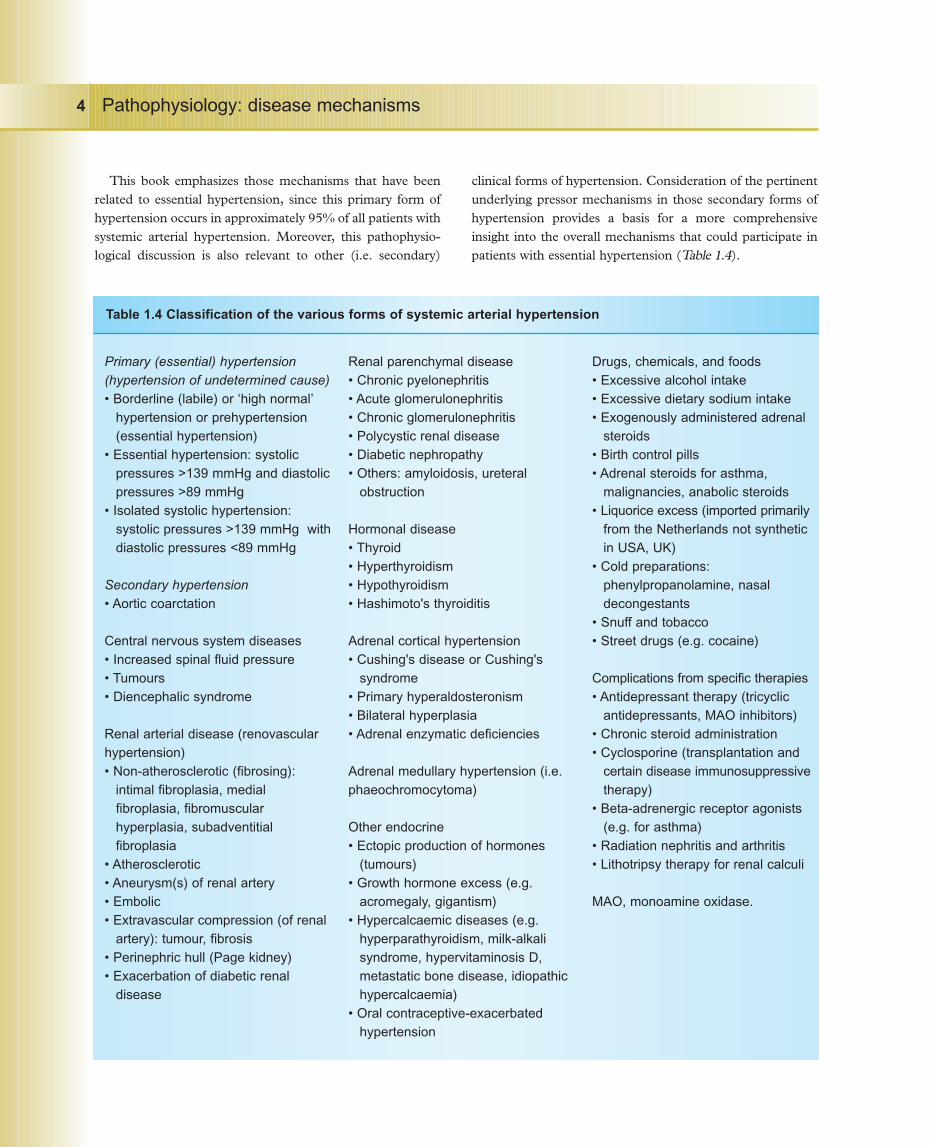
This book emphasizes those mechanisms that have beenrelated to essential hypertension, since this primary form ofhypertension occurs in approximately 95% of all patients withsystemic arterial hypertension. Moreover, this pathophysio-logical discussion is also relevant to other (i.e. secondary)
clinical forms of hypertension. Consideration of the pertinentunderlying pressor mechanisms in those secondary forms ofhypertension provides a basis for a more comprehensiveinsight into the overall mechanisms that could participate inpatients with essential hypertension (Table 1.4).
Pathophysiology: disease mechanisms4
Primary (essential) hypertension(hypertension of undetermined cause)• Borderline (labile) or ‘high normal’
hypertension or prehypertension(essential hypertension)
• Essential hypertension: systolicpressures >139 mmHg and diastolicpressures >89 mmHg
• Isolated systolic hypertension:systolic pressures >139 mmHg withdiastolic pressures <89 mmHg
Secondary hypertension• Aortic coarctation
Central nervous system diseases• Increased spinal fluid pressure• Tumours• Diencephalic syndrome
Renal arterial disease (renovascularhypertension)• Non-atherosclerotic (fibrosing):
intimal fibroplasia, medialfibroplasia, fibromuscularhyperplasia, subadventitialfibroplasia
• Atherosclerotic• Aneurysm(s) of renal artery• Embolic• Extravascular compression (of renal
artery): tumour, fibrosis• Perinephric hull (Page kidney)• Exacerbation of diabetic renal
disease
Renal parenchymal disease• Chronic pyelonephritis• Acute glomerulonephritis• Chronic glomerulonephritis• Polycystic renal disease• Diabetic nephropathy• Others: amyloidosis, ureteral
obstruction
Hormonal disease• Thyroid• Hyperthyroidism• Hypothyroidism• Hashimoto's thyroiditis
Adrenal cortical hypertension• Cushing's disease or Cushing's
syndrome• Primary hyperaldosteronism• Bilateral hyperplasia• Adrenal enzymatic deficiencies
Adrenal medullary hypertension (i.e.phaeochromocytoma)
Other endocrine• Ectopic production of hormones
(tumours)• Growth hormone excess (e.g.
acromegaly, gigantism)• Hypercalcaemic diseases (e.g.
hyperparathyroidism, milk-alkalisyndrome, hypervitaminosis D,metastatic bone disease, idiopathichypercalcaemia)
• Oral contraceptive-exacerbatedhypertension
Drugs, chemicals, and foods• Excessive alcohol intake• Excessive dietary sodium intake• Exogenously administered adrenal
steroids• Birth control pills• Adrenal steroids for asthma,
malignancies, anabolic steroids• Liquorice excess (imported primarily
from the Netherlands not syntheticin USA, UK)
• Cold preparations:phenylpropanolamine, nasaldecongestants
• Snuff and tobacco• Street drugs (e.g. cocaine)
Complications from specific therapies• Antidepressant therapy (tricyclic
antidepressants, MAO inhibitors)• Chronic steroid administration• Cyclosporine (transplantation and
certain disease immunosuppressivetherapy)
• Beta-adrenergic receptor agonists(e.g. for asthma)
• Radiation nephritis and arthritis• Lithotripsy therapy for renal calculi
MAO, monoamine oxidase.
Table 1.4 Classification of the various forms of systemic arterial hypertension
Hypertension ch1 16/10/08 14:51 Página 4

Arteriolar constrictionArteriolar (and, for that matter, venular) smooth muscletone is increased in hypertension, although all of themechanism(s) responsible are not entirely known. Nodoubt, this relates to the many pressor and depressor factorsthat normally participate in regulating vessel tone andcalibre and, hence, arterial pressure (Table 1.3). It followsthat these factors also participate in the increased vascularresistance in most patients with essential hypertension.Lessons concerning regulation of increased vascularresistance have been learned from the variety of secondaryforms of hypertension in which specific pressor anddepressor mechanisms are involved (Table 1.4).
It is likely that the increased vascular resistance in mostpatients with essential hypertension may be mediatedthrough more than one pressor mechanism. Some of thesemechanisms are predetermined by inborn genetic factors,since it has become increasingly apparent that thepathophysiological alterations in essential hypertension arepolygenetic in origin. Furthermore, many of the pressor anddepressor mechanisms that seem to be operative have beenwell documented to increase actively vascular smoothmuscle tone. Many new mechanisms are elucidated witheach passing year. Thus, vascular smooth muscle tone isabnormally increased as a result of one or more of thosefactors that participate in the underlying disease process andare then expressed in the clinical manifestations of thatpatient’s disease. As a consequence of the increased totalperipheral resistance, arterial pressure rises in order tomaintain tissue perfusion; this occurs at the expense of thevascular and cardiac systems, and the specific indices oforgan damage and functional impairment that secondarilyresult.
As suggested in Tables 1.2 and 1.3, the increased tone ofthe arteriolar or venular smooth muscle occurs no matterwhat mechanism(s) participate. Thus, for example, thevascular myocyte is constricted by enhanced adrenergicinput or elevated circulating levels of catecholamines;alterations in circulating or local autocrine/paracrine effectsof humoral substances; local or systemic participation ofvasoactive peptides (e.g. angiotensin II, endothelin); ions;and growth factors. Alternatively, increased vascularresistance may also be produced by reduced local orsystemic amounts of vasodilating agents, local vasoactivepeptides or ions, and vasoactive metabolites (Table 1.3).Whatever the myocytic stimulus, there is a resultant rise incytoplasmic free calcium ions from their resting state that
results in enhanced phosphorylation of myosin light chains.This increased calcium ionic milieu may be achieved eitherthrough an inflow of calcium ions through calcium- orother receptor-activated membrane channels or by a releaseof calcium ions from intracellular organelles, althoughcalcium may be released from the mitochondria or frombinding with protein substrates through secondarilyactivated biochemical processes. The net increase inintracytoplasmic calcium ion concentration promotes theformation of inositol triphosphate (IP3) and diacylglycerol.IP3 serves as the second messenger, mediating the calciumion release and the resulting mechanical coupling thatpermits an enhanced state of contractility of vascularsmooth muscle.
Arteriolar structureAnother factor participating in the increased vascularresistance of hypertension is an increased wall-to-lumenratio of the arteries and arterioles. This structural alterationin hypertension serves to amplify the arteriolar responsive-ness to constrictor stimuli that maintains the hypertensivedisease process. Recent investigations have suggested thatthe haemodynamic stress of vessel stretch may be animportant additional mechanism responsible for the vesselwall thickening, or even of myocytic hypertrophy of the leftventricle. Several reports have indicated that upon stretch ofthe ventricular or arteriolar (e.g. renal, coronary) myocyte,one or more of a vast array of ‘early genes’ or proto-oncogenes participate in initiating DNA-directed myocyticand collagen (and likely other) growth. Some of thesegrowth factors are themselves vasoconstrictors (e.g.angiotensin II, norepinephrine [noradrenaline], endothelin),and they may even be generated within the arteriolar orventricular endothelium or wall itself. Intriguingly, they mayalso participate in the separate but related process ofatherogenesis. Hence, this may explain the close relationshipof these two common and comorbid diseases (i.e.hypertensive vascular disease and atherosclerosis).
Pre- and postcapillary constrictionFor the most part, all patients with hypertension have anincreased arterial pressure that is associated with anincreased contractile state of vascular smooth muscle inboth the arterioles and venules. The movement of plasma orinterstitial fluid across the capillaries follows Starlingmechanics, and depends upon the hydrostatic and colloidosmotic pressures in the intravascular and interstitial
Pathophysiology: disease mechanisms 5
Hypertension ch1 16/10/08 14:51 Página 5
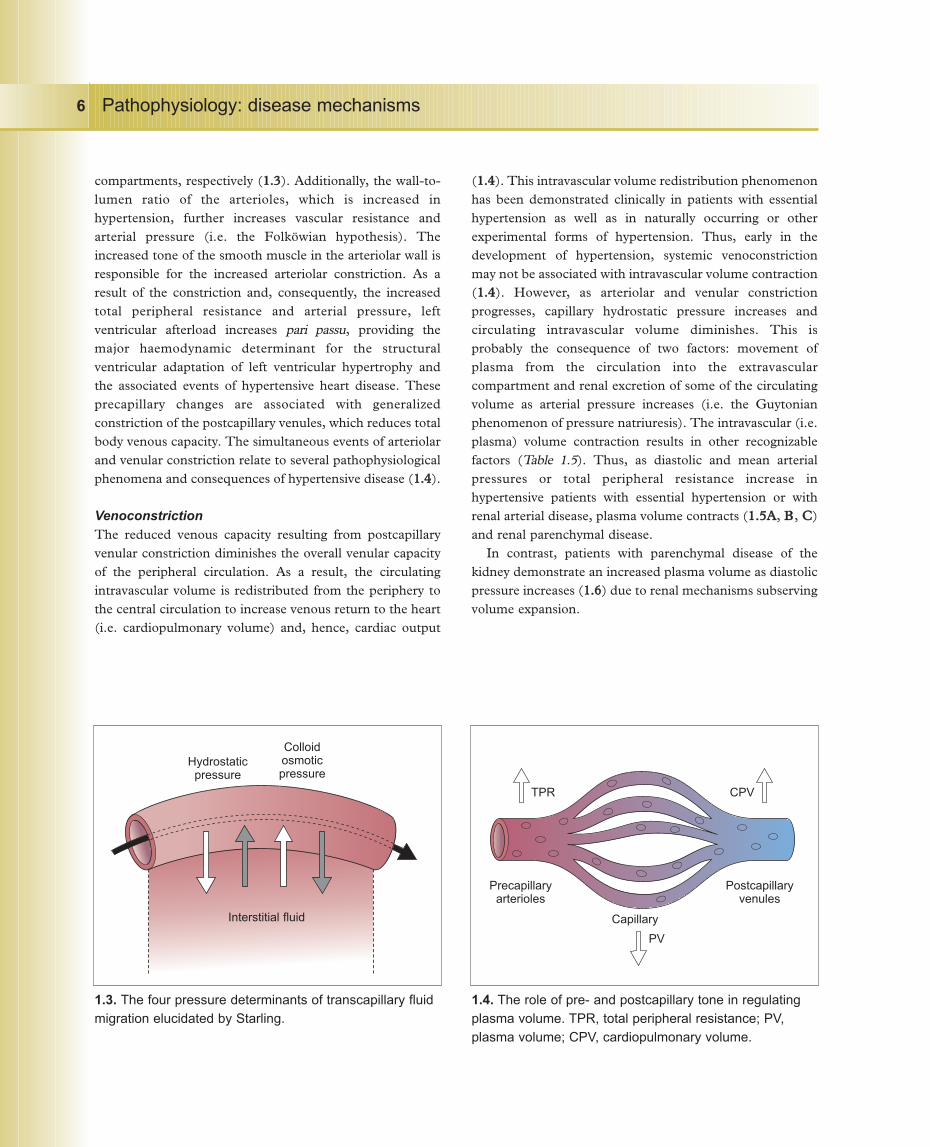
compartments, respectively (11..33). Additionally, the wall-to-lumen ratio of the arterioles, which is increased inhypertension, further increases vascular resistance andarterial pressure (i.e. the Folköwian hypothesis). Theincreased tone of the smooth muscle in the arteriolar wall isresponsible for the increased arteriolar constriction. As aresult of the constriction and, consequently, the increasedtotal peripheral resistance and arterial pressure, leftventricular afterload increases pari passu, providing themajor haemodynamic determinant for the structuralventricular adaptation of left ventricular hypertrophy andthe associated events of hypertensive heart disease. Theseprecapillary changes are associated with generalizedconstriction of the postcapillary venules, which reduces totalbody venous capacity. The simultaneous events of arteriolarand venular constriction relate to several pathophysiologicalphenomena and consequences of hypertensive disease (11..44).
VenoconstrictionThe reduced venous capacity resulting from postcapillaryvenular constriction diminishes the overall venular capacityof the peripheral circulation. As a result, the circulatingintravascular volume is redistributed from the periphery tothe central circulation to increase venous return to the heart(i.e. cardiopulmonary volume) and, hence, cardiac output
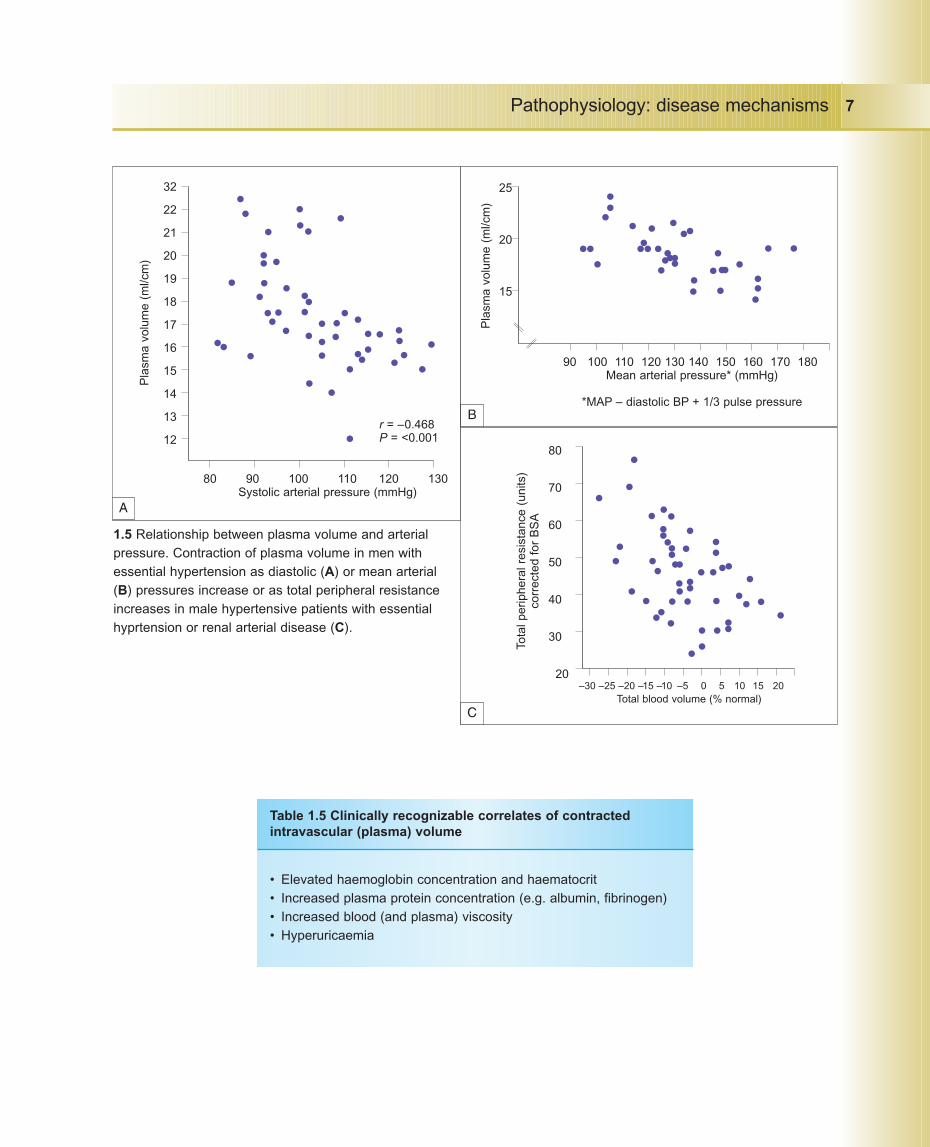
(11..44). This intravascular volume redistribution phenomenonhas been demonstrated clinically in patients with essentialhypertension as well as in naturally occurring or otherexperimental forms of hypertension. Thus, early in thedevelopment of hypertension, systemic venoconstrictionmay not be associated with intravascular volume contraction(11..44). However, as arteriolar and venular constrictionprogresses, capillary hydrostatic pressure increases andcirculating intravascular volume diminishes. This isprobably the consequence of two factors: movement ofplasma from the circulation into the extravascularcompartment and renal excretion of some of the circulatingvolume as arterial pressure increases (i.e. the Guytonianphenomenon of pressure natriuresis). The intravascular (i.e.plasma) volume contraction results in other recognizablefactors (Table 1.5). Thus, as diastolic and mean arterialpressures or total peripheral resistance increase inhypertensive patients with essential hypertension or withrenal arterial disease, plasma volume contracts (11..55AA, BB, CC)and renal parenchymal disease.
In contrast, patients with parenchymal disease of thekidney demonstrate an increased plasma volume as diastolicpressure increases (11..66) due to renal mechanisms subservingvolume expansion.
Pathophysiology: disease mechanisms6
1.3. The four pressure determinants of transcapillary fluidmigration elucidated by Starling.
1.4. The role of pre- and postcapillary tone in regulatingplasma volume. TPR, total peripheral resistance; PV,plasma volume; CPV, cardiopulmonary volume.
Hydrostaticpressure
Colloidosmoticpressure
Interstitial fluid
Precapillaryarterioles
Postcapillaryvenules
TPR CPV
PV
Capillary
Hypertension ch1 16/10/08 14:51 Página 6
Pathophysiology: disease mechanisms 7
1.5 Relationship between plasma volume and arterialpressure. Contraction of plasma volume in men withessential hypertension as diastolic (A) or mean arterial(B) pressures increase or as total peripheral resistanceincreases in male hypertensive patients with essentialhyprtension or renal arterial disease (C).
• Elevated haemoglobin concentration and haematocrit• Increased plasma protein concentration (e.g. albumin, fibrinogen)• Increased blood (and plasma) viscosity• Hyperuricaemia
Table 1.5 Clinically recognizable correlates of contractedintravascular (plasma) volume
80 90 100 110 120 130Systolic arterial pressure (mmHg)
32
22
21
20
19
18
17
16
15
14
13
12
Pla
sma
volu
me
(ml/c
m)
r = –0.468P = <0.001
90 100 110 120 130 140 150 160 170 180Mean arterial pressure* (mmHg)
*MAP – diastolic BP + 1/3 pulse pressure
25
20
15
Pla
sma
volu
me
(ml/c
m)
–30 –25 –20 –15 –10 –5 0 5 10 15 20Total blood volume (% normal)
80
70
60
50
40
30
20
Tota
l per
iphe
ral r
esis
tanc
e (u
nits
)co
rrec
ted
for
BS
A
A
B
C
Hypertension ch1 16/10/08 14:51 Página 7
High haematocrit and haemoglobinThe higher haematocrit and haemoglobin levels in essentialhypertension explain the clinical term ‘reactive’ or ‘relative’polycythaemia. This entity is frequently detected in patientswith essential hypertension and was first described byGaisböck at the turn of the twentieth century. Unlikepolycythaemia rubra vera, there is neither a leucocytosis orthrombocytosis, nor is there associated splenomegaly. Theelevated haemoglobin and haematocrit in Gaisböcksyndrome is classically described in the ‘ruddy’ patient withessential hypertension with contracted plasma volume. Thisrelative increase in red cell mass with a reduced plasmavolume has been measured in a large number of patientswith essential hypertension. In contrast, some patients havea volume-dependent essential hypertension in whom themagnitude of plasma volume is directly related to the heightof arterial pressure (Table 1.6).
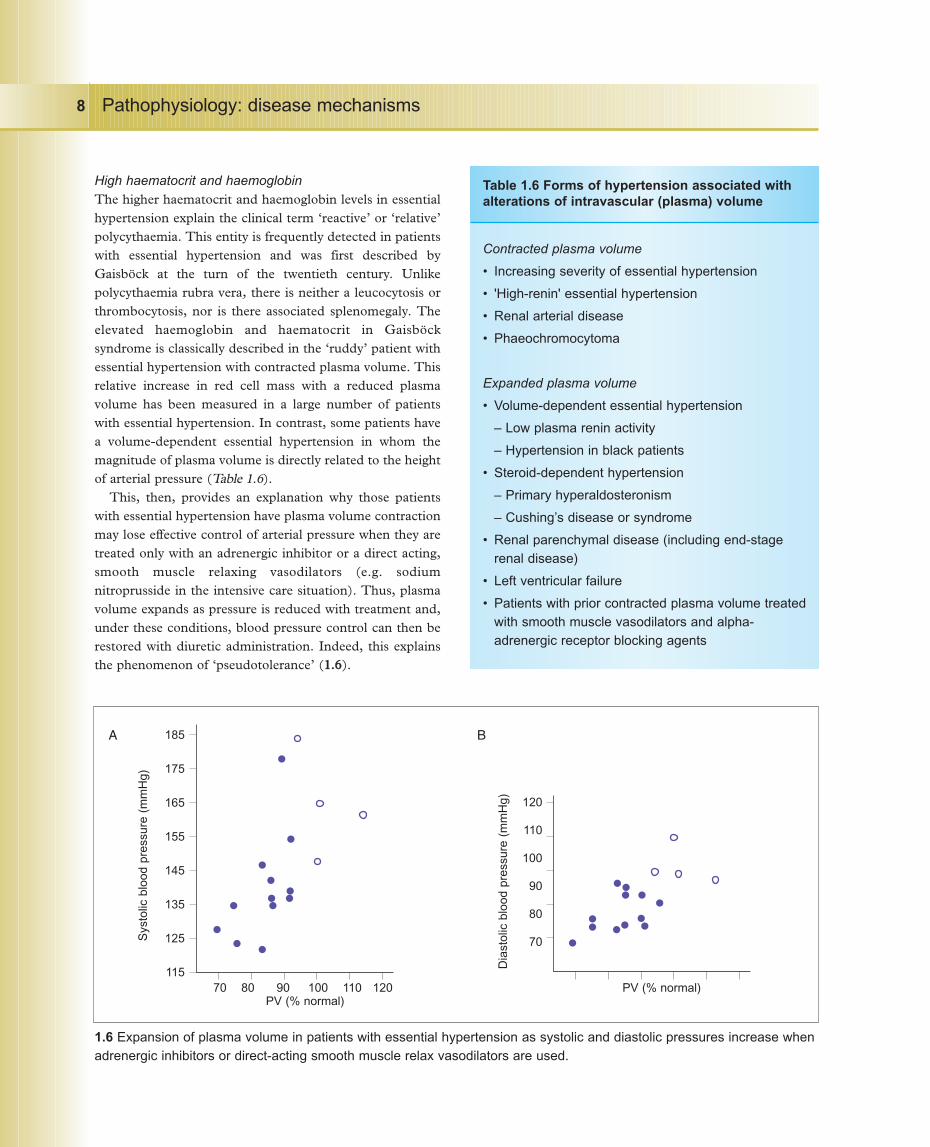
This, then, provides an explanation why those patientswith essential hypertension have plasma volume contractionmay lose effective control of arterial pressure when they aretreated only with an adrenergic inhibitor or a direct acting,smooth muscle relaxing vasodilators (e.g. sodiumnitroprusside in the intensive care situation). Thus, plasmavolume expands as pressure is reduced with treatment and,under these conditions, blood pressure control can then berestored with diuretic administration. Indeed, this explainsthe phenomenon of ‘pseudotolerance’ (11..66).
Pathophysiology: disease mechanisms8
Contracted plasma volume
• Increasing severity of essential hypertension
• 'High-renin' essential hypertension
• Renal arterial disease
• Phaeochromocytoma
Expanded plasma volume
• Volume-dependent essential hypertension
– Low plasma renin activity
– Hypertension in black patients
• Steroid-dependent hypertension
– Primary hyperaldosteronism
– Cushing’s disease or syndrome
• Renal parenchymal disease (including end-stage renal disease)
• Left ventricular failure
• Patients with prior contracted plasma volume treatedwith smooth muscle vasodilators and alpha-adrenergic receptor blocking agents
Table 1.6 Forms of hypertension associated withalterations of intravascular (plasma) volume
1.6 Expansion of plasma volume in patients with essential hypertension as systolic and diastolic pressures increase whenadrenergic inhibitors or direct-acting smooth muscle relax vasodilators are used.
70 80 90 100 110 120PV (% normal)
185
175
165
155
145
135
125
115
Sys
tolic
blo
od p
ress
ure
(mm
Hg)
PV (% normal)
120
110
100
90
80
70
Dia
stol
ic b
lood
pre
ssur
e (m
mH
g)
A B
Hypertension ch1 16/10/08 14:51 Página 8

OedemaA second clinical example of coincident pre- andpostcapillary vasoconstriction may be demonstrated in thosepatients with severe hypertensive retinopathy. It provides anexplanation for the transudation of protein through theretinal capillary bed in patients with acceleratedhypertension as well as those with papilloedema associatedwith malignant hypertension (see Chapter 2). A thirdexample relates to development of oedema in patientsreceiving calcium antagonists. This oedema is theconsequence not of renal-mediated fluid retention but,rather, of the potent drug-induced precapillary arteriolardilatation associated with reflex postcapillary constriction.This is particularly experienced with prolonged standing orwhen seated for a long time with the legs dependent.
High cardiac output hypertensionA fourth example of the phenomenon of pre- and post-capillary constriction provides, in part, a pathophysiologicalexplanation for the increased cardiac output and hyper-dynamic circulation observed during development ofessential hypertension. Thus, early in the elaboration ofhypertension (i.e. patients with borderline or ‘labile’hypertension), when blood pressure is elevated only at timesbut is normal at other times, cardiac output is increased.This increased output is related to the translocation of thecirculating intravascular volume from the periphery to thecentral circulation as a result of the postcapillary (i.e.venular) constriction. Although the total peripheralresistance at this stage is said to be ‘normal’, it has beensuggested that it is ‘inappropriately so’, since, should cardiacoutput become elevated to the same extent in normotensiveindividuals, their total peripheral resistance would be slightlyreduced. With progression of the hypertensive vasculardisease and, as the pre- and postcapillary vasoconstrictionincrease further, the intravascular (i.e. plasma) volumeprogressively contracts as described above. This contractionin circulating intravascular volume proportionallydiminishes the cardiopulmonary volume, decreases rightatrial venous return and, thus, the cardiac output is reducedto a more normal level than the output observed earlier inthe disease.
NephrosclerosisA fifth example, which has more recently become appreci-ated clinically, relates to the increased intraglomerular
hydrostatic pressure in patients with hypertensivenephrosclerosis (i.e. the Brenner hypothesis). Thus, bothafferent and efferent glomerular arteriolar constrictionoccurs in patients with prolonged systemic arterial hyper-tension, with renal parenchymal involvement favouringelevated glomerular hydrostatic capillary pressure,glomerular ultrafiltration of protein, and consequenthyalinosis and glomerulosclerosis. With therapeuticreduction of afferent and efferent arteriolar resistance (withangiotensin-converting enzyme inhibitors or angiotensin IIreceptor blockade), glomerular hydrostatic pressure will alsodiminish in association with reduced filtered protein andreversal or inhibition of further progression of glomerularsclerosis (see Chapter 6). These findings provide credibilityto the concept that angiotensin II participates in theprogression of nephrosclerosis in essential hypertension aswell as in diabetic renal disease; they also strongly suggestthat inhibition of angiotensin II confers significant benefit tothese patients.
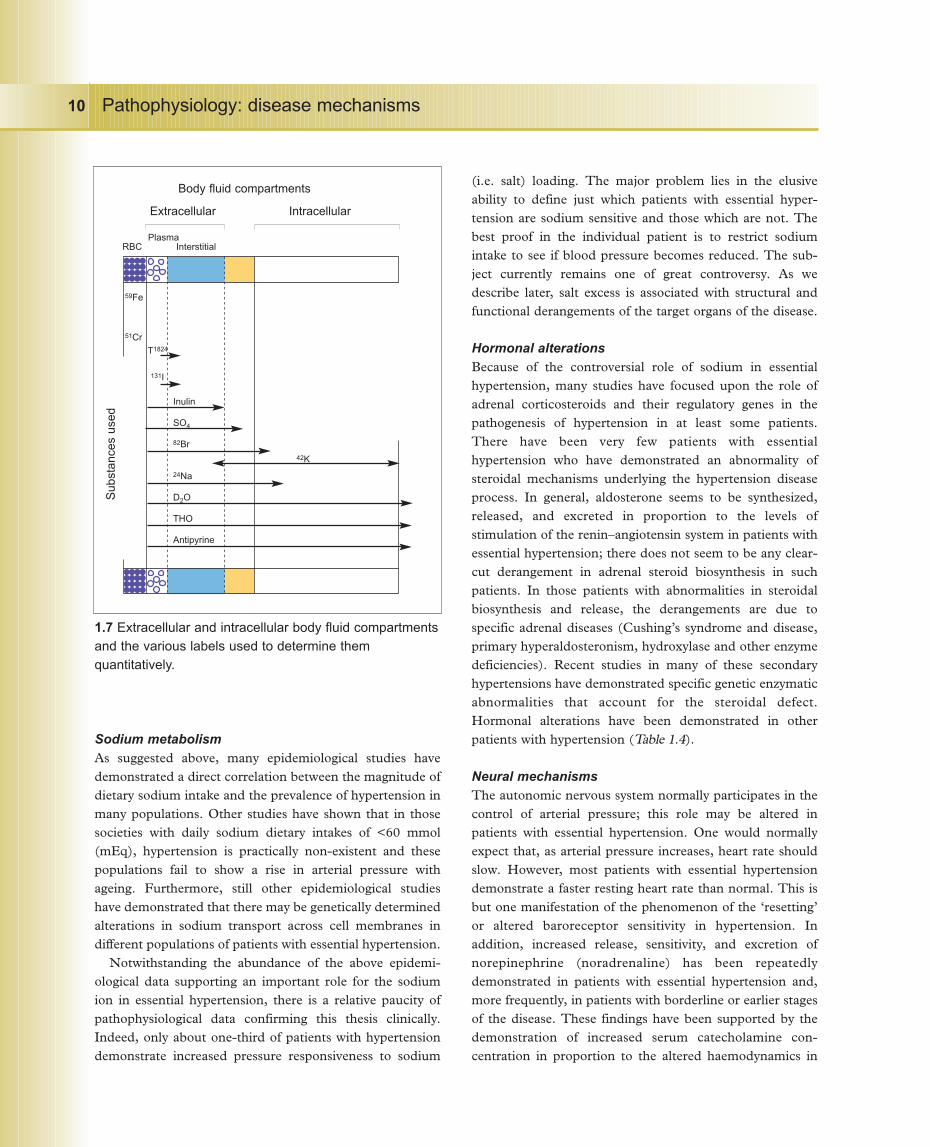
Fluid volume partitionsAs originally postulated by Starling, local haemodynamicand other pressure alterations are responsible for themovement of water across the major body fluidcompartments (11..33). These factors include the localcapillary hydrostatic and local tissue pressures as well as theprotein oncotic pressures, intravascularly and extra-vascularly. In general, total body water is normal in essentialhypertension and seems to be normally distributed betweenthe extracellular and intracellular fluid compartments.However, although there is much epidemiological evidencesuggesting deranged sodium handling in patients withhypertension, there is little evidence supporting the conceptthat total body sodium is increased in hypertensive diseaseor that it is associated with expanded total body water or,even, increased blood pressure sensitivity. In contrast,emerging data suggest other effects of sodium excess onheart, aorta, kidney, and vessels. In addition, there is goodclinical investigative evidence that the extracellular fluidvolume may be maldistributed in hypertension. Thus, asintravascular (i.e. plasma) volume becomes contracted inpatients with essential hypertension, it may be associatedwith greater interstitial fluid volume. This movement offluid from the intravascular to the extravascular (includinginterstitial) fluid compartments has specific pathophysiologicalimplications (11..77).
Pathophysiology: disease mechanisms 9
Hypertension ch1 16/10/08 14:51 Página 9
Sodium metabolismAs suggested above, many epidemiological studies havedemonstrated a direct correlation between the magnitude ofdietary sodium intake and the prevalence of hypertension inmany populations. Other studies have shown that in thosesocieties with daily sodium dietary intakes of <60 mmol(mEq), hypertension is practically non-existent and thesepopulations fail to show a rise in arterial pressure withageing. Furthermore, still other epidemiological studieshave demonstrated that there may be genetically determinedalterations in sodium transport across cell membranes indifferent populations of patients with essential hypertension.
Notwithstanding the abundance of the above epidemi-ological data supporting an important role for the sodiumion in essential hypertension, there is a relative paucity ofpathophysiological data confirming this thesis clinically.Indeed, only about one-third of patients with hypertensiondemonstrate increased pressure responsiveness to sodium
(i.e. salt) loading. The major problem lies in the elusiveability to define just which patients with essential hyper-tension are sodium sensitive and those which are not. Thebest proof in the individual patient is to restrict sodiumintake to see if blood pressure becomes reduced. The sub-ject currently remains one of great controversy. As wedescribe later, salt excess is associated with structural andfunctional derangements of the target organs of the disease.
Hormonal alterationsBecause of the controversial role of sodium in essentialhypertension, many studies have focused upon the role ofadrenal corticosteroids and their regulatory genes in thepathogenesis of hypertension in at least some patients.There have been very few patients with essentialhypertension who have demonstrated an abnormality ofsteroidal mechanisms underlying the hypertension diseaseprocess. In general, aldosterone seems to be synthesized,released, and excreted in proportion to the levels ofstimulation of the renin–angiotensin system in patients withessential hypertension; there does not seem to be any clear-cut derangement in adrenal steroid biosynthesis in suchpatients. In those patients with abnormalities in steroidalbiosynthesis and release, the derangements are due tospecific adrenal diseases (Cushing’s syndrome and disease,primary hyperaldosteronism, hydroxylase and other enzymedeficiencies). Recent studies in many of these secondaryhypertensions have demonstrated specific genetic enzymaticabnormalities that account for the steroidal defect.Hormonal alterations have been demonstrated in otherpatients with hypertension (Table 1.4).
Neural mechanismsThe autonomic nervous system normally participates in thecontrol of arterial pressure; this role may be altered inpatients with essential hypertension. One would normallyexpect that, as arterial pressure increases, heart rate shouldslow. However, most patients with essential hypertensiondemonstrate a faster resting heart rate than normal. This isbut one manifestation of the phenomenon of the ‘resetting’or altered baroreceptor sensitivity in hypertension. Inaddition, increased release, sensitivity, and excretion ofnorepinephrine (noradrenaline) has been repeatedlydemonstrated in patients with essential hypertension and,more frequently, in patients with borderline or earlier stagesof the disease. These findings have been supported by thedemonstration of increased serum catecholamine con-centration in proportion to the altered haemodynamics in
Pathophysiology: disease mechanisms10
1.7 Extracellular and intracellular body fluid compartmentsand the various labels used to determine themquantitatively.
Body fluid compartments
Extracellular Intracellular
Plasma RBC Interstitial
59Fe
51Cr
T1824
131I
Inulin
SO4
82Br
24Na
D2O
THO
Antipyrine
42K
Sub
stan
ces
used
Hypertension ch1 16/10/08 14:51 Página 10

these patients. The elevation of serum catecholamineconcentration in these patients, however, is not nearly ashigh as in patients with phaeochromocytoma.
It is of interest that in patients with less severe essentialhypertension, particularly those with a hyperdynamic beta-adrenergic circulatory state (with or without idiopathicmitral valve prolapse syndrome), serum norepinephrine(noradrenaline) concentration is frequently elevated. Thisfinding provides one explanation for the altered haemo-dynamic findings as well as the augmented myocardialcontractility, the idiopathic mitral valve prolapse, and theassociated cardiac dysrhythmias. In general, there have beenno alterations reported in catecholamine biosynthesis or inrelease or reuptake of these substances, although increasedresponsiveness of beta-adrenergic receptor sites has beenreported (see Chapter 5). Furthermore, the reported alteredresponses to upright tilting, Valsalva manoeuvres, andtyramine stimulation of norepinephrine (noradrenaline)release from nerve endings may provide a useful indicationof adrenergic neural participation in certain patients withessential hypertension.
Several years ago, the clonidine suppression test wasintroduced to differentiate patients with phaeochromo-cytoma from those patients with essential hypertension (whodemonstrate smaller elevations of plasma catecholamines).Clonidine (a centrally acting adrenergic inhibitor) admini-stration will suppress elevated catecholamine levels to
normal levels in patients with essential hypertension but notin those with phaeochromocytoma.
Renopressor system
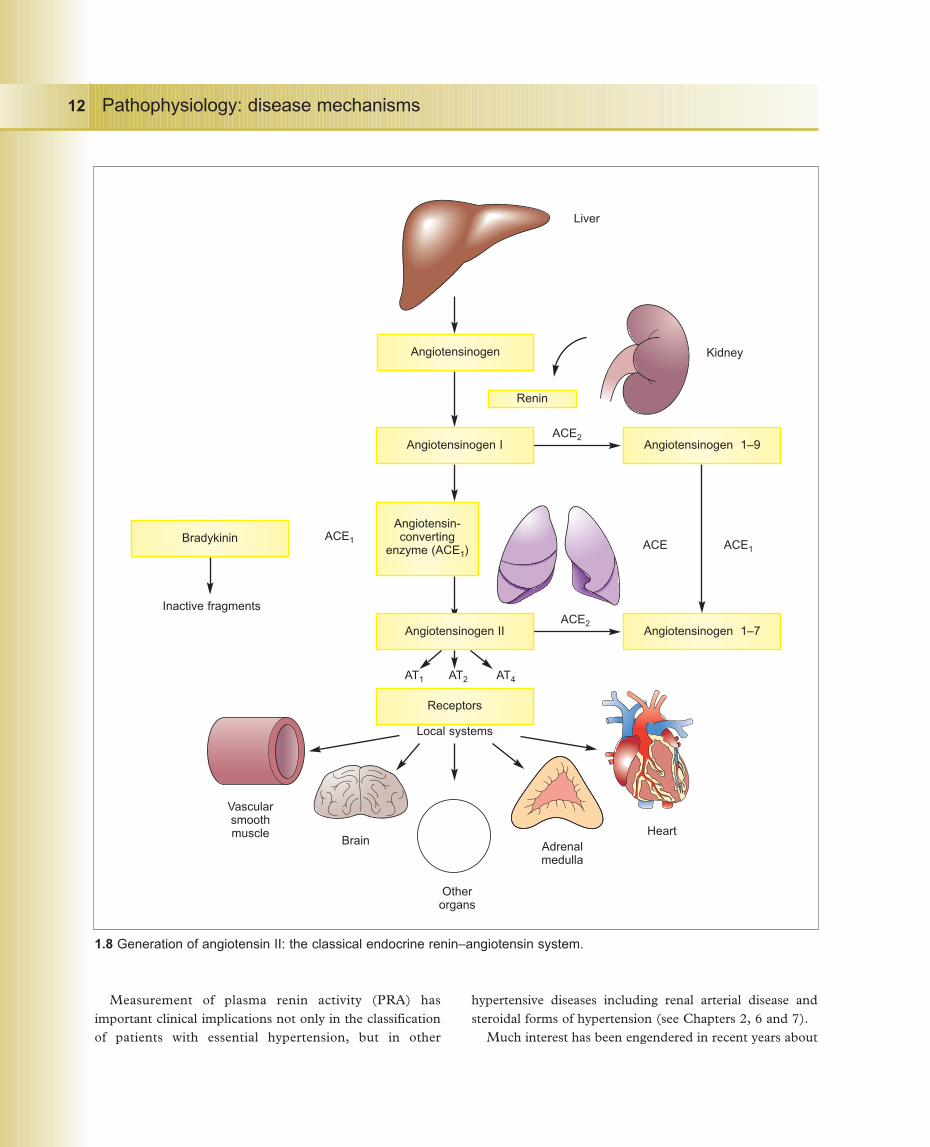
The enzyme renin is released from the juxtaglomerularapparatus of the kidney through several mechanisms (Table1.7). Renin acts on its circulating peptide substrateangiotensinogen, produced in the liver, resulting in thegeneration of the pressor octapeptide angiotensin II (11..88). Theoctapeptide apparently generates other peptides whose actionsare under active investigation. Angiotensin II has a number ofsites of action, most notably in blood vessels and adrenalcortex, to produce vasoconstriction and aldosterone release,respectively. In addition, angiotensin is also generated locallyin heart, vessels, kidneys, and other organs with specific localactions (Table 1.8). The precise roles for these local systems arenot yet clearly known but intracellular generation ofangiotensin II affects muscle protein synthesis, with inherentimplications relating to the development or reversal of vascularand ventricular hypertrophy. Local generation of angiotensinII may be of particular importance in: (a) the function of thecardiac or arteriolar myocyte which produces the peptide (anintracrine function); (b) the effect on neighbouring cells (anautocrine function); or (c) association with other hormones(e.g. kinins, catecholamines, atrial natriuretic peptide,endothelin) within that organ (a paracrine function) (11..99).
Pathophysiology: disease mechanisms 11
• Reduced renal blood flow and/orperfusion pressure
• Contracted intravascular volume
• Dietary sodium restriction (<100 mmol[mEq]/day)
• Increased beta-adrenergically mediatedneural input
• Reduced aldosterone levels in blood
• Upright posture
• Hormones or humoral agents (e.g.catecholamines)
• Drugs (e.g. diuretics)
Table 1.7 Mechanisms of increased renin release from the kidney
Site ActionVascular smooth muscle VasoconstrictionAdrenal medulla Release of catecholaminesAdrenal cortex AldosteroneMedulla of brain ThirstMedullary centres Augment adrenergic outflowParavertebral ganglia Augment norepinephrine
(noradrenaline) releaseLocal synthesis of angiotensin II in:Heart Myocytic hypertrophy, fibrosis,
apoptosisBrain Adrenergic outflowArteries Myocytic hypertrophy, fibrosisOther organs (uterus, liver, To be resolvedsalivary glands)
Table 1.8 Sites of action of angiotensin II
Hypertension ch1 16/10/08 14:51 Página 11
Pathophysiology: disease mechanisms12
1.8 Generation of angiotensin II: the classical endocrine renin–angiotensin system.
Liver
Kidney
HeartAdrenalmedulla
Otherorgans
Brain
Vascularsmoothmuscle
Angiotensinogen
Angiotensin-converting
enzyme (ACE1)
Receptors
Angiotensinogen 1–7
Angiotensinogen 1–9
Bradykinin
Angiotensinogen I
Angiotensinogen II
ACE2
ACE ACE1
ACE2
ACE1
Inactive fragments
AT1 AT2 AT4
Local systems
Renin
Measurement of plasma renin activity (PRA) hasimportant clinical implications not only in the classificationof patients with essential hypertension, but in other
hypertensive diseases including renal arterial disease andsteroidal forms of hypertension (see Chapters 2, 6 and 7).
Much interest has been engendered in recent years about
Hypertension ch1 16/10/08 14:51 Página 12
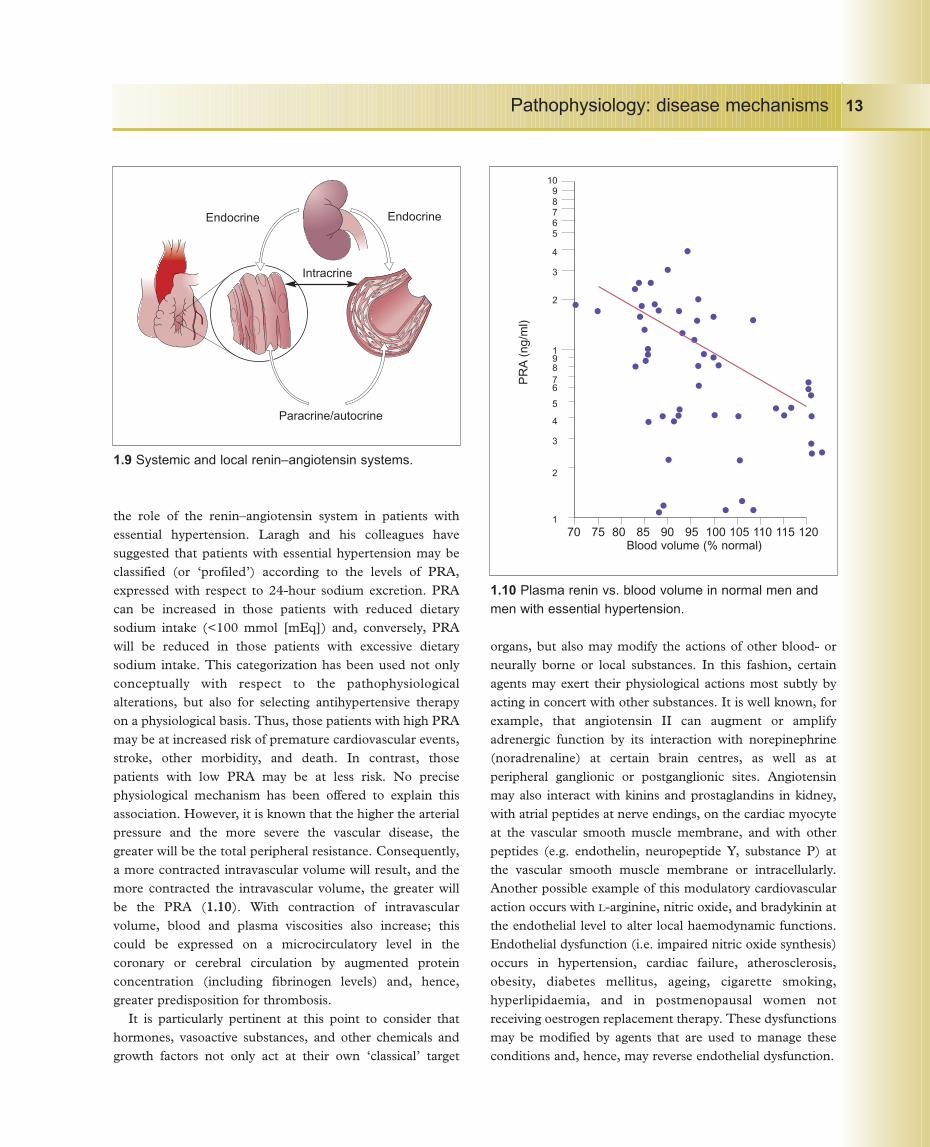
the role of the renin–angiotensin system in patients withessential hypertension. Laragh and his colleagues havesuggested that patients with essential hypertension may beclassified (or ‘profiled’) according to the levels of PRA,expressed with respect to 24-hour sodium excretion. PRAcan be increased in those patients with reduced dietarysodium intake (<100 mmol [mEq]) and, conversely, PRAwill be reduced in those patients with excessive dietarysodium intake. This categorization has been used not onlyconceptually with respect to the pathophysiologicalalterations, but also for selecting antihypertensive therapyon a physiological basis. Thus, those patients with high PRAmay be at increased risk of premature cardiovascular events,stroke, other morbidity, and death. In contrast, thosepatients with low PRA may be at less risk. No precisephysiological mechanism has been offered to explain thisassociation. However, it is known that the higher the arterialpressure and the more severe the vascular disease, thegreater will be the total peripheral resistance. Consequently,a more contracted intravascular volume will result, and themore contracted the intravascular volume, the greater willbe the PRA (11..1100). With contraction of intravascularvolume, blood and plasma viscosities also increase; thiscould be expressed on a microcirculatory level in thecoronary or cerebral circulation by augmented proteinconcentration (including fibrinogen levels) and, hence,greater predisposition for thrombosis.
It is particularly pertinent at this point to consider thathormones, vasoactive substances, and other chemicals andgrowth factors not only act at their own ‘classical’ target
organs, but also may modify the actions of other blood- orneurally borne or local substances. In this fashion, certainagents may exert their physiological actions most subtly byacting in concert with other substances. It is well known, forexample, that angiotensin II can augment or amplifyadrenergic function by its interaction with norepinephrine(noradrenaline) at certain brain centres, as well as atperipheral ganglionic or postganglionic sites. Angiotensinmay also interact with kinins and prostaglandins in kidney,with atrial peptides at nerve endings, on the cardiac myocyteat the vascular smooth muscle membrane, and with otherpeptides (e.g. endothelin, neuropeptide Y, substance P) atthe vascular smooth muscle membrane or intracellularly.Another possible example of this modulatory cardiovascularaction occurs with L-arginine, nitric oxide, and bradykinin atthe endothelial level to alter local haemodynamic functions.Endothelial dysfunction (i.e. impaired nitric oxide synthesis)occurs in hypertension, cardiac failure, atherosclerosis,obesity, diabetes mellitus, ageing, cigarette smoking,hyperlipidaemia, and in postmenopausal women notreceiving oestrogen replacement therapy. These dysfunctionsmay be modified by agents that are used to manage theseconditions and, hence, may reverse endothelial dysfunction.
Pathophysiology: disease mechanisms 13
1.9 Systemic and local renin–angiotensin systems.
1.10 Plasma renin vs. blood volume in normal men andmen with essential hypertension.
Endocrine Endocrine
Intracrine
Paracrine/autocrine
70 75 80 85 90 95 100 105 110 115 120Blood volume (% normal)
1098765
4
3
2
19876
5
4
3
2
1P
RA
(ng/
ml)
Hypertension ch1 16/10/08 14:51 Página 13

Further reading
Ross RC, Bowen-Pope DP, Raines EW: Platelets,macrophages, endothelium, and growth factors. Theireffects upon cells and their possible roles in atherogenesis.In: Atherosclerosis. KT Lee (ed). Annals N.Y. Acad. Sci.1985;445544:254–260. The first report demonstrating that theinitial functional derangement of the ventricle (myocyticstretch) initiates the process of hypertrophy through stimulatingDNA-mediated protein synthesis. It provides a model formany subsequent studies.
Libby P, Warner SJC, Salomon RN, Birinyi LK: Productionof platelet-derived growth factor-like mitogen by smoothmuscle cells from human atheroma. N. Engl. J. Med.1988;331188:1493–1498.
Sarzani R, Arnaldi G, Takasaki 1, Brecher P, ChobanianAV: Effects of hypertension and aging on platelet-derivedgrowth factor and platelet-derived growth factor receptorexpression in rat aorta and heart. Hypertension1991;1188(Suppl. 111):93–99.
These two references provide excellent discussions on how localvascular growth factors participate in atherogenesis. Mostinterestingly, these mitogenic factors in atherosclerosis may bethe same factors that participate in hypertension, therebyoffering a conceptual explanation as to how one diseaseexacerbates the other.
Page IH: Hypertension Mechanisms. Grune and Stratton,Orlando, FL; 1987.
Page IH: Pathogenesis of arterial hypertension. ].A.M.A.1949;114400:451–458.
Frohlich ED: (State of the Art): The first Irvine H. Pagelecture: The mosaic of hypertension: past, present, andfuture. J. Hypertension 1988;66(Suppl. 4):S2–S11. Thesethree references provide discussions on the mosaic concept ofPage relating to the multifactorial nature of hypertension andleft ventricular hypertrophy.
Frohlich ED, Apstein C, Chobanian AV, et al.: The heart inhypertension. N. Engl. J. Med. 1992;332277:998–1008.Summary of the heart in hypertension by working group of theNational Heart, Lung, and Blood Institute.
Frohlich ED, Kozul Vj, Tarazi RC, Dustan HP:Physiological comparison of labile and essentialhypertension. Circ. Res. 1970;2277(l):55–69.
Frohlich ED, Tarazi RC, Dustan HP: Clinical-physiologicalcorrelations in the development of hypertensive heartdisease. Circulation 1971;4444:446–455.
Dunn FG, Chandraratna P, de Carvalho JGR, Basta LL,Frohlich ED: Pathophysiologic assessment ofhypertensive heart disease with echocardiography. Am. J.Cardiol. 1977;3399:789–795. These three references are clinicalpathophysiological studies describing the development of labileand essential hypertension. The third reference provides thatfirst support to the former discussions on the clinical, structural,and functional progression of hypertensive heart disease.
Tarazi RC, Dustan HP, Frohlich ED, Gifford RW Jr,Hoffman GC: Plasma volume and chronic hypertension.Relationship to arterial pressure levels in different hyper-tensive diseases. Arch. Intern. Med. 1970;112255:835–842.
Tarazi RC: Haemodynamic role of extracellular fluidvolume. Circ. Res. 1976; 3388(Suppl 11):73–83.
Dustan HP, Tarazi RC, Frohlich ED: Functional correlatesof plasma renin activity in hypertensive patients.Circulation 1970;4411:555–567. These three references arestudies that develop the concept of fluid volume alterations inclinical hypertensionand the functional correlates of PRA inpatients with essential hypertension.
Sealeyj E, Laragh JH: The renin–angiotensin–aldosteronesystem for normal regulation of blood pressure andsodium and potassium homeostasis. In: Hypertension:Pathophysiology, Diagnosis, and Management. JH Laragh,BM Brenner (eds). Raven Press, New York, 1990,pp.1287–1317.
Bühler FR, Laragh JH, Baer L, Vaughan ED Jr, BrunnerHR: Propranolol inhibition of renin secretion: a specificapproach to diagnosis and treatment of renin-dependent hypertensive diseases. N. Engl. J. Med.1972;228877:1209–1214. These references introduce the conceptand therapeutic rationale for the profiling of PRA inhypertension.
Alderman MH, Madhavan S, Ooi WL, Cohan H, Sealey JE,Laragh JH: Association of the renin sodium profile withthe risk of myocardial infarction in patients withhypertension. N. Engl. J. Med. l991;332244:1098–1104. Thisreference and Bohler et al. (1972) profile PRA to hypertensiveoutcomes.
Pathophysiology: disease mechanisms14
Hypertension ch1 16/10/08 14:51 Página 14