Embed Size (px)
Citation preview

L
Arh
ALD
a
ARAA
KHLMRSS
1
medptmhfimi
Bf
1h
Digestive and Liver Disease 46 (2014) 257–263
Contents lists available at ScienceDirect
Digestive and Liver Disease
jou rna l h om epage: www.elsev ier .com/ locate /d ld
iver, Pancreas and Biliary Tract
n explorative data-analysis to support the choice between hepaticesection and radiofrequency ablation in the treatment ofepatocellular carcinoma
lessandro Cucchetti ∗, Fabio Piscaglia, Matteo Cescon, Carla Serra, Antonio Colecchia,orenzo Maroni, Laura Venerandi, Giorgio Ercolani, Antonio Daniele Pinnaepartment of Medical and Surgical Sciences, S.Orsola – Malpighi Hospital, Alma Mater Studiorum – University of Bologna, Bologna, Italy
r t i c l e i n f o
rticle history:eceived 28 May 2013ccepted 27 October 2013vailable online 24 November 2013
eywords:epatocellular carcinomaiver functiononte Carlo simulation
adiofrequency ablationurvivalurgical therapy
a b s t r a c t
Background: Whether to prefer hepatic resection or radiofrequency ablation as first line therapy forhepatocellular carcinoma is a matter of debate.Aims: To compare outcomes of resection and ablation, in the treatment of early hepatocellular carcinoma,through a decision-making analysis.Methods: Data of 388 cirrhotic patients undergoing resection and of 207 undergoing radiofrequencyablation were reviewed. Two distinct regression models were devised and used to perform sensitivityand probabilistic analyses, to overcome biases of covariate distributions.Results: Actuarial survival curves showed no difference between resection and ablation (P = 0.270) despitethe fact that ablated patients were older, with worse liver function and smaller, unifocal tumours(P < 0.05), suggesting a complex, non-linear relationship between clinical, tumoral variables and treat-ments. Sensitivity and probabilistic analyses suggested that the superiority of resection over ablation
decreased at higher Model for-End stage Liver Disease scores, and that ablation provided better resultsfor smaller tumours and higher Model for-End stage Liver Disease scores. In patients with 2–3 tumoursup to 3 cm, the two treatments produced opposite comparative results in relation to the Model for-Endstage Liver Disease score.Conclusions: The superiority, or the equivalence, of resection and ablation depends on the non-linearrelationship existing between treatment, tumour number, size and degree of liver dysfunction.© 2013 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
. Introduction
Hepatocellular carcinoma (HCC) is the most frequent primaryalignancy of the liver and is closely linked to chronic liver dis-
ase [1]. Surveillance programmes of subjects at risk have beeneveloped in many areas of the world; consequently, an increasedroportion of HCCs could be diagnosed at early stages [2,3]. Inhese cases, liver transplantation is theoretically the best treat-
ent, but the scarcity of donors limits this treatment. Currently,epatic resection (HR) and radiofrequency ablation (RFA) are the
rst line therapies considered potentially curative in the treat-ent of HCC and are offered in cases in which transplantations not an option or for candidates on the waiting-list. In the last
∗ Corresponding author at: Policlinico Sant’Orsola-Malpighi, University ofologna, Via Massarenti 9, 40138 Bologna, Italy. Tel.: +39 051 6363721;
ax: +39 051 304902.E-mail address: [email protected] (A. Cucchetti).
590-8658/$36.00 © 2013 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevierttp://dx.doi.org/10.1016/j.dld.2013.10.015
decade, a number of retrospective and randomized controlled tri-als (RCTs) which directly compared these two treatments have beenpublished. Available RCTs have not resolved the doubts regardingthe superiority of one treatment over the other, probably due tothe inclusion criteria adopted [4–6]. Observational studies havenot helped to clarify this topic since they have clearly shown thatthe patients undergoing HR or RFA were significantly different asregards the clinical and tumoral characteristics capable of affectingprognosis [7–16]; if all these biases are not adequately handled, theresults can be confounding.
The aim of the present study was to develop a decision-makinganalytic model, derived from a large series of patients treatedin a tertiary referral hospital, which included those clinical andtumoral features which are the main determinants of treatmentassignment and prognosis. A stratification of the analysis, for
tumour stage and degree of liver dysfunction, was applied ina sensitivity approach and in a probabilistic simulation, aimedat assessing effectiveness uncertainty of these two competingstrategies.Ltd. All rights reserved.

2 nd Liv
2
hpaSpapeawadawa
2
pphuAptciistar
2
flaaRaavdtSGboDig
2
pugrt
58 A. Cucchetti et al. / Digestive a
. Methods
The study was planned to develop two distinct proportionalazard prognostic models: one for HR patients and one for RFAatients, and to use results obtained to run sensitivity and prob-bilistic sensitivity analyses using a decision-tree model (TreeAgeoftware Inc., Williamstown, MA, USA). This approach allows com-aring the two treatment populations, even if the baseline clinicalnd tumoral characteristics are different inasmuch as the com-arison is not directly carried out on observed survival, but onxpected survival calculated using corresponding beta-coefficients,nd baseline hazard functions. Subsequently, a sensitivity analysisas carried out, in which one prognostic variable was kept fixed,
nd expected survivals for resection and ablation were compared atifferent variations of the remaining prognostic variables. A prob-bilistic analysis aimed at assessing the uncertainty of the modelas finally carried out. Additional details of the statistical analyses
re reported in the specific section.
.1. Patient population
Between January 1997 and November 2011, 388 cirrhoticatients underwent HR for HCC at a tertiary referral Hospital; theolicies of our centre regarding indications for hepatic resectionave already been published [17,18]. Details regarding study pop-lation selection and surgical approach can be found in Appendix. Between December 2001 and November 2011, 207 cirrhoticatients underwent RFA for HCC at three clinical units of the sameertiary referral hospital. The diagnosis of HCC was histologicallyonfirmed, before RFA, in 28 cases via percutaneous or open biopsy;n the remaining patients, it was based on guidelines for the non-nvasive assessment of HCC which had been released during thetudy inclusion period [19,20]. Details regarding policy of our Insti-ution and ablation technique can be found in Appendix A. Clinicalnd tumour characteristics of surgical and ablated patients areeported in Table 1.
.2. Follow-up
Following discharge, all patients were observed periodically atollow-up to exclude a possible recurrence of the HCC; biochemicaliver function tests, serum alpha-fetoprotein level measurement,nd US or CT/MRI were performed 3 and 6 months after dischargend then according to a semi-annual surveillance programme.ecurrent lesions were managed aggressively by a multimodalpproach, which included re-resection, TACE, percutaneous RFAnd PEI. For selected patients with transplantable recurrences, sal-age liver transplantation was also adopted. The treatment wasecided by the pattern of recurrence, liver functional reserve, andhe general condition of the patient at the time of the recurrence.ince the end of 2008, Sorafenib (Nexavar®; Bayer, Leverkusen,ermany) therapy has also been adopted, either alone or in com-ination with percutaneous approaches or TACE for treatmentf recurrences [21,22]. Follow-up data were collected until 31st
ecember 2012. Informed consent was obtained from each patientncluded in the study and the study protocol conforms to the ethicaluidelines of the 1975 Declaration of Helsinki.
.3. Statistical analysis
Categorical variables were reported as number of cases andrevalence, and differences between the subgroups were compared
sing the Fisher exact test. Continuous variables were investi-ated for their normal distribution (Kolmogorov–Sminov test) andeported as mean and standard deviation or medians and interquar-ile ranges (25th and 75th percentiles), as appropriate. Differenceser Disease 46 (2014) 257–263
between subgroups were investigated using Mann–Whitney test.All analyses were two-tailed. Effect size was also calculated for eachcovariate comparison [23]. Overall survival was the primary endpoint of the study and was computed from the day of HCC treat-ment (surgery or ablation) until the most recent follow-up or untilpatient death. Recurrence-free survival was computed from theday of surgery until the most recent follow-up visit or until clin-ical evidence of tumour recurrence. For RFA patients, the presenceof residual tumour at 1 month after the first ablation procedurewas not considered as recurrence, which was conversely defined,for these patients, as the occurrence of a new lesion distant from thepreviously treated nodule, regardless of timing, or tumour relapseof the treated nodule, 3 months after completion of treatmentsession. Ablated patients who did not achieve a complete responseafter 3 months were considered as having recurrence at the date ofthe last imaging technique. Transplanted patients were censoredthe day prior to transplantation.
Two distinct proportional hazard models were developed hav-ing patient survival as an outcome measure: one for the 388surgical patients and one for the 207 RFA patients. Tumour size,number (single versus multiple nodules) and Model for End-stageLiver Disease (MELD) score were selected for the multivariateregression analyses [24–26]. These variables were selected becausethe decision to perform surgery or ablation is mainly a func-tion of tumour burden and the degree of liver dysfunction. Oncebeta-coefficients and baseline cumulative hazard were obtainedfor each proportional hazard model, yearly survival estimationwas calculated using the following equation: S0(year) ̂ (EXP(PI)),where: S0(year) = −EXP(baseline cumulative hazard for eachyear) and PI = betaMELD × MELD(unit) + betamultiple × (1 = two orthree nodules; 0 = single nodule) + betasize × tumour size(cm). Beta-coefficients together with their 95% confidence intervals wereentered in the subsequent sensitivity and probabilistic models upto the 14th decimal place. Proportional hazard assumption foreach model was assessed by Schonfeld residuals analysis (P > 0.05in all cases) and non-linearity exclusion verified by Martingaleresiduals.
Yearly survival estimations obtained from Cox regressions wereconverted into annual mortality using the DEALE method [27]. Mor-tality excess due to different age and gender proportions in the twogroups were taken into account by subtracting the relative mortal-ities derived from the Italian National Institute of Statistics (ISTAT)[28]. A sensitivity analysis was carried out to obtain informationregarding the treatment preferred in relationship to clinical andtumoral characteristics. In particular, in this analysis, the covariatesMELD and number of nodules were maintained fixed at determinedvalues (i.e. MELD = 7–8 and single nodules) while tumour diameterwas varied between 1 and 5 cm. Both beta-coefficients and baselinecumulative hazard values, for all the three clinical variables, werevaried within their 95% confidence intervals, assuming a triangulardistribution. Sensitivity analysis included 388 patients for resectionarm and 207 for ablation arm. Uncertainty of the model was furtherexplored by running probabilistic analyses. In particular, differentclinical scenarios were simulated according to international guide-lines recommendations [19,20]. For each clinical subgroup, tumourdiameter and MELD score were assumed having a uniform distribu-tion, while beta-coefficients and baseline cumulative hazards werevaried within their 95% confidence intervals, assuming a triangulardistribution. For each subgroup, 1000 patients for each treatmentarm were assumed. Results of probabilistic analyses were mea-sured with both effect-size and number needed to treat (NNT)[29,30]. The NNT can be thought of as the number of patients who
need to be treated in order for one to benefit. In theory, the higherthe NNT, the less superior is one treatment against the comparativetreatment, because more individuals need to receive the specifictreatment to see a benefit in one. A significance level of 0.05 was
A. Cucchetti et al. / Digestive and Liver Disease 46 (2014) 257–263 259
Table 1Baseline clinical and tumoral characteristics of patients with HCC undergoing hepatic resection (HR) or radiofrequency ablation (RFA).
Variable HR (n = 388) RFA (n = 207) P Effect size
Age (years) 65 (58–71) 68 (60–75) 0.001 −0.315Male gender 302 (77.8%) 142 (68.6%) 0.017 0.262HBsAg+ 82 (21.1%) 33 (15.9%) 0.156 0.191Anti-HCV+ 273 (70.4%) 136 (65.7%) 0.265 0.118Serum total protein (g/dL) 7.6 (7.2–8.0) 7.4 (6.9–7.9) 0.001 0.339Serum albumin (g/dL) 3.9 (3.5–4.1) 3.8 (3.4–4.1) 0.051 0.194Total bilirubin (mg/dL) 0.81 (0.62–1.20) 1.12 (0.77–1.75) 0.001 −0.614PLT count (×103/mmc) 128 (94–175) 104 (73–146) 0.001 0.367PLT count ≤100 × 103/mmc 117 (30.2%) 99 (47.8%) 0.001 −0.415INR 1.15 (1.08–1.22) 1.21 (1.13–1.33) 0.001 −0.692Child–Pugh class A 374 (96.4%) 163 (78.7%) 0.001 1.089MELD score 8 (7–9) 9 (8–12) 0.001 −0.802Esophageal varices 102 (26.3%) 123 (59.4%) 0.001 −0.779Single tumoura 309 (79.6%) 184 (88.9%) 0.004 −0.395Largest tumour size (cm)a 3.5 (2.5–4.7) 2.4 (2.0–3.0) 0.001 0.783BCLC stage 0.001
0 27 (7.0%) 39 (18.8%) – −0.542A 257 (66.2%) 162 (78.3%) – −0.334B 104 (26.8%) 6 (2.9%) – 1.382
Surgical procedure –Wedge 213 (54.9%) – – –Segmentectomy 104 (26.8%) – – –Bisegmentectomy 45 (11.6%) – – –Major hepatectomy 26 (6.7%) – – –
Patient survival 0.2701-year (%) (95%C.I.) 88.1 (84.3–90.9) 92.5 (89.3–94.7) – −0.2613-year (%) (95%C.I.) 69.1 (63.5–73.9) 66.2 (57.5–73.6) – 0.0735-year (%) (95%C.I.) 57.4 (50.8–63.4) 43.2 (32.1–53.8) – 0.321
Recurrence-free survival 0.0011-year (%) (95%C.I.) 74.7 (69.8–80.7) 56.3 (48.8–63.0) – 0.4543-year (%) (95%C.I.) 43.8 (37.8–49.6) 24.7 (17.9–32.0) – 0.4795-year (%) (95%C.I.) 31.0 (24.7–37.4) 15.4 (9.2–22.9) – 0.494
Continuous variables are reported as medians and inter-quartile ranges (25–75th percentiles). For continuous variables, the effect size was measured after Log10 transfor-m oderate differences and >|0.5| = considerable differences. Abbreviations: MELD, Model forE rnational normalized ratio.
cteristics.
uRT(
3
otcomsowsduymtppw(rwro
Table 2Results from multivariate Cox regression in patients undergoing hepatic resectionand in patients undergoing radiofrequency ablation.
Variable Beta-coefficient (95% C.I.) P-value
Hepatic resectionMELD score (per unit increase) 0.132 (0.011–0.252) 0.032Two or three nodules vs. a single
nodule0.408 (−0.022 to 0.838) 0.063
Size of the largest tumour (percm increase)
0.162 (0.086–0.238) 0.001
Baseline cumulative hazard1 year 0.015 (0.010–0.021) –2 year 0.026 (0.019–0.034) –3 year 0.046 (0.035–0.057) –4 year 0.059 (0.046–0.074) –5 year 0.070 (0.055–0.087) –
Radiofrequency ablationMELD score (per unit increase) 0.083 (0.001–0.155) 0.049Two or three nodules vs. a single
nodule0.604 (−0.045 to 1.254) 0.068
Size of the largest tumour (percm increase)
0.337 (0.074–0.600) 0.012
Baseline cumulative hazard1 year 0.010 (0.005–0.016) –2 year 0.035 (0.023–0.048) –3 year 0.057 (0.040–0.077) –4 year 0.082 (0.059–0.108) –5 year 0.118 (0.085–0.160) –
Survival estimation for each year is calculated by the following equationS0(year) ̂ (EXP(PI)), where S0(year) = −EXP(baseline cumulative hazard for eachyear) and PI = betaMELD × MELD (unit) + betamultiple × (1 = two or three nodules;0 = single nodule) + beta × tumour size (cm). Baseline cumulative hazard was cal-
ation: <|0.1| = very small differences; |0.1|–|0.3| = small differences; |0.3|–|0.5| = mnd-stage Liver Disease; BCLC, Barcelona Clinic Liver Cancer; PLT, platelet; INR, Intea For surgical patients, these features were radiological and not histological chara
sed in all analyses. The statistical analysis was carried out using-project (cox.zph function; R version 2.13.0; Copyright (C) 2011he R Foundation for Statistical Computing) and SPSS 10.0 softwareSPSS, Chicago, IL, USA).
. Results
The baseline characteristics, comparative analysis and outcomesf the surgical and the RFA patients are reported in Table 1. Thewo groups were representative of the general clinical and tumoralharacteristics which regard the use of one treatment versus thether; in particular, RFA patients were significantly older, withore advanced liver dysfunction and with smaller, and more often
ingle, tumours (P < 0.05 in all cases). A higher male prevalence wasbserved in surgical patients. The 30-day mortality after surgeryas 2.3% and that after ablation was 0.5%; the median in-hospital
tay after surgery was 8 days (range: 3 days, 5 months) and 2ays after ablation (range: 0 days, 2 months). The median follow-p for the surgical patients was 29 months (range: 14 days, 12ears) and that of the ablated patients was 24 months (range: 1onth, 10 years). During these time periods, 142 patients out of
he 388 undergoing surgery, and 70 patients out of the 207 ablatedatients died. Conversely, 16 surgical (4.3%) and 20 ablated (9.7%)atients were transplanted. In particular, 54 surgical patients diedithout tumour recurrence (13.9%) and 88 died after recurrence
22.7%) whereas 13 ablated patients died without tumour recur-
ence (6.3%) and 57 died after recurrence (27.5%). Overall survivalas similar between the two groups (P = 0.270) but the survivalates reversed themselves over time, suggesting a different impactf clinical and tumour characteristics in determining prognosis;
size
culated by the means of Breslow estimator. Beta-coefficients together with their95% confidence intervals (inclusive of negative confidence limits regarding tumournumber) were used in the subsequent deterministic and probabilistic models.Coefficients and baseline hazard function were entered up to the 14th decimal place.

2 nd Liver Disease 46 (2014) 257–263
cv
3
mtdasa(ncwpsw2
awstauhvrrw(a(
3
Ts(tarnt1
<(MeaRbpswMhanc2
Table 3Second order Monte Carlo simulation of HCC patients undergoing hepatic resection(HR) or radiofrequency ablation (RFA) stratified by tumour size, number and MELDscore.
HR(n = 1000)
RFA(n = 1000)
Effectsize
Single nodule <2.0 cmMELD score 6–9
5-year life-expectancy (years) 4.41 ± 0.23 4.46 ± 0.16 −0.252Expected 5-year survival rate 81.0% 82.5% –Number needed to treat – 67 –
MELD score ≥105-year life-expectancy (years) 3.93 ± 0.59 4.22 ± 0.32 −0.611Expected 5-year survival rate 66.3% 74.9% –Number needed to treat – 12 –
Single nodule 2.0–3.0 cmMELD score 6–9
5-year life-expectancy (years) 4.30 ± 0.27 4.21 ± 0.28 0.327Expected 5-year survival rate 77.5% 74.8% –Number needed to treat 38 – –
MELD score ≥105-year life-expectancy (years) 3.74 ± 0.70 3.91 ± 0.46 −0.287Expected 5-year survival rate 60.6% 65.6% –Number needed to treat – 20 –
Single nodule 3.1–5.0 cmMELD score 6–9
5-year life-expectancy (years) 4.10 ± 0.35 3.72 ± 0.59 0.783Expected 5-year survival rate 71.3% 60.3% –Number needed to treat 9 – –
MELD score ≥105-year life-expectancy (years) 3.49 ± 0.75 3.37 ± 0.74 0.161Expected 5-year survival rate 53.5% 50.2% –Number needed to treat 31 – –
Two or three nodules ≤3.0 cmMELD score 6–9
5-year life-expectancy (years) 4.06 ± 0.38 3.87 ± 0.48 0.439Expected 5-year survival rate 70.1% 64.4% –Number needed to treat 18 – –
MELD score ≥105-year life-expectancy (years) 3.35 ± 0.82 3.49 ± 0.69 −0.185Expected 5-year survival rate 49.6% 53.5%Number needed to treat – 26
Effect size <|0.1| = very small differences; |0.1|–|0.3| = small differences;|0.3|–|0.5| = moderate differences and >|0.5| = considerable differences. Thenumber needed to treat (NNT) gives the number of people you would have to treatwith one intervention (compared to the control) to prevent one event. The higherthe NNT, the less effective the treatment. Continuous variables are reported asmeans and standard deviations. For tumour size and MELD score, the distributionwas assumed to be uniform. For tumours <2 cm, the size ranged between 0.8 and1.9 cm; for multiple tumours the size ranged 0.8 and 3 cm; for a MELD score ≥10
60 A. Cucchetti et al. / Digestive a
onversely, surgery led to significantly better recurrence-free sur-ival (P = 0.001).
.1. Sensitivity analysis
The results from the multivariate Cox model for the threeain determinants of treatment allocation, namely, liver func-
ion measured by the MELD score, tumour number and tumouriameter are reported in Table 2, together with baseline haz-rd function at different time points. Tumour size was thetrongest predictor of patient survival in both groups (P = 0.001fter resection and 0.012 after ablation) followed by MELD scoreP = 0.032 after resection and 0.049 after ablation) and tumourumber (P = 0.063 after resection and 0.068 after ablation). Betaoefficients and 95% confidence intervals were entered togetherith the baseline hazard function into the model. Since com-arative analysis of Table 1 showed a male predominance inurgical patients and an older age in ablated patients, the modelas adjusted for these two covariates, as described in Section
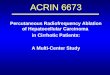
.The results of the sensitivity analysis, with varying tumour sizes
nd MELD scores in single nodules, are reported in Fig. 1. In patientsith a MELD of 7 or 8 and a single HCC (Panel A), RFA demonstrated
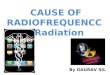
imilar, or even slightly better, life expectancy than resection whenhe tumour size was <1.8 cm; with a higher MELD score (Panels Bnd C), the benefit obtainable from ablation extends to tumoursp to 3 cm. Beyond this tumour size threshold, surgery results inigher life expectancy. The results of the sensitivity analyses, witharying tumour sizes and MELD scores in two or three nodules, areeported in Fig. 2. In patients with a MELD score of 7 or 8 (Panel A),esection provides better life expectancy than ablation, especiallyith the increased size of the largest tumour; at higher MELD scores
Panels B and C), the benefit obtainable from resection decreasesnd ablation results in better life expectancy for smaller tumourspanels b and c).
.2. Probabilistic analysis
The results of the Monte Carlo simulation are reported inable 3. For patients with single tumours <2 cm and a MELDcore <10, the two treatments show very similar survival rateseffect size <|0.3|). Even if survival was slightly longer after abla-ion, the NNT with RFA was very high; 67 patients needed to beblated before a survival advantage of one ablated patient overesection was achieved. Conversely, when liver function worsens,amely a MELD score ≥10, RFA offers a greater survival advan-age over resection (effect size >|0.5|) and an NNT which drops to2.
For single nodules of 2–3 cm, in patients having a MELD score10, surgery results in a very modest survival benefit over RFAeffect size: |0.3|–|0.5|) and an NNT of 38 patients; when the
ELD score is >10, the scenario changes and RFA has a mod-st survival benefit in comparison to surgery (effect size <|0.3|)nd an NNT of 20. Surgery leads to a large survival benefit overFA for patients with a MELD score <10 and a single noduleetween 3.1 and 5 cm (effect size >|0.5|) and an NNT of only 9atients; this gain decreases when the MELD score is >10 (effectize <|0.3|) and an NNT which goes up to 31. Similarly, for whatas observed for single nodules of 2–3 cm, in patients with aELD score <10 and two or three nodules up to 3 cm, surgery
as a modest survival benefit over RFA (effect size: |0.3|–|0.5|)
nd an NNT of 18 patients; when the MELD score is >10, the sce-ario changes, and RFA offers a very modest survival benefit inomparison to surgery (effect size <|0.3|) and an NNT as high as6.values ranged between 10 and 14. Patients were stratified according to tumourfeatures and MELD, following accepted clinical thresholds.
4. Discussion
The choice for resection or RFA for the treatment of HCC rep-resents a clinical dilemma which often occurs in clinical practice.A clear example comes from the national conference of the JapanSociety of Hepatology, held in 2009 when, to the question “Whichtreatment would you perform for 2-cm sized HCC nodules in patientswith Child–Pugh A liver function?”, 80% of surgeons responded“resection”, and 68% of non-surgeons responded “RFA” [31]. Evenif greater agreement was observed when asking about the opti-mal treatment of 3-cm sized nodules, these conclusions point outthe uncertainty related to the optimal therapeutic strategy for HCCpatients. The present analysis represents an in-depth evaluationof medical circumstances which can guide the therapeutic strat-egy of HCC, in cirrhotic patients, towards surgery or ablation. Inparticular, tumoral and liver function thresholds for an optimiza-tion of therapeutic choice were proposed, and the uncertainty
related to the natural variability of outcome after each treatmentwas explored to assess the effect size of one treatment over theother.
A. Cucchetti et al. / Digestive and Liver Disease 46 (2014) 257–263 261
Fig. 1. Results from the sensitivity analysis on a single tumour at varying MELD scores and tumour diameters. Expected values represent the life expectancy achievable withresection or ablation over a 5-year period. The covariates number of nodules and MELD score were maintained fixed at determined values (panel A, MELD = 7–8; panel B,M d 5 cmv distrib
stiarmnaqsdiiwbacasc
orptim
ELD 9–10; panel C, MELD 11–12) while tumour diameter was varied between 1 anariables, were varied within their 95% confidence intervals, assuming a triangular
Looking at patient characteristics, it is immediately clear thaturgical and ablated patients are significantly different regardingumoral and clinical characteristics. This is not surprising because,n clinical practice, older patients, with smaller tumours and a moredvanced degree of liver dysfunction more often undergo ablationather than surgery. This finding is very frequently found in theedical literature which compares resection to ablation [4–16]. Of
ote, in the RCT of Chen, the proportion of patients randomized toblation who refused treatment was quite high (21%) raising theuestion as to whether an RCT can really be conducted in a real-lifecenario [4,32]. When it is difficult to carry out prospective trialsue to different overwhelming practical and ethical problems, as
n the instance of HCC, modelling studies can help clarify specificssues. In the present analysis, a different methodological approach
as applied. The development of two distinct prognostic models,ased on the same clinical and tumoral variables and adequatelydjusted for age and sex, allowed a comparison of predicted out-omes of surgery and ablation through sensitivity and probabilisticnalyses. In particular, the Monte Carlo simulation gave us the pos-ibility of testing the uncertainty that could be expected from theomparison of the two therapies.
The sensitivity analysis pointed out that the benefit of resectionver ablation increased with increasing tumour size, whicheflected the fact that the larger the tumour, the lower the com-
lete response rate achievable with ablation, and, consequently,he lower the expected survival. At the same time, with an increas-ng degree of liver dysfunction the benefit of resection decreasedore rapidly than that of RFA, allowing ablation to achieve better
. Beta-coefficients and baseline cumulative hazard values, for all the three clinicalution.
survivals for larger tumour diameters. This is because ablation had alesser detrimental effect on liver functional reserve than resectionor, from the opposite point of view, the benefit obtainable fromresection in terms of oncological radicality was lost because of thepostoperative deterioration of liver function. These results pointedout how the outcomes of surgery and ablation were not linearlyrelated to tumour size or liver function but reversed themselves asthese characteristics varied. Such a non-linear relationship can wellexplain the disagreement observed in the literature and confirmrecent expert opinions regarding the impossibility of conducting areliable RCT [4–16,32].
Prognosis after each therapy is obviously accompanied by thereliability of the estimate consequent to the uncertainty related tothe procedure itself. In other words, similar patients could experi-ence different outcomes although undergoing the same procedure.This aspect is pointed out, in the present study, by the probabilis-tic analysis. In presence of a MELD score <10, RFA and surgeryobtained very similar results in treating single nodules <2 cm asseen by an effect size <|0.3| and an NNT of 67. This latter indicatormeant that 67 patients were needed to be treated with RFA beforean advantage over resection for one single patient was achieved.Obviously, this relatively high number of patients confirmed thatthe observed difference had no clinical significance and that thetwo procedures can bring similar outcomes. Nevertheless, the NNT
dropped to 12 for the same tumour size but with higher MELDscore; in this scenario, RFA could provide a reasonable benefit overresection, as confirmed by an effect size >|0.5|. For tumours between3.1 and 5 cm, resection can provide better results than RFA, with a
262 A. Cucchetti et al. / Digestive and Liver Disease 46 (2014) 257–263
F LD scod or abld hin th
rwpdzd
dalaotsApdaittwctippssia
ig. 2. Results from the sensitivity analysis on two or three tumours at varying MEiameters. Expected values represent the life-expectancy achievable with resectioniameters, and varying beta-coefficients and baseline cumulative hazard values wit
easonable NNT of 9 when the MELD score was <10; this benefitas, however, reduced for higher MELD score (NNT: 31). Finally,robabilistic analysis showed that single tumours of 2–3 cm iniameter, and two or three tumours <3 cm represented a greyone, in which the two procedures could be alternatively suggestedepending on the degree of liver dysfunction.
The present study has some limitations which deserve specificiscussion. First, the ability of the model to achieve a prognosisfter treatment is influenced by the characteristics of the popu-ation on the basis of which it is constructed. However, surgicalnd ablated patients, of the present series, were representativef the typical patients who undergo one or the other treatment,hus, limiting the possible bias which could derive from the super-election of individuals needed to find comparable patient groups.nother limitation is represented by the sample size of the twoopulations. It is logical to expect that larger sample size will pro-uce less uncertainty. This is the reason why we added NNT to thenalysis since a statistically significant difference did not necessar-ly imply a significant clinical difference. It must be also highlightedhat, on opposite, the absence of statistical difference did not implyhe equivalence of the two treatments. The present modelling studyas not aimed at replacing RCTs which remain the best clini-
al evidence available. However, until RCTs specifically designedo address the outcomes of the two treatments in different sett-ngs, related to tumour size and liver function, are carried out, theresent analysis can provide useful informations to plan furtherrospective studies for cases in which both treatments can be cho-
en. In particular, the possibility to conduct an equivalence trialeems quite unrealistic, and the present analysis can suggests clin-cal scenarios in which such condition will be encountered. Therere some additional aspects that need specific discussion. The studyres (panel A, MELD = 7–8; panel B, MELD 9–10; panel C, MELD 11–12) and tumouration over a 5-year period. Confidence intervals were calculated at different tumoureir respective ranges.
was conducted on the basis of tumour size, number and MELD toreduce at minimum the complexity of the model. There are, how-ever, some other clinical features that can drive the choice towardsone treatment or the other. The degree of portal hypertension, thepresence of comorbidities, which can represent contraindicationsto surgery, and the location of the tumour were not included inthe model. While the presence of comorbidities is likely capturedfrom the present age-adjustment, the remaining features probablyneed to be further investigated. In particular, portal hyperten-sion as a contraindication for surgery is still a matter of debate[33,34] and dedicated comparative studies of the two treatmentsfocused in patients with this feature should better clarify the role ofeach therapy. Location of the tumour represents another potentialconfounding variable that was not included in the present model.Even if in the present study an accurate assessment of the tumourdeep was not performed, this feature is probably already reflectedby the treatment choice, making present results consistent forpatients in whom both treatments could be adopted [35]; however,this is probably another aspect that needs dedicated studies.
In conclusion, we observed that the superiority, or a possibleequivalence, of resection and/or ablation in the treatment of HCCis modified by the relationship existing between tumour number,size, and the degree of liver dysfunction. For patients with a sin-gle tumour <2 cm and very well-preserved liver function, the twoprocedures seem to provide similar results whereas, for tumoursof 3–5 cm, resection can be a preferable option. The benefit obtain-able from surgery in comparison to ablation is reduced for more
advanced degrees of liver dysfunction. For single tumours of 2–3 cmand for multiple tumours, the two therapies provide oppositeresults in relation to the degree of liver dysfunction. The presentresults suggest that further studies should be focused on specific
nd Liv
cTta
CN
A
E
A
t
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[sis: surgical perspectives out of EASL/AASLD guidelines. European Journal of
A. Cucchetti et al. / Digestive a
ategories of tumour burden and the severity of liver dysfunction.he role of other clinical factors, such as portal hypertension and/orhe location of the tumour, has also to be considered in dedicatednalyses.
onflict of interesto conflict of interest exists.
cknowledgement
The study was supported in part by a grant from the Region ofmilia Romagna.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at http://dx.doi.org/10.1016/j.dld.2013.10.015.
eferences
[1] El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gas-troenterology 2012;142:1264–73.
[2] Singal AG, Conjeevaram HS, Volk ML, et al. Effectiveness of hepatocellular carci-noma surveillance in patients with cirrhosis. Cancer Epidemiology, Biomarkers& Prevention 2012;21:793–9.
[3] Santi V, Trevisani F, Gramenzi A, et al. Semiannual surveillance is superior toannual surveillance for the detection of early hepatocellular carcinoma andpatient survival. Journal of Hepatology 2010;53:291–7.
[4] Chen MS, Li JQ, Zheng Y, et al. A prospective randomized trial comparing percu-taneous local ablative therapy and partial hepatectomy for small hepatocellularcarcinoma. Annals of Surgery 2006;243:321–8.
[5] Huang J, Yan L, Cheng Z, et al. A randomized trial comparing radiofrequencyablation and surgical resection for HCC conforming to the Milan criteria. Annalsof Surgery 2010;252:903–12.
[6] Feng K, Yan J, Li X, et al. A randomized controlled trial of radiofrequency abla-tion and surgical resection in the treatment of small hepatocellular carcinoma.Journal of Hepatology 2012;57:794–802.
[7] Hung HH, Chiou YY, Hsia CY, et al. Survival rates are comparable after radiofre-quency ablation or surgery in patients with small hepatocellular carcinomas.Clinical Gastroenterology and Hepatology 2011;9:79–86.
[8] Takayama T, Makuuchi M, Hasegawa K. Single HCC smaller than 2 cm: surgeryor ablation? Surgeon’s perspective. Journal of Hepatobiliary Pancreatic Surgery2010;17:422–4.
[9] Ueno S, Sakoda M, Kubo F, et al. Surgical resection versus radiofrequency abla-tion for small hepatocellular carcinomas within the Milan criteria. Journal ofHepatobiliary Pancreatic Surgery 2009;16:359–66.
10] Nishikawa H, Inuzuka T, Takeda H, et al. Comparison of percutaneous radiofre-quency thermal ablation and surgical resection for small hepatocellularcarcinoma. BMC Gastroenterology 2011;11:143.
11] Guglielmi A, Ruzzenente A, Valdegamberi A, et al. Radiofrequency ablationversus surgical resection for the treatment of hepatocellular carcinoma in cir-rhosis. Journal of Gastrointestinal Surgery 2008;12:192–8.
12] Vivarelli M, Guglielmi A, Ruzzenente A, et al. Surgical resection versus percu-taneous radiofrequency ablation in the treatment of hepatocellular carcinomaon cirrhotic liver. Annals of Surgery 2004;240:102–7.
13] Hasegawa K, Makuuchi M, Takayama T, et al. Surgical resection vs. percu-
taneous ablation for hepatocellular carcinoma: a preliminary report of theJapanese nationwide survey. Journal of Hepatology 2008;49:589–94.14] Abu-Hilal M, Primrose JN, Casaril A, et al. Surgical resection versus radiofre-quency ablation in the treatment of small unifocal hepatocellular carcinoma.Journal of Gastrointestinal Surgery 2008;12:1521–6.
[
er Disease 46 (2014) 257–263 263
15] Montorsi M, Santambrogio R, Bianchi P, et al. Survival and recurrencesafter hepatic resection or radiofrequency for hepatocellular carcinoma in cir-rhotic patients: a multivariate analysis. Journal of Gastrointestinal Surgery2005;9:62–7.
16] Hong SN, Lee SY, Choi MS, et al. Comparing the outcomes of radiofrequencyablation and surgery in patients with a single small hepatocellular carci-noma and well-preserved hepatic function. Journal of Clinical Gastroenterology2005;39:247–52.
17] Cucchetti A, Piscaglia F, Cescon M, et al. Conditional survival after hepaticresection for hepatocellular carcinoma in cirrhotic patients. Clinical CancerResearch 2012;18:4397–405.
18] Cescon M, Colecchia A, Cucchetti A, et al. Value of transient elastographymeasured with FibroScan in predicting the outcome of hepatic resection forhepatocellular carcinoma. Annals of Surgery 2012;256:706–12.
19] European Association for the Study of the Liver; European Organisationfor Research and Treatment of Cancer. EASL-EORTC clinical practice guide-lines: management of hepatocellular carcinoma. Journal of Hepatology2012;56:908–43.
20] Bruix J, Sherman M, Llovet JM, et al. European Association for the Studyof the Liver. Clinical management of hepatocellular carcinoma. Conclusionsof the Barcelona-2000 EASL conference. Journal of Hepatology 2001;35:421–30.
21] Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib inpatients in the Asia-Pacific region with advanced hepatocellular carcinoma: aphase III randomised, double-blind, placebo-controlled trial. Lancet Oncology2009;10:25–34.
22] Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellularcarcinoma. New England Journal of Medicine 2008;359:378–90.
23] Wilson DB. Practical meta-analysis. California: George Mason University/SAGEPublications Inc.; 2001.
24] Wiesner R, Edwards E, Freeman R, et al. Model for end-stage liver dis-ease (MELD) and allocation of donor livers. Gastroenterology 2003;124:91–6.
25] Salerno F, Merli M, Cazzaniga M, et al. MELD score is better than Child–Pughscore in predicting 3-month survival of patients undergoing transjugular intra-hepatic portosystemic shunt. Journal of Hepatology 2002;36:494–500.
26] Huo TI, Wu JC, Lin HC, et al. Evaluation of the increase in model for end-stageliver disease (delta MELD) score over time as a prognostic predictor in patientswith advanced cirrhosis: risk factor analysis and comparison with initial MELDand Child–Turcotte–Pugh score. Journal of Hepatology 2005;42:826–32.
27] Beck JR, Pauker SG, Gottlieb JE, et al. A convenient approximation of lifeexpectancy (the “DEALE”). II. Use in medical decision-making. American Journalof Medicine 1982;73:889–97.
28] Italian National Institute of Statistics (ISTAT). Mortality tables; 2012. Availableat: http://demo.istat.it/ [accessed December 2012].
29] Laupacis A, Sackett DL, Roberts RS. An assessment of clinically useful meas-ures of the consequences of treatment. New England Journal of Medicine1988;318:1728–33.
30] Cook RJ, Sackett DL. The number needed to treat: a clinically useful measure oftreatment effect. British Medical Journal 1995;310:452–4.
31] Kudo M. Real practice of hepatocellular carcinoma in Japan: conclusions of theJapan Society of Hepatology 2009 Kobe Congress. Oncology 2010;78(Suppl.1):180–8.
32] Majno PE, Mentha G, Mazzaferro V. Partial hepatectomy versus radiofrequencyablation for hepatocellular carcinoma: confirming the trial that will neverbe, and some comments on the indications for liver resection. Hepatology2010;51:1116–8.
33] Ishizawa T, Hasegawa K, Aoki T, et al. Neither multiple tumors nor portalhypertension are surgical contraindications for hepatocellular carcinoma. Gas-troenterology 2008;134:1908–16.
34] Capussotti L, Ferrero A, Viganò L, et al. Liver resection for HCC with cirrho-
Surgical Oncology 2009;35:11–5.35] Cucchetti A, Piscaglia F, Cescon M, et al. Systematic review of surgical resection
vs. radiofrequency ablation for hepatocellular carcinoma. World Journal of Gas-troenterology 2013;19:4106–18.