Embed Size (px)
Citation preview

An Idea for a Mid to Long Term Strategy for Pradaxa
Background – Experience after the Pradaxa SPAF Launch
Confidential - Internal use only 2
• Patients on older OACs are accustomed to and many appear to like and expect frequent
interactions with the Health Care system and its staff
• Switches from older OACs to NOACs are uncommon in the marketplace
• Most new AF patients still are prescribed an older OAC
• Prescribers often want to know the extent of anticoagulation each patient is receiving via their
current anticoagulant
• External experts and the media have expressed concerns about a “one size fits all” OAC, since dose
adjusted OACs may have optimized outcomes
• Xarelto competes effectively against Pradaxa despite inferior ROCKET data
• Eliquis is perceived to have the best outcomes data of all NOACs
• FDA has indicated that only path towards approval of 110 mg dose would be Modeling &
Simulation results followed by a PK/PD study
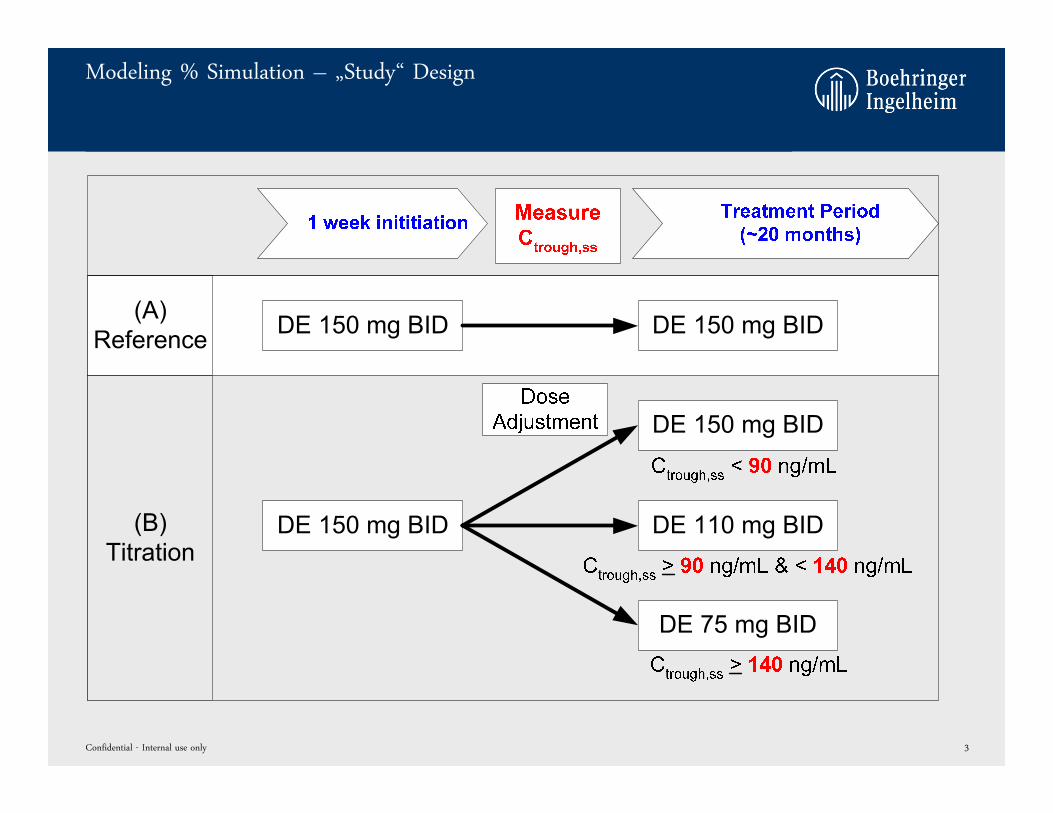
Modeling % Simulation – „Study“ Design
Confidential - Internal use only 3
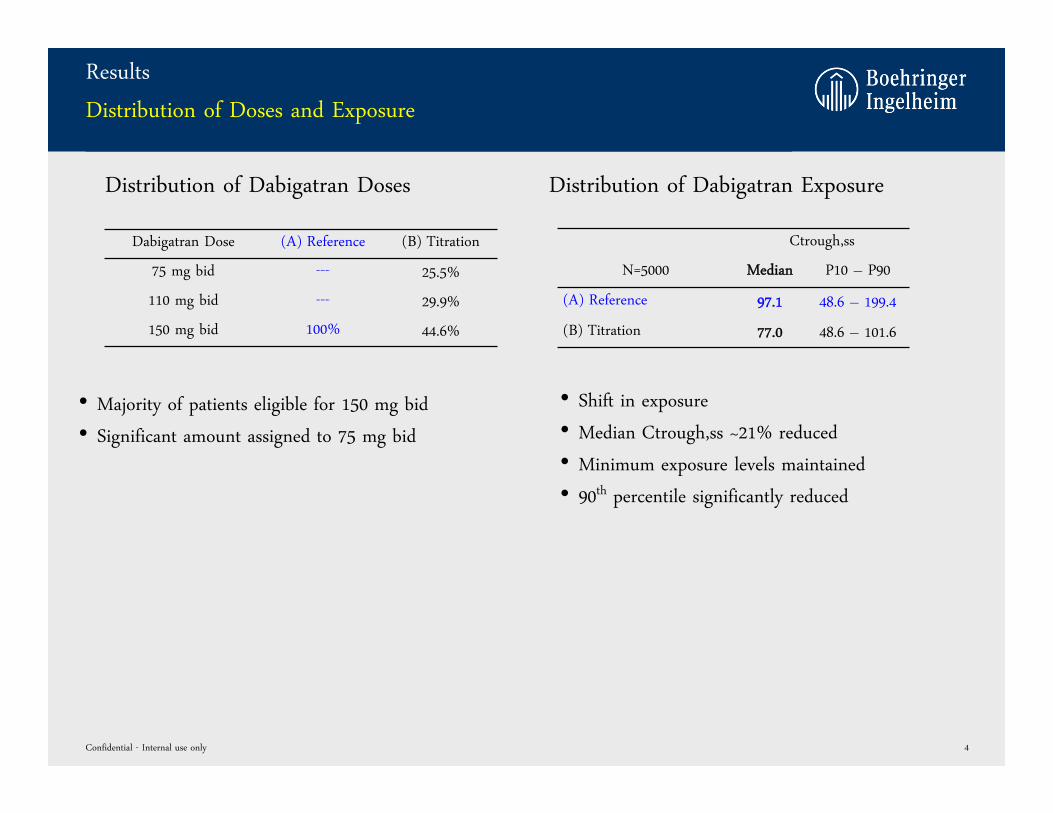
Results
Distribution of Doses and Exposure
Dabigatran Dose (A) Reference (B) Titration
75 mg bid --- 25.5%
110 mg bid --- 29.9%
150 mg bid 100% 44.6%
Confidential - Internal use only 4
• Majority of patients eligible for 150 mg bid
• Significant amount assigned to 75 mg bid
Ctrough,ss
N=5000 Median P10 – P90
(A) Reference 97.1 48.6 – 199.4
(B) Titration 77.0 48.6 – 101.6
• Shift in exposure
• Median Ctrough,ss ~21% reduced
• Minimum exposure levels maintained
• 90th percentile significantly reduced
Distribution of Dabigatran Doses Distribution of Dabigatran Exposure
Results
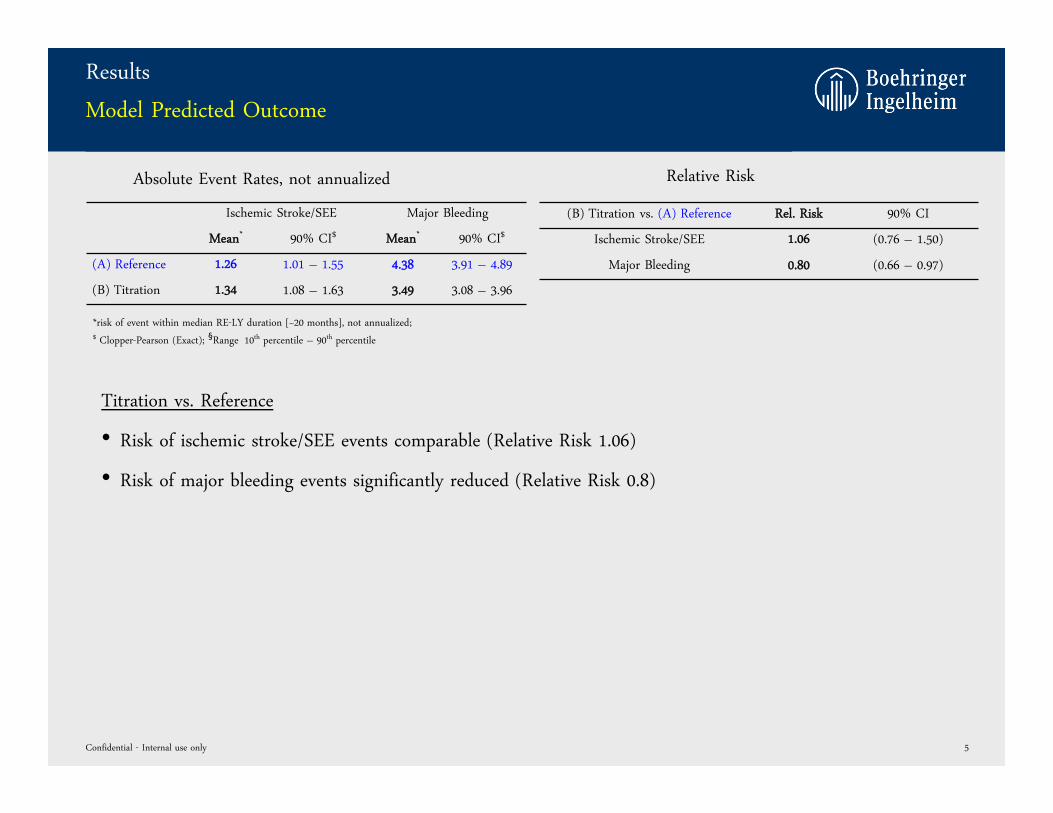
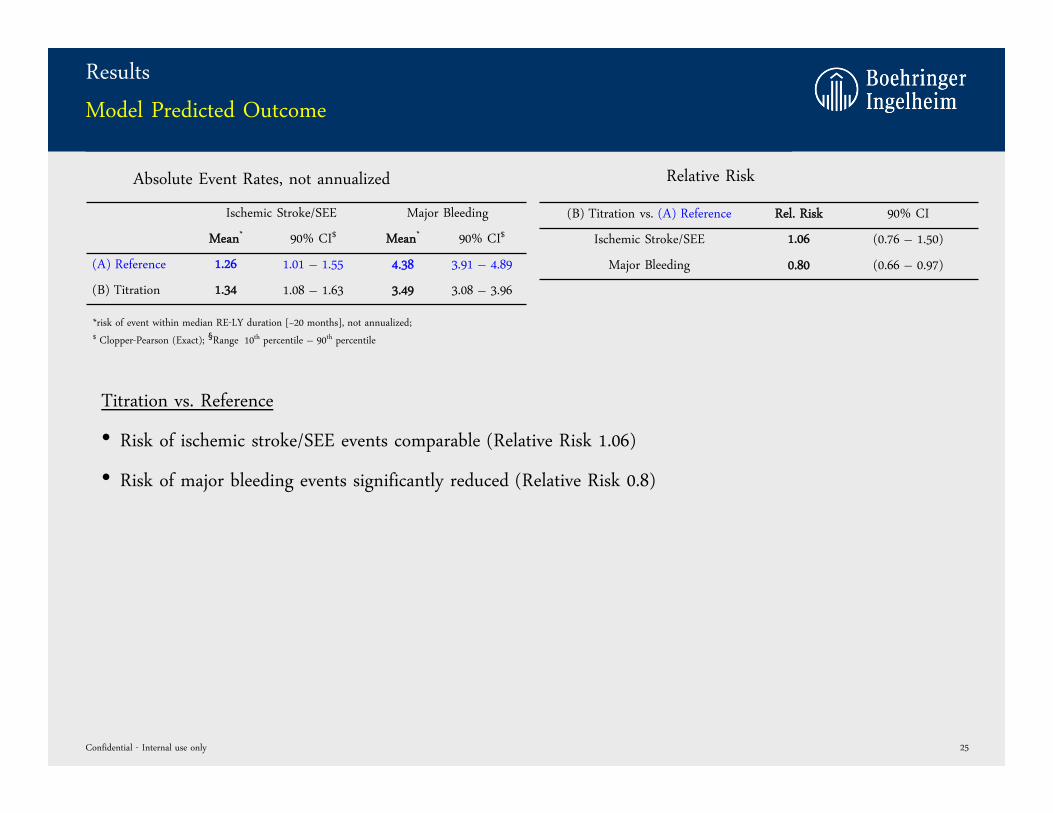
Model Predicted Outcome
Ischemic Stroke/SEE Major Bleeding
Mean* 90% CI$ Mean* 90% CI$
(A) Reference 1.26 1.01 – 1.55 4.38 3.91 – 4.89
(B) Titration 1.34 1.08 – 1.63 3.49 3.08 – 3.96
Confidential - Internal use only 5
*risk of event within median RE-LY duration [~20 months], not annualized; $ Clopper-Pearson (Exact); §Range 10th percentile – 90th percentile
Titration vs. Reference
• Risk of ischemic stroke/SEE events comparable (Relative Risk 1.06)
• Risk of major bleeding events significantly reduced (Relative Risk 0.8)
Absolute Event Rates, not annualized
(B) Titration vs. (A) Reference Rel. Risk 90% CI
Ischemic Stroke/SEE 1.06 (0.76 – 1.50)
Major Bleeding 0.80 (0.66 – 0.97)
Relative Risk
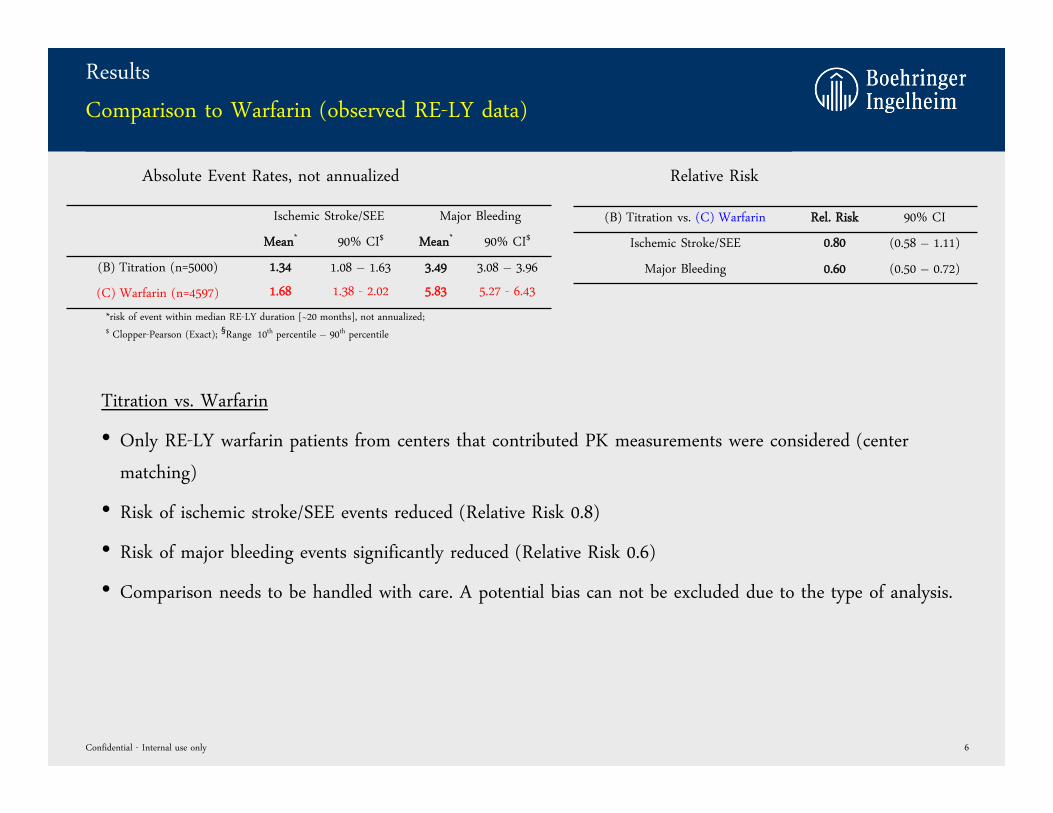
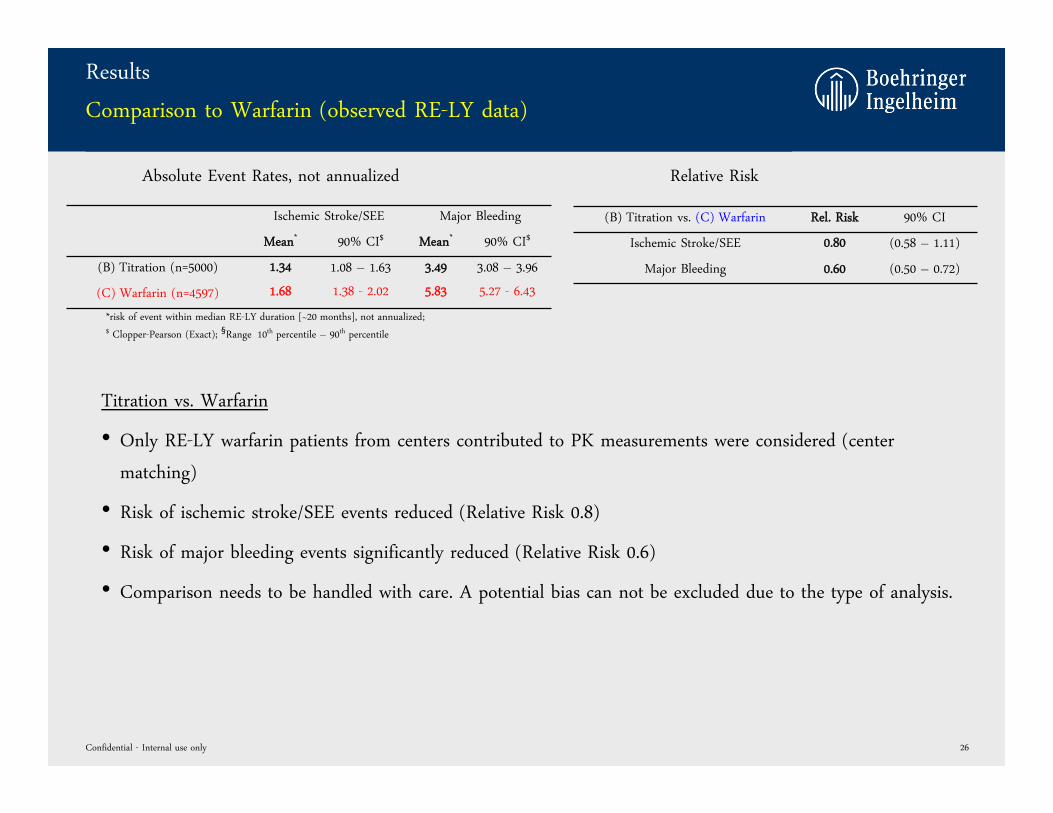
Results
Comparison to Warfarin (observed RE-LY data)
Ischemic Stroke/SEE Major Bleeding
Mean* 90% CI$ Mean* 90% CI$
(B) Titration (n=5000) 1.34 1.08 – 1.63 3.49 3.08 – 3.96
(C) Warfarin (n=4597) 1.68 1.38 - 2.02 5.83 5.27 - 6.43
Confidential - Internal use only 6
*risk of event within median RE-LY duration [~20 months], not annualized; $ Clopper-Pearson (Exact); §Range 10th percentile – 90th percentile
(B) Titration vs. (C) Warfarin Rel. Risk 90% CI
Ischemic Stroke/SEE 0.80 (0.58 – 1.11)
Major Bleeding 0.60 (0.50 – 0.72)
Relative RiskAbsolute Event Rates, not annualized
Titration vs. Warfarin
• Only RE-LY warfarin patients from centers that contributed PK measurements were considered (center
matching)
• Risk of ischemic stroke/SEE events reduced (Relative Risk 0.8)
• Risk of major bleeding events significantly reduced (Relative Risk 0.6)
• Comparison needs to be handled with care. A potential bias can not be excluded due to the type of analysis.
COMPARISON OF OBSERVED DABIGATRAN VS. OBSERVED
WARFARIN OUTCOMES FROM RE-LY
Impact of Dabigatran Dose Adjustment on Clinical Outcome in AF Patients
Confidential - Internal use only 7
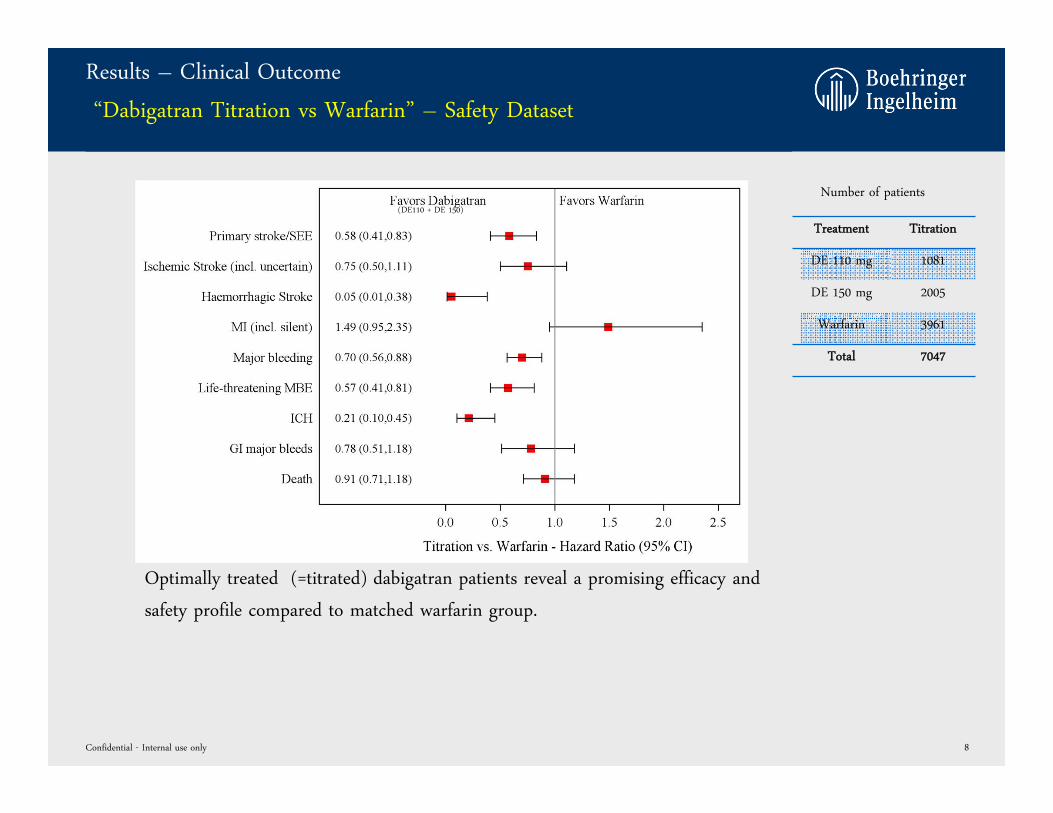
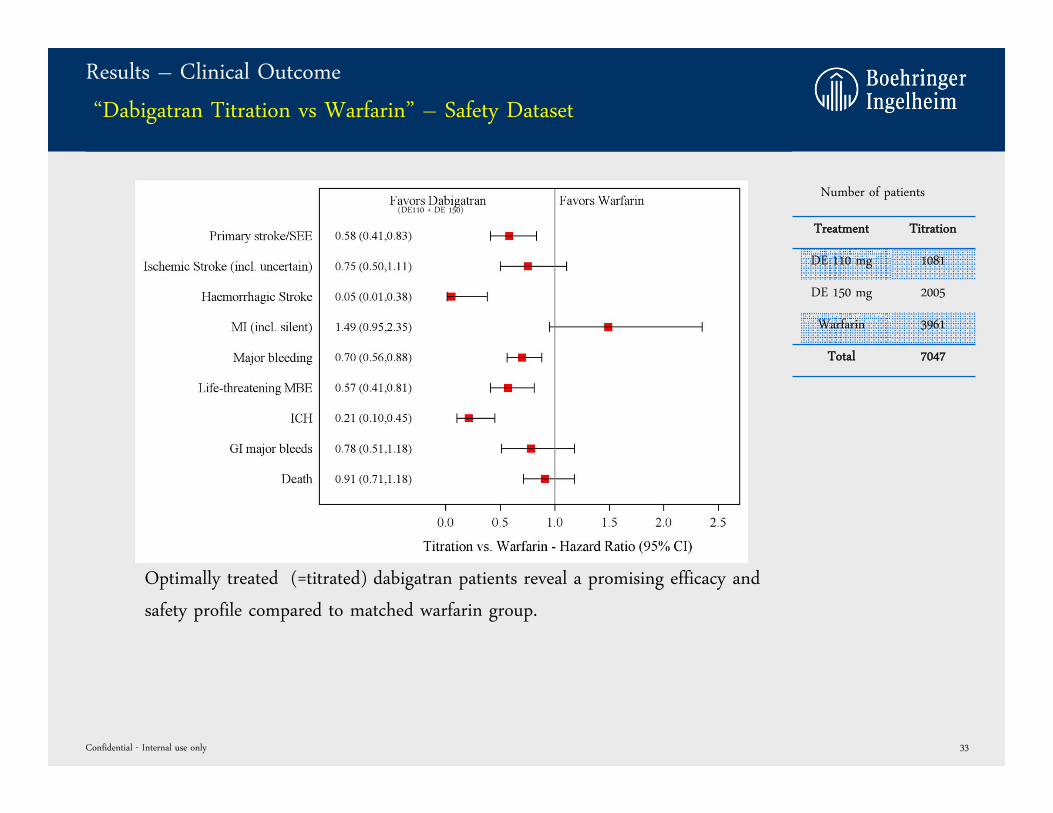
Results – Clinical Outcome
“Dabigatran Titration vs Warfarin” – Safety Dataset
Confidential - Internal use only 8
Treatment Titration
DE 110 mg 1081
DE 150 mg 2005
Warfarin 3961
Total 7047
Number of patients(DE110 + DE 150)
Optimally treated (=titrated) dabigatran patients reveal a promising efficacy and
safety profile compared to matched warfarin group.
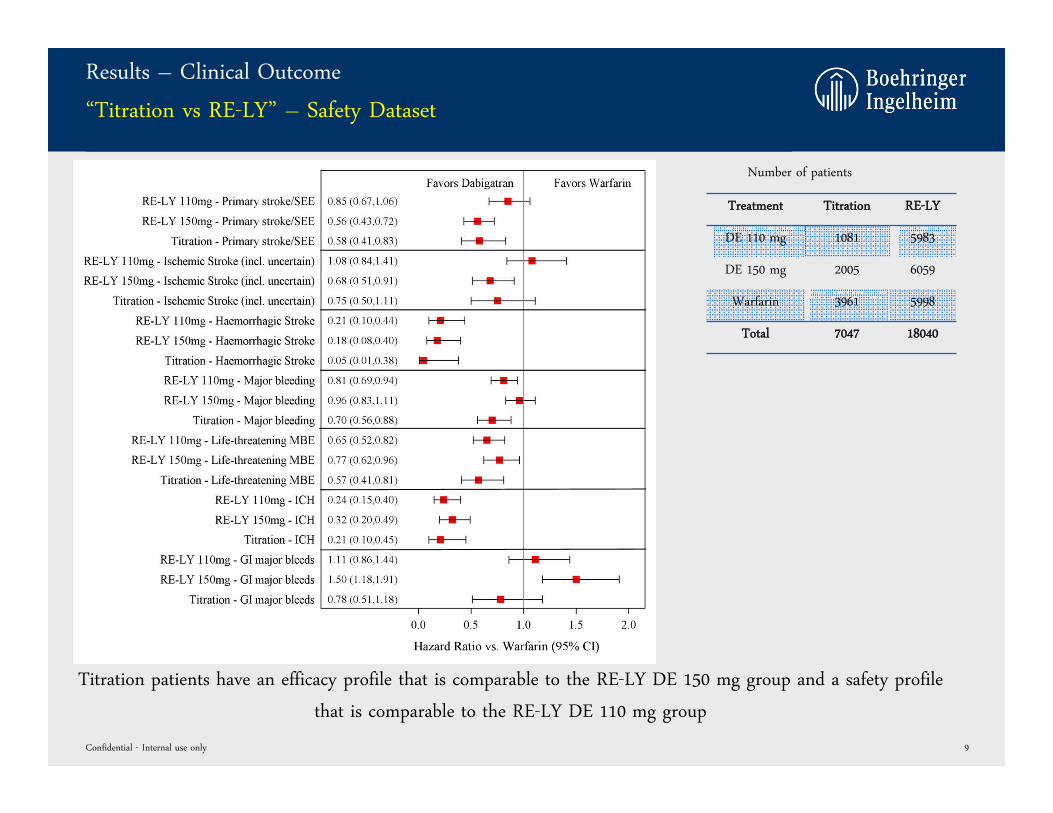
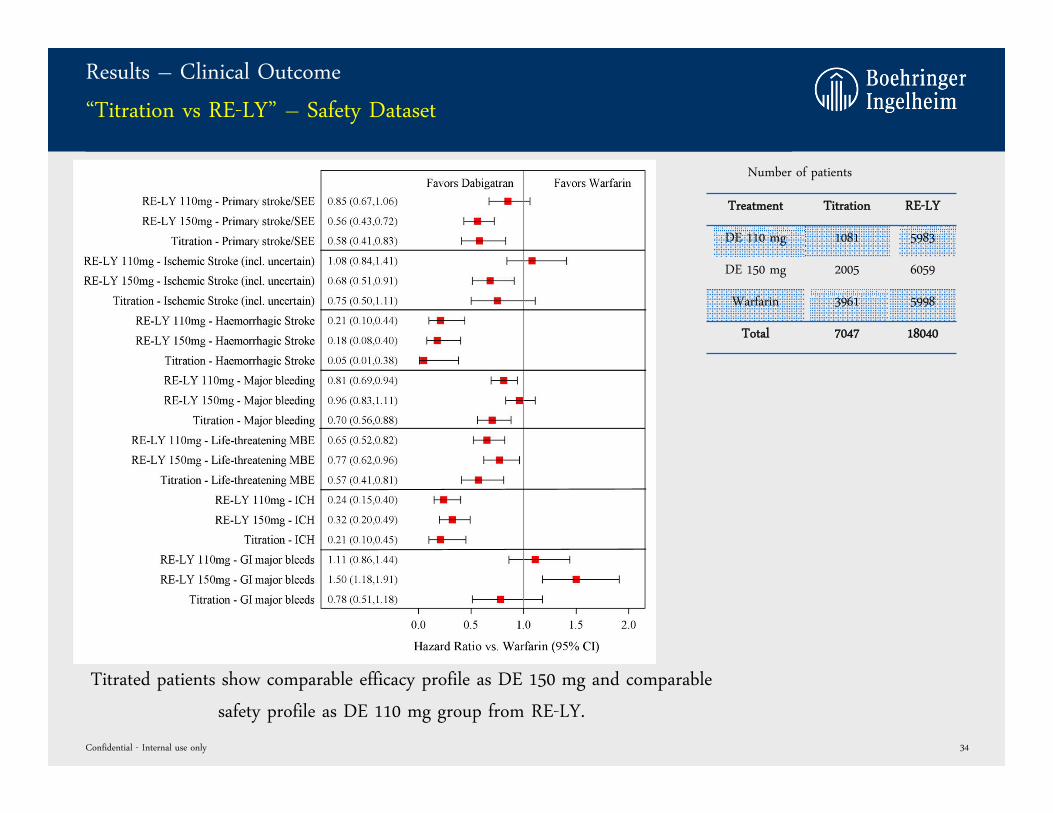
Results – Clinical Outcome
“Titration vs RE-LY” – Safety Dataset
Confidential - Internal use only 9
Treatment Titration RE-LY
DE 110 mg 1081 5983
DE 150 mg 2005 6059
Warfarin 3961 5998
Total 7047 18040
Number of patients
Titration patients have an efficacy profile that is comparable to the RE-LY DE 150 mg group and a safety profile
that is comparable to the RE-LY DE 110 mg group
Potential Mid to Long Term Strategy
• Discuss Modeling & Simulation data with FDA and explore potential path forward to approval of
such an approach:
• PK/PD study only acceptable?
• Trial with bleeding endpoints required?
• “Real world trial” using electronic health records of titration strategy as alternative? (e.g.
within regulated system such as KP which would be more feasible than “RE-LY 2” from a
budget and timeline perspective)
• Explore timing of such results compared to that of (1) globally available lab test, (2) a point of care
testing device, and (3) the Pradaxa antidote
If data acceptable to regulators: Re-Launch Pradaxa with titration strategy (resulting in significantly
fewer strokes and significantly fewer bleeding events compared to warfarin), Point of Care testing
device and availability of Antidote
Confidential - Internal use only 10
Open Questions
• Would we exclude patients from Pradaxa use in AF because of insufficient exposure?
• If yes, which percentage of the overall population would be excluded?
• Given a ≈40% intra-individual variability of DE concentrations, can a simple titration regimen be designed
with a low need for multiple titrations?
• Will some of the assumptions change over time with more familiarity in the Marketplace on NOACs without
the need for titration?
• Which extent of new data would be needed to reflect a titration strategy in the label (including differences
between countries)?
• Would this strategy endanger the superiority label vs. warfarin?
• What would be the implication of such a strategy for indications other than SPAF?
Confidential - Internal use only 11
Potential Mid to Long Term Strategy - Alternative
• BI has been approached by Astra Zeneca about a potential co-development and co-promotion of
their Direct Thrombin Inhibitor which is about to enter Phase III
• The AZ approach (received after the titration idea was developed at BI) is very similar to the
aforementioned potential BI strategy:
• Titration of dose, e.g. one week after first dosing
• Have specific lab test available at time of launch
• Have reversal agent available at time of launch
• AZ DTI is expected to be a once-daily therapy with low peak to trough ratio (exposure testing
potentially independent of timing of last dose) and low intra-individual variability
Confidential - Internal use only 12
Proposed Concrete Next Steps
1. Prepare meeting request and discuss Modeling data as well as potential PK/PD study with FDA
2. Conduct Market Research to test potential acceptance of titration strategy in Marketplace
3. Develop models assessing cost sensitivity to payers under different assumptions
4. Conduct Challenge Meeting to further define Pros and Cons of titration strategy including
MAPOR, Regulatory, Marketing, Medicine, IPM, etc.
5. Have VC with Astra Zeneca after US label of apixaban is available to further exchange thoughts
on a potential collaboration
Confidential - Internal use only 13
BACKUPs
Confidential - Internal use only 14
A Clinical Trial Simulation Analysis
May 08, 2012
Impact of Dabigatran Dose Adjustment on Clinical
Outcome in AF Patients
Objectives
• Evaluate the impact of dose adjustment (=“titration”) on clinical outcome in AF patients by clinical
trial simulations.
• Dose adjustment to 75, 110 and 150 mg BID based on trough concentration at steady-state
(Ctrough,ss) observed after one week dosing with DE 150 mg BID.
• Identification of optimal cut-off concentrations for dose adjustment.
• Comparison to warfarin data
Confidential - Internal use only 16
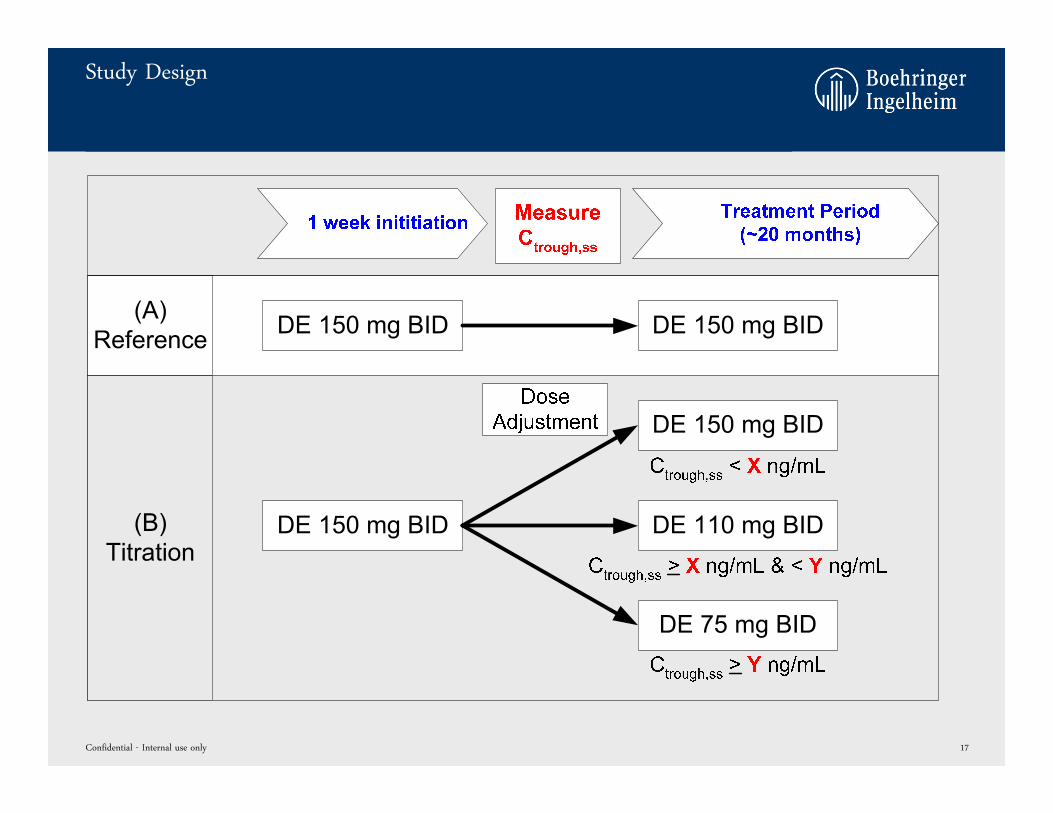
Study Design
Confidential - Internal use only 17
Methods
• Cut-off values between 0 ng/mL and 250 ng/mL (step size 10 ng/mL) were evaluated to identify
optimal cut-off concentrations for dose adjustment, resulting in 352 different combinations.
• 500 clinical trials with 5000 patients each were simulated for each of the 352 cut-off combinations.
• Patient characteristics were bootstrapped from RE-LY database.
• Ctrough,ss, ischemic stroke/SEE and major bleeding event rates were calculated.
Confidential - Internal use only 18
0 10 20 30 40 50 60 70 80 90 100
110
120
130
140
150
160
170
180
190
200
210
220
230
240
250
0102030405060708090
100110120130140150160170180190200210220230240250
-35.0 -32.5 -30.0 -27.5 -25.0 -22.5 -20.0 -17.5 -15.0 -12.5 -10.0 -7.5 -5.0 -2.5 0.0
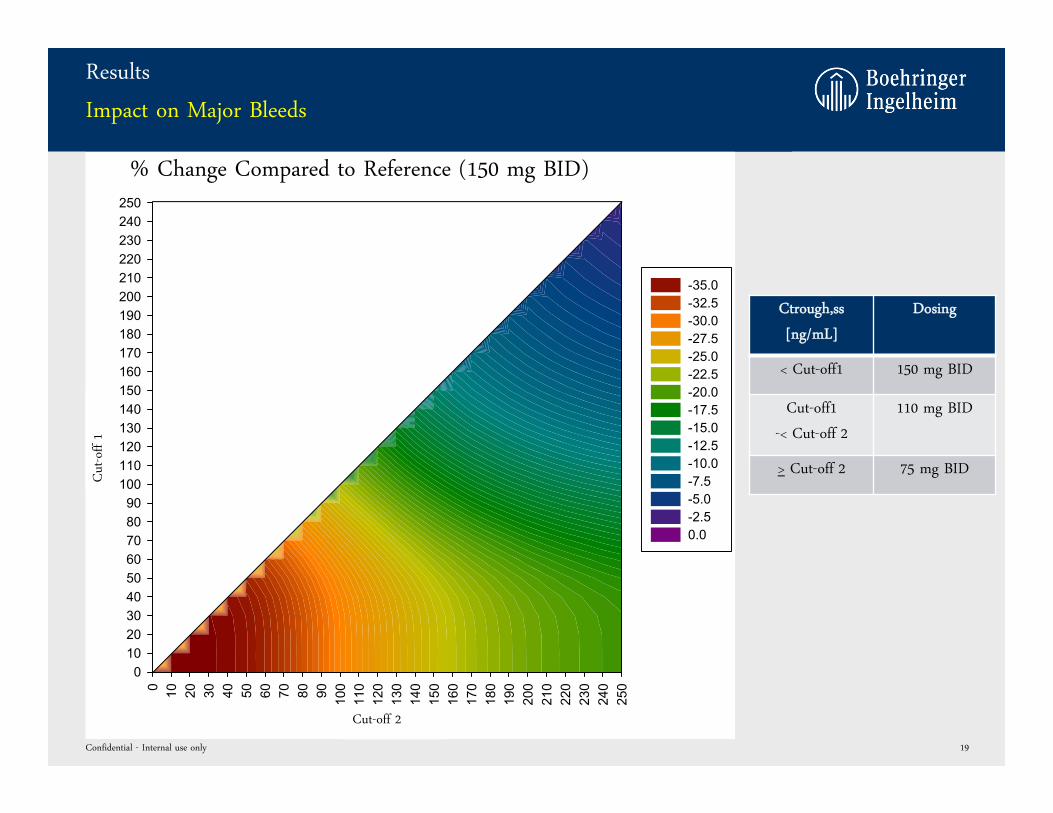
Results
Impact on Major Bleeds
Confidential - Internal use only 19
Cut-off 2
Cut
-off
1
% Change Compared to Reference (150 mg BID)
Ctrough,ss
[ng/mL]
Dosing
< Cut-off1 150 mg BID
Cut-off1
-< Cut-off 2
110 mg BID
> Cut-off 2 75 mg BID
0 10 20 30 40 50 60 70 80 90 100
110
120
130
140
150
160
170
180
190
200
210
220
230
240
250
0102030405060708090
100110120130140150160170180190200210220230240250
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5
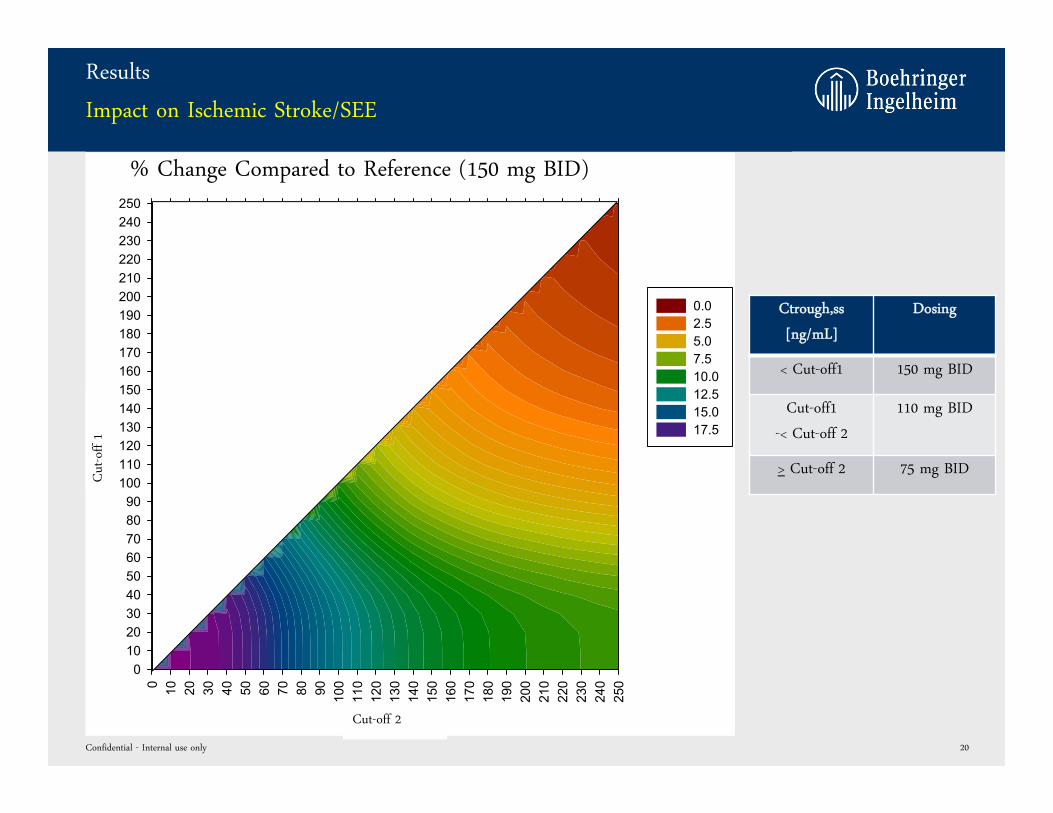
Results
Impact on Ischemic Stroke/SEE
Confidential - Internal use only 20
Cut-off 2
Cut
-off
1
% Change Compared to Reference (150 mg BID)
Ctrough,ss
[ng/mL]
Dosing
< Cut-off1 150 mg BID
Cut-off1
-< Cut-off 2
110 mg BID
> Cut-off 2 75 mg BID
0 10 20 30 40 50 60 70 80 90 100
110
120
130
140
150
160
170
180
190
200
210
220
230
240
250
0102030405060708090
100110120130140150160170180190200210220230240250
-6.0 -5.5 -5.0 -4.5 -4.0 -3.5 -3.0 -2.5 -2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0
Results
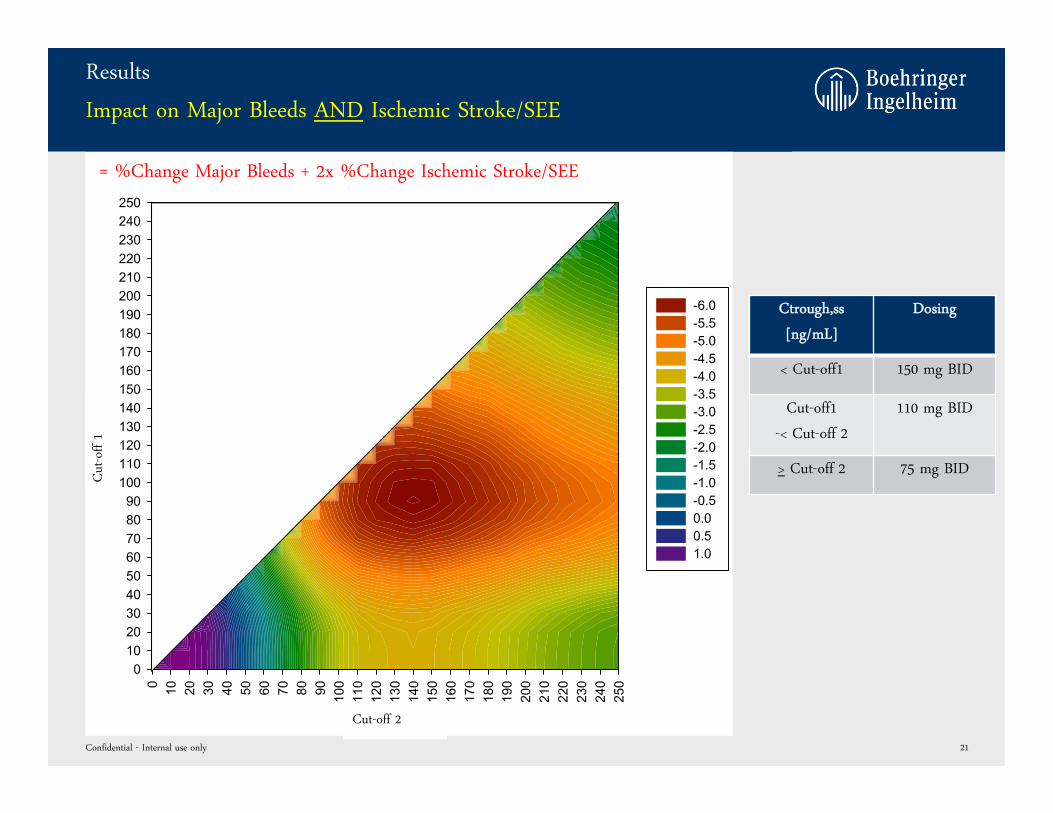
Impact on Major Bleeds AND Ischemic Stroke/SEE
Confidential - Internal use only 21
Cut-off 2
Cut
-off
1
Ctrough,ss
[ng/mL]
Dosing
< Cut-off1 150 mg BID
Cut-off1
-< Cut-off 2
110 mg BID
> Cut-off 2 75 mg BID
= %Change Major Bleeds + 2x %Change Ischemic Stroke/SEE
0 10 20 30 40 50 60 70 80 90 100
110
120
130
140
150
160
170
180
190
200
210
220
230
240
250
0102030405060708090
100110120130140150160170180190200210220230240250
-6.0 -5.5 -5.0 -4.5 -4.0 -3.5 -3.0 -2.5 -2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0
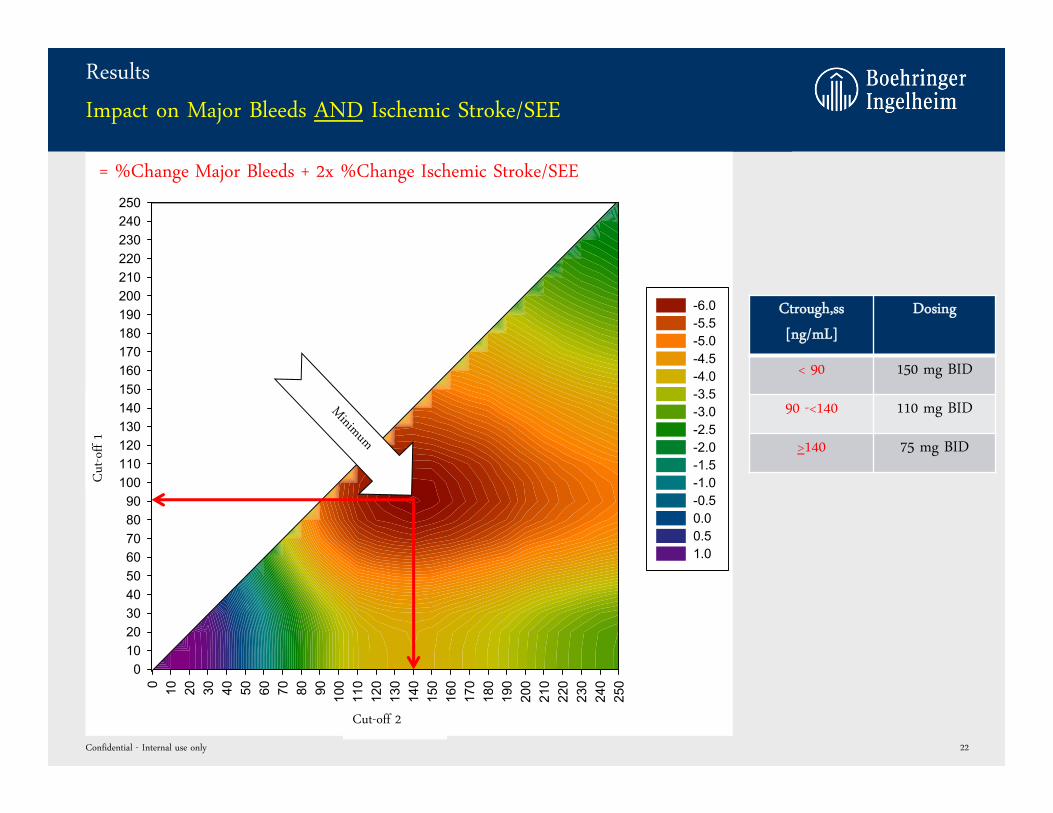
Results
Impact on Major Bleeds AND Ischemic Stroke/SEE
Confidential - Internal use only 22
Cut-off 2
Cut
-off
1
Ctrough,ss
[ng/mL]
Dosing
< 90 150 mg BID
90 -<140 110 mg BID
>140 75 mg BID
= %Change Major Bleeds + 2x %Change Ischemic Stroke/SEE
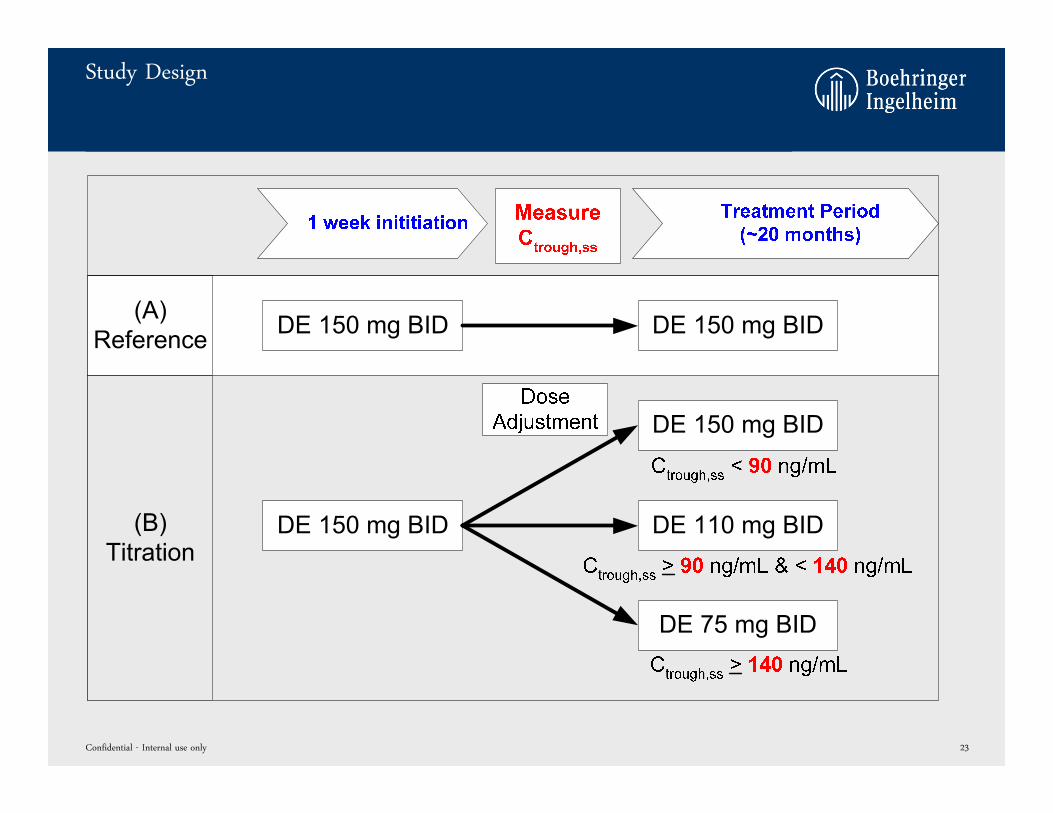
Study Design
Confidential - Internal use only 23
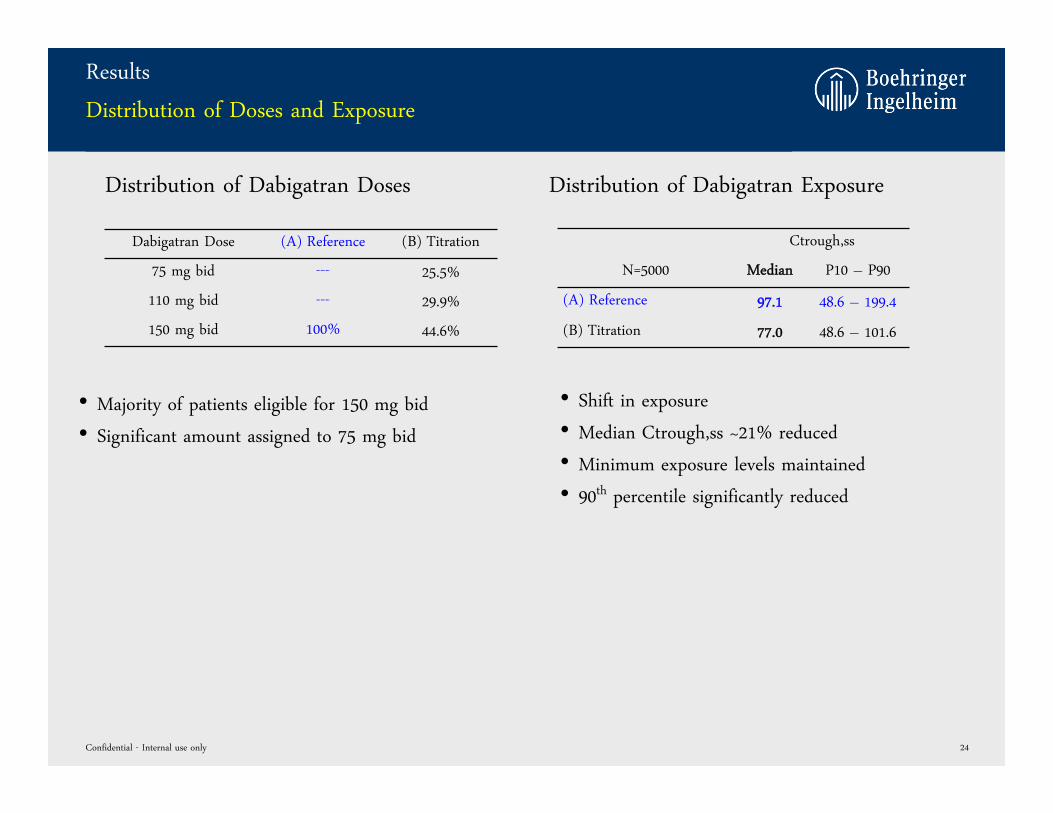
Results
Distribution of Doses and Exposure
Dabigatran Dose (A) Reference (B) Titration
75 mg bid --- 25.5%
110 mg bid --- 29.9%
150 mg bid 100% 44.6%
Confidential - Internal use only 24
• Majority of patients eligible for 150 mg bid
• Significant amount assigned to 75 mg bid
Ctrough,ss
N=5000 Median P10 – P90
(A) Reference 97.1 48.6 – 199.4
(B) Titration 77.0 48.6 – 101.6
• Shift in exposure
• Median Ctrough,ss ~21% reduced
• Minimum exposure levels maintained
• 90th percentile significantly reduced
Distribution of Dabigatran Doses Distribution of Dabigatran Exposure
Results
Model Predicted Outcome
Ischemic Stroke/SEE Major Bleeding
Mean* 90% CI$ Mean* 90% CI$
(A) Reference 1.26 1.01 – 1.55 4.38 3.91 – 4.89
(B) Titration 1.34 1.08 – 1.63 3.49 3.08 – 3.96
Confidential - Internal use only 25
*risk of event within median RE-LY duration [~20 months], not annualized; $ Clopper-Pearson (Exact); §Range 10th percentile – 90th percentile
Titration vs. Reference
• Risk of ischemic stroke/SEE events comparable (Relative Risk 1.06)
• Risk of major bleeding events significantly reduced (Relative Risk 0.8)
Absolute Event Rates, not annualized
(B) Titration vs. (A) Reference Rel. Risk 90% CI
Ischemic Stroke/SEE 1.06 (0.76 – 1.50)
Major Bleeding 0.80 (0.66 – 0.97)
Relative Risk
Results
Comparison to Warfarin (observed RE-LY data)
Ischemic Stroke/SEE Major Bleeding
Mean* 90% CI$ Mean* 90% CI$
(B) Titration (n=5000) 1.34 1.08 – 1.63 3.49 3.08 – 3.96
(C) Warfarin (n=4597) 1.68 1.38 - 2.02 5.83 5.27 - 6.43
Confidential - Internal use only 26
*risk of event within median RE-LY duration [~20 months], not annualized; $ Clopper-Pearson (Exact); §Range 10th percentile – 90th percentile
(B) Titration vs. (C) Warfarin Rel. Risk 90% CI
Ischemic Stroke/SEE 0.80 (0.58 – 1.11)
Major Bleeding 0.60 (0.50 – 0.72)
Relative RiskAbsolute Event Rates, not annualized
Titration vs. Warfarin
• Only RE-LY warfarin patients from centers contributed to PK measurements were considered (center
matching)
• Risk of ischemic stroke/SEE events reduced (Relative Risk 0.8)
• Risk of major bleeding events significantly reduced (Relative Risk 0.6)
• Comparison needs to be handled with care. A potential bias can not be excluded due to the type of analysis.
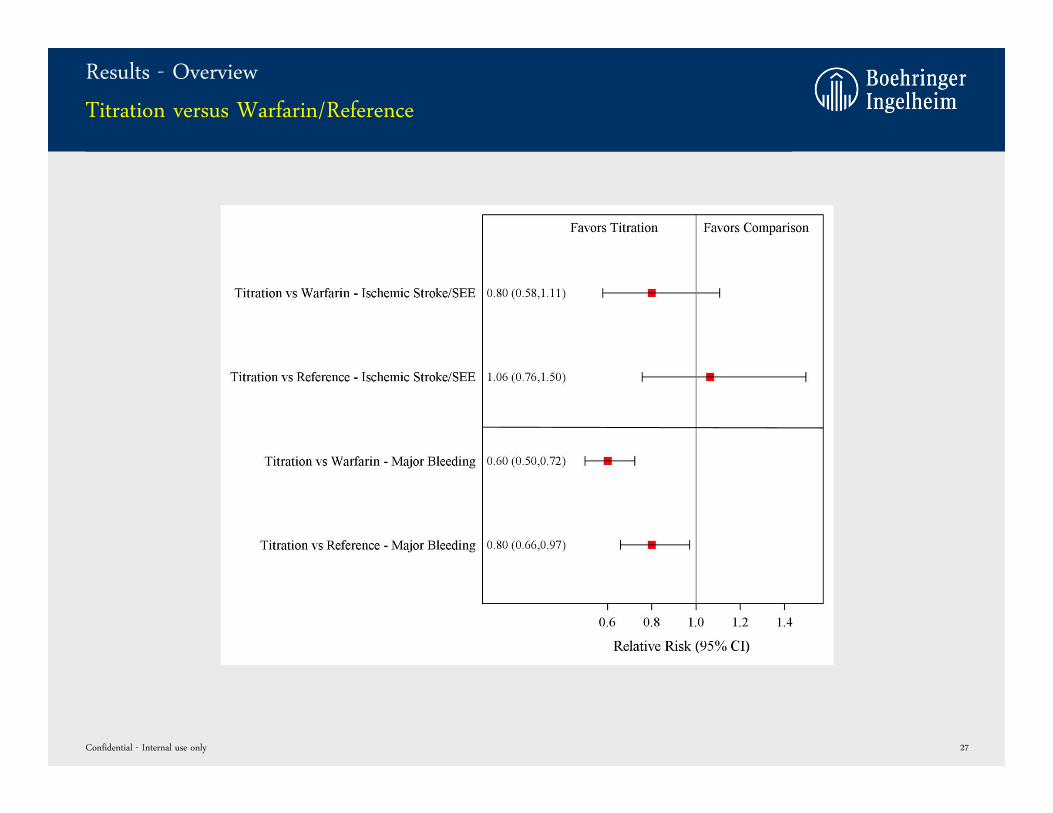
Results - Overview
Titration versus Warfarin/Reference
Confidential - Internal use only 27
Summary
Clinical Trial Simulation Analysis
• Extensive and comprehensive clinical trial simulation analyses were performed to investigate the impact of
dabigatran dose titration on the outcome in AF patients.
• Dabigatran Ctrough,ss values of 90 ng/mL and 140 ng/mL were identified as promising cut-off values to
assign dabigatran doses of 150 mg bid, 110 mg bid and 75 mg bid.
• Compared to a reference treatment (=DE 150 mg bid), dose adjustment showed a significant reduction of
major bleeding events (RR 0.8), while the ischemic stroke protection was maintained (RR 1.06).
• Compared to warfarin treatment, dose adjustment showed a significant reduction of ischemic stroke/SEE (RR
0.8) and major bleeding events (RR 0.6).
Confidential - Internal use only 28
COMPARISON OF OBSERVED DABIGATRAN VS. OBSERVED
WARFARIN OUTCOMES FROM RE-LY
Impact of Dabigatran Dose Adjustment on Clinical Outcome in AF Patients
Confidential - Internal use only 29
Background
• The comparison of the projected dabigatran versus the observed warfarin outcome is not considered as ideal
• Solution: Comparison of observed dabigatran versus observed warfarin outcomes from RE-LY in a matching
cohort
• Difficulty: Identification of the appropriate warfarin comparison group
• ~26% of dabigatran treated patients are expected to be assigned to the 75 mg bid dose and are
consequently not considerable for further analysis
• These patients are expected to be patients at higher risk for outcome events due to their demographic
characteristics
• It is therefore important to remove this population also from the warfarin group to ensure a fair
comparison between both groups
Confidential - Internal use only 30
Methods
1. All dabigatran treated patients from RE-LY with valid Ctrough,ss concentrations (n=8458) were assigned to their optimal
target dose (75, 110, 150), based on their measured trough concentrations in RE-LY assuming dose proportionality. If
more than 1 concentration was available, the median concentration was calculated.
2. A classification model was developed in dabigatran treated patients based on the propensity score method to identify
with baseline characteristics the patients assigned to “DE 75 mg bid” versus “not DE 75 mg bid”.
3. The developed classification model was applied to center matching warfarin patients from RE-LY to identify those
warfarin patients that are comparable to “optimal DE 75 mg” patients. Those patients were removed from the
comparison with the observed DE group.
4. Selection of patients for statistical comparison from RE-LY safety dataset
a) Dabigatran: only patients who were treated “optimally” based on their trough concentration were included (i.e.
predicted optimal dose = received dose in RE-LY)
b) Warfarin: only patients assigned to “not DE 75 mg bid” were included.
Confidential - Internal use only 31
Results
Database
• From the 8458 dabigatran treated RE-LY patients with valid Ctrough,ss values, 25.6%, 25.8% and 49.6% were
assigned to 75 mg, 110 mg and 150 mg bid as their “optimal” dose.
• From these 8458 patients, 3086 patients (36.5%) received the “optimal” dabigatran dose in RE-LY.
• A propensity score classification model was successfully developed.
• 1340 of 5301 center matching warfarin patients (25.3%) were identified as “75 mg patients” and excluded
• In depth comparison of patient characteristics of excluded dabigatran and excluded warfarin patients
showed no relevant difference in any of the relevant factors (e.g. CHADS2, CHADS VASc, HAS−BLED, age, etc.)
• Dabigatran and warfarin patients included in the analysis showed also no relevant difference in any of the
relevant patient characteristics
Confidential - Internal use only 32
Results – Clinical Outcome
“Dabigatran Titration vs Warfarin” – Safety Dataset
Confidential - Internal use only 33
Treatment Titration
DE 110 mg 1081
DE 150 mg 2005
Warfarin 3961
Total 7047
Number of patients(DE110 + DE 150)
Optimally treated (=titrated) dabigatran patients reveal a promising efficacy and
safety profile compared to matched warfarin group.
Results – Clinical Outcome
“Titration vs RE-LY” – Safety Dataset
Confidential - Internal use only 34
Treatment Titration RE-LY
DE 110 mg 1081 5983
DE 150 mg 2005 6059
Warfarin 3961 5998
Total 7047 18040
Number of patients
Titrated patients show comparable efficacy profile as DE 150 mg and comparable
safety profile as DE 110 mg group from RE-LY.
Summary
• A complex propensity score classification model was successfully developed and allowed a matched
warfarin comparison.
• Optimally treated (=titrated) dabigatran patients revealed a promising efficacy and safety profile
compared to matched warfarin group:
• Efficacy profile comparable to DE 150 mg group from RE-LY
• Safety profile comparable to DE 110 mg group from RE-LY
Confidential - Internal use only 35
Conclusion
• Comprehensive clinical trial simulation analyses identified promising cut-off values to assign optimal
dabigatran doses of 150, 110 and 75 mg bid.
• Optimally treated (=titrated) dabigatran patients revealed a promising efficacy and safety profile compared to
matched warfarin group.
• Future clinical studies might be required to confirm results.
• Dose titration based on exposure is a promising approach to significantly reduce major bleeding events while
maintaining the stroke protection in AF patients.
Confidential - Internal use only 36
backup
Confidential - Internal use only 37
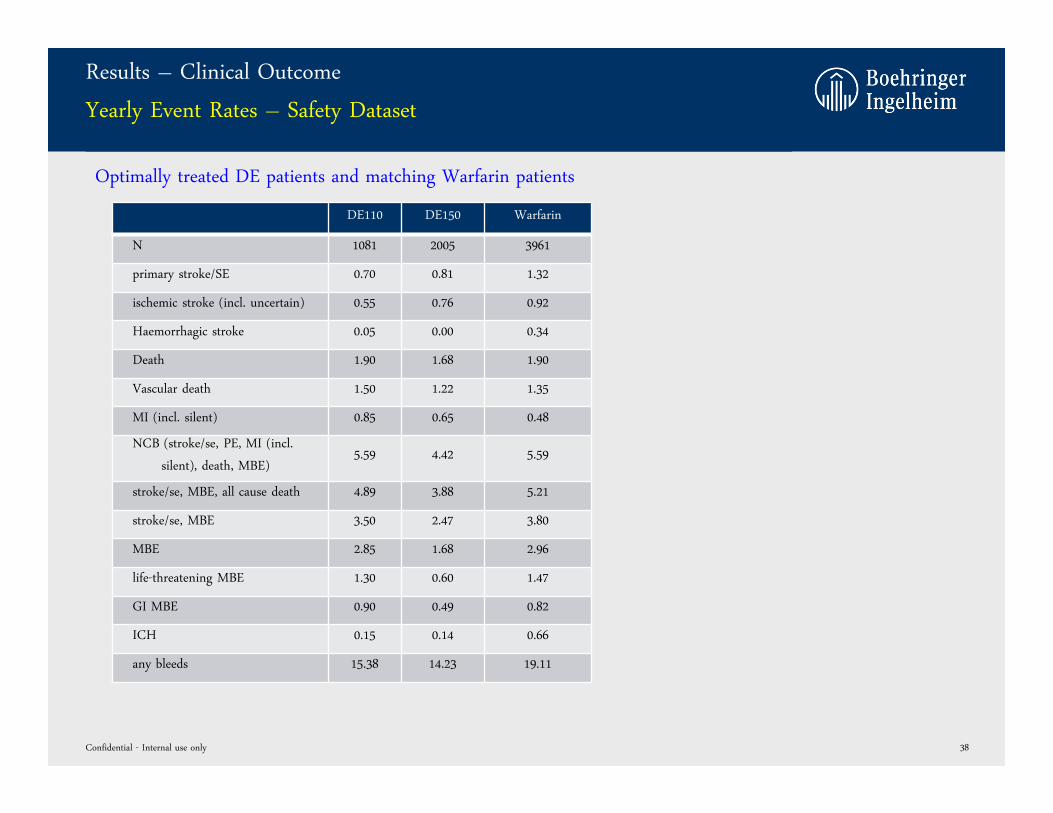
Results – Clinical Outcome
Yearly Event Rates – Safety Dataset
DE110 DE150 Warfarin
N 1081 2005 3961
primary stroke/SE 0.70 0.81 1.32
ischemic stroke (incl. uncertain) 0.55 0.76 0.92
Haemorrhagic stroke 0.05 0.00 0.34
Death 1.90 1.68 1.90
Vascular death 1.50 1.22 1.35
MI (incl. silent) 0.85 0.65 0.48
NCB (stroke/se, PE, MI (incl.
silent), death, MBE)5.59 4.42 5.59
stroke/se, MBE, all cause death 4.89 3.88 5.21
stroke/se, MBE 3.50 2.47 3.80
MBE 2.85 1.68 2.96
life-threatening MBE 1.30 0.60 1.47
GI MBE 0.90 0.49 0.82
ICH 0.15 0.14 0.66
any bleeds 15.38 14.23 19.11
Confidential - Internal use only 38
Optimally treated DE patients and matching Warfarin patients
Results - cut-off: 90 ng/mL and 140 ng/mL
Comparison to Warfarin (observed RE-LY data)
Confidential - Internal use only 39
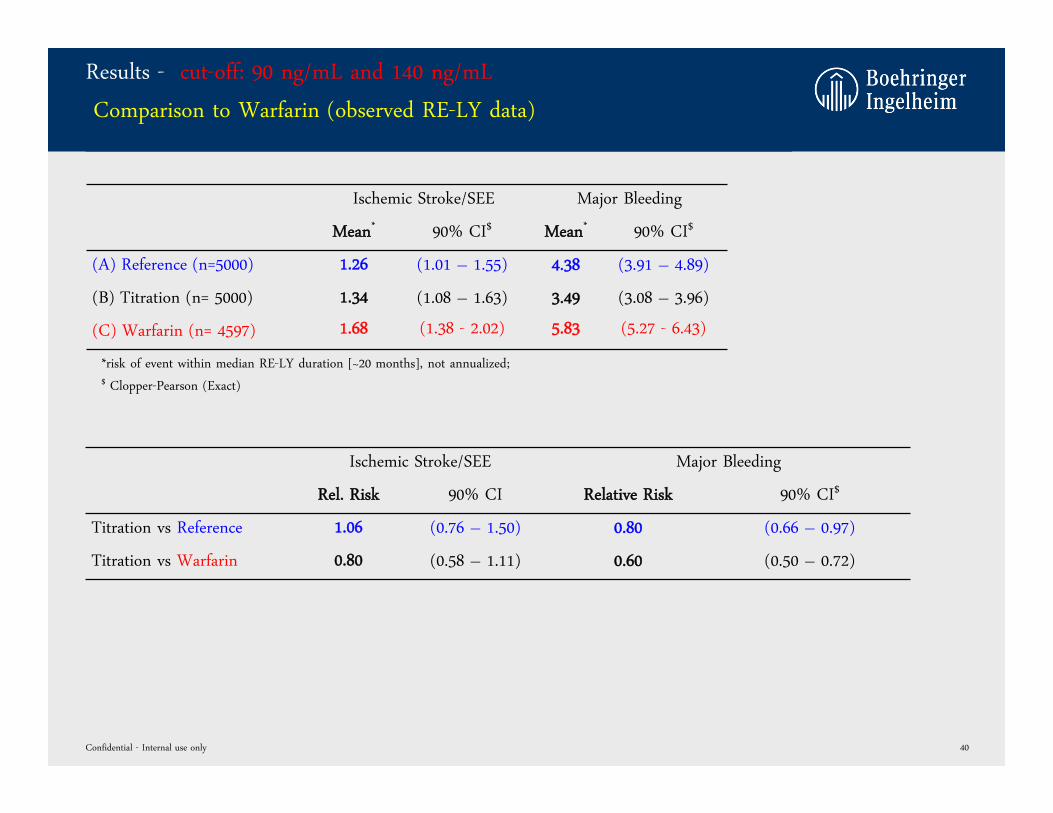
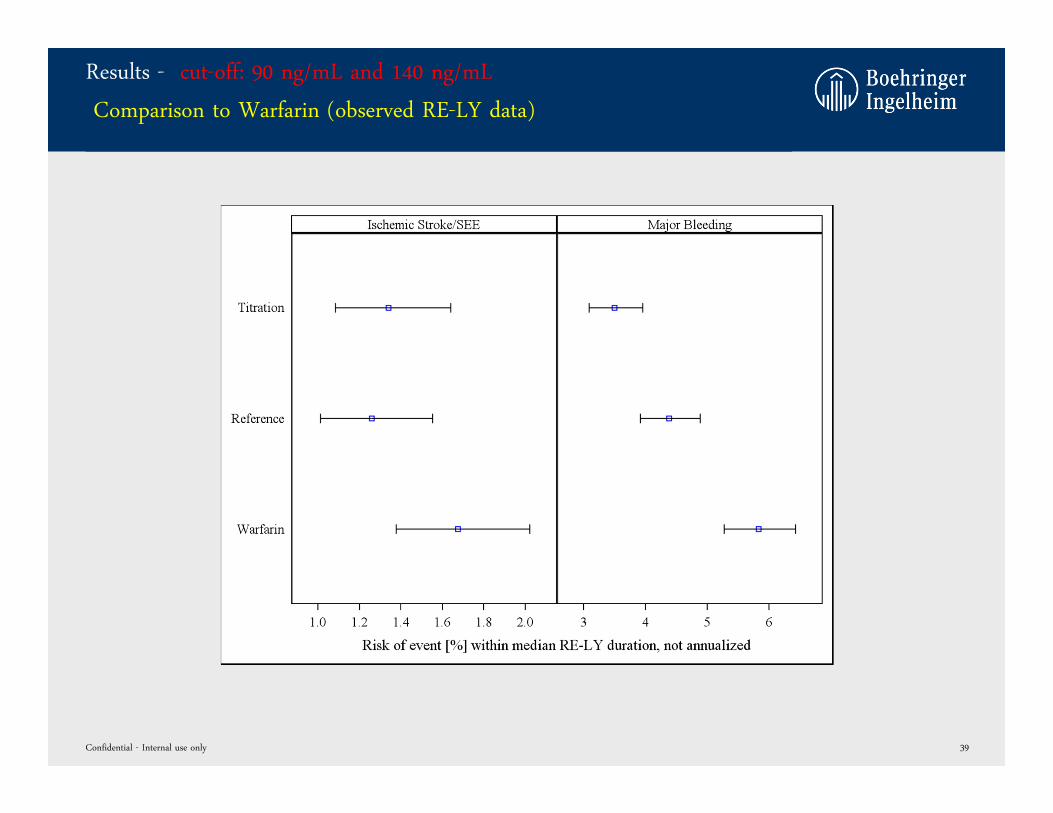
Results - cut-off: 90 ng/mL and 140 ng/mL
Comparison to Warfarin (observed RE-LY data)
Ischemic Stroke/SEE Major Bleeding
Mean* 90% CI$ Mean* 90% CI$
(A) Reference (n=5000) 1.26 (1.01 – 1.55) 4.38 (3.91 – 4.89)
(B) Titration (n= 5000) 1.34 (1.08 – 1.63) 3.49 (3.08 – 3.96)
(C) Warfarin (n= 4597) 1.68 (1.38 - 2.02) 5.83 (5.27 - 6.43)
Confidential - Internal use only 40
*risk of event within median RE-LY duration [~20 months], not annualized; $ Clopper-Pearson (Exact)
Ischemic Stroke/SEE Major Bleeding
Rel. Risk 90% CI Relative Risk 90% CI$
Titration vs Reference 1.06 (0.76 – 1.50) 0.80 (0.66 – 0.97)
Titration vs Warfarin 0.80 (0.58 – 1.11) 0.60 (0.50 – 0.72)
Background
Dose-Exposure-Response Relationship
Dose-Exposure Relationship
• Pharmacokinetic was thoroughly characterized in > 11.000 AF patients, OS patients, and healthy
subjects; relevant covariates were identified.
• Good predictive performance of dabigatran exposure.
Exposure-Response Relationship
• Exposure-response relationship was intensively characterized in >8000 AF patients from RE-LY
showing a significant relationship between dabigatran trough concentrations at steady-state
(Ctrough,ss) and major bleeding events and ischemic stroke/SEE events; relevant covariates were
identified.
• Bleeding and ischemic stroke/SEE model showed good predictive performance of outcome events
from remaining ~3500 RE-LY patients not included in analysis!!! (NEW)
Good predictive performance of available models justifies projection of “what-if” scenarios.
Confidential - Internal use only 41
A Clinical Trial Simulation Analysis-add on-
May 25, 2012
Impact of Dabigatran Dose Adjustment on Clinical
Outcome in AF Patients
Translational Medicine
Background
• In the original analysis, all patients were kept in the analysis, even if they had low exposure levels
which might have lead to insufficient stroke protection.
• How many patients had low exposure levels even under 150 mg BID?
• What is the impact if these patients are excluded from the analysis?
• What is the impact if these patients are up-titrated to 220 mg BID?
Confidential - Internal use only 43
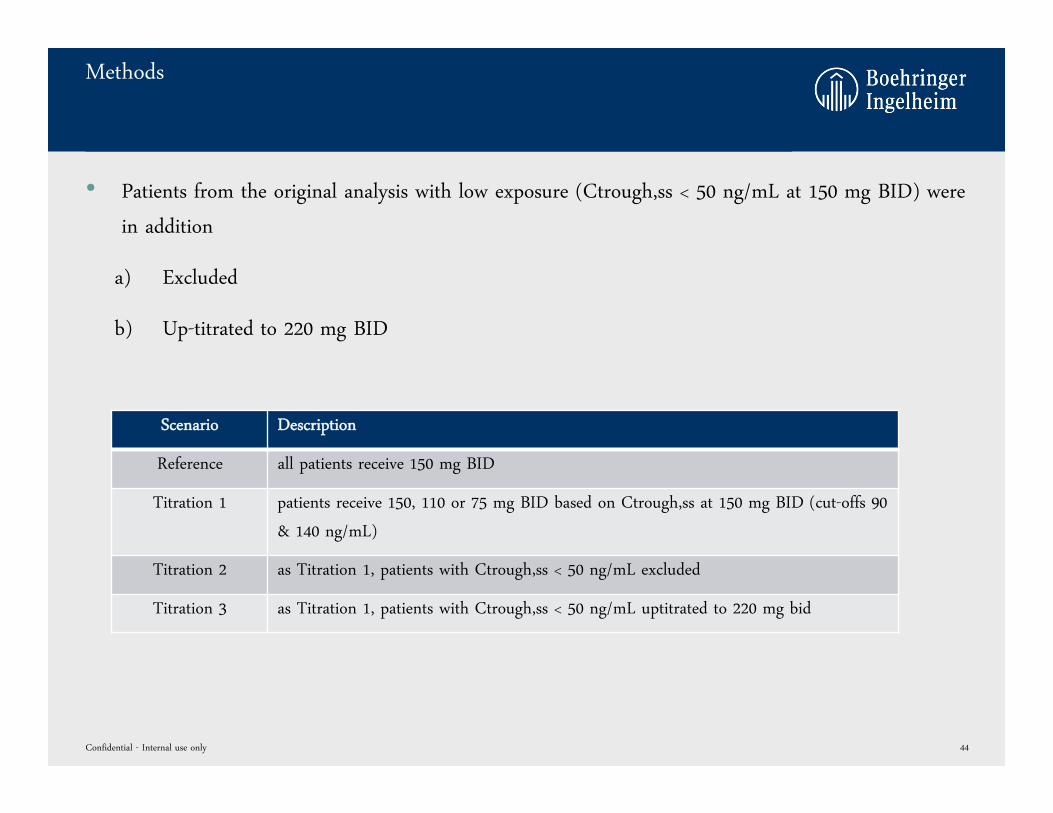
Methods
• Patients from the original analysis with low exposure (Ctrough,ss < 50 ng/mL at 150 mg BID) were
in addition
a) Excluded
b) Up-titrated to 220 mg BID
Confidential - Internal use only 44
Scenario Description
Reference all patients receive 150 mg BID
Titration 1 patients receive 150, 110 or 75 mg BID based on Ctrough,ss at 150 mg BID (cut-offs 90
& 140 ng/mL)
Titration 2 as Titration 1, patients with Ctrough,ss < 50 ng/mL excluded
Titration 3 as Titration 1, patients with Ctrough,ss < 50 ng/mL uptitrated to 220 mg bid
Results
Model Predicted Outcomes and Exposure
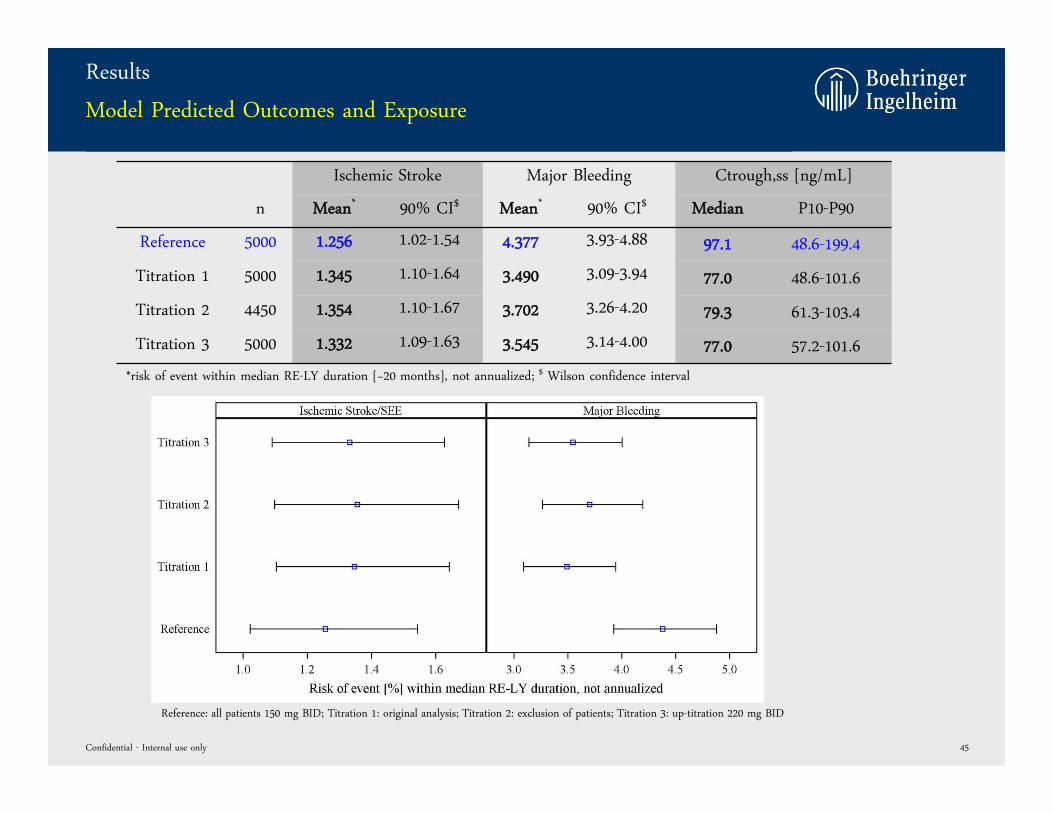
Ischemic Stroke Major Bleeding Ctrough,ss [ng/mL]
n Mean* 90% CI$ Mean* 90% CI$ Median P10-P90
Reference 5000 1.256 1.02-1.54 4.377 3.93-4.88 97.1 48.6-199.4
Titration 1 5000 1.345 1.10-1.64 3.490 3.09-3.94 77.0 48.6-101.6
Titration 2 4450 1.354 1.10-1.67 3.702 3.26-4.20 79.3 61.3-103.4
Titration 3 5000 1.332 1.09-1.63 3.545 3.14-4.00 77.0 57.2-101.6
Confidential - Internal use only 45
*risk of event within median RE-LY duration [~20 months], not annualized; $ Wilson confidence interval
Reference: all patients 150 mg BID; Titration 1: original analysis; Titration 2: exclusion of patients; Titration 3: up-titration 220 mg BID
Results
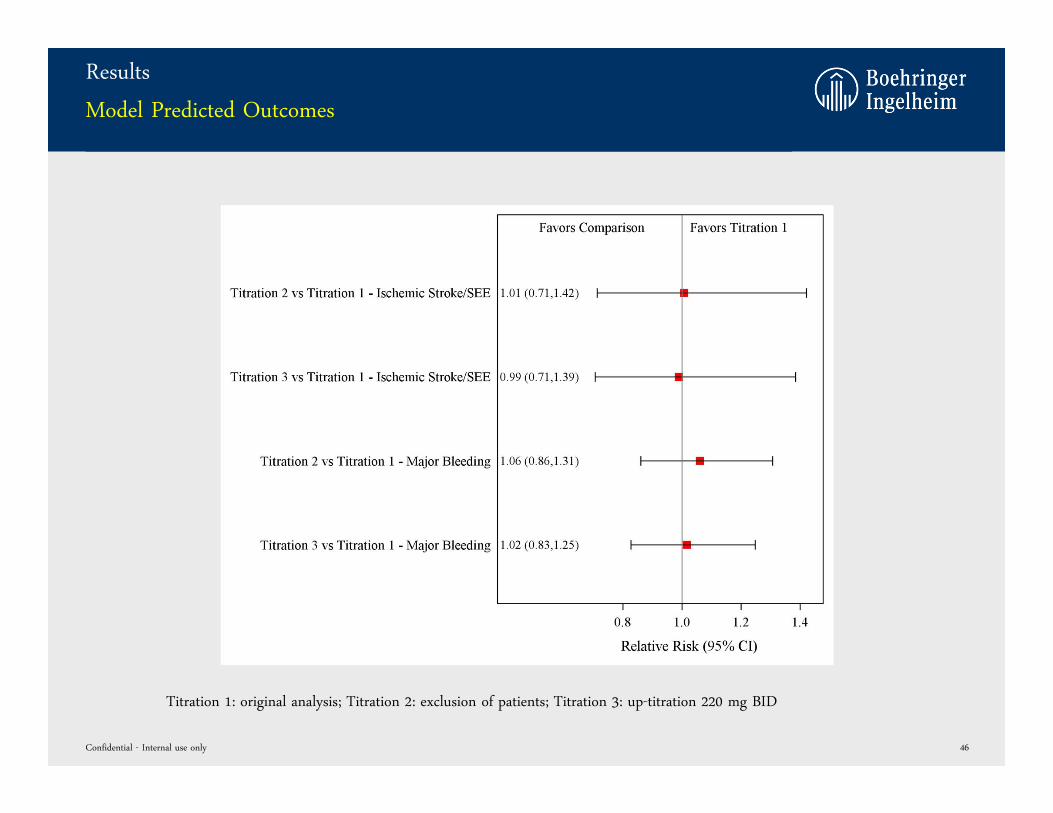
Model Predicted Outcomes
Confidential - Internal use only 46
Titration 1: original analysis; Titration 2: exclusion of patients; Titration 3: up-titration 220 mg BID
Results
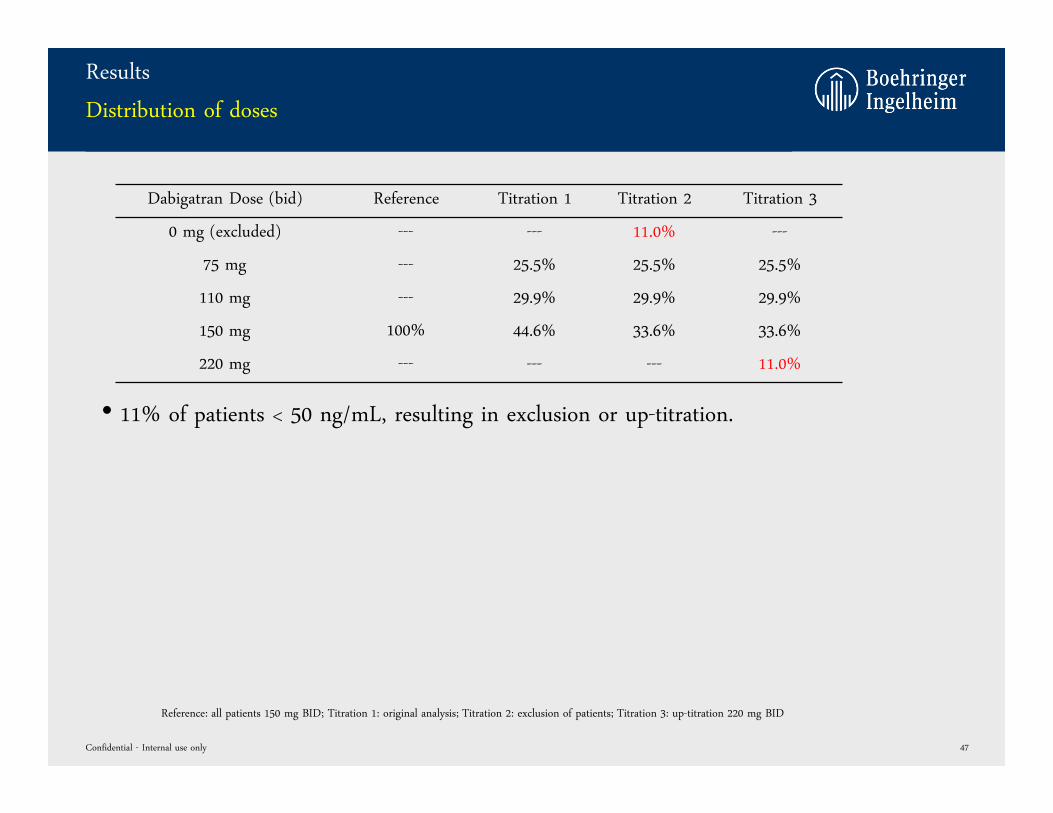
Distribution of doses
Dabigatran Dose (bid) Reference Titration 1 Titration 2 Titration 3
0 mg (excluded) --- --- 11.0% ---
75 mg --- 25.5% 25.5% 25.5%
110 mg --- 29.9% 29.9% 29.9%
150 mg 100% 44.6% 33.6% 33.6%
220 mg --- --- --- 11.0%
Confidential - Internal use only 47
• 11% of patients < 50 ng/mL, resulting in exclusion or up-titration.
Reference: all patients 150 mg BID; Titration 1: original analysis; Titration 2: exclusion of patients; Titration 3: up-titration 220 mg BID
Summary
• About 11% of the patients are predicted to have low exposure levels (Ctrough,ss < 50 ng/mL) after
treatment with DE 150 mg BID
• Exclusion of these patients (Titration 2) results in increased ischemic stroke/SEE (RR:1.01) and
major bleeding rates (RR:1.06) compared to original titration (Titration 1).
• Reason: the excluded patients are in general younger and healthier and have consequently a
lower risk for outcome events. If excluded a population at higher risk is generated.
• Up-titration of these patients (Titration 3) results in minor reduction in ischemic stroke/SEE (RR:
0.99) and in minor increase of major bleedings (RR: 1.02) compared to the original titration
analysis (Titration 1).
Confidential - Internal use only 48
Conclusion
• AF patients with low exposure have a minor impact on the overall outcome of the titration analysis.
• Up-titration or exclusion of patients with low exposure did not improve the outcome significantly.
• Threshold of low exposure (Ctrough,ss < 50 ng/mL) resulting in up-titration/exclusion was chosen
based on educated guess. A systematic review of the optimal cut-off value could be performed, but
is not expected to improve the outcome significantly.
Confidential - Internal use only 49
A Clinical Trial Simulation Analysis-back up slides-
July 11, 2012
Impact of Dabigatran Dose Adjustment on Clinical
Outcome in AF Patients
Global Translational Medicine
Pharmacometrics
Questions prepared
• What is the impact of intra-individual variability on the dose selection?
• What is the impact of the 10-16 h sampling window on the dose selection?
• How is the predictive performance of the dose-exposure-response model?
• Why is the projected percentage of patients on 75 mg BID so high?
Confidential - Internal use only 51
WHAT IS THE IMPACT OF INTRA-INDIVIDUAL VARIABILITY ON
THE DOSE SELECTION?
Confidential - Internal use only 52
Intra-individual Variability
Background
• The intra-individual pharmacokinetic variability was estimated based on the RE-LY dataset using a
population PK modeling approach.
• An intra-individual variability of 26.6 %CV on bioavailability was estimated.
• Results not officially reported yet.
Confidential - Internal use only 53
Intra-individual Variability
Methods
• Adapted RE-LY population PK model was used to predict the influence of intra-individual
variability on dose selection.
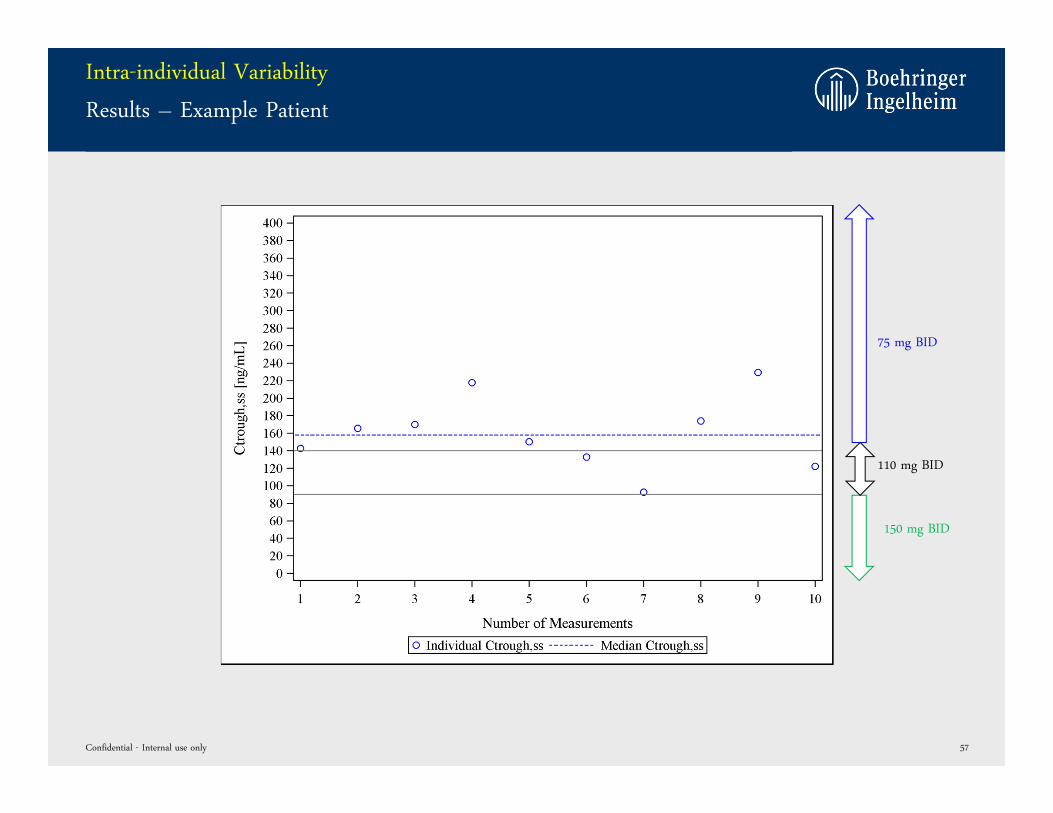
• Baseline demographics from 9521 AF patients from RE-LY were included. For each patient, 10
repeated measurements (Ctrough,ss). Overall, 500 clinical trials with 5000 patients each were
bootstrapped and simulated.
• For each patient at each replicate, the median Ctrough,ss across the 10 measurements was
calculated, assuming to represent the “true Ctrough,ss” value and consequently the “true target
dose”.
• Subsequently, the median of the first two up to ten trough concentrations was calculated and the
respective dose assigned.
• The assigned dose was compared to the true target dose.
Confidential - Internal use only 54
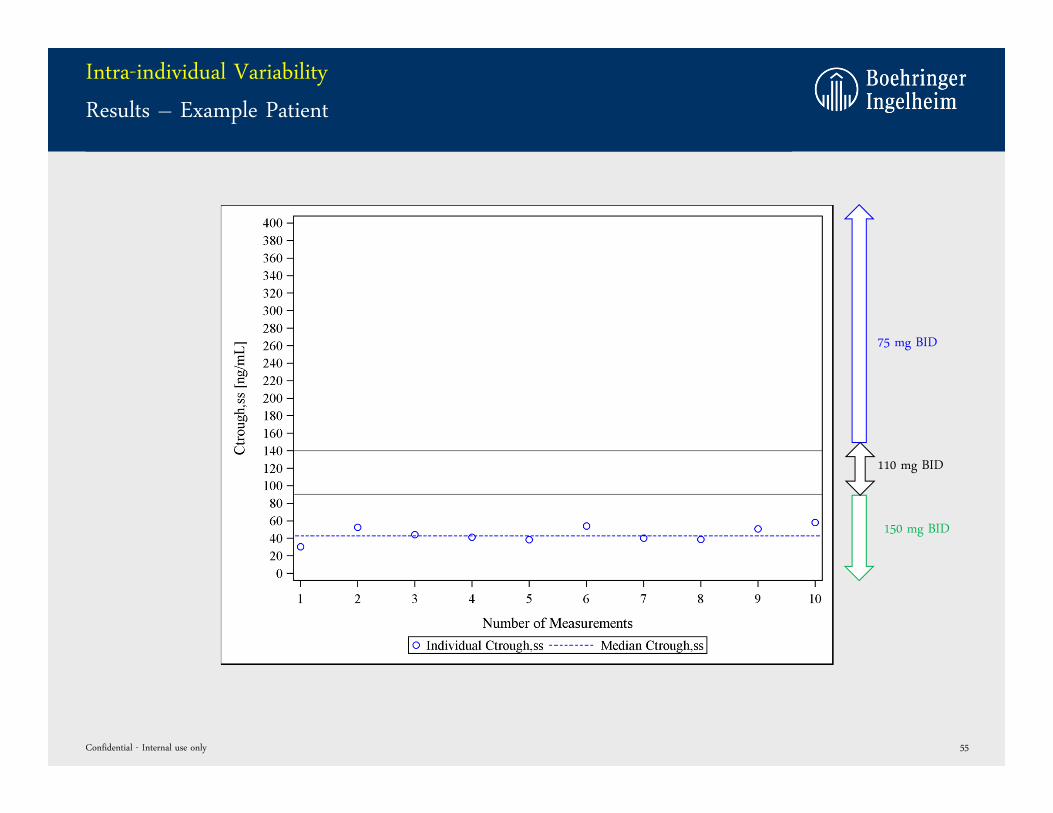
Intra-individual Variability
Results – Example Patient
Confidential - Internal use only 55
75 mg BID
110 mg BID
150 mg BID
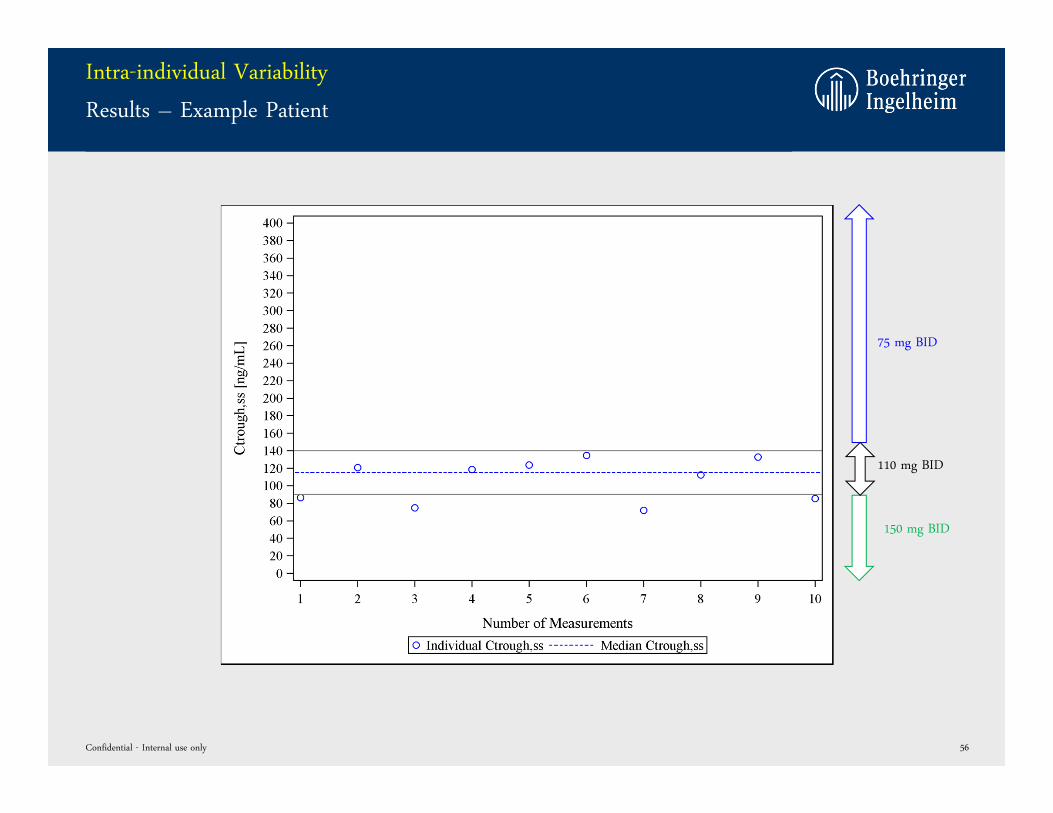
Intra-individual Variability
Results – Example Patient
Confidential - Internal use only 56
75 mg BID
110 mg BID
150 mg BID
Intra-individual Variability
Results – Example Patient
Confidential - Internal use only 57
75 mg BID
110 mg BID
150 mg BID
Intra-individual Variability
Results
Confidential - Internal use only 58
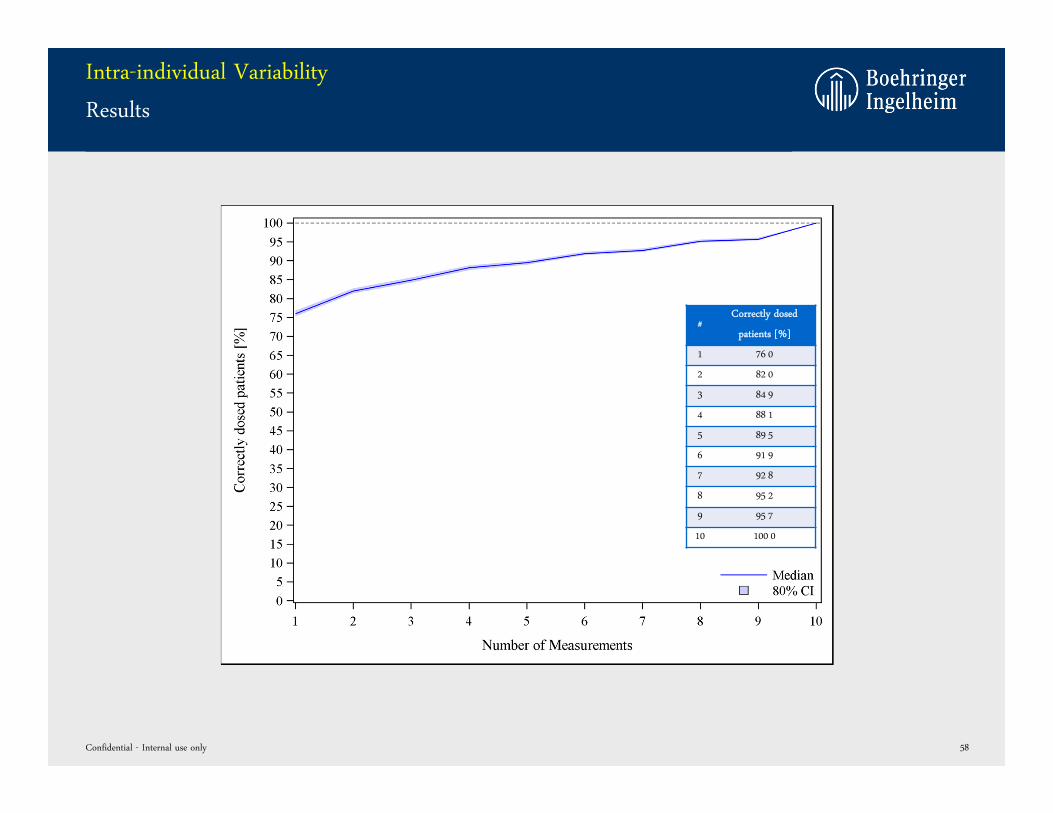
#Correctly dosed
patients [%]
1 76 0
2 82 0
3 84 9
4 88 1
5 89 5
6 91 9
7 92 8
8 95 2
9 95 7
10 100 0
Intra-individual Variability
Results – by dose group
Confidential - Internal use only 59
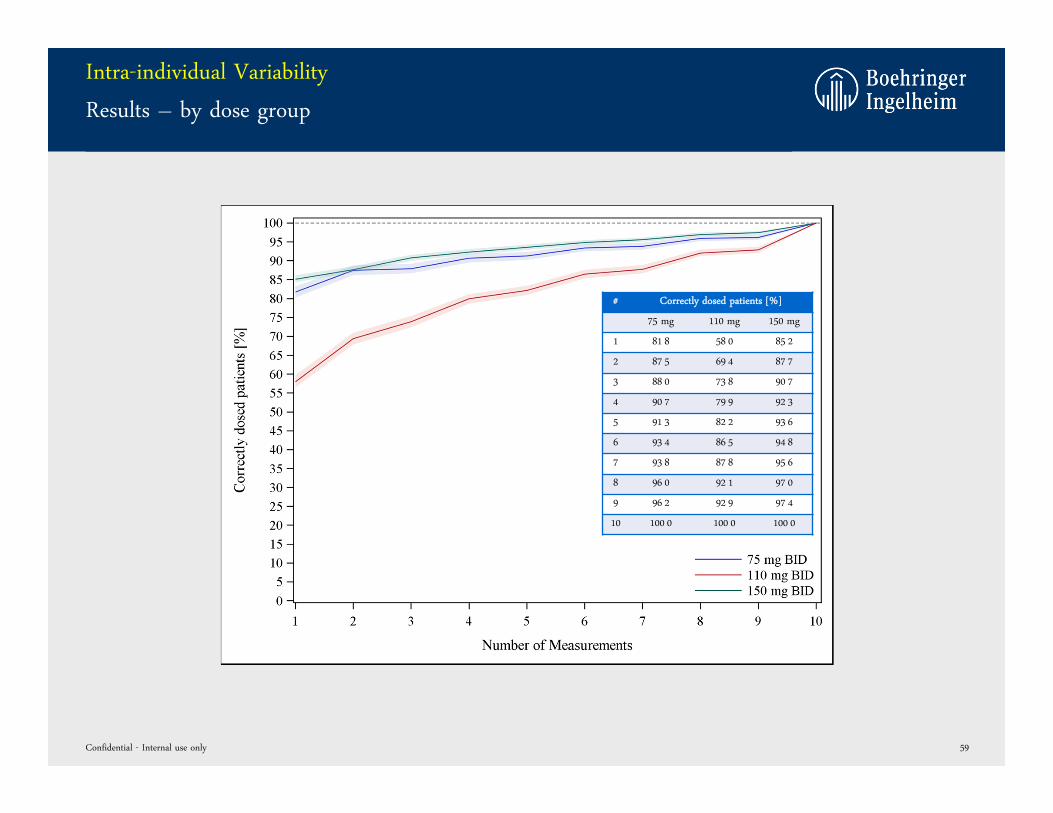
# Correctly dosed patients [%]
75 mg 110 mg 150 mg
1 81 8 58 0 85 2
2 87 5 69 4 87 7
3 88 0 73 8 90 7
4 90 7 79 9 92 3
5 91 3 82 2 93 6
6 93 4 86 5 94 8
7 93 8 87 8 95 6
8 96 0 92 1 97 0
9 96 2 92 9 97 4
10 100 0 100 0 100 0
Intra-individual Variability
Summary
• Intra-individual variability might influence dose selection.
• If only one measurement is taken per patient, >76% of patients are dosed correctly.
• At least 2 measurements are required to achieve an accuracy > 80%.
• Analysis by dose group showed, that the target doses DE 75 mg and DE 150 mg are relatively
robust against intra-individual variability.
After one measurement, already >82% of patients are dosed correctly.
• The DE 110 mg dose group was identified as more sensitive towards intra-individual variability.
Confidential - Internal use only 60
WHAT IS THE IMPACT OF THE 10-16 H SAMPLING WINDOW ON
THE DOSE SELECTION?
Confidential - Internal use only 61
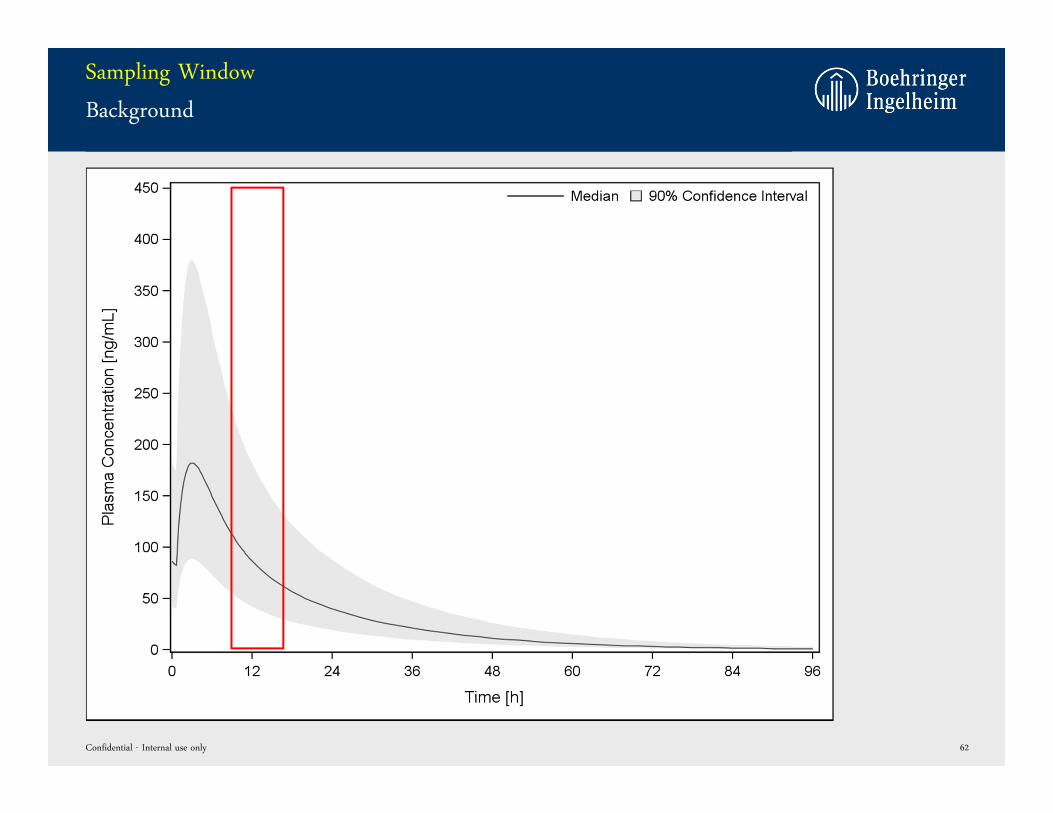
Sampling Window
Background
Confidential - Internal use only 62
Sampling Window
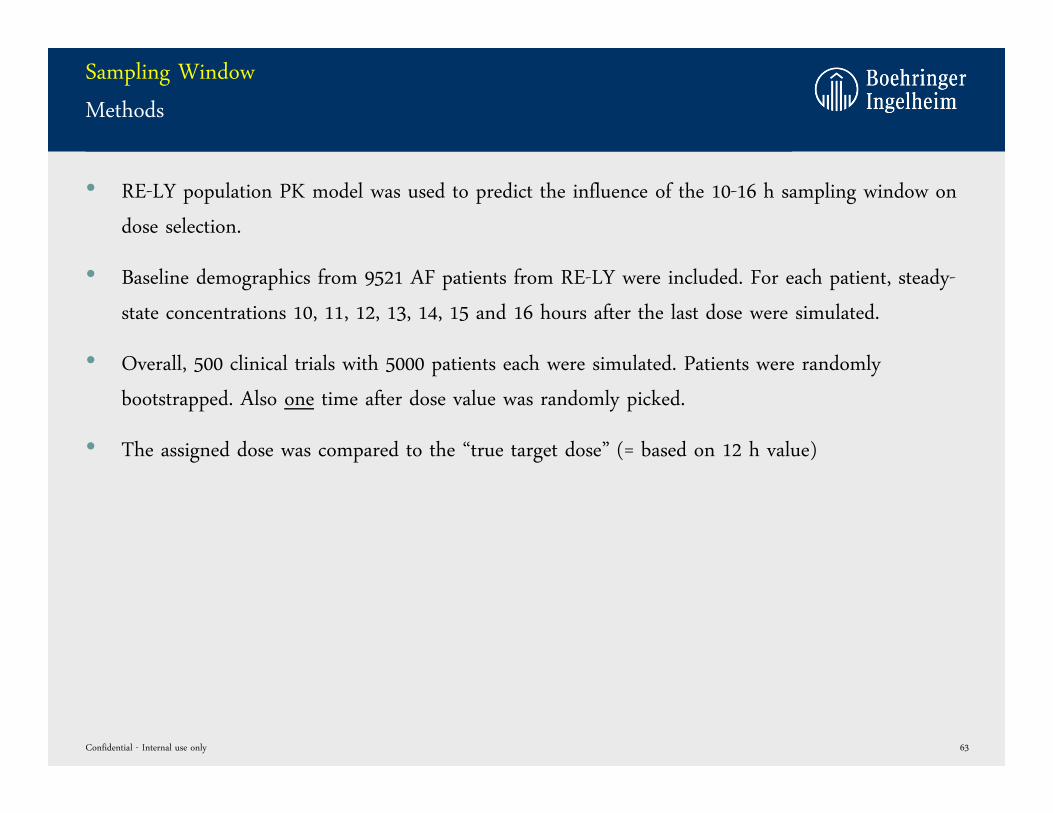
Methods
• RE-LY population PK model was used to predict the influence of the 10-16 h sampling window on
dose selection.
• Baseline demographics from 9521 AF patients from RE-LY were included. For each patient, steady-
state concentrations 10, 11, 12, 13, 14, 15 and 16 hours after the last dose were simulated.
• Overall, 500 clinical trials with 5000 patients each were simulated. Patients were randomly
bootstrapped. Also one time after dose value was randomly picked.
• The assigned dose was compared to the “true target dose” (= based on 12 h value)
Confidential - Internal use only 63
Sampling Window
Results – Example Patient
Confidential - Internal use only 64
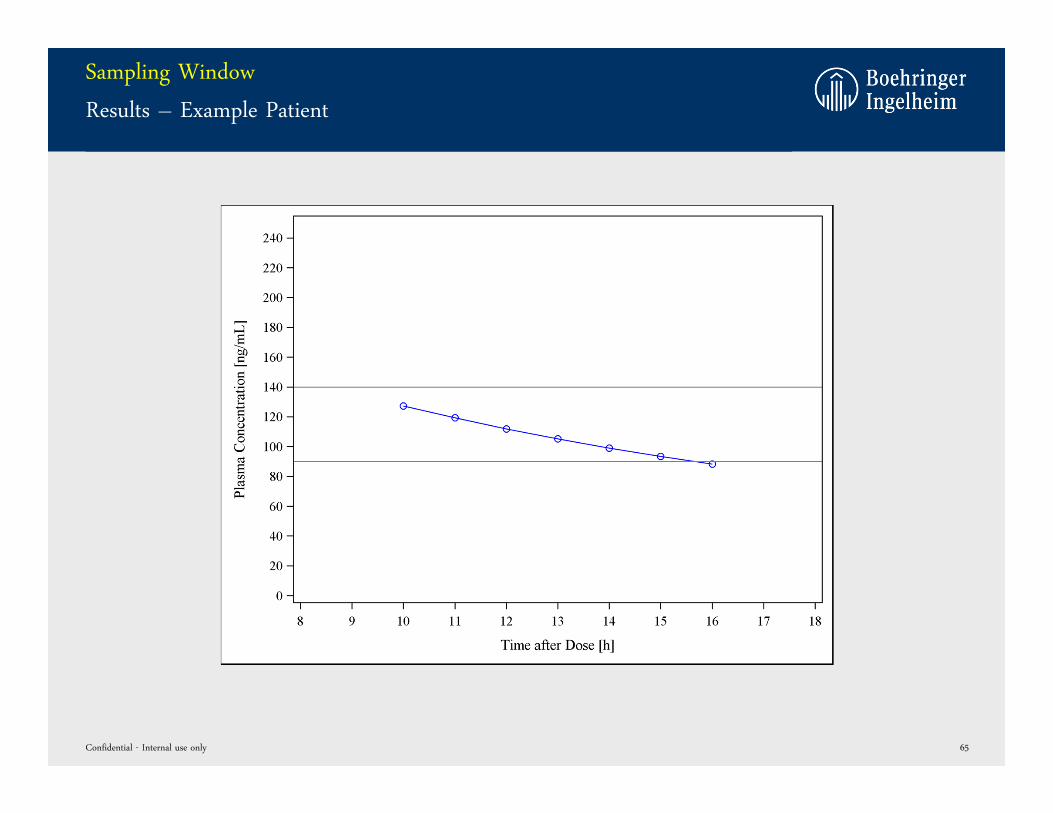
Sampling Window
Results – Example Patient
Confidential - Internal use only 65
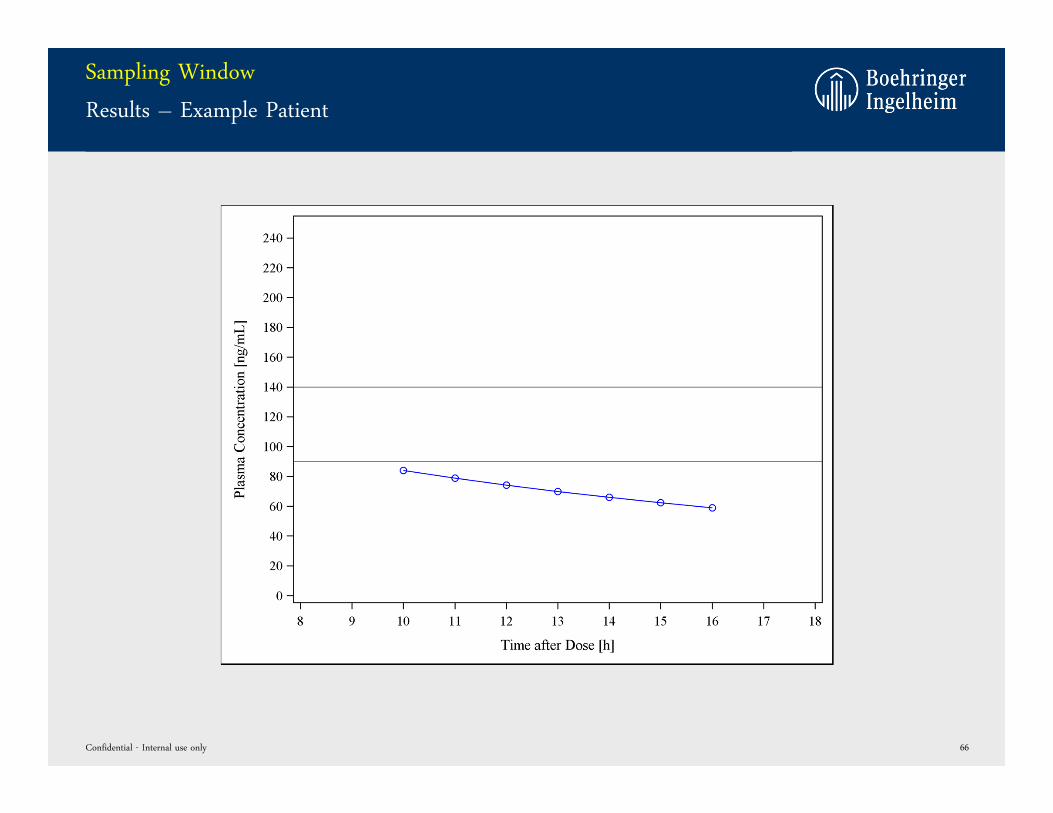
Sampling Window
Results – Example Patient
Confidential - Internal use only 66
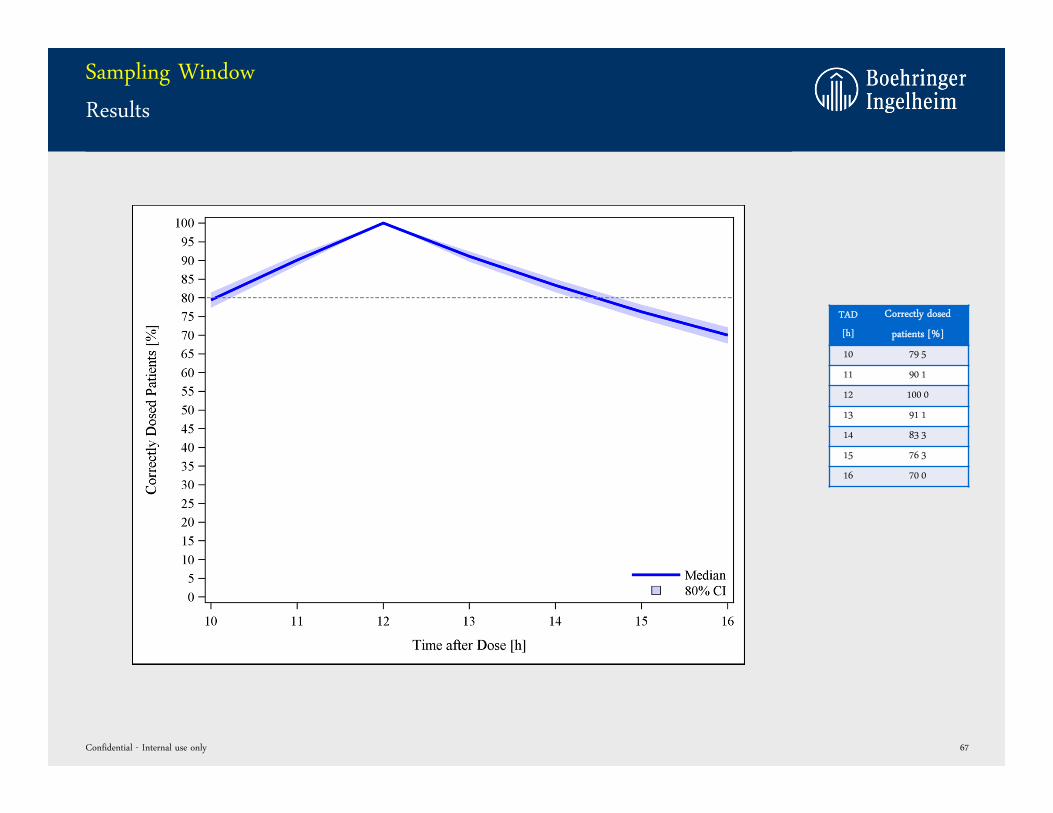
Sampling Window
Results
Confidential - Internal use only 67
TAD
[h]
Correctly dosed
patients [%]
10 79 5
11 90 1
12 100 0
13 91 1
14 83 3
15 76 3
16 70 0
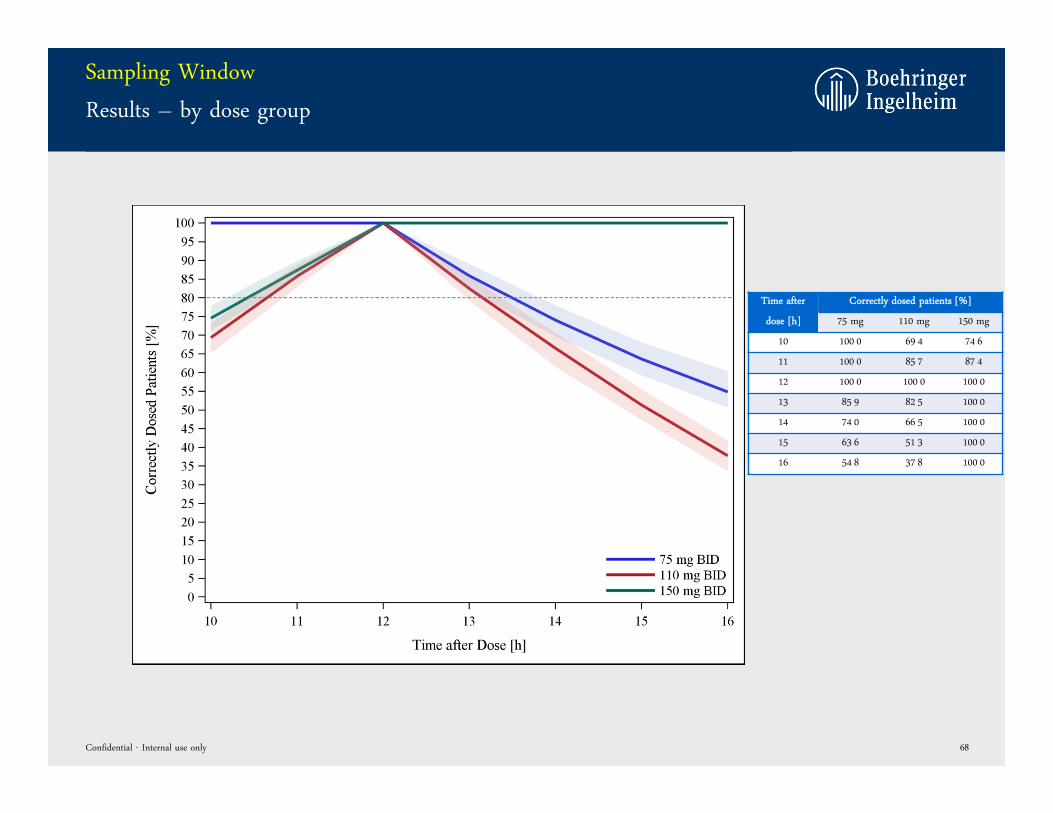
Sampling Window
Results – by dose group
Confidential - Internal use only 68
Time after
dose [h]
Correctly dosed patients [%]
75 mg 110 mg 150 mg
10 100 0 69 4 74 6
11 100 0 85 7 87 4
12 100 0 100 0 100 0
13 85 9 82 5 100 0
14 74 0 66 5 100 0
15 63 6 51 3 100 0
16 54 8 37 8 100 0
Sampling Window
Summary
• The time after dose of the Ctrough,ss value might influence dose selection.
• The time window between 10 – 14 hours results in a stable selection of the correct dose (>80%
correctly dosed patients).
• A more narrow time window of 11 – 13 hours would increase the precision to >90% correctly
dosed patients.
• Analysis by dose group showed, that the 110 mg BID target dose was most sensitive towards the
sampling window.
Confidential - Internal use only 69
HOW IS THE PREDICTIVE PERFORMANCE OF THE DOSE-
EXPOSURE-RESPONSE MODEL?
Confidential - Internal use only 70
Predictive Performance of Models
Background: Population PK Model RE-LY
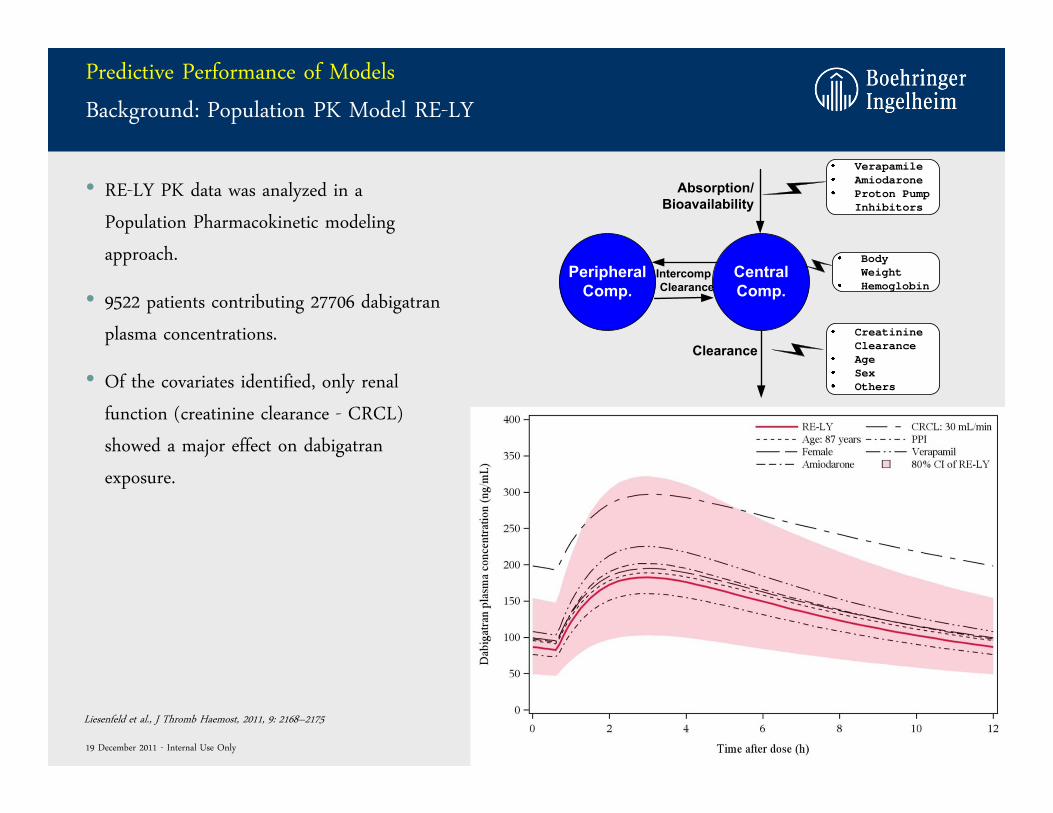
• RE-LY PK data was analyzed in a
Population Pharmacokinetic modeling
approach.
• 9522 patients contributing 27706 dabigatran
plasma concentrations.
• Of the covariates identified, only renal
function (creatinine clearance - CRCL)
showed a major effect on dabigatran
exposure.
CentralComp.
Absorption/Bioavailability
ClearanceCreatinineClearanceAgeSexOthers
PeripheralComp.
IntercompClearance
BodyWeightHemoglobin
VerapamileAmiodaroneProton PumpInhibitors
Liesenfeld et al., J Thromb Haemost, 2011, 9: 2168–2175
19 December 2011 - Internal Use Only
Predictive Performance of Models
Results: Population PK Model RE-LY
72
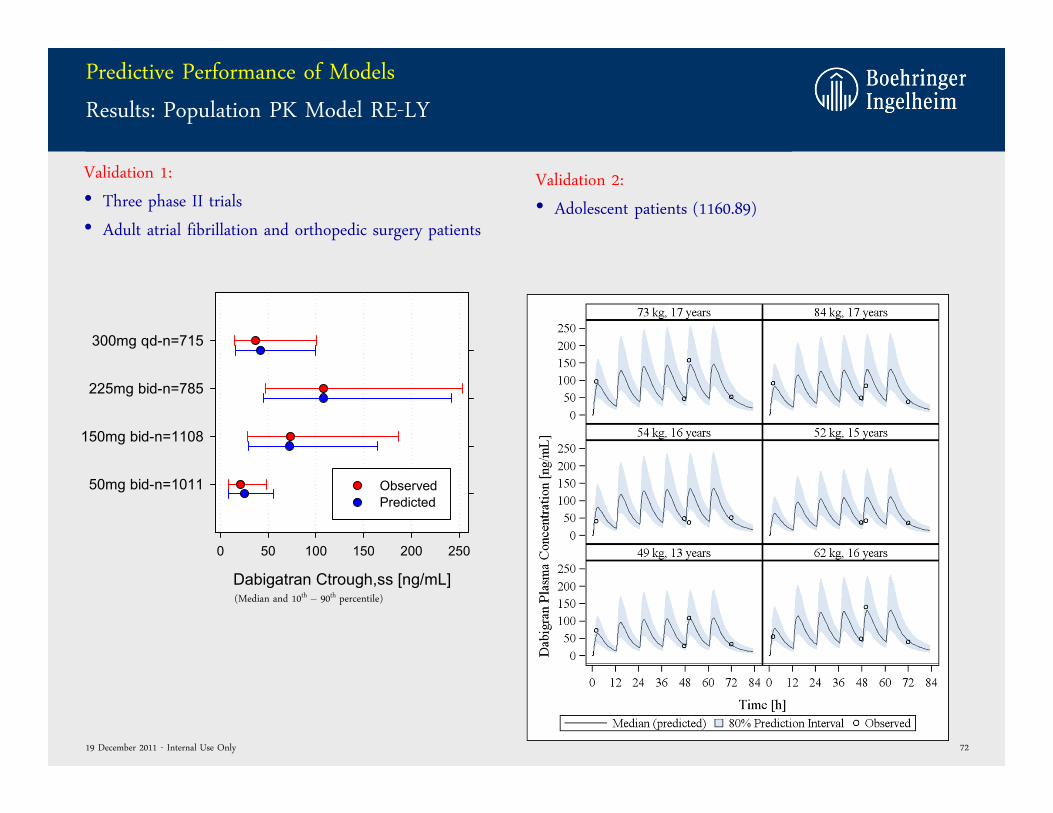
Validation 2:
• Adolescent patients (1160.89)
Dabigatran Ctrough,ss [ng/mL]
0 50 100 150 200 250
50mg bid-n=1011
150mg bid-n=1108
225mg bid-n=785
300mg qd-n=715
Observed Predicted
Validation 1:
• Three phase II trials
• Adult atrial fibrillation and orthopedic surgery patients
(Median and 10th – 90th percentile)
19 December 2011 - Internal Use Only
Predictive Performance of Models
Background: Exposure Response Model
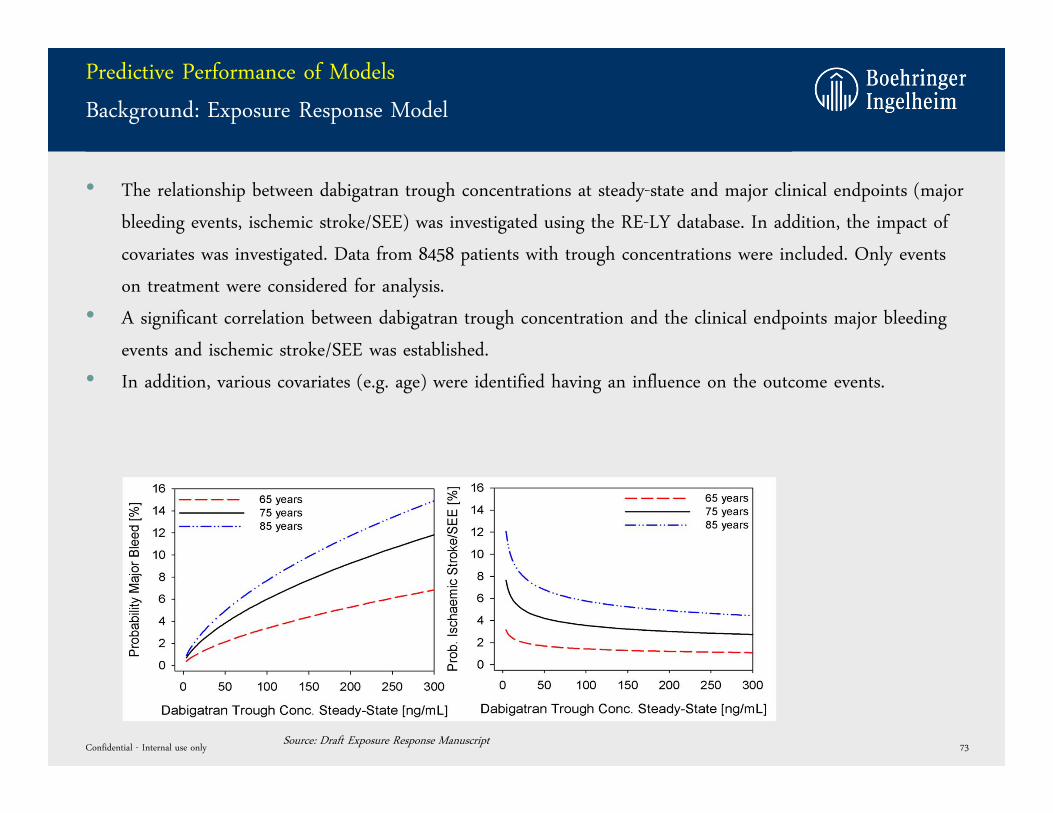
• The relationship between dabigatran trough concentrations at steady-state and major clinical endpoints (major
bleeding events, ischemic stroke/SEE) was investigated using the RE-LY database. In addition, the impact of
covariates was investigated. Data from 8458 patients with trough concentrations were included. Only events
on treatment were considered for analysis.
• A significant correlation between dabigatran trough concentration and the clinical endpoints major bleeding
events and ischemic stroke/SEE was established.
• In addition, various covariates (e.g. age) were identified having an influence on the outcome events.
Confidential - Internal use only 73Source: Draft Exposure Response Manuscript
Predictive Performance of Models
Result: Exposure Response Model
• The predictive performance of the final logistic regression models for major bleeding and ischemic stroke/SEE
was tested by projecting the event rates in the dabigatran patients without plasma concentration
measurements (N= 3,642).
• For these patients the trough plasma concentrations were predicted using the population PK model from RE-
LY, the individual stroke and bleed rates were calculated based on the final logistic regression models.
• Patients were sorted ascending according to their calculated risk and divided into deciles. For each of the 10
validation subgroup the mean predicted risk for an event and for no event was calculated and compared with
observed rates.
• The predictive performance was evaluated by the Hosmer and Lemeshow test.
• For major bleedings as well as for ischaemic stroke/SEE the P-value was > 0.05, indicating no significant
difference between the predicted and observed event rates.
Good predictive performance!
Confidential - Internal use only 74
Source: Draft Exposure Response Manuscript
Predictive Performance of Models
Result: Exposure Response Model
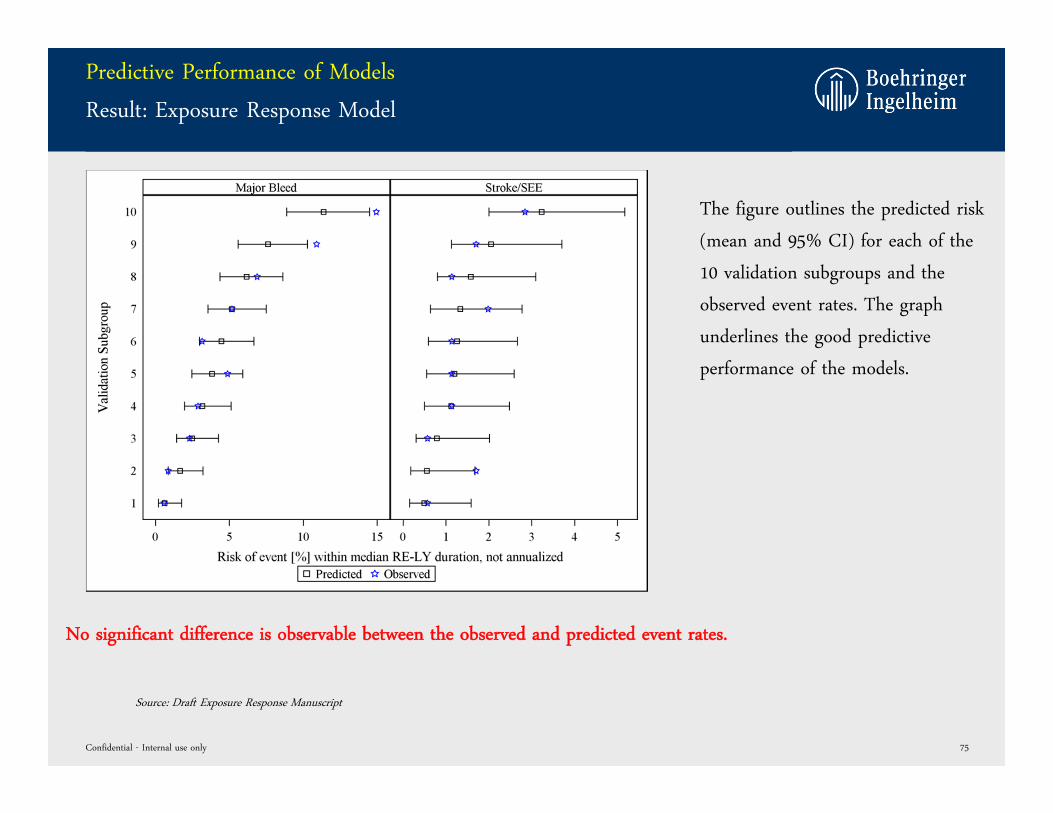
No significant difference is observable between the observed and predicted event rates.
Confidential - Internal use only 75
The figure outlines the predicted risk
(mean and 95% CI) for each of the
10 validation subgroups and the
observed event rates. The graph
underlines the good predictive
performance of the models.
Source: Draft Exposure Response Manuscript
Predictive Performance of Models
Summary
• The dose-exposure (=population PK) model as well as the exposure-response model have
shown an excellent descriptive as well as predictive performance.
• Important covariates influencing the dose-exposure-response relationship have been
identified.
• The excellent performance of the models allows prediction of untested scenarios.
Confidential - Internal use only 76
WHY IS THE PROJECTED PERCENTAGE OF PATIENTS ON 75 MG
BID SO HIGH?
Confidential - Internal use only 77
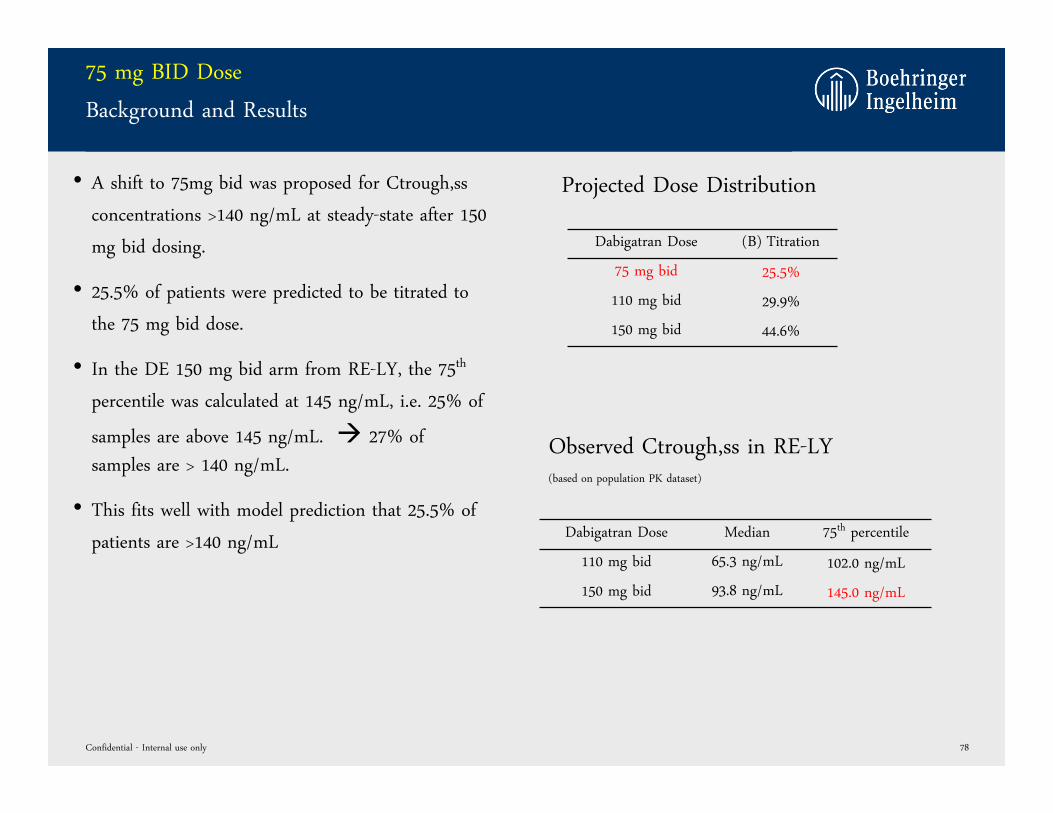
75 mg BID Dose
Background and Results
Dabigatran Dose (B) Titration
75 mg bid 25.5%
110 mg bid 29.9%
150 mg bid 44.6%
Confidential - Internal use only 78
• A shift to 75mg bid was proposed for Ctrough,ss
concentrations >140 ng/mL at steady-state after 150
mg bid dosing.
• 25.5% of patients were predicted to be titrated to
the 75 mg bid dose.
• In the DE 150 mg bid arm from RE-LY, the 75th
percentile was calculated at 145 ng/mL, i.e. 25% of
samples are above 145 ng/mL. 27% of samples are > 140 ng/mL.
• This fits well with model prediction that 25.5% of
patients are >140 ng/mL
Projected Dose Distribution
Observed Ctrough,ss in RE-LY(based on population PK dataset)
Dabigatran Dose Median 75th percentile
110 mg bid 65.3 ng/mL 102.0 ng/mL
150 mg bid 93.8 ng/mL 145.0 ng/mL
WHAT IS THE IMPACT ON OUTCOME EVENTS IF THE 110 MG
BID DOSE IS OMITTED?
Confidential - Internal use only 79
Cut-Off Ctrough,ss [ng/mL]
0 20 40 60 80 100 120 140 160 180 200 220 240 260
%C
hang
e M
ajor
Ble
eds
+ 2x
%C
hang
e Is
chem
ic S
troke
/SE
E
-8
-6
-4
-2
0
2
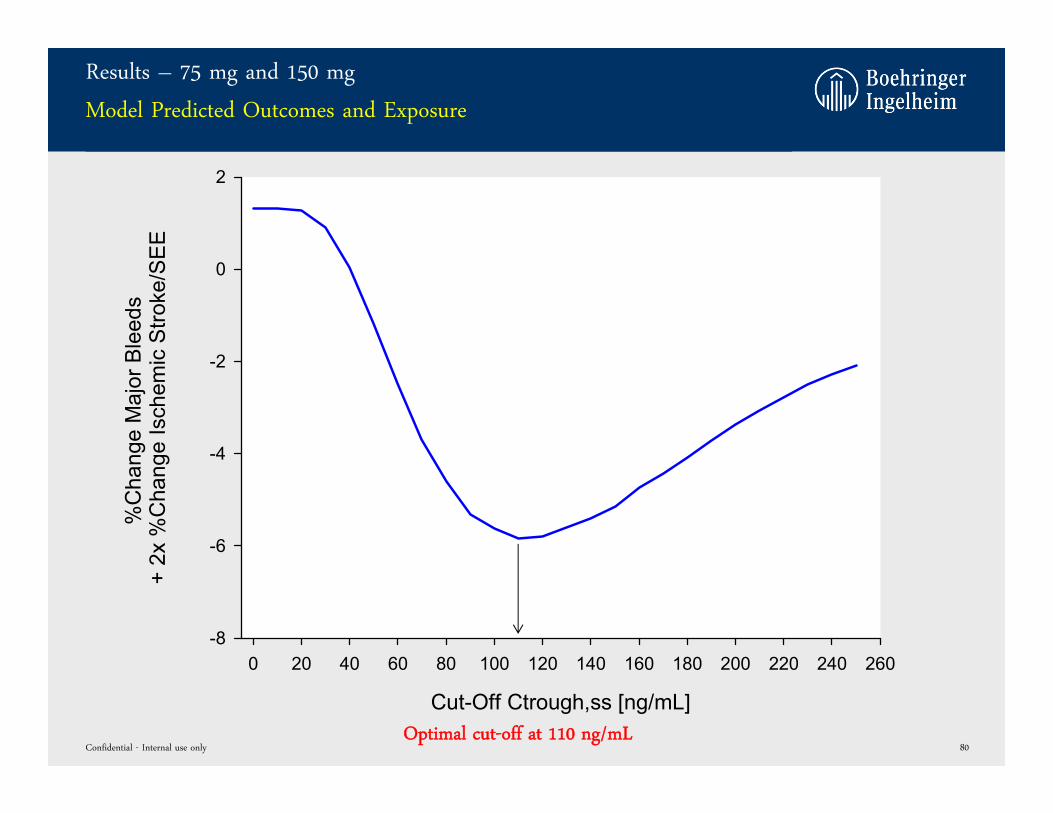
Results – 75 mg and 150 mg
Model Predicted Outcomes and Exposure
Confidential - Internal use only 80Optimal cut-off at 110 ng/mL
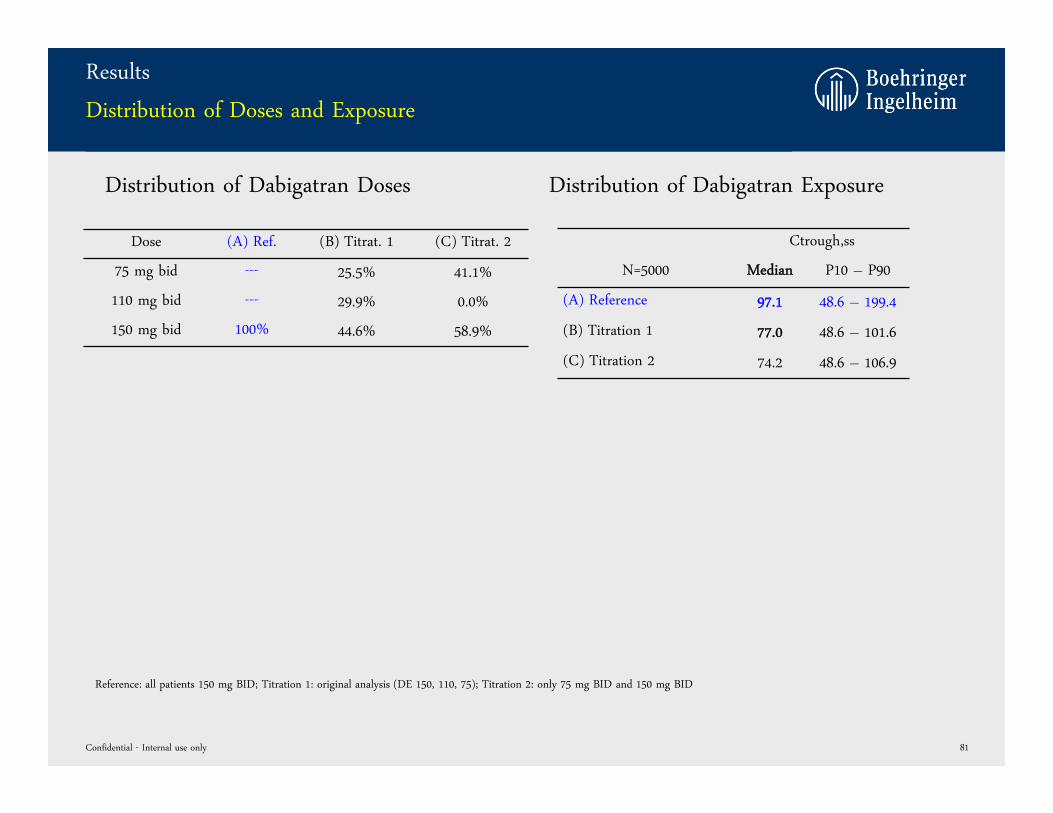
Results
Distribution of Doses and Exposure
Dose (A) Ref. (B) Titrat. 1 (C) Titrat. 2
75 mg bid --- 25.5% 41.1%
110 mg bid --- 29.9% 0.0%
150 mg bid 100% 44.6% 58.9%
Confidential - Internal use only 81
Ctrough,ss
N=5000 Median P10 – P90
(A) Reference 97.1 48.6 – 199.4
(B) Titration 1 77.0 48.6 – 101.6
(C) Titration 2 74.2 48.6 – 106.9
Distribution of Dabigatran Doses Distribution of Dabigatran Exposure
Reference: all patients 150 mg BID; Titration 1: original analysis (DE 150, 110, 75); Titration 2: only 75 mg BID and 150 mg BID
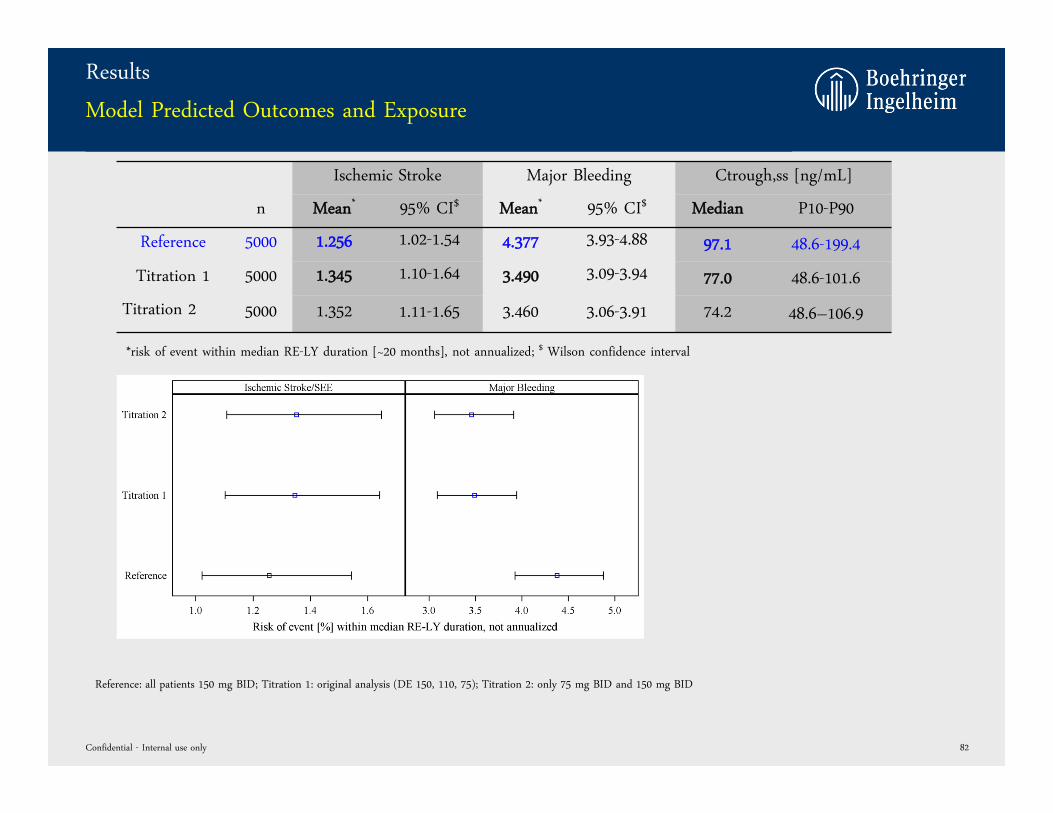
Results
Model Predicted Outcomes and Exposure
Ischemic Stroke Major Bleeding Ctrough,ss [ng/mL]
n Mean* 95% CI$ Mean* 95% CI$ Median P10-P90
Reference 5000 1.256 1.02-1.54 4.377 3.93-4.88 97.1 48.6-199.4
Titration 1 5000 1.345 1.10-1.64 3.490 3.09-3.94 77.0 48.6-101.6
Titration 2 5000 1.352 1.11-1.65 3.460 3.06-3.91 74.2 48.6–106.9
Confidential - Internal use only 82
*risk of event within median RE-LY duration [~20 months], not annualized; $ Wilson confidence interval
Reference: all patients 150 mg BID; Titration 1: original analysis (DE 150, 110, 75); Titration 2: only 75 mg BID and 150 mg BID
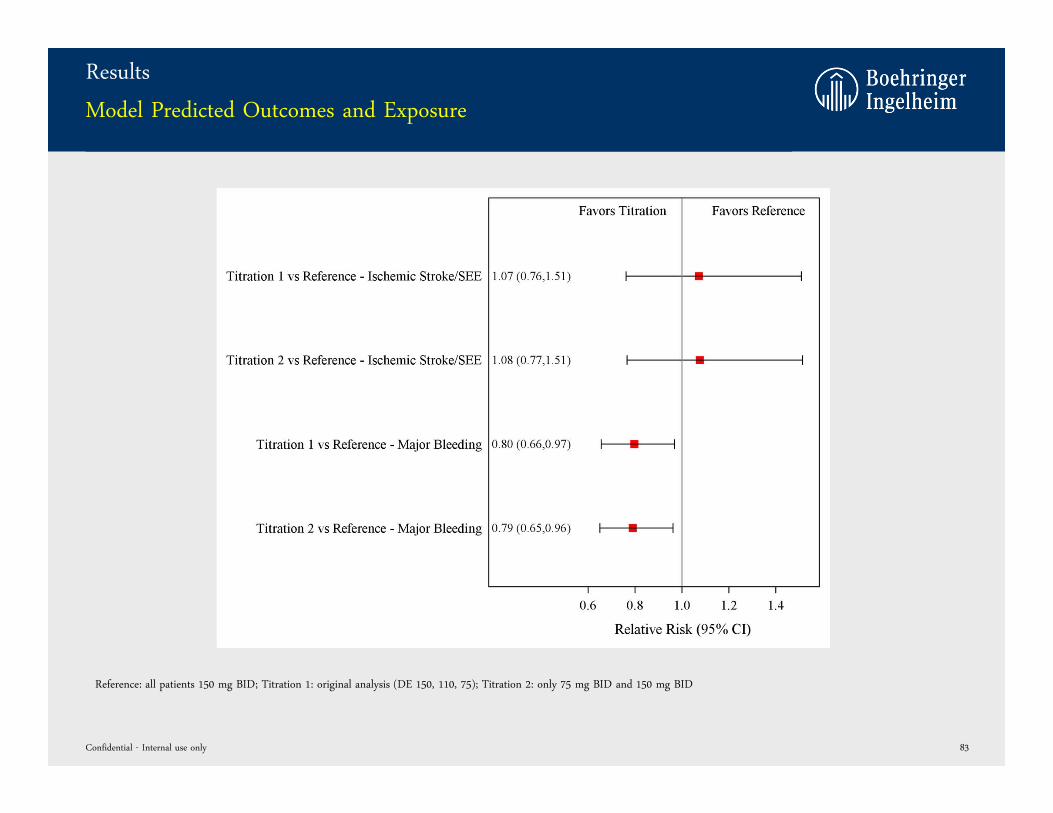
Results
Model Predicted Outcomes and Exposure
Confidential - Internal use only 83
Reference: all patients 150 mg BID; Titration 1: original analysis (DE 150, 110, 75); Titration 2: only 75 mg BID and 150 mg BID
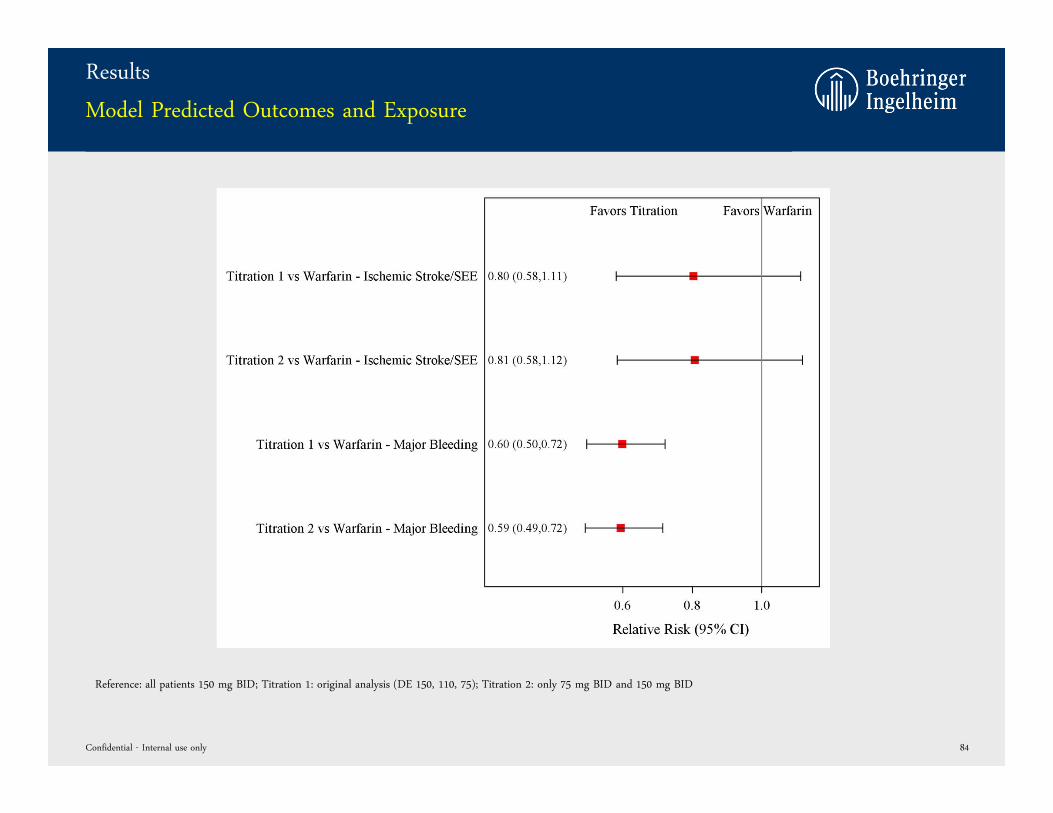
Results
Model Predicted Outcomes and Exposure
Confidential - Internal use only 84
Reference: all patients 150 mg BID; Titration 1: original analysis (DE 150, 110, 75); Titration 2: only 75 mg BID and 150 mg BID
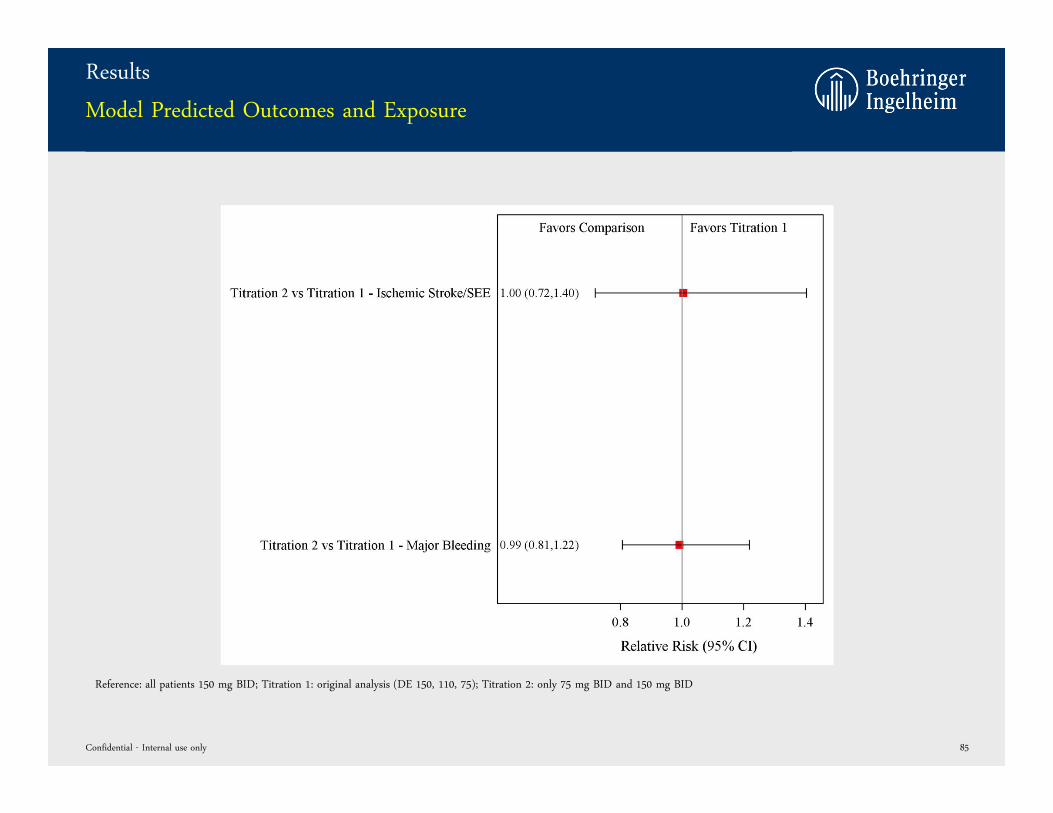
Results
Model Predicted Outcomes and Exposure
Confidential - Internal use only 85
Reference: all patients 150 mg BID; Titration 1: original analysis (DE 150, 110, 75); Titration 2: only 75 mg BID and 150 mg BID
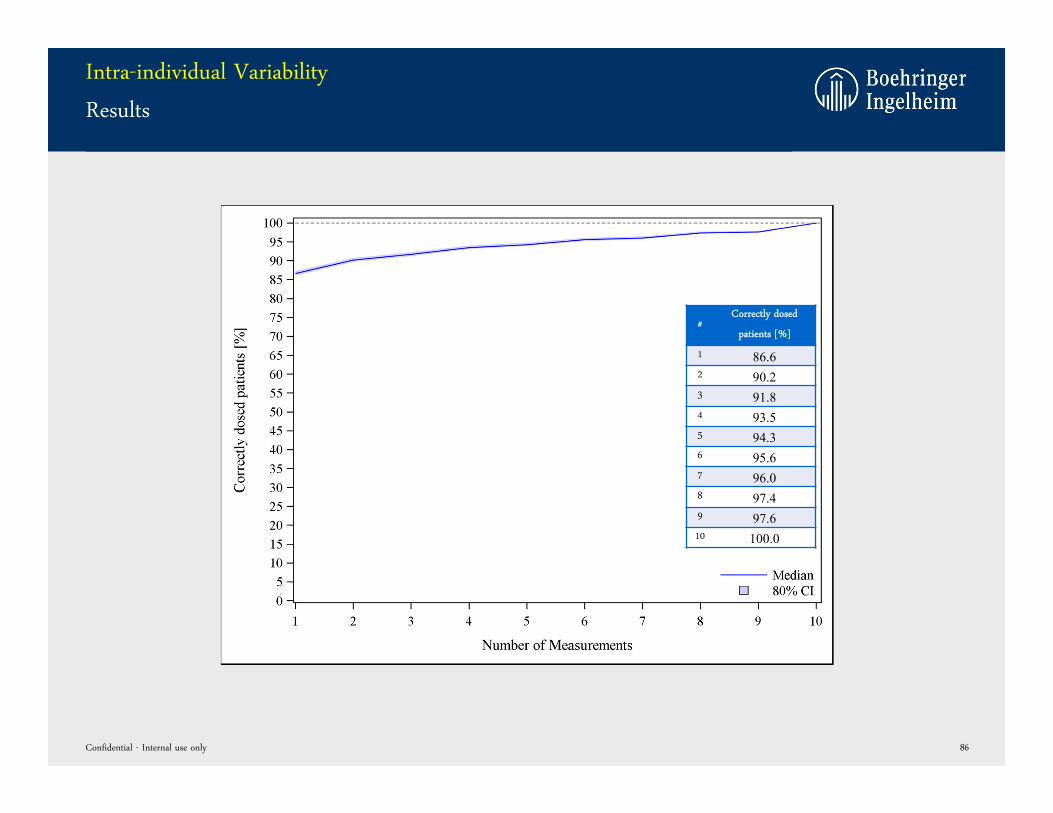
Intra-individual Variability
Results
Confidential - Internal use only 86
#Correctly dosed
patients [%]
1 86.62 90.23 91.84 93.55 94.36 95.67 96.08 97.49 97.610 100.0
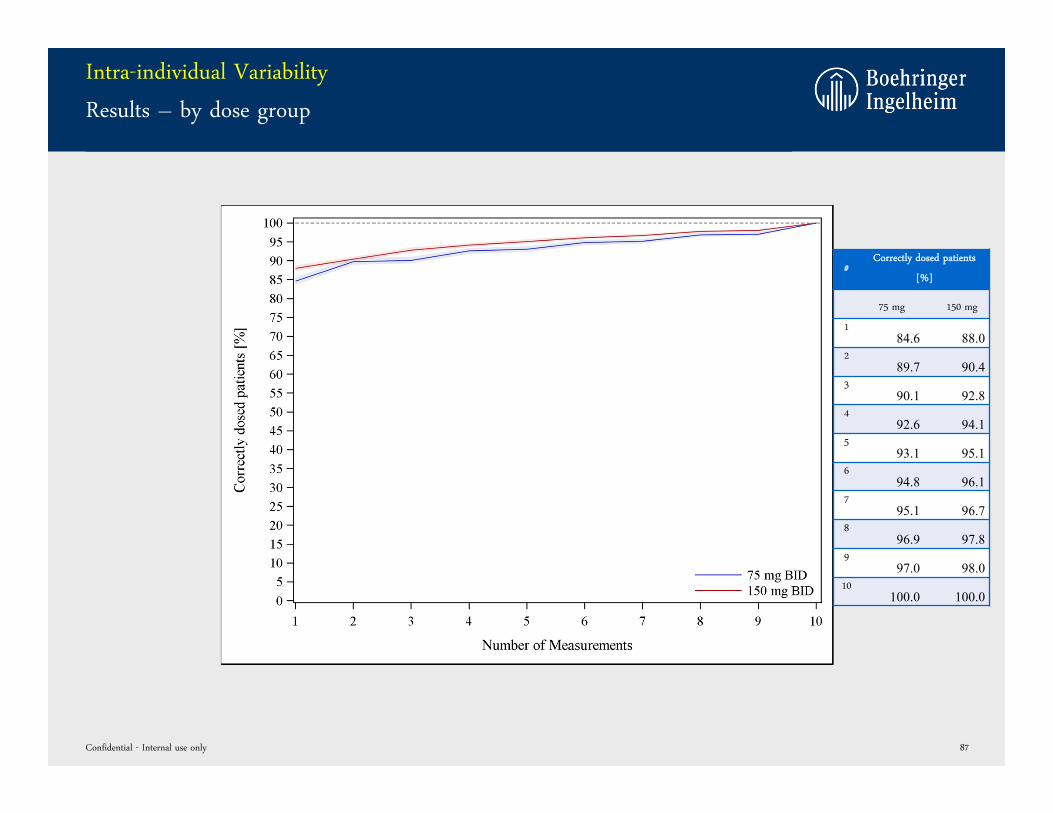
Intra-individual Variability
Results – by dose group
Confidential - Internal use only 87
#Correctly dosed patients
[%]
75 mg 150 mg
184.6 88.0
289.7 90.4
390.1 92.8
492.6 94.1
593.1 95.1
694.8 96.1
795.1 96.7
896.9 97.8
997.0 98.0
10100.0 100.0
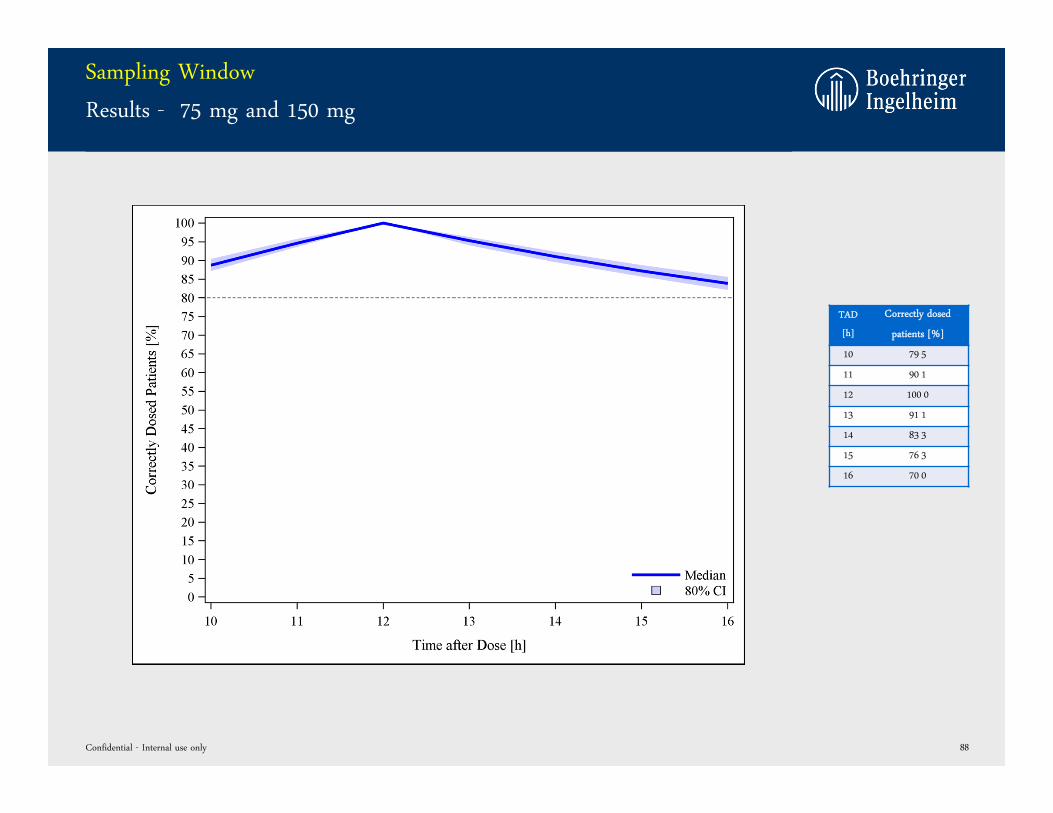
Sampling Window
Results - 75 mg and 150 mg
Confidential - Internal use only 88
TAD
[h]
Correctly dosed
patients [%]
10 79 5
11 90 1
12 100 0
13 91 1
14 83 3
15 76 3
16 70 0
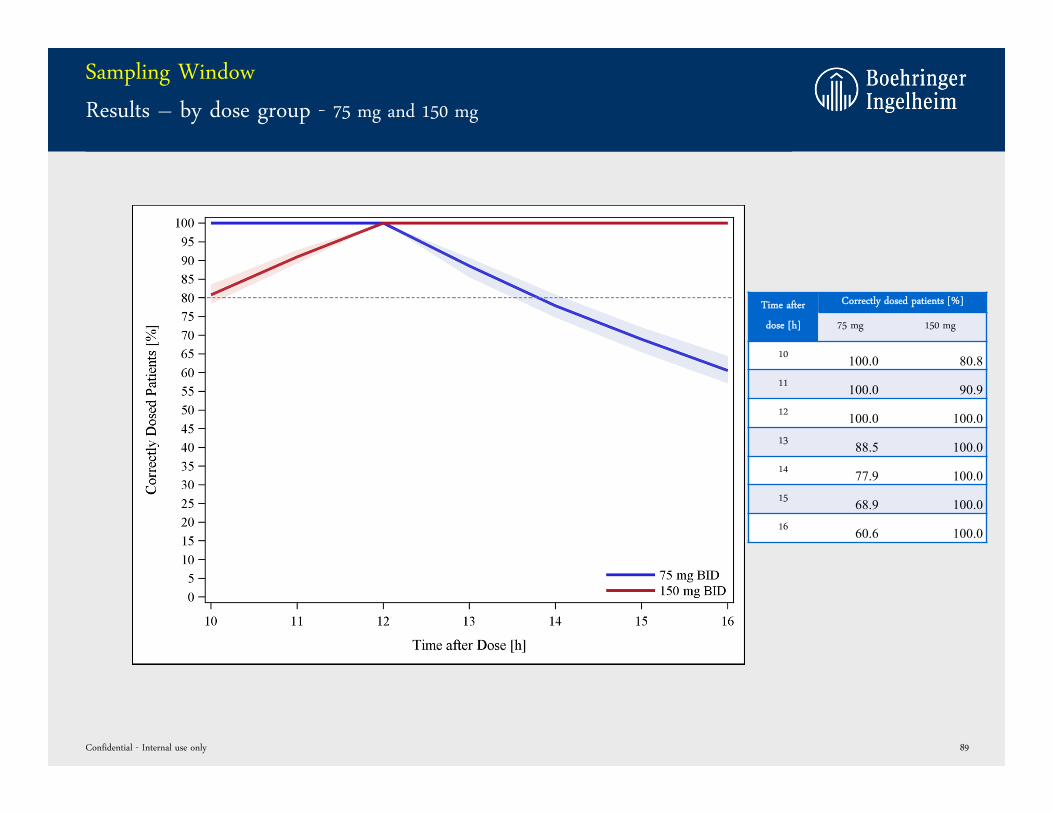
Sampling Window
Results – by dose group - 75 mg and 150 mg
Confidential - Internal use only 89
Time after
dose [h]
Correctly dosed patients [%]
75 mg 150 mg
10 100.0 80.811 100.0 90.912 100.0 100.013 88.5 100.014 77.9 100.015 68.9 100.016 60.6 100.0
backup
Confidential - Internal use only 90
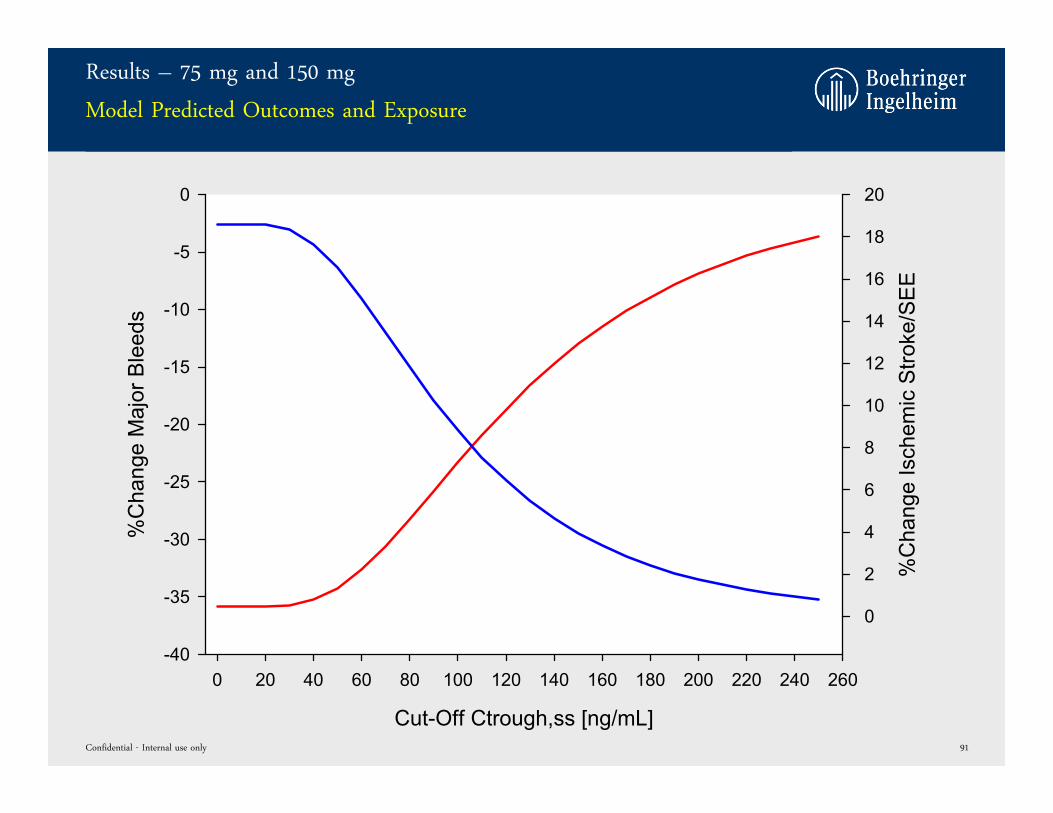
Cut-Off Ctrough,ss [ng/mL]
0 20 40 60 80 100 120 140 160 180 200 220 240 260
%C
hang
e M
ajor
Ble
eds
-40
-35
-30
-25
-20
-15
-10
-5
0
%C
hang
e Is
chem
ic S
troke
/SE
E
0
2
4
6
8
10
12
14
16
18
20
Results – 75 mg and 150 mg
Model Predicted Outcomes and Exposure
Confidential - Internal use only 91
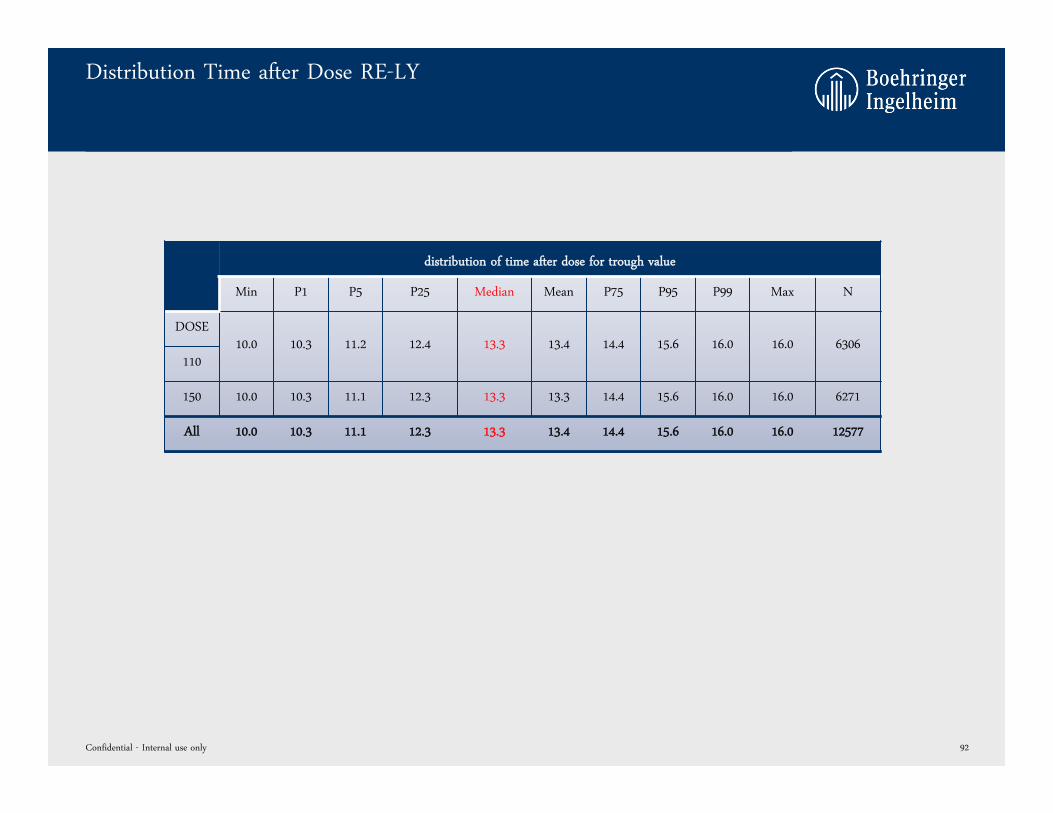
Distribution Time after Dose RE-LY
Confidential - Internal use only 92
distribution of time after dose for trough value
Min P1 P5 P25 Median Mean P75 P95 P99 Max N
DOSE10.0 10.3 11.2 12.4 13.3 13.4 14.4 15.6 16.0 16.0 6306
110
150 10.0 10.3 11.1 12.3 13.3 13.3 14.4 15.6 16.0 16.0 6271
All 10.0 10.3 11.1 12.3 13.3 13.4 14.4 15.6 16.0 16.0 12577
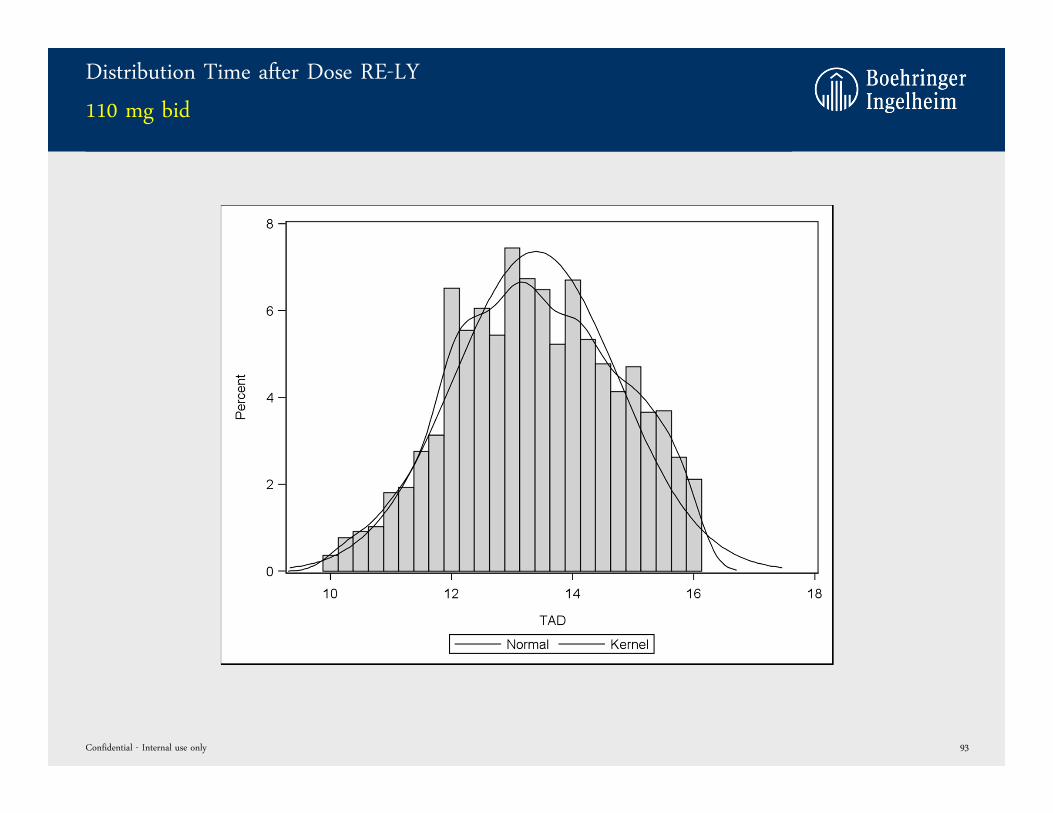
Distribution Time after Dose RE-LY
110 mg bid
Confidential - Internal use only 93

Distribution Time after Dose RE-LY
150 mg bid
Confidential - Internal use only 94
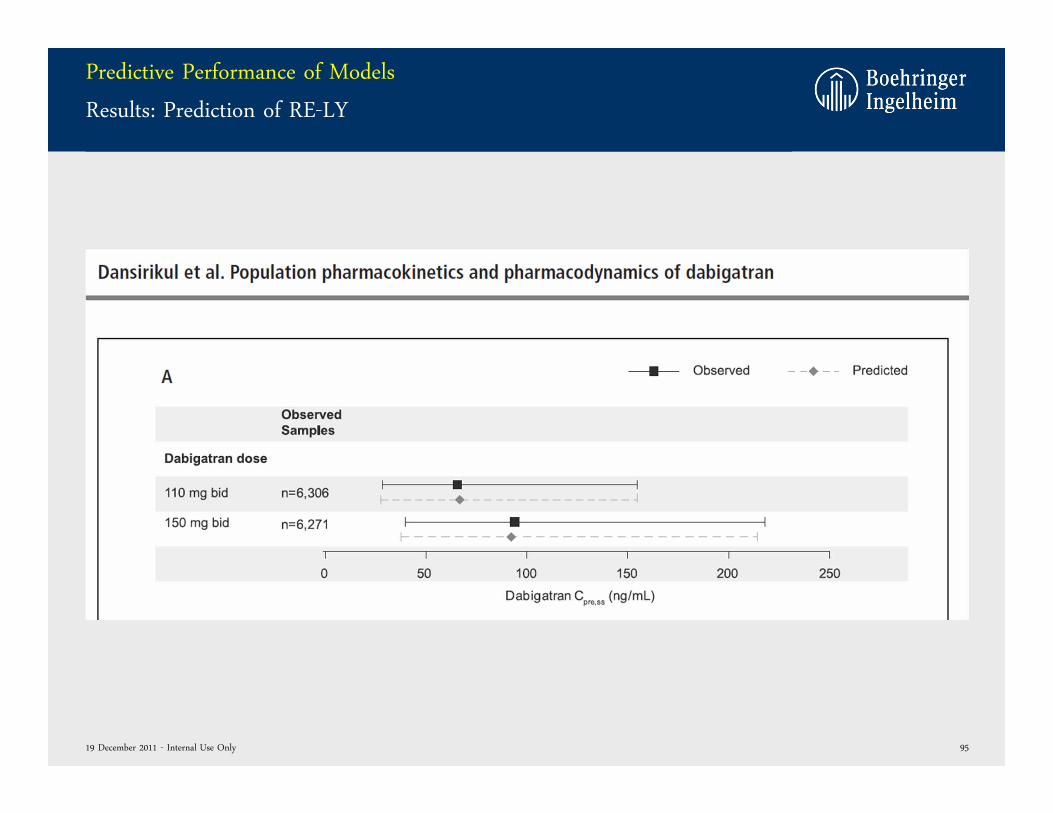
Predictive Performance of Models
Results: Prediction of RE-LY
9519 December 2011 - Internal Use Only
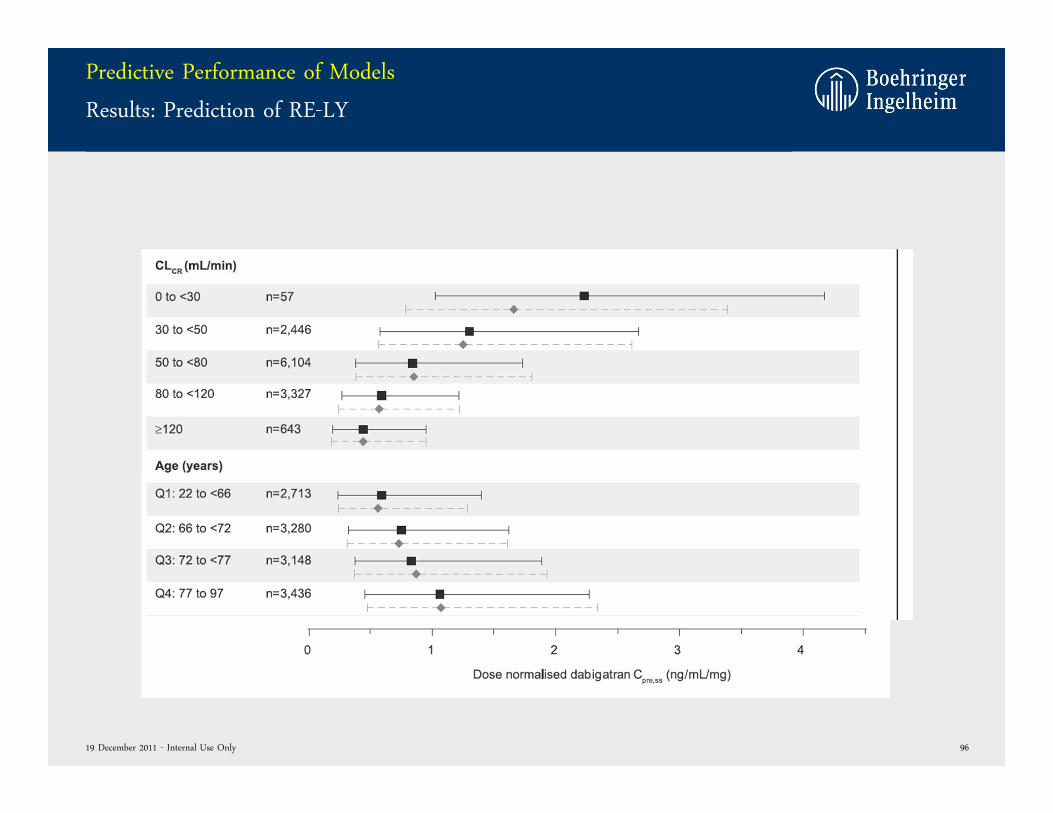
Predictive Performance of Models
Results: Prediction of RE-LY
9619 December 2011 - Internal Use Only
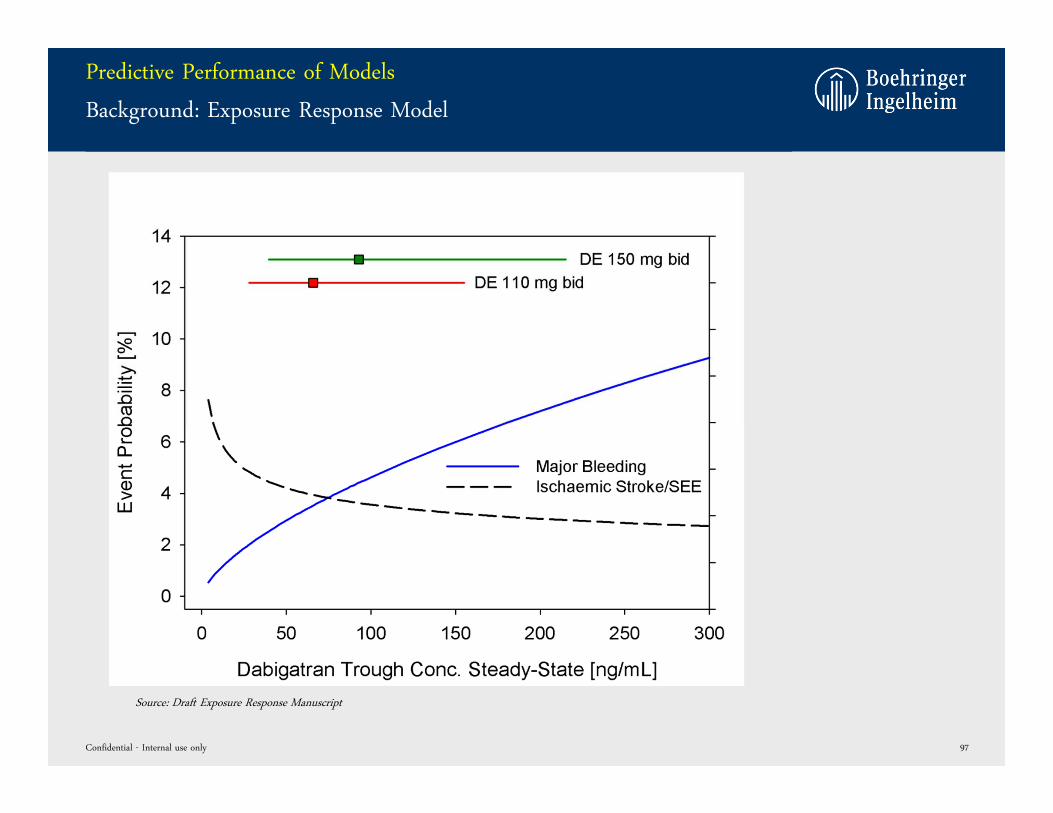
Predictive Performance of Models
Background: Exposure Response Model
Confidential - Internal use only 97
Source: Draft Exposure Response Manuscript
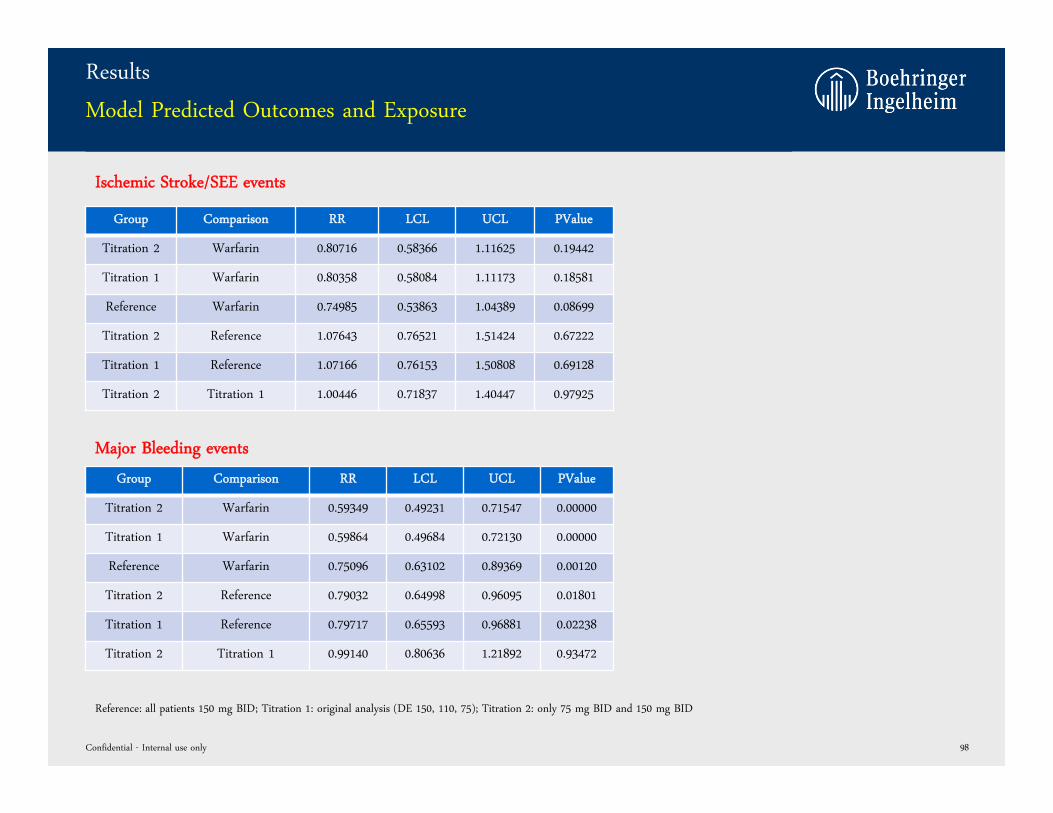
Results
Model Predicted Outcomes and Exposure
Confidential - Internal use only 98
Reference: all patients 150 mg BID; Titration 1: original analysis (DE 150, 110, 75); Titration 2: only 75 mg BID and 150 mg BID
Group Comparison RR LCL UCL PValue
Titration 2 Warfarin 0.80716 0.58366 1.11625 0.19442
Titration 1 Warfarin 0.80358 0.58084 1.11173 0.18581
Reference Warfarin 0.74985 0.53863 1.04389 0.08699
Titration 2 Reference 1.07643 0.76521 1.51424 0.67222
Titration 1 Reference 1.07166 0.76153 1.50808 0.69128
Titration 2 Titration 1 1.00446 0.71837 1.40447 0.97925
Group Comparison RR LCL UCL PValue
Titration 2 Warfarin 0.59349 0.49231 0.71547 0.00000
Titration 1 Warfarin 0.59864 0.49684 0.72130 0.00000
Reference Warfarin 0.75096 0.63102 0.89369 0.00120
Titration 2 Reference 0.79032 0.64998 0.96095 0.01801
Titration 1 Reference 0.79717 0.65593 0.96881 0.02238
Titration 2 Titration 1 0.99140 0.80636 1.21892 0.93472
Major Bleeding events
Ischemic Stroke/SEE events
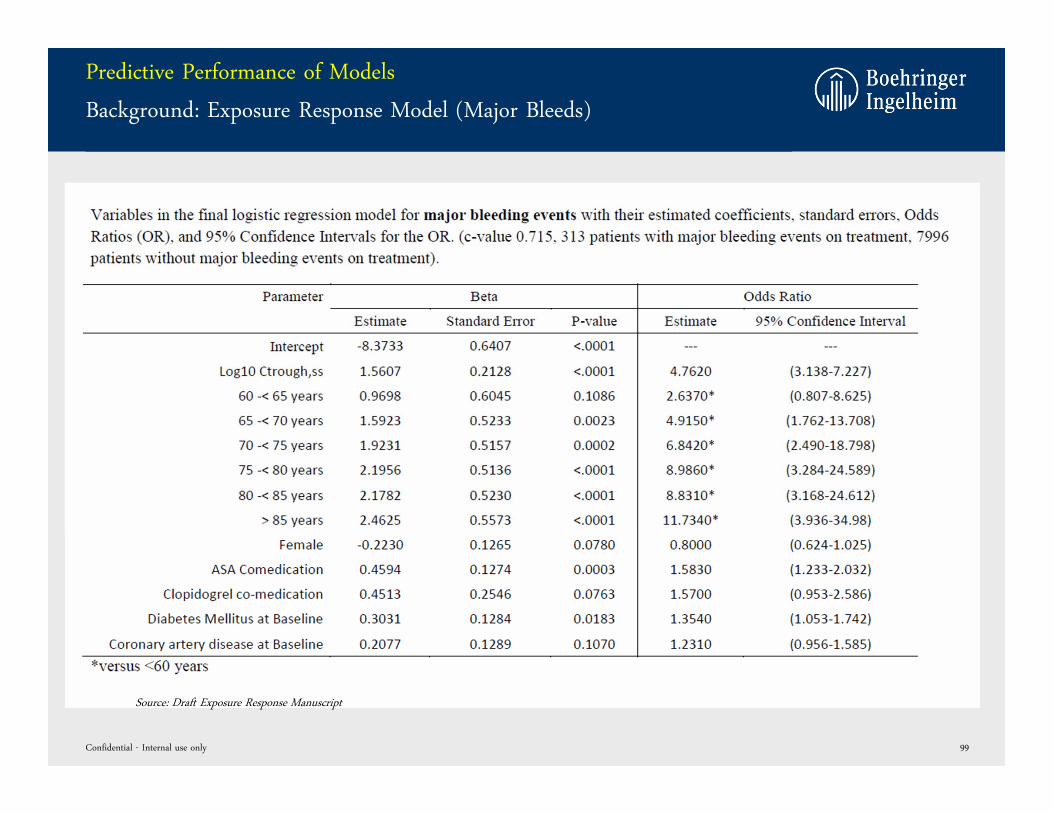
Predictive Performance of Models
Background: Exposure Response Model (Major Bleeds)
Confidential - Internal use only 99
Source: Draft Exposure Response Manuscript
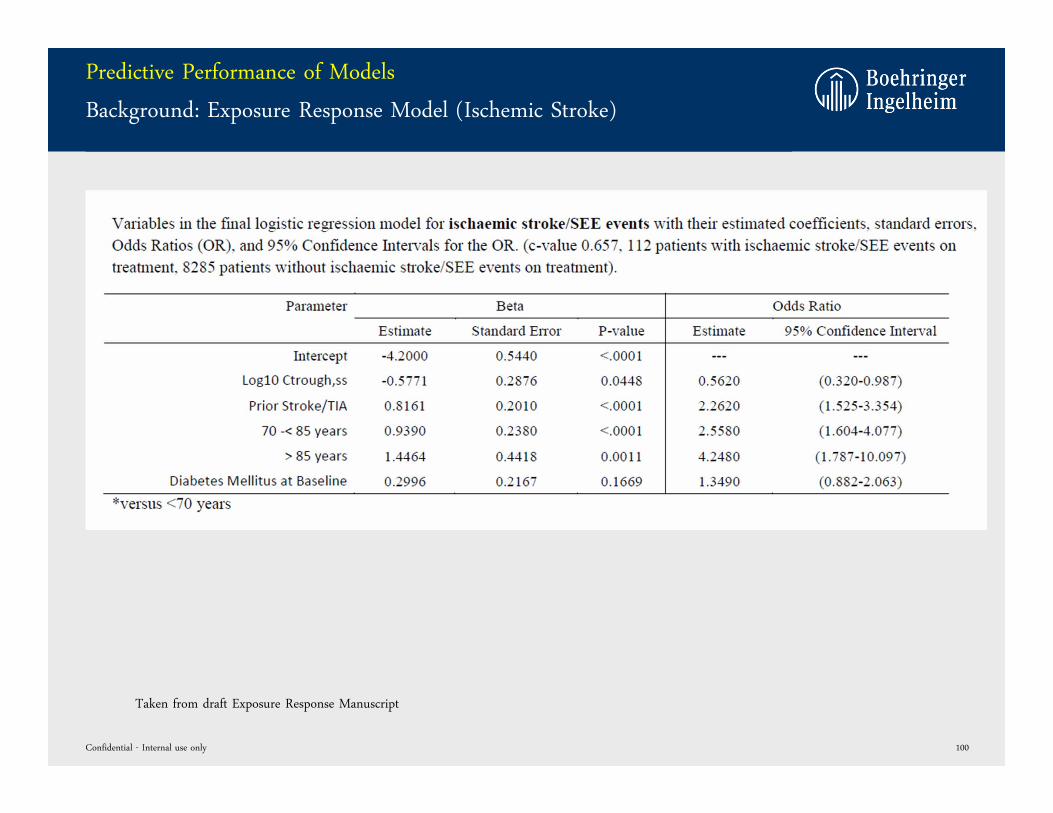
Predictive Performance of Models
Background: Exposure Response Model (Ischemic Stroke)
Confidential - Internal use only 100
Taken from draft Exposure Response Manuscript
RE-LY® Special AnalysisModelling vs. CHADS2 ≥ 3 or EU Label Recomm. Dosing
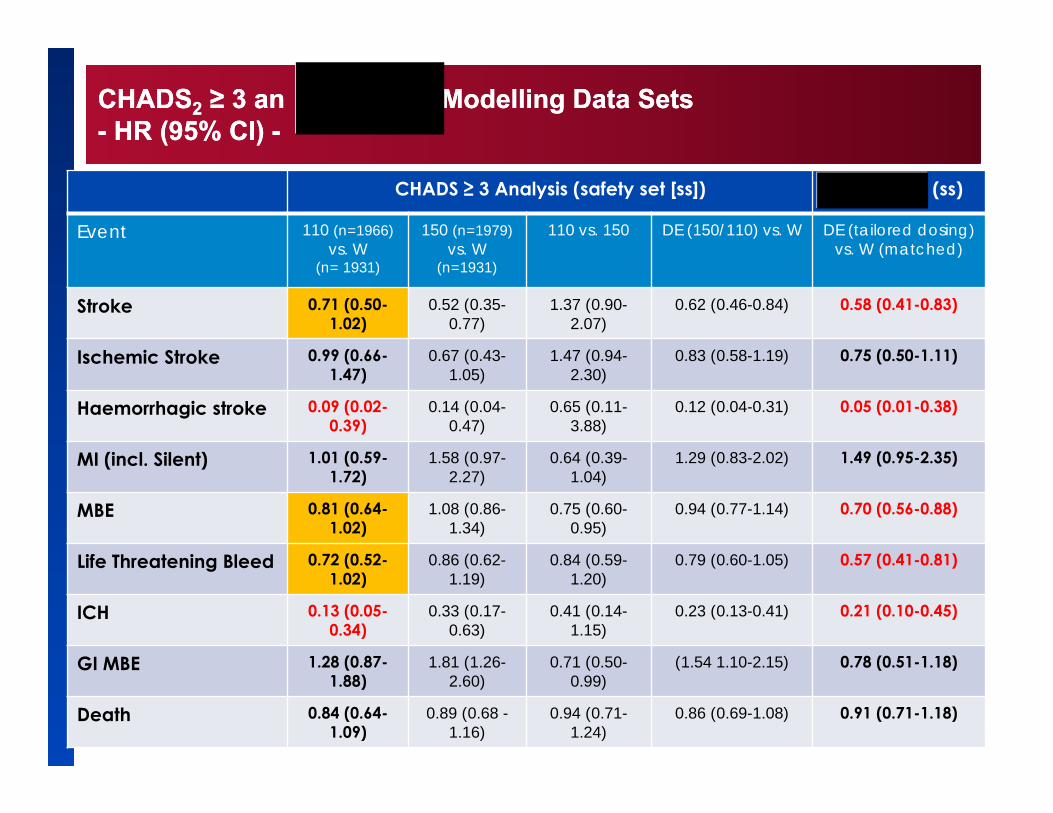
CHADS2 ≥ 3 an Modelling Data Sets- HR (95% CI) -CHADS2 ≥ 3 an Modelling Data Sets- HR (95% CI) -
CHADS ≥ 3 Analysis (safety set [ss]) (ss)
Event 110 (n=1966) vs. W
(n= 1931)
150 (n=1979) vs. W
(n=1931)
110 vs. 150 DE (150/110) vs. W DE (tailored dosing)vs. W (matched)
Stroke 0.71 (0.50-1.02)
0.52 (0.35-0.77)
1.37 (0.90-2.07)
0.62 (0.46-0.84) 0.58 (0.41-0.83)
Ischemic Stroke 0.99 (0.66-1.47)
0.67 (0.43-1.05)
1.47 (0.94-2.30)
0.83 (0.58-1.19) 0.75 (0.50-1.11)
Haemorrhagic stroke 0.09 (0.02-0.39)
0.14 (0.04-0.47)
0.65 (0.11-3.88)
0.12 (0.04-0.31) 0.05 (0.01-0.38)
MI (incl. Silent) 1.01 (0.59-1.72)
1.58 (0.97-2.27)
0.64 (0.39-1.04)
1.29 (0.83-2.02) 1.49 (0.95-2.35)
MBE 0.81 (0.64-1.02)
1.08 (0.86-1.34)
0.75 (0.60-0.95)
0.94 (0.77-1.14) 0.70 (0.56-0.88)
Life Threatening Bleed 0.72 (0.52-1.02)
0.86 (0.62-1.19)
0.84 (0.59-1.20)
0.79 (0.60-1.05) 0.57 (0.41-0.81)
ICH 0.13 (0.05-0.34)
0.33 (0.17-0.63)
0.41 (0.14-1.15)
0.23 (0.13-0.41) 0.21 (0.10-0.45)
GI MBE 1.28 (0.87-1.88)
1.81 (1.26-2.60)
0.71 (0.50-0.99)
(1.54 1.10-2.15) 0.78 (0.51-1.18)
Death 0.84 (0.64-1.09)
0.89 (0.68 -1.16)
0.94 (0.71-1.24)
0.86 (0.69-1.08) 0.91 (0.71-1.18)
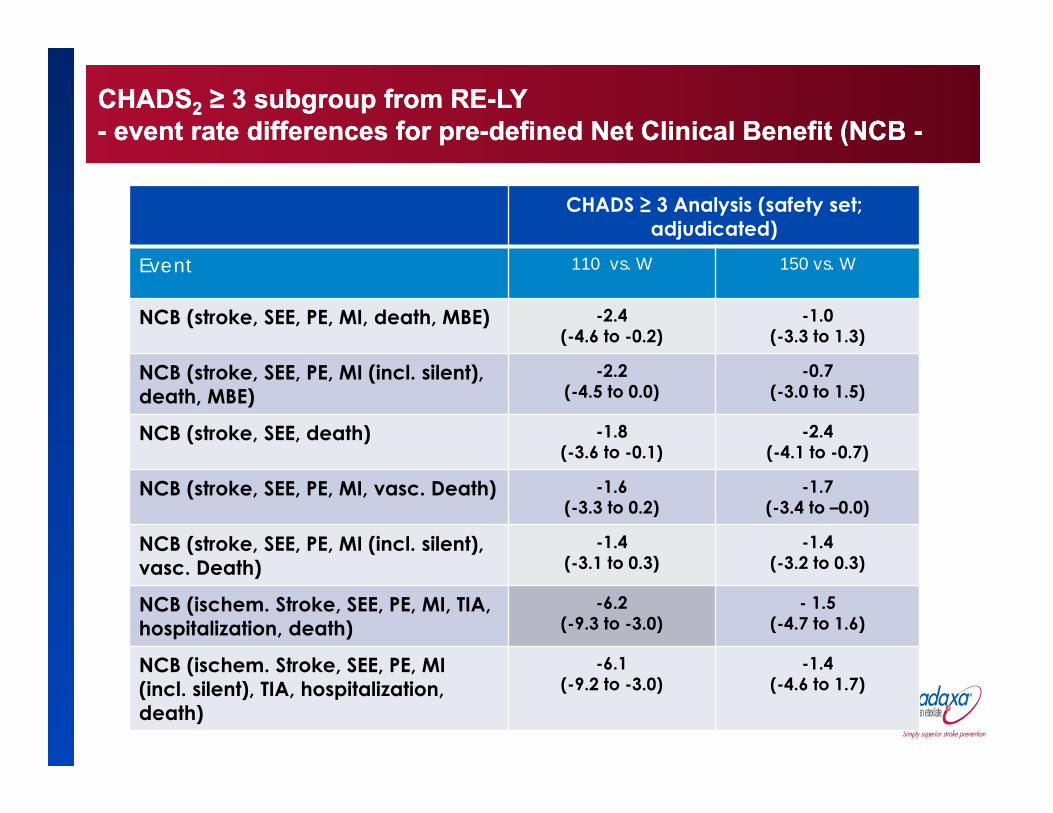
CHADS2 ≥ 3 subgroup from RE-LY- event rate differences for pre-defined Net Clinical Benefit (NCB -CHADS2 ≥ 3 subgroup from RE-LY- event rate differences for pre-defined Net Clinical Benefit (NCB -
CHADS ≥ 3 Analysis (safety set; adjudicated)
Event 110 vs. W 150 vs. W
NCB (stroke, SEE, PE, MI, death, MBE) -2.4 (-4.6 to -0.2)
-1.0(-3.3 to 1.3)
NCB (stroke, SEE, PE, MI (incl. silent), death, MBE)
-2.2 (-4.5 to 0.0)
-0.7(-3.0 to 1.5)
NCB (stroke, SEE, death) -1.8 (-3.6 to -0.1)
-2.4 (-4.1 to -0.7)
NCB (stroke, SEE, PE, MI, vasc. Death) -1.6 (-3.3 to 0.2)
-1.7 (-3.4 to –0.0)
NCB (stroke, SEE, PE, MI (incl. silent), vasc. Death)
-1.4 (-3.1 to 0.3)
-1.4 (-3.2 to 0.3)
NCB (ischem. Stroke, SEE, PE, MI, TIA, hospitalization, death)
-6.2(-9.3 to -3.0)
- 1.5 (-4.7 to 1.6)
NCB (ischem. Stroke, SEE, PE, MI (incl. silent), TIA, hospitalization, death)
-6.1 (-9.2 to -3.0)
-1.4 (-4.6 to 1.7)
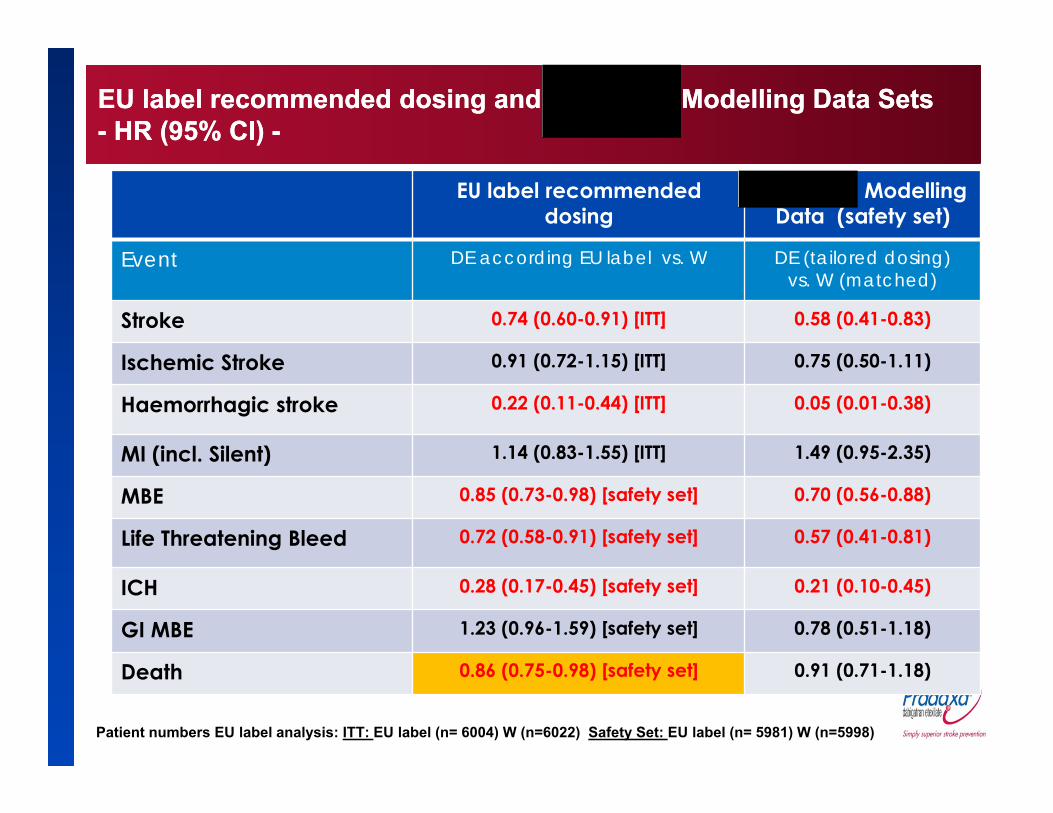
EU label recommended dosing and Modelling Data Sets - HR (95% CI) -EU label recommended dosing and Modelling Data Sets - HR (95% CI) -
EU label recommendeddosing
Modelling Data (safety set)
Event DE according EU label vs. W DE (tailored dosing)vs. W (matched)
Stroke 0.74 (0.60-0.91) [ITT] 0.58 (0.41-0.83)
Ischemic Stroke 0.91 (0.72-1.15) [ITT] 0.75 (0.50-1.11)
Haemorrhagic stroke 0.22 (0.11-0.44) [ITT] 0.05 (0.01-0.38)
MI (incl. Silent) 1.14 (0.83-1.55) [ITT] 1.49 (0.95-2.35)
MBE 0.85 (0.73-0.98) [safety set] 0.70 (0.56-0.88)
Life Threatening Bleed 0.72 (0.58-0.91) [safety set] 0.57 (0.41-0.81)
ICH 0.28 (0.17-0.45) [safety set] 0.21 (0.10-0.45)
GI MBE 1.23 (0.96-1.59) [safety set] 0.78 (0.51-1.18)
Death 0.86 (0.75-0.98) [safety set] 0.91 (0.71-1.18)
Patient numbers EU label analysis: ITT: EU label (n= 6004) W (n=6022) Safety Set: EU label (n= 5981) W (n=5998)




![Pradaxa · Pradaxa® [dabigatran etexilate] patient support booklet You have been given Pradaxa® to help reduce your risk of having a stroke due to atrial fibrillation](https://img.pdfslide.net/doc/110x75/5b0492937f8b9a89208ddebe/pradaxa-dabigatran-etexilate-patient-support-booklet-you-have-been-given-pradaxa.jpg)
























