Embed Size (px)
Citation preview

Abstract of Thesis entitled
“An Evidence-based Guideline of Using Mirror Therapy to Promote
Motor Function Recovery of Upper Limb in Stroke Patient”
Submitted by
Lau Yuen Pan
for the Degree of Master of Nursing
at the University of Hong Kong
in August 2014
Overview
Stroke is common around the world. It causes many disabilities every year.
Among the stroke survivors, half of them have the problem of hemiparesis. It still
persists and disturbs their lives more than half year. In Hong Kong, the hospital
setting is busy and standard stroke rehabilitation is not enough for recovery of stroke.
These lead to delay of rehabilitation process. Therefore, introduction of mirror therapy
is the alternatives to improve their motor function and quality of life with low cost
and manpower. Mirror therapy triggers the activation of the brain to help the recovery
of the motor function. Therefore, the aims of this research are to explore the
effectiveness of mirror therapy to help the stroke survivors to cope with the disability
of upper limb function and to develop an evidence-based guideline of using mirror
therapy for health care profession in Hong Kong setting.
Method
A literature review was conducted to evaluate the possibility of using mirror
therapy to improve stroke survivors’ upper limb motor function. The selected topic of
this study was that “in patients suffering from stroke with hemiparesis, how effective
is the mirror therapy in promoting motor function recovery of their paretic upper

limbs?” and the target group of this review was stroke patients. Database “ProQuest”
and “PubMed” were used for searching for the studies related to stroke and mirror
therapy and eight studies were found finally. Critical Appraisal tool from Scottish
Intercollegiate Guidelines Network was used to assess the quality of the studies.
Results
After summarized the studies, statistically significant results were noted towards
mirror therapy’s arm. Evidence showed that mirror therapy was a possible treatment
to improve patient’s upper limb function recovery with long term effect. The detail of
the studies provided useful information to develop the evidence-based guideline of
mirror therapy. A 4 weeks mirror therapy with 4 and 24 weeks follow-up was given to
stroke survivors to enhance their recovery. Assessment tools, the Action Research
Arm Test and the Functional Independence Measure, were used at baseline, after
intervention and during follow-up to assess their improvements.
Implementation potential was assessed to improve the transferability and
feasibility in Hong Kong public hospital setting. Implementation plan was proposed to
improve the communication between stakeholders. Evaluation plan was used to assess
the outcomes of survivors’ upper limb function and level of independence.
Satisfaction level of staff and patients were also included.
Conclusion
From the results of the relevant studies, mirror therapy is found to promote the
motor function recovery of upper limb in stroke survivors. It is worthwhile to conduct
this program to help the stroke survivors to improve quality of life.

An Evidence-based Guideline of Using Mirror Therapy to
Promote Motor Function Recovery of Upper Limb in Stroke
Patient
by
Lau Yuen Pan
B.Sc. (Nurs); H.K.U., R.N.
A thesis submitted in partial fulfilment of the requirements for
the Degree of Master of Nursing
at The University of Hong Kong
August 2014

i
Declaration
I declare that this thesis represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualifications.
…………………………………………………………….
Lau Yuen Pan

ii
Acknowledgements
I would like to express my great appreciation to my supervisor, Dr. Athena Hong,
for her valuable suggestions during the construction of my thesis in the past 2 years.
Without her opinions and guidance, this thesis would not have been possible. I also
take this opportunity to thank Dr. Daniel Fong and Dr. Patsy Chau for their valuable
information during tutorial which helped me in completing my thesis.
I am obliged to staff members of School of Nursing in the University of Hong
Kong for their help during my study in the Master of Nursing course. Secondly, I am
grateful to my colleague of my workplace whose willingness to share their knowledge
made me understands more on my thesis.
Lastly, I would also like to thank my friends and classmates for their sharing of
sadness and happiness during master work.

iii
TABLE OF CONTENTS
Page
Declaration………………………………………………………… i
Acknowledgement…………………………………………………. ii
Table of Contents………………………………………………….. iii
Chapter 1: Introduction…………………………………………. 1
1.1 Background……………………………………………………….. 1
1.2 Affirming Needs…………………………………………………...
1.2.1 Current Practice in Hong Kong……………………………..
1.2.2 Problem of Clinical Situation…………………………….....
1.2.3 Introduction of Mirror Therapy……………………………..
1.2.4 Affirming Needs of Mirror Therapy………………………...
2
2
3
4
5
1.3 Research Question, Objectives, Significance……………………
1.3.1 Research Question…………………………………………..
1.3.2 Objectives…………………………………………………...
1.3.3 Significance…………………………………………………
6
6
6
7
Chapter 2: Critical Appraisal…………………………………... 9
2.1 Search Strategies…………………………………………………..
2.1.1 Search Methodology………………………………………...
2.1.2 Keywords……………………………………………………
2.1.3 Selection Criteria……………………………………………
2.1.3.1 Inclusion Criteria…………………………………...
2.1.3.2 Exclusion Criteria…………………………………..
9
9
9
10
10
10
2.2 Appraisal Strategies………………………………………….…... 10

iv
Page
2.3 Appraisal Results………………………………………………....
2.3.1 Searching Results……………………………………………
2.3.2 Overview of the Research Design…………………………..
2.3.3 Subject Allocation…………………………………………...
2.3.4 Sample Size………………………………………………….
2.3.5 Application to Local Setting………………………………...
2.3.6 Summary of Quality Appraisal……………………………...
11
11
11
12
12
13
13
2.4 Summary and Synthesis of Results………………………………
2.4.1 Study Design………………………………………………...
2.4.2 Characteristics of the Subjects………………………………
2.4.3 Intervention and Control……………………………………
2.4.3.1 Consideration of Mirror……………………………
2.4.3.2 Execution of Movement during Therapy…………...
2.4.3.3 Therapy Intensity…………………………………...
2.4.3.4 Control Group………………………………………
2.4.4 Data Collection……………………………………………...
2.4.5 Outcome Measurement……………………………………...
2.4.6 Results of the Studies………………………………………..
14
15
15
17
17
18
18
19
19
20
21
2.4 Implication………………………………………………………… 22
Chapter 3: Translation and Implementation…………….. 24
3.1 Implementation Potential……………………………………………….. 24
3.1.1 Proposed Setting and Audience……………………………..
3.1.2 Transferability of the Findings………………………………
3.1.2.1 Target Setting and Population………………………
24
25
25

v
Page
3.1.2.2 Philosophy of Care………………………………….
3.1.2.3 Number of Patients Involved……………………….
3.1.2.4 Duration for Implementation and Evaluation………
3.1.3 Feasibility……………………………………………………
3.1.3.1 Freedom of Implementation………………………...
3.1.3.2 Interference with Routine…………………………..
3.1.3.3 Administration and Colleague Support…………….
3.1.3.4 Skills and Training………………………………….
3.1.3.5 Equipment and Facility……………………….…….
3.1.3.6 Measuring Tools for Evaluation…………….………
3.1.4 Cost and Benefit Ratio of Intervention……………….……..
3.1.4.1 Potential Risk and Benefit of Patients……………...
3.1.4.2 Potential Benefit of Staff and Hospital……….…….
3.1.4.3 Potential Material Costs…………….………………
3.1.4.4 Potential Non-material Costs……………………….
26
26
27
27
27
28
28
29
30
30
30
30
31
32
32
Chapter 4: Developing an Evidence-based Practice
Guideline…………………………………………………….
34
4.1 Title of the Evidence-based Guideline…………………………… 34
4.2 Background……………..………………………………………… 34
4.3 Purpose and Objectives of Guideline……………………………. 35
4.4 Target Group………………………………………………………
4.4.2 Target Population……………………………………………
4.4.1 Target Audience……………………………………………..
35
35
35
4.5 Level of Evidence and Grades of Recommendations…………... 36

vi
Page
4.6 Recommendations………………………………………………… 36
Chapter 5: Implementation Plan………………………….. 39
5.1 Stakeholders Identification…………………………………………...
5.1.1 Administrators……………………………………………….
5.1.2 Trainers……………………………………………………...
5.1.3 Users of the Evidenced-based Guideline……………………
39
39
40
40
5.2 Communication Plan…………………………………………………..
5.2.1 Setting up a Team……………………………………………
5.2.2 Communicating with Administrators………………………..
5.2.3 Briefing Session……………………………………………..
5.2.4 Training Session……………………………………………..
5.2.5 Initiating, Guiding and Sustaining the Intervention…………
40
40
41
42
42
42
5.3 Pilot Test…………………………………………………………………
5.3.1 Aims and Objectives of Pilot Test…………………………...
5.3.2 Recruitment and Duration…………………………………...
5.3.3 Evaluation of Pilot Test……………………………………...
5.3.3.1 Feasibility of Implementing Mirror Therapy……….
5.3.3.2 The difficulty of Subject Recruitment……………...
5.3.3.3 The Evidence-based Guideline in Local Setting……
5.3.3.4 The Acceptance of Staffs…………………………...
43
43
43
44
44
45
45
45
Chapter 6: Evaluation Plan….……………………………. 46
6.1 Identifying Outcomes………………………………………………….
6.1.1 Patient Outcomes……………………………………………
6.1.1.1 Primary Measurement………………………………
46
46
46

vii
Page
6.1.1.2 Secondary Measurement……………………………
6.1.1.3 Level of Satisfaction (Patient)……………………...
6.1.2 Healthcare Provider Outcomes……………………………...
6.1.2.1 Level of Satisfaction (Staff)………………………..
6.1.3 System Outcomes…………………………………………...
6.1.3.1 Length of Hospitalization…………………………..
46
47
47
47
48
48
6.2 Nature of Subjects…………………………………………………….. 48
6.3 Number of Subjects…………………………………………………… 48
6.4 Data Collection………………………………………………………… 49
6.5 Data Analysis…………………………………………………………… 50
6.6 Basis Criteria of Effective Guideline………………………………..
6.6.1 Upper Limb Motor Function of Patients…………………….
6.6.2 Level of Independence of Patients…………………………..
6.6.3 Level of Satisfaction of Patients…………………………….
6.6.4 Level of Satisfaction of Staffs……………………………….
6.6.5 Length of Hospitalization…………………………………...
51
51
51
52
52
52
Chapter 7: Conclusion…………………………………………… 53

viii
Page
Appendices
Appendix (A) Flow Chart of the Search Strategy……………………
Appendix (B) Quality Assessments of the Articles………………..…
Appendix (C) Table of Evidence……………………………………….
Appendix (D) Table of comparison……………………………………
Appendix (E): Potential Material Cost……………………………….
Appendix (F): Recommendation of Evidence-based Practice
Guideline (Detailed)…………………………………………………….
Appendix (G): Level of Evidence and Grades of Recommendation
Appendix (H): Time Frame of the Mirror Therapy Program………
Appendix (I): Post Pilot Study Questionnaire for Staff…………….
Appendix (J): Satisfaction Survey (Patient)………………………….
Appendix (K): Satisfaction Survey (Staff)…………………………….
54
55
61
72
74
75
81
82
83
84
85
References …………………………………………………………………… 86

1
Chapter 1: Introduction
1.1 Background
Stroke onset is unpredictable and sudden. It is the loss of brain function due to
insufficient blood supply to the brain. Patients usually suffer from disabilities on limb
function, language and speech (Bare & Smeltzer, 2004). Their physical activities are
highly affected after this shocking event.
In Hong Kong, stroke is the major cause of death and disability. It was the fourth
leading cause of dead (The department of health, 2012). According to the Hospital
Authority Statistical Report (2011), nearly 25 000 people suffered from stroke in 2010.
There are a huge number of patients in Hong Kong’s health care system.
Long term disability is a frequent consequence of people suffering from stroke.
Hemiparesis on upper limb, weakness on one side of limb, is one of the common
symptoms. Nearly 85% of stroke patients suffered from this problem (Duncan, 2002).
Among those sufferers, only half of them had the chance to recover some of the motor
function after 6 months (Kollen, 2003). As mentioned before that around 25 000
people suffered from stroke, nearly 12 000 stroke survivors had this problem and it
affected them more than 6 months. Declined hand function affected patients’ quality
of life and their abilities to cope with daily living tasks. Not only the physical ability,
but also their psychosocial aspect was affected as their self-esteem was related to their

2
functional abilities (Chang & Mackenzie, 1998). As a result, rehabilitation plays an
important part to stroke survivors in recovery from the influence of this disease.
Mirror therapy is a possible treatment for training of upper limb’s motor function
in stroke survivors (Atay et al., 2008; Baricich et al., 2013; Blasis et al., 2009; Chen et
al., 2013; Cho, et al., 2012; Dohle et al., 2009). Originally, it was used to manage
phantom pain in orthopedics (Ramachandran, as cited in Bayn et al., 2012). Then it
was firstly introduced in stroke rehabilitation field for upper limb motor function
training with positive results (Altschuler et al., 1999). Unlike other training exercise,
mirror therapy was focused on the virtual image of the affected limb which was
observed by the patients (Byan et al., 2012). The virtual image stimulated our brain to
trigger the recovery of the affected side.
1.2 Affirming Needs
1.2.1 Current Practice in Hong Kong
Nowadays, when stroke patients survive the acute phase, they are usually sent to
the stroke rehabilitation unit for further management. Rather than coping life
threatening situation, the goal of sub-acute phase in stroke patients is to improve their
motor function, activities of daily living and facilitate their road back to the society by
providing frequent and intense training (Collier, Dewey & Sherry, 2007).
Multidisciplinary teams are involved to the whole rehabilitation process (Johansson,

3
2011).
In Hong Kong public hospital’s stroke rehabilitation unit, patients’ condition is
assessed during admission. Then a comprehensive training is started as soon as it may
after elimination of unfavorable condition such as high blood pressure, dizziness.
Physiotherapist, occupational therapist, speech therapist and nurses incorporate into
the rehabilitation program to help the patients.
1.2.2 Problem of Clinical Situation
However, due to the shortage of manpower, the ratio of therapist to patient is
extremely low. The bed occupancy rate is usually over 100%. Training can only be
provided to patients for approximately an hour per day. Camicia et al. (2012)
suggested that three hours per day were the thresholds for optimal outcomes for stroke
rehabilitation. One hour is far less than the required standard. Furthermore, in order to
facilitate the discharge of patients, walking on their own is the most promising result.
Therefore, the focusing point of training is mainly on lower limb of the patient. Upper
limb’s training is usually neglected or far lesser. The rehabilitation of upper limb may
not be sufficient to provide good outcome to the patients.
On the other hand, for rehabilitation of motor function of the affected arm, there
are many methods for upper limb training, for example, robot-assisted arm training
(Archambault, Fung & Norouzi-Gheidari, 2012). However, they require large amount

4
of manpower for intensive treatment for the patients. Forced usage of affected limb
also induced distress, physical pain and eventually affected the recovery process
(Bauder, Liepert & Miltner, as cited Cho, Lee & Song, 2012).
1.2.3 Introduction of Mirror Therapy
In consequences, stroke survivors face a difficult time without adequate support
and training. Mirror therapy can be an alternative to help hemiparetic stroke patients
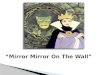
in training motor function. Patients sit close to a table with a mirror placed
perpendicular to the midline of the patients. Then the unaffected upper limb was
placed on the reflected side of the mirror and patients observed the movement of it
(Baricich, 2013). Figure (1) showed the arrangement during applying mirror therapy.
How does mirror therapy work? Funase et al. (2012) said that when patient
observed the movement of the virtual image of affected limb in the mirror, it activated
Affected Unaffected
Mirror on reflected side
Figure (1) – Preparation of Mirror therapy

5
the mirror-neuron system which would be activated when the brain tried to observe
and carry out an action (Cattaneo & Rizzolatti, 2009). Then the primary motor cortex
of the affected limb would be activated due to the observation of action by the mirror
neuron (Craighero & Fadiga, 2004). From the MRI study of Matthys et al. (2009),
mirror therapy induced activation of the brain area involved the motor system of the
non-moving hand. Therefore, it is believed that mirror therapy promotes the
rehabilitation of the paretic limb in stroke patients.
1.2.4 Affirming Needs of Mirror Therapy
Mirror therapy can improve the upper limb function of stroke survivors (Atay et
al., 2008; Baricich et al., 2013; Blasis et al., 2009; Chen et al., 2013; Cho, et al., 2012;
Dohle et al., 2009). It is also simple with only a handy mirror as the equipment. The
cost of using the therapy is comparatively low.
Moreover, mirror therapy is a patient-directed therapy (Atay et al., 2008).
Although nurse to patient ratio is low, nurses may provide sufficient training to
patients as application of mirror therapy is relatively simple. After teaching patients
about the concept and method, patients may continue their training on their own with
low supervision. Sufficient training can be provided to achieve the goal of
rehabilitation.
In addition, since nurses have most of the time accompanying patients, providing

6
training exercise from nurses can be more effective as good rapport can be built easier.
It facilitates the training participation of patients which is one of the important issues
in rehabilitation process (Johansson, 2011).
1.3 Research Question, Objectives, Significance
In this dissertation, the practice guideline of mirror therapy were formulated,
assessed and evaluated. The result and evaluation of the evidence-based integrative
review for mirror therapy were identified in the coming part. Then, the
implementation potential and the development of the evidence-based guideline were
provided. At last, the implementation plan and evaluation of the clinical guideline
were discussed.
1.3.1 Research Question
The following research question was used to guide the integrative review of
mirror therapy:
In patients suffering from stroke with hemiparesis, how effective is the mirror therapy
in promoting motor function recovery of their paretic upper limbs?
1.3.2 Objectives
The objectives of the integrative review were:
To perform a quality critical appraisal of the selected studies related to mirror
therapy;

7
To evaluate the effectiveness and feasibility of mirror therapy in promoting
motor function of upper limb on hemiparetic stroke survivors;
To develop an evidence-based clinical protocol in guiding health care providers
for using mirror therapy to help stroke survivors.
1.3.3 Significance
Mirror therapy is beneficial to patients, health care providers and the hospital.
For patients’ aspect, it may help stroke survivors to improve the motor function of
upper limb. Their activities of daily living can be improved and, as the result, quality
of their lives.
For the health care providers’ aspect, patients under mirror therapy require less
manpower for supervision. After simple education to patients, they can perform
mirror therapy by themselves. Nurses may maximize their usage of time and provide
sufficient training for patients even in the situation of shortage in manpower. Nurses
can also have more involvement in the rehabilitation process despite bed side care.
For hospital aspect, mirror therapy requires only simple equipment and less
manpower. Less cost is needed to provide the treatment. Besides, better rehabilitation
progress may shorten patients’ length of stay in the hospital and reduce the
re-admission rate. These may further lower the cost of providing the services.
In conclusion, an effective evidence-based mirror therapy can improve patients’

8
upper limb motor function, enhance the rehabilitation care by the health care
providers and reduce the cost of stroke care due to shorten of patients’ hospitalization.

9
Chapter 2: Critical Appraisal
After discussing the affirming needs of mirror therapy and the significance of
carrying out mirror therapy to hemiparetic stroke patients, the searching strategies,
appraisal strategies and summary will be discussed in this chapter. Then the results of
the integrative review will be summarized and synthesized.
2.1 Search Strategies
2.1.1 Search Methodology
From 1st July, 2013 to 9
th July, 2013, systematic literature searching was done. It
was based on the research question about mirror therapy which was used to improve
the recovery of motor function on upper limb in hemiparetic stroke survivors.
Therefore, the searching process was focused on the population “stroke” patient and
the intervention “mirror therapy”. Two electronic bibliographic databases, “ProQuest”
and “PubMed”, were used. After screening of topic and abstract, relevant studies were
identified and the reference lists of the findings were also screened for any additional
one. Then the duplicated studies were removed.
2.1.2 Keywords
The following keywords were used for searching. They included “stroke or CVA
or cerebrovascular accident or cerebrovascular disease”, “rehabilitation” and “mirror
therapy or mirror therapy hand”. By combining these groups of keywords, studies

10
with the linkage of stroke and mirror therapy could be found.
2.1.3 Selection Criteria
During screening of topic and abstract, the following criteria were used to
narrow down the selection of studies. The searching strategies’ details and results
could be found in Appendix (A).
2.1.3.1 Inclusion Criteria
Intervention mirror therapy was the main focus of consideration during searching.
The included studies only examined stroke patients with paretic upper limb. Adult
population aged over 18 was the selected target group. Clinical trials, for example
randomized controlled trials (RCTs), were the priority type of studies. Only full text
available studies were included so that the detail of the studies could be accessed. The
outcome measures must include the measurement of upper limb’s function before and
after the intervention.
2.1.3.2 Exclusion Criteria
Studies which focused on the lower limb of stroke patients were excluded. Also,
studies were excluded if there was no measurement on motor function.
2.2 Appraisal Strategies
The quality assessment for all selected studies was done with the use of the
Scottish Intercollegiate Guidelines Network (SIGN) methodology checklist (Scottish

11
Intercollegiate Guidelines Network, 2013). As only clinical trials were included,
checklist SIGN for controlled trials was used. There were fourteen questions in the
checklist to evaluate the internal validity of the studies (SIGN, 2013). The results of
the quality assessment could be found in Appendix (B).
2.3 Appraisal Results
2.3.1 Searching Results
244 studies were identified and screened from the selected databases. Eight
studies which fulfilled the guidance of the inclusion and exclusion criteria were
selected (Altschuler et al., 1999; Atay et al., 2008; Baricich et al., 2013; Bayn et al.,
2012; Blasis et al., 2009; Chen et al., 2013; Cho et al., 2012; Dohle et al., 2009). The
rejected studies were mainly due to duplication, not focus on upper limb’s function or
availability of full text. No additional study was captured from their reference lists.
2.3.2 Overview of the Research Design
All of the selected studies were RCTs between the year of 1999 and 2013. This
type of studies was in high level of evidence and was suitable for drawing conclusion
about the effect of an intervention (Beck & Polit, 2008). They clearly addressed their
purpose of conducting the studies. One of the studies used planned crossover to yield
sample size (Altschuler et al., 1999). However, the effect of the intervention given
first could carry over to the second intervention and affect the results (Beck & Polit,

12
2008). No wash-out period was mentioned in the studies and this may lead to
potential bias.
2.3.3 Subject Allocation
6 of the studies included the randomization methods (Atay et al., 2008; Baricich
et al., 2013; Bayn et al., 2012; Chen et al., 2013; Cho et al., 2012; Dohle et al., 2009).
Concealment method was only mentioned in 3 of the studies (Atay et al., 2008; Chen
et al., 2013; Dohle et al., 2009). Selection bias could occur in the other studies which
may lead to biased sample and lower the quality of the randomization. Fortunately, all
of these studies did the comparison of the baseline measurement. Only one of the
studies’ patients had different characteristics at the start of the study which the time
since stroke of the subjects varied from 6 months to 26 years (Altschuler et al., 1999).
6 of the studies had single blinding to assessor while it could only be done for the
subject allocation because the treatment of mirror therapy could not be hided from the
subjects and the treatment providers (Altschuler et al., 1999; Atay et al., 2008;
Baricich et al., 2013; Blasis et al., 2009; Chen et al., 2013; Dohle et al., 2009).
Performance bias of the subjects could be present as blinding of subject was not
available.
2.3.4 Sample Size
Sample size calculation was mentioned in 6 studies to reach the required sample

13
size to minimize the risk for type II error (Atay et al., 2008; Baricich et al., 2013;
Bayn et al., 2012; Blasis et al., 2009; Chen et al., 2013; Dohle et al., 2009). However,
only two studies mentioned about Intention-to-treat (Bayn et al., 2012; Blasis et al.,
2009). The other studies did not include the dropout subjects and this could lead to
bias with positive treatment effect (Beck & Polit, 2008). Luckily, the dropout rate was
below 20% in most of the studies except the one with 21% in its control group (Chen,
2013). Some of the reasons for the dropout were that subjects refused follow-up,
moved to other district, were clinically deteriorated or died. Also, the problem of
unplanned crossover was not easy to appear as subjects could not do the intervention
without the mirror and all the intervention group were carried out individually except
the one mentioned as grouped mirror therapy (Bayn et al., 2012).
2.3.5 Application to Local Setting
In Hong Kong, stroke patients are usually transferred to stroke rehabilitation
ward after acute management. In seven studies, mirror therapy were used in
institutional base which was similar to local rehabilitation setting (Atay et al., 2008;
Baricich et al., 2013; Bayn et al., 2012; Blasis et al., 2009; Chen et al., 2013; Cho et
al., 2012; Dohle et al., 2009). The remaining one did not mention on it (Altschuler et
al., 1999). One study was conducted in Taiwan which was in Chinese race (Chen et al.,
2013). On instruments, only simple material is needed for mirror therapy. Patients

14
usually discharge from the local setting at most three months due to the shortage of
bed in Hong Kong. Only three studies started the therapy within this time frame
(Baricich et al., 2013; Bayn et al., 2012; Dohle et al., 2009).
2.3.6 Summary of Quality Appraisal
By the use of SIGN form, seven of the studies were graded as “acceptable (+)”
(Atay et al., 2008; Baricich et al., 2013; Bayn et al., 2012; Blasis et al., 2009; Chen et
al., 2013; Cho, et al., 2012; Dohle et al., 2009). The reason was that they could fulfill
60% to 80% of the criteria in the SIGN form. The failing criteria were mainly due to
the studies which had not mention about concealment method and could only do the
assessor blinded studies. Potential bias could alert their quality so they were graded as
acceptable.
The remaining one was only achieved 40% of the criteria. It was graded as
“unacceptable (0)” as there was not enough information provided in the studies like
randomization method, concealment. Furthermore, the measurement tool was
subjective self-rating scale which was not reliable (Altschuler et al., 1999).
2.4 Summary and Synthesis of Results
In this part, the results of the integrative review would be discussed. Based on
the studies with higher quality ranked acceptable, subjects had better improvement in
motor function of upper limb in mirror therapy group. Subjects received conventional

15
stroke rehabilitation program as usual. Then mirror therapy was added into their
program for motor function training (Atay et al., 2008; Baricich et al., 2013; Blasis et
al., 2009; Chen et al., 2013; Dohle et al., 2009). Details were summarized in the table
of evidence in Appendix (C).
2.4.1 Study Design
The study type of all the selected studies was RCTs. Two of them were multi-site
studies (Chen et al., 2013; Blasis et al., 2009). One of them was RCTs with planned
crossover studies (Altschuler et al., 1999). RCTs are the suitable type of study in
proving the effectiveness of an intervention.
2.4.2 Characteristics of the subjects
The comparisons of subject characteristics were summarized in Appendix (D).
The number of subjects in the studies ranged from 9 to 48. The baseline
characteristics of the patients in most of the studies were similar. All included studies
recruited subjects with the first time having stroke (Atay et al., 2008; Baricich et al.,
2013; Bayn et al., 2012; Blasis et al., 2009; Chen et al., 2013; Cho et al., 2012; Dohle
et al., 2009). The mean ages of the studies were between 54.2 and 67.2 years old. As a
result, adult patients were the priority type of recruitment. On the other hand, the sex
of the subjects varied from 45.8% male to 72.2% male. Although the sex was slightly
towards male, it was not significant and it showed that mirror therapy would be

16
suitable for both sex.
Mirror therapy could be applied to patients from sub-acute to chronic state. 6
studies focused on sub-acute patients (Atay et al., 2008; Baricich et al., 2013; Bayn et
al., 2012; Cho et al., 2012; Dohle et al., 2009) and one study focused on chronic
stroke patients (Chen et al., 2013). Baricich et al. (2013) recruited subjects in
sub-acute state with average 0.77 months after stroke whereas Chen et al. (2013)
recruited subjects with average 20.6 months after stroke. All of them showed
statistically significant results on upper limbs’ motor function of stroke patients.
However, the improvement of upper limb function in the chronic stage was less than
those in sub-acute stages. It was believed that mirror therapy had to start as earlier as
possible in order to achieve a better progress.
When talking about subjects’ level of severity, the higher the severity was, the
better the improvement was noted. According to Dohle et al. (2009), the study
recruited patients with severe hemiparesis. The improvement had around 6 times
when compared with baseline. Also, it was hard to have other treatment for severe
hemiparesis in real setting. Therefore, mirror therapy was suitable for paretic patients
especially with severe condition.
Two of the studies were conducted in Asian culture (Chen et al., 2013; Cho et al.,
2012) while the other six were in western culture (Altschuler et al., 1999; Atay et al.,

17
2008; Baricich et al., 2013; Bayn et al., 2012; Blasis et al., 2009; 2012; Dohle et al.,
2009). In both culture situations, results were statistically significant towards mirror
therapy group. Therefore, the intervention did not affected by culture issue and it was
generalizable to local setting.
Besides, following instruction was essential for the intervention. Therefore, most
of the studies mentioned the inclusion criteria about the cognitive function of the
subjects who could follow commands. Some of the studies involved the use of
Mini-Mental State Examination (MMSE) for excluding patients with poor cognitive
function (Atay et al., 2008; Baricich et al., 2013; Chen et al., 2013; Cho et al., 2012).
2.4.3 Intervention and Control
Six studies included the standard stroke rehabilitation program for the patients
(Atay et al., 2008; Baricich et al., 2013; Bayn et al., 2012; Blasis et al., 2009; Chen et
al., 2013; Dohle et al., 2009). It included the use of neurorehabilitation techniques like
electrical stimulation, occupational therapy, physiotherapy and speech therapy.
2.4.3.1 Consideration of Mirror
Simple equipment was needed for mirror therapy. From the reviewed studies, the
size of the mirror varied from the length 30cm to 120cm. The most important
consideration was whether the reflection of the non-paretic upper limb could be seen
by the patients themselves. Another issue was that it had to be easy to carry and could

18
be placed on the table with little support. A simple bed side table with lock could be
used to support the mirror which was placed perpendicular to the midline of the
patients.
2.4.3.2 Execution of Movement during Therapy
The non-paretic upper limb placed on the reflecting side. The movement of the
upper limb included flexion and extension of shoulder, elbow and wrist, supination
and pronation of forearm (Atay et al., 2008; Baricich et al., 2013; Blasis et al., 2009;
Chen et al., 2013; Cho, et al., 2012; Dohle et al., 2009). Other motion like squeezing
sponges, flipping card could also be used (Chen et al., 2013). Apart from the
non-paretic limb, bilateral movement, that was the movement of paretic upper limb as
best as possible together with non-paretic upper limb, was involved in two of the
studies (Chen et al., 2013; Dohle et al., 2009).
2.4.3.3 Therapy Intensity
All the selected studies used mirror therapy in the intervention group with total
treatment duration ranged from 10 (Atay et al., 2008; Bayn et al., 2012) to 20 hours
(Chen et al., 2013). The optimal duration of mirror therapy had to be at least 15 hours
in 4 weeks for the whole treatment. Those studies whose training duration of mirror
therapy equal to or more than 10 hours in 4 weeks had statistically significant results
on motor function improvement (Baricich et al., 2013; Blasis et al., 2009; Chen et al.,

19
2013; Cho et al., 2012; Dohle et al., 2009). One of the studies resulted insignificantly
in motor function improvement was possibly due to lack intensity with only 10 hours
in 5 weeks (Byan et al., 2012). Details could be referred to the table of comparison (II)
in Appendix (D).
2.4.3.4 Control Group
There were three types of control group. Sham therapy was the replace of mirror
with other materials or covered up which led to the surface without reflecting the
movement of the upper limb (Altschuler et al., 1999; Atay et al., 2008; Baricich et al.,
2013; Bayn et al., 2012; Blasis et al., 2009). The second type was that the mirror was
removed (Dohle et al., 2009) and the last type was not included any sham therapy but
the standard rehabilitation were extended with extra time which was the same as the
mirror group (Chen et al., 2013; Cho et al., 2012).
2.4.4 Data Collection
Most of the studies had pre- and post- treatment evaluation (Altschuler et al.,
1999; Atay et al., 2008; Baricich et al., 2013; Bayn et al., 2012; Chen et al., 2013; Cho
et al, 2012; Dohle et al., 2009). Four of the studies were conducted follow-up to
subjects ranged from 1 week to 24 weeks (Atay et al., 2008; Baricich et al., 2013;
Blasis et al., 2009; Chen et al., 2013). The significant result of mirror therapy group
still persisted in the follow-up measurement and this showed that the intervention had

20
long term effect.
2.4.5 Outcome Measurement
Among the selected studies, most of them used the mean differences of changes
between intervention and control group for comparison. They included the description
of effect size and p-value in their results (Atay et al., 2008; Baricich et al., 2013; Bayn
et al., 2012; Blasis et al., 2009; Chen et al., 2013; Cho, et al., 2012; Dohle et al., 2009).
Six studies mentioned about confidence interval or alpha level (Atay et al., 2008;
Baricich et al., 2013; Bayn et al., 2012; Blasis et al., 2009; Chen et al., 2013; Dohle et
al., 2009). Therefore, the results were precise and conclusion could be drawn from
their data. However, Altschuler et al. (1999) reported no information about p-value or
confidence interval. One of the reasons was that this study was the pilot study of using
mirror therapy on stroke patients. No data could be referred from the previous study.
As mentioned above that measurement of motor function for upper limb was the
inclusion criteria, all of the selected studies included these kind of measurements, for
example Fugl-Meyer Assessment, Action Research Arm Test (Atay et al., 2008;
Baricich et al., 2013; Bayn et al., 2012; Blasis et al., 2009; Chen et al., 2013; Cho, et
al., 2012; Dohle et al., 2009). Although they were introduced by different people, they
were the same type of assessment tools for motor function (Lyle, 1981; Fugl-Meyer et
al., 1975).

21
Activities of daily living measurement and the level of independence were
second most common outcome measurements (Atay et al., 2008; Baricich et al., 2013;
Bayn et al., 2012; Chen et al., 2013; Dohle et al., 2009). Since one of the important
points in rehabilitation was to help patient back to the society, their level of taking
care of themselves was an important issue. Therefore, most studies included this kind
of assessment.
Other measurements like spasticity, sensation, reaction time, neglect and pain
were used in the selected studies (Atay et al., 2008; Bayn et al., 2012; Blasis et al.,
2009; Chen et al., 2013; Dohle et al., 2009).
2.4.6 Results of the Studies
As the goal of this review was to find out the effectiveness of mirror therapy on
stroke patients, subjects among 6 of the studies had significant effect on improvement
of their motor function for upper limb when compared with the control group (Atay et
al., 2008; Baricich et al., 2013; Blasis et al., 2009; Chen et al., 2013; Cho, et al., 2012
& Dohle et al., 2009). Altschuler et al. (1999) also reported improvement of upper
limb function but using self-design rating scale without testing of validity and
reliability. Bayn et al. (2012) reported no significant difference on motor function
between intervention and control group due to the treatment intensity. Overall, mirror
therapy was beneficial to upper limb function of stroke survivors.

22
2.5 Implication
Mirror therapy in stroke rehabilitation was firstly introduced by Altschuler and
his colleague in 1999. The development is just having about fifteen years with slow
progress. As the mechanism involves our most complicated part “brain”, the studies
become far more difficult. Many areas remain only hypothesis and the recruitment of
subject’s characteristics are not specific enough. Further studies to the mechanism of
activation in brain area are needed with the use of imaging in stroke patients. Also,
vigorous studies are performed to find out a more precise target group of patients
which are the most beneficial from the therapy. Nevertheless, it is surprised that this
cheap, simple treatment can improve motor function of paretic upper limb. It is
possible to try in the clinical setting by nurses in order to know more about its effect
on stroke patients.
There was limitation for the studies in this integrative review. Since mirror
therapy required the participants to focus on the reflecting surface to get the virtual
image of the paretic limb. However, all of the studies did not measure on their
compliance during intervention. Further studies are needed to assess whether the
patient was focused to the task during intervention.
In conclusion, integrative review was done and seven papers were found with
acceptable quality. Evidence had showed that mirror therapy could improve the

23
recovery of stroke survivors’ upper limb motor function with long lasting effect. At
the same time, their activities of daily living were improved and, therefore, quality of
their lives. It could be used in adult patient without any restriction to sex. Optimum
intensity was needed to achieve the effect of improvement. Moreover, the training
needed to start as earlier as possible. Apart from movement of the limb alone, object
could be used during the procedure. The intervention could be applicable to local
setting and help stroke survivors during their rehabilitation process.

24
Chapter 3: Translation and Implementation
From the previous charter, the integrative review was proved that mirror therapy
was beneficial to the recovery of upper limb function in stroke patients. In order to
formulate the evidence-based practice guideline, the implementation potential of
mirror therapy will be examined according to the following aspects: proposed
audience and setting, transferability, feasibility and cost and benefit ratio.
3.1 Implementation Potential
3.1.1 Proposed Setting and Audience
The proposed local setting is the stroke rehabilitation wards in Hong Kong public
hospital and the target audience is the patients who are having stroke staying in the
wards. The rehabilitation wards include one male and one female ward which have 40
beds in each of the ward. About 50% of patients are diagnosed with stroke and they
need to undergo rehabilitation as another half are patients with other diagnosis. The
geriatric day hospital is the out-patient clinic for the follow-up session of the stroke
patients.
Before transferring to rehabilitation wards, stroke patients receive treatment in
acute medical setting. Then they transfer to rehabilitation wards when the condition is
stabilized. In rehabilitation phase in the proposed setting, patients are under
multidisciplinary care with doctor, nurse, physiotherapist, occupational therapist,

25
speech therapist, dietitian and social worker. A weekly conference is held to integrate
the information of patient’s progress between different disciplines. The average length
of stay in the rehabilitation unit is around 4 to 6 weeks which depends on the
condition and progress of the patients. Then follow-up is arranged for review in the
community. Some of them continue their treatment in geriatric day hospital or
out-patient clinic of physiotherapy and occupation therapy.
3.1.2 Transferability of the Findings
It is important to generalize and transfer the findings from the reviewed studies
to the proposed setting. The following session will be discussed about the
transferability of the findings.
3.1.2.1 Target Setting and Population
The proposed setting of rehabilitation wards is similar to the setting of the
reviewed studies with the purpose of providing institutional rehabilitation to stroke
patients before going back to the society. Both the proposed setting and the reviewed
studies include multidisciplinary care to the patients. They can provide similar
services and environment to stroke patients for rehabilitation. For example,
multidisciplinary team can be referred for rehabilitation needs. Furthermore, patient
characteristics are similar in terms of mean age and gender. They are mostly elderly
patients and include both sexes in the proposed setting.

26
On the other hand, the main difference of the target population is that they come
from different countries and culture. Two of the reviewed studies included Asian
population (Chen, 2013; Cho et al., 2012) which was similar to Hong Kong’s culture.
The others were from western countries (Atay et al., 2008; Baricich et al., 2013; Bayn
et al., 2012; Dohle et al., 2009). Although they may have cultural difference, the aim
of rehabilitation is the same. Also, as both cultures’ target population have positive
results towards mirror therapy, it is believed that culture difference may not affect the
application of the intervention and the intervention of the reviewed studies may fit the
target population.
3.1.2.2 Philosophy of Care
The philosophy of care for the reviewed studies is similar to the purposed
rehabilitation wards which its mission is to give holistic care to patients having stroke.
It aims at providing intensive rehabilitation and mobilizing patients as early as
possible so as to improve their quality of life by recovery of motor function. They can
be prepared to reintegrate to the community with independence. Besides, it
emphasizes multidisciplinary care which is the same as the proposed setting.
Therefore, the proposed setting matches the philosophy of care of the intervention.
3.1.2.3 Number of Patients Involved
Each of the wards contains 40 beds with approximately 50% of patients who are

27
diagnosed with stroke. The admission rate of stroke patients are around 30 patients
each month for both wards. When compared with the mean sample size in the
reviewed studies which is around 36 patients, it is less than the reviewed setting but
still there are sufficient numbers of patients who can be benefit from the proposed
intervention.
3.1.2.4 Duration for Implementation and Evaluation
As discussed in Chapter 2, in order to have statistically significant results, the
optimal duration of mirror therapy was about 4 weeks. It matches the average length
of stay 4 to 6 weeks in the proposed setting. After that, a 4 weeks follow-up session is
normally arranged for patient discharged from the proposed setting. Then further
follow-up session will be arranged at least for a year. Adequate follow-up provides
chances for evaluation of patients’ condition and motor function. It is the same as the
integrated review that follow-up is needed to assess mirror therapy’s long term effect.
3.1.3 Feasibility
This part is going to discuss the feasibility of carrying out a new intervention. It
is important to get consent from the colleague and to solve those practical problems.
3.1.3.1 Freedom of Implementation
Nurses have the freedom to carry out the intervention as they are the
nurse-in-charge for the patients accompanying patients most of the time. They can

28
provide treatment to patients for their best interest. They can also terminate the
intervention if it is inappropriate based on their professional judgment. Senior nurses
can provide supervision and advice to their staffs during implementing the
intervention. Weekly conference allows multidisciplinary discussion to evaluate the
progress of patients so as to determine the continuation of the proposed intervention.
3.1.3.2 Interference with Routine
Mirror therapy has minimal interference with the routine care. As mentioned in
the previous chapter, mirror therapy has an advantage of requiring less manpower for
supervision. The setup is also simple. Although, from the summarized results in
Chapter 2, it was recommended to have 15 hours in 4 weeks, which was 45 minutes in
each working day, was needed to have a therapeutic effect. Patients have around 2
hours free time in the afternoon every day which would be a suitable time to conduct
the intervention. As a result, the intervention may not have much interference with the
current staff functions.
3.1.3.3 Administration and Colleague Support
Administration approval and support is an important issue in hospital setting
when trying to carry out a new intervention. In the proposed setting, the
administration is positive towards evidence-based-practice’s intervention which
mirror therapy can be one of them. The organization has good attitude on new

29
intervention as regular “Kaizen” program is launched which allows colleague to share
and approve their new interventions. The administration supports the intervention by
allowing prior study in destined ward setting before carrying out to the other suitable
area.
However, as the shortage of manpower still persists in Hong Kong public
hospital, the new intervention may increase the workload of colleague in the proposed
ward setting. It is one of the potential barriers to the proposed intervention. Sufficient
explanation is needed to reinforce the needs and benefit of the intervention.
3.1.3.4 Skills and Training
Although nursing staffs and allied health colleagues have experience in carrying
out stroke rehabilitation, the proposed intervention is rather new to the field. The
skills include setting of the intervention, education to patients and the evaluation of
patient’s performance.
Therefore, before implementation of the intervention, briefing and training
session will be arranged for all frontline staffs to facilitate smoothness of the
intervention and to equip knowledge and skills for mirror therapy. Weekly evaluation
will be conducted to update the information and receive feedback from the frontline
staffs during implementation of the intervention.
For the training session, staffs need to spend extra time from working hours.

30
Compensation for extra working time can be given back to staff when available based
on the hospital policy. This can help to maintain the morale of the colleague in coping
new routine and extra workload.
3.1.3.5 Equipment and Facility
Since mirror therapy only needs a handy mirror, the cost is relatively low.
Bed-side tables and geriatric chairs are available with sufficient among in the
proposed setting. Patients can conduct the intervention along bedside during sit out
position and there is no need to transfer to other place.
Printer, paper and computer are needed in preparing training material and
assessment form. They are readily available in each proposed ward setting.
3.1.3.6 Measuring Tools for Evaluation
From the reviewed studies, the upper limb motor function is the evaluation
method for the patients under mirror therapy. Validated measuring tools, the Action
Research Arm Test and the Functional Independence Test, are available and the
occupational therapist in the proposed ward is professional in performing it. The skills
in performing the tool can be taught during skill training session with the help of
occupational therapist.
3.1.4 Cost and Benefit Ratio of Intervention
3.1.4.1 Potential Risk and Benefit of Patients

31
From the integrative review, there was no evidence showing any risk to the
patient during implementation of the mirror therapy. No adverse effect was noted
during the procedure (Altschuler et al., 1999; Atay et al., 2008; Baricich et al., 2013;
Bayn et al., 2012; Blasis et al., 2009; Chen et al., 2013; Cho et al., 2012; Dohle et al.,
2009).
When the proposed intervention is implemented, patients’ motor function is the
most significant benefit from it. According to the integrative review, their activities of
daily living increase and their quality of life improve (Atay et al., 2008; Baricich et al.,
2013; Blasis et al., 2009; Chen et al., 2013; Cho et al., 2012; Dohle et al., 2009). They
can have a shorter length of stay in the hospital. Better motor function also allows
them to reintegrate to the community easier than not having the intervention.
3.1.4.2 Potential Benefit of Staff and Hospital
From the view of administration, shorter length of hospitalization indicates better
use of public hospital facilities. The cost of caring each patient in the hospital can be
decreased and more money can be saved. Moreover, better reintegration of patient to
the community can lower the potential chance of re-admission. This can further lower
the burden of needs of the hospital facilities. In a long run, the quality of care
provided by the health care profession can be increased because they can have more
time to care the patients.

32
3.1.4.3 Potential Material Costs
The material costs are mostly come from the manpower, the mirror and the
training material. The table in Appendix (E) showed that the estimated sum of cost are
$55 220.
The amount for caring 40 patients in 4 weeks looks like a huge amount of money.
However, when comparing the Table of Material Cost on not implementing the Mirror
Therapy in Appendix (E), it is around 30% less cost when using the proposed
intervention. Thus, implementation of mirror therapy can probably lower the material
cost by shortening the length of hospitalization.
3.1.4.4 Potential Non-material Costs
In a short run, staffs morale may be affected due to increase workload on
carrying out the intervention. If the length of hospitalization and the re-admission rate
reduce, the workload will be deducted and the working environment will be improved.
The morale will be increased in long term.
On patients’ aspect, they can have a higher satisfaction when the intervention
helps them in recovery of motor function. They can have a better quality of life after
discharge.
In conclusion, after discussing the implementation potential of the intervention, it
should be carried out with slightly changes needed so that the intervention can be

33
carried out in the local setting.

34
Chapter 4: Developing an Evidence-based Practice
Guideline
As discussed the implementation potential in the last chapter, an evidence-based
practice guideline will be developed. Based on the reviewed studies, purpose,
objectives, target audience and recommendations will be generated and listed in this
chapter.
4.1 Title of the Evidence-based Guideline
An Evidence-based Guideline of Using Mirror Therapy to Promote Motor Function
Recovery of Upper Limb in Stroke Patient
4.2 Background
Stroke is the major cause of disability in Hong Kong. Nearly 25 000 people
suffered from stroke in 2010 (the Hospital Authority Statistical Report, 2011). Half of
them had the problem of hemiparesis (Beiser et al., as cited in American Heart
Association, 2011). It is important to help the stroke survivors to cope with this
disease before facing the community.
This guideline was based on the integrative review of eight studies which
discussed the effectiveness of mirror therapy on hemiparesis of upper limb in stroke
patients (Altschuler et al., 1999; Atay et al., 2008; Baricich et al., 2013; Bayn et al.,
2012; Blasis et al., 2009; Chen et al., 2013; Cho et al., 2012; Dohle et al., 2009).

35
4.3 Purpose and Objectives of Guideline
The main purpose of this guideline is to help nurses in using mirror therapy on
hemiparetic stroke patients. It aims at promoting the recovery of upper limb motor
function of stroke survivors.
The objectives of the Guideline are:
To summarize the clinical evidence for mirror therapy on hemiparetic stroke
patients;
To formulate clinical practice instructions for the use of mirror therapy based on
the best evidence;
To improve the recovery of motor function on paretic upper limb;
To maximize the usage of time for the health care profession and, at the same time,
provide sufficient training to the patients;
To shorten the length of stay of patients and reduce the re-admission rate.
4.4 Target Group
4.4.1 Target Audience
This guideline is for nurses who attend to stroke patient with the right to assess
and carry out intervention to help them from the disease.
4.4.2 Target Population
The guideline applies to stroke patients in stroke rehabilitation wards aged 18

36
years or above who has the problem of hemiparesis on upper limb with understanding
of simple instruction.
4.5 Level of Evidence and Grades of Recommendations
The recommendations were made based on the level of evidence and grades of
recommendations produced by SIGN (Scottish Intercollegiate Guidelines Network,
2011). The table of the level of evidence and grades of recommendations could be
found in Appendix (G).
4.6 Recommendations
Here were the recommendations of the guideline. The details were presented in
Appendix (F).
Recommendation 1: Mirror therapy is proved to be effective on improving recovery of
upper limb motor function in stroke patients.
(Grades of Recommendation: A)
Recommendation 2: Mirror therapy should be used in stroke patient aged above 18
years old with first time having stroke. Also, it can be applied to both sexes.
(Grades of Recommendation: A)
Recommendation 3: Mirror therapy should be applied to stroke patients from
sub-acute to chronic state.
(Grades of Recommendation: A)

37
Recommendation 4: Patients should be able to understand and follow verbal
instructions.
(Grades of Recommendation: A)
Recommendation 5: Sitting position with a mirror sized enough for patient to see his
entire upper limb is needed for the use of mirror therapy on training of upper limb in
stroke patients. The non-paretic upper limb is placed on the reflecting side. Patients
observe the motion of the non-paretic side in the mirror as if the motion of the paretic
side.
(Grades of Recommendation: A)
Recommendation 6: The movement of the upper limb includes flexion and extension
of shoulder, elbow, wrist and finger, pronation and supination of forearm, moving arm
from side to side. Objects can be involved in the motion like squeezing sponges,
placing object in holes, flipping card.
(Grades of Recommendation: A)
Recommendation 7: Bilateral movement, which is the movement of paretic upper limb
together with non-paretic upper limb, should be involved.
(Grades of Recommendation: A)
Recommendation 8: Conventional stroke rehabilitation program, for example
occupational therapy and physiotherapy, should be included apart from mirror

38
therapy.
(Grades of Recommendation: A)
Recommendation 9: Patients should be in priority when the severity of patient’s
paretic upper limb was higher.
(Grades of Recommendation: A)
Recommendation 10: Mirror therapy should be applied equal to or more than 10 hours
in 4 weeks.
(Grades of Recommendation: A)
Recommendation 11: Assessment and evaluation should be done prior and after the
application of mirror therapy:
Measuring tool the Action Research Arm Test is recommended to use to evaluate
the progress of the upper limb motor function.
Measuring tool the Functional Independence Test should be used to assess the
independence of patients.
(Grades of Recommendation: A)
Recommendation 12: Follow-up session should be arranged to evaluate patient’s
progress of the paretic upper limb function. It is recommended to follow the progress
at least for half year.
(Grades of Recommendation: A)

39
Chapter 5: Implementation Plan
After formulating the evidence-based guideline, in this chapter the
communication plan and the pilot test will be discussed to ensure the smoothness and
success of the intervention. To set up a good communication plan, identification of the
stakeholders will be the first step. Communication plan will be developed between
each party of stakeholders so that the program can be maintained in the proposed
setting. Then, the implementation process will be evaluated by pilot test. At last, the
mirror therapy can be delivered smoothly and the frontline staff can provide good
services to the patient with better cooperation.
5.1 Stakeholders Identification
Stakeholder is the one who may involve in the innovation of the mirror therapy.
Identification of stakeholder is important as cooperation and support is essential on
carrying out the intervention. The Chief of Service, the Department Operations
Manager, the Ward Managers, ward and day hospital nurses, allied healthcare workers
and the healthcare assistance are the main stakeholders of the intervention.
5.1.1 Administrators
Administrators are responsible for the usage of limited resource in the
department. The Chief of Service, the Department Operations Manager, the Ward
Managers of the stroke rehabilitation wards and geriatric day hospital are the

40
administrators of this intervention. They make decision to approve any program in the
department of rehabilitation. Seeking for their approval and support is needed before
implementation.
5.1.2 Trainers
The core team members of the implementation team are responsible for the
leading of mirror therapy program based on the guideline. The team is the trainer of
the mirror therapy program. The occupational therapist also provides support to the
team for educating the intervention providers based on the guideline.
5.1.3 Users of the Evidenced-based Guideline
The implementation team, ward nurses and the healthcare assistance are the users
of the guideline. They maintain the operation of the intervention. Apart from the ward
frontline staffs, the colleagues in the day hospital are the users of the guideline who
carry out the intervention during patient’s follow-up.
5.2 Communication Plan
5.2.1 Setting up a Team
Good communication is very important. At the beginning, setting up of the
implementation team is needed to initialize the intervention. The proposer will be the
coordinator of the team. Three advanced practiced nurses, three registered nurses and
one occupational therapist will be involved as the core team members.

41
The advanced practice nurses are experienced so that they can give advice inside
the implementation team. Further research can be made if needed in order to get the
best evidence. Moreover, the registered nurses can act as a link between proposer and
the frontline staffs of wards and day hospital in order to ensure the coordination of the
intervention. The occupational therapist is responsible for providing information on
mirror therapy and the assessment skills.
5.2.2 Communicating with Administrators
Getting approval is an important issue of the implementation team since the
administrators control the usage of limited resources like equipment, manpower or
expenditure. It is a must to get approval from them. Individual meeting will be
conducted to set up communication with the Ward Managers, the Department
Operations Manager and at last the Chief of Service of the rehabilitation department.
Firstly, the team will approach ward managers to get their support. Then, in order to
promote this idea to the Department Operations Manager and Chief of Service for
granting permission, presentation will be held with the use of demonstration and
visual aids. The content will include the background, objective, significance of the
program, reviewed evidence, implementation potential and the developed guideline
with literature support. Feedback will be obtained from the administrative view during
the meeting.

42
5.2.3 Briefing Session
After getting approval, briefing session will be conducted to the stakeholders.
Healthcare providers in the target setting may join the session to know more about the
intervention and share their opinions. It, therefore, can help the implementation team
to explore different point of views. At the same time, doubt can be solved to convince
those oppose the intervention. After the session, questions and opinions will be
investigated and changes can be made to improve the intervention so as to meet the
target setting.
5.2.4 Training Session
As mirror therapy needs to be learnt before application, a training session will be
held for the nurses involved. Procedure of the application and assessment skills will
be taught by the implementation team based on the evidence-based guideline.
Materials, the mirror, will be available for demonstration and practice. Printed notes
and guideline will be provided for refreshing memory. Feedback and difficulty of
using mirror therapy can be obtained during practice. Further clarification can be
instantly made during training.
5.2.5 Initiating, Guiding and Sustaining the Intervention
The implementation team will have the duty of designing the time schedule of
the intervention and its evaluation. They will also monitor the program regularly to

43
maintain the progress of the intervention. Difficulties will be reviewed during the
regularly meeting in order to update the guideline and remove any obstacles. The
process and the result will be reported to the administrators to get continuation of the
program. Appendix (H) shows the time frame of the mirror therapy program.
5.3 Pilot Test
Pilot test aims at testing the feasibility of the intervention and, as a result,
improving it (Beck & Polit, 2008). During the study, the intervention will be carried
out in a small scale with similar workflow. The intervention will be tested to see if it
contains any problem in each procedure. Evaluation of information taken provides an
opportunity to reveal and modify the limitation of the proposed intervention.
5.3.1 Aims and Objectives of Pilot Test
The main objectives of the pilot test are:
To assess the feasibility of implementing the intervention.
To determine any difficulty of subject recruitment;
To examine the evidence-based guideline in local setting;
To examine the acceptance of staffs;
5.3.2 Recruitment and Duration
The target setting will be the stroke rehabilitation units including one male and
one female ward. The follow-up session will be held in the clinic of geriatric day

44
hospital. The target recruitment will be 5 patients in each ward (10 in totals). Each
subject will receive mirror therapy in weekdays (5 patients x 5 days x 4 weeks = 100
sessions). Each nurse will have sufficient chance to practice the intervention with
accounting for the possibility of subject withdrawal. As mentioned in Chapter 3 that
the admission rate is around 30 patients every month, 2 weeks will be needed to
recruit sufficient among of subjects.
Furthermore, in Chapter 2 summarized that the optimal duration of mirror
therapy is about 4 weeks. Assessment will be done before and after intervention for
the two wards’ nurses to practice their skills. After that, follow-up session will be
carried out 2 weeks after discharge of subjects so that the workflow of doing
follow-up assessment can be tested. The nurses in day hospital will have the chance of
practicing assessment for the subjects. All in all, 4 months will be needed to carry out
the pilot test. Detail can be found in Appendix (H).
5.3.3 Evaluation of Pilot Test
Based on the objectives, the following methods are used to evaluate the results of
the pilot test.
5.3.3.1 Feasibility of Implementing Mirror Therapy
The link nurses in the team can receive feedbacks from frontline staffs in wards
and geriatric day hospital. Regular meeting between implementation team will be held

45
to discuss the progress of the pilot test. At the end, the difficulties collected will be
summarized and evaluated to update the guideline.
5.3.3.2 The difficulty of Subject Recruitment
Individual interview will be conducted to patients who withdraw from the study.
The interview will be focused on the reason behind the withdrawal and the problem of
the workflow.
5.3.3.3 The Evidence-based Guideline in Local Setting
The nurses have to record the time of each session provided to patients. This can
provide the information whether the intervention can be provided in busy local setting
based on the guideline. Reason of not completing the session can also be noted so that
the guideline can be modified to suit the local setting.
5.3.3.4 The Acceptance of Staffs
A simple questionnaire (Appendix (I)) will be used to the frontline staffs for
examining their acceptance of the intervention. It will be delivered to the staffs after
the last session of mirror therapy. It will mainly focus on their opinions about the
intervention with their usual practice and their suggestions on conducting the whole
program.

46
Chapter 6: Evaluation Plan
Evaluation plan is needed to assess the effectiveness of the mirror therapy to the
local clinical setting. The aim of the mirror therapy is to promote the recovery of
motor function of upper limb on hemiparetic stroke patients. Thus, the outcome of the
mirror therapy is the upper limb motor function and the level of activities of daily
living. The satisfaction level is assessed for patients and healthcare provider.
6.1 Identifying Outcomes
6.1.1 Patient Outcomes
6.1.1.1 Primary Measurement
The measuring tool, the Action Research Arm Test, will be the primary outcome
measurement of mirror therapy to assess the recovery of upper limb motor function of
the patients (Baricich et al., 2013; Bayn et al., 2012; Dohle et al., 2009). It was highly
specific to assess the changes in upper limb function and it was used for evaluation of
clinical treatment (Lyle, 1981). In the test, Score ranged from 0 to 57 is recorded. 4
sub-scales, including grasp, grip, pinch and gross movement, are involved to assess
the function of the upper limb.
6.1.1.2 Secondary Measurement
For the secondary outcome measurement, the Functional Independence Measure
will be used to assess the self-caring ability (Baldry et al., 1995). The motor part will

47
be chosen as the motor function will be the focus of the studies with total score ranged
from 13 to 91. Eating, Bathing, toileting, dressing, grooming, bowel and bladder
control, transfer and mobility are involved in the measurement. It was widely used
assessment tools in the local setting for assessing stroke patient (Cheng et al., 2010)
and was also used in the reviewed studies (Atay et al., 2008; Baricich et al., 2013;
Dohle et al., 2009).
6.1.1.3 Level of Satisfaction (Patient)
A descriptive patient satisfaction survey will be used to assess the satisfaction of
patient on mirror therapy. Statements will be ranked by the patients from “very
unsatisfied” to “extremely satisfied”. Then Score represents each level and the sum of
the score can be calculated. The higher the score, the better the satisfaction level will
be. Appendix (J) shows the sample of the patient satisfaction survey.
6.1.2 Healthcare Providers Outcomes
The Outcome of the healthcare providers will be to measure their level of
satisfaction on this program.
6.1.2.1 Level of Satisfaction (Staff)
A staff satisfaction survey will be delivered to the healthcare providers to assess
their satisfaction level on the program. Score of 1 to 5 will be recorded in each
question. The higher the score means that the satisfaction level is higher. The

48
questions in the survey will focus on the information provided, workload, cooperation
between colleague and their knowledge on mirror therapy. Detail can be found in
Appendix (K).
6.1.3 System Outcomes
The patient’s length of hospitalization will be the system outcome measure in the
evaluation plan.
6.1.3.1 Length of Hospitalization
It refers to the number of days that the patients stay in the hospital. It starts from
the day of admission to the discharge day. This number can reflect the effectiveness of
the mirror therapy by showing whether this program can shorten the patients’ length
of hospital stay.
6.2 Nature of Subjects
Subjects will be included in the study when they are diagnosed with first time
having stroke with hemiparesis, adult with aged over 18 and they can follow
commands. Moreover, they have to be the patients admitted to the stroke
rehabilitation department.
6.3 Number of Subjects
In order to calculate the change of motor function before and after the
intervention with the use of measuring tools Action Research Arm Test, paired t-test is

49
used with the power of 0.8 and alpha 5%. The effect size is 0.6. As a result, 24
subjects are needed to be recruited. However, the dropout rate from the reviewed
studies is between 0% and 21% (Baricich et al., 2013; Chen et al., 2013). Since
follow-up will be needed for the studies, the possibility of dropping out of studies has
to be considered. When calculating the worst situation that 21% of subjects will be
dropped out of the studies, at least 31 subjects will be required to ensure a sufficient
number of subjects for the studies. Below is the calculation:
Required sample size: 24+7= 31 subjects
Dropout subjects: 31 x 21% = 6.51, ~7 subjects
6.4 Data Collection
For the patient outcomes, as discussed in the evidence-based guideline that the
measurement should be done before and after the intervention. Subjects will receive
baseline assessment for upper limb motor function and independence measure before
application of mirror therapy. Demographics details of patients will also be collected
at the same time. After 4 weeks mirror therapy treatment, post assessment will be
given to subjects before discharged to the community.
From the reviewed studies, 4 and 24 weeks are recommended to assess the
recovery of motor function after mirror therapy (Atay et al., 2008; Baricich et al.,
2013; Chen et al., 2013) Therefore, the motor function and independence

50
measurements will be assessed in the geriatric day hospital at 4 and 24 weeks after
discharge.
For the level of satisfaction of patients and healthcare providers, the satisfaction
survey will be delivered to them before and after the implementation. On the other
hand, the length of hospitalization will be collected after each discharge of the
patients.
6.5 Data Analysis
To compare the progress of patients before and after mirror therapy on the upper
limb motor function and the level of independence, paired t-test will be used to
compare the difference at baseline, week 4 and week 24.
For the satisfaction level of patients and healthcare providers, paired t-test will
be used to compare the difference of mean score before and after implementation of
mirror therapy.
For the patients’ length of hospitalization, paired t-test will also be used to
compare between the average length of stay and the length of stay in the hospital
database.
This quantitative data will be analyzed using the Statistical Package for the
Social Science (SPSS) for Windows.

51
6.6 Basis Criteria of Effective Guideline
The evaluation objectives is to determine whether there is significant
improvement in patient’s upper limb motor function, level of independence for
patients, level of satisfaction for patients and staffs and the length of hospitalization of
patients.
6.6.1 Upper Limb Motor Function of Patients
With the use of measuring tools Action Research Arm Test, mirror therapy will
be an effective treatment if there is significant improvement of upper limb motor
function on paretic side in the follow-up sessions when compared with the baseline
assessment.
In the reviewed studies, the significant improvement ranges from 12% to 585%
with different severity of impairment (Detail can be referred to Appendix (D)).
Therefore, the target improvement is more than 12% on the recovery of upper limb
motor function on paretic side.
6.6.2 Level of Independence of Patients
The secondary outcome is the improvement of level of independence of patients
based on the Functional Independence Measure. There were significant improvements
between 35% and 79% in the reviewed studies (Atay et al., 2008; Baricich et al., 2013;
Dohle et al., 2009). As a result, it is said to be effective when the level of

52
independence increases with at least 35% when compared with the baseline
assessment.
6.6.3 Level of Satisfaction of Patients
For the satisfaction level of patients, it is said to be an effective outcome if the
mean score before intervention is higher than the score after intervention.
6.6.4 Level of Satisfaction of Staffs
The healthcare providers outcomes is the increase of level of satisfaction based
on the self-designed satisfaction questionnaire. It is said to be effective if the mean
score after the implementation is higher than baseline.
6.6.5 Length of Hospitalization
The hospital can lower the material cost by shortening the length of stay of the
patients. It is said to be effective if it helps the patients to stay shorter in the hospital.

53
Chapter 7: Conclusion
From the eight reviewed studies, the results provide information to develop the
evidence-based guideline of mirror therapy for patients suffered from stroke with
hemiparesis. It is proved that mirror therapy program benefited upper limb motor
function recovery in stroke patients in acute to chronic phase.
By assessing the implementation potential, the proposed intervention can be
modified to fit the proposed setting. It is possible to incorporate into the usual practice
so that the stroke patients can receive a better rehabilitation progress. Pilot test
provides a chance to run the program in order to review and modify the intervention
by removing the obstacles. After that, implementation plan is used to improve
communication between different parties during conduction of intervention.
Evaluation plan is required to review the effectiveness of the intervention.
Based on the evidence-based guideline, it is believed that the healthcare
providers can cooperate effectively to provide mirror therapy to the patients and this
program can help the patients to cope with the disease of stroke. It can become one
part of the stroke rehabilitation program. However, further research is needed on
program’s application time, content and target population’s characteristics.

54
Appendix (A): Flow Chart of the Search Strategy
Stroke/ Post stroke/ Stroke
rehabilitation/ CVA/ CVA
rehabilitation/ Post CVA/
Cerebrovascular accident/
cerebrovascular disease
Mirror therapy/ Mirror therapy
and stroke/ Mirror therapy
rehabilitation/ Mirror therapy
hand
PubMed ProQuest
7/7/2013 9/7/2013
204 40
Topic screened
and abstract
read
Number of
selected articles 8 4
Selected articles
without
duplication
Search date
Database
Search
item
Article reviewed
from reference
list
Final Selection
8
0
8
Search Result
1 2
365825 7423 484257 6321 1 or 2
1 and 2 289 300

55
Appendix (B): Quality Assessments of the Articles [SIGN form (2012)]
Article
Statement
Baricich et al.
(2013)
Chen et al.
(2013)
Bayn et al.
(2012)
Cho et al.
(2012)
Blasis et al.
(2009)
Dohle et al.
(2009)
Atay et al.
(2008)
Altschuler et al.
(1999)
Section 1: Interval Validity
1.1 The study
addresses an
appropriate and
clearly focused
question
Yes Yes Yes Yes Yes Yes Yes Yes
1.2 The assignment
of subjects to
treatment groups is
randomized
Yes
(Randomization
scheme
generated by
software)
Yes
(Randomly
extracted
envelopes)
Yes
(Computer-gen
erated random
number
sequence)
Yes
(Random
allocation
software)
Can’t say
(Not mention
the method)
Yes
(Envelopes
with
randomization
sequence)
Yes
(Computer-gen
erated random
number list
with blocks)
Can’t say
(Not mention
the method)
1.3 An adequate
concealment
method is used
Can’t say Yes
(Sealed
envelopes)
Can’t say Can’t say Can’t say Yes
(Sealed
envelopes)
Yes
(Blinded doctor
for
randomization)
Can’t say
1.4 Subjects and
investigators are
Yes, assessor
blinded
Yes, assessor
blinded
No Can’t say Yes, assessor
blinded
Yes. Assessor
blinded
Yes. Assessor
blinded
Yes, assessor
blinded

56
Article
Statement
Baricich et al.
(2013)
Chen et al.
(2013)
Bayn et al.
(2012)
Cho et al.
(2012)
Blasis et al.
(2009)
Dohle et al.
(2009)
Atay et al.
(2008)
Altschuler et al.
(1999)
kept ‘blind’ about
treatment allocation
1.5 The treatment
and control groups
are similar at the
start of the trial
Yes Yes Yes Yes Yes Yes Yes No
(1 subject’s
time since
stroke was
different from
the others)
1.6 The only
difference between
groups is the
treatment under
investigation
Yes Yes Yes Yes Yes Yes Yes Yes
1.7 All relevant
outcomes are
measured in a
standard, valid and
reliable way
Yes Yes Yes Yes Yes Yes Yes Yes
1.8 What
percentage of the
I: 13/13: 0%
C:12/13: 3.8%
I: 11/16: 15%
(5 lost
I(1): 15/18: 5%
(3 discharged)
I: 13/14: 3.6%
(1 low
I: 22/24: 4.2%
(1 moved to
I: 6/18: 16.7%
(1 transferred
I: 17/20: 7.5%
(3 lost
I: 9/9: 0%
C: 9/9: 0%

57
Article
Statement
Baricich et al.
(2013)
Chen et al.
(2013)
Bayn et al.
(2012)
Cho et al.
(2012)
Blasis et al.
(2009)
Dohle et al.
(2009)
Atay et al.
(2008)
Altschuler et al.
(1999)
individuals or
clusters recruited
into each treatment
arm of the study
dropped out before
the study was
completed?
*Intervention group
=I
Control group =C
**follow-up/begin:
dropout rate
(1 new stroke
episode)
follow-up)
C: 10/17: 21%
(7 lost
follow-up)
I(2): 16/21:
8.3%
(2 discharged, 2
withdrawal, 1
died)
C: 18/21 =5%
(2 discharged, 1
withdrawal)
participation
rate)
C: 13/14: 3.6%
(1 low
participation
rate)
other city, 1
used other
treatment)
C: 17/24:
14.6%
(3 used other
treatment, 4
withdrawal)
out, 4 due to
insurance, 1
withdrawal)
C: 12/18:
16.7%
(2 transfer out,
1 deterioration,
1 due to
insurance, 2
withdrawal)
follow-up)
C: 19/20: 2.5%
(1 lost
follow-up)
(Planned
cross-over with
9 subjects)
1.9 All the subjects
are analyzed in the
groups to which
they were randomly
allocated (often
referred to as
intention to treat
analysis)
No No Yes No Yes No No No

58
Article
Statement
Baricich et al.
(2013)
Chen et al.
(2013)
Bayn et al.
(2012)
Cho et al.
(2012)
Blasis et al.
(2009)
Dohle et al.
(2009)
Atay et al.
(2008)
Altschuler et al.
(1999)
1.10 Where the
study is carried out
at more than one
site, results are
comparable for all
sites
Not applicable Can’t say
(No site
specific data
available)
Not applicable Not applicable Can’t say
(No site
specific data
available)
Not applicable Not applicable Not applicable
Section 2: Overall Assessment of the Study
2.1 How well was
the study done to
minimize bias?
- High quality (++)
- Acceptable (+)
- Low quality (0)
+ + + + + + + 0
2.2 Taking into
account clinical
considerations, your
evaluations of the
methodology used,
and the statistical
power of the study,
-Performance
bias was
present as
blinding of
subject was not
available
-Selection bias
-Performance
bias was
present as
blinding of
subject was not
available
-Overall effect
-Performance
bias was
present as
blinding of
subject was not
available
-Detection bias
-Performance
bias was
present as
blinding of
subject was not
available
-Detection bias
-Performance
bias was
present as
blinding of
subject was not
available
-Selection bias
-Performance
bias was
present as
blinding of
subject was not
available
-Overall effect
-Performance
bias was
present as
blinding of
subject was not
available
-Overall effect
-Performance
bias was
present as
blinding of
subject was not
available
-Selection bias

59
Article
Statement
Baricich et al.
(2013)
Chen et al.
(2013)
Bayn et al.
(2012)
Cho et al.
(2012)
Blasis et al.
(2009)
Dohle et al.
(2009)
Atay et al.
(2008)
Altschuler et al.
(1999)
are you certain that
the overall effect is
due to the study
intervention?
may be present
as unclear about
concealment
-Overall effect
was due to the
intervention
although mild
potential bias
was present
was due to the
intervention
although mild
potential bias
was present
was present as
no blinding was
noted
-Selection bias
may be present
as unclear about
concealment
-Overall effect
was due to the
intervention
although mild
potential bias
was present
may be present
as blinding of
assessor was
unclear
-Selection bias
may be present
as unclear about
concealment
-Overall effect
was due to the
intervention
although mild
potential bias
was present
may be present
as unclear about
concealment
-Overall effect
was due to the
intervention
although mild
potential bias
was present
was due to the
intervention
although mild
potential bias
was present
was due to the
intervention
although mild
potential bias
was present
was present as
unclear about
randomization
and
concealment
- Carry over
effect due to
crossover
method, no
wash out period
was mentioned
- Sample size
was small
-Overall effect
was highly
affected by the
potential bias
2.3 Are the results
of this study
directly applicable
Yes Yes Yes Yes Yes Yes Yes No

60
Article
Statement
Baricich et al.
(2013)
Chen et al.
(2013)
Bayn et al.
(2012)
Cho et al.
(2012)
Blasis et al.
(2009)
Dohle et al.
(2009)
Atay et al.
(2008)
Altschuler et al.
(1999)
to the patient group
targeted by this
guideline?
2.4 Notes:
Summaries the
authors’
conclusions. Add
any comments on
your own
assessment of the
study, and the
extent to which it
answers your
question and
mention any areas
of uncertainty
raised above.
The mirror
group had more
improvement in
upper limb
motor recovery
than control
group.
The mirror
group had more
improvement in
upper limb
motor recovery
than control
group but there
was no
difference on
ADL
performance.
There was no
significant
difference
between mirror
or control group
The mirror
group had more
improvement in
upper limb
motor recovery
than control
group
The mirror
group had more
improvement in
reducing pain
and enhancing
upper limb
motor function
than control
group
The mirror
group had more
improvement in
distal function
than control
group.
The mirror
group had more
improvement in
motor recovery
and
hand-related
functioning
than control
group. There
was no effect
on spasticity
The mirror
group had more
improvement in
motor recovery
of upper limb
than control
group but
majority of
potential bias
was present
which may
affect the result
Abbreviation: ADL =Activities of Daily Living

61
Appendix (C): Table of Evidence
Remarks:
*Sham therapy: Placebo treatment
**Bilateral movement: Apart from moving the non-paretic upper limb, moving of paretic upper limb as best as possible is also encouraged
***Effect size: The values of the results were the difference of mean score between the follow-up and baseline assessment. E.g. mean difference
(group) [p value]
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome measure Results and effect size***
Baricich et
al.
(2013)
RCTs 1+ - n =26
- Mean age
=66.6
- Male sex
=50%
- Mean time
since stroke
=0.77months
- First stroke
- ARAT at
baseline
=18.45/57
MT (n=13):
Detail
- Flexion /extension of
shoulder , elbow, wrist
- Pronation /supination
of forearm
Duration
- 30 min /day, 5 times
/week (first 2 weeks), 1
hour /day, 5 times /week
(last 2 weeks)
- Total time =15 hours
CT (n=13):
Detail
- Reflecting
part of the
mirror was
covered with
paper
Duration
- Same as MT
- Baseline
- 4 weeks
follow-up
Primary
1. ARAT
Secondary
2. MI
3. FIM
After 4 weeks,
-MT had greater improvement in
upper limb function than CT
1. 31.74 (MT) vs 12.67 (CT)
[p<0.05]
2. 36.73 (MT) vs 14.75 (CT)
[p<0.05]
-MT had greater improvement in
independence than CT
3. 41.18 (MT) vs 21.75 (CT)
[p<0.05]

62
(32.4%)
Remarks:
Assessor was blinded. Subject could not be blinded due to the intervention.
Abbreviation: CT = Control therapy, MT = Mirror therapy, ARAT = Action Research Arm Test, MI = Motricity Index of upper limb, FIM = Functional Independence
Measure

63
Bibliographi
c Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome
measure
Results and effect size***
Chen et al.
(2013)
RCTs 1+ - n =33
- Mean age
=54.2
- Male sex
=70%
- Mean time
since stroke
=20.6months
- Mean MMSE
=28.5
- FMA at
baseline =45.2
(68.5%)
MT (n=16):
Detail
- Squeezing sponges
/placing pegs in holes
/flipping card /touch
a switch or keyboard
- Flexion /extension
of wrist, finger
- Pronation
/supination of
forearm
- Bilateral
movement**
Duration
- 60 min /day, 5 days
/week, for 4 weeks
- Total time =20
hours
CT (n=17):
Detail
- Task-oriented
functional
practice for
motor control
training
- No sham
therapy*
Duration
- same as MT
- Baseline
- Post
treatment
- 24 weeks
follow-up
Primary
1. FMA
2. Kinematic
analysis
Secondary
3. rNSA
4. MAL
(Amount of
use)
5. MAL
(Quality of
movement)
6. ABILHAN
D
Post-treatment,
-MT had greater improvement in
upper limb function than CT
1. 5.31 (MT) vs 3.47(CT)
[p<0.05]
-MT had shorter reaction time
than CT
2. -0.06 (MT) vs 0.01 (CT)
[p<0.05]
-MT improved insignificantly in
sensation than CT
3. 12.63 (MT) vs 1.5 (CT)
[p=0.1]
On 24 weeks follow-up,
-No significant improvement of
ADL in MT was noted
4. 0.61 (MT) vs 0.44 (CT)
[p=0.45]
5. 0.77 (MT) vs 0.56 (CT)
[p=0.45]

64
6. 7.86 (MT) vs 9.06 (CT)
[p=0.43]
Remarks:
Assessor was blinded. Subject could not be blinded due to the intervention.
Multi-site studies: No site specific data was available.
Abbreviation: CT = conventional therapy, MT = mirror therapy, FMA =Fugl-Meyer Assessment, rNSA =Revised Nottingham Sensory Assessment, MAL = Motor Activity
Log, ADL =Activities of Daily Living

65
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome
measure
Results and effect size***
Bayn et al.
(2012)
RCTs 1+ - n =60
- Mean age
=67.2
- Male sex
=58%
- Mean time
since stroke
=1.5months
- First stroke
- ARAT at
baseline
=0.69/57
(1.2%)
- FMA at
baseline =4.1
(6.2%)
iMT (n=18):
Detail
- First week:
isolated
movements of
fingers, wrist,
lower arm, elbow
and shoulder joints
- Second & third
week: putting a ball
or bigger squares in
different directions
/moving sticks
/wipe-like
movements with a
cloth.
- Bilateral
movement**
Duration
- 30 min /day, 20
CT (n=21):
Detail
- same as
gMT but
wooden
board was
used
Duration
- Same as
gMT
gMT
(n=21):
Detail
- same as
iMT but
group of 2-6
patients was
used
Duration
- Baseline
- Post
treatment
Primary
1. ARAT
2. FMA
(Motor)
Secondary
3. BI
4. SIS
5. FMA
(arm
somatos
ensory)
6. FMA
(Range
of
motion)
7. FMA
(Pain)
8. MAS
(Finger)
Post-treatment,
-MT showed no effect on motor function of
upper limb, ADL & QoL
1. 3.4 (iMT), 1.1 (gMT) vs 2.8 (CT)
[p>0.05]
2. 3.2 (iMT), 5.1 (gMT) vs 5.2 (CT),
[p>0.05]
-No significant improvement of ADL, QoL in
MT was noted
3. 11.9 (iMT), 12.5 (gMT) vs 15.0 (CT),
[p>0.05]
4. 9.5 (iMT), 8.2 (gMT) vs 7.3 (CT),
[p>0.05]
-No significant improvement of upper limb
sensory, ROM and pain in MT was noted
5. 0.7 (iMT), 0.9 (gMT) vs 0.3 (CT),
[p>0.05]
6. -0.9 (iMT), -1.6 (gMT) vs -2.2 (CT),
[p>0.05]
7. -1.3 (iMT), -1.8 (gMT) vs -2.3 (CT),

66
sessions in 5 weeks
-Total time =10
hours
- Same as
iMT
9. MAS
(Wrist)
10. SCT
[p>0.05]
-No significant improvement of resistance in
movement for finger and wrist in MT was
noted
8. 1 (iMT), 0 (gMT) vs 0 (CT), [p<0.05]
9. 0 (iMT), 0 (gMT) vs 0 (CT), [p>0.05]
-MT had improvement on visuospatial neglect
10. 20 (iMT), 4.4 (gMT) vs -2.3 (CT),
[p<0.01]
Remarks:
Insignificant results may due to the duration (10 hours only) and intensity (5 weeks) of treatment.
There is no blinding.
Abbreviation: CT = Conventional therapy, iMT = Individual Mirror therapy, gMT =Group Mirror Therapy, FMA =Fugl-Meyer Assessment, ARAT =Action Research Arm
Test, BI =Barthel Index, SIS =Stroke Impact Scale, MAS =Modified Ashworth Scale, SCT =Star Cancellation Test, ADL =Activities of Daily Living, QoL =Quality of Life

67
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome measure Results and effect size***
Cho et al.
(2012)
RCTs 1+ - n =26
- Mean age
=57.1
- Male Sex
=57.7%
- Mean time
since stroke
=3.55months
- Mean MMSE
=25.4
- FMA at
baseline =19.1
(28.9%)
MT (n=14):
Detail
- Flexion
/extension of
elbow, wrist, hand
- Moving arm
from side to side
- Tapping the table
Duration
- 25 min x2 /day, 5
times /week, for 4
weeks
- Total time =16.7
hours
CT (n=14):
- No sham
therapy*
- Baseline
- Post
treatment
Primary
1. FMA (Shoulder
/elbow
/forearm)
2. FMA (Wrist)
3. FMA (Hand)
4. FMA
(Coordination)
5. BS (Upper
limb)
6. BS (Hand)
Secondary
7. MFT (Upper
limb)
8. MFT (Hand)
Post-treatment,
-MT had greater improvement in
upper limb motor function than CT
1. 9.5 (MT) vs 4.6 (CT) [p=0.001]
2. 2.8 (MT) vs 1.1 (CT) [p=0.013]
3. 4.2 (MT) vs 1.5 (CT) [p=0.017]
4. 0.7 (MT) vs 0.4 (CT) [p=0.278]
5. 1.8 (MT) vs 0.7 (CT) [p=0.02]
6. 1.9 (MT) vs 0.5 (CT) [p=0.002]
7. 5.0 (MT) vs 2.2 (CT) [p=0.004]
8. 3.1 (MT) vs 0.5 (CT) [p=0.001]
Remarks:
Blinding & concealment did not be mentioned in the article.
Abbreviation: CT = conventional therapy, MT = mirror therapy, FMA = Fugl-Meyer Assessment, BS = Brunnstrom Stages, MFT = Manual Function Test

68
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome measure Results and effect size***
Blasis et al.
(2009)
RCTs 1+ - n =48
- Mean age =58.3
- Male sex
=45.8%
- Mean time since
stroke =5months
- First stroke
- WMFT at
baseline =3.55/5
(71.0%)
MT (n=24):
Detail
- Flexion /extension of
shoulder, elbow, wrist
- Pronation /supination
of forearm
Duration
- 30 min /day, 5
sessions /week, for 1st
& 2nd week
- 60 min /day, 5
sessions /week, for 3rd
& 4th week
- Total time =15 hours
CT (n=24):
- Same as MT
but covered
mirror
Duration
- same as MT
- Baseline
- 1 week
follow-up
- 24 weeks
follow-up
Primary
1. Pain score
at rest
2. Pain score
on
movement
3. Pain tactile
allodynia
Secondary
4. WMFT
(functional
ability)
5. WMFT
(performanc
e time)
6. MAL
After 24 weeks,
-MT had greater pain control on upper limb
than CT
1. -2.9 (MT) vs 0.6 (CT) [p<0.001]
2. -3.9 (MT) vs 0.3 (CT) [p<0.001]
3. -3.3 (MT) vs 0.3 (CT) [p<0.001]
-MT had greater improvement in upper
limb motor function than CT
4. -1.6 (MT) vs 0.6 (CT) [p<0.001]
5. -2.0 (MT) vs 1.6 (CT) [p<0.001]
6. 2.3 (MT) vs 0.3 (CT) [p<0.001]
Remarks:
Assessor was blinded. Subject could not be blinded due to the intervention.
Abbreviation: CT = conventional therapy, MT = mirror therapy, WMFT = Wolf Motor Function Test

69
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome
measure
Results and effect size***
Dohle et al.
(2009)
RCTs 1+ - n =48
- Mean age
=56.5
- Male sex
=72.2%
- Mean time
since stroke
=0.9months
- First stroke
- ARAT at
baseline =0.7/57
(1.23%)
MT (n=18):
Detail
- Execution of arm,
hand, finger postures
- Bilateral movement**
Duration
- 30 min /day, 5 days
/week, for 6 weeks
- Total time =15 hours
CT (n=18):
Detail
- No mirror
- Movement
of both hand
Duration
- Same as MT
- Baseline
- Post
treatment
Primary
1. FMA
(hand
section)
2. ARAT
Secondary
3. FIM
4. Neglect
score
Post treatment,
-MT had greater improvement in
upper limb motor function than CT
1. 4.4 (MT) vs 1.4 (CT) [p<0.05]
2. 4.1 (MT) vs 3.1 (CT) [p<0.05]
-MT had greater improvement in
ADL than CT
3. 18.3 (MT) vs 16.9 (CT)
[p>0.05]
-MT had greater improvement on
neglect than CT
4. 0.9 (MT) vs 0.2 (CT) [p=0.005]
Remarks:
Assessor was blinded. Subject could not be blinded due to the intervention.
Randomization (Envelopes with randomization sequence) and concealment (Sealed envelopes) method were mentioned
Abbreviation: CT = Control therapy, MT = mirror therapy, FM = Fugl-Meyer assessment of upper extremity test, ARAT = Action Research Arm Test, FIM = Functional
Independence Measure, ADL =Activities of Daily Living

70
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome
measure
Results and effect size***
Atay et al.
(2008)
RCTs 1+ - n =36
- Mean age
=63.2
- Male sex
=52.8%
- Mean time
since stroke :5.5
months
- First stroke
- BS (Upper
limb) at
baseline =2.73
(45.5%)
MT (n=20):
Detail
- Flexion /extension of
wrist, finger
Duration
- 30 minutes /day, 5
days /week, for 4 weeks
- Total time =10 hours
CT (n=20):
Detail
- Same as MT
but covered
mirror
Duration
- Same as MT
- Baseline
- Post
treatment
- 24
weeks
follow-up
1. BS (Hand)
2. BS (Upper
limb)
3. MAS
4. FIM
self-care
items
At 24 weeks follow-up,
-MT had greater improvement in
upper limb motor function than CT
1. 1.4 (MT) vs 0.5 (CT)
[p=0.001]
2. 1.5 (MT) vs 0.3 (CT)
[p=0.001]
- No significant improvement of
spasticity in MT was noted
3. -0.3 (MT) vs -0.3 (CT)
[p=0.904]
-MT had greater improvement on
ADL than CT
4. 8.3 (MT) vs 1.8 (CT)
(p=0.001)
Remarks:
Assessor was blinded. Subject could not be blinded due to the intervention.
Randomization (Computer-generated random number list with blocks) and concealment (Blinded doctor for randomization) method were mentioned
Abbreviation: CT = conventional therapy, MT = mirror therapy, BS = Brunnstrom Stages, FIM = the Functional Independence Measure, MAS = Modified Ashworth Scale

71
Bibliographic
Citation
Study
type
Level of
Evidence
Patient
Characteristics
Interventions Comparison Length of
follow-up
Outcome measure Results and effect size***
Altschuler et
al.
(1999)
RCTs,
planned
crossov
er
1- - n=9
- Mean age
=58.2
- Male sex
=55.6%
- Mean time
from stroke :57.6
months
- Level of
severity =7
severe, 1
moderate, 1 mild
MT (n=9):
Detail
- 4 weeks MT, then 4
weeks CT
- Bilateral movement**
- Proximal and distal
movement
Duration
- 15 min x2 /day, 6
days /weeks, for 4
weeks
- Total time =12 hours
CT (n=9):
Detail
- 4 weeks CT,
then 4 weeks
MT
- Same as MT
but transparent
plastic sheet
was used
Duration
- Same as MT
- Baseline
- Post
treatment
- 4 weeks
follow-up
1. Self-rated
scale
-MT had greater improvement in
upper limb motor function than
CT
1. 0.36 (MT), 0.08 (CT)
[No P value]
Remarks:
Self-rated scale =Change from baseline in terms of range of motion, speed and accuracy (-3 to +3), 0 represent no change
1 subject’s time since stroke was largely different from the others and thus increased the mean time from stroke.
Assessor was blinded. Subject could not be blinded due to the intervention.
Randomization and concealment method were not mentioned.
Abbreviation: CT = conventional therapy, MT = mirror therapy

72
Appendix (D): Table of comparison (I)
Aspect
Articles
Quality of
studies
Significant
Result
Subject characteristics
Mean age Male sex Time after stroke (Month) First time stroke Level of severity* Difference Level** Improvement***
Baricich et al.
(2013) + Y 66.6 50% 0.77 Y 32.4% 55.7% 172%
Chen et al.
(2013) + Y 54.2 70% 20.6 Y 68.5% 8.1% 11.8%
Bayn et al.
(2012) + N 67.2 58% 1.5 Y 6.2% 6% 96.8%
Cho et al.
(2012) + Y 57.1 57.7% 3.55 Y 28.9% 26.1% 90.3%
Blasis et al.
(2009) + Y 58.3 45.8% 5 Y 71% 32% 45.1%
Dohle et al.
(2009) + Y 56.5 72.2% 0.9 Y 1.23% 7.2% 585%
Atay et al.
(2008) + Y 63.2 52.8% 5.5 Y 45.5% 25% 54.9%
Abbreviation: Y = Yes, N = No
* Level of severity = Mean Motor function score in Mirror group at baseline / Total score x 100%
** Difference level = Mean difference between pre- & post- score / Total score x 100%
***Improvement = Mean difference between pre- & post- score / Mean Motor function score in Mirror group at baseline x 100%

73
Appendix (D): Table of comparison (II)
Aspect
Articles
Quality of
studies
Significant
Result
Data
collection
(Week)
Treatment Intensity Practice of upper limb
Duration of
Therapy (Hour)
Treatment
period (Week)
Flexion and extension
of upper limb’s joint Use of objects
Bilateral
movement
Baricich et al.
(2013) + Y 4 15 4 Y
Chen et al.
(2013) + Y 24 20 4 Y Y Y
Bayn et al.
(2012) + N Post 10 5 Y Y
Cho et al.
(2012) + Y Post 16.7 4 Y
Blasis et al.
(2009) + Y 2 15 4 Y
Dohle et al.
(2009) + Y Post 15 6 Y Y
Atay et al.
(2008) + Y 24 10 4 Y
Abbreviation: Y = Yes, N = No, Post = Post-treatment

74
Appendix (E): Potential Material Cost
Table of Material Cost of Implementing Mirror Therapy
Procedure Item Amount Each
Cost
Total
Amount
Material of mirror
therapy
Mirror (60cm
x 30cm)
20 pieces $100 $2000
Training session Paper 100 sheets $0.2 $20
Printer ink 1 piece $100 $100
APN 3 Nurses for 2 hours $300 $1800
Nurse 35 nurses for 2 hours $170 $11 900
OT 1 OT for 2 hours $170 $340
Briefing Session Paper 50 sheets $0.2 $10
Printer ink 1 piece $100 $100
APN 3 Nurses for 1 hours $300 $900
Nurse 35 nurses for 1 hour $170 $5950
Allied health
(PT, OT)
20 colleague for 1 hour $170 $3400
Physician 5 physicians for 1 hour $300 $1500
Implementation of
mirror therapy
Nurse 6 nurses with 1 hour for
5 days a week, 4 weeks
$170 $20 400
Evaluation during
follow-up
Nurse 40 patients in each 4
weeks, 1 hour for each
follow-up patients
$170 $6800
Total $55 220
(Abbreviation: APN = Advanced Practice Nurse, PT = Physiotherapist, OT = Occupational
therapist)
Material Cost of not Implementing Mirror Therapy
Procedure Item Amount Each
Cost
Total
Amount
Estimated 7 days
longer in
hospitalization
Patient 40 patients $2000 $80 000
Total $80 000

75
Appendix (F): Recommendation of Evidence-based
Practice Guideline (Detailed)
Recommendations
A. Reason of Providing Mirror Therapy to Stroke Patient
Recommendation 1:
Mirror therapy is proved to be effective on improving recovery of upper limb
motor function in stroke patients.
Evidence:
Participants in mirror therapy group had statistically significant results on
improving their motor function of upper limb when compared with the control group
(Atay et al., 2008 (Level 1+); Baricich et al., 2013 (Level 1+); Blasis et al., 2009
(Level 1+); Chen et al., 2013 (Level 1+); Cho et al., 2012 (Level 1+); Dohle et al.,
2009 (Level 1+)).
(Grades of Recommendation: A)
B. Target population
Recommendation 1:
Mirror therapy should be used in stroke patient aged above 18 years old with
first time having stroke. Also, it can be applied to both sexes.
Evidence:
Studies had recruitment criteria of first time stroke, adult age with mean age
ranged from 54.2 to 67.2 years old. They also recruited both gender in their studies.
The results were significant in these requirements’ patients (Atay et al., 2008 (Level
1+); Baricich et al., 2013 (Level 1+); Blasis et al., 2009 (Level 1+); Chen et al., 2013
(Level 1+); Cho et al., 2012 (Level 1+); Dohle et al., 2009 (Level 1+)).

76
(Grades of Recommendation: A)
Recommendation 2:
Mirror therapy should be applied to stroke patients from sub-acute to chronic
state.
Evidence:
From the reviewed studies, the mean time from stroke ranged from 0.77 to 20.6
months. Both sub-acute and chronic phase had statistically significant result towards
mirror therapy group (Atay et al., 2008 (Level 1+); Baricich et al., 2013 (Level 1+);
Blasis et al., 2009 (Level 1+); Chen et al., 2013 (Level 1+); Cho et al., 2012 (Level
1+); Dohle et al., 2009 (Level 1+)).
(Grades of Recommendation: A)
Recommendation 3:
Patients should be able to understand and follow verbal instructions.
Evidence:
In order to carry out the intervention, patients had to be cooperated and
understood simple commands so that they could move their non-paretic upper limb
while looking at the reflected image (Atay et al., 2008 (Level 1+); Baricich et al.,
2013 (Level 1+); Chen et al., 2013 (Level 1+); Cho et al., 2012 (Level 1+)).
(Grades of Recommendation: A)
C. Application of mirror therapy on stroke patients
Recommendation 1:
Sitting position with a mirror sized enough for patient to see his entire upper
limb is needed for the use of mirror therapy on training of upper limb in stroke
patients. The non-paretic upper limb is placed on the reflecting side. Patients
observe the motion of the non-paretic side in the mirror as if the motion of the

77
paretic side.
Evidence:
Patients had to be in sitting position with a mirror positioned perpendicular to the
midline of the patients. Then they moved their unaffected upper limb in front of the
reflective surface. Patients were told to focus on the image of the mirror (Altschuler et
al., 1999 (Level 1-); Atay et al., 2008 (Level 1+); Baricich et al., 2013 (Level 1+);
Blasis et al., 2009 (Level 1+); Chen et al., 2013 (Level 1+); Cho et al., 2012 (Level
1+); Dohle et al., 2009 (Level 1+)).
(Grades of Recommendation: A)
Recommendation 2:
The movement of the upper limb should include flexion and extension of
shoulder, elbow, wrist and finger, pronation and supination of forearm, moving
arm from side to side. Objects can be involved in the motion like squeezing
sponges, placing object in holes, flipping card.
Evidence:
The movement included flexion and extension of shoulder, elbow, wrist and
pronation and supination of forearm (Atay et al., 2008 (Level 1+); Baricich et al.,
2013 (Level 1+); Blasis et al., 2009 (Level 1+); Chen et al., 2013 (Level 1+); Cho et
al., 2012 (Level 1+); Dohle et al., 2009 (Level 1+)). Flexion and extension of finger
was included in the motion (Atay et al., 2008 (Level 1+). The upper limb were also
move from side to side (Cho et al., 2012 (Level 1+). Objects were used to perform
fine motor tasks like squeezing sponges, placing pegs in holes or flipping cards (Chen
et al., 2013 Level 1+)).
(Grades of Recommendation: A)
Recommendation 3:
Bilateral movement, which is the movement of paretic upper limb together with

78
non-paretic upper limb, should be involved.
Evidence:
Patients were instructed to view the image in the mirror and perform bilateral
symmetrical movements (Chen et al., 2013 (Level 1+); Dohle et al., 2009 (Level 1+)).
(Grades of Recommendation: A)
Recommendation 4:
Conventional stroke rehabilitation program, for example occupational therapy
and physiotherapy, should be included apart from mirror therapy.
Evidence:
Patients received interdisciplinary rehabilitation as usual. It included occupational
therapy, physiotherapy and speech therapy (Atay et al., 2008 (Level 1+); Baricich et
al., 2013 (Level 1+); Blasis et al., 2009 (Level 1+); Chen et al., 2013 (Level 1+);
Dohle et al., 2009 (Level 1+)).
(Grades of Recommendation: A)
Recommendation 5:
Patients should be in priority when the severity of patient’s paretic upper limb
was higher.
Evidence:
When comparing the improvement with the level of severity at the beginning between
the reviewed studies, more severe impairment’s patients had more improvement in
their upper limb functions after having mirror therapy. Less improvement was noted
in less severe patients (Atay et al., 2008 (Level 1+); Baricich et al., 2013 (Level 1+);
Blasis et al., 2009 (Level 1+); Chen et al., 2013 (Level 1+); Cho et al., 2012 (Level
1+)).
(Grades of Recommendation: A)

79
D. Treatment Intensity of Mirror Therapy
Recommendation 1:
Mirror therapy should be applied equal to or more than 10 hours in 4 weeks
Evidence:
Only studies equal to or more than 10 hours in 4 weeks had statistically significant
outcomes towards mirror therapy group (Atay et al., 2008 (Level 1+); Baricich et al.,
2013 (Level 1+); Blasis et al., 2009 (Level 1+); Chen et al., 2013 (Level 1+); Cho et
al., 2012 (Level 1+); Dohle et al., 2009 (Level 1+)).
(Grades of Recommendation: A)
E. Assessment and Evaluation
Recommendation 1:
Assessment and evaluation should be done prior and after the application of
mirror therapy:
Measuring tool the Action Research Arm Test is recommended to use to
evaluate the progress of the upper limb motor function.
Measuring tool The Functional Independence Measure should be used to
assess the independence of patients.
Evidence:
The Action Research Arm Test was used to assess motor function of upper limb. Score
ranged from 0 to 57 was recorded. Total of 19 items were included with 4 sub-scales
which were grasp, grip, pinch and gross movement. (Baricich et al., 2013 (Level 1+);
Dohle et al., 2009 (Level 1+)). The Functional Independence Measure was used to
evaluate patients’ self-care ability (Atay et al., 2008 (Level 1+); Baricich et al., 2013
(Level 1+)).
(Grades of Recommendation: A)

80
Recommendation 2:
Follow-up session should be arranged to evaluate patient’s progress of the
paretic upper limb function. It is recommended to follow the progress at least for
half year.
Evidence:
24 weeks follow-up session was arranged to patients to evaluate the long term
progress of patients’ upper limb function. Statistically significant results were noted
even for long term follow-up in mirror therapy group (Atay et al., 2008 (Level 1+);
Chen et al., 2013 (Level 1+)).
(Grades of Recommendation: A)

81
Appendix (G): Level of Evidence and Grades of
Recommendation (SIGN, 2011)
Level of Evidence
1++ - High quality meta-analyses, systematic reviews of RCTs, or RCTs with a
very low risk of bias
1+ - Well conducted meta-analyses, systematic reviews, or RCTs with a low risk
of bias
1- - Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ - High quality systematic reviews of case control or cohort studies
- High quality case control or cohort studies with a very low risk of
confounding or bias and a high probability that the relationship is causal
2+ - Well conducted case control or cohort studies with a low risk of
confounding or bias and a moderate probability that the relationship is causal
2- - Case control or cohort studies with a high risk of confounding or bias and a
significant risk that the relationship is not causal
3 - Non-analytic studies, e.g. case reports, case series
4 - Expert opinion
Grades of Recommendation
A - At least one meta-analysis, systematic review, or RCT rated as 1++, and
directly applicable to the target population; or
- A body of evidence consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating overall consistency of
results
B - A body of evidence including studies rated as 2++, directly applicable to the
target population, and demonstrating overall consistency of results; or
- Extrapolated evidence from studies rated as 1++ or 1+
C - A body of evidence including studies rated as 2+, directly applicable to the
target population and demonstrating overall consistency of results; or
- Extrapolated evidence from studies rated as 2++
D - Evidence level 3 or 4; or
- Extrapolated evidence from studies rated as 2+
Note: The grade of recommendation relates to the strength of the evidence on which the
recommendation is based. It does not reflect the clinical importance of the recommendation.

82
Appendix (H): Time Frame of the Mirror Therapy Program
Stage Action Timeline (Months)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Communication Plan
Setting up of implementation
team
Communicating with
administrators
Material preparation
Briefing session
Training session
Pilot Test
Recruitment of Subject
Mirror therapy
Follow-up
Evaluation
Implementing mirror
therapy
Recruitment of Subject
Mirror therapy
Follow-up
Evaluation

83
Appendix (I): Post Pilot Study Questionnaire for Staff
Name: __________________(Optional) Date: ___________________________
Please fill in the questionnaire about the new intervention “Mirror Therapy”.
Circle the answer which is the most suitable.
Questions
Do not
agree Agree
Agree
most
1. Did you think that mirror therapy could help the
patient to cope with the disease?
0 1 2
2. Did you find mirror therapy difficult to conduct? 0 1 2
3. Was mirror therapy suitable to be added in the
routine?
0 1 2
4. Did the briefing and training session help you to
know more about mirror therapy?
0 1 2
5. What difficulty did you encounter during conducting mirror therapy?
_____________________________________________________________________
6. Did you have any suggestion on conducting mirror therapy?
_____________________________________________________________________
7. What additional information would you like to know in briefing or training session?
_____________________________________________________________________
8. Any other suggestion.
_____________________________________________________________________
Thank you very much!
Please return to the mirror therapy implementation team.

84
Appendix (J): Satisfaction Survey (Patient)
Name: __________________(Optional) Date: ___________________________
Please circle appropriately in the survey about the intervention “Mirror Therapy”.
Content
Very
Unsatisfied Unsatisfied Satisfied
Very
Satisfied
Extremely
Satisfied
1. Explanation of mirror
therapy 1 2 3 4 5
2. Staff attitude 1 2 3 4 5
3. Enough support when
needed 1 2 3 4 5
4. Enough training time 1 2 3 4 5
5. Material use (e.g.
mirror) 1 2 3 4 5
6. Environment 1 2 3 4 5
7. Feedback from
healthcare profession 1 2 3 4 5
8. Overall, how satisfied
with mirror therapy 1 2 3 4 5
Total score: ________
Thank you very much!
Please return to the mirror therapy implementation team.

85
Appendix (K): Satisfaction Survey (Staff)
Name: __________________(Optional) Date: ___________________________
Please circle appropriately in the survey about the intervention “Mirror Therapy”.
Content
Very
Unsatisfied Unsatisfied Satisfied
Very
Satisfied
Extremely
Satisfied
1. Aims and objectives 1 2 3 4 5
2. Briefing session 1 2 3 4 5
3. Training session 1 2 3 4 5
4. Guideline of mirror
therapy 1 2 3 4 5
5. Material use (e.g.
mirror) 1 2 3 4 5
6. Implementation time 1 2 3 4 5
7. Workload 1 2 3 4 5
8. Cooperation between
colleague 1 2 3 4 5
9. Knowledge of mirror
therapy 1 2 3 4 5
10. Overall, how satisfied
with mirror therapy 1 2 3 4 5
Total score: ________
Thank you very much!
Please return to the mirror therapy implementation team.

86
References:
Altschuler E.L., Foster C., Galasko D., Llewellyn D.M.E., Ramachandran V.S., Stone
L. & Wisdom S.B. (1999). Rehabilitation of hemiparesis after stroke with a
mirror. The Lancet, 353, 2035-2036.
American Heart Association (2011). Heart Disease and Stroke Statistics--2012
Update: A Report from the American Heart association. Dallas: American Heart
Association, the American Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Retrieved August 20, from
http://circ.ahajournals.org/content/125/1/e2.
Archambault P.S., Fung J. & Norouzi-Gheidari N. (2012). Effects of robot-assisted
therapy on stroke rehabilitation in upper limbs: systematic review and
meta-analysis of the literature. Journal of rehabilitation research and
development, 49(4), 479-496.
Atay M.B., Bussmann J.B., Koseoglu F., Selles R., Sezer N., Stam H.J., Subeyaz S. &
Yavuzer G. (2008). Mirror therapy improves hand function in subacute stroke: a
randomized controlled trial. Archives of physical medicine and rehabilitation, 89,
393-398.
Baldry J., Johnson J., Kidd D., Petruckevitch A., Rossiter D., Stewart G. & Thompson
A.J. (1995). The functional independence measure: a comparative validity and
reliability study. Disability and Rehabilitation, 17, 10–14
Bare, B. & Smeltzer S. C. (2004). Brunner & suddarth’s textbook of medical-surgical
nursing (10th
ed.). Philadelphia, US: Lippincott Williams & Wilkins.
Baricich A., Carda S., Cisari C., Invernizzi M., Lanzotti L. & Negrini S. (2013). The
value of adding mirror therapy for upper limb motor recovery of subacute stroke
patients: a randomized controlled trial. European journal of physical and

87
rehabilitation medicine, 49, 311-317.
Bayn M., Behrens J., Pohl M., Thieme H., Wurg M. & Zange C. (2012). Mirror
therapy for patients with severe arm paresis after stroke - a randomized
controlled trial. Clinical rehabilitation, 27(4), 314-327
Beck C.T. & Polit D.F. (2008). Nursing research: generating and assessing evidence
for nursing practice (8th
ed.). Philadelphia, US: Lippincott Williams & Wilkins.
Blasis E.D., Blasis V.D., Cacchio A., Santilli V. & Spacca G. (2009). Mirror therapy in
complex regional pain syndrome type 1 of the upper limb in stroke patients.
Neurorehabilitation and neural repair, 23(8), 792-799.
Camicia M., Mannava M.K., Sandel M.E., Sidney S., Terdiman J. & Wang H. (2012).
Daily treatment time and functional gains of stroke patients during inpatient
rehabilitation. The American Academy of Physical Medicine and Rehabilitation,
5(2), 122-128.
Cattaneo L. & Rizzolatti G. (2009). The mirror neuron system. Archives of Neurology,
66(5), 557-560.
Chang A.M., Mackenzie A.E. (1998). State self-esteem following stroke. Stroke,
29(11), 2325-2328.
Chen Y.T., Huang P.C., Lin K.C., Yang H.W. & Wu C.Y. (2013). Effects of mirror
therapy on motor and sensory recovery in chronic stroke: a randomized
controlled trial. Archives of physical medicine and rehabilitation, 94, 1023-1030.
Cheng S.K., Lee T.M., Leung A.W., Leung K.K. & Mak A.K. (2010). Functional gain
in hemorrhagic stroke patients is predicted by functional level and cognitive
abilities measured at hospital admission. NeuroRehabilitation, 27(4), 351-358.
Cho H., Lee M.M. & Song C.H. (2012). The mirror therapy program enhances upper
limb motor recovery and motor function in acute stroke patients. American
journal of physical medicine & rehabilitation, 91, 689-700.

88
Collier J.M., Dewey H.M. & Sherry L.J (2007). Stroke rehabilitation 2007: what
should it be? International journal of stroke, 2(3), 191-200.
Craighero L. & Fadiga L. (2004). Electrophysiology of action representation. Journal
of clinical neurophysiology, 21(3), 157-169.
The Department of Health (2012). Number of deaths by leading causes of death. Hong
Kong: The government of the Hong Kong Special Administrative Region,
Department of Health, Centre for Health Protection. Retrieved August 7, 2013,
from http://www.chp.gov.hk/en/data/4/10/27/380.html
Dohle C., Karbe H., Kust J., Nakaten A., Pullen J. & Rietz C. (2009). Mirror therapy
promotes recovery from severe hemiparesis: a randomized controlled trial.
Neurorehabilitation and neural repair, 23(3), 209-217.
Duncan P.W., Lai S.M., Perera S. & Studenski S. (2002). Persisting consequences of
stroke measured by the stroke impact scale. Stroke, 33(7), 1840-1844.
Fugl-Meyer A.R., Jaasko L., Leyman I., Olsson S. & Steglind S. (1975). The
post-stroke hemiplegic patient. Scandinavian journal of rehabilitation medicine,
7(13), 13-31.
Funase K., Higashi T., Kasai T., Liang N. & Tabira T. (2007). Increased corticospinal
excitability during direct observation of self-movement and indirect observation
with a mirror box. Neuroscience letters, 419(2), 108-112.
Hospital Authority (2012). Hospital Authority statistical report (2010-2011). Hong
Kong: Author. Retrieved August 7, 2013, from
http://www.ha.org.hk/upload/publication_15/411.pdf.
Johansson B.B. (2011). Current trends in stroke rehabilitation. A review with focus on
brain plasticity. Acta neurologica scandinavica, 123(3), 147-159.
Kollen B.J., Kwakkel G., Prevo A.J.H. & Van der Grond J. (2003). Probability of
regaining dexterity in the flaccid upper limb. Stroke, 34, 2181-2186.

89
Lyle, R.C. (1981). A performance test for assessment of upper limb function in
physical rehabilitation treatment and research. International journal of
rehabilitation research, 4(4), 483-492.
Scottish Intercollegiate Guidelines Network (2011). Sign 50: A guideline developer’s
handbook. Edinburgh: Scottish Intercollegiate Guidelines Network, Healthcare
Improvement Scotland. Retrieved December 14, 2013, from
http://www.sign.ac.uk/pdf/sign50.pdf.
Scottish Intercollegiate Guidelines Network (2013). Critical appraisal: notes and
checklists. Edinburgh: Scottish Intercollegiate Guidelines Network, Healthcare
Improvement Scotland. Retrieved August 14, 2013, from
http://www.sign.ac.uk/methodology/checklists.html.