Embed Size (px)
Citation preview

AN ECOLOGICAL APPROACH TO PLANNINGDYSFUNCTION: SCRIPT EXECUTION
Mathilde Chevignard1, Bernard Pillon2, Pascale Pradat-Diehl1, Chantal Taillefer1,Sylvie Rousseau1, Catherine Le Bras2 and Bruno Dubois2
(1Service de Rééducation Neurologique, 2INSERM EPI 007 and Fédération de Neurologie,Hôpital de la Salpêtrière, Paris, France)
ABSTRACT
Planning, which concerns many activities in everyday life, is a two-stage process. Thefirst one predetermines a course of actions aimed at achieving some specific goals. It isfounded on managerial knowledge or overlearned sequences of events and may be testedby script generation. The second stage entails monitoring and guiding the execution of theplan to a successful conclusion. It must take into account environmental contingencies andmay be tested by script execution. If the frontal lobes intervene not only in managerialknowledge (Grafman, 1989) but also in binding the plan with contextual environment(Damasio, Tranel and Damasio, 1991; Shallice and Burgess, 1991), script execution wouldbe more sensitive than script generation to planning deficits. To test this hypothesis, scriptexecution and script generation were compared in 11 patients with a dysexecutive syndromeand 10 matched controls, using three scripts of daily life activities: (1) ‘shopping forgroceries’; (2) ‘cooking’; (3) ‘answering a letter and finding the way to post the reply’.Two way ANOVAs showed more errors in execution than in generation, more errors inpatients than in controls, and a greater difference between execution and generation inpatients than in controls. Furthermore, ‘context neglect’ and ‘environmental adherence’were the two types of errors that best differentiated patients from controls. Finally, the totalnumber of errors in execution correlated with the score on behavioral questionnairesanswered by occupational therapists. These results confirm our hypothesis and suggest thatscript execution may be a valid ecological approach to estimate the severity of deficits indaily life activities.
Key words: script generation and execution, planning, dysexecutive syndrome,ecological approach, frontal lobe lesions, closed brain injury
INTRODUCTION
Planning is the ability to organize behavior in relation to a goal that must beachieved through a series of intermediate steps (Luria, 1966; Owen, 1997). Thisability is currently assessed with laboratory tests, such as maze tracing (Porteus,1959; Karnath, Wallesch and Zimmerman, 1991) and problem resolution (Luria,1966; Lhermitte, Derouesné and Signoret, 1972; Klosowska, 1976), including theTower of London Task (Shallice, 1982, 1988). The performance of patients withfrontal lobe lesions on such tests is regularly impaired (Owen, Downes,Sahakian et al., 1990; Morris, Miotto, Feigenbaum et al., 1997), underlining therole of the dorsolateral prefrontal cortex in cognitive organization (Stuss, Eskesand Foster, 1994). This cognitive role has recently been confirmed by PETstudies of normal subjects resolving Tower Tasks (Baker, Rogers, Owen et al.,
Cortex, (2000) 36, 649-669
1996; Owen, Doyon, Petrides et al., 1996). Planning is also important forbehavioral adaptation in daily life. For example, following frontal lobe surgery awoman failed to prepare an entire family meal, although she was capable ofcooking the individual dishes (Penfield and Evans, 1935). Since this description,several neuropsychological studies showed that daily life activities might beimpaired despite normal cognitive performance in the laboratory (Eslinger andDamasio, 1985; Shallice and Burgess, 1991). As underlined by the latter, thedifference might be due to the need of maintaining the plan over longer periodsof time in the face of competing alternatives in daily life situations.
However, assessing planning in daily life is difficult. Due to a reduction ininsight associated with frontal lobe lesions (Stuss, 1991; Prigatano, 1991),patients generally underestimate their functional impairment in everydaysituations. Relative’s or caregiver’s rating on behavioral scales (Lhermitte, Pillonand Serdaru, 1986) has been found to correlate with the metabolism of specificregions of the frontal cortex, namely orbitofrontal areas (Sarazin, Pillon,Giannakopoulos et al., 1998). Rating depends, however, on subjective feelingsand many caregivers also tend to underestimate the patient’s deficits. Therefore,more objective evaluations have been proposed, such as the Six Element or theMultiple Errands Tests (Shallice and Burgess, 1991), the Executive FunctionRoute Finding Test (Boyd and Sautter, 1993) or the Behavioural Assessment ofthe Dysexecutive Syndrome (Wilson, Evans, Emslie et al., 1998). Althoughecologically valid, these tests show a great variability of performance even innormal controls, some of them being as severely impaired as patients withfrontal-lobe lesions (Levine, Stuss, Milberg et al., 1998). The impairedperformance of normal subjects on these tasks underlines the importance ofusing more familiar plans of actions in order to limit the inter-individualvariability of normal control subjects and allow a better differentiation betweenpatients and controls. Naturalistic actions, even as simple as preparing a slice oftoast with butter and jam or packing a lunchbox, may be impaired in patientswith brain lesions, at least in cases of closed head injury (Schwartz,Montgomery, Buxbaum et al., 1998).
One recent cognitive model postulates that planning deficits are related toimpairments in a domain specific to managerial knowledge involved in therepresentation and manipulation of script-like structures (Grafman, 1989).Managerial Knowledge Units would be overlearned sequences of events with abeginning and a end and a hierarchical organization going from more abstract(eating to a restaurant) to more concrete levels (paying the bill). Frontal lobelesions would specifically affect this kind of representations. In agreement withthis hypothesis, script generation and sorting has been shown to be impaired inpatients with frontal-lobe lesions (Le Gall, Aubin, Alain et al., 1993; Godboutand Doyon, 1995). In previous studies, we found that these patients made errorsin ordering actions in the correct temporal sequence, failed to close scripts andremain within the stated boundaries, and made deviant estimates of actionimportance (Sirigu, Zalla, Pillon et al., 1995, 1996).
Script generation, which is mainly based on the ability to access script-related content, only involves the first stage of planning, i.e. thepredetermination of a course of action aimed at achieving some goal. The
650 Mathilde Chevignard and Others
second stage entails self-monitoring and guiding the execution of the plan to asuccessful conclusion (Hayes-Roth and Hayes-Roth, 1979). Two qualitativelydistinct processes could determine which particular schema of action would beactivated at a given moment of the script execution: an automatic process, theContention Scheduling, which would operate in familiar situations, and acontrolled process, the Supervisory Attentional System, which is thought tomodulate operations when situations are unfamiliar (Shallice, 1988). The twoprocesses could allow integration between plan execution and environmentalcontingencies by operations such as marker creation, marker triggering andevaluation of the consequences of action. Only the Supervisory AttentionalSystem would depend on the prefrontal cortex (Damasio, Tranel and Damasio,1991; Shallice and Burgess, 1991; Verin, Partiot, Pillon et al., 1993; Dubois,Levy, Verin et al., 1995).
If the frontal lobes are indeed involved in both managerial knowledge andmonitoring of action, script execution would be more sensitive than scriptgeneration to planning dysfunction. The first aim of the study was to test thishypothesis by comparing execution and generation of relatively familiar scripts,such as ‘shopping for groceries’, ‘cooking’ and ‘answering a letter and findingthe way to post the reply’ . The second aim of the study was to evaluate thevalidity of such script execution as an ecological approach to deficits of dailylife activities and to test the hypothesis that it provides a more reliable indicationof dysexecutive deficits in real life than performance in cognitive tests.
MATERIALS AND METHODS
Subjects
Patients
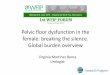
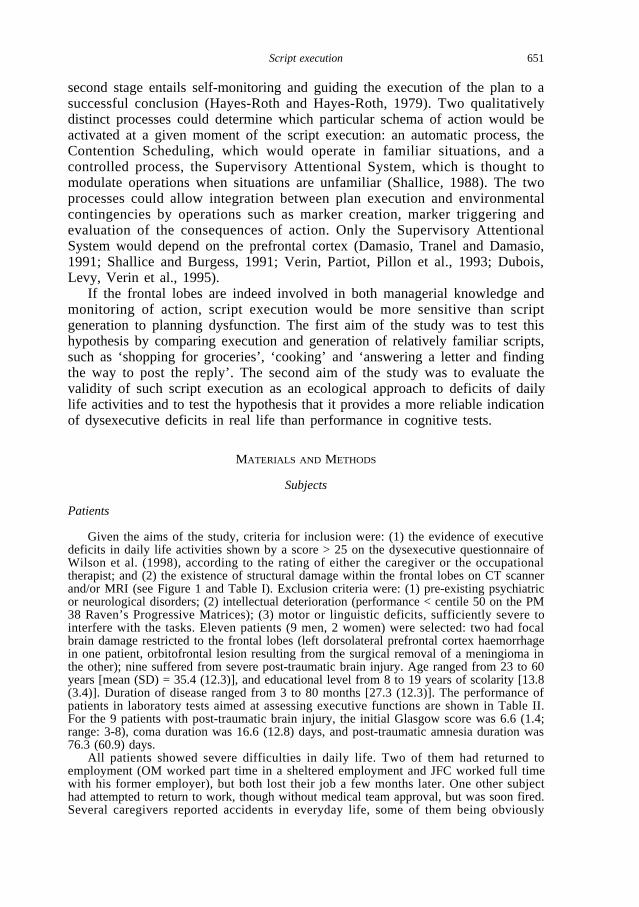
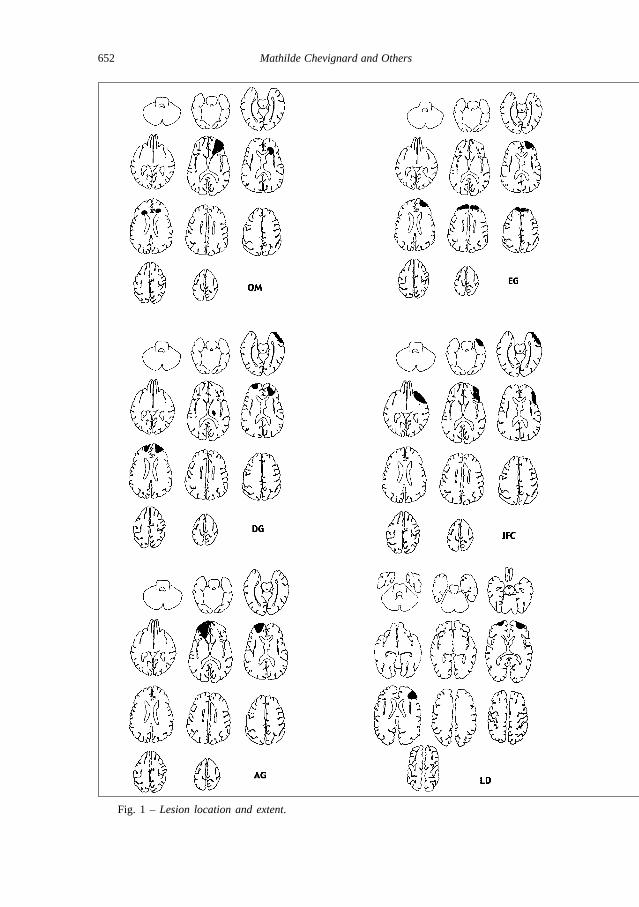
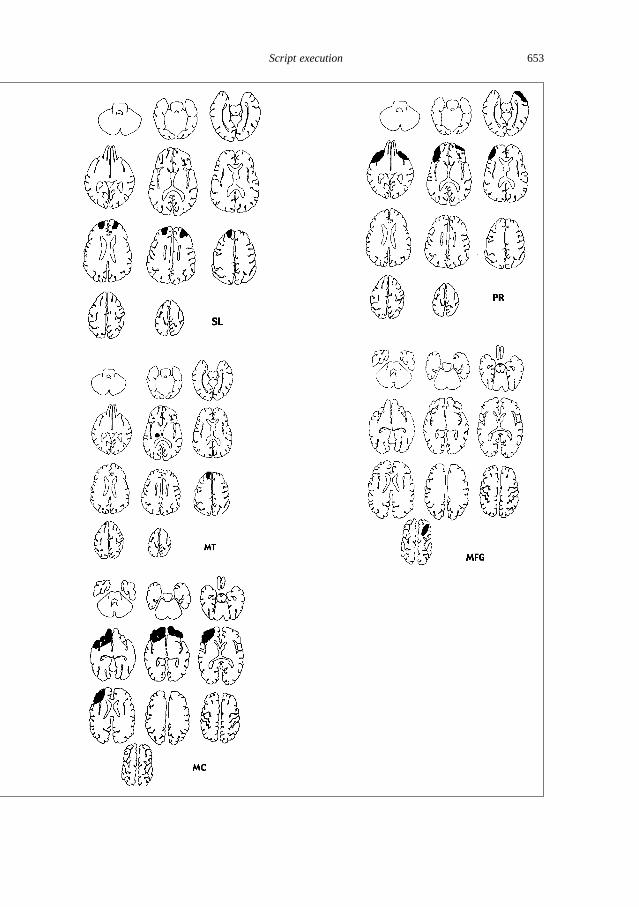
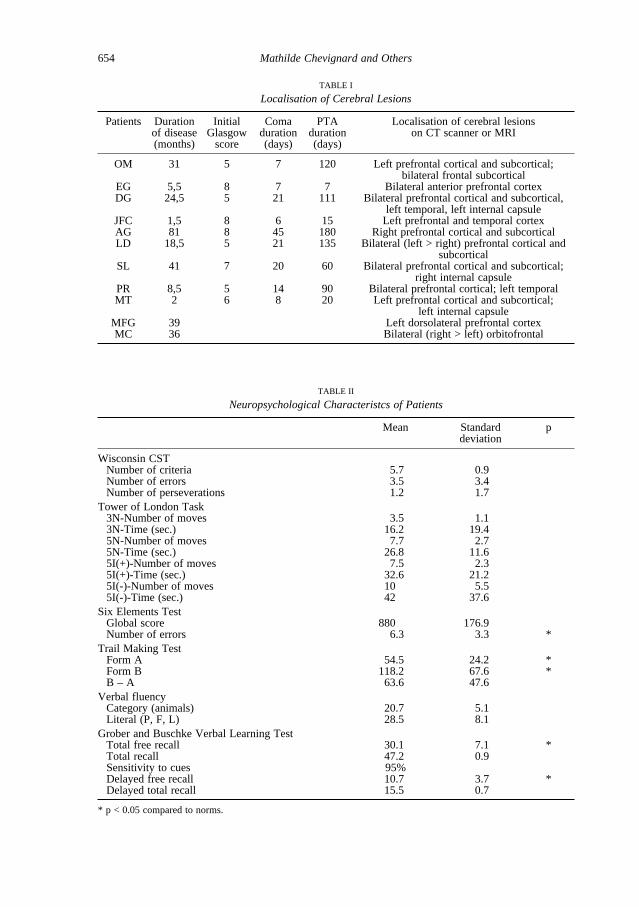
Given the aims of the study, criteria for inclusion were: (1) the evidence of executivedeficits in daily life activities shown by a score > 25 on the dysexecutive questionnaire ofWilson et al. (1998), according to the rating of either the caregiver or the occupationaltherapist; and (2) the existence of structural damage within the frontal lobes on CT scannerand/or MRI (see Figure 1 and Table I). Exclusion criteria were: (1) pre-existing psychiatricor neurological disorders; (2) intellectual deterioration (performance < centile 50 on the PM38 Raven’s Progressive Matrices); (3) motor or linguistic deficits, sufficiently severe tointerfere with the tasks. Eleven patients (9 men, 2 women) were selected: two had focalbrain damage restricted to the frontal lobes (left dorsolateral prefrontal cortex haemorrhagein one patient, orbitofrontal lesion resulting from the surgical removal of a meningioma inthe other); nine suffered from severe post-traumatic brain injury. Age ranged from 23 to 60years [mean (SD) = 35.4 (12.3)], and educational level from 8 to 19 years of scolarity [13.8(3.4)]. Duration of disease ranged from 3 to 80 months [27.3 (12.3)]. The performance ofpatients in laboratory tests aimed at assessing executive functions are shown in Table II.For the 9 patients with post-traumatic brain injury, the initial Glasgow score was 6.6 (1.4;range: 3-8), coma duration was 16.6 (12.8) days, and post-traumatic amnesia duration was76.3 (60.9) days.
All patients showed severe difficulties in daily life. Two of them had returned toemployment (OM worked part time in a sheltered employment and JFC worked full timewith his former employer), but both lost their job a few months later. One other subjecthad attempted to return to work, though without medical team approval, but was soon fired.Several caregivers reported accidents in everyday life, some of them being obviously
Script execution 651
652 Mathilde Chevignard and Others
Fig. 1 – Lesion location and extent.
Script execution 653
654 Mathilde Chevignard and Others
TABLE I
Localisation of Cerebral Lesions
Patients Duration Initial Coma PTA Localisation of cerebral lesionsof disease Glasgow duration duration on CT scanner or MRI(months) score (days) (days)
OM 31 5 7 120 Left prefrontal cortical and subcortical;bilateral frontal subcortical
EG 5,5 8 7 7 Bilateral anterior prefrontal cortexDG 24,5 5 21 111 Bilateral prefrontal cortical and subcortical,
left temporal, left internal capsuleJFC 1,5 8 6 15 Left prefrontal and temporal cortexAG 81 8 45 180 Right prefrontal cortical and subcorticalLD 18,5 5 21 135 Bilateral (left > right) prefrontal cortical and
subcorticalSL 41 7 20 60 Bilateral prefrontal cortical and subcortical;
right internal capsulePR 8,5 5 14 90 Bilateral prefrontal cortical; left temporalMT 2 6 8 20 Left prefrontal cortical and subcortical;
left internal capsuleMFG 39 Left dorsolateral prefrontal cortexMC 36 Bilateral (right > left) orbitofrontal
TABLE II
Neuropsychological Characteristcs of Patients
Mean Standard pdeviation
Wisconsin CSTNumber of criteria 5.7 0.9Number of errors 3.5 3.4Number of perseverations 1.2 1.7
Tower of London Task3N-Number of moves 3.5 1.13N-Time (sec.) 16.2 19.45N-Number of moves 7.7 2.75N-Time (sec.) 26.8 11.65I(+)-Number of moves 7.5 2.35I(+)-Time (sec.) 32.6 21.25I(-)-Number of moves 10 5.55I(-)-Time (sec.) 42 37.6
Six Elements TestGlobal score 880 176.9Number of errors 6.3 3.3 *
Trail Making TestForm A 54.5 24.2 *Form B 118.2 67.6 *B – A 63.6 47.6
Verbal fluencyCategory (animals) 20.7 5.1Literal (P, F, L) 28.5 8.1
Grober and Buschke Verbal Learning TestTotal free recall 30.1 7.1 *Total recall 47.2 0.9Sensitivity to cues 95%Delayed free recall 10.7 3.7 *Delayed total recall 15.5 0.7
* p < 0.05 compared to norms.
abnormal. One patient (DG), previously an engineering student, suffered burns while tryingto make holes in plastic bottles with a screwdriver previously heated on the stove; he thentook a shower ‘for 21 minutes’ and went to bed without calling a doctor, despite havingthird degree burns on all the upper part of his body. Although the caregivers were able tosignal behavioral disorders, they currently underestimated their importance and potentialconsequences: the score of the patients on the dysexecutive questionnaire (Wilson et al.,1998) was 26.9 (12.9) when rated by the caregivers versus 35.3 (13.0) when rated byoccupational therapists.
Controls
The control group comprised ten subjects with no history of neurological or psychiatricdisease. They were matched for sex (8 males, 2 females), age [31.6 (9.4) years] andeducation level [15.0 (2.1) years] with the frontal patients.
All subjects gave informed consent.
Script Presentation
We chose scripts among current activities of daily life. They had to be complex enoughto be sensitive to impaired dysexecutive functions and to be feasible in a rehabilitationcenter, over a relatively short time period. Three scripts were studied: (1) shopping forgroceries; (2) preparing two recipes of different levels of difficulty (scrambled eggs for twoand a chocolate cake); a written recipe was only proposed for the cake, as cookingscrambled eggs is easy, even without a wide experience of cooking; and (3) answering aletter and finding one’s way to a given post-box to post the reply. The familiarity of eachsubject with the scripts was previously controlled using a 3-point scale (0-2): never (0),sometimes (1), often put into practice (2). There was no significant difference in scriptfamiliarity between patients and controls. For each script, execution and verbal generationof actions were compared and the order of presentation was randomized.
Script Execution
The ‘shopping for groceries’ and ‘cooking’ scripts were performed on the same day.On a shelf, several items were displayed always in the same location: (1) salt, pepper andoil (usually found in a standard kitchen); (2) all the utensils necessary for the cookingactivity; and (3) some items unnecessary for this particular activity, but normally present ina kitchen, that were used as distracters. On the same shelf, there was a closed cookbook:the cake recipe was on page five. One of the examiners (MC) defined each activity with astatement describing its goal and the script’s starting point and ending point. The examinermade sure the subject had correctly understood the instructions and told him he couldwhenever necessary consult them on a cue card, which remained available throughout thetask. For ‘shopping for groceries’, the instructions were: “You must go shopping and buyeverything you need to cook scrambled eggs for two persons and bake a chocolate cake.The recipe for the cake is in this book. None of the ingredients are available here (exceptsalt, pepper and oil). The supermarket is not far from the hospital. We will take you there.You must do your shopping as if you were alone. Tell us when you have finished”. For the‘cooking’ activity, the instructions were: “You must bake a chocolate cake and cookscrambled eggs for two persons. The cake recipe is available in this book. All the utensilsyou need are available here (the examiner points to the shelf). You should use theingredients you have just bought. I cannot help you. You must act as if you were alone.Tell me when you have finished.”
The ‘answering a letter’ script was usually performed on another day. The activitystarted in the examiner’s office. The items displayed on the desk were always the same andin the same location. They comprised various types of paper, envelopes, stamps and a pen.The instructions were: “You must answer this letter fixing an appointment for a medicalexamination. You must then go and post it in the letterbox outside the rheumatology
Script execution 655
department. This place is unfamiliar to you. You must find your own way there. I cannothelp you. You must act as if you were alone. Tell me when you have finished.”
For each activity, two examiners were present. They followed the patient everywhereand both wrote down everything he did or said. They intervened only when the situationmight had become dangerous. The supermarket manager was aware of the study and gavehis consent.
Script Generation
As in script execution, the examiner first defined each activity with a statementdescribing the goal and the script’s starting point and ending point. Instructions were givenverbally and were displayed on a cue card, which remained available throughout the task.Before the subject started, the examiner made sure he had correctly understood theinstructions. For each script, the instructions stated that the subject had to write as manyactions as he could think of, and that the examiner could not help him at all.
Script Analysis
Script Execution
Once the two examiners had written down everything that happened during theexecution of each script, they were able to produce a comprehensive list of actions thatoccurred, regardless of the group. Error analysis was first tried using the framework of thecognitive model proposed by Lezak, Le Gall and Aubin (1994) according to which an errorof execution may reflect a dysfunction in ‘volition’, ‘planning’, ‘goal direction’ or ‘taskmonitoring’. Many errors could be interpreted, however, as a dysfunction in more than onelevel of the cognitive model. Consequently, five types of descriptive errors were firstdefined according to an inter-judge agreement: (1) omission: any action or sequence ofactions necessary for goal reaching which is omitted or incompletely performed, such asgoing to the supermarket without taking money; (2) addition: any action or sequence ofactions unnecessary for the completion of the task which is performed, such as buyingingredients not necessary for the cooking scripts; (3) inversion-substitution: any actionperformed out of the appropriate temporal sequence or any object that is misused orinappropriate to the sub-goal, such as putting the cake in the baker before lighting it orputting a salad bowl in the baker; (4) estimation error: poor estimation of the quantity ofingredients, of the size of an object, of space or time, such as putting too much sugar orchocolate in the cake; (5) commentary: any question, remark or joke addressed to theexaminers, although the patient had been instructed to act as if he were alone, such asasking how to do something. At this first step of analysis, each error was counted andincluded in only one category of error. Then, a second step analysis was made, taking intoaccount neuropsychological mechanisms and allowing to define a six-category classification:(1) context neglect: failure to respect instructions, poor evaluation of environment, such asnot taking the recipes into account or searching for spoons or tools in drawers instead ofusing those being on the working space; (2) control errors: inefficient monitoring of action,such as letting the cake to be burnt; (3) environmental adherence: inappropriate actioninduced by the presence of an object, such as washing plates being in the sink and notrequired by the scripts; (4) distractibility: behavioural sequence not contributing to goalachievement, such as exploring the kitchen or staying a long time without doing anything;(5) dependency: any question about the way to perform action, such as asking what therewas to do; and (6) behavioural disorder: any socially inappropriate or dangerous behaviour,such as making jokes about people in the shop or taking the hot scrambled eggs with thefingers. In this second step analysis, some errors could be also classified under two differentcategories of errors, or not classified, which accounts for the fact that the total number oferrors was not the same at the descriptive and the neuropsychological levels. A perfectinter-raters agreement was required to count or classify an error. These analyses were usedfor ‘shopping’, ‘cooking’ and ‘answering a letter’ scripts. As the way finding part of the
656 Mathilde Chevignard and Others
‘letter’ script is similar to the Executive Function Route-Finding Test of Boyd and Sautter(1993), it was analyzed according to both our and to their criteria, allowing the comparisonbetween the two methods.
Script Generation
In order to compare the performance in script execution and generation, we classifiedthe errors produced in script generation with the same framework as the execution errors.The existence of errors of ‘context neglect’, ‘estimation’ or ‘dependency’ may be surprisingin script generation. Some errors, however, could be observed. In generation, as inexecution, the recipes necessary to know which ingredient to buy could be neglected, thequantity of ingredients to use could be poorly estimated, and questions about the way toperform could be asked in spite of the consign to work alone. To allow comparison withprevious studies, the centrality of each evoked action and mean evocation time were alsoanalyzed. An action was considered as central when evoked by at least 70% of the controls.
Neuropsychological Evaluation
The cognitive assessment used the following laboratory tests: Modified Wisconsin CardSorting Test (Nelson, 1976), Trail Making Test (Reitan, 1958), category (animal names in60 sec.) and phonemic (words beginning with “P”, “F” and “L” in 60 sec.) verbal fluency(Benton, 1968), Grober and Buschke Verbal Learning Test (1987), planning tasks such asthe Tower of London Task (Shallice, 1982) and the Six Elements Task (Shallice andBurgess, 1991; Garnier, Enot-Joyeux, Jokic et al., 1998; Wilson et al., 1998).
The behavioral assessment included two questionnaires constructed to sample the rangeof dysexecutive problems commonly encountered in daily life: the Behavioral Scale(Lhermitte et al., 1986; Sarazin et al., 1998) and the Dysexecutive Questionnaire (Wilson,Alderman, Burgess et al., 1996; Wilson et al.,1998). The Behavioral Scale was designed toevaluate, by comparison with the premorbid state of the patient, the severity of frontal lobe-related behavioral abnormalities such as apathy, restlessness, stereotypy, impulsiveness,indifference, euphoria, disinterestedness, cheerfulness, dependence on social environment,indifference to rules, decrease in attention, dependence on stimuli from the physicalenvironment, programming disorders, personality changes, and impairment of intellectualand emotional control. The number of true/false answers to five items (giving a score from0, absence of impairment, to 5, severe impairment) assessed the importance of each of thesesixteen features (eighty items in all, presented in random order). The Behavioral Scale hasbeen shown to be sensitive to frontal lobe lesions (Lhermitte et al., 1986) and scoresobtained by patients with such lesions were significantly correlated with regional glucoseconsumption in orbitoventral areas, as determined using PET (Sarazin et al., 1998). The 20-item Dysexecutive Questionnaire samples four broad areas of dysexecutive changes:emotional or personality, motivational, behavioral and cognitive changes. Each item isscored on a five-point (0-4) Likert scale, ranging from never to very often. Bothquestionnaires have two versions: one to be administered to the patient and the other to thecaregiver or relative who is in close contact with the patient.
Data Analysis
Statistical analyses were performed with ANOVAs using group as between factor andexperimental condition (script execution and script generation) as within factor. Givenvariance heterogeneity, the group and condition effects were controlled with non-parametricanalyses, which gave similar results. We looked for a correlation between scores in theexperimental tasks and the performance in the laboratory evaluation of executive functionson one hand, the scores on the behavioural questionnaires on the other hand, using theSpearman rank correlation test.
Script execution 657
RESULTS
Script Execution
Analysis of Errors
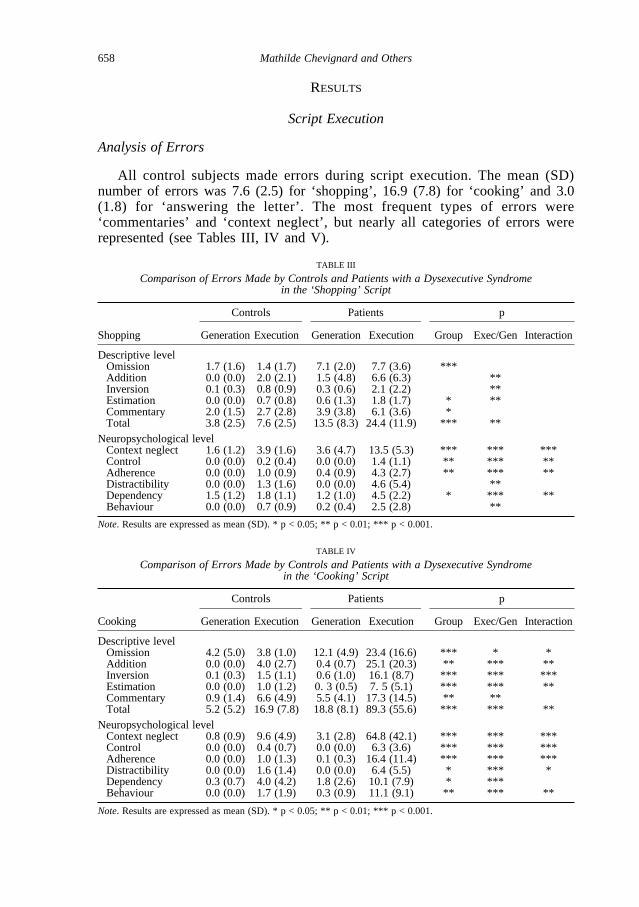
All control subjects made errors during script execution. The mean (SD)number of errors was 7.6 (2.5) for ‘shopping’, 16.9 (7.8) for ‘cooking’ and 3.0(1.8) for ‘answering the letter’. The most frequent types of errors were‘commentaries’ and ‘context neglect’, but nearly all categories of errors wererepresented (see Tables III, IV and V).
658 Mathilde Chevignard and Others
TABLE III
Comparison of Errors Made by Controls and Patients with a Dysexecutive Syndrome in the ‘Shopping’ Script
Controls Patients p
Shopping GenerationExecution Generation Execution Group Exec/Gen Interaction
Descriptive levelOmission 1.7 (1.6) 1.4 (1.7) 7.1 (2.0) 7.7 (3.6) ***Addition 0.0 (0.0) 2.0 (2.1) 1.5 (4.8) 6.6 (6.3) **Inversion 0.1 (0.3) 0.8 (0.9) 0.3 (0.6) 2.1 (2.2) **Estimation 0.0 (0.0) 0.7 (0.8) 0.6 (1.3) 1.8 (1.7) * **Commentary 2.0 (1.5) 2.7 (2.8) 3.9 (3.8) 6.1 (3.6) *Total 3.8 (2.5) 7.6 (2.5) 13.5 (8.3) 24.4 (11.9) *** **
Neuropsychological levelContext neglect 1.6 (1.2) 3.9 (1.6) 3.6 (4.7) 13.5 (5.3) *** *** ***Control 0.0 (0.0) 0.2 (0.4) 0.0 (0.0) 1.4 (1.1) ** *** **Adherence 0.0 (0.0) 1.0 (0.9) 0.4 (0.9) 4.3 (2.7) ** *** **Distractibility 0.0 (0.0) 1.3 (1.6) 0.0 (0.0) 4.6 (5.4) **Dependency 1.5 (1.2) 1.8 (1.1) 1.2 (1.0) 4.5 (2.2) * *** **Behaviour 0.0 (0.0) 0.7 (0.9) 0.2 (0.4) 2.5 (2.8) **
Note. Results are expressed as mean (SD). * p < 0.05; ** p < 0.01; *** p < 0.001.
TABLE IV
Comparison of Errors Made by Controls and Patients with a Dysexecutive Syndrome in the ‘Cooking’ Script
Controls Patients p
Cooking GenerationExecution Generation Execution Group Exec/Gen Interaction
Descriptive levelOmission 4.2 (5.0) 3.8 (1.0) 12.1 (4.9) 23.4 (16.6) *** * *Addition 0.0 (0.0) 4.0 (2.7) 0.4 (0.7) 25.1 (20.3) ** *** **Inversion 0.1 (0.3) 1.5 (1.1) 0.6 (1.0) 16.1 (8.7) *** *** ***Estimation 0.0 (0.0) 1.0 (1.2) 0. 3 (0.5) 7. 5 (5.1) *** *** **Commentary 0.9 (1.4) 6.6 (4.9) 5.5 (4.1) 17.3 (14.5) ** **Total 5.2 (5.2) 16.9 (7.8) 18.8 (8.1) 89.3 (55.6) *** *** **
Neuropsychological levelContext neglect 0.8 (0.9) 9.6 (4.9) 3.1 (2.8) 64.8 (42.1) *** *** ***Control 0.0 (0.0) 0.4 (0.7) 0.0 (0.0) 6.3 (3.6) *** *** ***Adherence 0.0 (0.0) 1.0 (1.3) 0.1 (0.3) 16.4 (11.4) *** *** ***Distractibility 0.0 (0.0) 1.6 (1.4) 0.0 (0.0) 6.4 (5.5) * *** *Dependency 0.3 (0.7) 4.0 (4.2) 1.8 (2.6) 10.1 (7.9) * ***Behaviour 0.0 (0.0) 1.7 (1.9) 0.3 (0.9) 11.1 (9.1) ** *** **
Note. Results are expressed as mean (SD). * p < 0.05; ** p < 0.01; *** p < 0.001.
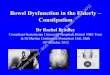
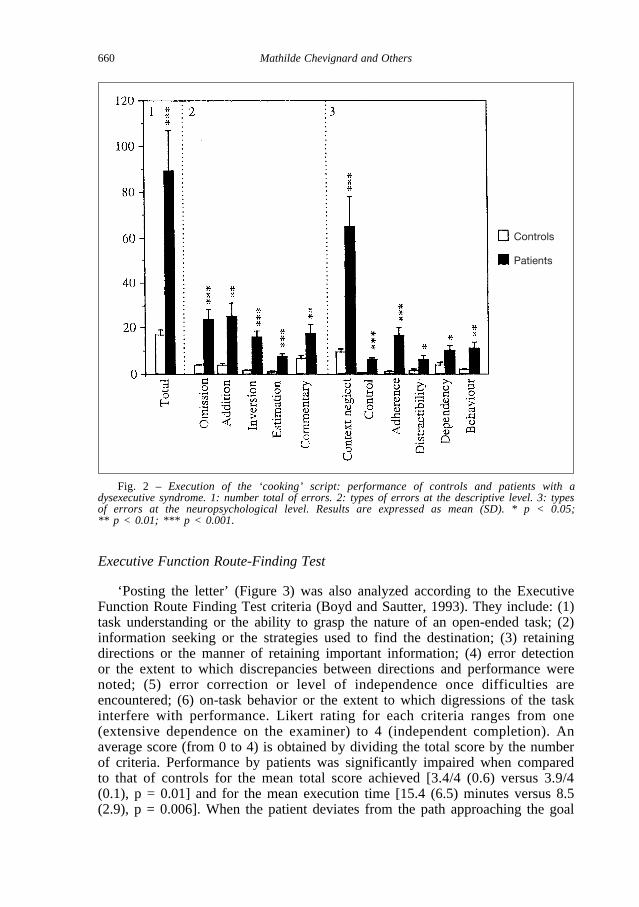
Patients made a significantly (p < 0.01) higher number of errors for the threescripts: 24.4 (11.9) for ‘shopping’, 89.3 (55.6) for ‘cooking’, and 14.1 (9.7) for‘answering the letter’. The difference between patients and controls wassignificant for nearly all categories of errors, particularly for ‘cooking’ (Figure2). However, ‘omissions’, ‘context neglect’ and ‘environmental adherence’ bestdifferentiated patients from controls for each of the three scripts.
The total number of errors in the execution of each of the three scripts wassignificantly correlated with that of the two others: rho = 0.7 (p < 0.03) for‘shopping’ and ‘cooking’; rho = 0.7 (p < 0.03) for ‘shopping’ and ‘answeringthe letter’; rho = 0.65 (p = 0.04) for ‘cooking’ and ‘answering the letter’.
Mean Script Execution Time
Script execution time, from the beginning to the end of the script, wassignificantly longer for the patient group than for controls: 20.5 (8.5) versus 10.5(2.3) minutes for ‘shopping’ (p = 0.0019); 81.2 (33.5) versus 51 (9.9) minutesfor ‘cooking’ (p = 0.013); and 17.9 (11.0) versus 10.2 (3.9) minutes for‘answering the letter’ (p = 0.05).
Money Spent in the Supermarket
There was no significant difference between the amount of money spent by the patients and the controls [54.9 (13.6) versus 55.2 (10.1) French francs] during shopping. Omissions were, however, more frequent in patientsthan in controls, suggesting that controls devoted more attention to prices thanpatients.
Script execution 659
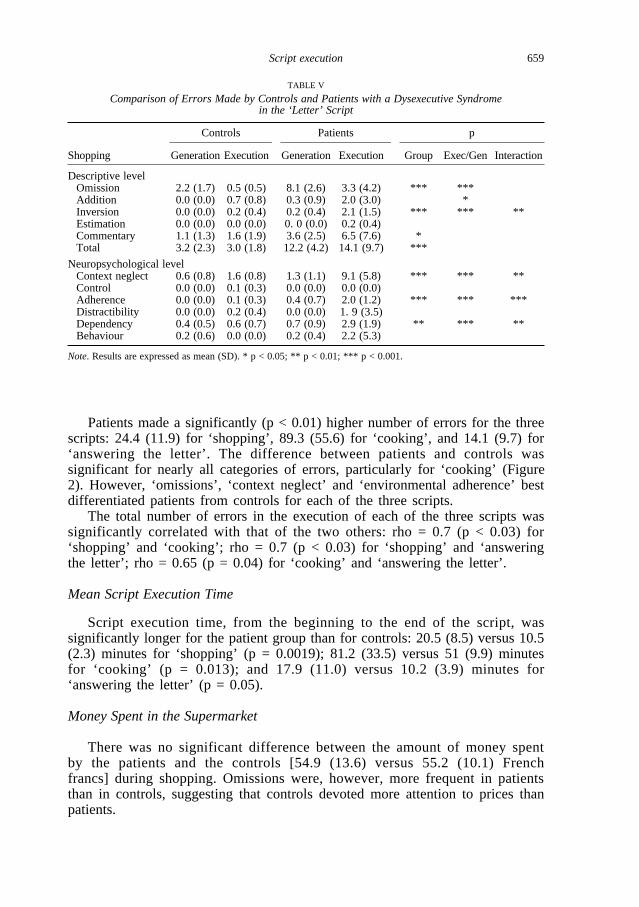
TABLE V
Comparison of Errors Made by Controls and Patients with a Dysexecutive Syndrome in the ‘Letter’ Script
Controls Patients p
Shopping GenerationExecution Generation Execution Group Exec/Gen Interaction
Descriptive levelOmission 2.2 (1.7) 0.5 (0.5) 8.1 (2.6) 3.3 (4.2) *** ***Addition 0.0 (0.0) 0.7 (0.8) 0.3 (0.9) 2.0 (3.0) *Inversion 0.0 (0.0) 0.2 (0.4) 0.2 (0.4) 2.1 (1.5) *** *** **Estimation 0.0 (0.0) 0.0 (0.0) 0. 0 (0.0) 0.2 (0.4)Commentary 1.1 (1.3) 1.6 (1.9) 3.6 (2.5) 6.5 (7.6) *Total 3.2 (2.3) 3.0 (1.8) 12.2 (4.2) 14.1 (9.7) ***
Neuropsychological levelContext neglect 0.6 (0.8) 1.6 (0.8) 1.3 (1.1) 9.1 (5.8) *** *** **Control 0.0 (0.0) 0.1 (0.3) 0.0 (0.0) 0.0 (0.0)Adherence 0.0 (0.0) 0.1 (0.3) 0.4 (0.7) 2.0 (1.2) *** *** ***Distractibility 0.0 (0.0) 0.2 (0.4) 0.0 (0.0) 1. 9 (3.5)Dependency 0.4 (0.5) 0.6 (0.7) 0.7 (0.9) 2.9 (1.9) ** *** **Behaviour 0.2 (0.6) 0.0 (0.0) 0.2 (0.4) 2.2 (5.3)
Note. Results are expressed as mean (SD). * p < 0.05; ** p < 0.01; *** p < 0.001.
Executive Function Route-Finding Test
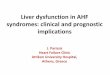
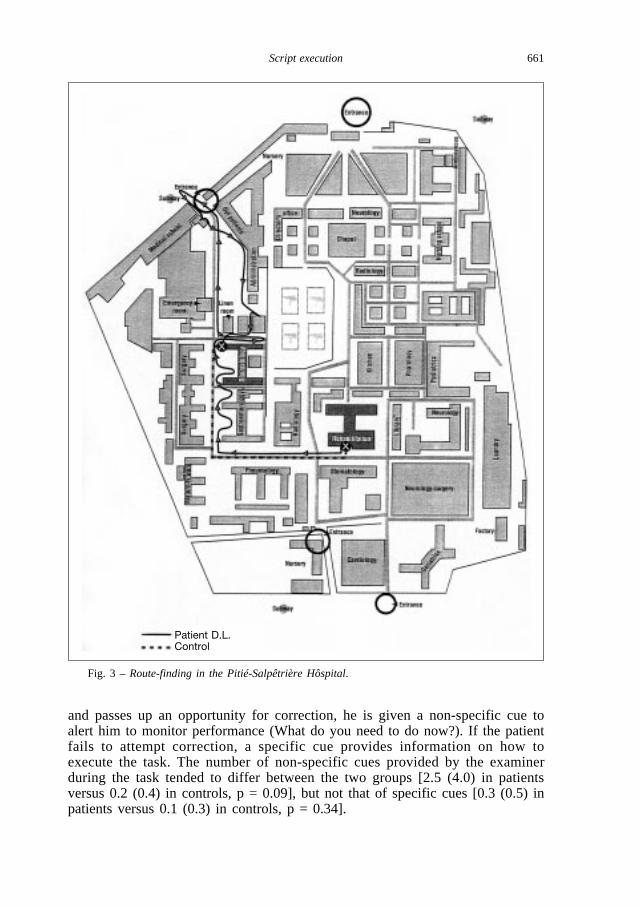
‘Posting the letter’ (Figure 3) was also analyzed according to the ExecutiveFunction Route Finding Test criteria (Boyd and Sautter, 1993). They include: (1)task understanding or the ability to grasp the nature of an open-ended task; (2)information seeking or the strategies used to find the destination; (3) retainingdirections or the manner of retaining important information; (4) error detectionor the extent to which discrepancies between directions and performance werenoted; (5) error correction or level of independence once difficulties areencountered; (6) on-task behavior or the extent to which digressions of the taskinterfere with performance. Likert rating for each criteria ranges from one(extensive dependence on the examiner) to 4 (independent completion). Anaverage score (from 0 to 4) is obtained by dividing the total score by the numberof criteria. Performance by patients was significantly impaired when comparedto that of controls for the mean total score achieved [3.4/4 (0.6) versus 3.9/4(0.1), p = 0.01] and for the mean execution time [15.4 (6.5) minutes versus 8.5(2.9), p = 0.006]. When the patient deviates from the path approaching the goal
660 Mathilde Chevignard and Others
Fig. 2 – Execution of the ‘cooking’ script: performance of controls and patients with adysexecutive syndrome. 1: number total of errors. 2: types of errors at the descriptive level. 3: typesof errors at the neuropsychological level. Results are expressed as mean (SD). * p < 0.05; ** p < 0.01; *** p < 0.001.
Controls
Patients
and passes up an opportunity for correction, he is given a non-specific cue toalert him to monitor performance (What do you need to do now?). If the patientfails to attempt correction, a specific cue provides information on how toexecute the task. The number of non-specific cues provided by the examinerduring the task tended to differ between the two groups [2.5 (4.0) in patientsversus 0.2 (0.4) in controls, p = 0.09], but not that of specific cues [0.3 (0.5) inpatients versus 0.1 (0.3) in controls, p = 0.34].
Script execution 661
Fig. 3 – Route-finding in the Pitié-Salpêtrière Hôspital.
Patient D.L.Control
The results of this analysis and of the ‘posting a letter’ error analysis werestrongly correlated: rho = – 0.79 (p = 0.0127) for the mean total score, and rho = 0.79 (p = 0.0127) for the mean execution time; correlation approachedsignificance for the number of non-specific cues: rho = 0.58 (p = 0.068).
Script Generation
Analysis of Errors
For controls, the mean (SD) number of errors was 4.5 (2.5) for ‘shopping’,7.3 (5.2) for ‘cooking’ and 3.4 (2.3) for ‘answering the letter’. The mostfrequent types of errors were ‘omissions’, ‘commentaries’, ‘context neglect’ and‘environmental adherence’ (see Tables III, IV and V).
Patients made a significantly (p < 0.01) higher number of errors for the threescripts: 14.5 (8.3) for ‘shopping’, 22.2 (8.1) for ‘cooking’, and 13.1 (4.2) for‘answering the letter’. The types of errors that best differentiated patients fromcontrols were ‘omissions’ and ‘commentaries’.
Centrality of Evoked Actions
The patients evoked significantly (p < 0.01) fewer central actions thancontrols in each script. However, the percentage of total evoked actions thatwere central did not differ between patients and controls.
Mean Evocation Time
The mean evocation time by action, time to generate a script from thebeginning to the end of the script divided by the number of actions generated,was significantly (p < 0.01) increased in patients for the ‘shopping’ and‘cooking’ scripts, but not for the ‘letter’ script.
Script Execution versus Script Generation
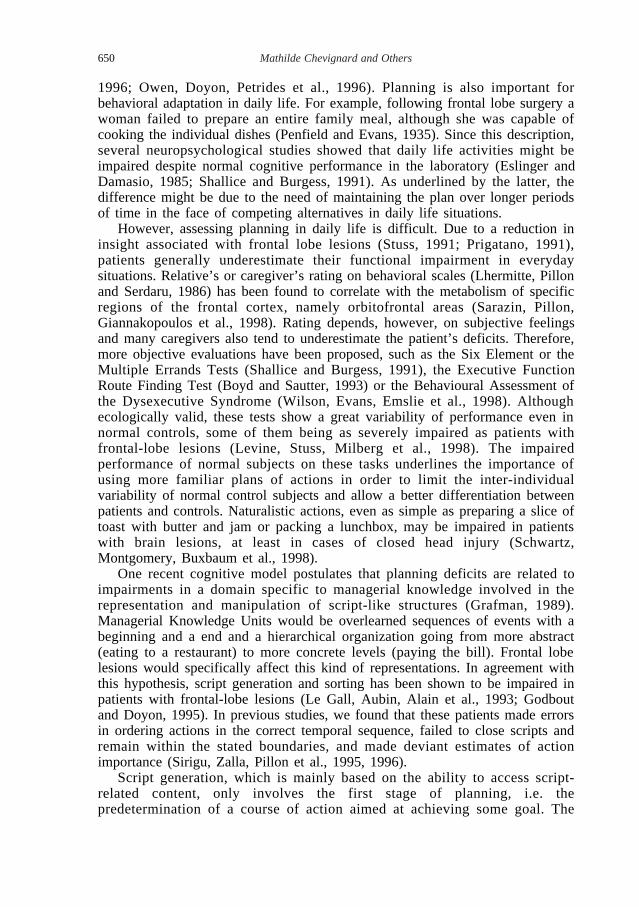
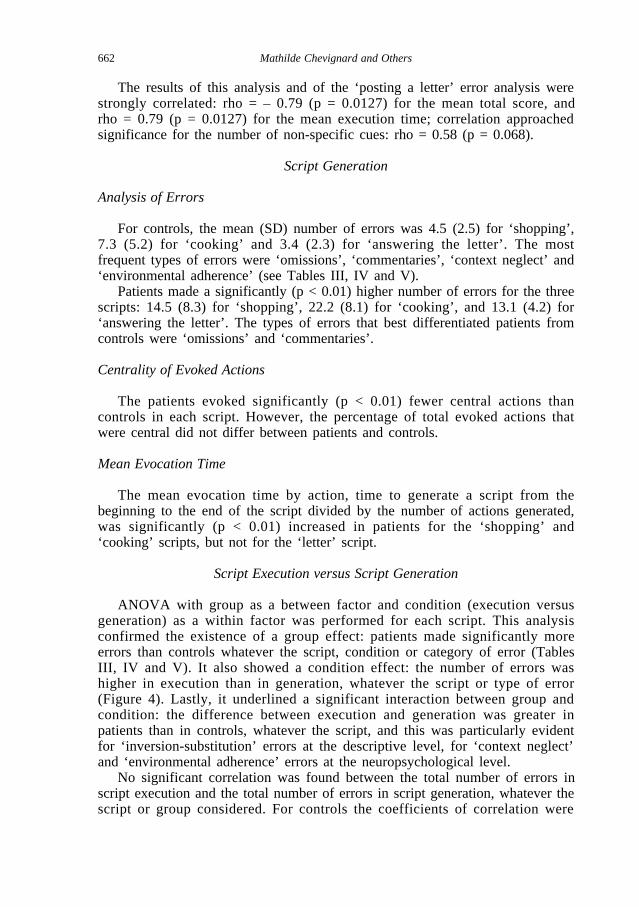
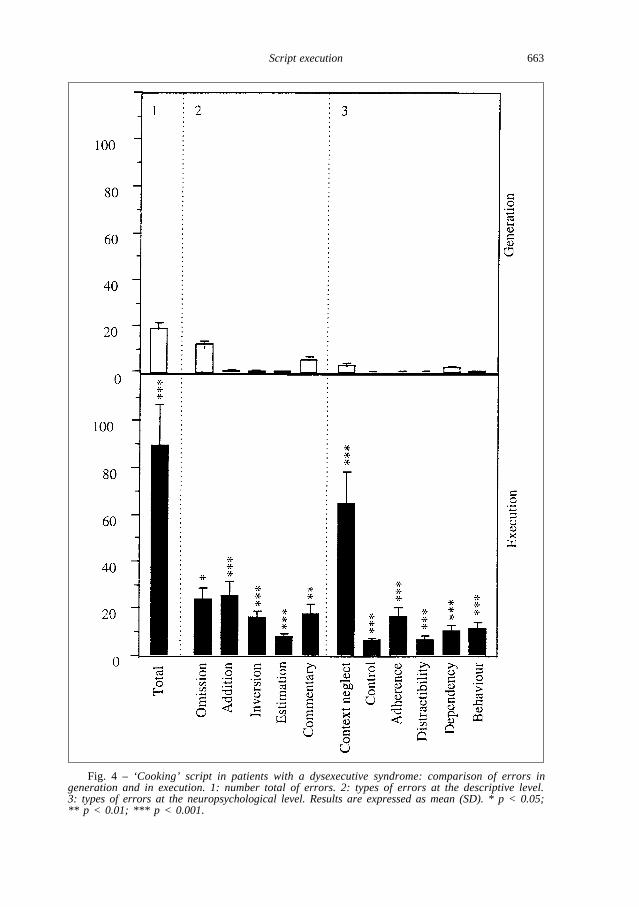
ANOVA with group as a between factor and condition (execution versusgeneration) as a within factor was performed for each script. This analysisconfirmed the existence of a group effect: patients made significantly moreerrors than controls whatever the script, condition or category of error (TablesIII, IV and V). It also showed a condition effect: the number of errors washigher in execution than in generation, whatever the script or type of error(Figure 4). Lastly, it underlined a significant interaction between group andcondition: the difference between execution and generation was greater inpatients than in controls, whatever the script, and this was particularly evidentfor ‘inversion-substitution’ errors at the descriptive level, for ‘context neglect’and ‘environmental adherence’ errors at the neuropsychological level.
No significant correlation was found between the total number of errors inscript execution and the total number of errors in script generation, whatever thescript or group considered. For controls the coefficients of correlation were
662 Mathilde Chevignard and Others
Script execution 663
Fig. 4 – ‘Cooking’ script in patients with a dysexecutive syndrome: comparison of errors ingeneration and in execution. 1: number total of errors. 2: types of errors at the descriptive level. 3: types of errors at the neuropsychological level. Results are expressed as mean (SD). * p < 0.05;** p < 0.01; *** p < 0.001.

rho = – 0.05 (p = 0.88) for ‘shopping’, rho = 0.30 (p = 0.37) for ‘cooking’, andrho = 0.50 (p = 0.13) for ‘answering the letter’. For patients the coefficients ofcorrelation were rho = 0.51 (p = 0.10) for ‘shopping’, rho = 0.20 (p = 0.53) for‘cooking’, and rho = 0.12 (p = 0.67) for ‘answering the letter’.
Correlation between Script Execution and Performance of Tests of ExecutiveFunctions
For patients, there was no significant correlation between the total number oferrors in the different scripts executed on one hand and the performance on testsof executive functions on the other hand.
Correlation between Script Execution and Scores on the Behavioral Scales
For patients, there was no significant correlation between the variousnumbers of errors in script execution and the global score on the BehavioralScale or the Dysexecutive Questionnaire answered either by the patient or by thecaregiver. For instance, for the total number of errors in execution of the‘cooking’ script, the coefficient of correlation with the Behavioural Scale wasrho = 0.17 (p = 0.59) when answered by the patient and rho = 0.42 (p = 0.18)when answered by the caregiver; the coefficient of correlation with theDysexecutive Questionnaire was rho = 0.05 (p = 0.88) when answered by thepatient, and rho = 0.29 (p = 0.36) when answered by the caregiver. By contrast,the same coefficients of correlation became significant if the questionnaires wereanswered by occupational therapists well acquainted with the patients. For theBehavioral Scale, the coefficient of correlation was rho = 0.77 (p = 0.02) withthe total number of errors in script execution, rho = 0.77 (p = 0.02) with thetotal number of errors in ‘cooking’, rho = 0.55 (p < 0.10) with the total numberof errors in ‘shopping’, and rho = 0.78 (p < 0.02) with the total number of errorsin ‘answering the letter’. For the Dysexecutive Questionnaire, the coefficient ofcorrelation was rho = 0.76 (p = 0.02) with the total number of errors in scriptexecution, rho = 0.74 (p < 0.03) with the total number of errors in ‘cooking’,rho = 0.57 (p < 0.10) with the total number of errors in ‘shopping’, and rho =0.82 (p = 0.01) with the total number of errors in ‘answering the letter’.
DISCUSSION
The first aim of the study was to compare execution and generation ofrelatively familiar scripts. Script execution, which includes monitoring of action,may be a better indicator of a planning dysfunction than script generation, whichinvestigates a specific category of knowledge and measures goal-related actionfluency. Script generation was, however, significantly impaired in patientscompared to controls, confirming previous studies implicating the frontal lobesin managerial knowledge (Le Gall et al., 1993; Godbout and Doyon, 1995). Asin our previous study (Sirigu et al., 1995), two different cognitive modes ofrepresenting actions could be hypothesised from an analysis of patients’
664 Mathilde Chevignard and Others
performance: (1) an associative level related to semantic knowledge andcentrality of actions, which was preserved in patients and could be under thecontrol of the temporal lobes; (2) a pragmatic level, using the goal of the planas a binding element between the actions, which was impaired in patients andcould require the involvement of the prefrontal cortex. The nature of pragmaticerrors, however, differed between the two studies: temporal ordering, included in‘inversion-substitution’ errors, was not significantly impaired in the presentstudy. By contrast, evocation of actions was slowed and patients made more‘omissions’ and ‘commentaries’. Differences in aetiology and location of lesionsmay influence the nature of errors. In the previous study, the lesions weremainly focal vascular and surgical lesions of the dorsolateral areas of theprefrontal cortex. In the present study, the lesions were mainly traumatic. Beingmore diffuse, the latter lesions could be responsible for cognitive slowing and‘omission’ errors, because activation deficits and limitation of attentionalresources are reported to be more severe in diffuse than in focal lesions(Schwartz et al., 1998). Involving orbital areas, the latter lesions could induce ahigher occurrence of ‘commentaries’, a sign of disinhibition associated withorbital dysfunction (Luria, 1966; Eslinger and Damasio, 1985). Despite thesediscrepancies, this study confirms the sensitivity of script generation to frontallobe damage, which disrupts the ability to mentally activate the correct sequenceof actions needed to achieve a goal, even for relatively familiar actions.
As planning impairment might result not only from a deficit of internalrepresentation, but also from a binding deficit between the plan and contextualinformation, we wanted to study the same patients in the real execution of thesame scripts. It might be postulated that the performance would improve in acontextual situation that could drive the patient and facilitate the bindingbetween actions. Conversely, our hypothesis was that this condition wouldincrease the deficit, since monitoring processes would be more highly solicitedby multiple sub-goal plans in open-ended situations, which would require theperformance of actions in parallel and suppression of distracters. Indeed, scriptexecution was more sensitive than script generation, both for controls and forpatients with dysexecutive deficits. This underlines the fact that planning shouldnot be restricted to managerial knowledge, but also includes the monitoring ofaction (Hayes-Roth and Hayes-Roth, 1979). It might also suggest that planningis not just a top-down predetermined sequential process (Grafman, 1989),including cognitive (Shallice and Burgess, 1991) and affective (Damasio et al.,1991) markers and able to reactivate after a delay previously generatedintentions; it would also be a bottom-up opportunistic process interacting withthe contextual environment to suggest decisions whenever promisingopportunities arise (Hayes-Roth and Hayes-Roth, 1979). This capacity for on-line adjustment is critical for behavioral adaptation.
The difference in number of errors between execution and generation washigher in patients than in controls, in agreement with our hypothesis that thefrontal lobes intervene not only in script representation, but also in the bindingbetween the plan of action and contextual environment. The fact that ‘contextneglect’ and ‘environmental adherence’ were errors that best differentiatedpatients from controls at the neuropsychological level further supports this
Script execution 665
interpretation. ‘Context neglect’ is commonly observed in laboratory testing ofpatients with frontal lobe lesions. It accounts for disturbances in the ability toanalyze data, the first stage of problem resolution, that may be compensated forby cues that direct attention to the pertinent information (Luria, 1966; Fasotti,1992; Aubin, Le Gall and Etcharry-Bouyx, 1997). This is consistent with thefrontal lobes being an area of sensorial integration (Fuster, 1989; Pandya andYeterian, 1996) and of control of attention (Mesulam, 1990; Godefroy, Lhuillierand Rousseaux, 1996). ‘Environmental adherence’ has also been described inpatients with frontal lobe lesions. It is responsible for pathological behaviors ofimitation, prehension and utilization commonly found in these patients(Lhermitte et al., 1986). It expresses the release of parietal lobe activities fromfrontal lobe inhibition, given that the dorsolateral prefrontal cortex and theparietal cortex are involved in the same lateral system responsive to externalinformation (Barbas and Pandya, 1989). The weakening control of theSupervisory Attentional System would predispose to environmental capture(Shallice, Burgess, Schon et al., 1989; Miotto and Morris, 1998).
The ‘cooking’ script was the most sensitive to executive dysfunction (seeTables III, IV and V). The total number of errors in execution of this scriptincreased from 16.9 in controls to 89.3 in patients and all types of errors weresignificantly increased in patients compared to controls. In this script, in contrastwith the other two, some actions had to be performed in parallel: for example,the scrambled eggs had to be prepared while the cake was being baked.Therefore, the planning deficit might be increased by competing actions at adecision node, i.e. when the subject has to set priorities in the face of two ormore competing tasks (Shallice and Burgess, 1991; Della Malva, Stuss, D’Altonet al., 1993). As the increase in number of errors was particularly dramatic for‘context neglect’, it may be suggested that contextual information may beespecially at risk when attentional resources are already required for theselection of the appropriate action.
The deficit in binding plan and contextual information explains why theexecution of familiar multiple-action scripts in an opened and interactiveenvironment was more sensitive to a dysexecutive syndrome than laboratorytests or script generation. The impaired performance in neuropsychological testswas particularly mild in this study, even for planning tests such as the Tower ofLondon or the Six Element Tasks (see Table II). The reliability of the scriptexecution procedure is underlined by the strong correlation observed between theperformance on the three scripts on one hand, and between ‘posting the letter’and the Executive Function Route-Finding Test on the other hand. Despite theecological value of script execution, the performance of patients was notcorrelated with the answers of patients or caregivers on the behavioral scales.Loss of insight is well known for patients with a dysexecutive syndrome whocommonly underestimate their deficits (Stuss, 1991; Prigatano, 1991). It is likelythe consequence of impaired autonoetic consciousness – the capacity to mentallyrepresent and become aware of subjective experiences in the past, present andfuture (Wheeler, Stuss and Tulving, 1997) – and related reality distortion(Johnson, 1997). Answers given by caregivers are usually more reliable (Sarazinet al., 1998; Wilson et al., 1998), although an underestimation was also observed
666 Mathilde Chevignard and Others
in our study. The long duration of the disease may explain this underestimation:(1) the caregiver implicitly adapts his behaviour to that of the patient andprogressively monitors the patient behavior, acting more or less as his ownfrontal lobe; (2) the patient recovers a sufficient degree of autonomy to stayalone at home with less control from the caregiver; (3) the patient’s errorsprogressively become more similar to those produced by normal subjects and thecaregivers consider more the final result than the way of organizing the differentsteps. Such an underestimation was not detected with more objective observers,since significant coefficients of correlation were found with the scores answeredby the occupational therapist on the two behavioral scales which were aimed atassessing the severity of frontal lobe-related behavioral abnormalities (Lhermitteet al., 1986) and broad areas of dysexecutive changes (Wilson et al., 1998).
In conclusion, a continuous interaction with the environment may help toshape an action plan, but also provoke action slips due to competing alternativesfor control and selection of action (Reason, 1979; Shallice, 1988). Action slips areobserved even in normal subjects. However, the impaired monitoring of actionassociated with frontal lobe lesion or dysfunction results in both ‘context neglect’,inducing a poorer action plan, and ‘environmental adherence’, which increases thenumber of action slips, explaining why script execution is more sensitive thanscript generation or laboratory tests. Therefore, script execution seems to be thebest predictor of the behavioral adaptation of patients with dysexecutive deficitsto daily life activities, which require a plan with multiple sub-goals to be executedin open situations and its execution to be adapted to contextual information.Although the method may appear time-consuming, it has the advantage of givinga more exact appreciation of the patient’s deficits outside the laboratory and oforienting rehabilitation in relation to the actual deficits of each patient.
Acknowledgements. This work was supported by a grant from the “Assistance Publique– Hôpitaux de Paris” and a grant from the “Programme de Recherche Incitatif de l’IFR deNeurosciences du CHU Pitié-Salpêtrière (Paris, France)”.
REFERENCES
AUBIN, G., LE GALL , D., and ETCHARRY-BOUYX, F. Niveaux cognitifs de la résolution de problèmesnumériques: À propos d’une observation de syndrome frontal. Revue Neuropsychologique, 7:411-433, 1997.
BAKER, S.C., ROGERS, R.D., OWEN, A.M., FRITH, C.D., DOLAN, R.J., FRACKOWIAK, R.S., and ROBBINS,T.W. Neural systems engaged by planning: A PET study of the Tower of London task.Neuropsychologia, 34:515-526, 1996.
BARBAS, H., and PANDYA , D.N. Architecture and intrinsic connections of the prefrontal cortex in therhesus monkey. Journal of Comparative Neurology, 286:353-375, 1989.
BENTON, A.L. Differential behavioural effects in frontal lobe disease. Neuropsychologia, 6:53-60, 1968.BOYD, T.M., and SAUTTER, S.W. Route-finding: A measure of everyday executive functioning in the
head-injured adult. Applications of Cognitive Psychology, 7:171-181, 1993.DAMASIO, A.R., TRANEL, D., and DAMASIO, H. Somatic markers and the guidance of behavior: Theory
and preliminary testing. In H.S. Levin, H.M. Eisenberg and A.L. Benton (Eds.), Frontal LobeFunction and Dysfunction. Oxford: Oxford University Press, 1991, pp. 217-229.
DELLA MALVA , C.L., STUSS, D.T., D’A LTON, J., and WILLMER, J. Capture errors and sequencing afterfrontal brain lesions. Neuropsychologia, 31:363-372, 1993.
DUBOIS, B., LEVY, R., VÉRIN, M., TEIXEIRA-FERREIRA, C., and PILLON, B. Experimental approach toprefrontal functions in Humans. In J. Grafman, F. Boller and K.J. Holyoak (Eds.), Structure andFunctions of the Human Prefrontal Cortex. Annals of the New York Academy of Sciences 1995;179, pp. 41-60.
Script execution 667
ESLINGER, P.J., and DAMASIO, A.R. Severe disturbance of higher cognition after bilateral frontal lobeablation: Patient EVR. Neurology, 35:1731-1741, 1985.
FASSOTI, L. Arithmetical Word Problem Solving after Frontal Lobe Damage. A CognitiveNeuropsychological Approach. Amsterdam: Swets & Zeitlinger, 1992.
FUSTER, J.M. The Prefrontal Cortex. 2nd ed. New York: Raven Press, 1989.GARNIER, C., ENOT-JOYEUX, F., JOKIC, C., LE THIEC, F., DESGRANGES, B., and EUSTACHE, F. Une
évaluation des fonctions exécutives chez les traumatisés crâniens: L’adaptation du test des sixéléments. Revue de Neuropsychologie, 8:385-414, 1998.
GODBOUT, L., and DOYON, J. Mental representation of knowledge following frontal-lobe or postrolandiclesions. Neuropsychologia, 33:1671-1696, 1995.
GODEFROY, O., LHUILLIER, C., and ROUSSEAUX, M. Non-spatial attention disorders in patients withprefrontal or posterior brain damage. Brain, 119:191-202, 1996.
GRAFMAN, J. Plans, actions and mental sets: Managerial knowledge units in the frontal lobes. In E.Perecman (Ed.), Integrating Theory and Practice in Clinical Neuropsychology. Hillsdale, NJ:Erlbaum, 1989, pp. 93-138.
GROBER, E., and BUSCHKE, H. Genuine memory deficits in dementia. Developmental Neuropsychology,3: 13-36, 1987.
JOHNSON, M.K. Source monitoring and memory distortion. Philosophical Transactions of the RoyalSociety of London, B 352:1733-1745, 1997.
HAYES-ROTH, B., and HAYES-ROTH, F. A cognitive model of planning. Cognitive Science, 3:245-262,1979.
KARNATH, H.O., WALLESCH, C.W., and ZIMMERMAN , P. Mental planning and anticipatory processes withacute and chronic frontal lobe lesions: A comparison of maze performance in routine and nonroutine situations. Neuropsychologia, 29:271-290, 1991.
KLOSOWSKA, D. Relation between ability to program actions and location of brain damage. PolishPsychology Bulletin, 7:245-255, 1976.
LE GALL , D., AUBIN, G., ALAIN , P.H., and EMILE, J. Script et syndrome frontal: À propos de deuxobservations. Revue Neuropsychologique, 3:87-110, 1993.
LEZAC, M.D., LE GALL , D., and AUBIN, G. Evaluation des fonctions exécutives lors des atteintes deslobes frontaux. Revue Neuropsychologique, 4:327-343, 1994.
LEVINE, B., STUSS, D.T., MILBERG, W.P., ALEXANDER, M.P., SCHWARTZ, M., and MACDONALD, R. Theeffects of focal and diffuse brain damage on strategy application: Evidence from focal lesions,traumatic brain injury and normal aging. JINS, 4:247-264, 1998.
LHERMITTE, F., DÉROUESNÉ, J, and SIGNORET, J.L. Analyse neuropsychologique du syndrome frontal.Revue Neurologique, 127:415-440, 1972.
LHERMITTE, F., PILLON, B., and SERDARU, M. Human autonomy and the frontal lobes. Part I: Imitationand utilization behaviours: A neuropsychological study of 75 patients. Annnals of Neurology, 19:326-34, 1986.
LURIA, A.R. Higher Cortical Functions in Man. New York, NY: Basic Books Inc., 1966.MESULAM, M.M. Large-scale neurocognitive networks and distributed processing for attention, language
and memory. Annals of Neurology, 28:597-613, 1990.MIOTTO, E.C., and MORRIS, R.G. Virtual planning in patients with frontal lobe lesions. Cortex, 34:639-
657, 1998.MORRIS, R.G., MIOTTO, E.C., FEIGENBAUM, J.D., BULLOCK, P., and POLKEY, C.E. The effect of goal-
subgoal conflict on planning ability after frontal and temporal lobe lesions in humans.Neuropsychologia, 35:1147-1157, 1997.
NELSON, H.E. A modified Card Sorting Test sensitive to frontal lobe defect. Cortex, 12:313-324, 1976.OWEN, A., DOWNES, J.D., SAHAKIAN , B.J., POLKEY, C.E., ROBBINS, T.W. Planning and spatial working
memory following frontal lobe lesions in man. Neuropsychologia, 28:1021-1034, 1990.OWEN, A.M., DOYON, J., PETRIDES, M., and EVANS, A.C. Planning and spatial working memory: A
positron emission tomography study in humans. European Journal of Neuroscience, 8:353-364,1996.
OWEN, A. Cognitive planning in humans: Neuropsychological, neuroanatomical andneuropharmacological perspectives. Progress in Neurobiology, 53:431-450, 1997.
PANDYA , D.N., and YETERIAN, E.H. Morphological correlations of human and monkey frontal lobe. InA.R. Damasio, H. Damasio and Y. Christen (Eds.), Neurobiology of Decision-Making. Berlin:Springer-Verlag, 1996, pp. 13-46.
PENFIELD, W., and EVANS, J. The frontal lobe in man: A clinical study of maximum removals. Brain, 58:115-133, 1935.
PORTEUS, S.D. The Maze Test and Clinical Psychology. Palo Alto, CA: Pacific Books, 1959.PRIGATANO, G.P. Disturbances of self-awareness of deficit after traumatic brain injury. In G.P. Prigatano
and D.L. Schacter (Eds.), Awareness of Deficit after Brain Injury. Clinical and Theoretical Issues.Oxford: Oxford University Press, 1991, pp. 111-126.
REASON, J.T. Actions not as planned: The price of automatisation. In G. Underwood and R. Stevens
668 Mathilde Chevignard and Others
(Eds.) Aspects of Consciousness, vol 1. London: Academic Press, 1979, pp. 67-89.REITAN, R.M. Validity of the trail making test as an indication of organic brain damage. Perceptual
Motor Skills, 8:271-276, 1958.SARAZIN, M., PILLON, B., GIANNAKOPOULOS, P., RANCUREL, G., SAMSON, Y., and DUBOIS, B. Clinico-
metabolic dissociation of cognitive functions and social behaviours in frontal-lobe lesions.Neurology, 51:142-148, 1998.
SCHWARTZ, M.F., MONTGOMERY, M.W., BUXBAUM , L.J., LEE, S.S., CAREW, T.G., COSLETT, B.H., et al.Naturalistic action impairment in closed head injury. Neuropsychology, 12:13-28, 1998.
SHALLICE, T. Specific impairments of planning. Philosophical Transaction of the Royal Society ofLondon B298: 199-209, 1982.
SHALLICE, T. The Allocation of Processing Resources: Higher Level Control. From Neuropsychology toMental Structures. Cambridge: Cambridge University Press, 1988, pp. 328-352.
SHALLICE, T., and BURGESS, P. Deficits in strategy application following frontal lobe damage in man.Brain, 114:727-742, 1991.
SHALLICE, T., BURGESS, P.W., SCHON, F., and BAXTER, D.M. The origins of utilization behavour. Brain,112: 1587-1598, 1989.
SIRIGU, A., ZALLA , T., PILLON, B., GRAFMAN, J., AGID, Y., and DUBOIS, B. Selective impairments inmanagerial knowledge following prefrontal cortex damage. Cortex, 31:301-316, 1995.
SIRIGU, A., ZALLA , T., PILLON, B., GRAFMAN, J., AGID, Y., and DUBOIS, B. Selective deficits in scriptsequence and boundary analysis following lesions in the prefrontal cortex. Cortex, 32:297-310,1996.
STUSS, D.T. Disturbances of self-awareness after frontal system damage. In G.P. Prigatano and D.L.Schacter (Eds.), Awareness of Deficit after Brain Injury. Clinical and Theoretical Issues. Oxford:Oxford University Press, 1991, pp. 63-83.
STUSS, D.T., ESKES, G.A., and FOSTER, J.K. Experimental neuropsychological studies of frontal lobefunctions. In F. Boller and J. Grafman (Eds.), Handbook of Neuropsychology, vol 9. Amsterdam:Elsevier Science Publishers, 1994, pp. 149-185.
VÉRIN, M., PARTIOT, A., PILLON, B., MALAPANI , C., AGID, Y., and DUBOIS, B. Delayed response tasks andprefrontal lesions in man: Evidence for self-generated patterns of behaviour with poorenvironmental modulation. Neuropsychologia, 31:1379-1396, 1993.
WHEELER, M.A., STUSS, D.T., and TULVING, E. Toward a theory of episodic memory: The frontal lobesand autonoetic consciousness. Psychology Bulletin, 121:331-354, 1997.
WILSON, B.A., ALDERMAN, N., BURGESS, P., EMSLIE, H., and EVANS, J. Behavioural Assessment of theDysexecutive Syndrome. Bury St Edmunds, Suffolk: Thames Valley Test Company, 1996.
WILSON, B.A., EVANS, J.J., EMSLIE, H., ALDERMAN, M., and BURGESS, P. The development of anecologically valid test for assessing patients with a dysexecutive syndrome. NeuropsychologicalRehabilitation, 8:213-228, 1998.
Bernard Pillon, Centre de Neuropsychologie, Fédération de Neurologie, Hôpital de la Salpêtrière, 47 Boulevard de l’Hôpital, 75651 Pariscedex 13, France. E-mail: [email protected]
(Received 13 July 1999; accepted 21 March 2000)
Script execution 669