Embed Size (px)
Citation preview

RESPIRATORY MEDICINE (1999) 93, 700-708
An investigation of factors limiting aerobic capacity in patients with ankylosing spondylitis
R. CARTER*, I? RIANTAWAN”, S. W. BANHAM* AND R. D. STURROCK~
*Department of Respiratory Medicine and +Centre For Rheumatic Diseases, Royal Infirmay, Glasgow, U.K.
Ankylosing spondylitis (AS) has been shown to produce exercise limitation and breathlessness. The purpose of this study was to investigate factors which may be responsible for limiting aerobic capacity in patients with AS.
Twenty patients with no other cardio-respiratory disease performed integrative cardiopulmonary exercise testing (CPET). The results were compared to 20 age and gender matched healthy controls. Variables that might influence exercise tolerance, including pulmonary function tests (body plethysmography), respiratory muscle strength (MIP, MEP) and endurance (Tlim), AS severity assessment including chest expansion (CE), thoracolumber movement (TL), wall tragus distance and peripheral muscle strength assessed by maximum voluntary contraction of the knee extensors (Qds), hand grip strength and lean body mass (LBM), were measured in the patients with AS and used as explanatory variables against the peak 90, achieved during CPET.
AS subjects achieved a lower peak VO, than controls (252+ 1.4 vs. 33.1 k1.6 ml kgg’min-‘, rnean+~~~, P=O.OOl). When compared with controls, ventilatory response (?n/6C02) in AS was elevated (P=O.Ol); however gas exchange indices, transcutaneous blood gases and breathing reserve were similar to controls. AS subjects developed a higher HR/V02 response (P<O.Ol) on exertion but without associated abnormalities in ECG, blood pressure response or anaerobic threshold. The AS group experienced a greater degree of leg fatigue (P < 0.01) than controls at peak exercise. Although the breathlessness scores (BS) were comparable to controls at peak exercise, the slopes of the relationship between BS and work rate (WR) [AS 0.054 (0. l), Controls 0.043 (0.06); P < 0.051 and BS and % predicted oxygen uptake [AS 0.084 (0.18), Controls 0.045 (0.06); P<O.Ol] were steeper in the AS subjects.
There was weak association between peak VO, and vital capacity (r2% 12.0), MIP (11.8) but no association between Tlim, CE, Wall tragus distance or TL movement. The strongest association with aerobic capacity was between measurements of peripheral muscle strength (Qds; r=0.75 ; hand grip; r=0.47) accounting for 53% (P<O.OOl) and 23.5% (P<O.Ol)of the total variance in peak V02, respectively. The addition of LBM to Qds in the regression model significantly improved the explained variance to 783% (P<O.OOl).
This study shows that peripheral muscle function is the most important determinant of exercise intolerance in AS patients suggesting that deconditioning is the main factor in the production of the reduced aerobic capacity.
RESPIR. MED. (1999) 93, 700-708 0 1999 HARCOURT PUBLISHERS LTD
Introduction Ankylosing spondylitis (AS) is a chronic inflammatory arthropathy characterized by progressive stiffness and eventual fusion of the axial skeleton. A restrictive ventilatory defect has been extensively reported (l-6) in association with this condition but the relationship of the musculo-skeletal limitations and pulmonary impairment in affecting exercise tolerance has not been extensively investigated. Grimby et al. reported that four out of eight patients with AS complained of breathlessness on exertion (7) and in a study by Elliot et
Received 24 February 1999 and accepted in revised form 8 June 1999. Correspondence should be addressed to: Roger Carter, Principal Clinical Scientist, Department of Respiratory Medicine, Queen Elizabeth Building, Royal Infirmary, Alexandra Parade, Glasgow, G31 2ES, U.K.
0954-6111/99/100700+09 $12*00/O
al. there was significant reduction in exercise capacity of 6 patients with AS when compared to age matched controls and this was attributed to deconditioning or cardiovascular impairment (8). Anthropometric or musculoskeletal factors, as well as pulmonary function abnormalities, contribute to exercise intolerance but the relative contribution of these factors to the reduction of aerobic capacity in AS patients has not been quantitatively examined. Improved knowledge in this area would be of clinical importance, both in understanding the pathophysiological basis of exercise limitation and devising effective training/rehabilitation stra- tegies for sufferers of this condition.
The object of the present study was to identify and determine the individual and additive influence of respira- tory variables, AS severity and general fitness/decondition- ing on overall aerobic power, as assessed by maximal oxygen uptake during an integrative cardiopulmonary exercise test in AS patients.
@J 1999 HARCOLJRT PUBLISHERS LTD

AEROBICCAPACITYINANKYLOSING ~~NDYL~TIS 701
Patients and methods
PATIENT POPULATION
Twenty patients (13 male/7 female; mean age 46.5 SD 11.6 years) with definite AS (modified New York criteria) (9) were recruited from a tertiary referral AS Clinic. The recruitment was carried out with no reference to the presence of respiratory symptoms or exercise/smoking habits. Patients with a history of cardiac disease or taking beta-blockers, patients with exposure to radiation, asbestos or drugs associated with pneumonitis and patients with chest pain on deep inspiration were excluded, as were patients with significant pain in the hip, knee or ankle joints or with hip replacement precluding optimal exercise performance. Twenty age and gender matched healthy volunteers served as controls. Written informed consent was obtained from each subject prior to testing and the study was approved by the hospital ethics committee.
AS SEVERITY
Chest expansion was measured circumferentially around the chest wall at the level of the fourth intercostal space with the subject standing with hands on head and arms flexed in the frontal plane (18). The total range of the thoracolumber (TL) movement in the sagital plane was measured using a spondylometer and expressed as degrees (19). Wall tragus distance was used as an index of thoracic kyphosis and expressed in centimetres.
PULMONARY FUNCTION TESTING
Lung volumes and specific airways conductance (SG,,) were measured using a constant volume body plethysmo- graph (PK Morgan, Rainham, U.K.). The highest value obtained from three technically acceptable manoeuvres was reported as the vital capacity (VC). Mean values of thoracic gas volume (TGV), total lung capacity (TLC), and specific airway conductance (SG,,) were calculated from three technically satisfactory tests. Transfer factor for carbon monoxide was measured by the modified single breath technique (10) using a validated Transflow System (PK Morgan) (11). All procedures were performed in accor- dance with guidelines recommended by the British Thoracic Society and the Association of Respiratory Technicians and Physiologists (12). Standard reference values for lung volumes (13) conductance, and transfer factor (DL,,) were used (14). In AS subjects, the calculation of predicted values was based on the height prior to the onset of disease where this was reliable, or on arm span measurements.
Maximum voluntary ventilation was measured over 15 s using the pneumotachometer of the plethysmograph system. Each subject produced three efforts separated by a minimum of 3 min for recovery. The highest value was chosen for the subsequent calculation of the breathing reserve (BR) by the formula:
BR% = [l - Vzmax/MVV] x 100
RESPIRATORY MUSCLE FUNCTION AND ENDURANCE
Maximal inspiratory pressure, at functional residual capacity volume and expiratory pressure at total lung capacity were measured using a digital mouth pressure meter (Precision Medical, York, U.K.). This equipment has been shown to provide reliable and accurate measures of maximum respiratory pressures in normal subjects and in patients with respiratory disorders (15). A minimum of five efforts were made for each manoeuvre until three readings were obtained within 10%. The highest reading was taken to reflect peak pressure.
Respiratory muscle endurance was assessed using an assisted breathing protocol (16,17). The subject, with a noseclip in place, sat and breathed through a resistive training device (Pflex, Health Scan, U.S.A.) incorporating six adjustable alinear inspiratory orifices and a one-way expiratory valve. Mouth pressure was continuously dis- played on an oscilloscope for visual feedback via a differential pressure transducer connected to the mouth- piece of the resistive training device. The subject was instructed to inspire and expire according to the sound signal generated from an electrical metronome. Inspiratory duration (Ti) was set at 1.7 s and total breath duration (Ttot) at 2.6 s, producing a duty cycle (Ti/Ttot) of 0.4 and a breathing frequency of 14 mini. A square wave and target line were set on the oscilloscope screen and the subject was encouraged to maintain the required breathing pattern and target pressure for as long as possible. During testing the target pressure was set at 70% of MIP. The subject was encouraged to maintain the target pressure on the breathing pattern. Endurance time was defined as the moment at which the subject was unable to maintain the target pressure for three consecutive breaths.
PERIPHERAL MUSCLE FUNCTION
Peripheral muscle function was assessed by measuring both muscle strength (Knee extensors and hand grip) and amount (lean body mass). The force of the maximum voluntary contraction of the knee extensors was measured by the method described by Edwards et al. (20). The subject sat upright in an adjustable straight-backed chair with the lower leg dependent and the knee flexed to 90”. A cuff was placed round the leg just proximal to the maleolar and attached horizontally to an electrical strain gauge (Cranley and Co., U.K.) with a digital readout. The subjects performed three maximal voluntary contractions at ap- proximately 1 min intervals. The greatest peak force achieved was recorded. Peak tort was calculated from the product of four and the distance between mid-knee joint and mid-point of the lower leg strap, and was expressed in Newton-metre (N-m). Since the quadriceps femorus is the principle muscle engaged in knee extension the maximal force is abbreviated to Qds (21).
Right hand grip strength was measured using a hand- held dynometer (Takei Company, Japan) with digital readout. Peak grip strength was recorded from the

702 R. &RTER ETAL.
maximum of three efforts separated by 1 min intervals and expressed in kilogram watts (kgw). Lean body mass (LBM) was calculated from the sum of skinfold thicknesses at four sites, namely biceps, triceps, subscapula and superiliac
regions as described by Durning et al. (22) and expressed in kilograms.
CARDIOPULMONARY EXERCISE TESTING
Symptom limited exercise tests (CPET) were performed using an electrically braked bicycle ergometer (CardioKi- netics Ltd, Salford, U.K.) with the subject breathing through a low dead space, low resistance valve box. The valve box incorporates a flexible pneumotachograph system in the mouth-piece assembly (Flexiflow, PK Morgan, Rainham, U.K.) for the measurement of minute ventila- tion. The expired limb is fed through a mixing chamber from which samples of expired gas are analysed for the fractional concentrations of carbon dioxide and oxygen using an infrared spectrometer and fuel cell/zirconium analyser, respectively (Benchmark Exercise System, PK Morgan). The gas analysers were calibrated with certified gas mixtures and the pneumotachograph system was verified using a 3 1 syringe before each exercise test. Throughout each test, minute ventilation #E), oxygen consumption @OS), and carbon dioxide production (i7C02) were measured by on-line ventilation and expired gas analysis using standard equations (23). The ventilatory anaerobic threshold on exertion was calculated by the curve fitting method using a plot of *O, against *CO* (24).
Transcutaneous oxygen (t&02) and carbon dioxide (tcPCO3 tensions were monitored using a combined heated electrode (TINA, Radiometer Ltd, Copenhagen, Denmark) and its monitoring system (TCM3) after an in tivo calibration using an arterialized ear lobe capillary sample. This system has been validated against blood sampled directly from an arterial canmda during exercise in our laboratory (25-27) and has been shown to provide a reliable non-invasive assessment of gas exchange during exercise. The transcutaneous values and mixed expired gas values were used to derive the dead space ventilation to tidal volume ratio (V,/V-r) and the alveolar-arterial oxygen gradient (AaO,) using standard formulae (23).
Subjects were initially monitored for 2 min at rest whilst seated on the bicycle ergometer. They were then instructed to cycle with no additional load for 2 min. Thereafter the workload was increased by increments of 25 watts every 2 min and the subjects were encouraged to continue exercising until they could no longer sustain the desired pedalling frequency of 50 rpm. Exercise variables including transcutaneous values were measured or averaged over the last 30 s of each workload and at peak exercise. Exercise parameters were compared with the reference values of Jones et al. (28). The modified Borg category Scale (29) was used to rate the intensity of breathlessness and leg fatigue. An explanation of the scale was given prior to the tests and the scale was positioned in front of the subject. The subject was instructed to give a breathlessness score (BS) at the end of each workload and at peak exercise where, in addition, a
leg fatigue score was elicited (LS). BS values so obtained allowed the changes in magnitude of breathlessness in relation to work rate (WR) and oxygen uptake expressed as percent predicted maximum (irO*%) to be examined. The slopes of ABS/AV02% and ABS/AWR were expressed as means of slope from linear regression analysis of each subject’s data.
STATISTICAL METHODS
Descriptive data are presented as mean+ standard devia- tion (SD). Comparisons between the normal and AS subjects were performed using unpaired Student’s t-tests for continuous variables. Simple linear regression and Spear- man correlation coefficients were used to assess the relationship between peak QO, and other variables. The additive influence of explanatory variables and peak \iO, was examined using forward step-wise regression analysis. The proportion of variance accounted for by each relation- ship is reported as ?, expressed as a percentage. Level of probability was calculated from F or partial F values and statistical significance was assessed at the 5% level. A Minitab statistical package (Minitab Inc., U.S.A.) was used for data analysis.
Results The AS subjects exhibited a range of functional impairment and degree of spinal mobility. Chest expansion was 2.02 ems ( f 0.7 l), thoracolumber movement measured in the sagital plane was 51.4( & 17.7)% and wall tragus distance as an index of thoracic kyphosis was 16.9(-t 6.1) ems.
Patient demographic data and pulmonary function tests in comparison with the control group are presented in Table 1. VC and TLC were significantly smaller in the AS group averaging 78% and 86% of predicted, respectively (P<O@l). There was no significant difference between other parameters of lung function in AS subjects as compared to controls. In comparison with the control group there was no significant difference in measures of respiratory muscle strength although respiratory muscle endurance measurements were significantly shorter in AS subjects [Mean Tlim 130 (116) s] compared to controls [Tlim 258 (106); P<O.Ol]. Static peripheral skeletal muscle strength was significantly lower in the patients with AS than in the control subjects [Qds 69.5 (22.9) vs. 95.1 (15.6); PC O-01: Handgrip strength, kgW 35.3 (11.7) vs. 42.7 ( 9.9); P e O-05; respectively].
AEROBIC CAPACITY AND SYMPTOMS
Exercise data and modified Borg Scores for the AS subjects and controls is presented in Table 1. AS subjects achieved a lower work capacity averaging 123 watts compared with 148 watts in controls (P=O.Ol). Peak 60, was significantly lower in the AS group with a mean of 25.2+ 1.4 (75% predicted) compared to 33.1k1.6 ml kg-’ min-’ in the controls. The majority of the subjects in both groups ceased

AEROBIC CAPACITY IN ANKYLOSING SPDNDYL~S 703
TABLE 1. Comparison of baseline data and peak exercise values between Ankylosing Spondyhtis (AS) and control subjects
Age, years Gender, male:female Smokers: non-smokers Heigh, cm Weight, kg VC, % predicted FRC, % predicted RV, % predicted TLC, % predicted SGaw, kPa,-‘s-i DLCO, % predicted MVV, 1 min-’ MEP, cm water MIP, cm water Tlim, s Qds (% predicted) Hand grip strength, kgW Lean body mass (kg) Peak 902, 1 min-’ Peak 602, ml kg-‘min-’ Peak VO2, % predicted Work Capacity, watts Peak VC02, 1 min- ’ BS LS
Controls n=20 As subjects n=20
46.4 (12.2) 13:7 7:13 169 (9.0)
66.2 (13.7) 106 (18.9) 115 (21.7) 103 (25.1) 104 (15.3) 2.3 (0.5) 103 (19.9) 133 (6.6)
117-7 (32.9) 90.3 (29.9) 258 (106) 95.0 (15.0) 42.7 (9.9) 57.9 (10.2) 2.31 (2.4) 33.1 (10.2)
93 (9.7) 148 (24.6)
2.54 (2.0) 6.7 (3.5) 7.1 (3.2)
46.5 (12.3) 13:7 9:ll 167 (8.1)
57.5 (11.3)* 78 (12.0)*
122 (38.6) 110 (30.1) 86 (15.3)*
2.5 (0.4) 98 (23.7)
106 (7.4)* 111.4 (37.7) Ill.4 (37.7)
130 (116)* 69.5 (22.9)* 35.3 (11.7)* 49.6 (11.4)* 1.82 (2.6)* 25.2 (9.9)*
75 (10.6)* 123 (21.3)* 2.0 (3.1)* 6.5 (3.7) 8.7 (2.5)
*Values are Mean (SD). P-eO.01.
TABLE 2. Respiratory variables at rest and peak exercise in Ankylosing Spondylitis and controls
Control n=20 AS n=20
Rest Peak exericise Rest Peak exercise
f, Breaths mitt-’ VT, 1 VE, 1
tcPO,, mmHg tcPO,, mmHg vC/h--vD/vT
Aa?z, mHg
VIE/VCO& 1 I- l
BR, %
14 (4) 30 (10) 0.14 (0.2) 2.28 (0.95) 5.74 (1.2) 68.1 (15.9)
89 (8.2) 94 (10.1) 37 (3.7) 41 (5.1)
0.33 (0.09) 0.19 (0.05) 12 (4.6) 14 (5.3)
23.7 (4.5) 49 (10.2)
16 (3) 3s (12)* 0.45 (0.2) 1.81 (0.83)* 7.2 (2.1) 63.2 (18.9) 88 (0.1) 91 (11.2) 36 (3.9) 39 (4.9)
0.35 (0.10) 0.22 (0.06) 15 (5.2) 17 (6.0)
26.8 (4.1)* 40 (11.1)
Values are Mean (SD). *P-co.01
exercising complaining of leg fatigue. Leg fatigue scores P<O.Ol; respectively] were steeper in the AS group reported by AS subjects were higher than those reported by compared to controls. This indicates a higher intensity of control subjects at 8.7kO.3 and 7.1 kO.5, respectively breathing effort perceived among the AS subjects for (PcO.01). Mean breathlessness scores (BS) at peak exercise equivalent levels of work rate and oxygen uptake achieved. were comparable between the two groups. However, mean Table 2 shows the respiratory variables at rest and peak slopes of ABS/AWR [O-O54 (SD 0.1) vs. 0.043 (0.06), exercise. The ventilatory response (Vn/irCOz) on exertion P=O.O3] and ABS/AV02% rO.084 (0.18) vs. 0.045 (0.0.06) was higher in the AS subjects compared to controls

704 R. CARTER ETAL.
TABLE 3. Cardiocirculatory variables and peak exercise cardiac responses in ankylosing spondylitis (AS) and control subjects
Controls As subjects
Maximum HR, bts min-’ BP systolic, mmHg BP diastolic, mmHg HR/V02, bts 1-i Oxygen pulse, ml bt- ’ AT, 1 mini AT, % predicted VO2 max
*Values are Mean (SD). P<O.Ol.
161 (17.9) 153 (15.3) 160 (19.2) 166 (18.9) 81 (10.1) 83 (11.3)
39.5 (4.9) 50.0 (5.8)* 14.6 (2.9) 12.0 (3-l)* 1.35 (0.32) 1.10 (0.26)*
52 (5.0) 44 (5.1)
TABLE 4. The individual influences of explanatory variables on peak VO2 in 20 ankylosing spondylitis (AS) subjects
(“L:: MIP Tlim CR
(2~) Hand grip LBM Age Wall-tragus TL
(cm I-W) (4 (cm> (WV (ks) distance mobility
r2 12 (%) 11.8 0 0 53.0 23.5 13.5 10.7 0 0 F 4.29 4.21 0.49 0.25 22.16 8.35 4.9 3.87 0.67 0.07 P-value 0.05 0.05 0.49 0.62 <O.OOl 0.008 0.03 0.06 0.42 0.79
(26.8 + 1.1 and 23.7kO.9 l/l, respectively P=O.Ol) although breathing reserve (BR) remained adequate in both groups. The significantly smaller mean tidal volume and higher mean breathing frequency in the AS subjects compared to controls indicate the tendency of the AS subjects to reach higher levels of ventilation by shallower but more rapid breathing. There was no significant difference between indices of gas exchange (tcPO2, tcPCO2, Vr-,/Vr and Aa02 gradient ) at rest and at peak exercise in the AS subjects compared to controls. Table 3 shows the cardiocirculatory responses to exercise. AS subjects achieved a mean maximum heart rate of 85% predicted maximum. The heart rate response (HR/VO,) on exertion was elevated in AS subjects compared to controls (50.0f 3.5 and 39.5f 3.0 bts 1-i PcO.01). The AT (% predicted maximum V02) was significantly reduced in the AS group (44k2.1 and 52 + 1.9%, respectively P< 0.01) although this is still within the normal predicted range. Blood pressure response to exercise was not significantly different in the two groups.
RELATIONSHIP BETWEEN PHYSIOLOGICAL VARIABLES, BREATHLESSNESS AND EXERCISE PARAMETERS IN AS SUBJECTS
Table f shows the relationship between aerobic capacity (peak V02) and explanatory variables in AS subjects. There was only weak association between peak 902 and VC (?=12%) and peak902 and MIP (?=11.8%). Respiratory muscle endurance was not significantly related to aerobic power either directly or with the addition of other variables.
There was no direct association between aerobic power and chest expansion (CE) and the addition of other variables did not improve the total variance explained.
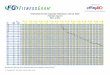
The strongest relationship between aerobic power and physiological variables were those which measured periph- eral strength. Qds (r=0.75) and handgrip strength (r=0.47) accounted for 53% and 23.5% (?) of the total variance (P<O.OOl and P<O.Ol, respectively). Since Qds was the single variable which exhibited the strongest association with peak 902 (Fig. l), other variables were added to the regression model in a step-wise fashion in order to explain the largest amount of the variability in peak 902 in this patient group. The addition of LBM significantly improved the explained variance to 78.3%. The addition of any other variable did not improve the explained variability in peak VO,. There was no significant association between any lung function variable, respiratory or skeletal muscle strength and endurance and aerobic capacity in the control group.
The best model explaining variability in peak VO, is as follows:
VOz peak (1min-i) =0.378 + 0.011 Qds (N-m) + 0.005 LBM (kg)
(F = 44.2), P< 0.001,2=‘78.3%, residuals SD 0.29, n= 20)
Discussion
This study found that mild to moderate ankylosing spondylitis was associated with a reduced aerobic capacity on exercise testing but that this reduction in aerobic

AEROBIC CAPACIRINANKYLOSJNG SPOND~ITIS 705
0 20 40 60 80 100 120 140 160 180 200
Qds Wm)
FIG. 1. Linear regression of peak 90, on Qds in 20 ankylosing spondylitis (AS) subjects. Peak V02(ml kg-‘min-‘) = 14.7 f0.10 Qds (N-m) [ adj.? 53.0%, F=22.16, P<O.OOl, n=20].
capacity was unrelated to the degree of the axial skeletal abnormality or respiratory muscle performance. Peripheral muscle factors, in particular, peripheral muscle strength and lean body mass, were most closely related to aerobic capacity in patients with mild to moderate ankylosing spondylitis.
The findings of mild to moderate reductions in vital capacity and total lung capacity are in agreement with previous studies (l-6). The normal transfer factor for carbon monoxide found in the AS subjects also agrees with other studies (7,8).
There was a reduced aerobic capacity in exercise testing in the present study which confirms earlier findings (8). Reduced ventilatory capacity was the aspect of pulmonary function most closely associated with exercise limitation although this association was weak. Previous authors have also found abnormalities of gas exchange on exercise testing in AS subjects. Thus Renzetti et aI. (30) observed an increased physiological dead space (VojVr) and mild arterial desaturation in 12 AS patients and postulated that the spondylitic process led to a relative decrease in ventilation in the upper part of the lung, whereas increased diaphragmatic excursions caused a relative increase in ventilation in the lower lung, regions leading to a widening of ventilation/perfusion ratios. Studies on regional ventila- tion in AS have shown conflicting results. Using Krypton 81M washout, Parkin et al. (31) found no significant differences in regional ventilation between 27 AS and 18 control subjects. In contrast, Stewart et al. (32) observed a reduction in inhaled xenon reaching the lung apices but normal xenon perfusion in nine AS subjects and suggested a relative impairment of apical ventilation in AS. It was suggested that this ventilation/perfusion abnormality con- tributes to inefficient gas exchange and reduced aerobic capacity in AS patients. In the present study although there is an impaired aerobic capacity in the AS subjects compared to the controls there is no evidence of gas exchange abnormalities at rest or during exercise, in AS subjects with
no cardiac or pulmonary parenchymal disease. This is in agreement with the findings of Miller and Sproule (33). There was a raised ventilatory response (irn/VCOz) in the AS patients compared to controls with a more rapid shallow breathing response on exertion. This is similar to finding in other studies of patients with spinal deformity (34-37). Even with the reduction in vital capacity, AS patients had a similar breathing reserve at peak 90, compared to controls suggesting the utilization of the same proportion of their ventilatory capacity at peak exercise.
Cardiac responses to exercise differed in the AS subjects compared to controls. AS subjects achieved the same maximal heart rate as normal subjects but at a reduced aerobic capacity suggesting a higher than normal heart rate response and a reduced stroke volume at equivalent work rates. It has previously been shown that a high heart rate response occurs when work is performed by a smaller muscle mass (38). The raised heart rate response and reduced aerobic capacity found in the AS subjects may therefore be a reflection of this reduced lean body mass.
Martinez et al. (39) recently highlighted the limitation of cardiopulmonary exercise testing in separating cardiac limitation from deconditioning. The findings of normal blood pressure response, normal oxygen pulse and an anaerobic threshold which, although lower than the control group, is within the normal range does not suggest any significant cardiac or vascular limitation on exercise testing in the AS subjects. An analysis of physiological variables that might affect exercise tolerance showed that aerobic capacity in AS patients was most closely related to peripheral muscle function. Pulmonary impairment and the severity of chest restriction appeared to influence aerobic capacity only weakly and to the same degree, suggesting that chest restriction in AS may express its influence on aerobic capacity through a reduction in vital capacity. In a study by Kearon et al. (37) a reduced work capacity was unrelated to the severity or nature of the spinal deformity in idiopathic scoliosis, but was related to

706 R. CARTER ETAL.
the reduction in vital capacity. They suggested, however, that the relationships between spinal deformity and pulmonary impairment and of pulmonary impairment to disability are so variable in these patients that no direct relationship between deformity and disability could be identified. Previous authors have shown a relationship between the degree of spinal deformity and aerobic capacity (40-41). Chong et al. (40) reported a definite trend between the angle of scoliosis and peak oxygen consumption in 38 subjects with spinal deformity. In the present study the weak association between the pulmonary impairment and degree of spinal abnormality may only reflect the mild to moderate status of the spinal deformity in this patient group.
The present study emphasizes the importance of assessing peripheral muscle function when evaluating exercise intol- erance. The most striking difference between patients with AS and the control group was in the measurements of peripheral skeletal muscle strength and lean body mass which were significantly reduced compared to controls. Peripheral muscle impairment has also been implicated as a contributor to reduced exercise capacity in other cardio- respiratory disorders (37,42,43). In patients with idiopathic scoliosis (37) peripheral muscle function, particularly leg muscularity, had the dominant influence on work capacity. In children with cystic fibrosis muscularity, as well as the degree of airflow obstruction, has been shown to contribute to reduced aerobic capacity (42). Peripheral muscle strength has also been found to be related to exercise performance in chronic heart failure but not in normal subjects (44). This last finding is in keeping with the conclusions of a study by Killian et al. (45) who observed that symptoms of leg fatigue rather than dyspnoea were frequently limiting exercise in patients with mild to moderate COPD. This is similar to the present study, in that leg fatigue was scored more highly than dyspnoea during exercise in the patients with ankylosing spondylitis, and was the main reason for termination of exercise in these patents. In a study of exercise limitation in COPD by Gosselink et al. (46) isometric quadriceps force (QF) was significantly related to 90, max (r=0.55). This suggests that peripheral muscle function as well as lung function is an important determinant of exercise capacity in COPD. Our findings in patients with ankylosing spondylitis, who do not show any major impairment in pulmonary function, suggests that peripheral muscle function is the most important determi- nant of aerobic capacity in these patients. Reduced muscle function may be caused by loss of endurance, loss of strength of the muscle or both. In patients with COPD it is suggested that inactivity, hypoxaemia and malnourishment in combination lead to alterations in fibre type distribution, reduction in capillary density, decrease in mitochondrial population and ‘inertia’ in the oxidative machinery of peripheral muscles (46,47). If muscle oxidative metabolism reaches its limits owing to lack of oxygen delivery or inefficient utilization then the muscles will switch to anaerobic metabolism resulting in intra-muscular lactic acidosis which will contribute to reduced exercise capacity. In the present study, the anaerobic threshold on exertion was significantly reduced in ankylosing spondylitis com- pared to normal controls suggesting that similar mechan-
isms of peripheral muscle impairment may be operative in these patients. A further explanation for the reduced aerobic capacity could be loss of muscle mass, resulting in a reduction in muscle strength, compromising its ability to overcome the load applied to the muscle during exercise. The relationship between aerobic capacity and the volume of muscle to do work is well recognised in healthy children and young adults (48,49). In addition, lean body mass has been shown to complement measures of pulmonary function in the prediction of disability in adults with pulmonary impairment (50,51). Previous studies in patients with idiopathic scoliosis (37), cystic fibrosis (42) and COPD (47) have demonstrated a negative influence of the reduction in lean body mass on exercise performance. A study by Palange et al. (47) has shown an inverse correlation between percent ideal body weight and %‘Oz time constant during moderate exercise demonstrating that in COPD patients, the decline in body mass parallels the impairment of muscle aerobic capacity. We have found that the inclusion of lean body mass (LBM) to the regression analysis with Qds significantly improved the explained variance. Lean body mass can be used as an index of muscle mass (52) and the metabolic demands of the muscles during exercise will decrease with a reduction in mass. Hence, LBM exerts a significance influence on peak 7j02. Thus impaired peripheral muscle strength and reduced muscle mass contribute to the reduced aerobic capacity in patents with ankylosing spondylitis which is similar to the findings in patients with other forms of cardio-respiratory disorders.
This study shows that aerobic capacity is commonly reduced in patients with AS. Although a degree of restrictive defect is not uncommon, pulmonary impairment does not significantly limit aerobic capacity in this group of AS patients. This study suggests that peripheral muscle function is the most important determinant of exercise intolerance in mild to moderate AS patients. Diseases leading to spinal deformity vary from trivial to grossly deforming with respiratory failure and car pulmonale. In patients with more severe pulmonary or spinal deformity other factors, including pulmonary impairment, would be expected to play a greater role in exercise limitation. Previous studies, however, have shown that lung function and nutritional status were independent in advanced cystic fibrosis (42). In addition, Bjure et al. (53) have shown that cardiovascular and peripheral muscle training improved work capacity in patients with idiopathic scoliosis, despite moderately severe pulmonary impairment which remained unchanged. As Kearon et al. (37) have suggested, this emphasizes that peripheral muscle conditioning and their circulatory interaction are clinically important determi- nants of functional status in patients with spinal deformity. Peripheral muscle training has also been found to improve exercise tolerance in coronary artery disease (53) and COAD (54). Interactions aimed at improving peripheral muscle function in patients with ankylosing spondylitis would also be expected to improve exercise tolerance and reduce exertional symptoms.
The reason for reduced peripheral muscle function in patients with ankylosing spondylitis is complex. Muscle weakness and fatigue may occur secondary to inadequate

AEROBIC CAPACITYINANKKOSNG SPONDYLITIS 707
muscle deconditioning. A possible explanation of this impaired muscle function in AS is the relative lack of physical activity consequent to the chronic nature of the disease. Cosmetics may play an important role, in that the deformed patients will not expose themselves in the usual sporting activities. In addition, altered transmission of stress through a deformed spine may lead to pain which limits activity. The findings of this study therefore suggest that a strategy to improve muscle function should be given priority in any rehabilitation/training programme in AS patients.
References 1. Rogan MC, Needham CD, McDonald I., Effect of
ankylosing spondylitis on ventilatory function. Clin Sci 1955; 14: 91-96.
2. Sharp JT, Sweany SK, Henry JP, Pietras RJ, Meadows WR. Lung and Thoracic compliances in ankylosing spondylitis. J Lab Clin Med 1964; 63: 254-263.
3. Feltelius N, Hedenstrom H, Hillerdal G, Hallgren R. Pulmonary involvement in ankylosing spondylitis. Ann Rheum Dis 1986; 45: 736-740.
4. Citrin DL, Boyd G, Bradley GW. Ventilatory function and transfer factor in ankylosing spondylitis. Scot Med J 1973; 18: 109-113.
5. Miller JM, Sproule BJ. Pulmonary function in ankylos- ing spondylitis. Am Rev Respi Dis 1964; 90: 376-382.
6. Fisher LR, Crawley MID, Holgate ST. Relation between chest expansion, pulmonary function and exercise tolerance in patients with ankylosing spondy- litis. Ann Rheum Dis 1990; 49: 921-925.
7. Grimby G, Fugl-Meyer AR, Blomstrand A. Partition- ing of the contributions of rib cage and abdomen to ventilation in ankylosing spondylitis. Thorax 1974; 29: 179-184.
8. Elliot CG, Hill TR, Adams TE, Crapo RO, Nietrzeba RM, Gardner RM. Exercise performance of subjects with ankylosing spondylitis and limited chest expan- sion. Bull Eur Physiopathol Respir 1985; 21: 363-368.
9. Goie The HS, Steven MM, Van Der Linden SM, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis: A comparison of the Rome, New York and modified New York in patients with a positive clinical history screening test for ankylosing spondylitis. Br J Rheumatol 1985; 24: 242-249.
10. Ogilvie CM, Forster RE, Blakemore WS, Morton JW. A standardized breath holding technique for the clinical measurement of the diffusing capacity of the lung for carbon monoxide. J Clin Invest 1957; 36: 1-17.
11. Carter R. A validation of the Morgan Transflow for the measurement of the single breath diffusing capacity. Inspire 1997; 1: 10-l 1.
12. The British Thoracic Society and the Association of Respiratory Technicians and Physiologists. Guidelines for the measurement of respiratory function. Resp Med 1994; 88: 165-194.
13. Grimby G, Soderholm B. Spirometric studies in normal subjects. III Static lung volumes and maximum voluntary ventilation in adults with a note on physical fitness. Acta Med &and 1963; 173: 199-206.
14. Cotes JE, Chinn DJ, Quanjer PH, Rota J, Yemault JC. Standardisation of the measurement of transfer factor (diffusing capacity). Report of Working Party: Stan- dardisation of Lung Function Tests, European Com- munity for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J 1993; 6 (Suppl. 16): 41-52.
15. Hamnegard CH, Wragg S, Kyroussis D, Aquilina R, Moxham J, Green M. Portable measurement of maximum mouth pressures. Eur Respir J 1994; 7: 398401.
16. Nava S, Crotti P, Gurrieri G, Fracchia C, Rampulla C. Effect of a B2-agonist (Broxaterol) on respiratory muscle strength and endurance in patients with COPD with irreversible airways obstruction. Chest 1992; 101: 133-140.
17. Belman MJ, Shadmehr R. Targeted resistive ventila- tory muscle training in chronic obstructive pulmonary disease. J Appl Physiol 1988; 65: 2726-2735.
18. Moll JMH, Wright V. An objective clinical study of chest expansion. Ann Rheum Dis 1972; 31: 1-8.
19. Sturrock RD, Wojtulewski JA, Hart FD. Spondylo- metry in a normal population and ‘in ankylosing spondylitis. Rheumatol Rehab 1973; 12: 135-142.
20. Edwards RHT, Young A, Hosking GP, Jones DA. Human skeletal muscle function: Description of tests and normal values. Clin Sci Mol Med 1977; 52: 283- 290.
21. Houtz SJ, Fisher FJ. Analysis of muscle action and joint excursion during exercise on a stationary bicycle. J Bone Joint Surg (Am) 1959; 41: 123-131.
22. Durnin JVGA, Womersley J. Body fat assessed from total body density and its estimation from skinfold thicknesses: measurements on 481 men and women aged 16 to 72 years. Br J Nutr 1974; 32: 77-97.
23, Cotes JE. Lung Function 4th Ed, Oxford: Blackwell, Scientific Publications 1978.
24. Beaver Wl, Wasserman K, Whipp BJA. New method for detecting anaerobic threshold by gas exchange. J Appl Physiol986; 60: 202&2027.
25. Carter R. Transcutaneous oxygen and carbon dioxide monitoring in the adult patient. Care Crit Ill 1988; 4: 13-15.
26. Carter R. The measurement of transcutaneous oxygen and carbon dioxide tension during exercise testing. Breath 1989; 38: 2-6.
27. Sridhar MK, Carter R, Moran F, Banham SW. Use of a combined oxygen and carbon dioxide electrode in the estimation of gas exchange during exercise. Thorax 1993; 48: 643-647.
28. Jones NL, Makrides L, Hitchcock C, Chypehar T, McCartney N. Normal standards for an incremental progressive cycle ergometer test. Am Rev Respir Dis 1985; 131:700-708.
29. Borg GAV. Psychophysical bases of perceived exertion. Med Sci Sports Exert 1982; 14: 377-381.

708 R. CARTERETAL.
30. Renzetti AD, Nicholas W, Dutton RE, Jivoff L. Some effects of akylosing spondylitis on pulmonary gas exchange. New Eng J Med 1960; 262: 215-218.
31. Parkin A, Robinson PJ, Hickling P. Regional lung ventilation in ankylosing s$ondylitis. Br J Radio1 1982; 55: 833-836.
32. Stewart RM, Ridyard JB, Pearson JD. Regional lung function in ankylosing spondylitis. Thorax 1976; 31: 433-437.
33. Miller JM, Sproule BJ. Pulmonary function in ankylos- ing spondylitis. Am Rev Respir Dis 1964; 90: 376-382.
34. DiRocco PJ, Breed AL, Carlin JL, Reddan WG. Physical work capacity in adolescent patients with mild idiopathic scoliosis. Arch Phys Med Rehabil 1983; 64: 476-478.
35. Kesten S, Garfinkle SK, Wright T, Rebuck AS. Impaired exercise capacity in adults with moderate scoliosis. *Chest 1991; 99: 663-666.
36. Bjure J, Grimby G, Nachemson A, Lindh M. The effect of physical training in girls with idiopathic scoliosis. Acta Orthop Stand 1969; 40: 325-333.
37. Kearon C, Viviani GR, Killian KJ. Factors influencing work capacity in adolescent idiopathic thoracic scolio- sis. Am Rev Respir Dis 1993; 148: 295-303.
38. Cotes JE, Berry G, Burkinshaw L, Davies CTM, Hall AM, Jones PRM, Knibbs AV. Cardiac frequency during submaximal exercise in young adults; relation to lean body mass, total body potassium and amount of leg muscle. Q J Exp Physiol 1973; 58: 239-250.
39. Martinez FJ, Stanopoulos I, Acero R, Becker FS, Pickering R, Beamis JF. Graded comprehensive cardiopulmonary exercise testing in the evaluation of dyspnoea unexplained by routine evaluation. Chest 1994; 105: 168-174.
40. Chong KC, Letts RM, Cumming GR. Influence of spinal curvature on exercise capacity. J Pediatr Orthop 1981; 1: 251-254.
*41. DiRocco PJ, Vaccaro P. Cardiopulmonary function- ing in adolescent patients with mild idiopathic scoliosis. Arch Phys Med Rehabil 1988; 69: 198-201.
42. Marcotte JE, Canny GJ, Grisdale R, Desmond K et al. Effects of nutritional status on exercise performance in advanced cystic fibrosis. Chest 1986; 90: 375-379.
43. Coates AL, Boyce P, Muller D, Meams M, Godfrey S. The role of nutritional status, airways obstruction, hypoxia and abnormalities of serum lipid composition in limiting exercise tolerance in children with cystic fibrosis. Acta Physiol Stand 1980; 69: 353-358.
44. Lipkin DP, Jones DA, Round JM, Poole-Wilson PP. Abnormalities of skeletal muscle in patients with chronic heart failure. Int J Cardiol 1988; 18: 187-195.
45. Killian KJ, Leblanc P, Martin DH, Summers E, Jones NL, Moran Campbell EJ. Exercise capacity and ventilatory, circulatory, and symptom limitation in patients with chronic airflow limitation. Am Rev Respir Dis 1992; 146: 935-940.
46. Gosselink R, Roosters T, Decramer M. Peripheral muscle weakness contributes to exercise limitation in COPD. Am J Respir Crit Care Med 1996; 153: 976-980.
47. Palange P, Forte S, Onorati P, Paravati V, Manfredi F, Serra P, Carlone S. Effect of reduced body weight on muscle aerobic capacity in patients with COPD. Chest 1998; 114: 12-18.
48. Davies CTM. Maximum aerobic power in relation to body composition in healthy sedentary adults. Hum Biol 1972; 44: 127-139.
49. Davies CTM. Body composition and maximal exercise performance in children. Hum Biol 1972; 44: 195-214.
50. Cotes JE, Zejda J, King B. Lung function impairment as a guide to exercise limitation in work related lung disorders. Am Rev Respir Dis 1988; 137: 1089-1093.
5 1. Schols AMW, Mostert R, Soeters PB, Wouters EFM. Body composition and exercise performance in patients with chronic obstructive pulmonary disease. Thorax 1991; 46: 695-699.
52. Lukaski HC. Methods for the assessment of human body composition: traditional and new. Am J Clin Nutr 1987; 46: 537-556.
53. McCartney N, McKelvie RS, Haslam DRS, Jones NL. Usefulness of weightlifting training in improving strength and maximum power output in coronary artery disease. Am J Cardiol 1991; 67: 939-945.
54. Simpson K, Killian K, McCartney N, Stubbing DG, Jones NL. Randomized controlled trial of weightlifting exercise in patients with chronic airflow limitation. Thorax 1992; 47: 70-75.