Embed Size (px)
Citation preview
Establishing an Occupational Health and Infection Control Program in a Large Ambulatory Care Facility
April 2011
Principal Investigator/Applicant Annalee Yassi
RS2008‐IG23

INNOVATION AT WORK: FINAL REPORT FILE #: RS2008-IG23
Establishing an Occupational Health and Infection Control Program in a
ty Large Ambulatory Care FaciliAnnalee Yassi, Elizabeth Bryce, L
arf, Lyndsay O’Hara. inda Kingsbury,
Sydney Sch
pril 2011 A This research is supported with funds from WorkSafeBC (Workers' Compensation Board of British Columbia).
1 | P a g e
Table of Contents
Research/Project Findings and Workplace Health and Safety Implications……………………… 3 Executive Summary……………………………………………………………………………………………………….. 4
………………………………………………………………... 8 The Research Problem and Context……………… Methodology and Research/Project Findings
Project Timeline………………………………………………………………………………………………...11 Part 1‐ Workplace Assessments …………………………………………………………………………13 Part 2‐ Glo‐Germ Environmental Audits …..……………………………….....................................18 Part 3‐ Knowledge, Attitudes and Practice Survey ………………………………………………21
Part 4‐ Healthcare Worker and Public Education Sessions…………………………………...33 Implications for future research/projects on workplace health and safety……………………..34 Identification of immediate and long‐term benefits of the findings or results………………….35 Identification of relevant user groups for the research/project results…………………………..38 Dissemination/knowledge transfer……………………………………………………………………………….39
eferences… R …………………………………………………………………………………………………………………40
ppendix I‐ A Logical Framework Analysis……………………………………………………………………….43
ppendix II‐ A Workplace Assessment Tool ………………...…………………………………………………44
ppendix III A
‐ Glo‐Germ Environmental Audit Template ………………………………………..……..63
Appendix IV‐ Knowledge, Attitudes and Practice Worker Questionnaire…………………….…64
ppendix V‐ A
FAQ Sheet…………………………………………………………………………………………….….75
Appendix VI‐ Infection Control Basics for Medical Students…………………………………………80
2 | P a g e

Research/Project Findings and Workplace Health and Safety Implications
• Ambulatory care poses similar hazards to healthcare workers as acute care but this is not
necessarily appreciated when the infrastructure requirements are established. Building in an
Occupational Health and Infection Prevention and Control program into the management
structure for all ambulatory care partners (private, public and teaching staff) is important and
can be done retrospectively.
• Workplace assessments using a comprehensive checklist can catalyze improvements in
workplace conditions. Several themes regarding concerns and immediate concerns emerged
from the assessments;
a) Lack of signage, manuals and directives; b) physical plant issues c) equipment and procedures;
d) ergonomics and e) workplace practice.
• Glo ‐Germ environmental audits conducted in 15 clinical areas revealed significant deficiencies in
cleaning technique and frequency. Cleaning protocols were geared more towards office/hotel
requirements than the level of cleaning needed for an active healthcare treatment centre.
• Little is known regarding healthcare worker knowledge and practice related to infection control
and occupational health in this setting .A survey of ambulatory care staff revealed inadequate
ct, workers tended to overestimate their knowledge knowledge in these areas; in fa
• The survey also revealed that application of knowledge in practice was problematic; there was
an association between knowledge deficits and poor practice. There were significant differences
in knowledge and practice between clinical and administrative staff.
• Education sessions focusing on infection prevention and control basics are well received by both
staff and the community. Frequent and targeted educational initiatives to promote healthier
ambulatory care environments are essential in this increasingly complex care environment.
3 | P a g e

Executive Summary
Little has been documented regarding changing risks, worker safety, knowledge, and
models to deliver effective Infection Prevention and Control and Occupational Health
programs in outpatient settings. And yet ambulatory care is becoming increasingly more
complex both from a patient management perspective and in regards to the demands
placed on staff.
This Innovation‐at‐work project focused on the development and implementation of a
collaborative occupational health and infection control program that recognized and met
the needs of the three partners (Vancouver Coastal Health, University of British Columbia
and private ventures (housekeeping, food services and physicians’ offices]) in the Gordon
and Leslie Diamond Ambulatory Care Centre. Many aspects of internationally
recommended occupational health programs were not included in this assessment.
Specifically, the full scope of primary, secondary, and tertiary prevention activities of
occupational health programs needed to address the physical, chemical, biological,
ergonomic, psychosocial and safety hazards in the workplace, were not fully addressed in
this assessment, nor was the role of joint labour‐management health and safety
committees. Rather, the model developed was based on locally‐accepted roles for
occupational health practitioners focusing on preventing healthcare acquired infections in
patients and health workers. This more narrow scope was adopted in order to increase the
likelihood that the model developed could be readily applied to other partnership
healthcare settings with similar more narrow conceptions of the role of occupational health
programs.
4 | P a g e
5 | P a g e
The first task was to complete a pre‐established review that focused on identifying the gaps
in occupational health and infection control knowledge and practices as well as the
operational requirements for a functional program. This was followed by extensive
education session, the refinement of existing assessment/audit tools to suit an ambulatory
care environment and the integration of occupational health and infection control expertise
into the existing operational structure of the facility. Existing cleaning protocols were
reviewed and recommendations were made to better reflect the needs of the healthcare
environment. All of the findings and recommendations were circulated to the Centre
partners and staff (where appropriate). Policies and procedures were revised or
developed to address the identified needs as the final phase of the project.
The workplace assessment findings (Phase 1) highlighted several themes; a) lack of
signage, manuals and directives (e.g. hand hygiene and personal protective equipment
[PPE] posters); b) physical plant issues (e.g. lack of waste disposal systems such as bedpan
decontaminators in areas with an identified need); c) equipment design, placement and/or
procedural deficiencies (e.g. availability and location of first aid kits); d) ergonomics (e.g.
poor shelving and file storage); and e) workplace practice (e.g. routine cleaning of patient
equipment and chemical storage). One of the key lessons learned was the desirability of
carefully anticipating future needs during the design phase ‐ particularly with regard to
the documented increasing level of acuity in ambulatory patients.
The survey of ambulatory care staff revealed inadequate knowledge with regard to
infection control and occupational health practices; in fact workers seemed not to possess
the knowledge that they believed they had Application of knowledge in practice was
problematic, and there was an association between knowledge deficits and poor practice.
There were significant differences between clinical and administrative staff in knowledge

6 | P a g e
and practice, likely reflecting the lack of educational sessions for administrative personnel
who often direct policy that impacts worker safety and infection prevention. Targeted and
sustained educational initiatives to promote healthier ambulatory care environments are
essential to ensuring a healthy and safe workplace. These need to be tailored to meet the
needs of ambulatory care, carefully documented when they occur and results reported to
the centre’s operational team.
Glo‐Germ Environmental audits highlighted significant gaps in cleaning processes in
addition to a disconnect between what contracted cleaners felt they were responsible for
cleaning and what nursing staff felt was their responsibility. The review of the cleaning
protocol revealed that the type and level of cleaning was what one would expect in an office
rather than a healthcare facility. This required considerable changes in practice and more
clearly defined roles as to cleaning responsibilities in the building.
Rec mom endations and Lessons Learned:
1. Needs assessments using tools such as a workplace assessment checklist, Glo‐Germ
environmental audits and worker knowledge, attitudes and practice questionnaires
inform the development and implementation of new programs, services and
educational initiatives.
2. Staff must have access to regular, documented in‐services targeted at both clinical
and non‐clinical staff.
3. To be successful, occupational health and infection control should become part of
the administrative structure and be represented on relevant committees. This
process should engage all the partners in the Centre.
4. Cleaning contracts should be reviewed (ideally before the tender process is
complete) to ensure that the cleaning requirements reflect the acuity of the

7 | P a g e
population and are not biased towards office style cleaning. Responsibilities for
cleaning equipment and examining room items should be clearly designated to
nursing and housekeeping staff to ensure all items are regularly cleaned. Audits of
cleaning serve as both an educational tool for staff and a quality control measure.
5. Infrastructure, operational and physical plant design should plan for an increasingly
complex care as ambulatory care services continue to increase in acuity and volume.
6. Deliberately building in redundancies in the design of the physical plant would
address changes due to re‐allocation of space and the development of new
technologies.
7. Algorithms to identify and manage patients at high risk for transmission of
communicable diseases would be helpful in preventing clusters of healthcare
associated infections. These algorithms should be tailored to suit the needs of
ambulatory care and not simply extrapolated from acute care policies and
procedures.
8. Infection Control and Occupational Health resources that are required should
consider the range of services i.e. consultation, education, training, workplace
assessments and policy/procedure development.

The Research Problem and Context There is increasing focus on the importance of maintaining the health of healthcare
workers (HCWs)1‐4 but given the varied environments in which healthcare is now
administered5‐7, the challenges to reach all workers are greater than ever before8. In the
United States, from 1975 to 1995, the number of hospitals decreased from 7,126 to 6,291,
hospital beds declined from 1.47 million to 1.08 million, patient admissions decreased by
5%, the average length of patient stay was reduced by 33%, and inpatient surgical
procedures decreased by 27%8. In Canada, admissions declined in 1993, stabilizing at 3.1
million per year between 1998 and 20039. The number of patient visits to ambulatory units
in acute care hospitals, including day surgery visits, exceeded 50 million in 2002‐2003 in
Canada9.
While a considerable amount of hospital care and financial resources have shifted from
inpatient settings to ambulatory clinics, Infection Prevention and Control (IPC) and
Occupational Health (OH) delivery has not kept pace with the changing health delivery
model. Information on patient safety in this new dynamic is just being published10‐13,
however, little has been documented regarding changing risks, worker safety, knowledge,
and models to deliver effective IPC and OH programs in outpatient settings. Assessing
HCW knowledge of correct IPC and OH practices is a key first step in determining worker
needs and in designing programs and their delivery.
Healthcare is becoming a more integrated service with partnerships involving the public
and private sectors emerging. This is nicely illustrated in the Gordon and Leslie Diamond
Centre, a new ambulatory care centre in Vancouver that is a merger of hospital clinics,
8 | P a g e

private physician offices, food services and the University of British Columbia. While these
important partnerships have been formed, collaboration in key areas such as Infection
Control (IC) and Occupational Health (OH) were lagging behind. It is well known that a
IC/OH successful program improves health and safety within a workplace, decreases injury
and disease, reduces stress, and increases over‐all safety culture. At the onset of the
project, the Gordon and Leslie Diamond Centre did not have a single seamless formal
program in place for all healthcare workers and partners. Our proposal aimed to develop
and implement a comprehensive collaborative occupational health and infection control
program that recognized and met the needs of all partners in the Diamond Centre. This
model could then be applied to other partnership healthcare settings.
Setting: The Gordon and Leslie Diamond Health Care Centre (DHCC) is a new 11‐storey,
365,000 square foot, healthcare facility located on the Vancouver General Hospital campus,
in Vancouver, British Columbia (BC), Canada. It is a private‐public partnership formed by
Vancouver Coastal Health (VCH), the University of British Columbia (UBC) and a private
contractor managing the physical plant. Tenants include private physicians, VCH
ambulatory clinics and services, and UBC offices, classrooms, study areas, and a biomedical
library. The ambulatory care centre also includes food services, housekeeping services, and
other support services. Vancouver Coastal Health recognized the need for a comprehensive
IPC and OH program and funding from WorkSafeBC’s Innovation at Work fund provided
the opportunity to conduct a preliminary needs assessment to determine gaps prior to
9 | P a g e
establishing an OH and IPC program.
Beginning in January of 2007, an interdisciplinary team of infection control practitioners,
and occupational health professionals conducted a preliminary needs assessment for

10 | P a g e
occupational health and infection control within the Diamond Centre. This Phase 1 work
was very well‐received and there was strong interest in proceeding to the second phase of
work. Our team submitted an Innovations‐at‐work proposal for Phase 2, to complete the
needs assessment (obtaining missing information from worker groups that were not well‐
covered in Phase 1, such as the medical practitioners; complete workplace audits and key
informant interviews), circulate the results to all partners, and in collaboration with the
staff (both public and private), design, implement and evaluate a functioning program.
There were no well‐described models of how to implement an occupational health
program in a multi‐partnered healthcare environment, particularly where there are both
public and private sector partners. Secondly, although SARS, and more recently pandemic
planning, had illustrated the desirability of a well‐integrated occupational health and
infection control approach, there were no models in BC for providing occupational health
and infection to a large multi‐faceted setting such as this. This innovation‐at‐work proposal
ocused on these two significant issues. f

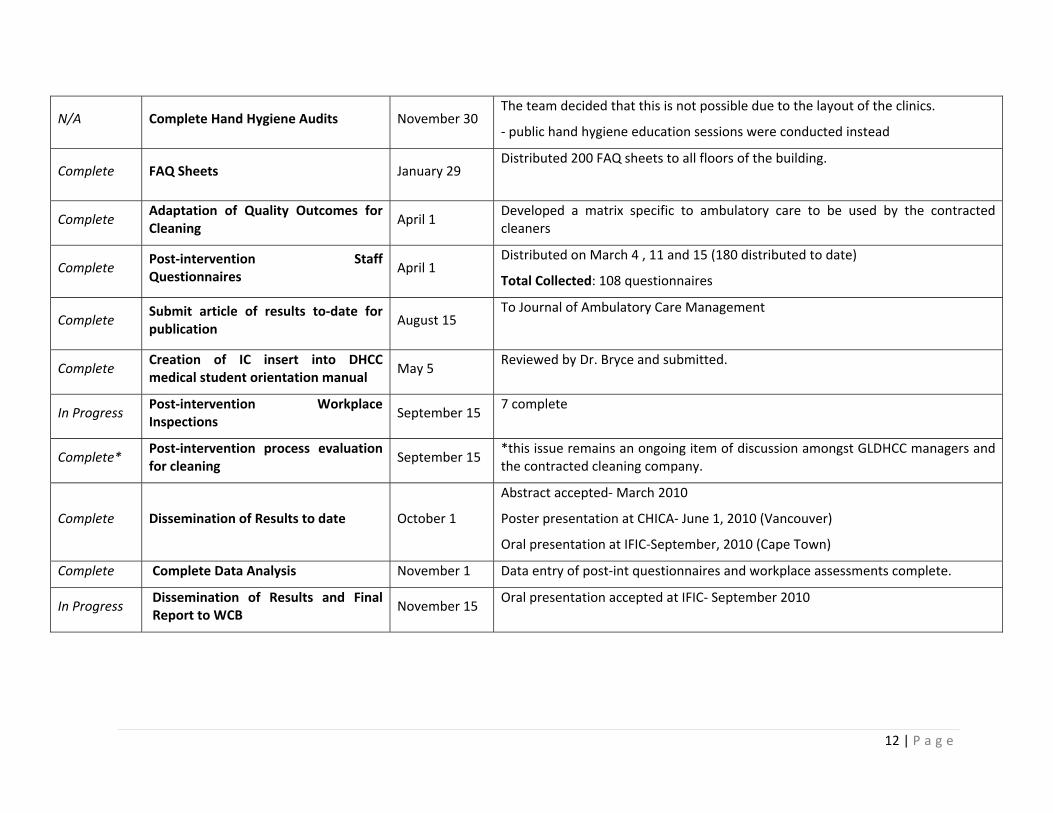
Project Timeline STATUS DELIVERABLE TARGET DATE NOTES
Complete
Establish an IC/OH Committee July 29
Joint occupation health and safety committee with infection control representation.
Remain present at monthly Building Managers' meetings and other administrative functions as: “GLDHCC IC & OH Subcommittee”
Complete Pre‐intervention Staff Questionnaires September 1
Total collected: 98 questionnaires
Data Analysis Complete: Summary tables compiled, to be integrated into article/report.
Room bookings confirmed (8/17)
BLJC notified (8/26)
HCW Education Session Complete (starting August 31)
Confirmed dates/times:
8/31 – 1pm, 2pm (DHCC 5213): Attendance= 6
9/6‐ 2:30pm (SOT unit): Attendance= 9
9/8 – 9am, 10am, 11am (DHCC 5213: Attendance= 11
9/15 – 1pm, 2pm, 3pm (DHCC 5213): Attendance= 6
9/23 – 9am, 10am, 11am (DHCC 5213): Attendance= 55
10/8 – 9am, 10am, 11am (DHCC 2264):Attendance= 31
10/15 – 1pm, 2pm, 3pm (DHCC 4223): Attendance=28
Complete Public Hand Hygiene Session in Lobby September 3 & October 6
Sept 3 Staff Attendance: 76 ++ (only staff signed in, but many others from public participated)
Oct 6 Attendance: 38 staff and 62 visitors
Complete Progress Report to WCB Mid‐October Sent to Penny Lowe on October 9th
6 month no‐cost extension granted.
Complete Complete Workplace Inspections November 30 7 complete
Complete Complete Environmental Audits November 30 DONE: Perform Glo‐Germ standards (w/photos)
DONE: 15 clinical areas complete to date with 14 touch points in each
11 | P a g e
12 | P a g e
N/A Complete Hand Hygiene Audits November 30 The team decided that this is not possible due to the layout of the clinics.
‐ public hand hygiene education sessions were conducted instead
Complete FAQ Sheets January 29 Distributed 200 FAQ sheets to all floors of the building.
Complete Adaptation of Quality Outcomes for Cleaning
April 1 Developed a matrix specific to ambulatory care to be used by the contracted cleaners
Complete Post‐intervention Staff Questionnaires
April 1 Distributed on March 4 , 11 and 15 (180 distributed to date)
Total Collected: 108 questionnaires
Complete Submit article of results to‐date for publication
August 15 To Journal of Ambulatory Care Management
Complete Creation of IC insert into DHCC medical student orientation manual
May 5 Reviewed by Dr. Bryce and submitted.
In Progress Post‐intervention Workplace Inspections
September 15 7 complete
Complete* Post‐intervention process evaluation for cleaning
September 15 *this issue remains an ongoing item of discussion amongst GLDHCC managers and the contracted cleaning company.
Complete Dissemination of Results to date October 1
Abstract accepted‐ March 2010
Poster presentation at CHICA‐ June 1, 2010 (Vancouver)
Oral presentation at IFIC‐September, 2010 (Cape Town)
Complete Complete Data Analysis November 1 Data entry of post‐int questionnaires and workplace assessments complete.
In Progress Dissemination of Results and Final Report to WCB
November 15 Oral presentation accepted at IFIC‐ September 2010

Methodology and Research/Project Findings
The research team employed complementary qualitative and quantitative methods to
evaluate the determinants of a comprehensive OH and IPC program in the ambulatory care
facility and to categorize the gaps between needs and the current level of service. (See
Logical Framework Analysis in Appendix I) In addition to a literature review,
environmental audits using Glo‐Germ were conducted; workplace assessments were
performed, and questionnaires were administered to individuals employed in the building
to ascertain HCW knowledge and practice. A quasi‐experimental design was used to assess
the effectiveness of the education and training initiatives by re‐administering the
uestionnaire. q
Part 1 Workplace Assessments
METHODOLOGY
The workplace assessment tool was adapted from a tool previously used by team members
in South Africa, Ecuador and Canada. (See Appendix II) A team consisting of a senior
infection control practitioner, a research coordinator and the unit manager conducted the
workplace assessments, covering five domains: physical environment, specific occupational
health practices and hazards, specific infection control practices, equipment and
procedures, and ergonomics. Potential risks were reported as satisfactory (S), as a hazard
requiring correction but not needing immediate correction (C), or as a hazard requiring
immediate correction (IC). Not applicable (N/A) was also provided as an option. Figure 1
documents the areas inspected.
13 | P a g e

Figure 1: f GLDHCC Clinics where workplace audits we
funding)
List o re conducted
inspectClinics in BLUE were ed in 2008 (prior to WCBlinics in RED were inspected in 2009 linics highlighted in GREEN were inspected in 2010 CC
CLINIC Adult Metabolic Clinic Burns Clinic/Hand Injury Clinic/ Trauma Services Clinic/ Ortho‐T
inic rauma Clinic/
Plastic Surgery ClCardiac Ultrasound/ Stress Lab Cardiac Rehab/ Pacemaker Clinic Complex Joint Clinic Complex Pain Services Dentistry Clinic Dermatology‐ Wound Healing x2 Diabetes Clinic/ Nutrition Counselling Epilepsy Clinic ENT Clinic Gastroenterology (UBC?) Geriatric Rapid Access Clinic HIV/AIDS Clinic/ Infectious Diseases
dicine Clinic Clinic/ Minor Surgery/ Home IV Clinic/
Tropical MeInternal Medicine Rapid Access Clinic Neuro‐otology Podiatry Clinic Radiology and Ultrasound Respiratory Clinic Solid Organ Transplant Clinic/ Kidney Diseases Clinic Stroke Prevention Clinic Urology/Prostate Clinic Women’s Clinic Lab Services
14 | P a g e

RESULTS
A total of 14 workplace assessments were conducted. Seven were conducted prior to
education and training sessions (Adult Metabolic Clinic, Complex Joint Clinic, Dermatology‐
Wound Healing, Diabetes Clinic/ Nutrition Counselling, Geriatric Rapid Access Clinic,
HIV/AIDS Clinic/ Infectious Diseases Clinic/ Minor Surgery/ Home IV Clinic/ Tropical
Medicine Clinic, Podiatry Clinic) and seven after these interventions (Cardiac Ultrasound/
Stress Lab Cardiac Rehab/ Pacemaker Clinic, Complex Pain Services, Epilepsy Clinic, ENT
Clinic, Internal Medicine Rapid Access Clinic, Stroke Prevention Clinic, Urology/Prostate
Clinic). A total of 73 Concerns and 22 Immediate Concerns were identified in the first round
of workplace assessments compared to 56 Concerns and 13 Immediate Concerns identified
in the second round. An average of 13 employees work each day per clinical area with a
range of patient visits from 4 (adult metabolic diseases) to 65 (ortho trauma/complex
joint). The acuity of illness in the patients who attended, varied significantly between
clinics as did the degree of assistance that patients required with ambulation, wound and
respiratory care and the time spent on each visit. Although different clinical areas were
assessed in the first and second rounds, the general themes of concerns and immediate
concerns were similar; a) Lack of signage, manuals and directives; b) physical plant issues
c) equipment and procedures; d) ergonomics an
15 | P a g e
d e) workplace practice.
a) Lack of signage, manuals and directives. Several nurse managers expressed desire
for more multi‐lingual hand hygiene and signage depicting instructions for use of
personal protective equipment. Signage was also lacking for blood and body fluid
exposure management, OH and safety reporting procedures as well as WorkSafeBC
reporting procedures. The greatest total number of ‘Concerns’ and ‘Immediate

Concerns’ reported were in regards to the accessibility of occupational health
minutes and information.
b) Physical plant issues. Most of the concerns and immediate concerns identified in this
section were the result of a change in the original intent of the physical space. For
example, a large room was divided into three smaller treatment rooms with the
addition of floor‐to‐ceiling room dividers. This then resulted in inadequate lighting
and ventilation in two of the treatment rooms. Similar constraints were noted with
sink numbers and placement in a few clinical areas originally intended for
administrative purposes. Several concerns regarding the location of electrical
outlets were also identified. One clinic in particular expressed frustration with
having to run long extension cords across examination rooms in order to plug in
equipment; this posed a safety hazard for staff and patients. Storage for supplies
was limited in some clinics resulting in clutter that made thorough cleaning of
surfaces difficult. Bedpan decontaminators for human waste disposal were required
in some of the clinics; this had not been considered in the original design of the
building. Patients may attend clinics daily and for long periods of time (e.g. bone
marrow and solid transplant, renal clinics); waiting areas for patients and their
families was limited in som
16 | P a g e
e clinics.
c) Equipment and procedures: Better positioning and number of safe sharps disposal
units were required in some clinical areas. Many clinical areas also reported being
unsure of where to find a first aid kit. Few units had their own first aid kit or knew
where to locate one even though most managers thought that there was a first aid
kit available to them somewhere on the floor. Increasingly complex technology

results in more equipment and increasing acuity of care requires more care
supplies; unfortunately there was limited storage space in the building to
accommodate current let alone future needs.
d) Ergonomics: Many staff identified shelving as a concern or an immediate concern.
Some clinical areas assessed had large filing cabinets places on the ground making it
uncomfortable for staff to file patient records. Conversely, some clinics identified
shelves that were to o high to reach without standing on a chair or stool as a concern.
e) Workplace practices: Inconsistent practices in cleaning of patient care equipment
such as examination tables. (e.g. some examining tables had soiled sheets) was
noted both by housekeeping and clinical staff (see Glo‐Germ environmental audits
for further details). Chemicals were not always stored appropriately and expiry
dates were not carefully monitored in several clinical areas. However, several
clinical areas exhibited model practices in this regard. For example, the
podiatry/wound healing, infectious disease and HIV clinics had meticulously labeled
containers with close attention paid to expiry dates. On a positive note, many of the
staff in clinical areas assessed had completed the online infection control module
and infection control procedures were prominently displayed on a bulletin board.
17 | P a g e
Lessons Learned: While it is impossible to identify all the needs of an ambulatory care
centre prior to construction, careful consideration must be given to anticipated future
needs particularly with regard to the documented increasing level of acuity in ambulatory
patients. The need for waste disposal systems, electrical outlets to meet increasing
technological demands, storage space for care supplies, patient and family space for those

18 | P a g e
who attend clinics on multiple days for long periods of time (e.g. bone marrow transplant
clinics), ventilation requirements for higher risk clinics (e.g. respiratory outpatient
services) should be considered and additional capacity or redundancies built into the
physical plant. The process of conducting workplace assessments at the GLDHCC also
informed the creation of a comprehensive “Field Guide for Workplace Assessments in
Healthcare” currently being piloted in South African hospitals.
Part 2 Environmental Audits Using GloGerm
METHODOLOGY
Environmental marking measured the thoroughness of cleaning using a surrogate marking
system. A colourless UV solution was applied to high‐touch objects and surfaces in the
client/patient/resident environment prior to cleaning, followed by detection of residual
marker with the use of a UV light source immediately after cleaning, .14‐17 The
environmental audits were conducted in 15 clinical areas using a template developed at
Vancouver Coastal Health (see Appendix III). At the end of the clinic day, surfaces were
marked with Glo‐Germ before cleaning occurred. The surfaces and objects were re‐
examined the following morning (using the UV light source) and results recorded prior to
the first patient. This methodology was quantified:
a) by calculating the percentage of marked objects/surfaces that were cleaned in a
particular room or area; and/or
b) by deriving a cleaning score (e.g., 3 = heavy fluorescence, 2 = moderate fluorescence, 1 =
light fluorescence, 0 = no fluorescence). For the purposes of this study, a 3 or 2 was coded
as a “FAIL” and a 1 or 0 was coded as a “PASS.” Results are shown in Figure 2 below.

RESULTS Figure 2: GloGerm Environmental Audit: SUMMARY OF RESULTS Data Collected: August 2009‐November 2009 Collected By: Cole Hilliard and Lyndsay O’Hara Total Observations: 15 clinical areas, 14 items each
Location Pass Fail
1 Door Handle 7 8
2 Light Switch 12 3
3 Sink 11 4
4 Taps 9 6
5 Soap Dispenser 8 7
6 Paper Towel Dispenser 4 11
7 Chairs 9 6
8 Bedside Table 13 2
9 Bed Rails 10 5
10 Bed Mattress 13 2
11 Sharps Container 2 13
12 Handle Overhead Lamp 4 11
13 Stool 10 5
14 Toilet Seat 11 4
TOTAL 123 (58.6%) 87 (41.4%)
19 | P a g e

GloGerm Environmental Results Pass/Fail Results by Item
Clinical areas audited include: Burns Clinic, Ortho Trauma Clinic (x2), Infectious Disease
Clinic, Geriatric Rapid Access Clinic, Internal Med Rapid Access Clinic, Diabetes Clinic (x2), Epilepsy Clinic, Dermatology/Wound Healing Clinic, Adult Metabolic Clinic, Complex Joint Clinic, Pacemaker Clinic, Stroke Prevention Clinic, Podiatry Clinic
20 | P a g e
Lessons Learned: These findings, in addition to an informal qualitative survey of nursing
staff, highlighted significant gaps in cleaning processes in addition to a disconnect between
what contracted cleaners felt they were responsible for cleaning and what nursing staff felt
was their responsibility. The review of the cleaning protocol revealed that the type and
level of cleaning was what one would expect in an office rather than a healthcare facility. In

response to this disconnect, the project coordinator and a senior infection control
practitioner worked with the contracted cleaning company and the building management
to collaboratively revise the cleaning processes (including frequency) at the Gordon and
Leslie Diamond Health Care Centre. The research team hopes this will inform the RFP
rocess when cleaning contract comes is to be renewed. p
Part 3 Knowledge, Attitudes and Practices Survey
METHODOLOGY
A previously validated questionnaire 18 19 consisting of 103 items (see Appendix IV) was
administered by two research team members to facility staff. A total of 150 pre‐
intervention questionnaires and 180 post‐intervention questionnaires were distributed
throughout the facility utilizing convenience sampling methods, targeting VCH, UBC and
private physician office staff equally. Respondents were offered a $5 coffee card upon
completion of the questionnaire that was submitted anonymously. The questionnaire
consisted of five sections related to OH and IPC issues: 1) baseline demographics; 2) self‐
perception of knowledge; 3) knowledge assessment; 4) practices, and 5) perception of
risks. Respondents were asked to rate their knowledge on a 5‐point Likert scale. The
questionnaires were coded to ensure confidentiality and took approximately 20 minutes to
complete. After statistical analyses were complete, findings were distributed to all clinics
in the form of an “FAQ S
21 | P a g e
heet” (see Appendix V).
Statistical Analysis: Standard descriptive statistics (e.g., frequency and percent) were
calculated to analyze demographic data and characterize the distribution of variables.
Fisher’s exact test was used in analysis of questions regarding knowledge, practice, risk

perception and training to compare results between occupational groups. All tests were
two‐sided significance levels of p≤0.05 estimated from S‐Plus 8.0 statistical analysis
software. Partially missing values were automatically excluded from the analyses.
RESULTS
A total of 98/150 (65%) questionnaires were returned (Table 1) with physicians and
surgeons comprising 3.1%, nurses accounting for 17.3% administrative staff comprising
36.7%; 9.2% were technicians and 33.7% of respondents identified themselves as
pharmacists, dieticians, psychologists, researchers, and other allied health professions. It
should be noted that housekeeping staff are not included in this survey as they are
contracted employees. However, this subgroup could also be at considerable risk of
hysical and biological hazards. exposure to chemical, p
a) Access to expertise:
Many respondents did not know how to contact OH or IPC services (OH =63 % “yes”’ IPC =
60% “yes”‐ See Table 2) and were even less confident in their ability to contact their OHS
representative (41%). Seventy percent of respondents felt confident in how to contact the
fire/safety steward. Only 44% of staff reported OHS training in the last two years and only
half of health workers surveyed (49%) recalled being screened for TB upon hiring,
however, 94% of nurses reported being screened for TB. No physician had received OH
training upon hiring.
22 | P a g e
b) Self perception of knowledge:
Thirty‐five percent of workers rated their overall OH and IPC knowledge as a 3 (“More or
less”) and of particular concern, 35% of respondents reported having very little knowledge

of IPC practices (Table 3). Only 29% felt confident in their knowledge and rated their IPC
and OH knowledge as a 4 or 5 (“Quite a bit/Very high”). Nurses did (94%) feel they had a
good grasp of basic infection control concepts compared to only 14% of staff with
administrative duties who rated their knowledge of OH and IPC policies as a 4 or 5 (“Quite
a bit/Very high”). Fifty percent in the ‘Other’ category rated their infection control
1 or 2 (“Not at all/A bit”). knowledge as a
23 | P a g e
c) Knowledge
The knowledge section of the questionnaire highlighted deficiencies in awareness of
correct IPC practices (Table 4 and 5). As shown in Table 4, seventy‐six percent of
respondents reported that they know when to use PPE and 71% know how to put on and
take off PPE. Of note, 21% did not know when to use gloves and 35% and 37% did not
know when or how respectively to use a N95 respirator. There was a significant difference
in the number of correct responses between clinical staff and non‐clinical staff as to when
to use an N95 respirator (p<0.0001) and when to use a surgical mask (p=0.0016). Only
32% of the respondents replied correctly to the question on the importance of
environmental cleaning, highlighting the lack of understanding the hand hygiene, and not
cleaning was the most important practice in infection prevention. (Table 5). More direct
patient care staff (69%) answered this question correctly than did administrative staff
(11%: p<0.0001). A large proportion of respondents (47%) thought that needles should be
recapped before disposal in a sharps container and similarly. This question was also
answered correctly by more direct patient care staff (81%) than administrative staff (37%:
p<0.0001). More than 20% of respondents thought that they should change their work
practice if a patient is known to have HIV or Hepatitis. Thirty‐three percent believed that

glove use is always recommended, rather than only when there is anticipated risk of blood
and body fluid exposure. On a positive note, 91% of respondents knew that all needle‐stick
and sharp injuries must be evaluated by occupational health and an impressive 99% were
sure that patients who are verbally abusive are not permitted to do so as part of their right
to care. Knowledge regarding proper waste disposal was quite high with 89% of
respondents responding correctly when asked if general waste and medical waste can be
mixed in the same container if there are no sharps. It should also be noted that 90% knew
inen must be placed in leak‐proof bags. that blood and body fluid soaked l
24 | P a g e
d) Knowledge applied to practice
The knowledge in practice section of the questionnaire (Table 6) identified several issues
of concern; some of these were consistent with reported knowledge gaps in the previous
section and other practices were incongruent with the reported knowledge. For example,
49% of respondents would deliberately change their IPC approach if a patient was known
to have HIV, Hepatitis B or C, a clear misunderstanding of the concept of Standard
Precautions. Thirty‐two percent of respondents reported recapping needles in practice
(Clinical staff: 75%, Non‐clinical staff: 50%: p=0.0004). Low scores (51% and 48%) were
identified in practices related to health and safety policies and procedures such as
reporting of health and safety problems and concerns. Interestingly, 98% of respondents
reported that they would change their gloves between patients, but only 70% always
cleaned their hands between patients. Practices pertaining to workplace violence also
received low scores. Only 30% of respondents always assessed patient’s potential for
aggressive behavior upon admission and 37% always made suggestions for controlling
workplace violence. There were several differences in the number of correct responses

between clinical and administrative groups that were significant regarding physical
environment, specific occupational health practices and hazards, specific infection control
ractices, and ergonomics (Table 6). p
Lessons Learned: The workers questionnaire results suggest that in general, respondents
did not apply in practice what they know, and may not possess the knowledge that they
thought they knew. For example, self‐reported knowledge scores regarding when and how
to use goggles were quite high (76% and 77% respectively), yet in practice, only 40%
always use eye protection (other than prescription glasses) during procedures with
potential for splashes and aerosols. Conversely, it was also evident that a lack of
knowledge translates into practice. For example, knowledge and corresponding practice
scores related to glove use were both quite high, while both knowledge and practice scores
related to recapping needles were low and of particular concern. Only 37% would make a
25 | P a g e
suggestion to control workplace violence.
The questionnaire results reveal significant differences in the level of knowledge and
correct practice between clinical staff and technical and administrative staff. All results
regarding when and how to use PPE varied between the different professions and
occupations. Most of the findings reflect the fact that administrative staff do not don and
doff PPE on a regular basis and would therefore not be expected to know the correct
manner of doing so. Differences between occupational groups in the knowledge evaluation
questions as shown in Table 5 were not significant with the exception of knowledge
regarding frequent cleaning of the environment, footrests, and recapping needles. In
contrast, the percentage of correct responses in the section of the questionnaire focusing

26 | P a g e
on knowledge applied to practice (table 6), the majority of items showed significant
differences between occupations. It should also be noted that there were high numbers of
“Not applicable” responses recorded by administrative staff. Although administrative staff
is not traditionally expected to possess high levels of clinical knowledge, it is essential that
they possess basic occupational health and infection control knowledge to understand staff
needs. This is especially relevant in the ambulatory care setting where clerks and
receptionists often perform clinical duties such as intake, room cleaning and waste
disposal.
It was also abundantly clear that healthcare workers did not know how to access IPC and
OH expertise available to them. The questionnaire finding that 63% or respondents knew
how to contact OH, 60% knew how to contact IPC services and only 41% were aware of
how to contact their OHS representative, clearly illustrates a need to communicate roles
and responsibilities to ensure that all workers understand to whom they should report
injuries, hazards and risks in their workplace. Similar findings have been reported in
traditional healthcare settings (i.e. acute hospital) in the past, but much has been done in
recent years to prioritize and protect the health of healthcare workers in acute care18‐20. It
is essential to determine how to effectively break down these barriers and create an
environment in ambulatory care settings that is more conducive to communication and
support.

Table 1 – Descriptive statistics of worker questionnaire respondents
Occupation Group
Physician Nurse Admin Technician Other TOTAL
N (%) 3 (3.1%) 17 (17.3%) 36 (36.7%) 9 (9.2%) 33 (33.7%) 98 (100%)
Median Age Range (Years) 40-49 40-49 40-49 30-39 30-39 40-49
Male 66.6% 0.0% 5.9% 22.2% 3.2% 19.6%Female 33.3% 100.0% 94.1% 77.8% 96.8% 80.4%
Mean Years In Office (SD) 16.7 (11.5) 5.5 (5.8) 5.2 (5.2) 5.4 (6.0) 2.7 (2.3) 4.8 (5.5)
Mean Years In Building (SD) 3.0 (0) 2.2 (0.9) 4.9 (7.9) 2.2 (1.0) 1.9 (1.0) 2.6 (3.5)
Unionized 0.0% 83.3% 94.1% 66.7% 18.2% 59.2%
UBC - 16.7% - 33.3% 3.0% 10.2%
VCH 33.3% 66.7% 94.7% 55.6% 18.2% 53.1%
Private Physician or Group 33.3% 5.5% 5.3% 11.1% 72.7% 29.6%
Private Other 33.3% 11.1% - - 6.1% 7.1%
Private Ambulatory Unit 33.3% 5.7% 5.9% 11.1% 21.2% 12.4%
UBC Ambulatory Unit 66.6% 2.9% - - - 10.3%
VCH Ambulatory Unit - 54.3% 82.4% 33.3% 21.2% 46.4%
Medical Laboratory - - 5.9% - 3.0% 2.1%
Administration - 25.7% - - 27.3% 18.6%
Other - 11.4% 5.9% 55.6% 27.2% 19.6%
Physicians= including SurgeonsAdministrator= Clerks, Receptionists, Managers and AdministratorsTechnician= Technologist, Technicians, TherapistsOther= Pharmacist, Dietician, Psychologist, Researcher, Social Worker, AudiologyUnions include: AAPS, BCNU, CUPE2950, HEU, HSA
Dem
ogra
phic
sEm
ploy
erW
orki
ng A
rea
27 | P a g e

Table 2 – Proportion of respondents who know how to contact health professionals, who have had TB screening upon hiring, who have had BBF exposure in the last 2 years, and who have prior OH education.
Occupation Group
Yes No Yes No Yes No Yes No Yes No Yes No
OH Dept. 100.0% 0.0% 100.0% 0.0% 53.3% 46.7% 75.0% 25.0% 44.8% 55.2% 62.8% 37.2%
OH & Safety Represent 66.7% 33.3% 80.0% 20.0% 32.2% 67.8% 55.6% 44.4% 25.0% 75.0% 41.1% 58.9%
Infection Control 100.0% 0.0% 100.0% 0.0% 45.2% 54.8% 75.0% 25.0% 45.2% 54.8% 60.0% 40.0%
Safety/Fire Dept. 66.7% 33.3% 87.5% 12.5% 62.3% 37.1% 75.0% 25.0% 69.0% 31.0% 70.3% 29.7%
33.3% 66.7% 94.0% 6.0% 46.9% 53.1% 55.6% 44.4% 23.3% 76.7% 48.9% 51.1%
0.0% 100.0% 5.9% 94.1% 5.7% 94.3% 0.0% 100.0% 3.2% 96.8% 4.2% 95.8%
0.0% 100.0% 54.5% 45.5% 30.4% 69.6% 50.0% 50.0% 10.7% 89.3% 26.8% 73.2%
66.7% 33.3% 62.5% 37.5% 35.3% 64.7% 62.5% 37.5% 36.7% 63.3% 44.4% 55.6%
TOTALPhysician Nurse Administrator Technician Other
Sharp Injury or BBF In Last 2 Yrs
Screened For TB Upon Hiring
OH Evaluation Upon Hiring
OH Training In Last 2 YrsTB
scr
eeni
ng, B
BF e
xpos
ure,
OH
ed
ucat
ion
Know
how
to c
onta
ct th
e fo
llow
ing:
Physician= including Surgeons Administrator= Clerks, Receptionists, Managers and Administrators Technician= Technologist, Technicians, Therapists Other= Pharmacist, Dietician, Psychologist, Researcher, Social Worker, Audiology
28 | P a g e

29 | P a g e
Table 3 – Proportion of respondents self‐reporting of Infection Control (IC) knowledge and Occupational Health (OH) knowledge
Physician Nurse Administrator Technician Other TOTAL
Infe
ctio
n C
ontro
lK
now
ledg
e
Not at all / A bit 0.0% 0.0% 45.7% 22.2% 50.1% 35.4% More or
less 33.3% 5.9% 40.0% 44.4% 43.8% 35.4% Quite a bit
/ Very high 66.7% 94.1% 14.3% 33.4% 6.1% 29.2%
Rep
ortin
g K
now
ledg
e Yes 66.7% 94.1% 51.4% 66.7% 56.2% 62.5% No 33.3% 5.9% 31.4% 11.1% 21.9% 15.6% Not Sure 0.0% 0.0% 17.2% 22.2% 21.9% 21.9%
Physician= including Surgeons Administrator= Clerks, Receptionists, Managers and Administrators Technician= Technologist, Technicians,
Therapists Other= Pharmacist, Dietician, Psychologist, Researcher, Social Worker, Audiology
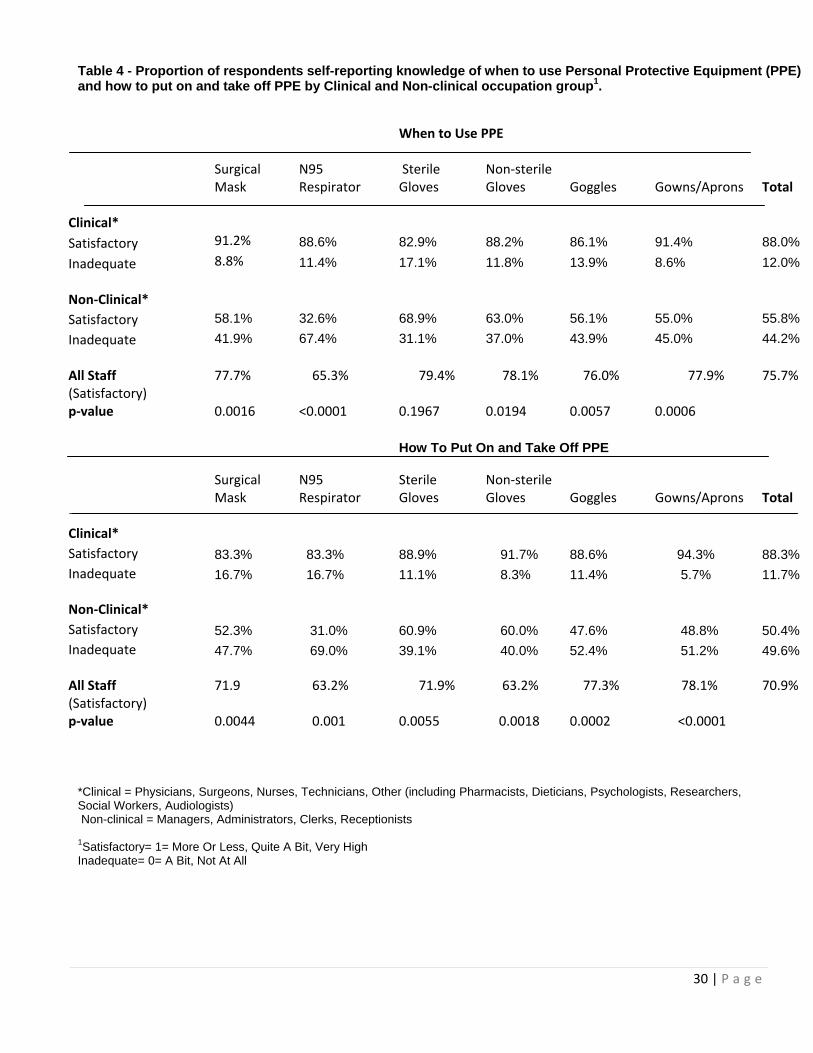
Table 4 - Proportion of respondents self-reporting knowledge of when to use Personal Protective Equipment (PPE) and how to put on and take off PPE by Clinical and Non-clinical occupation group1.
When to Use PPE
Surgical Mask
N95 Respirator
Sterile Gloves
Non‐sterile Gloves Goggles Gowns/Aprons Total
Clinical* Satisfactory 91.2% 88.6% 82.9% 88.2% 86.1% 91.4% 88.0%Inadequate 8.8% 11.4% 17.1% 11.8% 13.9% 8.6% 12.0% Non‐Clinical*
Satisfactory 58.1% 32.6% 68.9% 63.0% 56.1% 55.0% 55.8%Inadequate 41.9% 67.4% 31.1% 37.0% 43.9% 45.0% 44.2% All Staff 77.7% 65.3% 79.4% 78.1% 76.0% 77.9%
75.7%
(Satisfactory) p‐value 0.0016 <0.0001 0.1967 0.0194 0.0057 0.0006
How To Put On and Take Off PPE
Surgical Mask
N95 Respirator
Sterile Gloves
Non‐sterile Gloves Goggles Gowns/Aprons Total
Clinical* Satisfactory 83.3% 83.3% 88.9% 91.7% 88.6% 94.3% 88.3%Inadequate 16.7% 16.7% 11.1% 8.3% 11.4% 5.7% 11.7% Non‐Clinical* Satisfactory 52.3% 31.0% 60.9% 60.0% 47.6% 48.8% 50.4%Inadequate 47.7% 69.0% 39.1% 40.0% 52.4% 51.2% 49.6% All Staff 71.9 63.2% 71.9% 63.2% 77.3% 78.1%
70.9%
(Satisfactory) p‐value 0.0044 0.001 0.0055 0.0018 0.0002 <0.0001
*Clinical = Physicians, Surgeons, Nurses, Technicians, Other (including Pharmacists, Dieticians, Psychologists, Researchers, Social Workers, Audiologists) Non-clinical = Managers, Administrators, Clerks, Receptionists 1Satisfactory= 1= More Or Less, Quite A Bit, Very High Inadequate= 0= A Bit, Not At All
30 | P a g e

Table 5 - Proportion correctly answering Knowledge Evaluation questions by occupation group.1
Clinical* Non-clinical*
All Staff
p-value
PHYSICAL ENVIRONMENT
Frequent cleaning of the environment is not the most important practice to prevent infections 69% 11%
32%
<0.0001
Local exhaust ventilation such as hoods is needed to protect people from breathing in harmful vapours 74% 87%
82%
0.158
SPECIFIC OCCUPATIONAL HEALTH PRACTICES AND HAZARDS All needle-stick and sharp injuries must be evaluated by an occupational health responsible/service 94% 88%
91%
0.4762
First aid kits should be centrally located in one area of the floor/building 74% 78% 77% 0.8014 Patients who are verbally abusive are not permitted to do so as part of their right to care 100% 98%
99%
1
I am capable of recognizing potentially aggressive patients 78% 71% 73% 0.6356 I know how to assess patients potential aggressive behaviour 69% 48% 56% 0.0562 SPECIFIC INFECTION CONTROL PRACTICES Needles should not be recapped before disposing in a sharps container 81% 37% 53% <0.0001 The use of gloves is always recommended, not only when the risk of blood and body fluid exposure is present 69% 60%
63%
0.0799
Patients with suspected TB cannot sit in the waiting room with other patients 78% 87% 83%
1
Having food or drinks in the clean storage places or in the medication room/work station is not permitted 94% 88%
91%
0.4752
If a patient is known to have HIV or Hepatitis you should not change your work practice 89% 72%
78%
0.0729
ERGONOMICS Twisting can be as bad for your back as lifting 97% 89% 92% 0.2513 Foot rests under desks and at work stations are not primarily used to rest your legs 97% 63%
76%
<0.0001
EQUIPMENT AND PROCEDURES It's OK to have mobile X-ray equipment used in a clinic with a number of patients because they usually don't stay long in the clinic enough to have significant exposure 91% 88%
89%
0.7397
BBF soaked linen cannot be put in any plastic bag 94% 87% 90% 0.3166 General waste and medical waste can be mixed in the same container if there are no sharps 92% 87%
89%
0.7414
1 The correct statement has been provided for clarity. The Worker Questionnaire does not explicitly state the correct answer, as written above.
*Clinical= Physicians, Surgeons, Nurses, Technicians, and Other (including Pharmacists, Dieticians, Psychologists, Researchers, Social Workers and Audiologists) Non-Clinical= Office Managers, Administrators, Clerks, Receptionists
31 | P a g e

Table 6 - Proportion of respondents correctly practicing IC and OH & Safety Procedures' Evaluation tasks by occupation group. 1
Clinical* Non-clinical* All Staff
p-value
PHYSICAL ENVIRONMENT Always use local exhaust ventilation when working with harmful chemicals 100% 83% 91%
<0.0001
Always report witnessed spills 68% 65% 66% 0.7646 SPECIFIC OCCUPATIONAL HEALTH PRACTICES AND HAZARDS
Always use eye protection (other than prescription glasses) during procedures with potential for splashes 38% 44% 40%
0.4723
Always wear hearing protection in noisy areas 36% 36% 36% 1 Always report health and safety problems to the occupational health service 54% 47% 51%
0.3962
Always report health and safety problems to occupational health & safety committee/representative 48% 47% 48%
1
Always make suggestions for correcting health and safety problems to the occupational health service 31% 24% 27%
0.3421
Always make suggestions for correcting health and safety problems to the occupational health & safety representative 28% 29% 28%
1
Always assess patients potential for aggressive behaviour upon admission 43% 16% 30%
<0.0001
Always communicate to co-workers about potentially aggressive patients 75% 62% 68%
0.0673
Always report workplace violence incidents to managers 96% 67% 78% <0.0001 Always make suggestions for controlling workplace violence 52% 26% 37%
0.0003
SPECIFIC INFECTION CONTROL PRACTICES Always clean hands between the care of patients 79% 58% 70% 0.0022 Never change procedures if a patient is known to have HIV, Hepatitis B, and/or Hepatitis C 72% 23% 51%
<0.0001
Never recap needles 75% 50% 68% 0.0004 Always change gloves (if worn) between patients 97% 100% 98% 0.2462 Always wear N95 respirators when caring for patients with airborne diseases such as TB 85% 67% 81%
0.0046
Always utilize the online Infection Control Manual as an effective workplace tool 18% 16% 17%
0.8509
Always dispose of sharps in a sharps container 100% 94% 98% 0.0289 Never work in situations where patients suspected of having TB are seen at clinic/office 46% 39% 43%
0.3908
ERGONOMICS Always ask for help to reposition or to lift heavy objects or patients 62% 50% 56%
0.1169
Always use lifting devices that are provided 47% 83% 57% <0.0001
EQUIPMENT AND PROCEDURES Always use guards on machinery 71% 67% 70% 0.6467
1 The correct statement has been provided for clarity. The Worker Questionnaire does not explicitly state the correct answer, as written above. *Clinical= Physicians, Surgeons, Nurses, Technicians, and Other (including Pharmacists, Dieticians, Psychologists, Researchers, Social Workers and Audiologists) *Non-Clinical= Office Managers, Administrators, Clerks, Receptionists
32 | P a g e
Part 4 Healthcare worker and public education sessions
A total of 7 education sessions were held for all staff at the Gordon and Leslie Diamond
Health Care Centre with 146 staff members in total attending. The content of these
sessions included basic infection control and occupational health principles as well as a
specific focus on the prevention and control of influenza like illness in light of the H1N1
outbreak. Two full‐day interactive public hand hygiene demonstrations were also held in
the lobby of the facility. These sessions allowed the public to test their hand washing
technique using Glo‐Germ to mimic soap. Informational brochures and question/answer
periods were also included in the sessions. These events garnered interest from 176
attendees. All sessions received positive feedback from staff and members of the public
alike.
33 | P a g e
Implications for future research/projects on workplace health and safety
The ambulatory care setting offers distinct advantages to patients, by combining disciplines
in one central location and offering a variety of diagnostic tests on an outpatient basis.
Outpatients are now more likely to have unstable medical conditions that can pose an IPC
or OH risk to healthcare workers who traditionally have not received comprehensive
training in these fields compared to their acute care colleagues. Further coordinated efforts
are necessary to protect workers in ambulatory care facilities from the possibilities of
infections and occupational risks, while also considering the unique challenges and benefits
presented by this setting.
Ambulatory care medical procedures may put patients and staff at risk of infections. While
this risk is still considered low21 when compared to hospital‐based care, there is a risk to
workers, and sometimes patients, as more complex and invasive procedures are performed
in this setting. Surgical procedures that were once carried out in a hospital are now done in
an ambulatory care setting22, 23 resulting in greater exposure to blood and body fluids for
workers and patients alike. Our findings suggest that staff in ambulatory care settings have
not been reached by traditional training methods in occupational health and safety and
infection control based on the intellectual knowledge scores. The Joint Commission’s
Surveillance, Prevention and Control of Infection Standards for Ambulatory Care espouse
principles which are almost identical to the standards for a hospital setting24. This is
warranted as hospital settings and ambulatory care are moving in the direction of
providing the same care. Special attention must be paid to education and communication
due to the diverse worker population who may not possess the basics in IPC.
34 | P a g e

In addition, it is noted that the scope of occupational health services considered in this
study was much more narrow than the internationally‐recommended roles for
occupational health practitioners in primary, secondary, and tertiary prevention regarding
the full array of physical, chemical, biological, ergonomic and psychosocial hazards in
workplace settings, nor did this study explore the adequacy of joint labour‐employer health
and safety committee functions. Rather, this study adopted a much more narrow concept
of the role of occupational health services commonly accepted in this jurisdiction, in order
to develop recommendations that would be more readily implemented. Further research
is therefore still needed in this area.
Identification of immediate and longterm benefits of the findings or res ltu s
1. Ambulatory care visits continue to increase. The findings of this project have
informed the following recommendations to improve occupational health and
infection control in ambulatory care settings:
2. Needs assessment using tools such as a workplace assessment checklist, Glo‐Germ
environmental audits and worker knowledge, attitudes and practice questionnaires
inform the development and implementation of new programs, services and
35 | P a g e
educational initiatives.
3. Staff need to have access to regular, documented in‐services targeted at clinical and
non‐clinical staff. The results of the questionnaire suggest that gaps in knowledge
and practice exist in ambulatory care and that targeted training and educational
initiatives are necessary. These sessions can provide education and training on
occupational health and infection control basics, while also providing a venue for
the delivery of specific messages as in the case of pandemic H1N1.
4. An occupational health and infection control program should be part of the
administrative structure and represented on relevant committees. Strong
managerial support and engagement by all public and private organizations
represented in ambulatory care partnerships is required during all phases of
rprogram design and delivery to ensure both healthcare wo ker and patient safety.
5. Examine cleaning contracts to ensure that the cleaning requirements reflect the
acuity of the population and are not biased towards office style cleaning. Roles and
responsibilities of front‐line healthcare workers and cleaning staff need to be clearly
outlined to ensure that all items and equipment are cleaned regularly. Audits of
process (i.e. how cleaning occurs) and glo‐germ audits (or similar technology using
fluorescent markers that examine cleaning efficacy) serve as both an educational
tool (for both healthcare workers and housekeeping staff) and a quality
improvement measure.
6. Plans for ambulatory care services must consider the increasing volume and
complexity. This includes consideration of issues such as waste disposal facilities,
storage space for more acute care patient supplies, ambulation aides, improved
lighting, and adequate space for procedure rooms.
7. To that end, thoughtful consideration should be give to deliberately building in
redundancies to address physical plant changes due to re‐allocation of space and the
development of new technologies (e.g. extra electrical outlets, moveable partitions).
36 | P a g e

37 | P a g e
8. Algorithms to identify and manage patients at high risk for transmission of
communicable diseases would be beneficial. These algorithms should not simply be
extrapolated from acute care settings but developed to reflect the needs and patient
flow in an outpatient setting.
9. The Infection Control and Occupational Health resources required should consider
consultation, education/training, workplace assessments, investigations and
policy/procedure development. The resources required will of course depend on
the size of the facility and the population served. For the Gordon and Leslie
Diamond Health Care Centre, a new 11‐storey, 365,000 square foot healthcare
facility, we recommend a 0.5 FTE Infection Control Practitioner and a 0.25 FTE
Occupational Health Professional.

Identification of relevant user groups for the research/project results
The research team anticipates that the recommendations made above will be useful for
planning purposes for anyone who is involved in establishing an occupational health
and/or infection control program in an ambulatory care setting. The findings of this
project are particularly relevant to the following user groups in the ambulatory care
setting:
• trative personnel Executive/adminis
• Clinical Managers
• s Building/Administrative Manager
• Contracted Cleaning Company
• staff Front‐line clinical
• Non‐clinical staff
• ators Medical educ
• Researchers
• The general public
38 | P a g e
Dissemination/knowledge transfer The research team met once per month with the Diamond Centre User’s Committee to
share progress and results and to request feedback and input. Activities that promote a
two‐way dialogue, not a one‐way flow of information (such as face‐to‐face meetings or
briefings) are a very effective way to reach decision makers such as managers, senior
administrators and health authority executives.
As mentioned previously, findings were disseminated front‐line workers as “FAQ Sheets”
as well as during education sessions. The findings of this project informed the development
of a section focusing on Infection Prevention and Control to be included in the handbook
for new medical students (Appendix VI).
The research team also presented results at the Canadian and Hospital Infection Control
Association conference in Vancouver.
The findings from the worker knowledge, attitudes and practice questionnaires have been
accepted for publication in the peer‐reviewed Journal of Ambulatory Care Management.
The article is entitled: “Preventing infections in the ambulatory care workforce: What do
healthcare workers know and do?”
This final report will also be distributed to the GLDHCC user committee as well as any
individuals who are interested.
39 | P a g e

REF RE ENCES
1. Yassi, A., Pawson, D., Leary, T., Sikorski, J., Parent, D., Gilbert, M., et al. Trends in
Workplace Injuries, Illness, and Policies in Healthcare across Canada: Workers’
Compensation Patterns and Policy Changes in Healthcare Organizations. Report for
Health Canada 2004.
2. O'Brien‐Pallas, L., Shamian, J., Thomson, D., Alksnis, C., Koehoorn, M., Kerr, M., et al.
(2004) Work‐related disability in Canadian nurse. Journal of Nursing Scholarship,
36(4), 352‐7.
3. Shamian, J., & El‐Jardali, F. (2007) Healthy workplaces for health workers in Canada:
knowledge transfer and uptake in policy and practice. Healthcare Papers, 7(Special
Issue No), 6‐25.
4. Guzman, J., Yassi, A., Baril, R., & Loisel, P. (2008) Decreasing occupational injury and
disability: the convergence of systems theory, knowledge transfer and action
research. Work, 30(3), 229‐39.
5. Parker, E., Margolis, L.H., Eng, E., & Henriquez‐Roldan, C. (2003) Assessing the
capacity of health departments to engage in community‐based participatory public
health. American Journal of Public Health, 93(3), 472‐477.
6. Browna, L., & Barnett, J.R. (2004) Is the corporate transformation of hospitals
creating a new hybrid health care space? A case study of the impact of co‐location of
Socialpublic and private hospitals in Australia. Science & Medicine, 58(2), 427‐444.
7. Lucarelli, P. Thinking outside the exam room: accessing community resources for
patients in ambulatory care settings. Nurs Econ, 2008, 26(4), 272‐5.
40 | P a g e

8. Jarvis, W.R. (2001) IC and changing health‐care delivery systems. Emerg Infect Dis,
37(2), 170‐ .
9. Canadian Institute for Health Information. (2005) Hospital Trends in Canada –
Results of a Project to Create a Historical Series of Statistical and Financial Data for
Canadian Hospitals Over Twenty‐Seven Years. Available from: www.cihi.ca
10. Menachemi, N., Chukmaitov, A., Brown, L., Saunders, C., & Brooks, R. (2008) Quality
of care in accredited and nonaccredited ambulatory surgical centers. Jt Comm J Qual
Patient Saf, 34(9), 546‐51.
11. Shostek, K. Developing a culture of safety in ambulatory care settings. (2007)
Journal of Ambulatory Care Management, 30(2), 105‐12.
12. Hammons, T., Piland, N., Small, S., Hatlie, M., & Burstin, H. (2003) Ambulatory patient
safety. What we know and need to know. Journal of Ambulatory Care Management,
26(1), 63‐82.
13. Wallace, C., & Quattrone, M. (2007) Risk management tips for ambulatory surgery
l acenters. Journal of Ambu atory Care Man gement, 30(2), 114‐5.
14. Carling PC, Parry MF, Von Beheren SM. Identifying opportunities to enhance
environmental cleaning in 23 acute care hospitals. Infect Control Hosp Epidemiol
2008;29(1):1‐7.
15. Alfa MJ, Dueck C, Olson N, Degagne P, Papetti S, Wald A, et al. UV‐visible marker
confirms that environmental persistence of Clostridium difficile spores in toilets of
patients with C. Difficile associated diarrhea is associated with lack of compliance
with cleaning protocol. BMC Infect Dis 2008;8:64. 169.
41 | P a g e

16. Carling PC, Von Beheren S, Kim P, Woods C. Intensive care unit environmental
cleaning: an evaluation in sixteen hospitals using a novel assessment tool. J Hosp
Infect 2008;68(1):39‐44. 171.
17. Blue J, O'Neill C, Speziale P, Revill J, Ramage L, Ballantyne L. Use of a fluorescent
chemical as a quality indicator for a hospital cleaning program. Can J Infect Control
2008;23(4):216‐9.
18. Hersey, J.C., & Martin, L.S. IC. (1995) Use of IC guidelines by workers in healthcare
facilities to prevent occupational transmission of HBV and HIV: results from a
national survey. Todays OrNurse.17(3), 3748, 1995.
19. Villeneuve, J. (1998) The ceiling lift: An efficient way to prevent injuries to nursing
staff. Journal of Healthcare Safety, Compliance and IC, 9‐24.
20. Begue, R.E., & Gee, S.Q. (1998) Improving influenza immunization among healthcare
7), 518‐20. workers. Infect Control Hosp Epidemiol, 19(
21. Friedman, C., & Petersen, K.H. (2003) IC in Ambulatory Care: Jones & Bartlett
Publishers.
22. Davis, J.E. (1993) Ambulatory surgery ... how far can we go? Med Clin North Am,
77(2), 365‐75.
23. Manian, F.A. (1997) Surveillance of surgical site infections in alternative settings:
exploring the current options. Am J Infect Control, 25(2), 102‐5.
24. Joint Commission on Accreditation of Healthcare Organizations. (2000) Surveillance,
Prevention and Control of Infection Standards for Ambulatory Care. #6332.
42 | P a g e

43 | P a g e
Additional Relevant References
1‐ Gamage B, Moore D, Copes R, et al. BC Interdisciplinary Respiratory Protection Study
Group. Protecting health care workers from SARS and other respiratory pathogens: a
review of the infection‐control literature. Am J Infect Control 2005; 33(2):114‐121.
2‐ Talbot TR, Bradley SE, Cosgrove SE et al. Influenza vaccination of healthcare workers and
vaccine allocation for healthcare workers during vaccine shortages. Infect Control Hosp
Epidemiol 2005;26(11):882‐890.
3‐ Wilde JA, McMillan JA, et al. Effectiveness of influenza vaccine in health care professionals:
a randomized trial. JAMA 1999; 281(10):908‐913.
4‐ Johnson DF, Druce JD, Birch C, et al, A quantitative assessment of the efficacy of surgical and
N95 masks to filter influenza virus in patients with acute influenza infection. Clin Infect Dis
2009; 49(2):275‐277.
5‐ Grayson ML, Melvani S Druce J, et al. Efficacy of soap and water and alcohol based hand‐rub
preparations against live H1N1 influenza virus on the hands of human volunteers. Clin
Infect Dis 2009;48(3):285‐291.
6‐ Sydnor ERM and Perl TM. Hospital Epidemiology and Infection Control in Acute‐Care
Setting. Clin Micro Rev 2011; 241:141‐173.
7‐ Loeb M Dafoe N, Mahony J. et al. Surgical mask vs N95 respirator for preventing influenza
among health care workers: a randomized trial [published online Oct 1, 2009] JAMA 2009,
302(17) 1865‐1871.
44 | P a g e
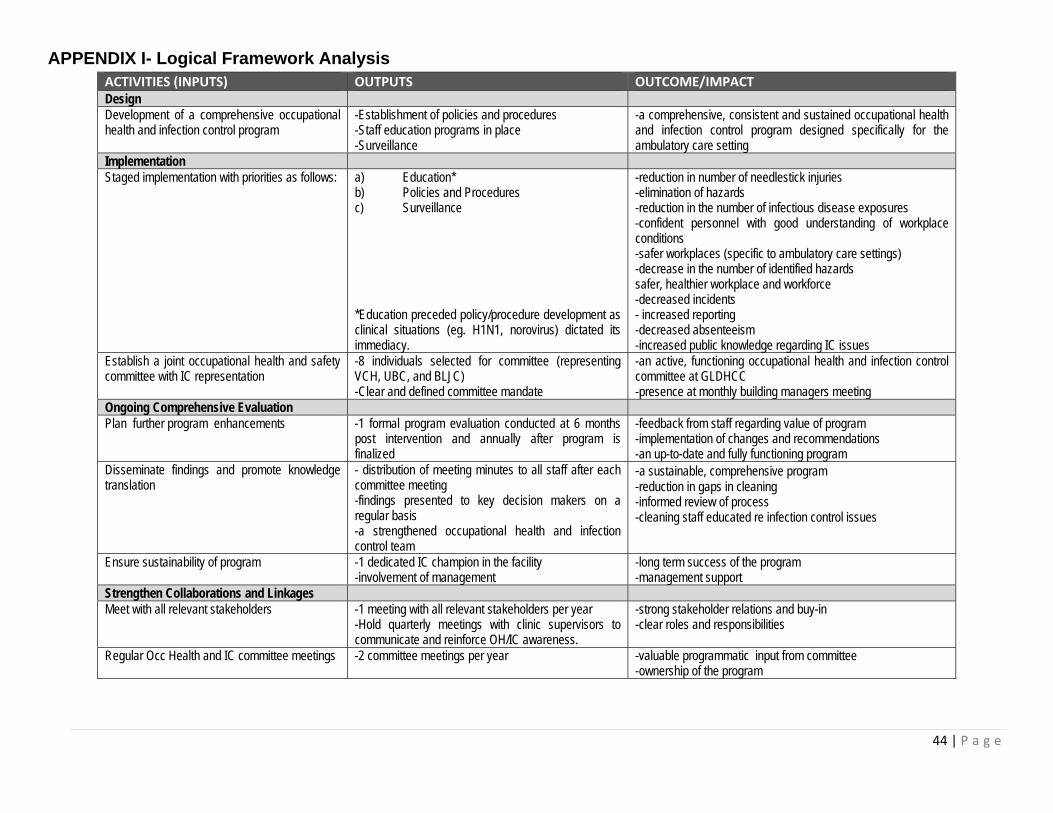
APPENDIX I- Logical Framework Analysis ACTIVITIES (INPUTS) OUTPUTS OUTCOME/IMPACT Design Development of a comprehensive occupational health and infection control program
-Establishment of policies and procedures -Staff education programs in place -Surveillance
-a comprehensive, consistent and sustained occupational health and infection control program designed specifically for the ambulatory care setting
Implementation Staged implementation with priorities as follows: a) Education*
b) Policies and Procedures c) Surveillance *Education preceded policy/procedure development as clinical situations (eg. H1N1, norovirus) dictated its immediacy.
-reduction in number of needlestick injuries -elimination of hazards -reduction in the number of infectious disease exposures -confident personnel with good understanding of workplace conditions -safer workplaces (specific to ambulatory care settings) -decrease in the number of identified hazards safer, healthier workplace and workforce -decreased incidents - increased reporting -decreased absenteeism -increased public knowledge regarding IC issues
Establish a joint occupational health and safety committee with IC representation
-8 individuals selected for committee (representing VCH, UBC, and BLJC) -Clear and defined committee mandate
-an active, functioning occupational health and infection control committee at GLDHCC -presence at monthly building managers meeting
Ongoing Comprehensive Evaluation Plan further program enhancements -1 formal program evaluation conducted at 6 months
post intervention and annually after program is finalized
-feedback from staff regarding value of program -implementation of changes and recommendations -an up-to-date and fully functioning program
Disseminate findings and promote knowledge translation
- distribution of meeting minutes to all staff after each committee meeting -findings presented to key decision makers on a regular basis -a strengthened occupational health and infection control team
-a sustainable, comprehensive program -reduction in gaps in cleaning -informed review of process -cleaning staff educated re infection control issues
Ensure sustainability of program -1 dedicated IC champion in the facility -involvement of management
-long term success of the program -management support
Strengthen Collaborations and Linkages Meet with all relevant stakeholders -1 meeting with all relevant stakeholders per year
-Hold quarterly meetings with clinic supervisors to communicate and reinforce OH/IC awareness.
-strong stakeholder relations and buy-in -clear roles and responsibilities
Regular Occ Health and IC committee meetings -2 committee meetings per year -valuable programmatic input from committee -ownership of the program

45 | P a g e
APPENDIX II- Workplace Assessment Tool Name of Department/Unit :_____________________________
Date of Inspection:______________________________________
No. examination rooms:___________ No. Patients:_______________ Persons Conducting Inspection:___________________________ _____________________________________________________ _____________________________________________________ _____________________________________________________
Unit Supervisor:___________________________________
Number of Employees on unit: ____________
Number of Employees working at this moment: ____________
Number of Nurses:_____
Number of Nursing Assistants: _______
Number of Doctors: ______
Number of Unit Clerks/receptionists:_____
Number of Contracted Workers:__________
Number of “other” personnel: _______ Unit’s Worker Health & Safety Rep. present? Y / N Name:_______________________________________________
Hazard classification Hazard Elements Physical hazards Ionising and non-ionising radiation, noise, vibration, heat, cold, ventilation, illumination,
electricity, fire, sharps Chemical hazards Natural and synthetic compounds that may be in the state of a dust, gas, vapour or fluids Biological hazards Viruses, fungi, parasites, bacteria, pests, reptiles, animals Ergonomic hazards Equipment, tools, work processes, poor lighting, workplace layout and design Safety hazards Trip, slip, fall, unsafe and unguarded equipment, confined spaces, obstructed work areas and
passageways Psychosocial hazards
Aggression, violence,, shift work, emotional stress, over-crowding, understaffing, excessive pace of work, poor interpersonal relationships, fatigue, harassment
Inspection categories:
Satisfactory (S) Hazard requires correction but not an immediate hazard (C)
Hazard requiring immediate correction (IC)
Not Applicable (N/A)

46 | P a g e
ITEM / DESCRIPTION INSPECTION CATEGORY
Comments/Recommended Controls Person Responsible & Due Date
PHYSICAL ENVIRONMENT S C IC N/A
1) Floors, walls, doors, shelves and ceilings
a) floors slip- proof
b) floors, walls, doors and ceilings clean and intact
c) floors and doors clear of obstructions
d) good drainage for spills
e) changes in floor levels clearly marked
f) no moulds (eg. mildew) or fungus
g) no cords on floors or other tripping hazards
h) asbestos labeled and properly removed
i) shelves present and adequate to support material
j) steps and rails
k) ramps for disabled
47 | P a g e
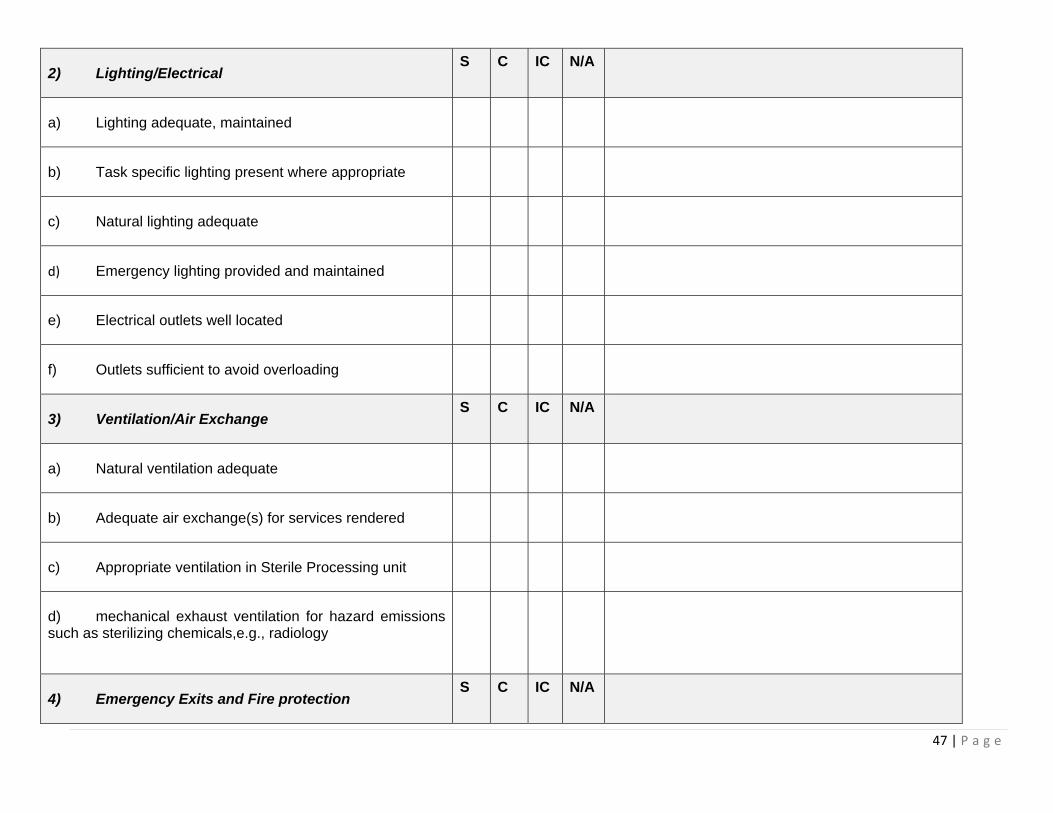
2) Lighting/Electrical S C IC N/A
a) Lighting adequate, maintained
b) Task specific lighting present where appropriate
c) Natural lighting adequate
d) Emergency lighting provided and maintained
e) Electrical outlets well located
f) Outlets sufficient to avoid overloading
3) Ventilation/Air Exchange S C IC N/A
a) Natural ventilation adequate
b) Adequate air exchange(s) for services rendered
c) Appropriate ventilation in Sterile Processing unit
d) mechanical exhaust ventilation for hazard emissions such as sterilizing chemicals,e.g., radiology
4) Emergency Exits and Fire protection S C IC N/A

48 | P a g e
a) Emergency exits visible
b) Emergency exits free from obstruction
c) Emergency evacuation plan posted
d) Fire extinguishers present
e) Fire extinguishers regularly inspected
f) Fire protection equipment (e.g. hoses) accessible and maintained
g) Sprinkler systems maintained
5) Clean and Orderly Appearance, enough room to work
S C IC N/A
a) Hallways
b) Examination/treatment rooms
c) Storage rooms
d) Utility rooms
e) Medication rooms
49 | P a g e
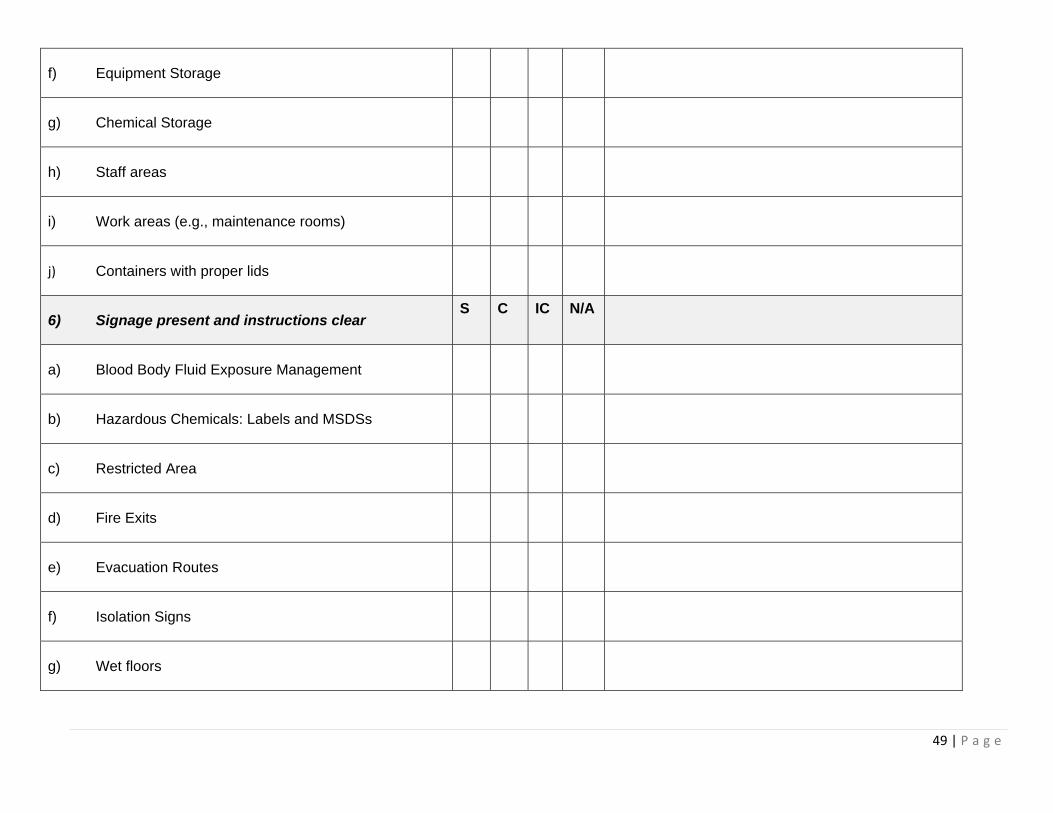
f) Equipment Storage
g) Chemical Storage
h) Staff areas
i) Work areas (e.g., maintenance rooms)
j) Containers with proper lids
6) Signage present and instructions clear S C IC N/A
a) Blood Body Fluid Exposure Management
b) Hazardous Chemicals: Labels and MSDSs
c) Restricted Area
d) Fire Exits
e) Evacuation Routes
f) Isolation Signs
g) Wet floors

50 | P a g e
h) Eye wash stations (eg, in laboratories, chemical storage areas)
i) Instructions for use of Personal Protective Equipment
j) Noise protection required
k) Biohazardous area
l) Radiation area
m) Hand hygiene posters
7) Waste Disposal S C IC N/A
a) Written Biohazardous waste protocol present
b) Written regular waste disposal protocol present
c) Appropriately labeled containers/bags for biohazardous waste
d) Waste facility are clean and well maintained
e) Body fluids, feces disposed of in bedpan cleaner
SPECIFIC OCCUPATIONAL HEALTH PRACTICES AND HAZARDS
S C IC N/A

51 | P a g e
8) First aid
a) appropriate contents
b) at least 1 kit per work area present
c) kits maintained
d) easily accessible
e) personnel trained in first aid, posted and available
f) disaster plan posted (eg, fire or emergency evacuation route)
9) Occupational Health and Safety Act accessible
S C IC N/A
a) OHS Reporting procedures posters displayed
b) Workers’ Compensation Reporting procedures posters displayed
c) Basic Conditions of Employment Act displayed
d) Incidents/accidents reported, registers kept and investigated
e) Health and safety complaint forms available, used and responded to

52 | P a g e
f) Occupational Health and Safety procedures accessible
g) Minutes of OHS Committee posted or passed out
h) Copy of the compliance certificate displayed
i) Injury On Duty register available
j) The facility have an OH physician
k) The facility’s mission/value statement mentions the health and safety of workers as being a priority
l) Vaccination are mandatory for HCWs as a condition of employment
m) The facility provides baseline skin testing for TB exposure monitoring
n) There is a policy or mechanism in place that allows workers to provide feedback to management regarding workplace health and safety concerns
o) There are at least monthly communication methods of OH information to staff
p) Staff training have an occupational health component
10) Psychosocial hazards S C IC N/A
a) Measures in place for reporting workplace violence

53 | P a g e
b) Procedures for handling aggressive patients
c) Staff identification badges worn
d) Contact numbers for Security posted
e) Security available and immediately accessible
f) Entrances Exits, parking areas and outside walkways well lit and secure
g) Access is controlled
h) No working alone
i) staffing patterns and workload
j) teamwork
k) Nurse autonomy for decision-making
l) Effective Communication
m) Supportive Climate
n) Education to meet staff learning needs on violence in the workplace

54 | P a g e
o) Protective security devices
11) Chemical hazards
S C IC N/A
a) All chemical containers labeled
b) Material Safety Data Sheets (MSDSs) available and up-to-date
c) Workers educated and trained about chemical hazards
d) More hazardous chemicals replaced with less hazardous chemicals
e) Adequate time for pesticide residue to be reduced; Switch to less hazardous types of pest control.
12) Radiation Hazards S C IC N/A
a) Lasers shielded, ventilated and eye protection provided
b) X-ray equipment shielded and tested regularly
c) Adequate distance of the exposure button from machine (>1m)

55 | P a g e
SPECIFIC INFECTION CONTROL PRACTICES S C IC N/A
13) Sinks
a) Number of sinks present in area
b) Sink for each examination/treatment room
c) Sinks clean and well maintained
d) Sink present in dirty utility room
e) Sink present in clean room
f) “Clean” and “Dirty” sinks identified
g) Antiseptic soap or alcohol hand rub available
h) Towels available

56 | P a g e
14) Suitable Personal Protective Equipment Adequate supplies of:
S C IC N/A
a) Non-sterile gloves, non-latex
b) Sterile gloves, non-latex
c) Surgical masks
d) N95 respirators supplied
e) N95 respirators in adequate amounts
f) N95 respirator training on fit checking and/or fit testing
g) Protective eyewear
h) Fluid impermeable gowns
i) Isolation gowns or aprons
15) Infection control organizational resource
a) The facility has an IC officer
b) There is active surveillance of nosocomial infection in your facility
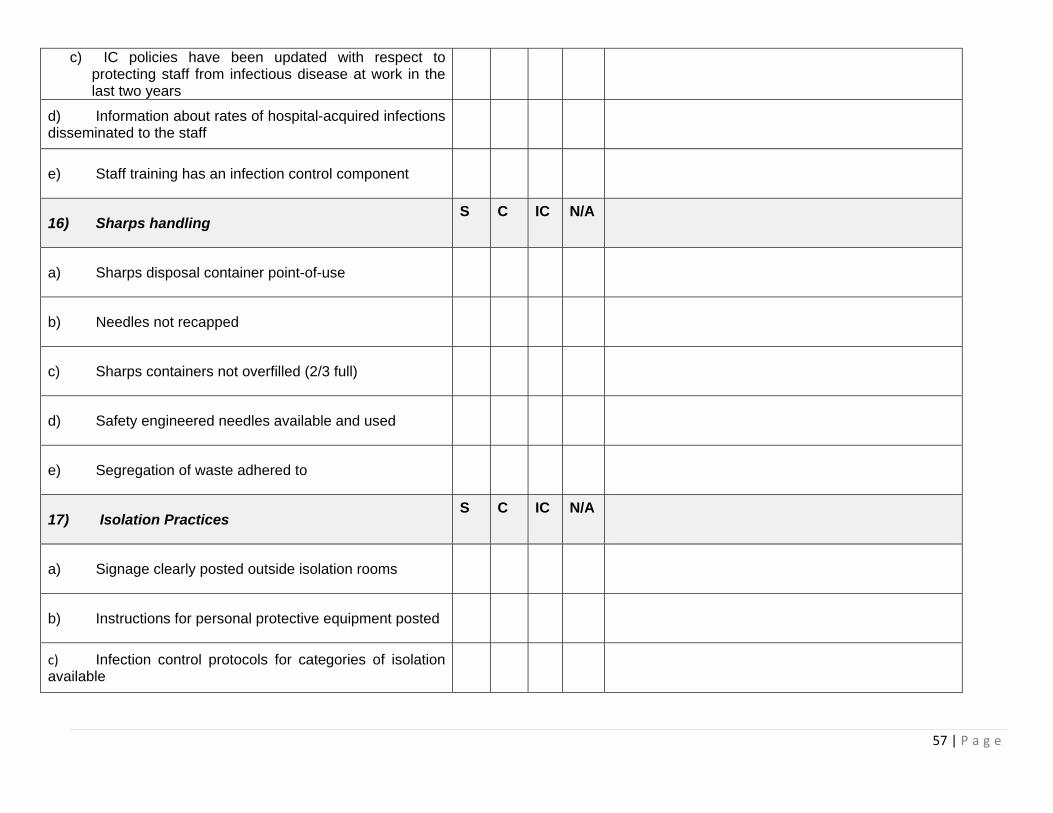
57 | P a g e
c) IC policies have been updated with respect to protecting staff from infectious disease at work in the last two years
d) Information about rates of hospital-acquired infections disseminated to the staff
e) Staff training has an infection control component
16) Sharps handling S C IC N/A
a) Sharps disposal container point-of-use
b) Needles not recapped
c) Sharps containers not overfilled (2/3 full)
d) Safety engineered needles available and used
e) Segregation of waste adhered to
17) Isolation Practices S C IC N/A
a) Signage clearly posted outside isolation rooms
b) Instructions for personal protective equipment posted
c) Infection control protocols for categories of isolation available

58 | P a g e
d) Effective education and training in all infection control procedures
18) Patient Care areas: Treatment Room/Examination Room
S C IC N/A
a) No evidence of food consumption by staff
b) No evidence of consumption of beverages by staff
c) No evidence of food storage in medication refrigerators
d) No evidence of smoking by staff
e) Adequate distance (greater than one metre between beds
f) Infection Control Manual accessible
19) Staff areas S C IC N/A
a) Staff toilets clean
b) Staff toilets with adequate toilet paper and towels (preferably paper) and soap
c) Staff lounge present and clean with no medical supplies or devices present
d) Staff lockers/change area accessible and available

59 | P a g e
EQUIPMENT AND PROCEDURES S C IC N/A
20) Patient Care Areas
a) Glucometers, oximeters, monitoring equipment clean and well maintained
b) Patient lifts available, maintained and clean
c) Bedpans, commodes available and clean
21) Laboratory Areas: Outpatient Laboratory S C IC N/A
a) Centrifuges, automated equipment clean and well maintained
b) Biosafety cabinets present and regularly inspected
c) Chemical hoods present and regularly inspected
d) Splashguards in place where specimens are opened
e) Compressed gases secured, regularly inspected and maintained
f) Chemical flammable safety storage cabinets available and used
g) Equipment and supplies designated as single use not reused (e.g. blood tubes)
h) Chemicals clearly labeled

60 | P a g e
i) Goggles and face shields available
j) Eye wash facilities and safety showers maintained
k) Fire extinguishers available
22) Radiology S C IC N/A
a) Rooms properly marked and only authorized workers permitted in
b) Room doors closed when equipment in use
c) Rooms lead lined
d) Where portable X ray units used, only patient and authorized worker allowed in room
e) Personal dosimeters worn by workers
f) Exposure levels recorded and analyzed
g) Appropriate eye protection provided
h) Lead aprons and collars worn
i) Radiological solutions handled appropriately

61 | P a g e
j) Lead aprons clean and intact
k) Staff in radiology have exposure badges
23) Maintenance areas S C IC N/A
a) Motorised equipment maintained and inspected regularly
b) electrical tools and cords maintained and grounded
c) Hand tools maintained
d) Machine guarding provided and maintained
e) Reduce noise at source
f) Ear protection provided
g) Vessels under pressure maintained and regularly inspected (certificate of manpower)
h) Chemicals clearly labeled
i) Proper lock-out (disconnect) system for all equipment
j) Steam, gas and water pipes clearly marked
k) Ladders maintained in good condition
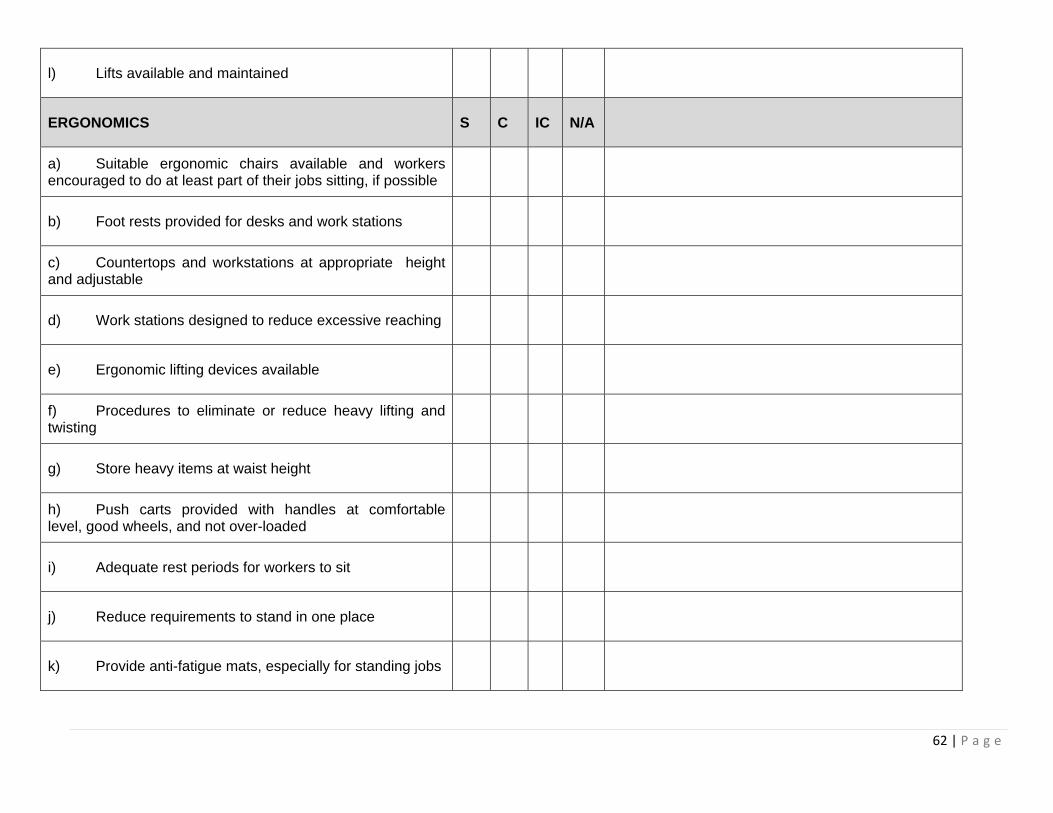
62 | P a g e
l) Lifts available and maintained
ERGONOMICS S C IC N/A
a) Suitable ergonomic chairs available and workers encouraged to do at least part of their jobs sitting, if possible
b) Foot rests provided for desks and work stations
c) Countertops and workstations at appropriate height and adjustable
d) Work stations designed to reduce excessive reaching
e) Ergonomic lifting devices available
f) Procedures to eliminate or reduce heavy lifting and twisting
g) Store heavy items at waist height
h) Push carts provided with handles at comfortable level, good wheels, and not over-loaded
i) Adequate rest periods for workers to sit
j) Reduce requirements to stand in one place
k) Provide anti-fatigue mats, especially for standing jobs
63 | P a g e
l) Comfortable, cushioned footwear provided and worn
m) Adequate numbers of staff to reduce overuse injuries
n) Pregnant workers don’t stand all shift or sit all shift
o) Provide tilt bins with hydraulic lifts
p) Use turntables and conveyors where material needs to be moved
Description of the Service including number of rooms, floor plans, number and location of fixed equipment such as sinks, general layout by drawing a block diagram (use additional page). The block diagram is a map of the workplace and its hazards: ___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
_

64 | P a g e
APPENDIX III- Glo-Germ Environmental Audit Template
Glo‐Germ Environmental Audit Diamond Centre Date: ______________________________________ Location: ____________________________________
Location Pass Fail
1 Door Handle
2 Light Switch
3 Sink
4 Taps
5 Soap Dispenser
6 Paper Towel Dispenser
7 Chairs
8 Bedside Table
9 Bed Rails
10 Bed Mattress
11 Sharps Container
12 Handle Overhead Lamp
13 Stool
14 Toilet Seat
15
16
17
18
19

65 | P a g e
APPENDIX IV- Knowledge, Attitudes and Practice Worker Questionnaire
HEALTH & SAFETY QUESTIONNAIRE As part of an occupational health and safety project conducted by the Infection Control & Occupational Health Subcommittee and funded by WorkSafeBC, we would like to ask you to fill out this questionnaire. This form is divided into four sections. The first section asks you to tell us about your profession and your workplace experiences. The second section asks you about previous education and training, and the third section is an assessment of your knowledge of infection control and occupational safety. The fourth section is a self-report of what your work practices are. Your answers will be confidential and free of personal identification. Your participation in this research is completely voluntary. Refusal to participate will involve no penalty or loss of benefits to which you are otherwise entitled. Please note that by completing this questionnaire, you are voluntarily agreeing to participate in this research study. You will remain anonymous and your data will be treated confidentially at all times. You may withdraw from this study at any moment. WHEN COMPLETED: PLEASE LEAVE WITH RECEPTIONIST OR SLIDE UNDER DOOR OF INFECTION CONTROL OFFICE 4221. TO BE ELIGIBLE FOR A STARBUCKS GIFT CARD, RETURN TO A RESEARCH TEAM REPRESENTATIVE. Interviewee Code (This allows us to track these forms with a follow-up study while protecting your identity.)
Please write the first three letters of your mother’s first name
And the first three letters of your mother’s maiden surname SECTION 1 Information About You
1. Are you employed by:
University of British Columbia Vancouver Coastal Health Private physician or group of physicians Private other
_____________________
2. What is your occupation? (Please, mark only one answer)
Physician Surgeon Nurse Therapist Manager/administrator Clerk/Receptionist Technologist/technician
(specify) ________________________ Student (specify) __________________ Researcher ___________________
Other (specify) ________________________
3. Age: Less than 20 20-29 30-39 40-49 50-59 more than 60
4. Sex: Male Female
5. What is the area you work in? (Please, mark only one answer)
Private ambulatory unit UBC ambulatory unit VCH ambulatory unit Maintenance Food outlet Medical
Laboratory (specify): _________________________ Housekeeping Administration Security Sterile processing
department Other: (specify) _________________________
6. Are you unionized? YES NO
Please name the union to which you belong:__________________________________
7. How many years have you worked in this clinic/office? ______________

66 | P a g e
8. How long have you worked in this building? ______________
9. Do you know how to contact the Occupational Health Department (Worksafe & Wellness VCH)?
YES NO Can’t remember
10. Do you know how to contact your joint occupational health and safety committee representative?
YES NO Can’t remember
11. Do you know how to contact Infection Control?
YES NO Can’t remember
12. Do you know how to contact your internal unit or department safety/fire officer?
YES NO Can’t remember
13. Did you have a needle stick/sharp injury or other exposure to blood or body fluids in the last 2 years?
YES NO Can’t remember
If YES, to the above question, to whom did you report the injury or exposure?
Occupational Health Infection Control First Aid Health and Safety Committee representative Colleague Supervisor Other (please specify) ______________________ I did not report
If you have NOT reported, please check off all that apply:
Did not know how or to whom to report it Did not think it was serious or anything needed to be done for follow-up Thought I would be blamed or made to feel bad for allowing this to happen Other (please specify) ______________________
14. Have you been vaccinated for influenza this year? YES NO Can’t remember
15. Do you get vaccinated for influenza every year? YES NO Can’t
remember
16. Have you been vaccinated for Hepatitis B? YES NO Can’t remember
17. If YES to Q16, have you completed all 3 doses? YES NO Can’t
remember
18. If NO to Q15 or Q16, describe reasons: _________________________________________
19. Were you screened for tuberculosis upon employment? YES NO Can’t remember
20. Do you ever use a N95 respirator? YES NO Can’t remember
I don’t know what a N95 respirator is
21. Did you have an occupational health evaluation upon hiring? YES NO Can’t remember

67 | P a g e
SECTION 2 Self-evaluation on learning activities and practices Please mark the option which best reflects your practices.
1. Have you received health & safety training in the last 2 years? YES NO
2. Please identify the training you have had in the past 2 years. (Mark with an X)
Training Taken YES NO Not Applicable
a. Hand Hygiene
b. Isolation Procedures
c. Use of personal protective equipment
d. Needle-stick and sharps injury prevention
e. HIV/AIDS prevention
f. Waste disposal management
g. Chemical hazards including chemicals used for cleaning
h Ventilation requirements
i. Machine hazards
j. Safe patient handling or prevention of back injuries
k. Violence prevention
l. Accessing first aid for injuries
m. Psycho-social stresses at work
n. Reporting injuries through Employee Incident Report
o. Emergency procedures
p. Online infection control module
3. Do you know how to access the online infection control manual? YES NO
4. Rate your knowledge about infection control practices. 1 Not at all
2 A bit
3 More or less
4 Quite a bit
5 Very High
5. Rate your knowledge about WHEN to use the following personal protective equipment:
1 Not at all
2 A bit
3 More or less
4 Quite a bit
5 Very High
Not applicable
Surgical mask
N95 respirator
Sterile gloves
Non sterile gloves
Goggles
Gowns/Aprons
6. Rate your knowledge about HOW to put on and take off the following personal protective equipment:
68 | P a g e
1 Not at all
2 A bit
3 More or less
4 Quite a bit
5 Very High
Not applicable
Surgical mask
N95 respirator
Sterile gloves
Non sterile gloves
Goggles
Gowns/Aprons
7. Rate your knowledge about recommended procedures and protocol during the following outbreaks:
1 Not at all
2 A bit
3 More or less
4 Quite a bit
5 Very High Unsure
Influenza
Gastrointestinal (GI)
8. I know how to report a workplace risk/hazard YES NO Not Sure
9. I know how to report a workplace injury through an employee incident report. YES NO Not Sure
SECTION 3 Knowledge evaluation Please mark YES or NO
1. Needles should be recapped before disposing in a sharps container. YES NO
2. The most important practice to prevent infections is the frequent cleaning of the environment.
YES NO
3. The use of gloves is recommended only when the risk of blood and body fluid exposure is present.
YES NO
4. Patients with suspected tuberculosis can sit in the waiting room with other patients.
YES NO
5. All needle-stick and sharp injuries must be evaluated by an occupational health responsible/service.
YES NO
6. Having food or drinks in the clean storage places or in the medication room/ work station is permitted as long as the items are disposed of afterwards.
YES NO
7. The Infection Control manual available at the Front Desk is a valuable tool for proper cleaning protocol.
YES NO
8. Local exhaust ventilation such as hoods is needed to protect people from breathing in harmful vapours.
YES NO
69 | P a g e
9. First aid kits should be centrally located in one area of the floor/building.
YES NO
10. Patients who are verbally abusive are permitted to do so as part of their right to care.
YES NO
11. If a patient is known to have HIV or Hepatitis you should change your work practice.
YES NO
12. As long as you know how to lift heavy things properly your risk of back injury is minimal.
YES NO
13. It’s OK to have mobile X-Ray equipment used in a clinic with a number of patients because they usually don’t stay in the clinic long enough to have significant exposure.
YES NO
14. Twisting can be as bad for your back as lifting. YES NO
15. Foot rests under desks and at work stations are primarily used to rest your legs.
YES NO
16. Blood / body fluid soaked linen can be put in any plastic bag. YES NO
17. General waste and medical waste can be mixed in the same container if there are no sharps.
YES NO
18. I am capable of recognizing potentially aggressive patients YES NO
19. I know how to assess patients potential aggressive behaviour. YES NO
SECTION 4 Infection control and occupational health and safety procedures’ evaluation Please mark the option which best reflects your practices.
1. I use eye protection (others than prescription glasses) during procedures with potential for splashes and aerosols:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
2. I clean my hands between the care of patients:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
3. I change my procedures if I know a patient has HIV, hepatitis B or C:
Never Half of the time Always

70 | P a g e
0% 25% 50% 75% 100% Not applicable
4. I recap needles:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
5. I change gloves (if worn) between patients:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
6. I ask for help to reposition or to lift heavy objects or patients:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
7. I use local exhaust ventilation when working with harmful chemicals:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
8. I wear N95 respirators when caring for patients with airborne diseases such as TB:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
9. I wear hearing protection in noisy areas:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
10. I use lifting devices that are provided:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
11. I use guards on machinery:
Never Half of the time Always

71 | P a g e
0% 25% 50% 75% 100% Not applicable
12. I report spills I see:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
13. I report health and safety problems to the occupational health service:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
14. I report health and safety problems to my occupational health and safety committee/representative:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
15. I make suggestions for correcting health and safety problems to the occupational health service:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
16. I make suggestions for correcting health and safety problems to my occupational health and safety committee representative:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
17. I dispose of sharps in a sharps container:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
18. I work in situations where patients suspected of having TB are seen at clinic/office:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
19. I assess patients' potential for aggressive behaviour upon admission:
Never Half of the time Always

72 | P a g e
0% 25% 50% 75% 100% Not applicable
20. I communicate to co-workers about potentially aggressive patients:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
21. I report workplace violence incidents to managers:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
22. I make suggestions for controlling workplace violence:
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
23. I utilize the online Infection Control manual as an effective workplace tool.
Never Half of the time Always
0% 25% 50% 75% 100% Not applicable
If you do not use the online Infection Control manual, who do you seek Infection Control knowledge from (please
specify):______________________________________________________________________________
SECTION 5 In the following section, we would like to ask you about the safety climate, attitude and perception in safety and risk in your current work area. There are no “right” or “wrong” answers. Please tell us your choice for each of the following statements (check only one scale per question) 1. I think about how my job or work area can be made safer and make suggestions:
Never Half of the time Always Not applicable
0% 25% 50% 75% 100%
2. I get clear supervision regarding safe work practices:
Never Half of the time Always Not applicable
0% 25% 50% 75% 100%
73 | P a g e
3. I feel safe from violence at work:
Never Half of the time Always Not applicable
0% 25% 50% 75% 100%
4. I am encouraged to report injuries and illness at work:
Never Half of the time Always Not applicable
0% 25% 50% 75% 100%
5. On my unit, non-compliance with infection control and safety practices are corrected:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
6. On my unit, people are recognized for complying with infection control and safety practices:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
7. In my current work area, there is open communication between supervisors and staff:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
8. In my current work area, follow-up investigations of reported incidents are a priority with management:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
9. In my current work area, supervisors and infection control representatives work together to ensure the safest possible working conditions with regards to infectious diseases:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
74 | P a g e
10. In my current work area, I believe that management attitudes about routine infection control practices influence employee behaviour:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
11. I have too much to do to always follow routine infection control practices:
Strongly disagree
Somewhat disagree
Neither agree nor disagree
Agree Strongly agree
Not applicable
0% 25% 50% 75% 100%
12. If I contracted infectious disease from direct patient contact, I believe the impact on my own health would be:
Extremely severe
Severe Moderate Mild Minimal Don’t know
0% 25% 50% 75% 100%
13. I believe my own risk for contracting infectious disease by caring for patients with the infectious diseases is:
Extremely severe
Severe Moderate Mild Minimal Don’t know
0% 25% 50% 75% 100%
14. I believe the risk of transmitting infectious disease such as influenza to others close to me (e.g. family, friends) is:
Extremely severe
Severe Moderate Mild Minimal Don’t know
0% 25% 50% 75% 100%
15. I like to think things over carefully before I act:
Never Half of the time Always Not applicable
0% 25% 50% 75% 100%
16. I follow the safety rules for infection control at work:
Never Half of the time Always Not applicable
0% 25% 50% 75% 100%
17. I make my own judgements as to when to use Personal Protective Equipment (PPE) to prevent infectious disease transmissions:
Never Half of the time Always Not applicable
75 | P a g e
0% 25% 50% 75% 100%
18. For areas where you feel that your practices are less than what you feel is recommended, why do you think this is?
Not at all important
Not very important
More or less important
Quite important
Very Important
Not applicable
Not enough time
Unavailability of proper equipment
Unavailability of proper space
Do not feel the risk requires it
Peer pressure
Not well enough trained
Proper supervision not provided
Other (please specify)
____________________________
If you have any comments or suggestions, please write them in the space provided below. Thank you for your time and your answers.
__________________________________________________________________________________________________________________________________________________________________

APPENDIX V- FAQ Sheet
Dear Colleagues, Thank you for taking the time to complete The Health and Safety Questionnaire for the ongoing WorkSafe BC funded project assessing occupational health and infection control needs at the Gordon and Leslie Diamond Health Care Centre. Your responses and feedback are extremely valuable and greatly appreciated. Attached are the results of the questionnaire showing percentages of CORRECT responses. Please take a moment to review and see where strengths and weaknesses in your knowledge and practice exist. Highlighted in red are results that are particularly noteworthy. We have also included some helpful key points to remember in the survey section and as an attachment. We will be re-administering the questionnaire in the near future and look forward to your continued support and participation. Starbucks gift cards will be distributed! If you have any questions or comments, please feel free to email Lyndsay at [email protected] or call 604-827-3010 Dr. Elizabeth Bryce, Dr. Annalee Yassi, Linda Kingsbury and Lyndsay O’Hara
76 | P a g e
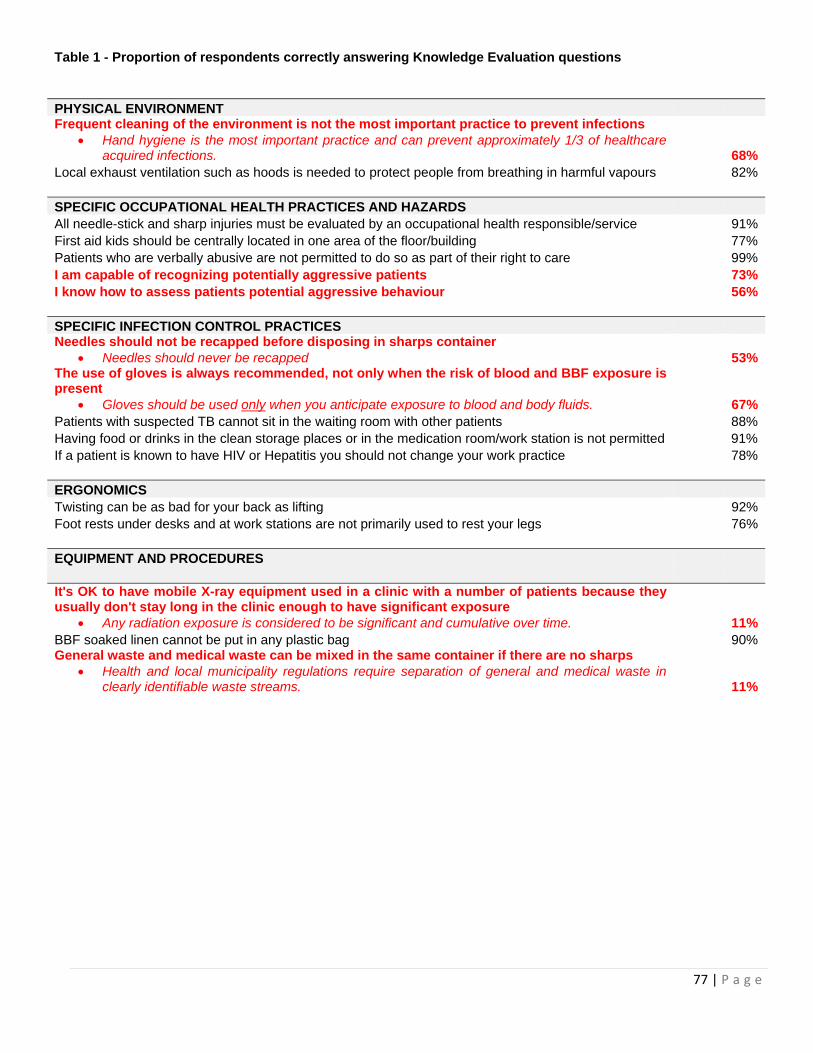
77 | P a g e
Table 1 - Proportion of respondents correctly answering Knowledge Evaluation questions PHYSICAL ENVIRONMENT Frequent cleaning of the environment is not the most important practice to prevent infections
• Hand hygiene is the most important practice and can prevent approximately 1/3 of healthcare acquired infections. 68%
Local exhaust ventilation such as hoods is needed to protect people from breathing in harmful vapours 82% SPECIFIC OCCUPATIONAL HEALTH PRACTICES AND HAZARDS All needle-stick and sharp injuries must be evaluated by an occupational health responsible/service 91%First aid kids should be centrally located in one area of the floor/building 77%Patients who are verbally abusive are not permitted to do so as part of their right to care 99%I am capable of recognizing potentially aggressive patients 73%I know how to assess patients potential aggressive behaviour 56% SPECIFIC INFECTION CONTROL PRACTICES Needles should not be recapped before disposing in sharps container
• Needles should never be recapped 53%The use of gloves is always recommended, not only when the risk of blood and BBF exposure is present
• Gloves should be used only when you anticipate exposure to blood and body fluids. 67%Patients with suspected TB cannot sit in the waiting room with other patients 88%Having food or drinks in the clean storage places or in the medication room/work station is not permitted 91%If a patient is known to have HIV or Hepatitis you should not change your work practice 78% ERGONOMICS Twisting can be as bad for your back as lifting 92%Foot rests under desks and at work stations are not primarily used to rest your legs 76% EQUIPMENT AND PROCEDURES It's OK to have mobile X-ray equipment used in a clinic with a number of patients because they usually don't stay long in the clinic enough to have significant exposure
• Any radiation exposure is considered to be significant and cumulative over time. 11%BBF soaked linen cannot be put in any plastic bag 90%General waste and medical waste can be mixed in the same container if there are no sharps
• Health and local municipality regulations require separation of general and medical waste in clearly identifiable waste streams. 11%
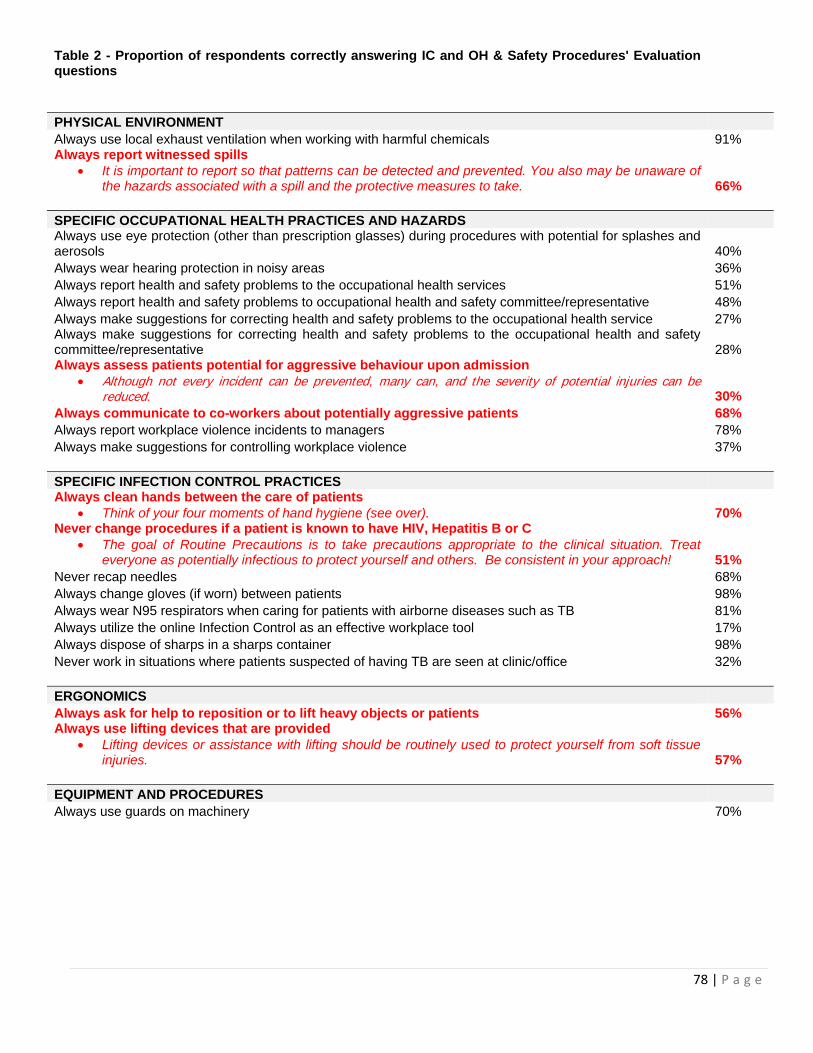
78 | P a g e
Table 2 - Proportion of respondents correctly answering IC and OH & Safety Procedures' Evaluation questions PHYSICAL ENVIRONMENT Always use local exhaust ventilation when working with harmful chemicals 91% Always report witnessed spills
• It is important to report so that patterns can be detected and prevented. You also may be unaware of the hazards associated with a spill and the protective measures to take. 66%
SPECIFIC OCCUPATIONAL HEALTH PRACTICES AND HAZARDS Always use eye protection (other than prescription glasses) during procedures with potential for splashes and aerosols 40% Always wear hearing protection in noisy areas 36% Always report health and safety problems to the occupational health services 51% Always report health and safety problems to occupational health and safety committee/representative 48% Always make suggestions for correcting health and safety problems to the occupational health service 27% Always make suggestions for correcting health and safety problems to the occupational health and safety committee/representative 28% Always assess patients potential for aggressive behaviour upon admission
• Although not every incident can be prevented, many can, and the severity of potential injuries can be reduced. 30%
Always communicate to co-workers about potentially aggressive patients 68% Always report workplace violence incidents to managers 78% Always make suggestions for controlling workplace violence 37% SPECIFIC INFECTION CONTROL PRACTICES Always clean hands between the care of patients
• Think of your four moments of hand hygiene (see over). 70% Never change procedures if a patient is known to have HIV, Hepatitis B or C
• The goal of Routine Precautions is to take precautions appropriate to the clinical situation. Treat everyone as potentially infectious to protect yourself and others. Be consistent in your approach! 51%
Never recap needles 68% Always change gloves (if worn) between patients 98% Always wear N95 respirators when caring for patients with airborne diseases such as TB 81% Always utilize the online Infection Control as an effective workplace tool 17% Always dispose of sharps in a sharps container 98% Never work in situations where patients suspected of having TB are seen at clinic/office 32% ERGONOMICS Always ask for help to reposition or to lift heavy objects or patients 56% Always use lifting devices that are provided
• Lifting devices or assistance with lifting should be routinely used to protect yourself from soft tissue injuries. 57%
EQUIPMENT AND PROCEDURES Always use guards on machinery 70%

Key Points to Remember
Hand hygiene IS the single most important thing you can do to prevent infections! YOUR 4 MOMENTS OF HAND HYGIENE: 1‐Before initial patient/patient environment contact 2‐ Before aseptic procedure 3‐After body fluid exposure risk 4‐After patient/patient environment contact
Routine or Standard Infection Control Practices These are the practices you use every day to prevent transmission of infections between yourself and your patient or client, yourself and other healthcare workers, and from patient to patient. It applies to all people who may be affected such as residents, patients, staff and visitors These practices are directed at ALL body substances including blood, secretions, and excretions, as well as mucous membranes and non‐intact skin.
Sharps Disposal Needles should NEVER be recapped. Specially designed sharps containers are used for disposal. Please pay attentions when depositing your sharps as occasionally a sharp may protrude from the container. Ensure that sharps disposal containers are readily accessible and emptied/replaced regularly.
Personal Protective Equipment When are GLOVES required? • Touching body secretions and excretions • Touching mucous membranes • Touching non‐intact skin • Gloves are NOT a substitute for hand hygiene • Use the right type of glove for the task • Sterile gloves are generally only used for sterile procedures. Non‐sterile gloves can be used for most
patient care. • Gloves are NOT required when pushing a wheelchair or stretcher, between contact with different
patients (always use different gloves), when feeding or dressing a patient who is not in isolation.
When to use an N95 respirator vs. a surgical mask? N95 respirators: • For airborne isolation when entering the room. • Requires a yearly fit test. • Must perform a fit check to ensure a good seal every time you wear it. Surgical masks are recommended: • For healthcare personnel to protect patients during aseptic procedures. • For anyone entering the room of a patient in droplet isolation. • For healthcare personnel to protect patients who are immuno‐compromised. • For patients in airborne or protective isolation when leaving the room is necessary. • For healthcare personnel during patient care activities likely to generate sprays of blood, body fluids,
secretions or excretions.
Waste Management
Biomedical Waste 1. Non‐Anatomical Waste is: (Deposited in YELLOW garbage bags/containers)
• all sharps • chemotherapy waste • suction liners, pleuravacs containing blood • any disposal item grossly soiled or that on compression leaks blood or body fluids • lab cultures or specimens
2. Anatomical Waste is: (Deposited in RED garbage bags/containers) • human tissue or body parts • animal tissue or body parts
Non‐biomedical Waste
79 | P a g e

The following is NOT biomedical waste and can be deposited in regular DARK GREEN or BLACK garbage bags: • suction tubing and catheters, empty catheter bags, blue disposable pads, paper towels or packaging,
intravenous bags, soiled but not leaking dressings.
Ergonomics Always ask for help to reposition or to lift heavy objects or patients. Always use lifting devices that are provided.
Rules for Safe Lifting Use the following acronym as a guide when engaging in client handling procedures:
Back Straight Avoid Twisting Close to Body Keep Smooth
BACK STRAIGHT
• Discs can tolerate larger compressive loads when the back is straight. • Discs are weaker when lifting in a flexed position. • Maintain the spine’s neutral curves. • Keeps spine aligned and moving smoothly. • Minimizes stress on spine. • Imaginary line to maintain curves in balance
AVOID TWISTING • Discs are weaker when lifting is combined with twisting. • Joints are designed to prevent rotation. • If you twist when you lift the joints become inflamed and sore.
CLOSE TO YOUR BODY • If an object is at a greater distance from your body for lifting, your back muscles and joints have to
work harder to lift the weight creating greater stress on your back. • If you keep the exact same load close to your body, the lesser distance creates a lighter load and
less stress on your back. KEEP SMOOTH
• Jerking increases the load on the discs. Aggression When should a violent incident be reported? A violent incident should be reported every time a staff member is: • Threatened verbally or physically e.g., a patient makes a threat to harm staff or family of staff; a visitor yells and swears at staff • At risk of being injured or harmed e.g., a visitor in a work area carrying a weapon; a patient kicking at staff but not connecting; a patient tries to throw or break furniture • Traumatized psychologically e.g., a staff member witnesses a co‐worker being attacked; a patient makes racist/sexual comments to staff • Physically injured as a result of aggression/violence How should violent incidents be reported? A description of the incident should be: • recorded on an employee accident/injury report form and/or other related forms (e.g. a patient record, unusual incident report form) • communicated to the person in charge Communication! • Develop and execute a communication plan to ensure all management, supervisors and workers are informed about occupational health and infection control policies and procedures. • Ensure all levels of the organization are included in the development and execution of the communication plan to promote “buy‐in” and support from everyone. • Provide updated information to all staff on a regular basis • Ensure information is accessible to all staff • Ensure all levels of the organization are included in communication
80 | P a g e

All rights reserved. The Workers’ Compensation Board of B.C. encourages the copying, reproduction, and distribution of this document to promote
health and safety in the workplace, provided that the Workers’ Compensation Board of B.C. is acknowledged. However, no part of this publication may be copied, reproduced, or distributed for profit or other
commercial enterprise or may be incorporated into any other publication without written permission of the Workers’ Compensation Board of B.C.
Additional copies of this publication may be obtained by contacting:
Research Secretariat 6951 Westminster Highway Richmond, B.C. V7C 1C6
Phone (604) 244-6300 / Fax (604) 244-6299 Email: [email protected]
81 | P a g e
APPENDIX VI- Infection Control Basics for Medical Students INFECTION CONTROL & OCCUPATIONAL HEALTH SYNOPSIS
T
he goal of this outline is to inform you about how you can best protect yourself and your patients from acquiring and transmitting organisms.
Key Points to Always Keep in Mind
Routine Practices are the infection prevention and control practices applied to prevent the spread of infectious diseases. The principle is to treat all patients as if they may be infected with, or capable of transmitting, an infectious disease.
Comply with Airborne/Droplet/Contact Precaution Signage
Pay special attention and ask what to do if you see an isolation sign. Wear appropriate personal protective equipment if necessary. If you don’t know how to remove PPE safely without
contaminating yourself; ask for help
• •
Take Care of Your Own Health
inations. • Don't come to work if you are ill.
Maintain your immunizations, particularly influenza vacc Ensure that your fit testing for N95 respirator is current. •• Practice Proper Respiratory Cough Etiquette
and co• • ugh or sneeze into your upper sleeve if possible. Cover your mouth and nose while coughing or sneezing
If you use a tissue, dispose of the tissue in a waste receptacle. Clean your hands after coughing or blowing your nose.
Don't touch your eyes or mucous membranes with your fingers. •• Practice Correct Waste Segregation It is important to note that although biomedical material may be infectious, not all biomedical material is biomedical waste
as referenced in the CCME guidelines. Practicing correct waste segregation is important. Practice Safe Sharps Techniques Dispose of sharps immediately after use in an approved sharps container. Always look at the sharps container when
disposing of the needle. Many injuries occur because of not looking directly at the sharps container during disposal. Do not recap needles before disposal and do not expect someone else to dispose of sharps that you have used.
Steps to Follow When Examining a Patient 1. Clean Your Hands • visibly If your hands are soiled, wash your hands with soap and warm water. Dry with a single‐ use towel. Use the
towel to turn off the taps and open the door. If not visibly soiled, you may also use waterless hand sanitizer. • Clean your hands between contact with every patient/client, before eating or handling food, after using the toilet,
r PPE. whenever hands are soiled, before donning and after removal of gloves and othe
• 2. Maintain a Clean Environment
Discard any dirty items (i.e. tongue depressors and otoscope tips) immediately. • removing and before replacing the exam paper), countertops] with the
ient/client. Clean surfaces [e.g. examining bed (after antiseptic wipes provided between each pat
• Clean up any body fluid spills immediately. 3. Clean Your Hands Again Before Exiting the Room
Test Your Knowledge…..Complete the Online Infection Control Module! http://picnetbc.ca//sites/picnetbc2/files/Online_IC_Module/lesson/IC_Basic_v3.html For More Information: VCH Regional Infection Control Manual- http://vchconnect.vch.ca/icmanual/ How to Contact Infection Control: Sydney Scharf, Senior Infection Control Practitioner, VGH (604) 875-4002