Embed Size (px)
Citation preview
An Emergency Department Guideline for the Diagnosisof Pulmonary Embolism: An Outcome Study
Michael D. Brown, MD, MSc, Steven J. Vance, MD, Jeffery A. Kline, MD
AbstractObjective: To assess the clinical outcome of patientssuspected of pulmonary embolism (PE) following implemen-tation of an emergency department (ED) diagnostic guideline.Methods: A prospective observational study of all patientssuspected of PE who presented to the ED during a four-monthstudy period. The authors’ modification of the Charlottecriteria recommended D-dimer testing in those younger than70 years of age with a low clinical suspicion of PE and nounexplained hypoxemia, unilateral leg swelling, recentsurgery, hemoptysis, pregnancy, or prolonged duration ofsymptoms. The primary outcome was the identification ofvenous thromboembolism during a three-month follow-upperiod. The negative predictive value of the overall diagnosticstrategy and the test characteristics of D-dimer werecalculated. Results: A total of 1,207 consecutive patientswere evaluated for suspected PE; 71 (5.8%) were diagnosed
with venous thromboembolism. One missed case of PE wasidentified on follow-up, yielding a negative predictive valueof 99.9% (95% confidence interval [CI] = 99.5% to 100%). Themissed case was a patient who presented with pleuritic chestpain and shortness of breath; a chest radiograph revealedpneumothorax, and the physician decided not to pursue thepositive D-dimer result. The patient returned six weeks laterwith PE. Subgroup analysis of patients having D-dimerperformed (n = 677) yields a sensitivity of 0.93 (95% CI = 0.77to 0.98) and a specificity of 0.74 (95% CI = 0.70 to 0.77).Conclusions: Implementation of a PE diagnostic guidelinein a community ED setting is safe and has improved thespecificity of the enzyme-linked immunosorbent assayD-dimer test when compared with previous studies.Key words: pulmonary embolism; diagnosis; guideline.ACADEMIC EMERGENCY MEDICINE 2005; 12:20–25.
The evaluation of patients suspected of pulmonaryembolism (PE) is complex, and numerous diagnosticstrategies have been suggested.1–7 Clinical guidelinesor protocols may assist physicians with complicateddiagnostic algorithms and improve care by decreasinginappropriate variance in practice style.8,9 At the sametime, algorithms that reduce patient care into a se-quence of binary decisions often do injustice to thecomplexity of medicine.10 The rationale for a PE rule-out protocol has been described; however, the safetyand efficiency of a PE rule-out protocol awaits empiricconfirmation.11,12
Generally, simple innovations spread faster thancomplicated ones.13 A prediction rule will be used if itmakes clinical sense and is simple.14 One of the aimsof our PE diagnostic guideline was to simplify thecomplicated algorithms and decision rules that have
been proposed.1 The guideline focus was on pretestprobability assessment and the appropriate use ofD-dimer testing.7,8,12 The implementation of a PE rule-out protocol or guideline requires the understandingand approval of physicians at the local level. Theemergency physicians at our institution agreed tostart with empiric clinical judgment to arrive ata pretest probability for PE and then apply a modifi-cation of the Charlotte criteria to assist in diagnosticdecision making.7,15 This provided shape and struc-ture to our clinical judgment yet maintained thedecision-making flexibility that is often requiredwhen applying rules to the individual patient.16 Fora PE rule-out protocol to be considered safe, it hasbeen recommended that the posttest probability ofa negative workup be ,1%12 or that the upper 95%confidence limit be ,3%.1
There has been a call for increased implementationresearch and, more specifically, the evaluation ofdiagnostic strategies in practice.17 The primary objec-tive of our study was to determine the safety of a PEdiagnostic guideline in the emergency department(ED) setting based on the number of cases of missedPE identified over a three-month follow-up period. Asecondary objective was to assess the efficiency of theguideline by determining the test performance ofD-dimer in the low-risk subgroup and the rate ofnegative formal imaging for PE after implementationof our PE rule-out protocol.
From the Grand Rapids MERC/Michigan State University Programin Emergency Medicine (MDB, SJV), Grand Rapids, MI; andDepartment of Emergency Medicine, Carolinas Medical Center(JAK), Charlotte, NC.Received May 3, 2004; revision received July 24, 2004; acceptedAugust 2, 2004.Supported in part by K-30 award #HL04113 from National Heart,Lung, and Blood Institute.Address for correspondence: Michael D. Brown, MD, MSc, Spec-trum Health—Butterworth, Emergency Medicine, 100 MichiganAvenue NE, Grand Rapids, MI 49503. Fax: 616-391-3674; e-mail:[email protected]:10.1197/j.aem.2004.08.046
20 Brown et al. d PE DIAGNOSTIC GUIDELINE

METHODS
Study Design. This prospective observational studyassessed the clinical outcome of patients suspected ofPE following implementation of an ED diagnosticguideline. The guideline was introduced and ap-proved by the Department of Emergency Medicinefive months before initiation of the study. To encour-age appropriate use of the enzyme-linked immuno-sorbent assay (ELISA) D-dimer as outlined in theguideline, the summary (Table 1) was embeddedin the software of the electronic medical record andshowed as a ‘‘pop-up’’ on the order entry screenwhenever a physician ordered a D-dimer test.9,18
Physicians were also encouraged to utilize a simpleworksheet that included a summary flow diagram andthe following questions: 1) Does the patient typicallyseek care at Spectrum Health? 2) What is the pretestprobability for PE: low (,20%), intermediate, or high?The hospital’s institutional review board approved theobservational study and required written or verbalinformed consent for follow-up contact only.
Study Setting and Population. The study wasconducted at two community EDs with a combinedannual ED census of approximately 130,000 in 2003.Spectrum Health—Butterworth is an urban teachinghospital with 30 emergency medicine residents and 31full-time attending physicians. Spectrum Health—Blodgett is an affiliated suburban hospital withoutan emergency medicine residency program and 15full-time attending physicians. Patients were enrolledfor 15 weeks, from May 21 to August 28, 2003.
The study population consisted of a consecutivesample of adult patients (18 years or older) presentingto the ED with clinical suspicion of acute PE. Patientswere identified either by completion of a PE worksheetby the emergency physician or by research staff usingthe electronic medical record to identify all patientshaving had a diagnostic test for PE during each weekof the study period. Diagnostic tests queried on theelectronic medical record included all ED patientshaving had a D-dimer test, computerized tomography(CT) pulmonary angiography, combined CT venogra-phy and pulmonary angiography (CTVPA), ventila-tion-perfusion scintillation lung scan, or pulmonary
angiography. All potential patients identified in theelectronic medical record screen performed by theresearch staff were reviewed by one of the investiga-tors (SJV) to confirm that these patients were eligiblefor study enrollment (clinical suspicion for PE).
Study Protocol. The Charlotte criteria are based ona set of predictors derived from a typical outpatientED population.15 We used a modification of this rule(Table 1) that retained the four strongest predictors,because in a derivation population it was found thatthe presence of any one of these predictors increasedthe pretest probability of PE into the moderate to highrange. Other modifications were based on the desireto minimize false-positive D-dimer test results. Priorwork has shown that elder patients often havecomorbidities that result in a significant decrease inthe specificity of the D-dimer test to an unacceptablylow level (14%–17%).19–21 Receiver operating charac-teristic curve analysis on age in the original databasefor the Charlotte criteria indicated a minimal changein the likelihood ratio negative with adjustment of agefrom 50 to 70 years. Moreover, prior work has shownthat approximately 75% of all healthy, pregnantwomen have a D-dimer level above the traditionalcutoff of 500 ng/mL.22 Accordingly, we modified theCharlotte rule such that patients aged 70 years orolder and pregnant patients were ineligible forD-dimer testing. Because we were concerned abouta possible decrease in sensitivity of the D-dimer withprolonged duration of symptoms, patients withsymptoms present for $4 days were also consideredineligible for D-dimer testing.21
According to the diagnostic guideline, all adultpatients presenting with suspicion for PE were firststratified into low (, 20%) or moderate to high pretestprobability risk groups using the empiric clinicaljudgment of the treating physician. The guidelinerecommended that patients with moderate to highprobability of PE undergo diagnostic imaging to assessfor suspected PE without obtaining a D-dimer level.D-dimer testing was recommended for patients withlow probability for PE as determined by the empiricjudgment of the treating physician. However, if any ofthe following criteria were present, the guidelinesuggested that the patient was ineligible for D-dimertesting: unexplained hypoxia (pulse oximetry ,95%),unilateral leg swelling, surgery within the past fourweeks, hemoptysis, pregnancy, age 70 years or older,or duration of symptoms $4 days (Table 1). Diagnosticimaging was recommended for patients having a pos-itive D-dimer (ELISA D-dimer $500 ng/mL). Due tothe wide range of reported sensitivity of CT angiogra-phy23–25 and the uncertain significance of a missed sub-segmental PE,26 the guideline suggested CTVPA as theimaging modality of choice.27,28 However, CTVPA wasnot recommended in patients with renal insufficiency,pregnancy, or allergy to iodinated contrast dye.6 In
TABLE 1. Summary of Diagnostic Guideline forAppropriate Use of D-dimer Testing
D-dimer testing not recommended if any one of the following:Unexplained hypoxia (pulse oximetry ,95%)Unilateral leg swellingRecent surgery (within past four weeks)HemoptysisPregnancyAge 70 years or olderDuration of symptoms $4 days
ACAD EMERG MED d January 2005, Vol. 12, No. 1 d www.aemj.org 21

such cases, the guideline suggested that the treatingphysician consult with the radiologist regarding im-aging alternatives.
Measurements. Although a positive pulmonary an-giogram or autopsy has historically been the referencestandard for the diagnosis of PE, we considered anyone of the following as acceptable surrogate referencestandards: 1) CT or pulmonary angiography positivefor PE, 2) lower extremity imaging (Doppler ultraso-nography or CT venography) positive for deep veinthrombosis, 3) high probability ventilation-perfusionscintillation lung scan, or 4) death secondary tovenous thromboembolism. Similar to most contempo-rary PE studies, the absence of a thromboembolicevent over a minimum of three months was consid-ered the reference standard for ruling out PE.1,29–31
Following a negative ED workup for PE, researchstaff ascertained the occurrence of venous thrombo-embolism over the following three months by search-ing the electronic medical record and completinga data collection form on all subjects. Although theelectronic medical record was used as the primarysource for follow-up on all patients, for those patientswho did not confirm with the emergency physicianthat they routinely utilize the Spectrum Health systemfor their health care needs, a member of the researchstaff attempted scripted telephone follow-up afterthree months to determine if they had been diagnosedwith venous thromboembolism since the time of EDdischarge. If contact by telephone was unsuccessfulafter three attempts on different days, a questionnairewas sent via U.S. mail. Kent County medical examinerrecords were searched for matches for all enrolledsubjects over the three-month follow-up period. Inaddition, if both telephone and mail follow-upattempts were unsuccessful, a search of the socialsecurity death index was performed. Data wereentered into Microsoft Access 2000 (Microsoft Corp.,Redmond, WA).
Primary Outcome Measurement. The primary out-come was the negative predictive value of the pro-tocol. Any patient diagnosed as having venousthromboembolism (deep vein thrombosis or PE) inthe three-month period following a negative EDevaluation for PE was considered a missed PE (false-negative workup). Because the exact cause of death isoften uncertain when an autopsy is not performed, wecalculated the results on a ‘‘worst-case’’ scenario basis,which assumes all unexpected deaths of unknowncause to be secondary to PE. An unexpected death ofuncertain cause was defined as a patient younger than90 years of age with absence of a clear alternativemechanism of death (e.g., trauma, septic shock, in-tracranial hemorrhage), a defined end-stage diseasebeing treated with comfort care only (e.g., metastaticcancer, end-stage renal failure with withdrawal of
dialysis), hospice care, and absence of a ‘‘do not re-suscitate’’ order. The objective was a 99% negativepredictive value (1% false-negative rate).
Data Analysis. The negative predictive value of thediagnostic guideline was calculated as the number ofpatients with a negative workup for PE in the ED andno evidence of thromboembolism on follow-up (truenegatives) divided by the total number of patientswith a negative ED workup (true negatives and falsenegatives).
Statistical analysis was performed using simpleproportions with 95% confidence intervals (CIs) whereappropriate. Statistical tests were performed using theSAS statistical application program (version 8.0; SASInstitute Inc., Cary, NC) and Confidence IntervalAnalysis (version 2.0; University of Southampton,Southampton, England).
The sample size was calculated based on an esti-mated negative predictive value of 99.5% with a 95%CI width of 0.8. In order to obtain a 95% CI of 99.1% to99.9% for the negative predictive value, we estimatedthat a total sample size of 1,193 subjects would berequired based on an estimated PE prevalence of 20%.
RESULTS
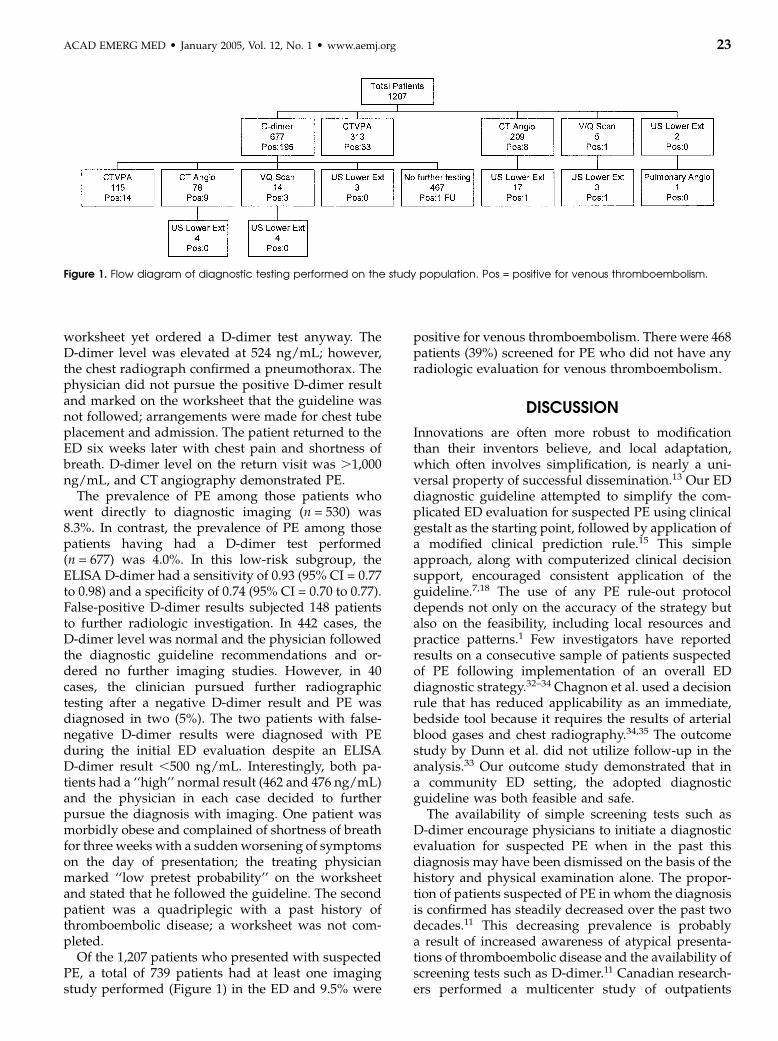
Characteristics of Study Subjects. The study cohortincluded 1,207 patients with a mean age of 48 years(range, 18–96 years) and a 2:1 female predominance(n = 792). Seventy-one (5.8%) were diagnosed withvenous thromboembolism; 70 were diagnosed withPE during the initial ED visit, and one missed case wasidentified at three-month follow-up. The 1,137 patientswith a negative ED evaluation had three-monthfollow-up performed using the electronic medicalrecord. In addition, three-month telephone or mailcontact was attempted on 896 patients who were notconfirmed by the treating emergency physician asroutinely seeking care through the Spectrum Healthsystem; telephone or mail follow-up was successful in52%. In those discharged from the ED followinga negative workup, follow-up confirmed 22 deaths;no deaths were directly attributable to PE. The di-agnostic testing strategy used by the treating physi-cians is summarized in Figure 1.
Main Results. Following implementation of the EDdiagnostic guideline, the overall miss rate was 0.1%(1/1,137), resulting in a negative predictive value of99.9% (95% CI = 99.5% to 100%). The only definitivelyconfirmed missed case was a 48-year-old man witha history of spontaneous pneumothorax and PE whopresented with sudden onset of pleuritic chest painassociated with shortness of breath and hypoxia.Examination revealed tachycardia and decreasedbreath sounds on the left. The treating physician hadmarked ‘‘intermediate pretest probability’’ on the
22 Brown et al. d PE DIAGNOSTIC GUIDELINE
worksheet yet ordered a D-dimer test anyway. TheD-dimer level was elevated at 524 ng/mL; however,the chest radiograph confirmed a pneumothorax. Thephysician did not pursue the positive D-dimer resultand marked on the worksheet that the guideline wasnot followed; arrangements were made for chest tubeplacement and admission. The patient returned to theED six weeks later with chest pain and shortness ofbreath. D-dimer level on the return visit was .1,000ng/mL, and CT angiography demonstrated PE.
The prevalence of PE among those patients whowent directly to diagnostic imaging (n = 530) was8.3%. In contrast, the prevalence of PE among thosepatients having had a D-dimer test performed(n = 677) was 4.0%. In this low-risk subgroup, theELISA D-dimer had a sensitivity of 0.93 (95% CI = 0.77to 0.98) and a specificity of 0.74 (95% CI = 0.70 to 0.77).False-positive D-dimer results subjected 148 patientsto further radiologic investigation. In 442 cases, theD-dimer level was normal and the physician followedthe diagnostic guideline recommendations and or-dered no further imaging studies. However, in 40cases, the clinician pursued further radiographictesting after a negative D-dimer result and PE wasdiagnosed in two (5%). The two patients with false-negative D-dimer results were diagnosed with PEduring the initial ED evaluation despite an ELISAD-dimer result ,500 ng/mL. Interestingly, both pa-tients had a ‘‘high’’ normal result (462 and 476 ng/mL)and the physician in each case decided to furtherpursue the diagnosis with imaging. One patient wasmorbidly obese and complained of shortness of breathfor three weeks with a sudden worsening of symptomson the day of presentation; the treating physicianmarked ‘‘low pretest probability’’ on the worksheetand stated that he followed the guideline. The secondpatient was a quadriplegic with a past history ofthromboembolic disease; a worksheet was not com-pleted.
Of the 1,207 patients who presented with suspectedPE, a total of 739 patients had at least one imagingstudy performed (Figure 1) in the ED and 9.5% were
positive for venous thromboembolism. There were 468patients (39%) screened for PE who did not have anyradiologic evaluation for venous thromboembolism.
DISCUSSION
Innovations are often more robust to modificationthan their inventors believe, and local adaptation,which often involves simplification, is nearly a uni-versal property of successful dissemination.13 Our EDdiagnostic guideline attempted to simplify the com-plicated ED evaluation for suspected PE using clinicalgestalt as the starting point, followed by application ofa modified clinical prediction rule.15 This simpleapproach, along with computerized clinical decisionsupport, encouraged consistent application of theguideline.7,18 The use of any PE rule-out protocoldepends not only on the accuracy of the strategy butalso on the feasibility, including local resources andpractice patterns.1 Few investigators have reportedresults on a consecutive sample of patients suspectedof PE following implementation of an overall EDdiagnostic strategy.32–34 Chagnon et al. used a decisionrule that has reduced applicability as an immediate,bedside tool because it requires the results of arterialblood gases and chest radiography.34,35 The outcomestudy by Dunn et al. did not utilize follow-up in theanalysis.33 Our outcome study demonstrated that ina community ED setting, the adopted diagnosticguideline was both feasible and safe.
The availability of simple screening tests such asD-dimer encourage physicians to initiate a diagnosticevaluation for suspected PE when in the past thisdiagnosis may have been dismissed on the basis of thehistory and physical examination alone. The propor-tion of patients suspected of PE in whom the diagnosisis confirmed has steadily decreased over the past twodecades.11 This decreasing prevalence is probablya result of increased awareness of atypical presenta-tions of thromboembolic disease and the availability ofscreening tests such as D-dimer.11 Canadian research-ers performed a multicenter study of outpatients
Figure 1. Flow diagram of diagnostic testing performed on the study population. Pos = positive for venous thromboembolism.
ACAD EMERG MED d January 2005, Vol. 12, No. 1 d www.aemj.org 23

suspected of PE and reported a prevalence of 9%.36
The lower prevalence of PE (6%) in our studypopulation confirms this trend and may reflect physi-cian concern for malpractice litigation in the UnitedStates. Our prevalence was similar to that in an ED-based study that assessed the efficiency and effective-ness of using D-dimer testing as a screening test forPE.33 If physicians are now ordering D-dimer tests onpatients with a very low pretest probability, whichinevitably results in some false-positive results, it mustbe questioned whether these subjects with very lowsuspicion for PE are being exposed to unnecessaryradiologic studies. It has been suggested that at least50% of patients screened with D-dimer testing musthave a negative result in order to avoid increasedutilization of radiographic imaging.12 Of the totalnumber of D-dimer tests obtained in our studypopulation, 71% were negative. Use of the guidelineimproved the specificity of the ELISA D-dimer testwhen compared with previously reported studies.19
We believe that use of our diagnostic guideline wouldhave had a similar effect on the test characteristics ofa turbidimetric D-dimer test.37,38
LIMITATIONS
The primary objective of this study was to evaluatethe safety of an ED diagnostic guideline for PE. Due toincorporation bias, the classic test characteristics (i.e.,sensitivity, specificity) of the overall guideline cannotbe accurately assessed because portions of the di-agnostic guideline were also considered the criterionstandard for identifying the presence of venousthromboembolism (i.e., false-positive diagnostic im-aging could not be ascertained). A secondary objectivewas to determine if use of the guideline wouldimprove D-dimer test performance. Thus, the resultsof this subgroup analysis must be interpreted andapplied with caution because selection bias wasintentionally introduced within the guideline. Thetest characteristics of the ELISA D-dimer reported inthis study should only be applied to a restricted low-risk patient population as described.
If a clinical decision support instrument is to besuccessful, physicians must be allowed to exercisetheir clinical judgment and override the guidelinerecommendations.18 There were 20 instances in whichthe physician ordered a D-dimer test in patients 70years of age or older. As expected, the specificityamong this elder subgroup was very low at 26%. Weidentified a number of cases in which the physicianordered a D-dimer test and then chose to disregard theresult; an imaging study was ordered on 40 patientsdespite a negative D-dimer result. To order a diagnos-tic study and then discard the result would appear tobe a waste of health care resources. However, theguideline allowed for flexibility with application to theindividual patient; this explains how two patients with
false-negative D-dimer results were diagnosed withPE in the ED. It may be argued that these two patientsshould have gone directly to imaging without D-dimertesting because both had risk factors for PE (morbidobesity and immobility). However, these are examplesof traditional, population-based risk factors associatedwith venous thromboembolism that may influenceclinical decision making on the individual patient yetmay not be strong enough predictors in databasesderived from ED patients to incorporate into a pre-diction rule.39
Ideally, all patients suspected of PE would have hadan estimate of pretest probability documented. Theinvestigators had discussed the possibility of creatinga system whereby the entry of an order for a D-dimertest or a radiologic imaging study for PE would not beprocessed without a completed pretest probabilityestimate on an electronic form. This option was metwith resistance by the local clinicians and was viewedas obstructing physician efficiency and patient flow.Instead, physicians were ‘‘encouraged’’ to completea pretest probability assessment form. The compliancewith this approach was too low to be of any use in theanalysis. Performing three-month follow-up using theelectronic medical record was very efficient andaccurate. Telephone follow-up was resource intensivewith very low yield. Investigators performing follow-up for outcome studies or quality assurance auditsshould consider using the electronic medical record asa reliable and efficient source of data.
Our modifications to the Charlotte rule could bereconsidered. The decision to exclude patients for pro-longed duration of symptoms was based on indicativerather than conclusive evidence.21,40 Our secondaryanalysis did not show additional benefit to includingthis term in the screening process.
CONCLUSIONS
Clinical guidelines have the potential to improvehealth outcomes and reduce costs. However, the bestcare for the majority of patients, as recommended inthe guideline, may be inappropriate for the individualpatient.10 Physicians must continue to use goodclinical judgment when deciding to follow any guide-line.8 This outcome study has demonstrated thatimplementation of a PE diagnostic guideline in a com-munity hospital ED is safe and efficient.
The authors thank Jan Anderson, RN, Jennifer Kolenda, BA,Nikalus Sheridan, and Laurel Viewig, BS, for assistance with datamanagement and Thomas Summerfelt, PhD, and Steve Korzeniew-ski, BA, for assistance with statistical analysis.
References
1. Kruip MJ, Leclercq MG, van der Heul C, Prins MH, Buller HR.Diagnostic strategies for excluding pulmonary embolism inclinical outcome studies: a systematic review. Ann Intern Med.2003; 138:941–51.
24 Brown et al. d PE DIAGNOSTIC GUIDELINE
2. Wells PS, Ginsberg JS, Anderson DR, et al. Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism. Ann Intern Med. 1998; 129:997–1005.
3. Perrier A, Desmarais S, Miron MJ, et al. Non-invasivediagnosis of venous thromboembolism in outpatients. Lancet.1999; 353:190–5.
4. Michiels JJ. Rational diagnosis of pulmonary embolism(RADIA PE) in symptomatic outpatients with suspected PE: animproved strategy to exclude or diagnose venousthromboembolism by the sequential use of a clinical model,rapid ELISA D-dimer test, perfusion lung scan,ultrasonography, spiral CT, and pulmonary angiography.Semin Thromb Hemost. 1998; 24:413–8.
5. Gallagher EJ. Clots in the lung. Ann Emerg Med. 2000; 35:181–7.6. Fedullo PF, Tapson VF. The evaluation of suspected pulmonary
embolism. N Engl J Med. 2003; 349:1247–56.7. Chunilal SD, Eikelboom JW, Attia J, et al. Does this patient
have pulmonary embolism? JAMA. 2003; 290:2849–58.8. Fesmire FM, Kline JA, Wolf SJ, et al. Clinical policy: Critical
issues in the evaluation and management of adult patientspresenting with suspected pulmonary embolism. Ann EmergMed. 2003; 41:257–70.
9. Buller-Close K, Schriger D, Baraff L. Heterogeneous effect of anemergency department expert charting system. Ann EmergMed. 2003; 41:644–52.
10. Woolf SH, Grol R, Hutchinson A, Eccles M, Grimshaw J.Clinical guidelines: Potential benefits, limitations, and harmsof clinical guidelines. BMJ. 1999; 318:527–30.
11. Kelly J, Hunt BJ. A clinical probability assessment and D-dimermeasurement should be the initial step in the investigation ofsuspected venous thromboembolism. Chest. 2003; 124:1116–9.
12. Kline J, Wells P. Methodology for a rapid protocol to rule outpulmonary embolism in the emergency department. AnnEmerg Med. 2003; 42:266–75.
13. Berwick DM. Disseminating innovations in health care. JAMA.2003; 289:1969–75.
14. Laupacis A, Sekar N, Stiell IG. Clinical prediction rules. Areview and suggested modifications of methodologicalstandards. JAMA. 1997; 277:488–94.
15. Kline JA, Nelson RD, Jackson RE, Courtney DM. Criteria forthe safe use of D-dimer testing in emergency departmentpatients with suspected pulmonary embolism: a multicenterUS study. Ann Emerg Med. 2002; 39:144–52.
16. Gallagher EJ. The intrinsic fallibility of clinical judgment. AnnEmerg Med. 2003; 42:403–4.
17. Knottnerus JA, van Weel C, Muris JWM. Evidence base ofclinical diagnosis: Evaluation of diagnostic procedures. BMJ.2002; 324:477–80.
18. Bates DW, Kuperman GJ, Wang S, et al. Ten commandmentsfor effective clinical decision support: making the practice ofevidence-based medicine a reality. J Am Med Inform Assoc.2003; 10:523–30.
19. Brown MD, Rowe BH, Reeves MJ, Bermingham JM, GoldhaberSZ. The accuracy of the enzyme-linked immunosorbent assayD-dimer test in the diagnosis of pulmonary embolism: a meta-analysis. Ann Emerg Med. 2002; 40:133–44.
20. Righini M, Goehring C, Bounameaux H, Perrier A. Effects ofage on the performance of common diagnostic tests forpulmonary embolism. Am J Med. 2000; 109:357–61.
21. Heit JA, Minor TA, Andrews JC, Larson DR, Li H, Nichols WL.Determinants of plasma fibrin D-dimer sensitivity for acutepulmonary embolism as defined by pulmonary angiography.Arch Pathol Lab Med. 1999; 123:235–40.
22. Giavarina D, Mezzena G, Dorizzi RM, Soffiati G. Referenceinterval of D-dimer in pregnant women. Clin Biochem. 2001;34:331–3.
23. Rathbun SW, Raskob GE, Whitsett TL. Sensitivity andspecificity of helical computed tomography in the diagnosis of
pulmonary embolism: a systematic review. Ann Intern Med.2000; 132:227–32.
24. Mullins MD, Becker DM, Hagspiel KD, Philbrick JT. The role ofspiral volumetric computed tomography in the diagnosis ofpulmonary embolism. Arch Intern Med. 2000; 160:293–8.
25. Perrier A, Howarth N, Didier D, et al. Performance of helicalcomputed tomography in unselected outpatients withsuspected pulmonary embolism. Ann Intern Med. 2001;135:88–97.
26. Swensen SJ, Sheedy PF II, Ryu JH, et al. Outcomes afterwithholding anticoagulation from patients with suspectedacute pulmonary embolism and negative computedtomographic findings: a cohort study. Mayo Clin Proc. 2002;77:130–8.
27. Richman PB, Wood J, Kasper DM, et al. Contribution ofindirect computed tomography venography to computedtomography angiography of the chest for the diagnosis ofthromboembolic disease in two United States emergencydepartments. J Thromb Haemost. 2003; 1:652–7.
28. Katz DS, Loud PA, Bruce D, et al. Combined CT venographyand pulmonary angiography: a comprehensive review.Radiographics. 2002; 22:S3–19.
29. Michiels JJ, Perrier A, Bounameaux H. Should a normalD-dimer rule out angiographic pulmonary embolism orunfavorable outcome in patients left untreated? ThrombHaemost. 2001; 85:753–4.
30. Wolfe TR, Hartsell SC. Pulmonary embolism: making sense ofthe diagnostic evaluation. Ann Emerg Med. 2001; 37:504–14.
31. Bossuyt PM, Reitsma JB, Bruns DE, et al. Towards completeand accurate reporting of studies of diagnostic accuracy: theSTARD initiative. BMJ. 2003; 326:41–4.
32. Kruip MJ, Slob MJ, Schijen JH, van der Heul C, Buller HR. Useof a clinical decision rule in combination with D-dimerconcentration in diagnostic workup of patients with suspectedpulmonary embolism: a prospective management study. ArchIntern Med. 2002; 162:1631–5.
33. Dunn KL, Wolf JP, Dorfman DM, Fitzpatrick P, Baker JL,Goldhaber SZ. Normal D-dimer levels in emergencydepartment patients suspected of acute pulmonary embolism.J Am Coll Cardiol. 2002; 40:1475–8.
34. Chagnon I, Bounameaux H, Aujesky D, et al. Comparison oftwo clinical prediction rules and implicit assessment amongpatients with suspected pulmonary embolism. Am J Med.2002; 113:269–75.
35. Wicki J, Perneger TV, Junod AF, Bounameaux H, Perrier A.Assessing clinical probability of pulmonary embolism in theemergency ward: a simple score. Arch Intern Med. 2001;161:92–7.
36. Wells PS, Anderson DR, Rodger M, et al. Excluding pulmonaryembolism at the bedside without diagnostic imaging:management of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and d-dimer. Ann Intern Med. 2001; 135:98–107.
37. Schrecengost JE, LeGallo RD, Boyd JC, et al. Comparison ofdiagnostic accuracies in outpatients and hospitalized patientsof D-dimer testing for the evaluation of suspected pulmonaryembolism. Clin Chem. 2003; 49:1483–90.
38. Brown MD, Lau J, Nelson RD, Kline JA. Turbidimetric D-dimertest in the diagnosis of pulmonary embolism: a metaanalysis.Clin Chem. 2003; 49:1846–53.
39. Rockhill B. The privatization of risk. Am J Public Health. 2001;91:365–8.
40. Kuruvilla J, Wells PS, Morrow B, MacKinnon K, Keeney M,Kovacs MJ. Prospective assessment of the natural history ofpositive D-dimer results in persons with acute venousthromboembolism (DVT or PE). Thromb Haemost. 2003; 89:284–7.
ACAD EMERG MED d January 2005, Vol. 12, No. 1 d www.aemj.org 25