Embed Size (px)
Citation preview
An Independent Assessment of the Health,Human Services, Cultural and EducationalNeeds of Montgomery County
David Barton Smith, PhDwith the assistance of Janet Davidson, MBA,David Ford, MA,Christopher Hopson, MA and David Laufe, MBA
Fox School of Business and Management, TempleUniversity
October 2006
SOUTHEASTERNREGION
2
TABLE OF CONTENTSPreface ....................................................................................................................................................3
Introduction............................................................................................................................................4
Quantitative Assessment ........................................................................................................................6
Environmental System ......................................................................................................................6
Healthcare System ............................................................................................................................7
Educational System ........................................................................................................................11
Criminal Justice System ..................................................................................................................12
Social Service System ......................................................................................................................13
Qualitative Assessment..........................................................................................................................16
Conclusions ..........................................................................................................................................27
Recommendations ................................................................................................................................29
Appendices
Appendix I. Demographic Changes 1990-2000 ......................................................................................................................................35
Appendix II. Detailed Demographic Profile 2000 ....................................................................................................................................37
TABLE OF CONTENTS
PREFACEPREFACE
3 Preface
The 10 organizations supporting this project careabout the health and social services needs ofMontgomery County residents and fund efforts toaddress them. We hope that others in the private,nonprofit, and public sectors will join us in using thisreport as a resource and in addressing some of thepriorities it identifies.
This report on the Southeast Region is anindependent assessment, authored by a research teamfrom Temple University under the direction of DavidBarton Smith, Ph.D., professor in the Department ofRisk, Insurance and Healthcare Management in theFox School of Business. It provides the opportunityto see ourselves as outsiders see us, both in terms ofour strengths and our challenges. We hope that it willhelp to stimulate productive conversations amongSoutheast region residents and the organizations thatserve them. Significant improvements will come onlythrough the combined efforts and resources of manyindividuals and organizations that share acommitment and special affection for MontgomeryCounty and its communities.
We are most appreciative of the help provided bymany people and organizations in the SoutheastRegion in the completion of this project. Manyprofessionals took the time out of their busy schedulesto participate in key informant sessions and provided
much insightful input. We would particularly like toacknowledge the assistance of Gail Wright, director ofCommunity Services for Bryn Mawr Hospital, andRuth Sperber, executive director of ElderNet. Theproduction of this report has been, in its broadestsense, a community affair. Thanks to all those in thatcommunity who assisted.
We look forward to continuing this effort together toimprove the health and quality of life in MontgomeryCounty, its regions and its communities.
Independence Foundation
Merck and Company Inc.
Montgomery County Foundation Inc.
Montgomery County Health and Human Services
North Penn United Way
North Penn Community Health Foundation
The Philadelphia Foundation
Phoenixville Community Health Foundation
United Way of Southeastern Pennsylvania
United Way of Western Montgomery County
INTRODUCTIONINTRODUCTION
4 Introduction
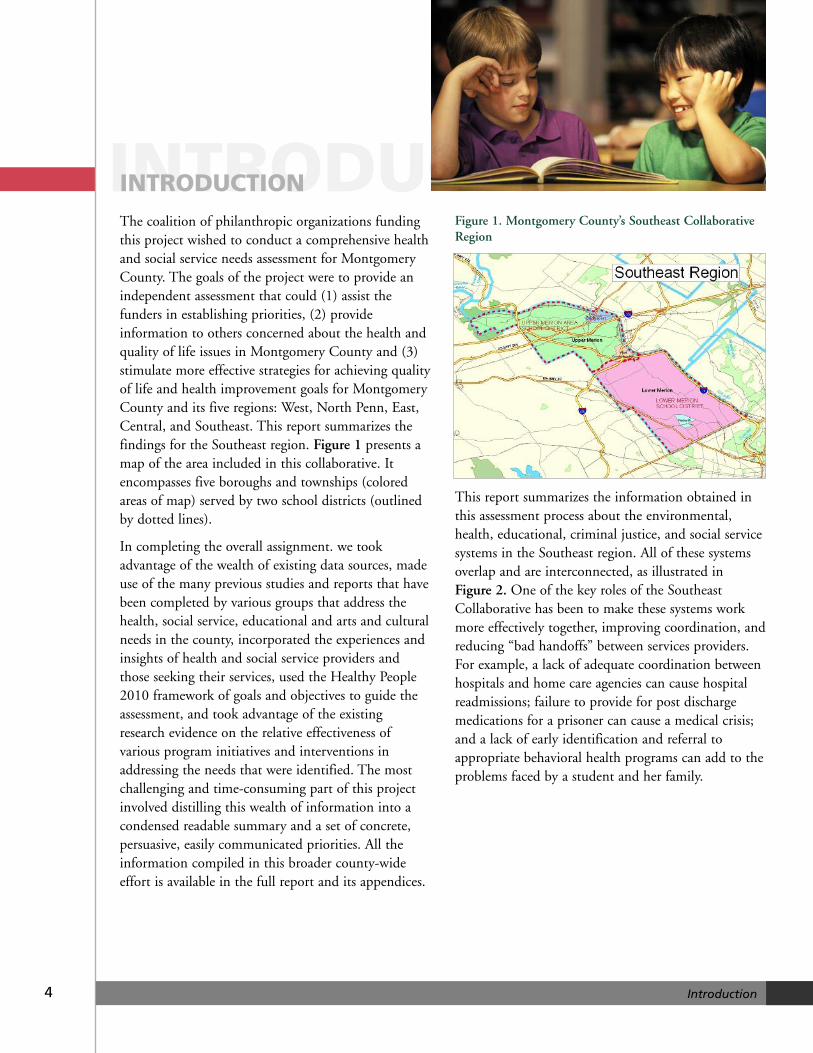
The coalition of philanthropic organizations fundingthis project wished to conduct a comprehensive healthand social service needs assessment for MontgomeryCounty. The goals of the project were to provide anindependent assessment that could (1) assist thefunders in establishing priorities, (2) provideinformation to others concerned about the health andquality of life issues in Montgomery County and (3)stimulate more effective strategies for achieving qualityof life and health improvement goals for MontgomeryCounty and its five regions: West, North Penn, East,Central, and Southeast. This report summarizes thefindings for the Southeast region. Figure 1 presents amap of the area included in this collaborative. Itencompasses five boroughs and townships (coloredareas of map) served by two school districts (outlinedby dotted lines).
In completing the overall assignment. we tookadvantage of the wealth of existing data sources, madeuse of the many previous studies and reports that havebeen completed by various groups that address thehealth, social service, educational and arts and culturalneeds in the county, incorporated the experiences andinsights of health and social service providers andthose seeking their services, used the Healthy People2010 framework of goals and objectives to guide theassessment, and took advantage of the existingresearch evidence on the relative effectiveness ofvarious program initiatives and interventions inaddressing the needs that were identified. The mostchallenging and time-consuming part of this projectinvolved distilling this wealth of information into acondensed readable summary and a set of concrete,persuasive, easily communicated priorities. All theinformation compiled in this broader county-wideeffort is available in the full report and its appendices.
Figure 1. Montgomery County’s Southeast CollaborativeRegion
This report summarizes the information obtained inthis assessment process about the environmental,health, educational, criminal justice, and social servicesystems in the Southeast region. All of these systemsoverlap and are interconnected, as illustrated in Figure 2. One of the key roles of the SoutheastCollaborative has been to make these systems workmore effectively together, improving coordination, andreducing “bad handoffs” between services providers.For example, a lack of adequate coordination betweenhospitals and home care agencies can cause hospitalreadmissions; failure to provide for post dischargemedications for a prisoner can cause a medical crisis;and a lack of early identification and referral toappropriate behavioral health programs can add to theproblems faced by a student and her family.
5
Figure 2. Systems Addressing the Needs of MontgomeryCounty Residents
This report first supplies a brief statistical summary ofwhat can be measured at the regional level about theperformance of each of these systems. It then providesa qualitative assessment of the performance of each ofthese systems through the insights of key informantdiscussion groups that were interviewed for theproject. The final section summarizes and makesrecommendations about the most important prioritiesthat need to be addressed.
Introduction
6
Environmental SystemFor our purposes, the “environment” includes all thosecharacteristics of the Southeast region that shape thecontext in which the healthcare, educational, criminaljustice and social service systems operate. Thatincludes the physical environment, demographic, andsocial and cultural characteristics that shape the needsfor services within the healthcare, educational,criminal justice, and social service systems.
Physical Environment
The Southeastern region is bordered by Valley ForgeNational Park and the King of Prussia Mall to itsnorth and the Schuylkill River to its east, DelawareCounty to its west, and Philadelphia to its south. Oneof the older Philadelphia suburbs for the city’saffluent, it is connected to the city by the R5 rail lineand insulated from the rest of the county. Four sites,two in Upper Merion and two in King of Prussia, arefederal Environmental Protection Agency superfundsites. There are a total of 17 superfund sites inMontgomery County, the largest number of anycounty in Pennsylvania.
Demographics
The Southeast region, with a total population of96,763 in 2000, is one of the more densely populatedand least rapidly growing regions of the county.Addressing both the threats and taking advantage ofthe opportunities those changes pose should be amajor focus of the Southeast Collaborative. Thosechanges include the following:
• Mature population. The Southeast region grewonly 3.3 percent, matching that of Pennsylvaniaas a whole. There was a 4.9 percent decline inthe under-five population and a 5.5 percentdecline in the 25-40 year old population,
matched with by a 14.5 percent increase in the75-84 population, and a 45.3 percent increase inthe over-85 population.
• Affluent and most educated. The region has thehighest percent of person people over 25 with abachelor’s degree or a higher professional degree:59 percent. Twenty percent of the householdshave incomes of $150,000 or more, more thantwice the percent in any other region of thecounty. Yet, 4.2 percent of individuals in theSoutheast region, in all age groups, are living inpoverty and that rate has increased since 1990.
• Growing diversity. The Asian population hasdoubled in size and the small Hispanicpopulation has increased 39 percent. Themajority of the Asians are either from India orChina, and Asians account for 4.7 percent of thepopulation of the region. The African Americanpopulation grew 12 percent, and AfricanAmericans account for 4.3 percent of the region’spopulation.
More detail about the demographic changes in theregion between 1990 and 2000 is provided inAppendix I.
The 2000 census provides some numbers about thesize of the population with special needs in the regionthat are useful in thinking about services.
• 5.2 percent (994) of those 5 to 20 years of age,9.7 percent (5,434) of those age 21 to 64, and29 percent (4,581) of those over the age of 65have a disability.
• 315 grandparents serve as primary care givers fortheir grandchildren.
• 2,616 (2.9 percent) persons over five years of agehave limited English proficiency.
QUANTITATIVEASSESSMENTQUANTITATIVEASSESSMENT
Quantitative Assessment
• 5.2 percent (4073) of persons in the civilianlabor force were unemployed.
• 1.9 percent (472) of families live below thepoverty level.
• 5.9 percent (2,277) of households have nomotor vehicle available.
• 31.7. percent (3,463) of renter-occupiedhouseholds and 21.4 percent (5,049) of owner-occupied households spend more than 30percent of their income on housing costs,passing beyond the threshold of what is generallydefined as affordable housing.
More detail on the demographic profile of theSoutheast region in 2000 is provided in Appendix II.
Arts and Culture
The Southeast region of Montgomery County shapesthe arts and cultural environment of the Philadelphiametropolitan area. It encompasses the largestconcentration of private liberal arts colleges in thearea. Its residents include major supporters and boardmembers of most of the Philadelphia area arts andcultural institutions. The relocation of its BarnesFoundation collection, a world treasure, has been thefocus of international attention. Such local institutionsas the Main Line Art Center and the Bryn Mawr FilmInstitute draw participants of all ages and from all overthe metropolitan area.
Healthcare System
Resources
• The combined 634 licensed acute hospital bedof Lankenau and Bryn Mawr Hospital translateinto a bed-to-population ratio for the region of6.5 beds per 1,000 population, in contrast to 2.5beds per 1,000 Montgomery County and 2.7 forPennsylvania
• The 151-bed Bryn Mawr RehabilitationHospital provides the only resource of its kind inthe county.
• The region is well supplied with specialists and,overall, the region is served by almost 1,000
physicians. This translated into a physicianpopulation ratio more than three times that forPennsylvania as a whole.
• In contrast to the Western, North Penn andCentral regions of the county, the Southeasternregion is a net exporter of specialty physicianand acute hospital services
As described in the full report, lack of access to goodprimary care can increase rates of preventable hospitaladmissions, and lack of access to adequate care afterhospital discharge can increase the rates of hospitalreadmissions. The costs of these preventableadmissions and readmissions probably far exceed thecost of providing adequate primary care and postdischarge services. (See discussion of the PennsylvaniaHealth Care Cost Containment Council estimates inthe full county report). The Southeastern region iswell supplied with primary care and post-hospitaldischarge services.
Health, Access, and Behavioral RiskProblems in the Central Region
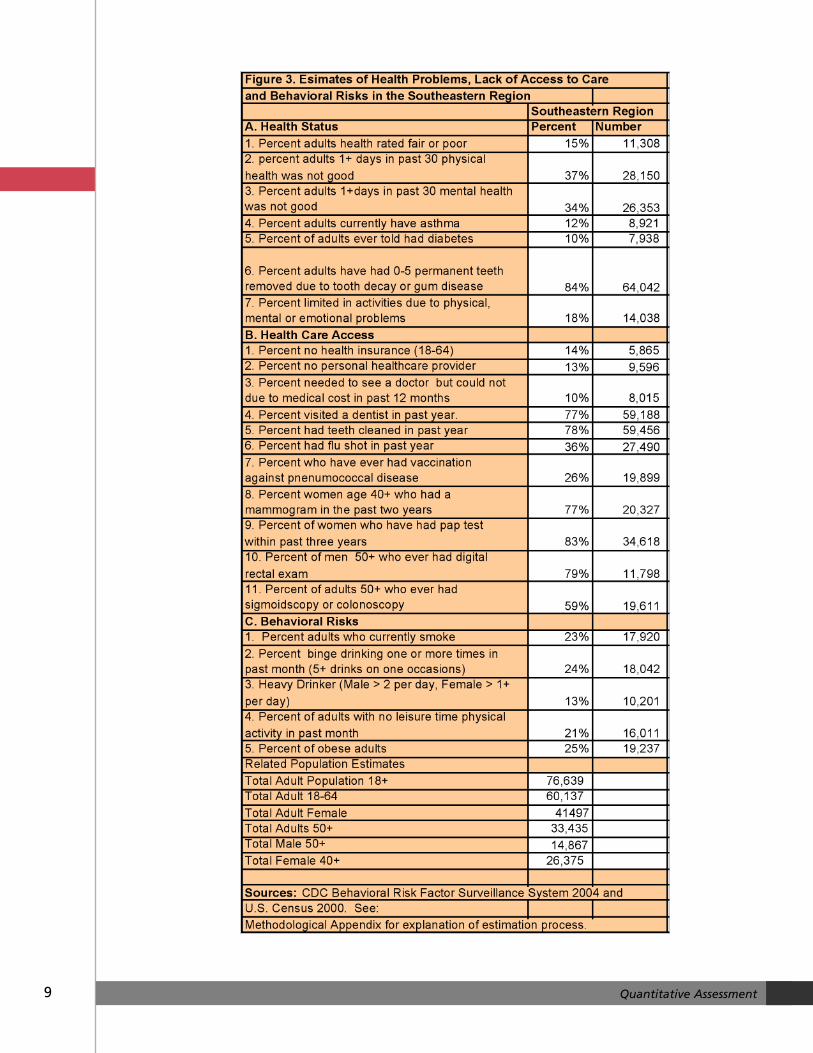
Figure 3 provides estimates based on the statewideCenters for Disease Control’s 2004 Behavioral RiskFactor Survey (BRFS) conducted by the PennsylvaniaDepartment of Health. We have selected 23 keyindicators of health, access and behavioral riskproblems. Income and age have large effects on theseindicators in a population. We have used 2000 censusestimates of age and income in the region to createestimates of the value of these indicators for the regionas a whole. Our estimates suggest the following:
• 15 percent (11,308) of the region’s populationover the age of 18 would rate their health fair orpoor and 37 percent (28,150) had one or moredays in the past 30 when their health was notgood.
• 10 percent (7,938) of adults in the region havebeen told at some time they had diabetes, and12 percent (8,921) have been told that they haveasthma. Prevalence rates among children wouldbe expected to be roughly comparable andhigher in the lower income population. Asthma-related childhood hospitalization and death ratesin lower income neighborhoods in the UnitedStates have risen.
7 Quantitative Assessment
8 Quantitative Assessment
• 16 percent (12,597) of adults in the region havelost more than five of their permanent teeth dueto tooth decay or gum disease, while 23 percent(17,541) have not visited a dentist in the pastyear.
• 14 percent (5,865) of adults between the age of18 and 65 in the region have no healthinsurance, 13 percent (9,596) of adults have nopersonal healthcare provider and 10 percent(8,015) chose not to see a physician when theyneeded to in the last year because of cost.
• 23 percent (56,048) of women over the age of40 have not had a mammogram in the past twoyears, 17 percent (6,879) of adult women havenot had a pap test within the past three years, 21percent (1,635) of men over the age of 50 have
never had a digital rectal exam, and 41 percent(13,824)) of adults over 50 have never had asigmoidscopy or colonoscopy.
• 23 percent (17,920) of adults currently smoke,24 percent (18,042) binge drink, 21 percent(16,011) did not participate in any leisure timephysical activity in the last month, and 25percent (19,237) are obese. According to the2003 Pennsylvania Youth Survey, about 25percent of high school seniors report currentlysmoking and 31 percent report binge drinking,and the rates in the Southeast region areprobably roughly comparable.
• Estimates for all of these indicators are somewhatbetter for the Southeastern region than for thecounty as a whole.
9 Quantitative Assessment
Birth and Death Outcomes
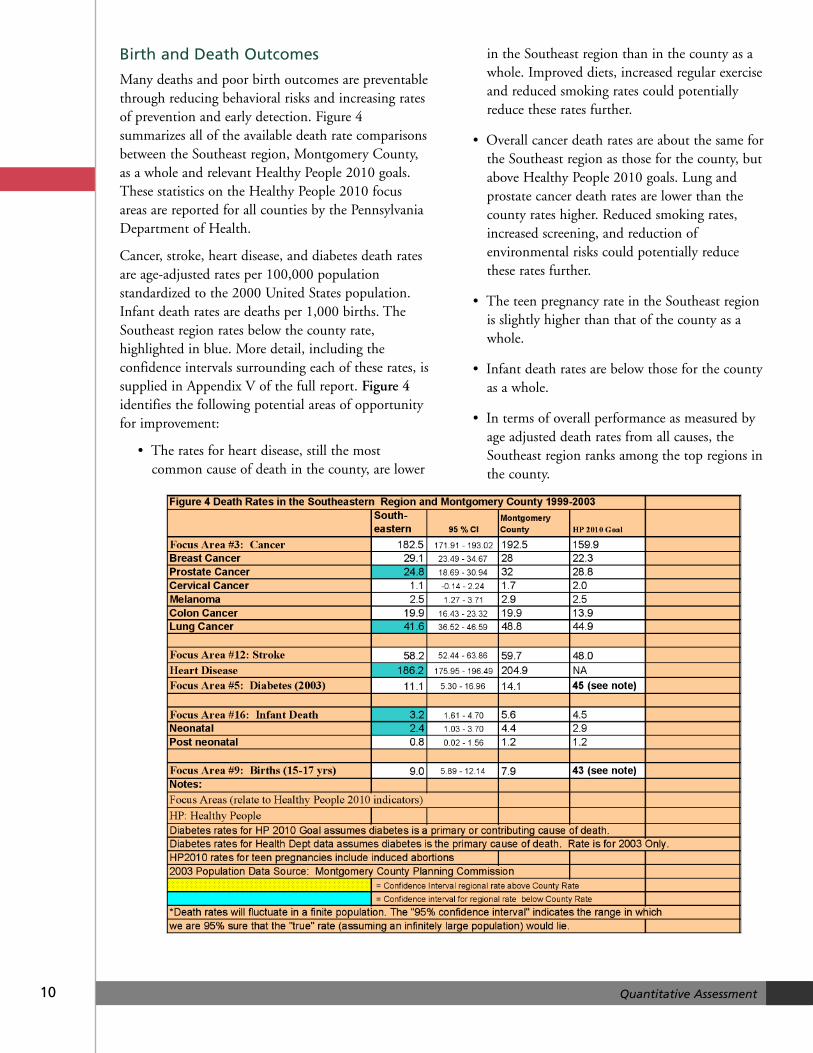
Many deaths and poor birth outcomes are preventablethrough reducing behavioral risks and increasing ratesof prevention and early detection. Figure 4summarizes all of the available death rate comparisonsbetween the Southeast region, Montgomery County,as a whole and relevant Healthy People 2010 goals.These statistics on the Healthy People 2010 focusareas are reported for all counties by the PennsylvaniaDepartment of Health.
Cancer, stroke, heart disease, and diabetes death ratesare age-adjusted rates per 100,000 populationstandardized to the 2000 United States population.Infant death rates are deaths per 1,000 births. TheSoutheast region rates below the county rate,highlighted in blue. More detail, including theconfidence intervals surrounding each of these rates, issupplied in Appendix V of the full report. Figure 4identifies the following potential areas of opportunityfor improvement:
• The rates for heart disease, still the mostcommon cause of death in the county, are lower
in the Southeast region than in the county as awhole. Improved diets, increased regular exerciseand reduced smoking rates could potentiallyreduce these rates further.
• Overall cancer death rates are about the same forthe Southeast region as those for the county, butabove Healthy People 2010 goals. Lung andprostate cancer death rates are lower than thecounty rates higher. Reduced smoking rates,increased screening, and reduction ofenvironmental risks could potentially reducethese rates further.
• The teen pregnancy rate in the Southeast regionis slightly higher than that of the county as awhole.
• Infant death rates are below those for the countyas a whole.
• In terms of overall performance as measured byage adjusted death rates from all causes, theSoutheast region ranks among the top regions inthe county.
10 Quantitative Assessment
Educational System
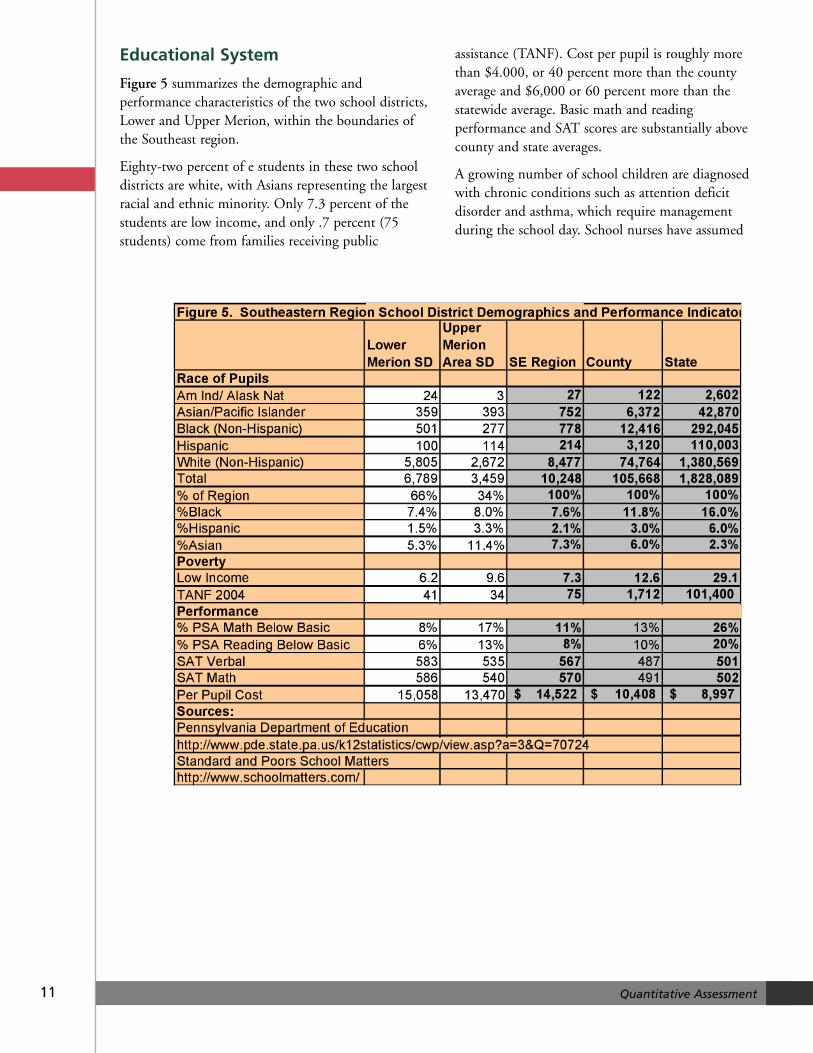
Figure 5 summarizes the demographic andperformance characteristics of the two school districts,Lower and Upper Merion, within the boundaries ofthe Southeast region.
Eighty-two percent of e students in these two schooldistricts are white, with Asians representing the largestracial and ethnic minority. Only 7.3 percent of thestudents are low income, and only .7 percent (75students) come from families receiving public
assistance (TANF). Cost per pupil is roughly morethan $4.000, or 40 percent more than the countyaverage and $6,000 or 60 percent more than thestatewide average. Basic math and readingperformance and SAT scores are substantially abovecounty and state averages.
A growing number of school children are diagnosedwith chronic conditions such as attention deficitdisorder and asthma, which require managementduring the school day. School nurses have assumed
11 Quantitative Assessment
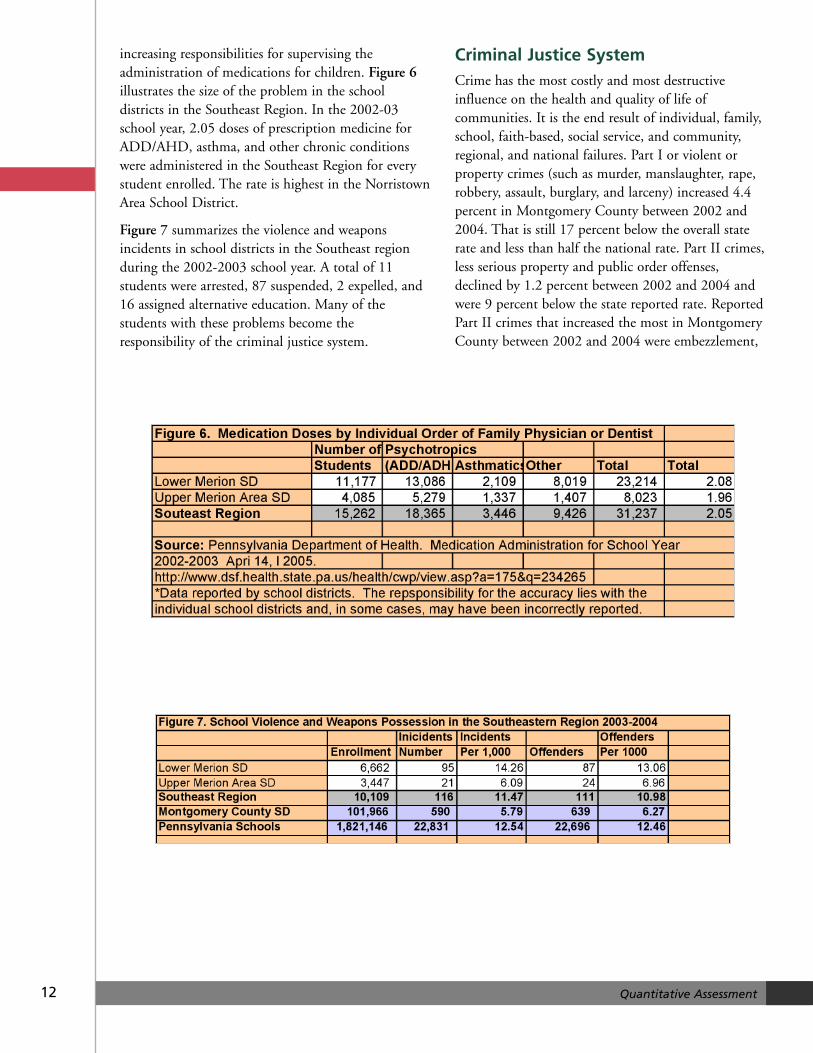
increasing responsibilities for supervising theadministration of medications for children. Figure 6illustrates the size of the problem in the schooldistricts in the Southeast Region. In the 2002-03school year, 2.05 doses of prescription medicine forADD/AHD, asthma, and other chronic conditionswere administered in the Southeast Region for everystudent enrolled. The rate is highest in the NorristownArea School District.
Figure 7 summarizes the violence and weaponsincidents in school districts in the Southeast regionduring the 2002-2003 school year. A total of 11students were arrested, 87 suspended, 2 expelled, and16 assigned alternative education. Many of thestudents with these problems become theresponsibility of the criminal justice system.
Criminal Justice SystemCrime has the most costly and most destructiveinfluence on the health and quality of life ofcommunities. It is the end result of individual, family,school, faith-based, social service, and community,regional, and national failures. Part I or violent orproperty crimes (such as murder, manslaughter, rape,robbery, assault, burglary, and larceny) increased 4.4percent in Montgomery County between 2002 and2004. That is still 17 percent below the overall staterate and less than half the national rate. Part II crimes,less serious property and public order offenses,declined by 1.2 percent between 2002 and 2004 andwere 9 percent below the state reported rate. ReportedPart II crimes that increased the most in MontgomeryCounty between 2002 and 2004 were embezzlement,
12 Quantitative Assessment
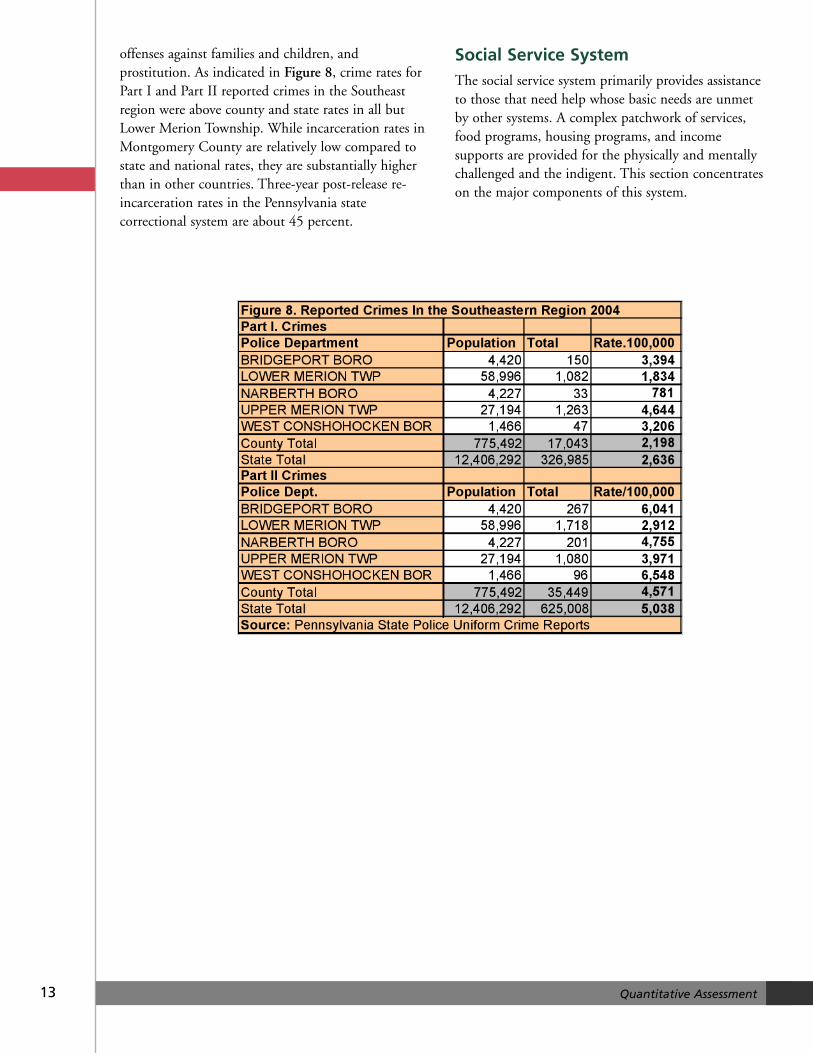
offenses against families and children, andprostitution. As indicated in Figure 8, crime rates forPart I and Part II reported crimes in the Southeastregion were above county and state rates in all butLower Merion Township. While incarceration rates inMontgomery County are relatively low compared tostate and national rates, they are substantially higherthan in other countries. Three-year post-release re-incarceration rates in the Pennsylvania statecorrectional system are about 45 percent.
Social Service SystemThe social service system primarily provides assistanceto those that need help whose basic needs are unmetby other systems. A complex patchwork of services,food programs, housing programs, and incomesupports are provided for the physically and mentallychallenged and the indigent. This section concentrateson the major components of this system.
13 Quantitative Assessment
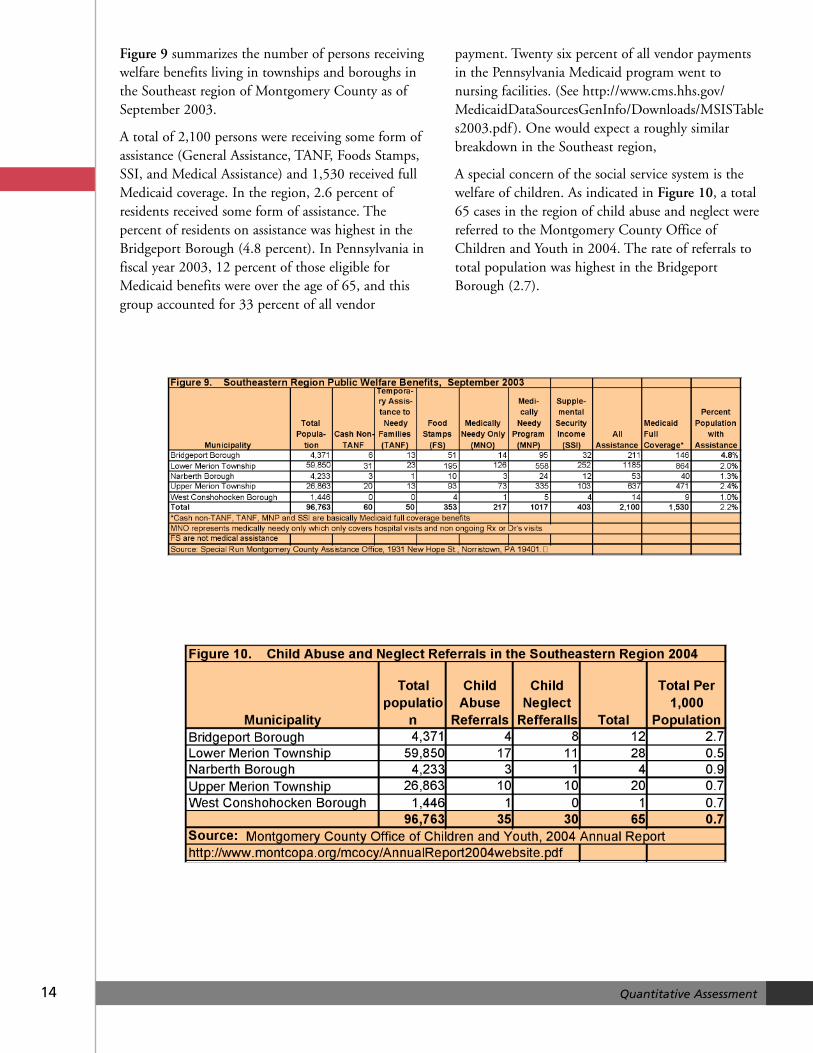
Figure 9 summarizes the number of persons receivingwelfare benefits living in townships and boroughs inthe Southeast region of Montgomery County as ofSeptember 2003.
A total of 2,100 persons were receiving some form ofassistance (General Assistance, TANF, Foods Stamps,SSI, and Medical Assistance) and 1,530 received fullMedicaid coverage. In the region, 2.6 percent ofresidents received some form of assistance. Thepercent of residents on assistance was highest in theBridgeport Borough (4.8 percent). In Pennsylvania infiscal year 2003, 12 percent of those eligible forMedicaid benefits were over the age of 65, and thisgroup accounted for 33 percent of all vendor
payment. Twenty six percent of all vendor paymentsin the Pennsylvania Medicaid program went tonursing facilities. (See http://www.cms.hhs.gov/MedicaidDataSourcesGenInfo/Downloads/MSISTables2003.pdf ). One would expect a roughly similarbreakdown in the Southeast region,
A special concern of the social service system is thewelfare of children. As indicated in Figure 10, a total65 cases in the region of child abuse and neglect werereferred to the Montgomery County Office ofChildren and Youth in 2004. The rate of referrals tototal population was highest in the BridgeportBorough (2.7).
14 Quantitative Assessment
15 Quantitative Assessment
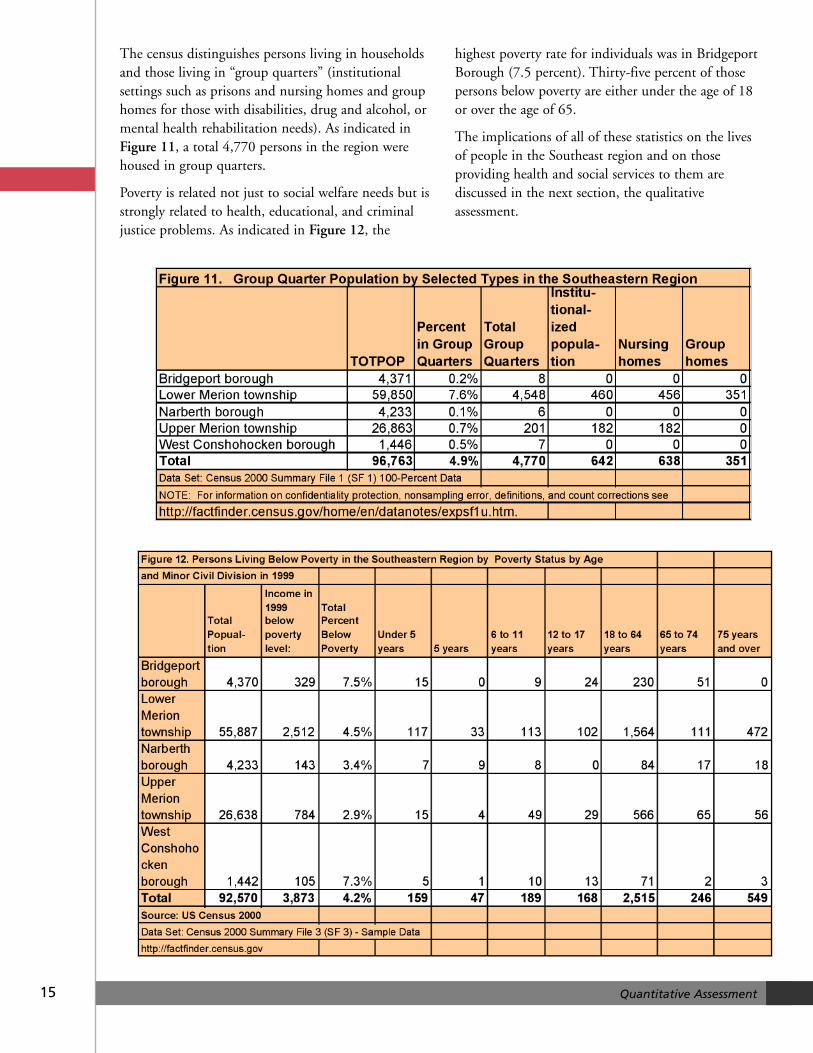
The census distinguishes persons living in householdsand those living in “group quarters” (institutionalsettings such as prisons and nursing homes and grouphomes for those with disabilities, drug and alcohol, ormental health rehabilitation needs). As indicated inFigure 11, a total 4,770 persons in the region werehoused in group quarters.
Poverty is related not just to social welfare needs but isstrongly related to health, educational, and criminaljustice problems. As indicated in Figure 12, the
highest poverty rate for individuals was in BridgeportBorough (7.5 percent). Thirty-five percent of thosepersons below poverty are either under the age of 18or over the age of 65.
The implications of all of these statistics on the livesof people in the Southeast region and on thoseproviding health and social services to them arediscussed in the next section, the qualitativeassessment.
QUALITATIVE ASSESSMENTQUALITATIVEASSESSMENTThe qualitative assessment involved listening to peoplerepresenting all the different perspectives touched onby the statistics in the previous section. Thirteenseparate hour-and-a-half group discussions were heldwith key service providers in these different areas. TheSoutheast Regional Collaborative assisted in selectingthe participants and hosting the sessions. A total ofmore than 50 professionals participated in thesesessions.
Session 1: Home Health
The participants included seven representatives ofhospitals and home care organizations.
When asked about the positive and unique aspects ofthe region, the participants said that diabeteseducation, resources and support funded by the BrynMawr Hospital Foundation was very valuable. Onefor-profit home health organization prided itself onkeeping rates as low as possible and providing“scholarships” for people who cannot afford care.Nurses are well organized into teams and meet patientneeds in all areas except in psychiatry. There areinpatient hospice care and chronic care teams.
Issues
Medical services. The working poor [Medicaidineligibles] need medical homes and longer range care,particularly for psychiatric services. There is a high rateof binge drinking in the over-65 population resulting inminor (car) accidents, slip-and-fall incidents, andacceleration of general disease. Another issue is thatLower Merion Township has one of the highest rates ofbreast cancer (and associated deaths) in the UnitedStates. Dental care is needed among those withoutresources and dental insurance. People are aging in placeand more support is needed for them.
Transportation. Emergency Medical Technicians assessand sometimes deny (paid) transportation to thehospital. Emergency Medical Services (EMS) will notbe reimbursed for transport to a doctor’s office underMedicare rules. A bad option is a “social service”admission to the hospital, which sometimes happens.
Coordination of care (for the elderly). Patients arereleased too quickly from the hospital and too late inthe day (sometimes as late as midnight). Workingfamilies cannot take care of their elderly. One nursemade a home visit at 1:00 a.m. People needinformation, medications, and other auxiliary carewhen they are discharged. Some families think thataids from home care agencies or hospice care staff willcome and stay with their family member while theygo to work.
Technology. There are electronic medical records butthe computers aren’t linked. This is not a HealthInsurance Portability and Accountability Act (HIPPA)issue but a really burdensome problem for nurses.Some people are using USB drives to carry theirmedical records.
Advance directives. Many people are aware of thembut they need to be on standardized forms and widelydistributed. The primary care provider should discussthis difficult matter with the patient. Hospital staffoften finds that medical information is incorrect orcontradictory. There are significant barriers. Some arecultural or religious, and the forms are confusing.Education is needed about what a hospice can andcannot do, as well as other end-of-life issues. Aphysician can be the barrier to moving people intoend-of-life care. They suggested using FILE of LIFEon the refrigerator, which comes with a windowsticker (like ChildFind). Hospice care doesn’t require aspecific Do Not Resuscitate (DNR) order. In nursing
16 Qualitative Assessment

homes, when they call 911 the paramedics must“work the code.” Bracelets that list all relevant DNRinformation are available in Pennsylvania.
Information. An information center and website isneeded for the entire region. It should show the name,phone number, and services an organization provides.
The participants suggested that community educationabout end-of-life issues would help enhancecommunity knowledge. They suggested that animproved information system would help the workingpoor and underinsured identify services for home care,dental care, and mental health services.
Session 2: Wellness
The participants included representatives from seniorservices, a hospital administrator, fitness instructors,representatives from a women’s center, and someoneworking with victims of domestic violence.
When asked about the positive and unique aspects ofthe region, the participants said that there are manysocial services available in the region. These include ahigh-quality pre-K program that is used at some sitesabout “words can hurt as much as our hands.” Thereis a 24-hour domestic violence hotline; the police offervictims information and a women’s center will contactthem within 24 hours. Pottstown police have a socialworker screening domestic violence calls. Police aretrained during role call to address domestic violenceissues. There is a Yellow Dress presentation in school;it is a reenactment of the story of a girl killed thenight before her prom; facilitators lead follow upclassroom discussions. There are healthy relationshipworkshops at the colleges even though campus policedo not want to deal with domestic violence issues.
The senior center Ask-a-Nurse program has caughtheart attacks, strokes, and infections. Congregational(parish) nurses provided the same services until thefunding was cut. There was also a workshop onmedical errors. People were given Take-Me-to-Your-Dr. brown bags that they were to fill with theirmedications when they visited the doctor. There areprograms to incorporate fitness and wellness intopeople’s lives and collaboration with Blue Cross forpeople who cannot afford it.
There is a Telephone Reassurance Line, a volunteerContact Care Line, and a follow-up to home healthcare. The follow-up is a weekly or daily call at thesame time each day that continues until the person isreached; if not, the police are called. They have beentrying to implement it countywide because theworking poor cannot afford the service. Mail carriersare trained to recognize that that mail hasn’t beenpicked up. “Some people will call the post office andask the post office to keep an eye on their elderly or illfriends and relatives. We heard about one postalworker was doing the bills for an elderly woman.Another time, the postmaster from Haverford calledabout a woman from Chester County who picked upmail in the post office dressed in a black plastic trashbag. She was in bad shape under the bag, and theyhelped her. “The Main Line has a lot of sick, stubbornpeople.”
The participants said that it was important to facilitatenurse home visits and expedite needed services. Theysuggested that the community would be well servedthrough health education, outreach, and servicecoordination. They suggested that schools should postwellness and fitness information on school websites aswell as sending the information home. They alsowould like to see more support for school nurses whogather information and send it to parents. Theymentioned that the domestic violence coloring booksfor children are costly but very useful.
Session 3: Discharge Planners
The participants included representatives oforganizations providing support to parents, andpeople making home visits to new parents, the elderlyand the homebound.
When asked about the positive and unique aspects ofthe region, the participants said that there arecommunity partnerships that include a communityadvisory council (in existence for six years) thatsupports networking among agencies. Healthadvocates are available to provide information topregnant and parenting women in laymen’s terms. Thenumbers of healthy births and good outcomes haveincreased. Outreach workers have eliminated barriersto accessing OB and pediatric services. A FamilyService Plan provides information about healthy
17 Qualitative Assessment

babies, life skills, and dads’ participation. Children’sHealth Insurance Plan (CHIP) enrollment helpsprovide pediatric care.
Although the numbers of meals-on-wheels deliveredhas gone down (because of recent increases in thenumber of people living in assisted living facilities)this is a very efficient program that spends 98.5percent of its resources on food. Volunteers go to all,not just the poor and elderly (there is no means testand only 20 percent of participants receive subsidies).The program addresses social isolation. Deliverersnotice if someone is in trouble or if he doesn’t answerthe door. The program can be used to ask people ifthey need other kinds of help by including a surveywith the food.
The Kelly Ann Dolan fund provides some financialhelp for parents with a seriously ill child. However,private donations are slowing down. The PewCharitable Trusts funds ElderWise, which provides in-home counseling for the elderly.
Issues
Housing. The Section 8 list is closed. People with highor outstanding medical bills frequently are poor.
Utilities. The Low Income Home Energy AssistanceProgram (LIHEAP) doesn’t work for many people.However, PECO doesn’t turn off the heat if there is ababy in the home.
Case management. People over 65 should have a nursehome visit on hospital discharge for an assessment oftheir needs. The HMOs control the number of homevisits as well as the agency the case manager uses. Casemanagers believe that nurse home visits pay forthemselves, and even though they are covered byinsurance policies, some Medicare HMO might denypayment for them. Case managers do not always ask ifthere is someone to help in the home, if patients canmanage to get food, or if the patient knows thesymptoms of an infection. Many HMOs will not payfor nurses to provide those services. Some people willnot sign up for food stamps because they do not knowthere are no implications to enrolling.
Medicare managed care. As of 01/01/06, KeystoneMercy Health Plan (KMHP) dual eligibles, unlessthey actively choose not to, will become part ofKeystone 65 even if they do not want to belong to a
Medicare HMO. They will have to pay out-of-pocketcosts and the participants do not know what willhappen to the PACE (low-income pharmacy)program.
They questioned the usefulness of Medicare Part D.The cost of premiums will go up for people enrollingafter May 1. The participants believe that increasingthe premiums is a strategy to force people into HMOsbecause Part D will require a premium. People whoare just beyond the poverty level may have a very hardtime. APPRISE volunteers perform Medicare benefitcounseling and will help people with Part D decisions.
Pregnant and parenting women. Healthy BeginningsPlus serves women up to 185 percent of the federalpoverty limit but once their babies are born they maynot be able to find services for themselves or theirchildren (the children aren’t necessarily covered byCHIP or MA). The Adult Basic Coverage Program iscapped and not well resourced.
Parental support. “Not everyone can even take publictransportation to get back to the NICU (newbornintensive care unit).” One outreach worker is trying toestablish a newborn NICU parents’ group. Parentsneed a lot of support when a baby is sick and a groupcould provide a range of services and supplies. Therehave been parent outreach meetings in the past butthe outreach worker said that people must becontacted in person in order to make a realconnection to others in the same “boat.” One agencyholds client meetings, adopt-a-family opportunities (achance to obtain free food and gifts for holidays), andprovides free baby supplies. Activities have includedinviting moms to Montgomery County Vocationaland Technical School for hair and nails services and tolisten to a lecture on domestic violence. Outreachworkers check baby seatbelt safety when clients cometo meetings. They have a giveback program so thatequipment can be re-cycled to other clients. Theymentioned that more breast pumps are needed as wellas funding for other baby and new mom basics(bedding, pads, and formula). There is a long waitinglist for their services. It was suggested that breastpumps be rented but it is hard to get them back. Itwas suggested that for $10,000 they could buy breastpumps from a durable medical equipment providerand rent them for $20. When the pumps came back,the money could be returned.
18 Qualitative Assessment

19 Qualitative Assessment
It was suggested that knowledgeable volunteers beplaced at senior centers to answer questions aboutMedicare. It was also noted that enhanced casemanagement for seniors and pregnant and parentingwomen could make a big difference in their outcomes.
Session 4: Preschool Age Children
The participants included two preschool programdirectors.
When asked about the positive and unique aspects ofthe region, the participants talked about theirprograms. Both participants said they use the libraryand local businesses as trip destinations.
One director taught a “mommy & me” program thatis intentionally inclusive of special needs children, andrequires parents to attend—no nannies. The programprovides support for parents who might not bereceptive to the fact that their children have aproblem. One offshoot was a co-op group that mettwo days/week so that parents of children withproblems could have some time off. Sometimesteachers or parents will catch a problem but it cantake the Intermediate Unit (IU) a long time toevaluate. Many people who recognize that theirchildren have a problem cannot afford to have themevaluated privately. She works with the MontgomeryCounty IU.
The other was the director of a local childcarepreschool that served a racially mixed population oflow-to-moderate income families from the area andfrom Philadelphia who work locally. She noted, “Ibelieve that positive experiences when they are littlewill set the stage for academic success when they areolder.” She works directly with feeder elementaryschools and uses the criteria provided by Kindergartenteachers to enhance her curriculum. She also usesHandwriting Without Tears. She is using PATHWAYSand TEACH to educate her staff and is a KeystoneStars center working on her National Association forthe Education of Young Children (NAEYC)accreditation. She helps families sign up for CHIP andthe Montgomery County Association for the Blindthat provides eye screens. She has a dental program toexamine their teeth. There is a link to a local privateschool and older students who come and work withthe younger children. There are also links to twochurches that supply toys and other materials.
Issues
Training. Teachers should be trained to look forchildren who need early intervention services. Asyoung as 18 months, a knowledgeable person can tellthat a child is not on the right trajectory. Parents mustbe a child’s’ advocate. Pediatricians aren’t necessarilypicking up these issues. Currently, many pediatricoffices do not have call hours so parents can ask non-emergent questions. “They are assembly-linepractices.” Minimum wage childcare workers may lackthe training to understand what they are seeing.Eventually problems that could be addressed throughearly intervention services become issues for childrenin elementary school.
Children’s needs. There is a great need for nurturing.Many children from 18 months to 8 years old are inchildcare for almost 12 hours/day. There are eligiblechildren in the township but no Head Start class inLower Merion. Children talk about the TV showsthey watch over the weekend even though they receivethe Lower Merion weekend information.
Many children are overweight. Parents need supportto encourage exercise and good nutrition in theirchildren. Children may receive a healthy breakfast atschool but parents send lunch and many salty andprocessed foods. Thirty-three percent of students haveasthma and/or allergies.
Parenting skills. Parents need time management andparenting skills. Many need a support group to talkfreely. The participants suggested if centers suppliedchildcare and dinner, more people would attendeducational sessions.
Staffing. It is hard to find qualified preschool staffbecause the pay is so low. Staff is burned out by Fridayand Monday is hard. Many are part-time staff.
The participants suggested that parents needinformation about nutrition education and samples ofhealthy lunch menus. They noted that preschoolsneed support to reach NAEYC standards. Thisincludes curriculum material for young children andtheir teachers. Further, they would appreciate beingable to purchase small manipulatives (such as puzzles,beads, toys, and counting games) and large, grossmotor development equipment like climbing toys,tricycles, and playground equipment.
20 Qualitative Assessment
Session 5: Elementary and SecondarySchool Age Children
The participants included a counselor at a localelementary school, a county mental health worker,and director of an alternative school program.
When asked about the positive and unique aspects ofthe region, the participants said elementary schoolcounselors work with child study teams to meetacademic social and emotional needs, providedevelopmental guidance, and engage students andtheir families in community service. There is supportfor Second Step, a violence prevention programfunded through Safe and Drug Free Schools. TheChildren’s Aid Society helps at-risk children and theirfamilies strengthen their futures through culturallysensitive services that are professional, responsive,child centered and family focused—several peoplenoted that it is a great organization. A classroomguidance curriculum aligned with NationalAssociation of Counselors, Personal Social AcademicCareers, provides career development, decision-making and problem solving. There is a career faireach spring for fifth grade parents.
Lower Merion has a variety of services (psychological,special needs psychology, occupational therapy andspeech therapy). The school nurses do a great joblinking children to services they need. Crisisintervention is available for children who do not needhospitalization but are in serious trouble n terms ofmental health. The Oleos Bullying PreventionProgram is funded by Montgomery County FamilyServices. This program grew out of three suicides.
The Safe Kids Program is designed to prevent sexualabuse. A video is viewed and a discussion is facilitatedby Family Services. Parents have a chance to view andreact to the video. About 10 children have been pulledout of the viewings. Starting in children experience aprogressive curriculum: first grade (safe touching) andfourth grade (assertiveness). There is also Second Step.Participants report that the Base Service Unit (LowerMerion Counseling services) has improved. LowerMerion students are placed in inclusive classes. Fouralternative schools provide academic programs fornon-traditional learners.
Issues
Finding help. Getting immediate help can becumbersome and frustrating when a child is in crisis(abused, suicidal, significant family problems). Despitemany services, it takes time to get through thebureaucracy. There are not enough services to meetthe needs of special needs students. Administrativesupport would be helpful (an intern, aparaprofessional or secretary). It is difficult to getbehavioral and physical health supports and servicesfor students without insurance and there is no clinicwith a sliding scale. Services are fragmented andeveryone needs a “concierge” to negotiate the system:for elderly, resource availability for younger families:how to get your children into after-school programs,get WIC services, and work through networks at alocal level.
School nurses. They are doing much more than theyused to. They work to get children an ACCESS cardbut even with it, dental care is nearly impossible. Theyadminister medications to special needs students whohave swallowing issues, diabetic students on insulin,allergic students with epinephrine pens (57 students inLower Merion who have strong peanut allergies),medications for students with ADD; and studentswith colostomy bags. Based on the Individuals withDisabilities Education Act (IDEA) settlement, somepercentage of the 130 students who are not in school,are returning. They will require many resources.
Mental illness. Children who are suicidal are not ableto access good care. They end up at Bryn MawrHospital as emergent and given outpatient services.There are no inpatient facilities for children andadolescents. Young people who require crisisintervention are sent to Building 50 at NorristownState Hospital. There is a crisis intervention activity(not hospitalization but better than and moreemergent than outpatient.). The Base Service Unit cansee them for mental health, and drugs and alcohol.Pennsylvania has licensed professional counselorsLPCs) and southeastern Pennsylvania has adolescentbeds). Parents can petition courts to be involved inchildren’s lives based on a “duty to warn.”
There is a good home and school visitor in LowerMerion, but families still have gaps and need more
21 Qualitative Assessment
services. There used to be a hospital-based clinic foryouth and families with a sliding scale, art therapy andfamily service that met many needs. A range ofoutpatient and intensive outpatient services; and aclinic for youth and family. There is an overlap withthe Base Service Unit. Current services organizationsinclude the Lower Merion Counseling, CatholicCharities and Jewish Family Services. The county-funded facility is a Christian organization. Somepeople care that it has a cross on the logo. Participantssaid county funding probably should not be used tofund a religious organization.
There is a need to work with families and parents whoare resistant to working with the schools. Help peoplewho need more grassroots kind of services. Parentsneed to have someone to help them negotiate thesystem when they transition from early intervention toelementary school services.
Cultural competence. There are few services availableif you do not speak English or if you are a person ofmodest means. Language issues are a real problem.
Housing. Housing is huge issue for Services to Childrenin their Own Home (SCOH) families in particular.
Recommendations
• Fund Family Services to continue Safe KidsProgram.
• Fund services for children who need services lessserious than hospitalization.
• Fund the FAST Program (Families and SchoolTogether) Get parents early in elementaryschools to provide support group; have familytherapists to help break down the barriers.
• Fund FLOW (Future Leaders of the World)program.
• Fund family support services for parents to learnto cope with children with mental health issues.Or if the parent has mental health needs,children may be neglected.
• Support schools to work with children andadults with the various abilities: parents mayhave many limitations- understanding, literacy,problem solving, decision making.
• Provide emotional support for people in crisis.
• Provide speech therapy services: children orelderly not covered by insurance.
• Fund alternative learning activities; for example, itwould be helpful to integrate community activitiesinto curriculum (such as cooking for meals onwheels, making birdhouses for the park).
• Fund in-home, pre-SCOH services.
• Fund transportation for elderly in particular
• Develop a life skills program.
• Provide training for nonprofit organizations,such as college courses or professionaldevelopment with Continuing Education Unit(CEU) credits).
Session 6: Recreation
The participants included the director of a localrecreation center and the director of a social programfor gay, lesbian, bisexual transgender, and other(GLBTO) questioning youth and their straight allies,and a Lower Merion Township recreation official.
When asked about the positive and unique aspects ofthe region, the participants said the community centerprovides social, athletic, mentoring, and educationalafter-school programs for elementary through highschool-age students. There are two staff, limitedvolunteer help, and no membership fees. Programsinclude sports, which are taught in clinics, summercamps, and playgrounds.
The director of the social program for gay and lesbianyouth said her organization provides a safe andhealthy environment, some education (speakers,transgender panels, and physicians to talk about sexualissues), structured discussions, social activities, and aplace where young people (14-22) can feel safe. Thereare opportunities to bring in supportive adults, holdan alternative prom, and a few dances. Young peoplefind the organization through facultyrecommendations, community information, throughthe Internet, from guidance counselors, flyers, andword-of-mouth. Each year the ages get youngerbecause the local colleges have started providing betterprograms and activities for older students at college.
22 Qualitative Assessment
Issues
Teen programming. There is minimal teen recreationprogramming in Lower Merion Township. In additionto programming, there is a need for more space,equipment (particularly computers, as many Ardmorestudents do not have computers at home), and staff.Centers need funding for SAT courses for studentswho cannot afford Kaplan.
The township could develop multiple communitycenters to serve different parts of the area. However, inany case, young people need a place to go, where theyfeel comfortable, or they get into trouble. The GLBTQgroup would like its own drop-in space and funding tocontinue programs and for special events. The groupwould like to provide counseling, (GLBTQ youth havea rate of suicide three to four times that of other teens)but there are liability and insurance issues. They need acomputer printer, up-to-date Web site. “It is not likelythat GLBTQ students would be comfortable in a newcommunity center; it would be too hard for youngpeople to go to a gay program. Plus, centers are limitedin terms what they can do without parental consent.Some of these are children whose parents evict themwhen they find out they are gay.”
The participants said that community center boardsneed training and although they have mixed funding,both directors explained that the centers areunderstaffed and under resourced. They would like tosee township support for multicultural youth activitiesin traditional and non-traditional settings.
Session 7: Elderly
The participants included a long-term care casemanager; transportation service providers; a geriatricnurse, and staff from a senior center, the Alzheimer’sAssociation, and ElderNet.
When asked about the positive and unique aspects ofthe region, the participants said there are significanttransportation services available for the elderly inLower Merion Township. People receive sometransportation to doctors’ appointments, seniorcenters, and adult day care. Services are available tolow income people, not just the elderly.
People are assessed, a care plan is developed andoptions are developed. Referrals for services comefrom hospital staff, community based organizations,
and by word of mouth. Sometimes people who needfood or medications receive them through theagencies. Senior centers provide hundreds of mealseach week.
There is a program at several hospitals designed toprevent and decrease functional decline and deliriumin hospitalized elderly by using mobility. The programhas decreased falls, increased Press Gainy scores andenhanced customer satisfaction. It has decreased theuse of catheters and diapers, liberalized diets for agedcardiac patients including menu options that they canhave anytime, and helped them use the phone.
Issues
Medicare. No one knows what will happen when thenew Medicare laws limit the number of doctor visits.There is tremendous confusion over health insurance,which is expected to worsen, and about financial issues,such as electronic deposit of Social Security checks.
Medical transport. There are problems withambulance transport- much of it is not reimbursedand expensive. TransNet is not permitted to crosscounty lines. The rules are stringent (the elderly mustwait outside, calls must be made 24 hours in advance,the rides are often late, and there are limited hours).There are few support services for early-onset (<60)Alzheimer’s. It is hard to find rides for chemotherapybecause it is so many times each week. However,dialysis is a priority for community transport.
Hospital discharge. It is difficult for the elderly to gohome alone after hospital discharge. They are told toappeal to their insurer and/or Medicare to stay extradays in the hospital. Sometimes they need help gettingsettled, but many balk at asking for more help. Hospitalsprovide a cab voucher and let them go home. There is abreak in continuity: nobody calls. We should look at thelaws particularly around early dementia.
Older people need someone to “run interference forthem.” One participant told the story of a woman whofelt numb on one side of her body. There was a nurse atchurch who said, “You have to be seen at the hospital.”She insisted on being seen by a physician (she wouldn’tgo to the ER) and she had Doppler studies and was inthe hospital two days later. Physicians’ officereceptionists need training. They only believe aprofessional who tells them something is wrong.

23 Qualitative Assessment
The participants suggested that improving aftercareassessment and enhancing case management in thecommunity would make a real difference for seniors.They also suggested providing personal care/homehealth aide training in order to support thedevelopment of more informal caregivers: for example,training for families so they learn how to fill in whenother services aren’t available.
Session 8: Housing and Transportation
The participants included two representatives ofhousing organizations, a staffer on code violation andhandicapped access, and a borough transportationdirector
When asked about the positive and unique aspects ofthe region, the participants said the townshipambulance service provides support and referral toeveryone. The borough does not use a means test toprovide information to people who call. They providetelephone reassurance and friendly visiting. Oneagency provides volunteers to transport the elderly totheir doctors’ appointments, to the grocery, and to doodd jobs that are too small for a contractor. There area few small grants available to help people in direstraights. There are programs to serve the mentally ill,younger disabled and older adults. There are someefforts in older boroughs to provide work inneighborhood revitalization efforts.
Issues
Housing. Affordable housing and reliabletransportation are critical. Some private money isavailable for housing but it is affected by marketforces. Some areas of the county need much moremoney because market forces will not operate there aseffectively as in Lower Merion. Resources should beput into developing lower-cost apartments overstorefronts. Site acquisition is often difficult, expensesduring development may be unpredictable, or amunicipality may not let it happen. Housing in somecommunities is difficult to obtain or it is old and inpoor condition. Many houses need lead abatement,and there are big houses with one bathroom and nosink. Houses now sell in three months to out-of-townlandlords who make them rental properties. The moreaffordable rentals are in places with no transportation.It is hard to go across the county.
Funding. Organizations must limit their work, not towhere the need is the greatest, but to where there isfunding. Smaller boroughs need grant writers to helpthem identify funding. Smaller, disadvantaged townsneed operating support from foundations becausestate programs tend to be short term. The participantssuggested that the state could “prime the pump” byproviding funds to spruce up an area.
Transportation. The Area Agency on Agingconducted a survey in Montgomery County, whichhas a large aging population. ElderNet was created as aresult in 1975. It keeps detailed phone logs aboutneeds that are expressed, which yield new programs.For example, older adults do not want to stop driving.They start by self-regulating: they do not drive atnight, in bad weather, long distances, or on badhighways. But driving is a form of socializing, andthey need it to access to medical care. There are highexpenses associated with keeping a car.
How ElderNet transportation works.In 1989, theelderly needed 50 rides /month, and it was easy tostaff. Currently, ElderNet provides over 200rides/month, and it is underutilized. The incomeguidelines are $28,000 for a single person and$34,000 for a couple. Shared rides are availablethrough Paratransit and Bennet cab. The rider isresponsible for 15 percent of the cost and the balanceis funded through the lottery.) Aging participants haveto wait outside their homes and the cabs aren’t ontime. ElderNet volunteer drivers go into the doctor’soffice with the client, but there aren’t enough drivers.They also transport mental health clients and much ofthe transportation is for physical therapyappointments.
There is some money available to provide rides througha contractor. Rides were limited to one/week but thereare more now. They can transport ambulatory patientsbut there is no capacity for the wheelchair bound.Shopping is hard for the elderly and the disabledbecause they cannot carry and they cannot reach.Volunteer shoppers visit and do small jobs for them(e.g., change a bulb). Transportation is a difficult job forvolunteers and it is hard to recruit them.
There is little support from the business community.Some contributions come from people receiving theservices. Part of the transportation problem stemsfrom the way the county has developed the rural,

24 Qualitative Assessment
more affordable areas. Buses may not run anymorethan once an hour. “There is no upside for a politicianto put affordable housing in his backyard.”
The participants suggested that agencies already doingthe work need more staff. They would like to seesupport for the planning process and to limit the riskexposure of agencies working to address housing andtransportation.
Session 9: Behavioral Health
The participants included representatives from theMontgomery County Office of Mental Health adultservices, a family services agency, a for-profitbehavioral health provider, a youth aid panel, and anonprofit local mental health agency.
When asked about the positive and unique aspects ofthe region, the participants said agencies providingservices link to the community through the BaseService Unit that is operated through a subcontract.They provide monitoring, receive complaints andcalls, and work with the state hospital on dischargeplanning for people returned to the community. Oneagency provides individual, family, marital, adolescentsand children’s therapy as well as the Families AndSchools Together (FAST) Program at schools. There isoutreach to people with on the Main Line withbehavioral health problems. They receive servicesthrough the following models: inpatient, outpatient,partial, intensive out patient services, drug and alcoholand traditional out patient services.
Montgomery County trains community volunteers asan alternative to adjudication for first time offenders.They receive referrals from the police for those whowould benefit from a second chance (shoplifting,trespassing, drugs and alcohol). A coalition concernedwith youth safety and health promotes dialogueamong the schools, police and the mental healthproviders to bridge the public- private school gap. Ayouth panel meets with students and families todiscuss social norms such as drinking as a rite ofpassage. One agency provides play therapy with littlechildren. National Alliance for the Mentally Ill(NAMI) has a Web site with resources for Bucks,Montgomery County, Delaware, Chester andPhiladelphia counties.
“There are no homeless in Lower Merion.”
Issues
Alcohol use. There is an epidemic of younger andmore serious drinking among girls. Parents are blaséabout drinking; it is seen as a rite of passage andyoung people are hiding it. Parents do not understandthe dangers. There has not been an increase in the useof the School Assistance Program. There are norehabilitation or detoxification units located nearby.There is a great deal of denial and a high level of stresson young people with few outlets.
Chronically mentally ill. Much of the work is withchronically mentally ill who also have physicalproblems. Children’s crisis services are far away (inAbington) and the stationery for the facility has across on its logo, which makes it uninviting to manyof the people who would use the service. Thechronically mentally ill can only go to the Bryn MawrFamily Health Office, which has relocated toBroomall. The shuttle from the hospital only runsuntil 1:00 p.m.
It is hard to obtain dental care for people on Medicaidin this region. Only one dentist in Norristown istaking the ACCESS card.
Daytime and evening counseling appointments areneeded, and a coordinating system of informationthrough an updated Web site is needed.
Transportation is an issue.
Youth services. The Youth Aid Panel hears cases ofyoung people who were bored and got into trouble.For example, Lower Merion needs a skateboard park.A larger, better-equipped, multi-service YMCA isneeded. The Pottstown Y is a good model: it includesa senior center and is multinational and wellintegrated. When the private schools build andexpand, they ask to use the public school fields.
“There is little for kids and families in theArdmore revitalization. There is no towncenter, no place to bring people together,no bulletin board. You need to have a bigcenter with indoor and outdoor facilities.”

25 Qualitative Assessment
Needed services. Low-income single parents have fewservices—no support groups, no childcare—and, as aresult, many children are left alone at an early age.There is one substance abuse transition house. Peopleoften need to access services in Norristown and theycannot get there. Some participants reported that it isdifficult to obtain HIV testing and counseling. Therearen’t enough psychiatric services. Children and Youthdoes not have much of a presence in Lower Merion,and there aren’t enough beds for children and teens.Paoli closed its mental health unit; Friends Hospitalhas become a for-profit entity and its crisis ER will beseparate. Admission directly to Friends will be separateas well.
Geriatric services. There aren’t enough geriatricservices in the area. Mercy Fitzgerald closed its seniorservices beds. Eagleville has a geri-psychiatric unit thatis doing well. Horizon (a for-profit entity) rents spaceat Eagleville Hospital. Riverside, a satellite ofEagleville, is located in West and North Philadelphiaand Coatesville. Wills Eye has geri-psychiatric services.
It is expensive to provide psychiatric services to seniors ifthe medical model is used. Bryn Mawr Hospital triesnot to send people away. Depression and anxiety for theaging and the physically compromised go together.Parity for mental and physical health services is about 50percent. It is hard to get providers (physicians) to handlethese patients. After the acute phase ends, step- downservices are hard to find. Montgomery County has fourbeds that are the medical model for psychiatry, but notnecessarily for the elderly. Montgomery County looks atregional services. This is an area that needs a great dealof support.
The participants suggested that the region needsenhanced accessibility to psychiatric services for youthand the elderly. More public education andinformation about drug and alcohol use among teensis needed. They said that people need transportationto get to needed services. Finally, they suggested thatthe county should provide information and materialsin a variety of languages.
Session 10: Public Safety
The participants included three police officers fromtwo townships.
When asked about the positive and unique aspects ofthe region, the participants said there were significantaccomplishments in community policing includingthe DARE Programs. They provide more services withless money. At the beginning, parents’ sessions werepoorly attended. While the Civilian Police Academyexperienced a low turnout in Lower Merion, the Copsand Kids program in grade schools is more aboutrelationship building. They used examples of domesticviolence and the use of pepper spray, and childrenunderstood what they were saying.
Issues
New trends. There is bullying and cyber harassment, acrime that didn’t exist a few years ago. They seeidentify theft, scams such as the PECO tree service,and domestic violence among the “upper crust.” “He’son the phone with his lawyer and she’s on the phonewith hers. They live in a house big enough so theywouldn’t even bump into each other for years at atime. But both are trying to develop a paper trail.”
The police struggle with budget cuts and more restrictedaccess to schools with a curriculum pressure on testing.There is less parental involvement “My parents will bein France until April.” Alcohol abuse is underreportedby the schools and the community. There is a significantdrug scene including homicides in drug deals. Drugsused to be products of the Vietnam era and homegrown. Today, cheap pure heroin is available and we areseeing 13-year-old addicts.
The participantssuggested thatsupporting theNAACP ParentingSkills Program inNorristown mighthelp to reduce truancy. Parents need family-orientedparenting skills because the police can only treatsymptoms. Participants suggested that the middleschool and high school life-skills training–conflictresolution program should be offered for credit.
Participants agreed that it was important to meet thestandards set by state police about diversity. It wassuggested that the Civilian Review Board should bere-implemented. All agreed that there was a lotfragmentation of services: there are 47 police
“We do not treat socialproblems; we just movethem.”
26 Qualitative Assessment
departments and 101 volunteer fire departments inthe county.
Session 11: Arts and Culture
Participants included representatives from an artcenter and a local theatre.
The art school’s mission is to provide affordable andaccessible art for all.
Session 12: Minorities and New Immigrants
The participants included a minister and arepresentative of a senior center
Issues
The new immigrants are Mexican landscapers. TheEnglish as a second language (ESL) classes are full.Some property owners are dropping out of Section 8housing because they believe they can get reliable rentfrom the new immigrants who will work two or threejobs in order to buy a house. “They have a goal andthey walk to work carrying their lunch in order to savethe money they need to buy a house.”
The service companies hire them: “Make sure yousend me Mexicans all the time.”
“What happens to others? In many cases these aredisposable people, and others have to pick up the cost.”
The participants suggested that support for ESLclasses is really key to helping people assimilate;however, until immigrants are able to speak and readEnglish, it remains important to provide translation ofneeded documents. It was suggested that we shouldteach Spanish in elementary schools and re-allocatethe cost of the burden.
Session 13: Sustained Funding for NewProjects
1. Community-based organizations are stretchedthin and need support.
2. It is not necessary to “reinvent the wheel”; lookat what is actually going on.
3. Provide sustained support of a crumblinginfrastructure, but also encourage consolidationto reduce fragmentation.

27 Conclusions
SummaryThe quantitative assessment of the Southeast regionpresented in this report describes an areageographically insulated from the rest of the county. Ithas a stable, aging population whose 3.3 percentgrowth matches that of the state as a whole. TheSoutheast region has the highest average income,highest average educational level and the lowestpoverty rate of any of the county’s five regions. Theregion has an acute hospital bed and physicianpopulation ratios that are more than twice that of thecounty as a whole. It provides healthcare services to apopulation well beyond its boundaries. Its publicschools receive 40 percent more funding per pupilthan county as a whole. School achievement testperformance and average SAT scores are the highestamong the county’s five regions. Yet, its healthindicators are only slightly better, and its crime ratefor more serious crimes (Part I crimes) are slightlyworse than those for the county as a whole.
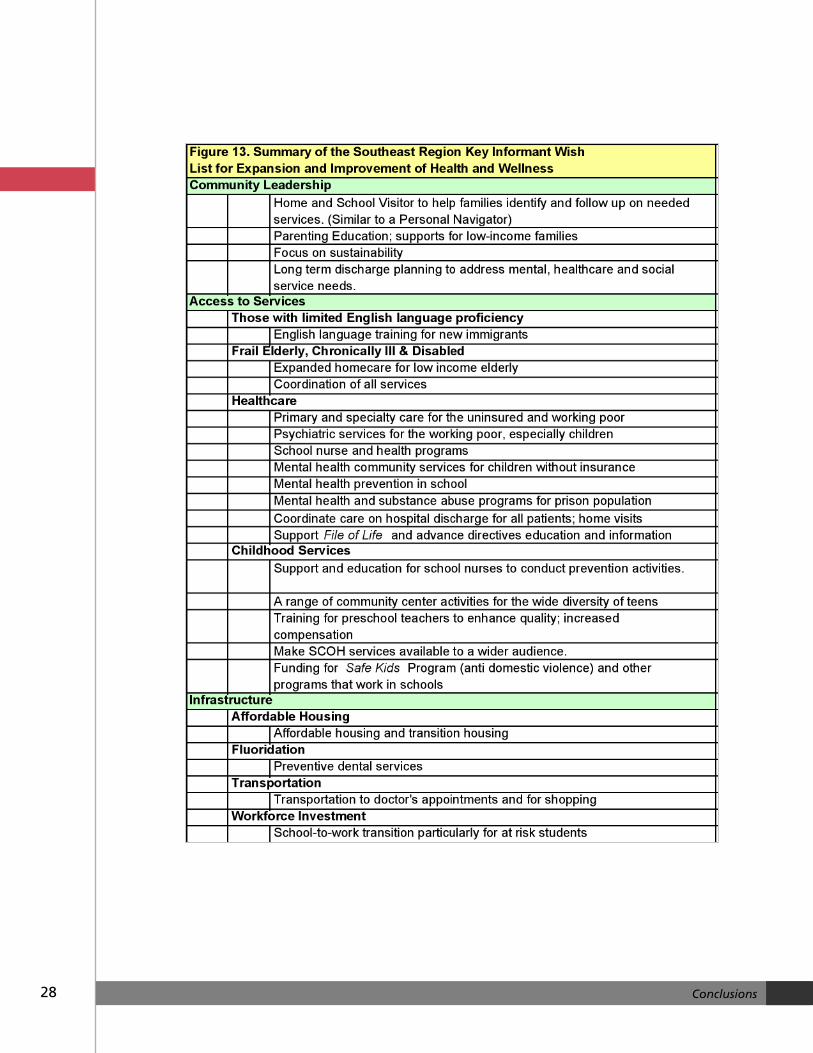
However, the 50 key informants we met with, assummarized in the qualitative assessment in thisreport, expressed concern about essentially the sameissues as did those in other regions of the county.They identified as priorities for improving the healthand quality of life of the region, the need for moreeffective community leadership, improved access toservices, and an improved basic infrastructure. Their“wish list” is summarized in Figure 13. They focusedon three general needs: (1) better leadership trainingfor parents, peers, and community members so thatthey can better perform their roles and serve as moreeffective advocates for the support of critical servicesand needed institutional changes; (2) expanded andeasier access to services across systems (healthcare,schools, criminal justice and social services); and (3)assurance that the basic infrastructure was in place sothat services—housing, fluoridation, information,transportation and workforce development—can be
provided cost effectively.
In the full report, we assess Montgomery County’sefforts to address the health and social needs of itspopulation. The major challenges it faces are:
• The fragmentation of services.
• The concentration of the largest health andsocial service needs in Norristown and a fewboroughs that by themselves lack adequateresources to address them.
• The financial pressures and demands fornarrowly focused accountability on providersthat undermine their capacity to address thecomplex needs of the population and furtherfragment care.
Most participants in the collaborative support the twobasic long range goals of the national Healthy People2010 initiative: (1) longer, higher quality lives and (2)the elimination of the disparities in opportunities forachieving such lives. They are less clear on how best toachieve these two goals. In the full report, we spell outmore specific, measurable, longer-range objectivesrelated to these two goals and some possible “middlerange” strategies for achieving them. Those strategiesinclude (1) a coordinated countywide initiative toreduce smoking, obesity and sedentary life styles, (2)implementation of life transition plans for the firstfive years of life and service provider discharges, (3)expanded school health programs, (4) creation of aconsolidated funding and coordination plan, and (5) acoordinated advocacy program. In ourrecommendations in this report, however, we focus onthe more immediate opportunities.
CONCLUSIONSCONCLUSIONS
28 Conclusions
29 Recommendations
The statistical analysis and our discussions with keyinformants presented in this regional report identifiedmany needs. We focus on what we believe are the bestimmediate opportunities for moving the regiontowards longer, higher quality lives and theelimination of the disparities in achieving such livesWhile there are variations in emphasis by region, theopportunities in each region are essentially the same.Thus, the more the regions can work together, themore successful they will be in taking advantage ofthose opportunities.
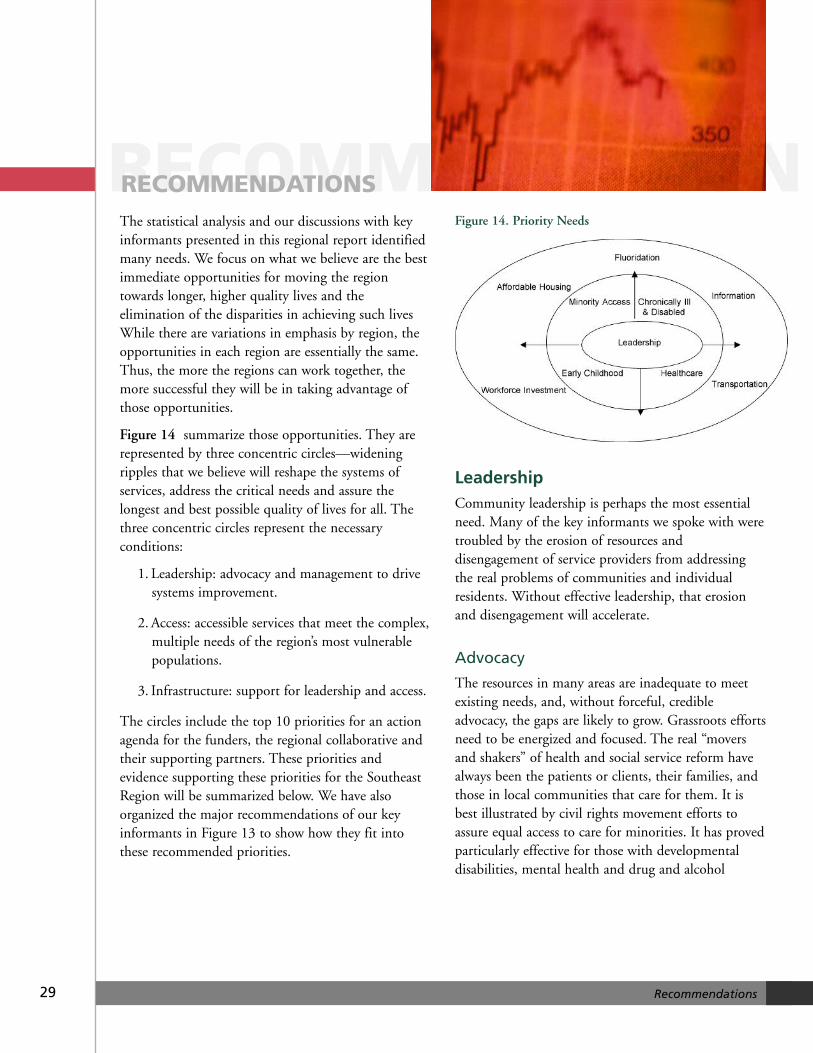
Figure 14 summarize those opportunities. They arerepresented by three concentric circles—wideningripples that we believe will reshape the systems ofservices, address the critical needs and assure thelongest and best possible quality of lives for all. Thethree concentric circles represent the necessaryconditions:
1. Leadership: advocacy and management to drivesystems improvement.
2. Access: accessible services that meet the complex,multiple needs of the region’s most vulnerablepopulations.
3. Infrastructure: support for leadership and access.
The circles include the top 10 priorities for an actionagenda for the funders, the regional collaborative andtheir supporting partners. These priorities andevidence supporting these priorities for the SoutheastRegion will be summarized below. We have alsoorganized the major recommendations of our keyinformants in Figure 13 to show how they fit intothese recommended priorities.
Figure 14. Priority Needs
LeadershipCommunity leadership is perhaps the most essentialneed. Many of the key informants we spoke with weretroubled by the erosion of resources anddisengagement of service providers from addressingthe real problems of communities and individualresidents. Without effective leadership, that erosionand disengagement will accelerate.
Advocacy
The resources in many areas are inadequate to meetexisting needs, and, without forceful, credibleadvocacy, the gaps are likely to grow. Grassroots effortsneed to be energized and focused. The real “moversand shakers” of health and social service reform havealways been the patients or clients, their families, andthose in local communities that care for them. It isbest illustrated by civil rights movement efforts toassure equal access to care for minorities. It has provedparticularly effective for those with developmentaldisabilities, mental health and drug and alcohol
RECOMMENDATIONRECOMMENDATIONS

30 Recommendations
problems, and chronic conditions. The arts andcultural efforts have always helped to communicatetheir needs in their most human and persuasivefashion and to create the pride and sense ofcommunity that is necessary to address them. Animmediate priority should be to advocate for localleadership training and development.
Management
Advocacy will not be effective if resources are notmanaged efficiently and squandered by duplication.Management is by far most underdevelopedcomponent of the health and social service systems.Consumers, service providers, and funders face abewildering fragmented maze that requires heroiceffort to assure people get what they need, providersrespond effectively to those needs and funders preservescarce resources. In general, nothing is a more neededand more challenging task than the effectiveharnessing of public, private, and voluntary sectorefforts. In Montgomery County, partly as a result ofthe commonwealth structure of governance,historically independent development of variouscomponents of the county and the Southeast region,aversion to al control, uncritical faith in the market.
It is not just the consumers of services that haveproblems in figuring how things work. Many of thekey informants we talked with were often equallybewildered. The Southeast Regional Collaborativerepresents as much a symptom of the problem as apromise of its resolution. Many of the key informantswe talked with had difficulty clearly explaining themission and goals of the collaboratives: Are theysimply an informal way of meeting to shareinformation and identify resources for addressing theneeds of their individual clients, or are they a policymaking body with the authority to allocate resourcesand impose order on the service system? Are they acounty initiative or the outgrowth of local serviceprovider efforts? Even in the Southeast region answersdiffered. Just as with the other collaboratives, theanswer lies somewhere between the promise acoherent system and the embodiment of a fragmentedsystem that defends insular prerogatives and studiouslyavoid addressing the underlying structural problems.The partners in this project can play a critical role inshaping the evolution of these organizations. We seefour immediate management priorities:
1. Clarify the role of the collaboratives in theplanning and management of services andprovide them with the budgets and authoritythat is appropriate.
2. Concentrate the resources on where the need isgreatest. Norristown has by far the greatest needsand several other smaller pockets of need requireattention. The partners in the Bucks CountyHealth Improvement Program chose to pooltheir resources and concentrate them where theywere needed the most. An even more convincingcase for such concentration could be made inMontgomery County and in the Southeastregion.
3. Expand the partnership to include the leadershipof all of key resources that have a stake in theeffective addressing of needs in the county. Thepartners in this project should be commendedfor their leadership in initiating this effort,pooling their resources and moving away from apiecemeal, fragmented approach. However, it hasbecome clear that the goals and the resultingactions necessary to achieve them far exceedtheir limited resources. Many other stakeholderswill need to come to the table. This includesleadership from private business, the largerhealth systems, schools, universities, and otherresearch institutions equally concerned about thefuture health and quality of life of MontgomeryCounty residents.
4. Invest in the ongoing maintenance of amanagement reporting process. Reports such asthis by themselves are lifeless, soon dated, and,at best, relegated to end tables in reception areas.An ongoing reporting process, a “leadershipdashboard” that lets leaders know whether theyare moving in the right directions and aids inmidcourse corrections would breathe life into it.It could also help to facilitate greater consensusabout what is important enough to measure andhow to collect and report it. Such a reportingprocess could provide transparency, align goalsand objectives with activities, and assist inleadership development and programrefinement.

31 Recommendations
AccessThe key immediate access priorities are those thatmake the greatest contribution to reducing disparitiesin opportunities for a healthy, high quality life. Theyfocus on the regions vulnerable populations for whomaccess to appropriate services is the largest challenge.
Enfranchising Montgomery County’sMinority Communities
The civil rights era produced a new definition of whatit means to be an American and Montgomery Countyhas benefited from this change. The ImmigrationReform Act of 1965 eliminated a quota system thatfavored Northern Europeans and largely excludedimmigration from other continents. While in theSoutheast region 55 percent of its residents reportGerman, Irish, Italian, and English ancestry and it isstill 89 percent white, it has begun to match some ofthe broader racial and ethnic diversity of the region asa whole. While the white population in the Southeastregion declined by 1.3 percent between the last twocensuses, the black population increased by 12.4percent, the Hispanic population by 39 percent, andthe Asian population by 99 percent. In the region,10,517 persons over the age of five speak a languageother than English in the home (11.5 percent) and2,616 report limited English proficiency. The futuredevelopment of the region, just as elsewhere hinges onits ability to accommodate this demographic shift thatwill, in the nation as a whole, result in non-Hispanicwhites becoming a minority population by 2060.Service providers have lagged in adapting to thesedemographic shifts. Many of these new immigrants, asdo many African Americans, feel disenfranchised inthe county’s health and social service system. Whilerarely expressing their dissatisfaction directly toproviders of services, many feel excluded andunwelcome. The research literature suggests that thesefeelings contribute to disparities in accessingappropriate services. Our review indicates that theimmediate priorities should be to (1) support fullcompliance for all health and social services providerswith Title VI Civil Rights guidelines, including those forlimited English proficiency language services, (2) increaseminority representation on staffs and governing bodies,and (3) expand activities that create a more inclusiveand welcoming atmosphere.
Enhancing Early Childhood Services
The population of children under the age of five inthe region declined by 4.9 percent in the last decadeto 5,218. Almost half of this population is enrolledeither in nursery school programs (1,732) orkindergarten (1,060). According to some of our keyinformants, there is a shortage of such services andmany families have difficulty finding quality nurseryand preschool places for their children. Sixty-five childabuse and neglect referrals to the County Office ofChildren and Youth took place in the Southeast in2004. In 315 households the grandparents serve as theprimary caregivers for their grandchildren. Almost twodoses of psychotropic medications for attention deficitdisorder and other conditions are dispensed in schoolsin the region for every child enrolled. The servicesprovided to children and their parents in the first fiveyears of life are a key to breaking the cycle ofdisadvantaged. Such programs as Head Start havedemonstrated their effectiveness in long term schoolsuccess and success in adult life. After the first 28days, external causes, such as infections, accidents andphysical abuse are the predominant causes of death forinfants in Montgomery County. Early diagnosis andtreatment of learning and developmental disordersimprove outcomes but, according to the keyinformants we talked with, such efforts are more likelyto be delayed among low-income children. Low- andmoderate-income parents cannot afford to stay athome, nor can they afford high-quality day care andpreschool care without assistance. Yet, enriched highquality day care and preschool programs are ideallocations for facilitating parental education, preventiveand early intervention services. An immediate priorityshould be advocacy for investment in enriching,subsidizing, and expanding high-quality day care andpreschool programs for low- and moderate-incomefamilies.
Expanding Services for the Chronically Illand Disabled.
The number of persons over the age of 85 in theregion grew 45 percent in the last decade to 2,300. Inthe region 4,153 householders are over the age of 65.Of the 15,790 persons living in the region over 65,4,581 (or 29 percent) report at least one disability.The census reports 638 persons living in nursinghomes in the region. Demographic shifts, accelerated
32 Recommendations
by the growth of senior housing and private assistedliving in Montgomery County are on a collisioncourse with anticipated Medicare and Medicaidcutbacks. Low- and moderate-income families will bemost affected by that collision. An immediate priorityshould be to advocate for support for these informal careproviders that have to adapt to the growing financialconstraints on the system and assist them in by expandingthe alternative supportive housing options for the frailelderly.
Increasing Access to Health Care
Approximately 14 percent or 5,865 adults in theSoutheast region between the ages of 18 and 64 haveno health insurance. Thirteen percent of adults or9,596 have no personal healthcare provider and 10percent ($8,.015) needed to see a doctor in the lasttwelve months but could not because of the cost. Evenwith the abundant resources available in the region,low-income or uninsured persons are often forced torely on Philadelphia medical school services and theseoften involve long delays and difficulties in arrangingtransportation. An immediate priority should be toinvest in facilitating insurance coverage, expandingmedical homes, and assuring access to specialty anddiagnostic services for the low-income population.
InfrastructureThe best health care, educational and social services inthe world are worthless if people lack shelter, live inan environment that undermines whatever help theycan receive, do not know about the services, andcannot get to them. A small but growing number ofpeople in the Southeast region lack these basic needs.
Affordable Housing
Twenty-four percent or 8,512 households in theSoutheast region allocate more than 30 percent oftheir income for housing, above the federally definedthreshold for affordability. Many of the servicesproviders (policemen, childcare providers, nurses, andteachers) commute to this region creating problemswith turnover, and loss of community cohesiveness.Service providers seeking sheltered or transitionalhousing for their homeless, disabled or recoveringmental health and drug and alcohol clients have also
been caught in this same squeeze. The lack ofsufficient transitional housing that can assist them inovercoming their problems—mental illness, drug andalcohol, domestic abuse, and, increasingly, simplyeconomic circumstances—that led to homelessnesstraps them at this level. They represent the tip of theiceberg: a growing population is on the edge ofhomelessness.
In 2005 the fair market rent for a two-bedroomapartment in Montgomery County was $947/month,which, to be affordable, would require an hourly wageof $18 for a 40-hour week. The Housing ChoiceVoucher Program (formerly the Section 8 Voucher andCertificate Programs) was designed to provideaffordable housing to low-wage workers in the privatemarket and avoid the concentration of low-incomefamilies in public housing projects. The county hasclosed the waiting list for such vouchers andanticipates that budget cuts will curtail the overallnumber of vouchers that are available in the future.Even for those with vouchers, the housing that meetsthe requirements of the program is often unavailable.In a county where transportation is a major problem,low- and moderate-income workers in the countymust travel long distances in the search of affordablehousing. This in turn creates a critical problem foremployers in recruiting and retaining workers,particularly in health and human services where thewages for the bulk of the workforce are relatively low.In short, there is an affordable housing crisis in theSoutheast Region and in Montgomery County. Theimmediate priorities are (1) expanding the capacity ofsupportive transitional housing programs and (2)increasing the stock of affordable housing either throughadditional voucher subsidies, development requirements,or voluntary initiatives.
FluoridationDental decay is the most common chronic condition.About 12,262 or 16 percent of all adults in the regionhave had more than five teeth removed because of toothdecay or gum disease. Dental care can be costly, healthinsurance coverage is more limited, and many low andmoderate income persons cannot afford the out-of-pocket costs. About 17,627 or 23 percent of adults inthe region, mostly those with low or moderate incomefailed to visit a dentist in the last year. For children

33 Recommendations
dental decay affects school performance and for adults itmay limit their employment opportunities. For the poor,payment is so restrictive under the Medicaid program,that few dentists participate. In many cases, the onlyhope for receiving care is to travel to the clinics operatedby the dental schools in Philadelphia. The distance andlimitations in pubic transportation make this aparticular hardship for low- and moderate-incomeresidents in the Southeast Region of MontgomeryCounty.
Fluoridation is an ignored but critical infrastructureinvestment. As a vivid and concrete example of thecosts incurred from the failure to invest in the healthof the community as a whole, it has critical symbolicvalue in the struggle to revitalize a sense ofcommunity in Montgomery County. No investmentin health appears to provide a better return. Everydollar investment in fluoridation produces theequivalent benefit in oral health roughly $38 in directdental services. Montgomery County lags far behindthe nation and state in making such investments. Ofthe population served by public water systems, 66percent of the United States and 54 percent of thePennsylvania receive optimally fluoridated water. Incontrast, of the 41 water systems in MontgomeryCounty, only the Borough of Pottstown’s municipalwater system fluoridates its water. Ten years ago,California lagged similarly and the CaliforniaEndowment was able through advocacy and selectiveinvestment to bring the state up to the nationalaverage. The immediate priority is a fluoridationcampaign in Montgomery County that will increase theproportion of the population covered by optimallyfluoridated water supplies at least to the nationalaverage.
Information
No group that we interviewed in the Southeast regionand no prior studies on Montgomery County havefailed to mention the lack of adequate information onwhere to go and how to get services. A Web-basedapproach to providing an easily searchable,maintained, and updated directory of services in thecounty is currently a joint project of the North PennCommunity Health Foundation and MontgomeryCounty Foundation. However, what is most critical inmaking sure people get what they really need, or a
least have an equal chance of getting it, is informationabout supply, demand and rationing procedures. Forexample, there is no shortage of assisted living units inMontgomery County that charge as much as $6,000 amonth to private- pay clients, and there is no shortageof information about these units (facility directories,advertising, mail solicitations, Web sites, and the like).There is, however, a severe shortage of affordablehousing and transitional housing programs, andservice providers have a lot of difficulty gettinginformation they need to help their clients. Theimmediate priority is for an ongoing regional populationplanning process that identifies shortages and eitherdevelops plans for eliminating them or creates atransparent rationing system for the fair allocation ofresources.
Transportation
In the last decade, no needs assessment study in thiscounty, whether it was looked at arts and culture,health services, or social services, has failed to mentiontransportation as a top concern. This was also aconcern of the key informants we spoke with in theSoutheast region. In the long term, success inaddressing this need can be facilitated by the county’ssuccess in implementing its development plan forincreasing residential density in the county’s urbancenters and expanding the use of publictransportation. Expansion of inventive programs inthe county, such as one for low-income, workingsingle mothers who need automobiles and one forhiring of recent retirees as subcontractors to transportthe frail elderly on a private pay basis, can helpalleviate parts of this problem. More than 82 percentof residents in the Southeast region who workcommute by automobile. About 5.9 percent or 2,277of housing units in the region lack an automobile.The lack of an automobile is not just a consequence ofpoverty: it is a barrier to escaping it. Some haveproposed tax deductions for automobile ownership forlow-income workers to assist them in taking advantageof employment opportunities. Successful privatelyfunded programs such as Vehicles for Change inWashington, DC and Working Wheels in Seattle helpto provide loans and decent cars to poor workers.Family Services of Montgomery County Ways toWork program provides a model innovative programtargeting working single mothers but the funds
34 Recommendations
provide for only a limited number of loans (less than20 a year) and the eligibility requirements arerestrictive. The immediate priority to advocate forfurther expansion of automobile grant and loan programsis for Montgomery County’s working poor.
Workforce Investment
In 2000, 5.2 percent (or 4,073) adults in the regionseeking employment were unemployed. The shift froma manufacturing to a service economy has adverselyaffected the Southeast region and many of thoseemployed are underemployed in low wage jobs. Thecounty as a whole faces a growing population thatattracts affluent young families and retirement ageseniors, affordable housing shortages, transportationproblems, tightening health and social servicesfinancing, and an aging health and social serviceworkforce. This translates into a looming “perfectstorm” of workforce shortages that will adversely affectthese services and the quality of life of all ofMontgomery County’s residents. The PennsylvaniaCenter for Health Careers forecasts a shortage of 7percent (or 120) licensed practical nurses shortage anda shortage of 11 percent (or 1,090) registered nursesin Montgomery County for 2010. The first babyboomers turn 65 in 2011. Currently, 37 percent of
Montgomery County’s registered nurses workforce and47 percent of its licensed practical nurses are over age50. The combined growth of Montgomery County’selderly population with its greater care needs and theaging of its nursing workforce will greatly exacerbatethese shortages. The largest current shortages of high-quality staff as reported by the key informants wespoke with, however, are in day care, behavioralhealth, and personal care attendants. Relatively lowwages and the high cost of living increase recruitmentdifficulties and turnover. These recruitment andretention problems are likely to increase.Underemployed residents of the Southeast region areideally positioned to take advantage of these loomingshortages. The immediate priority is to advocate for thefurther supplementation of loans and scholarships to easeentry for low- and moderate-income students and in waysto support more livable wages in critical health andsocial service workforce shortage areas.
These immediate priority needs in leadership, accessto services and infrastructure in the Southeast region’scommunities are also critical strategic investments. Inthe long run, they will produce the increased qualityof life, health, and equality of opportunity for whichall residents will take great pride in helping to achieveand those living elsewhere will strive to emulate.
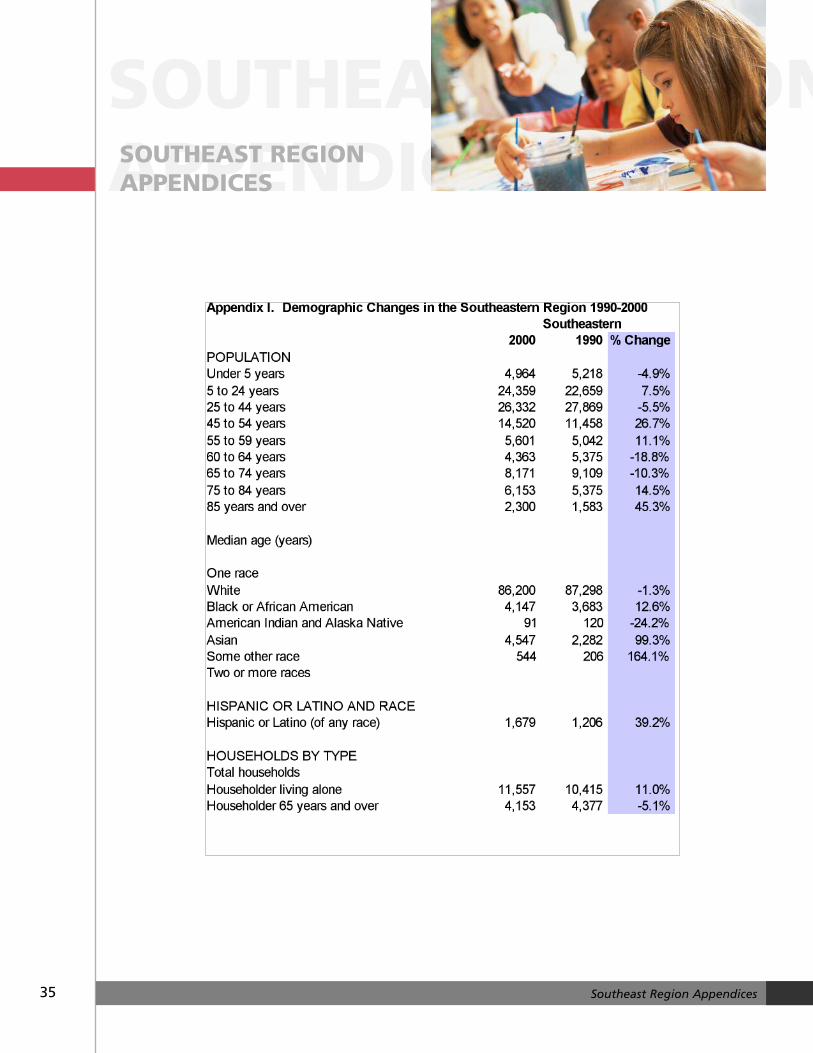
35 Southeast Region Appendices
SOUTHEAST REGIONAPPENDICESSOUTHEAST REGIONAPPENDICES
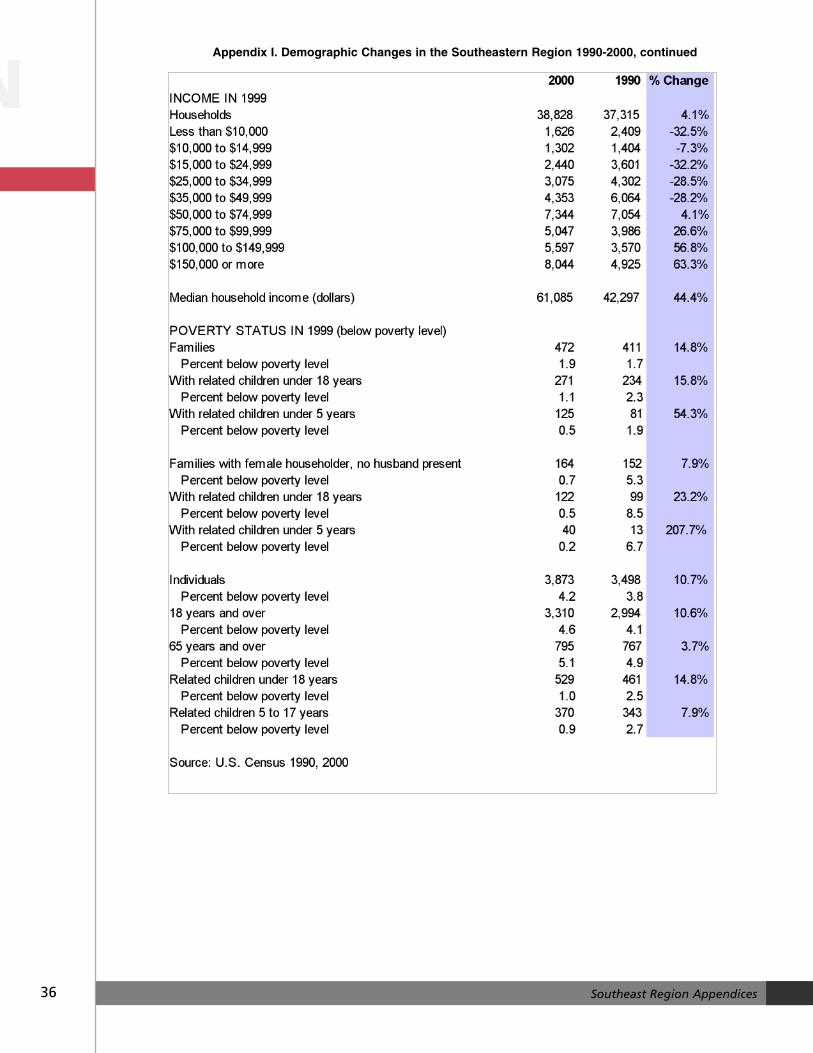
36 Southeast Region Appendices
NAppendix I. Demographic Changes in the Southeastern Region 1990-2000, continued
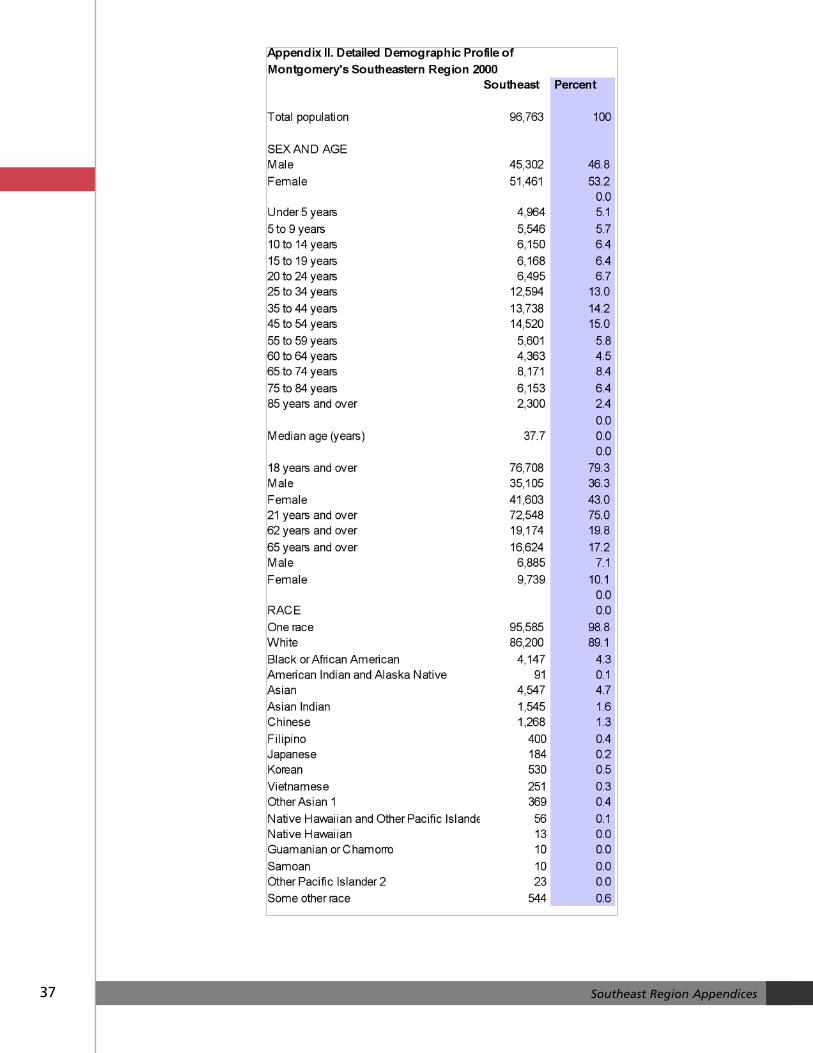
37 Southeast Region Appendices
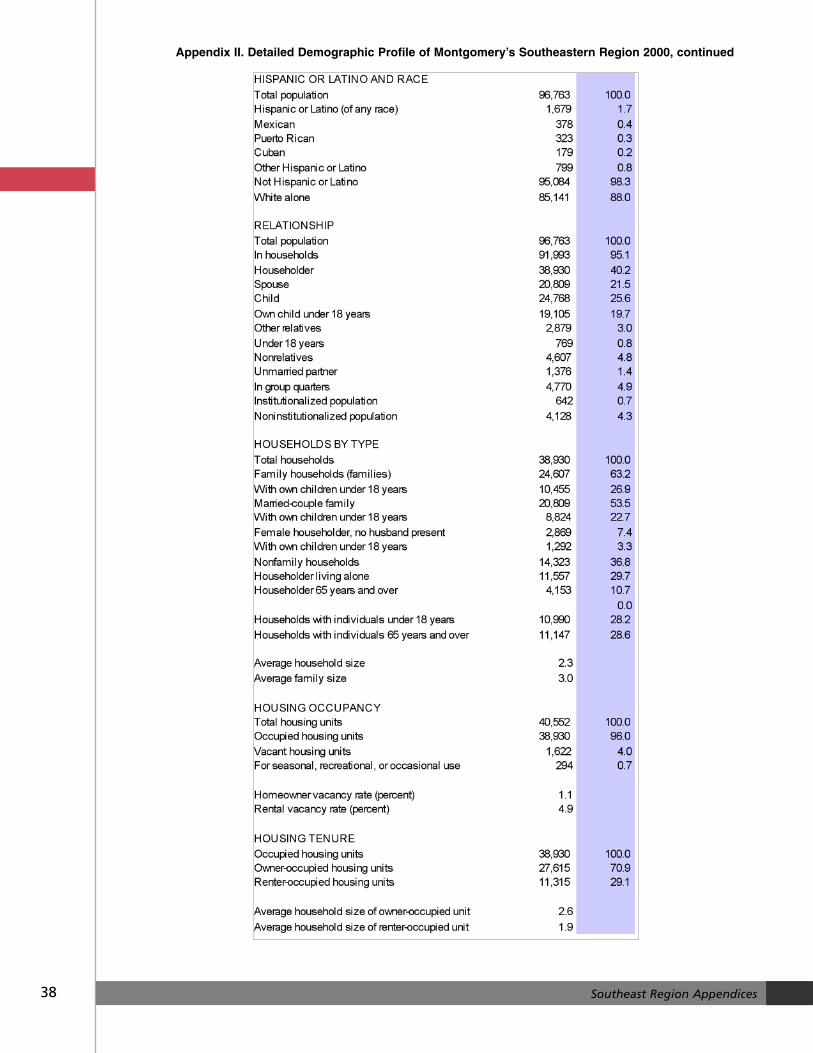
38 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued
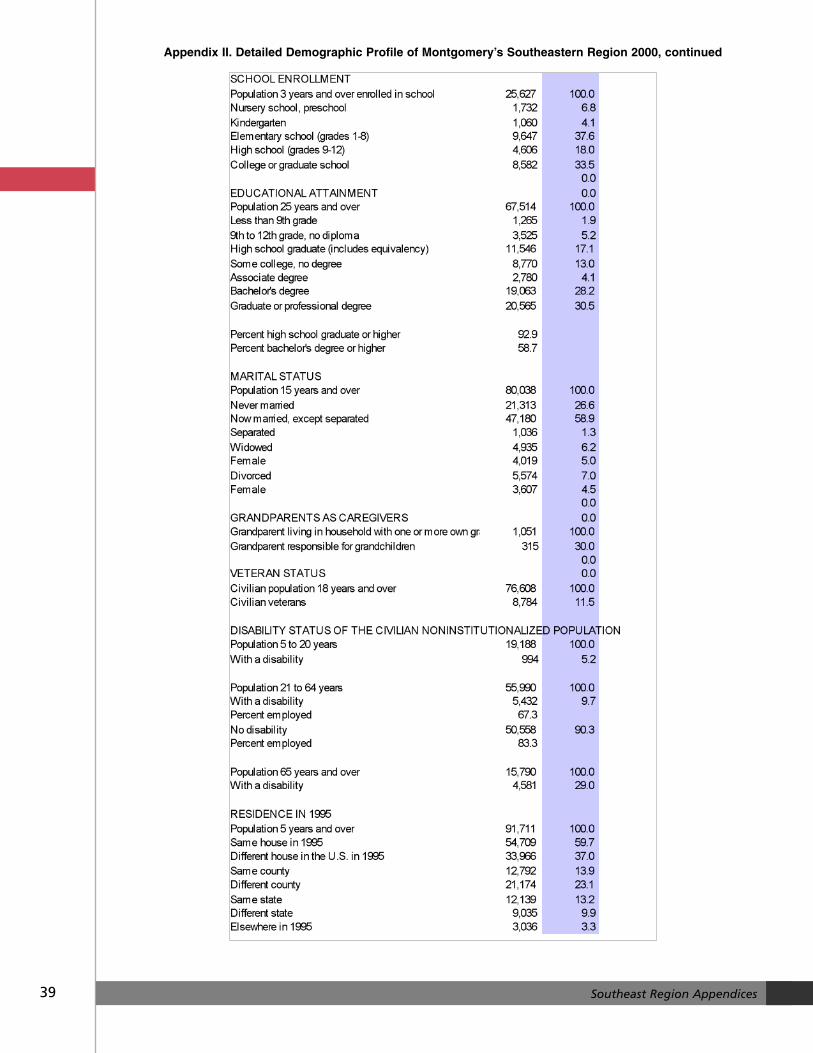
39 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued
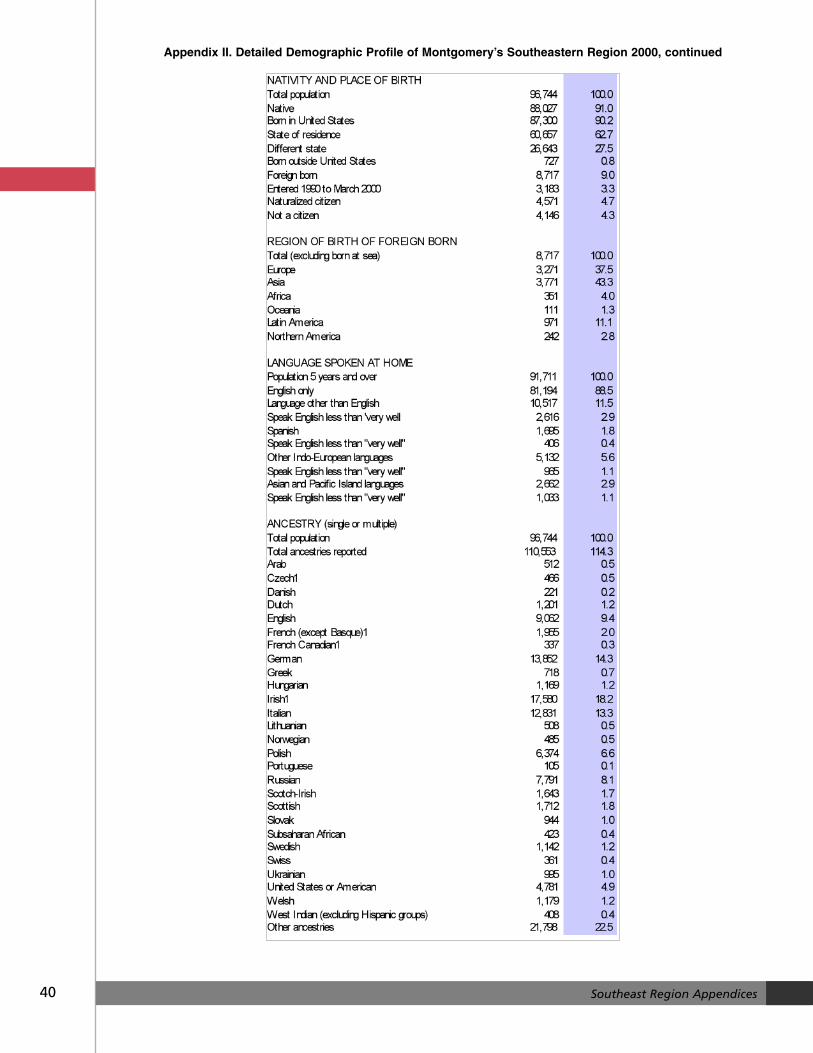
40 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued
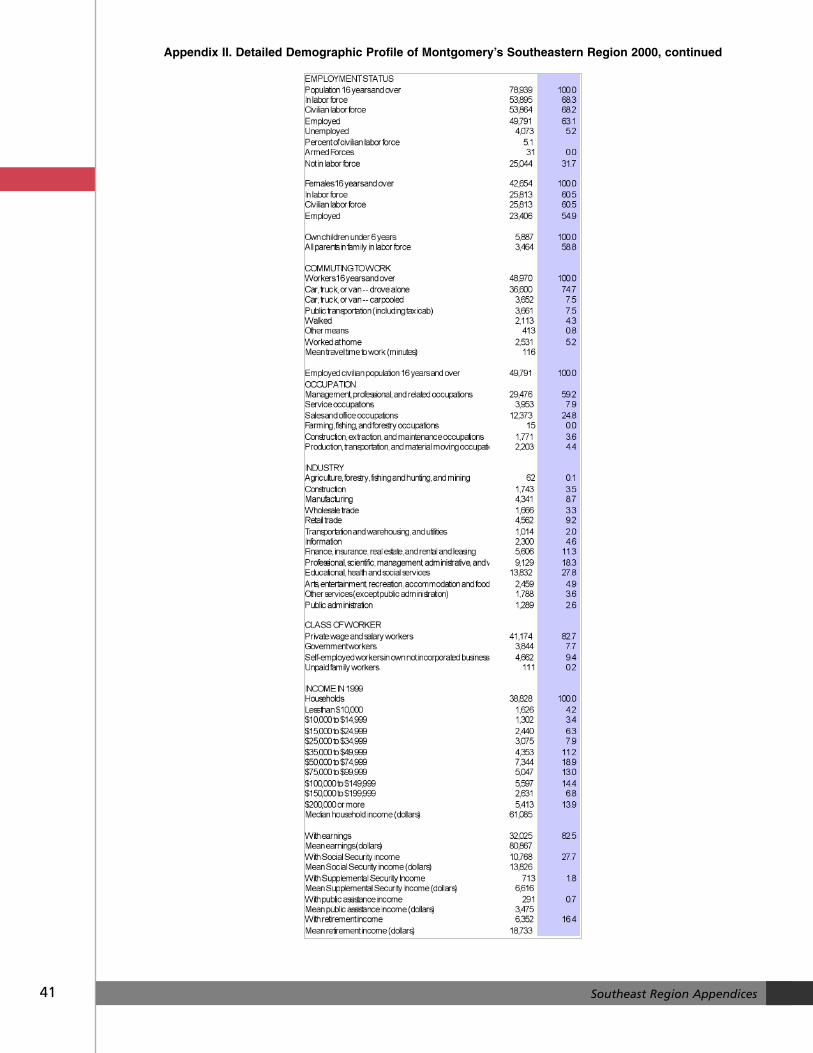
41 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued
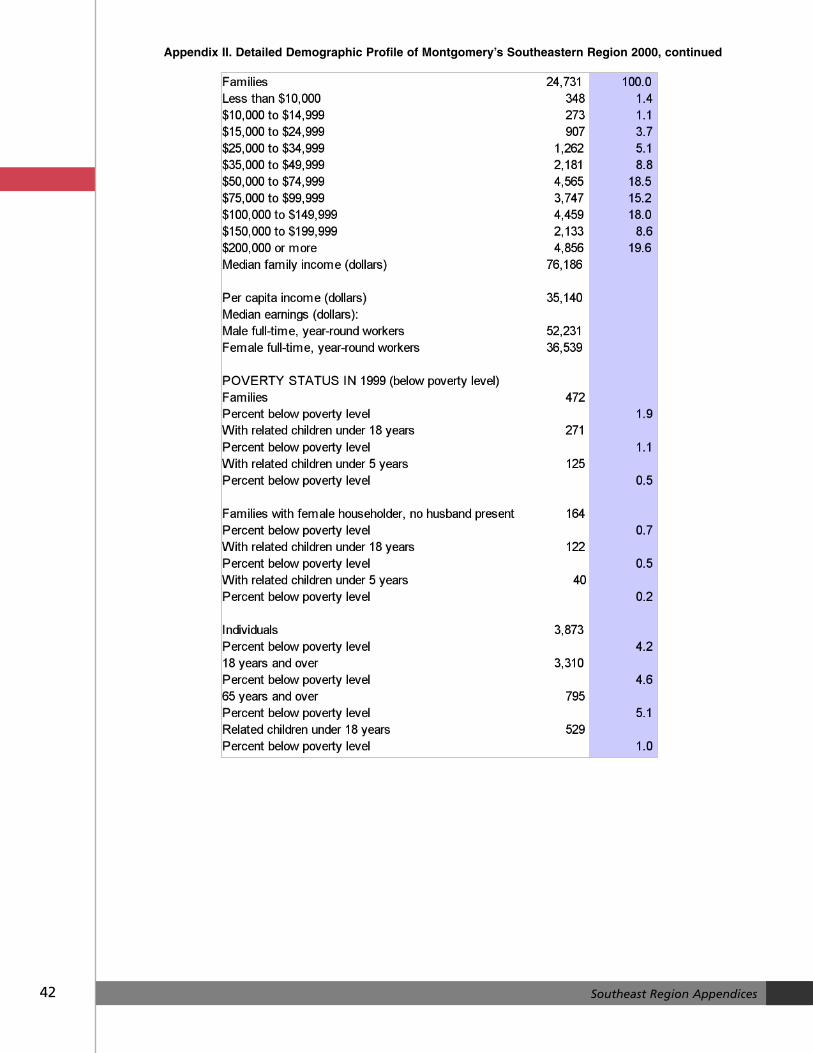
42 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued
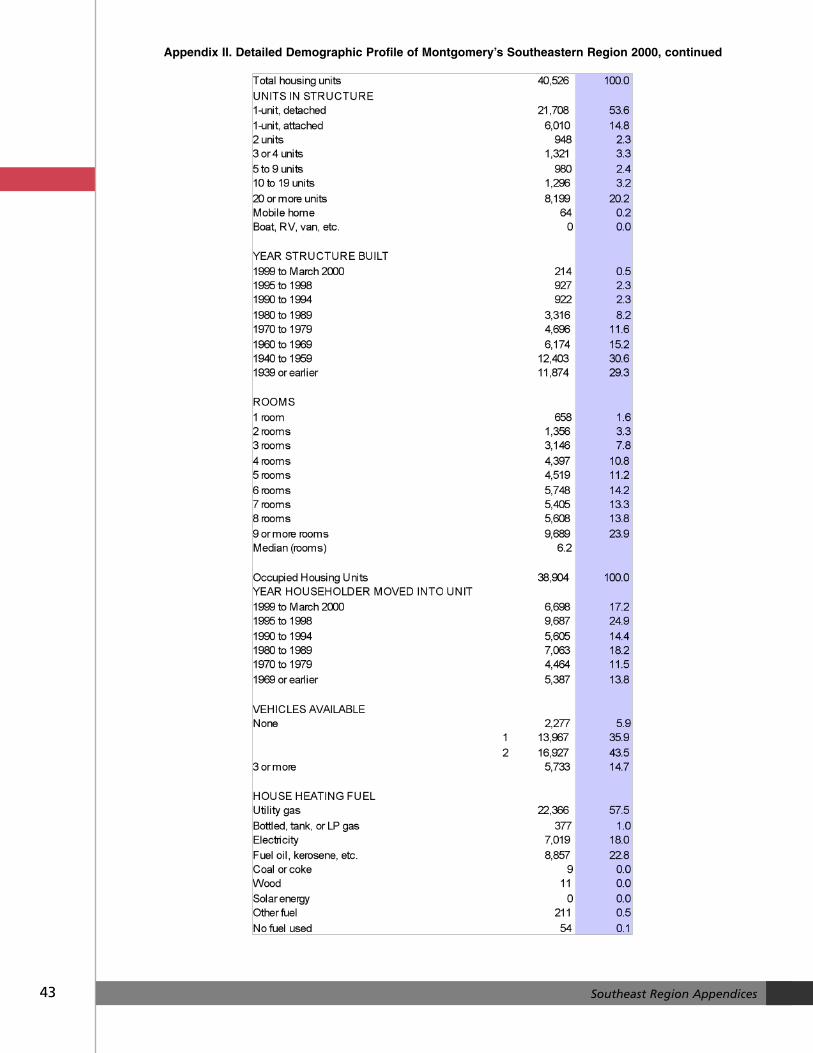
43 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued
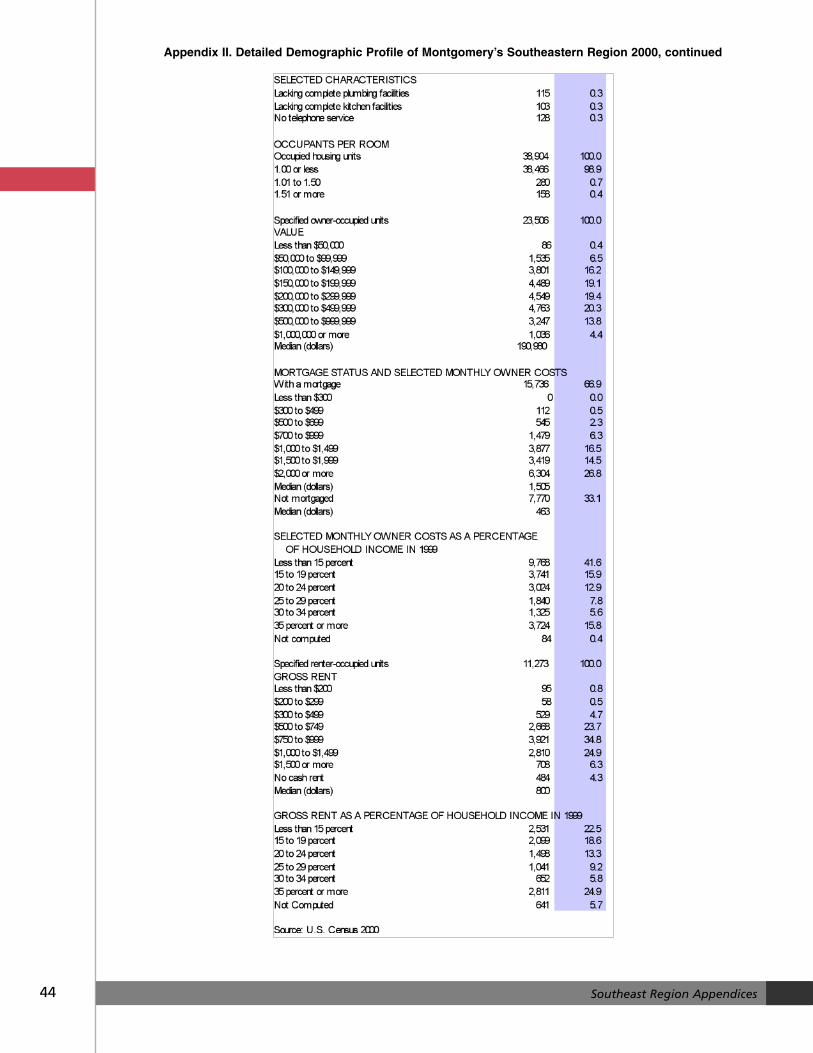
44 Southeast Region Appendices
Appendix II. Detailed Demographic Profile of Montgomery’s Southeastern Region 2000, continued





























