Embed Size (px)
Citation preview

SPECIAL CONTRIBUTION
An International Urogynecological Association(IUGA)/International Continence Society (ICS)joint terminology and classification of the complicationsrelated to native tissue female pelvic floor surgery
Bernard T. Haylen & Robert M. Freeman & Joseph Lee &
Steven E. Swift & Michel Cosson & Jan Deprest &Peter L. Dwyer & Brigitte Fatton & Ervin Kocjancic &
Chris Maher & Eckhard Petri & Diaa E. Rizk &
Gabriel N. Schaer & Ralph Webb
Received: 14 December 2011 /Accepted: 30 December 2011 /Published online: 12 April 2012# The International Urogynecological Association 2012
AbstractIntroduction and hypothesis A terminology and standardizedclassification has yet to be developed for those complicationsrelated to native tissue female pelvic floor surgery.Methods This report on the terminology and classificationcombines the input of members of the Standardization and
Terminology Committees of two International Organiza-tions, the International Urogynecological Association(IUGA) and the International Continence Society (ICS)and a Joint IUGA/ICS Working Group on ComplicationsTerminology, assisted at intervals by many external refer-ees. A process of rounds of internal and external review
International Urogynecology Journal, Vol. 23, No. 5, 2012. Copyright2012. This material is reproduced with permission of Wiley-Liss, Inc.,a subsidiary of John Wiley & Sons, Inc., and the InternationalUrogynecological Association.
This document is being published simultaneously in Neurourology andUrodynamics (NAU) and the International Urogynecology Journal(IUJ), the respective journals of the sponsoring organizations, theInternational Continence Society (ICS) and the InternationalUrogynecological Association (IUGA) in the closest issue of eachjournal to the end of April, 2012.
Standardization and Terminology Committee (IUGA)—Bernard T.Haylen, Robert M. Freeman, Joseph Lee, Steven E. Swift, Peter L.Dwyer, Eckhard Petri, Diaa E. Rizk, Gabriel N. Schaer
Standardization Steering Committee (ICS)—Robert M Freeman, RalphJ. Webb
Joint IUGA/ICS Working Group on Complications Terminology -Bernard T. Haylen, Robert M. Freeman, Steven E. Swift, MichelCosson, Chris Maher, Jan Deprest, Peter L. Dwyer, Brigitte Fatton,Ralph J. Webb
B. T. HaylenUniversity of New South Wales,Sydney, NSW, Australia
R. M. FreemanDerriford Hospital,Plymouth, Devon, UK
J. LeeMonash Medical Centre,Melbourne, VIC, Australia
S. E. SwiftMedical University of South Carolina,Charleston, SC, USA
Int Urogynecol J (2012) 23:515–526DOI 10.1007/s00192-011-1659-x

took place with decision making by collective opinion(consensus).Results A terminology and classification of complicationsrelated to native tissue female pelvic floor surgery has beendeveloped, with the classification based on category (C), time(T), and site (S) classes and divisions that should encompassall conceivable scenarios for describing operative complica-tions and healing abnormalities. The CTS code for eachcomplication, involving three (or four) letters and threenumerals, is likely to be very suitable for any surgical auditor registry, particularly one that is procedure-specific. Users ofthe classification have been assisted by case examples, colourcharts and online aids (www.icsoffice.org/ntcomplication).Conclusions A consensus-based terminology and classifica-tion report for complications in native tissue female pelvicfloor surgery has been produced. It is aimed at being a signif-icant aid to clinical practice and particularly to research.
Keywords Classification . Complication . Native tissue .
Female pelvic floor surgery
Preface
The Standardization and Terminology Committee of theInternational Urogynecological Association (IUGA), theStandardization Steering Committee of the InternationalContinence Society (ICS) and the Joint IUGA/ICS WorkingGroup on Complications Terminology seek to provide aterminology and a standardized classification for those com-plications arising from native tissue female pelvic floorsurgery. This document follows a similar document [1] forthose complications related directly to the insertion of pros-theses (meshes, implants, tapes) and grafts, also in femalepelvic floor surgery. It would then be, amongst its variousother possible applications such as medical records andsurgical audits (often procedure-specific), the basis for sci-entific clinical studies comparing complications from thedifferent types of female pelvic floor surgery. As the firstaim is to standardize the terminology used in this classifi-cation, the terms used in the title need to be initially defined.
Classification: A systematic arrangement into classesor groups based on perceived common characteristics[2]. N.B. Division: A separation into two or more parts.Complication: A morbid process or event that occursduring the course of a surgery that is not an essentialpart of that surgery (“surgery” replacing “disease” inthe definition; “course” includes postoperative of what-ever duration) [2].Related: Connected [3].Tissue: A collection of similar cells and the intercellu-lar substances surrounding them [2].Native: Pertaining to birth [2]. Autologous [2].
Introduction
In January 2011, the IUGA/ICS Joint Terminology andClassification of Complications related directly to the inser-tion of Prostheses (meshes, implants, tapes) and Grafts inFemale Pelvic Floor Surgery was simultaneously publishedin the International Urogynecology Journal and Neurourol-ogy and Urodynamics [1]. As usage of this classificationwas then proposed for large randomized clinical trials ofpelvic floor surgeries involving both (1) the insertion ofprostheses or grafts and (2) the use of native tissues alone,it became more evident that an equivalent classification forthe latter indication was not available.
The need and request for an equivalent native tissuesurgical classification (by clinical researchers) was deemeda separate challenge in itself after the efforts in producingthe first document. Desirably, if one was trying to comparesurgical complications, it would be easiest if the classifica-tions of the complications of the two different sets of
M. CossonUniversity Hospital,Lille, France
J. DeprestUniversity Hospital,UZ Leuven, Belgium
P. L. DwyerMercy Hospital for Women,Melbourne, VIC, Australia
B. FattonUniversity Hospital( Clermont-Ferrand, France
E. KocjancicDepartment of Urology, University of Illinois( Chicago, IL, USA
C. MaherWesley Hospital( Brisbane, QLD, Australia
E. PetriUrogynaecology Department, University of Greifswald,Greifswald, Germany
D. E. RizkPeterborough, ON, Canada
G. N. SchaerKantonsspital( Aarau, Switzerland
R. WebbNorfolk & Norwich University Hospital( Norfolk, UK
B. T. Haylen (*)St Vincent’s Clinic,Suite 904, 438 Victoria Street,Darlinghurst 2010 NSW, Australiae-mail: [email protected]
516 Int Urogynecol J (2012) 23:515–526

surgeries were of a similar style. Essentially, they werebeing performed in the same anatomical setting, involvingsimilar healing processes and a similar timeframe for heal-ing. The main difference was whether a surgical prosthesisor graft was additionally being introduced. An attempt wasthen made to apply the category (C), time (T), and site (S)classification for the prostheses and grafts [1] to nativetissue surgery. It became clear that this style of classificationmight also be suitable for the latter indication.
The analysis of synthetic meshes by Amid [4] may nothave been performed for suture materials in native tissuesurgery, particularly around the vagina, although many of
the findings and subsequent conclusions in relation to an“ideal” mesh material of Amid [4] and others [5, 6] [1]might still apply. Many healing abnormalities could occurwith the use of permanent sutures as might be required forsurgical strength and durability in such scenarios as vaginalvault suspension procedures, e.g., uterosacral or sacrospi-nous ligament colpopexies. Braided sutures, if left exposedto the vaginal cavity rather than buried beneath vaginal skin,appear particularly prone to the formation of surroundinginflammation, e.g., granulation.
Historically, discontinuation of a surgical procedure orthe use of a particular material in that procedure occurs
Table 1 Terminology involved in the classification
Int Urogynecol J (2012) 23:515–526 517

generally due to either (1) a lack of efficacy or (2) the natureor frequency of complications. Native tissue repairs are notwithout complications. It was noted [1] that prostheses orgrafts potentially add to the complication profile the aspectsof (1) trauma of insertion; (2) reaction of the body to theprosthesis in terms of inflammation or infection; (3) thestability of the prosthesis over time; (4) morbidity at thedonor site from harvesting an autologous graft. On reflec-tion, points (1) to (3) might still apply to certain permanentsuture materials in native tissue surgery.
The classification of complications based on category (C),time (T), and site (S) is consistent with the previous report forprostheses and grafts [1] and might appear familiar and againinitially complex. It is hoped that the following outline andexplanatory notes, as well as user-friendly tables and caseexamples might alleviate any residual concerns in regards tocomplexity. It would be of greater concern if the classificationdid not cover all the different complication scenarios, suchthat previously undefined additional terminology might beneeded.
Proposed new definitions
Complications involving native tissue female pelvic floorsurgery need to involve the following viewpoints of (1) localcomplications; (2) complications to surrounding organs; (3)systemic complications. As in the earlier document [1], thegeneric term of “erosion” (medically defined as the “state ofbeing worn away, as by friction or pressure” [2], does notnecessarily suit the clinical scenarios encountered. Its use isbest avoided to be replaced by terms with greater physicalspecificity and clarity.
The additional terms to be used are:
Prominence: Parts that protrude beyond the surfacewith no epithelial separation [2].Separation: Physically disconnected [3], e.g., vaginalepithelium.Exposure: A condition of displaying, revealing, exhib-iting, or making accessible [3] (e.g., a permanent suturevisualized through separated vaginal epithelium).Extrusion: Passage gradually out of a body structure ortissue [2] (e.g., a permanent suture protruding into thevaginal cavity—see patient 555 (Table 4) and caseexample 8.Compromise: Bring into danger [3].Perforation: Abnormal opening into a hollow organ orviscus [2].Dehiscence: A bursting open, splitting, or gaping alongnatural or sutured lines [2].Sinus tract formation: (Localized) formation of a fistu-lous tract towards vagina or skin, where there is no visiblesuture material in the vaginal lumen or overlying skin.
Granulation: Fleshy connective tissue projections on thesurface of a wound, ulcer or inflamed tissue surface [2].Ulcer: A lesion through the skin or a mucous membraneresulting from loss of tissue, usually with inflammation.Invagination: Vaginal mucosa folded and entrappedon itself, characterized by a fixed and tight area onexamination [7].
Category, time, and site (CTS) classification
The overall aim of the classification is to summarize any ofa large range of possible clinical scenarios into a code (“anumeric system for ordering and classifying information”—[2]) using as few as three numerals and three (or four)letters. No additional verbal description, possibly involvingundefined terminology, should be necessary.
Selection of categories
The selection of category (C) has used the principal that theleast severe complication would occur within the anatomicalsite of the procedure. More severe complications would in-volve (1) increasing involvement of surrounding anatomicalstructures; (2) involvement of surrounding organs; and (3)systemic compromise. The following seven categories (bynumber) have been formed:
1. Vaginal complication—no epithelial separation: Thisincorporates the terms prominence or excessive degreesof scarring or tethering.
2. Vaginal complication—smaller epithelial separa-tion or ulcer: A smaller (1 cm or less) degree ofvaginal epithelial separation or ulcer formation isinvolved.
3. Vaginal complication—larger epithelial separation orulcer or suture extrusion: A larger degree (more than1 cm) of vaginal epithelial separation or ulcer formation orsuture extrusion is involved.
Categories 1–3 have been separated into the followingdivisions:
1A–3A: Asymptomatic—abnormal finding: Theseare generally physician diagnosed at any ep-isode of clinical care. It can be argued that the“abnormal finding” aspects of category 1A,in particular, are not really complications asthe patient is not bothered by the potentialproblem. It may be, however, that the womanmay not have engaged in an activity that is
518 Int Urogynecol J (2012) 23:515–526

Tab
le2
Aclassificatio
nby
catego
ry(C),tim
e(T),andsite
(S)of
complications
relatedto
nativ
etissuefemalepelvic
floo
rsurgery
Int Urogynecol J (2012) 23:515–526 519

likely to provoke symptoms for herself, e.g.,pain or bleeding during sexual intercourse (orfor her partner), which would convert thesecomplications to category 1B.
1Aa–3Aa: Asymptomatic—abnormal finding: The ad-dition of an “a” specifies that the patient expe-riences no pain in association with theabnormal finding.
1B–3B: Symptomatic—unusual discomfort orpain; dyspareunia (for either partner).Bleeding or discharge may be possiblesymptoms.
1Bb–3Bb: Symptomatic—provoked pain only (dur-ing vaginal examination): The additionof a “b” to the category code specifiesthat pain, provoked only during vaginalexamination, is associated with the ab-normal finding.
1Bc–3Bc: Symptomatic—pain during sexual inter-course: The addition of a “c” to the cat-egory code specifies that pain, provokedduring sexual intercourse (patient only),is associated with the abnormal finding.
1Bd–3 Bd: Symptomatic—pain during physicalactivities: The addition of a “d” to the cate-gory code specifies that pain, provoked duringphysical activities, is associated with the ab-normal finding.
1Be–3Be: Symptomatic—spontaneous pain: Theaddition of an “e” to the category codespecifies that pain, spontaneously present
(i.e., without physical activity), is associatedwith the abnormal finding.
1C–3C: Clinical infection/inflammation: Signs oflocal tenderness are suggestive with thecombination of redness and a purulent dis-charge being more conclusive. The presenceof granulation should be accepted as repre-senting ongoing inflammation.
1C–3C (b–e): Infection—pain: The addition of the letters“b” through to “e” specifies that pain (asdefined in Table 3) is part or all of the infectedabnormal finding.
1D–3D: Abscess formation: This is a more seriouspossibility.
1D–3D (b–e): Infection—pain: The addition of the letters“b” through to “e” specifies that pain (as de-fined in Table 3) is part of the abnormal find-ing associated with abscess formation.
Category 4: Urinary tract compromise or perforation:This category class has been subdivided into:
4A: Small intraoperative defect: e.g., bladder perfora-tion. Such a complication does not generally createlonger-term compromise for the bladder if the defectis recognized and oversewn (if necessary), and someminor precautions are taken, e.g., short-term bladderdrainage, with suitable antibiotics commenced.
4B: Other lower urinary tract (bladder or urethral)complication or compromise: This division wouldincorporate injuries causing longer-term bladder issues,e.g., ongoing suture perforation, fistula, calculus aroundthe suture. This category also incorporates urinary re-tention directly related to the procedure requiring sub-sequent surgical intervention (apart from any form ofbladder drainage). The time and site divisions relates tothose for the surgical intervention.
4C: Ureteric or upper tract complication or compro-mise: This division is self-explanatory.
Category 5: Rectal or bowel compromise or perforation:This category class has been subdivided into:
Table 3 Grades of pain: subclassification of complication category
To specify the presence of pain (by patient only, not the partner) as partor all of the abnormal finding and the grade in terms of the presenceand severity or symptoms
a Asymptomatic or no pain
b Provoked pain only (during vaginal examination)
c Pain during sexual intercourse
d Pain during physical activities
e Spontaneous pain
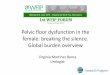
Fig. 1 Anterior midline 1.5 cm vaginal ulcer following removal of anethibond suture and granulation and after diathermy. Presentation withvaginal bleeding was 3 years after an anterior compartment repairincluding the insertion of the permanent suture for uterosacral ligamentplication. Classification: 3C T4 S1
520 Int Urogynecol J (2012) 23:515–526

5A: Small intraoperative defect: Such a complicationmay not generally be expected to cause compromiseif the defect is recognized and oversewn (as neces-sary) with appropriate precautions taken, e.g., short-term bowel rest is instituted with suitable antibioticscommenced.
5B: Rectal injury or compromise: This division wouldincorporate injuries causing longer-term rectal issues,e.g., ongoing suture perforation, fistula.
5C: Small or large bowel injury or compromise: Thisdivision would incorporate injuries causing longer-termbowel issues, e.g., ongoing suture perforation, fistula,obstruction.
5D: Abscess formation from bowel injury/compromise
Category 6: Skin and/or musculoskeletal complications:
6A: Asymptomatic: Physician-diagnosed complication atany episode of care.
6B: Symptomatic: e.g., discharge, pain, lump6C: Infection from skin ormusculoskeletal complication:
including sinus tract formation6D: Abscess formation from skin or musculoskeletal
complication:
Category 7: Patient compromise:This category recognizes that the patient might be
brought into systemic danger with some of the compli-cations in addition to any localized complication.
7A: Bleeding complication including hematoma: Thisdivision refers to any clinically diagnosed haematoma
as well as those where blood transfusion or surgicalintervention is a consideration.
7B: Major degree of resuscitation or intensive care:This division refers to significant hemodynamic orcardiopulmonary resuscitation directly related to theprocedure, and/or patient transfer for management inintensive care facilities. Included in this division ishematoma associated with sepsis, thus increasing pa-tient compromise.
7C: Mortality: The native tissue surgery, while not nec-essarily fatal at the time, has set in train further morbidevents leading to mortality.
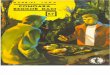
Fig. 2 Rectovaginal fistula presenting 4 weeks (photo taken at3 months) after a posterior vaginal repair concomitant with a vaginalhysterectomy and anterior vaginal repair. Presenting symptom wasvaginal passage of feces. Classification 5B T2 S3
Fig. 3 Ethibond suture in the bladder of a woman presenting withrecurrent urinary tract infections 7 years after a Burch colopsuspension.Classification: 4B T4 S3
Fig. 4 Abnormal scarring with “tethering” presenting 3 years after aBurch colposuspension and causing dyspareunia. Classification: 1BcT4 S1
Int Urogynecol J (2012) 23:515–526 521

N.B. Because of their systemic nature, 7B and 7Cwill generally not have a specific site division. Theywill then be denoted S 0.
Selection of time (T) divisions
The time (T) for the complication is when it is clinicallydiagnosed. This section incorporates four time periods, all
of the possible episodes where clinical care might be givenby the physician or sought by the patient. It might notalways be possible to predict with any particular surgerywhen particular complications might be more frequentlydiagnosed. This would depend on the results of a procedure-specific surgical audit using the classification. The earliesttime division (T1) might involve more perioperative issues,while later divisions (T2–T4)might be biased towards healingabnormality issues.
T1: Intraoperative—48 h: Perioperative complicationsclearly more likely.
T2: 48 h–2months: Bleeding, infection or healing com-plications more likely.
T3: 2–12 months: Later healing abnormalities more likely.T4: Over 12 months: Late healing abnormalities and oth-
er suture complications more likely.
Selection of site (S) divisions
The selection of these divisions incorporates the currentsites where complications have been noted:
S0: Systemic complications (no specific site): As men-tioned earlier, category divisions 7B (septic hematomaa possible exception) and 7C which are generallysystemic complications will be denoted S 0.
Fig. 5 Urethrovaginal fistula presenting 9 weeks after an anteriorvaginal repair. Classification: 4B T3 S1
Fig. 6 Pelvic pain, droppinghemoglobin consistent withhemorrhage in first 24 h after avaginal hysterectomy and CTevidence of a vaginal vaulthematoma. Managedconservatively for 4 days,evidence of sepsis (fever,increasing white cell count)prompted vaginal drainage andintravenous antibiotics.Classification: 7B T2 S3(initially 7A T1 S3)
522 Int Urogynecol J (2012) 23:515–526

S1: Vaginal: area of suture line: Perhaps the commonestsite for complications from native tissue vaginal sur-gery is close to the vaginal suture line.
S2: Vaginal: away from the vaginal suture line: As mostsuture lines would be midline, this would generally belateral in the vagina.
S3: Adjoining viscus: This division incorporates anyextraperitoneal, bladder, or rectal complication,but not intra-abdominal complications which areS5.
S4: Skin or musculoskeletal site: This division is relevantto any skin or musculoskeletal complications away
Fig. 7 Clinical evidence of vaginal urine loss 36 h after an anteriorcolporrhaphy (two previous anterior repairs). Deeper insertion of lat-eral fascial suture ligates the distal urethra near the vesico-ureteric
junction. CT evidence of discontinuity to distal urethra and extravasa-tion. Managed by interval stenting until extravasation proved to haveceased. Classification: 4C T1 S3
Int Urogynecol J (2012) 23:515–526 523

from the sites of the primary wound. Included mightbe cutaneous sinus or fistula formation and deep mus-cle pain from suture fixation.
S5: Intra-abdominal: Included in this section would bebowel perforation or obstruction.
CTS Classification: (Complete code):
Example of complete CTS code: 3B/T2/S3 (for sim-plicity, there is no “C” in front of the category class anddivision). The letters a to e may be added to the cate-gory code, e.g., 3Bc/T2/S3 to indicate that pain is partof the abnormality (“c”—pain with intercourse).
Classification guidelines
The following should be noted:
Multiple complications may occur in the same patient:These should be reported separately as noted in Table 4.There may be early and late complications in the samepatient: Again, these should be reported separately.All complications should be listedIf there is progression of a particular complication overtime, the highest final category is to be used: Progres-sion of an exposure or vaginal ulcer from asymptomaticto symptomatic; an exposure progresses from smaller tolarger; hematoma progresses from aseptic to septic.
Classification limitations
The classification does not note the specific type ofmaterial (suture) used: Use of permanent sutures otherthan those with the least morbidity (as described in the
“Introduction”) might be further reflected in an in-creased rate of the healing abnormalities.Functional issues (e.g., voiding and defecatory dysfunc-tion) are not included: Voiding dysfunction can bedefined as abnormally slow (assessed by urine flow ratedata) and/or incomplete (assessed by postvoid residual)micturition [8]. Surgical intervention for severe voidingdysfunction, namely urinary retention is included insection 4B.Urinary tract infections have not been included.Recurrences: Permanent sutures, like meshes andgrafts, are often used to prevent recurrence of pelvicorgan prolapse. However, the addition of permanentsutures might still fail to achieve a successful outcome(over whatever period) and a recurrence occurs. How-ever, it should be emphasized that recurrence is not acomplication.
Tables and case examples
Table 1: The definitions of terms used in the classification.Table 2: A classification by category (C), time (T), and
site (S) of complications directly related to nativetissue female pelvic floor surgery.
Table 3: Subclassification of categories 1 to 3 to specifythat pain is part of the abnormal finding and theimpact of that finding on patient’s symptoms.
Table 4: An example of a non-procedure specific table ofcomplications directly related to native tissuefemale pelvic floor surgery using the category(C), Time (T) and Site (S) system. The CTSClassification Code is placed adjacent to a de-scription of the complication.
Case Examples: Figs: 1–8: Eight clinical scenarios, thecomplications and the respective classi-fication codes.
Discussion
The present classification has been developed to be sensitiveto all possible physical complications related to native tissuefemale pelvic floor surgery. Both perioperative complicationsand healing abnormalities are covered. While this creates alarge number of possible scenarios, appropriate organizationhas still been possible by category (C), time (T), and site (S).The end point is a code of three letters (four if “a” to “e” areused) and three numerals. The addition of the pain subclassi-fication reflects the recognition of the authors that chronicpain, especially if in the higher subclasses (“c” to “e”), can
Fig. 8 Extruded goretex suture at posterior vaginal vault (behindcervix) 4 years after a sacrospinous hysteropexy. Only symptom wasintermittent PV bleeding. Classification: 3C T4 S1
524 Int Urogynecol J (2012) 23:515–526

be among the most disabling surgical outcomes from anyfemale pelvic floor surgery.
A key advantage of a standardized classification is thatall parties involved in female pelvic floor surgery includingsurgeons, physicians, nurses, allied health professionals, andindustry will be referring to the same clinical issue. It isanticipated that a (CTS) codified table of complications willbe a necessary part of reports of surgical procedures relevantto this document. The addition the current classification ofcomplications to the previous one [1] allows comparisonstudies of surgeries without and with prostheses and grafts.
It is acknowledged that to optimize the coverage ofcomplications, the classification [1] might still appear com-plex and not immediately mastered. However, as noted inthe Introduction, we anticipate that the patient cases (Table 4)
and case examples (Figs. 1, 2, 3, 4, 5, 6, 7, and 8) provided, thecolor charts, the ICS-IUGA Native Tissue (NT) ComplicationClassification Calculator (www.icsoffice.org/ntcomplication),as well as the experience with the previous classification [1]will ameliorate any initial concerns.
As with the earlier document [1], it has been a consensusview of the authors that a formal academic terminology andclassification should be completed prior to attempts at fur-ther simplification. The latter might run the risk of compro-mising coverage of complications.
Acknowledgements The co-authors acknowledge the support andgoodwill of the IUGA and ICS leadership in this third Joint Reportfrom the two Societies, following on from the Joint Reports on (1)Terminology for Female Pelvic Floor Dysfunction [8] and (2) Prosthe-ses and Graft Complications [1]. We thank Mr. Dominic Turner and
Table 4 Subclassification of categories 1 to 3 to specify that pain is part of the abnormal finding and the impact of that finding on patient’ssymptoms
Int Urogynecol J (2012) 23:515–526 525

Mr. Ashley Brookes from the ICS Office for their assistance andexpertise in developing the online aids to the previous document [1]and, to a lesser degree, the current document. Dr. Paul Moran from theBritish Society of Urogynaecology has also assisted in the progresstowards an ICS-IUGA Registry of Prosthesis and Graft Complications.
This document has involved five rounds of full review by co-authors and website publication. The comments of the following ex-ternal referees are gratefully acknowledged: Professor Linda Cardozo,Professor Mary Fitzgerald, Professor Elisabeth Constantini, ProfessorPeter Dietz, Professor Gamal Ghoniem, Professor Biagio Adile, Dr.Andri Nieuwoudt, Dr. Luis Abranches, Dr. Jia Wen, Dr. Giuseppe DiPaola, Dr. Antoine van Vijfeijken, Dr. Pail de Flamingh, Mr. P Jamjute,Mr. Declan Keane, Dr. Ahmed el Ghiaty, Dr. Joseph Gauta, Dr. AnnetteHolden.
Additional case examples and photos from Professor Peter Petros,Dr. Anna Rosamilia, Professor Judith Gow, Dr. Hanna Krause and Dr.Ian Tucker have been greatly appreciated.
Conflicts of interest
BT Haylen: No disclosuresRM Freeman: Educational meetings: Astellas and Pfizer. All incomefrom commercial trials and some of the honoraria go to his research fund.Locality lead for the NIHR Peninsula Collaboration for Leadership inApplied Health Research and Care (PenCLAHRC). PROSPECT: A grantholder for this nationally funded trial of prolapse surgery.J Lee: AMS: Acceptance of paid travel expenses or honoraria. AMS:Acceptance of payment for research (AMS external research grant).SE Swift: Pfizer: Acceptance of paid travel expenses or honoraria;Acceptance of payment for research. Astellas: Consultant.M Cosson: Ethicon: Acceptance of paid travel expenses or honoraria;Acceptance of payment for research; Consultant. AMS: Acceptance ofpaid travel expenses and honoraria; Acceptance of payment for re-search; Consultant.J Deprest: AMS: Acceptance of paid travel expenses or honoraria;Acceptance of payment for research; Consultant. Bard: Acceptance ofpaid travel expenses or honoraria; Consultant. Ethicon (J and J): Accep-tance of paid travel expenses or honoraria; Acceptance of payment forresearch; Consultant. Dynamesh: Acceptance of payment for research.PL Dwyer: Department research grant from American Medical Systems(AMS).B Fatton: Astellas: Consultant. Coloplast: Acceptance of payment forresearch. Ethicon (J and J): Acceptance of paid travel expenses orhonoraria. Novartis: Consultant.E Kocjancic: Coloplast: Consultant. Bard: Acceptance of paid travelexpenses or honoraria. AMS: Shareholder. Astellas: Consultant. Pfizer:Acceptance of paid travel expenses or honoraria.
C Maher: Director, Urogynaecology Society of AustralasiaE Petri: No disclosures.DE Rizk: No disclosures.GN Schaer: Astellas: Holding a position of influence in anotherprofessional society/association. Pfizer: Holding a position of influencein another professional society/association. Gynecare (Ethicon): Holdinga position of influence in another professional society/association.Novartis: Holding a position of influence in another professionalsociety/associationR Webb: Travel bursaries or honoraria: Pfizer or Astellas. Lecturefees: (departmental) Pfizer, Astellas. Research: Allergan Astellas.
References
1. Haylen BT, Freeman RM, Swift SE, Cosson M, Davila GW,Deprest J, Dwyer PL, Fatton B, Kocjancic E, Lee J, Maher C,Petri E, Rizk DE, Sand PK, Schaer GN, Webb RJ (2011) AnInternational Urogynecological Association (IUGA)/Internation-al Continence Society (ICS) joint terminology and classificationof the complications related directly to the insertion of pros-theses (meshes, implants, tapes) and grafts in female pelvicfloor surgery. Int Urogynecol J 22:3–15, and Neurourol Urodyn30: 5–15
2. Stedman’s Medical Dictionary (2006) Lippincott, Williams andWilkins. Baltimore. U.S.A.
3. Concise Oxford Dictionary (1995) Clarendon Press. Oxford4. Amid P (1997) Classification of biomaterials and their relative
complications in an abdominal wall hernia surgery. Hernia 1:15–215. Rosch R, Junge K, Hölzl F et al (2004) How to construct a mesh. In:
Schumpelick V, Nyhus LM (eds) Meshes: benefits and risks.Springer, Berlin, pp 179–184
6. Deprest J, Zheng F, Konstantinovic M et al (2006) The biologybehind fascial defects and the use of implants in pelvic organprolapse repair. Int Urogynecol J 17:S16–S25
7. Schmid C, O’Rouke P, Maher C (2011) Vaginal invagination. IntUrogynecol J Pelvic Floor Dysfunct 22(Suppl 1):S53–S54.doi:10.1007/s00192-011-1434-z, 22
8. Haylen BT, De Ridder D, Freeman RM, Swift SE, Berghmans B,Lee J, Monga A, Petri E, Rizk DE, Sand PK, Schaer GN (2010) AnInternational Urogynecological Association (IUGA)/InternationalContinence Society (ICS) joint report on the terminology for pelvicfloor dysfunction. Int Urogynecol J 21:5–26, and Neurourol Urodyn29:4–20
526 Int Urogynecol J (2012) 23:515–526