Embed Size (px)
Citation preview

An Audit of Death Certification at a District General Hospital
Hannah BarrettMedical Student
Imperial College London

The Question
• How well are death certificates completed at University Hospital of North Durham?
• Do doctors need further advice on how to complete death certificates correctly?

Method
• First 100 death certificates in July– mortuary records
• Recorded – date of death– ward – cause of death cascade

Method
• Cause of death cascades were reviewed and graded– Two histopathologists separately
• Disagreement– Consensus meeting (third tie breaker)

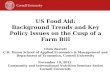
Grading
Part 1
Logical certificate, completed appropriately (1)
Logical certificate but with minor errors (2)
Illogical or inappropriately completed certificate (3)
Certificate completed in a manner which should have been rejected by the Registrar (4)

Grade 1 Grade 3
1a Pneumonia
b Immobility
c Stroke
2 Peripheral vascular disease
1a Lung cancer
b Advanced dementia, frailty of old age and anaemia
c Chest infection

Grading
Part 2
Correctly used
Contained information which should have been included in Part I
Irrelevant information included
Contained information both non-specific and incorrect

Grading
49
15
31
5
1
2
3
4

Use of Part 2
38
29
29
4Irrelevant
OK
Part I
Non specif icand w rong

Number of deaths in each ward over the study time period
0
5
10
15
20
25
Res
pira
tory
Eld
erly
car
e
Car
diol
ogy/
Dia
bete
s
Med
ical
Adm
issi
ons
Gas
troe
nter
olog
y
Eld
erly
car
e/D
emen
tia/
Rhe
umat
olog
y
Sur
gica
l war
ds(c
ombi
ned)
Oth
er
Ward
Nu
mb
er o
f d
eath
s

By organ system
9
18
33
15
25 Elderly
GI/Gastro
Respiratory
Other
Cardiovascular

Difficult certificates
% Pneum Sepsis FoOA CVD Neop
1 25.5 28.6 21.7 58.3 69.2
2 4.3 57.1 34.8 25.0 7.7
3 63.8 0 34.8 16.7 15.4
4 6.4 14.3 8.7 0 7.7

Inter-observer variation
• 23 cases rated differently
• Fleiss kappa results = 0.63 – Substantial agreement

Complexity
• Was a longer (? more complicated) certificate more likely to be wrong?

Training
• Already received– Undergraduate instruction– Preparing for practice– Induction– Interactive session early in training

Conclusions
• Despite efforts to educated junior doctors avoidable errors are frequently made– Guidance (ONS) Sept 08
• Part II often a waste paper basket

Conclusions
• Poor– Infections (especially pneumonia) – Frailty of old age
• Good– Malignancy – Cardiovascular

Action
• Focused interactive session• Further interventions
– Individual performance data– Approachable source of assistance– Formal policy potentially leading to remedial
action– Discussion group session
• Reaudit
























![[PVG] Hannah Montana - Hannah Montana 3](https://img.pdfslide.net/doc/110x75/56d6bf381a28ab30169562c0/pvg-hannah-montana-hannah-montana-3.jpg)



