Embed Size (px)
Citation preview
An Organisation-wide Policy for the Management of Incidents
Diversity Statement This document is underpinned by the Trust’s principle of treating and caring for our staff, visitors and patients as individuals by means of dignity and respect regardless of gender, race, ethnicity, religion/belief, sexual orientation and or disability. This document will be reviewed and measured against Trust diversity values, standards and targets that are
currently contained with the strategy for fairness and equality
Consultation This policy was reviewed with the following individuals and groups
Nursing and Medical Directors Human Resources Managers Clinical Risk Assurance Committee
members Health and Safety Committee members
Patient Safety Advisors Modern Matrons
University Hospitals Bristol (NHS) Foundation Trust is referred to throughout this document as UH Bristol TRUST.
Version: 4 Ratified by: Clinical Risk Assurance Committee
(CRAC) + Trust Health and Safety Committee (H & S)
Date ratified: July 2008 Name of originator/author: Nicola Henderson Melanie Fewkes
Patient Safety Manager and Head of Health and Safety Services
Name of responsible committee: CRAC + H & S + Trust Governance and Risk Management Committee
Date issued: March 2009 Review date: March 2012 Target audience: All UH Bristol Trust staff in clinical and
non-clinical roles

2
Contents Section Page
1 Introduction 4
2 Purpose 4
3 Definitions 5
4 Duties 7
4.1 Role of affected/involved staff member 7
4.2 Role of line manager 7
4.3 Role of senior manager 8
4.4 Role of risk manager/equivalent 9
4.5 Role of nominated director(s) 9
4.6 Role of chief executive 10
4.7 Role of the board 10
4.8 Role of the committee with overarching responsibility for risk management 10
4.9 Role of any other committees/groups with responsibilities for incident management 10
5 Communication and Notification 10
5.1 Patient/relative/visitor/contractor communication & support 10
5.2 Process by which to raise concerns 11
5.3 Internal communication 11
5.4 External stakeholder notification 11
5.5 Media involvement 11
6 Incident Investigation Procedure 12
6.1 Incident grading and appropriate levels of investigations 13
6.2 Responsibility for investigation 13
6.3 Root cause analysis 13
6.4 Recommendations and action planning 14
6.5 Monitoring of action plans 14
6.6 Process of ensuring continual risk reduction following the implementation of action plans 15

3
6.7 Involvement of relevant stakeholders 15
6.8 Sharing of lessons learnt 15
7 Incident & Causal Factor Analysis 15
7.1 Responsibility for incident analysis 15
7.2 Responsibility for causal factor analysis post investigation 16
8 Hotline Arrangements 16
8.1 Management responsibility 16
8.2 Phone lines 16
8.3 Staffing 16
8.4 Capacity to manage calls over time 16
8.5 Documentation 16
8.6 Record keeping 16
8.7 IT and postal arrangements 16
9.1 Monitoring effectiveness 17
10 Dissemination, implementation and access to this policy 18
11 Review, updating and archiving of this document 18
12 References 18
Appendices 19
Appendix A Incident reporting form 20
Appendix B High Risk Incident Checklist
Instruction for managers
Flow chart for RIDDOR reportable incidents
Example of RIDDOR incident investigations
Medication incidents and classification
Guide to incident form completion
22
23
25
26
31
32
Appendix C Risk matrix Managers Guide 33
Appendix D List of reportable incidents (including those which will be deemed serious)
Examples of Clinical (patient safety) and non clinical incidents
36
Appendix E List of internal and external stakeholders 38
Appendix F List of associated policies 40
Appendix G Guidance on how to write a statement 41
4
Appendix H Incident investigation techniques
Root Cause Analysis
‘5 whys’
‘fishbone’
NPSA 7 steps to patient safety
ALARM list of contributory factors in incidents
NPSA Incident decision tree for involvement of individual members of staff
Trust template for recording incident investigations
NPSA incident reporting tools for use from 2008 onwards (patient safety incidents)
Example of use of NPSA reporting tools
43
44
45
47
48
49
50
51
52
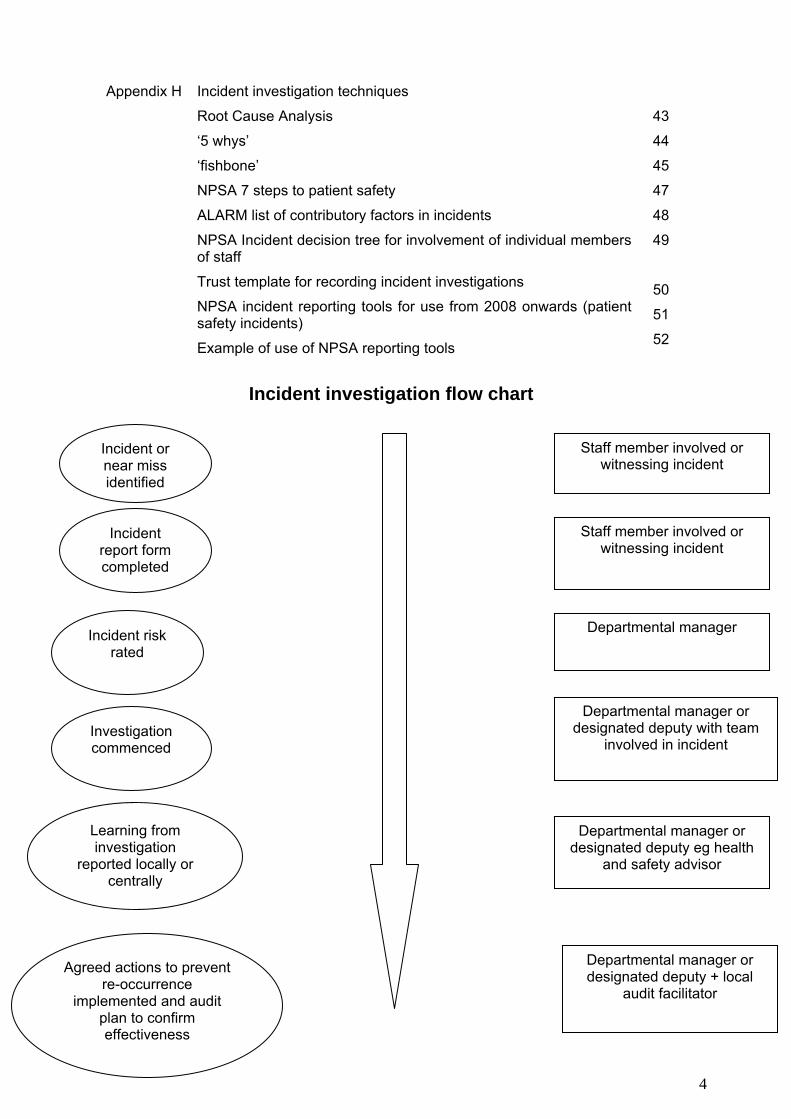
Incident investigation flow chart
Incident or near miss identified
Incident report form completed
Incident risk rated
Investigation commenced
Learning from investigation
reported locally or centrally
Agreed actions to prevent re-occurrence
implemented and audit plan to confirm effectiveness
Staff member involved or witnessing incident
Staff member involved or witnessing incident
Departmental manager
Departmental manager or designated deputy with team
involved in incident
Departmental manager or designated deputy eg health
and safety advisor
Departmental manager or designated deputy + local
audit facilitator

5
1 Introduction As part of the Risk Management Strategy, UH Bristol Trust supports prompt reporting of all incidents whether clinical, non-clinical or ‘near misses’ to improve patient and staff safety and quality of care. This policy and guidelines will be reviewed and ratified by the designated sub committees of the Trust Board. The agenda of the Trust Board meetings reflects the pre-eminence afforded to risk management. Reporting, investigation and learning from incidents is a key element of risk management activity. In relation to patient safety it is supported by the adoption of the ‘Safer Patients Initiative’ work-streams including Executive ‘walk-rounds’. 2 The aim of this document is to support all staff by providing:
• Information about the Trust’s incident reporting systems • Guidance of investigation procedures at individual, local and Trust level • Information relating to professional, statutory and legal duties • Tools for the investigation and identification of learning from incidents
The Mission Statement for UH Bristol Trust states: ‘We will provide patient care, education and research of the highest quality In pursuit of this mission we will by guided by the following values We will put patients first We involve, develop and support staff We promote innovation and improvement We pursue excellence in everything We respect others and treat everyone as equals We work in partnership to improve the health and well-being of the community, within a sustainable environment We are accountable for our use of public resources’ (UH Bristol Trust internet Feb 2008)
As an example, Trust Board Meeting agendas prioritise a regular report on governance to include patient, staff and visitor safety.
2 Purpose and Culture The purpose of this Trust-wide policy is to ensure there is a structured, consistent and systematic approach to the reporting and investigation of incidents which led to, or could have led to harm. All staff are encouraged to report adverse event/incidents/accidents via the adverse incident reporting procedure. The UH Bristol Trust Policy and Procedure on ‘Speaking Out’ 2007 (HR web Appendix F) enables staff to voice concerns about any aspect of suspected malpractice. This would include investigation of patient care and health and safety issues (section1). In addition, staff to whom an incident or near miss is reported (whether by a patient, visitor or colleague) are under a similar obligation to respond in accordance with this policy. The Trust supports an open and ‘fair blame’ culture throughout the organisation in the reporting and management of incidents. The adverse incident process must therefore be viewed as non-threatening to ensure openness among staff. This will enable lessons to be learnt from incident and near miss reporting to promote a safer environment. The policy covers:
2 Superceded by ‘Patient Safety First’ campaign 2009

6
• All incidents involving patient care, whether resulting in actual injury or harm, or the potential to cause injury or harm (near miss).
• All non-clinical incidents/accidents involving patients, staff and visitors whilst on Trust property
NB: For all research related serious adverse events, specific guidance is available (Appendix F) Through the data and learning obtained from review of reported incidents the Trust is able to introduce changes to practice which will improve safety for patients, staff, visitors and contractors. Qualitative and quantitative data analysis will be used and reported throughout the organisation to facilitate this. Details of the procedures to be followed are attached to this policy in the appendices
3. Definitions and Table of Abbreviations
Adverse incident: An event or circumstance that could or did lead to unintended or unexpected harm, loss or damage. Could apply to patients, staff and visitors.
Patient safety Incident: also known as a clinical incident. ‘Any unintended or unexpected incident that could have or did lead to harm for one or more patients’. NPSA 7 Steps to Patient Safety (2004)
Serious adverse incident: (also known as serious untoward incident) any event or circumstance arising that could have or did lead to serious unintended or unexpected harm, loss or damage. (Serious Untoward Incident Policy 2007 Appendix F)
Serious adverse event: This term is specific to clinical research and involves and relates to any untoward medical occurrence in a subject (or child in utero) during clinical research involving a pharmaceutical product, medical device, or clinical intervention that:
1. is fatal
2. is life-threatening
3. requires hospitalisation or prolongation of existing hospitalisation
4. results in persistent or significant disability or incapacity
5. is manifested in a congenital anomaly or birth defect
Hazard: anything with the potential to cause harm Risk: The likelihood that the harm from one or more hazards is realised. UH Bristol Trust
Risk Management Strategy defines risk as a “hazard or exposure to danger or the chance of loss or harm”. (UH Bristol Trust Risk Management Strategy 2007 4.1)
Likelihood: see Appendix C for explanation of likelihood ratings used in UH Bristol Trust Near miss: a potential incident that was prevented but if allowed to progress would have
resulted in either a clinical or non-clinical incident Harm: see Appendix C for explanation of grading of actual harm used in UH Bristol Trust No harm: an incident that reached its full conclusion but caused no harm to the individual Grade or risk rating: see Appendix C for explanation of risk ratings used in UH Bristol
Trust Investigation: the relevant level of review of the events leading up to an incident to
determine what happened, to whom and why ie the root cause/s Risk reduction: the adoption of a risk based approach to the prevention of hazard,
mitigation of impact and response to reported incidents

7
Causal factors: the underlying elements which contributed to the incident. These have various classifications depending on the nature of the particular incident. See appendix H for examples of techniques
Table 1
Glossary of acronyms in frequent use in relation to incident investigations
ALARM Association of Litigation and Risk Managers
CEMACH Confidential Enquiry into Maternal and Child Health
CRAC Clinical Risk Assurance Committee
DoH Department of Health
EA Environment Agency
FT Foundation Trust
GMC General Medical Council
HCAI Healthcare Associated Infection
HPA Health Protection Agency
HPU Health Protection Unit.
HSE Health and Safety Executive
MHRA Medicines and Healthcare Products Regulatory Agency
MEMO Medical Equipment Management Organisation
NHSLA National Health Service Litigation Agency
NHS National Health Service
NRLS National Reporting and Learning System
NMC Nursing and Midwifery Council
NPSA National Patient Safety Agency
NRLS National Reporting and Learning System
PALS Patient Advice and Liaison Service
RCA Root Cause Analysis
RIDDOR Reporting of Injuries Diseases and Dangerous Occurrences Regulations (1995)
SHA Strategic Health Authority
SHoT Serious Hazards of Transfusion
8
4 Duties
Staff member/s directly involved in incident Appendix B Procedure for paper incident reporting • The reporting of incidents/accidents/ near misses is everyone’s responsibility. • All staff involved in an incident/accident/ near miss must ensure an Adverse Incident
form has been completed (Appendix A). • If medication incident/near miss has occurred, a Medication Error Monitoring
Proforma must also be completed (Appendix A) • Remove equipment and associated items from circulation if a fault suspected and
label • Retain disposable items involved with suspected defect. • The *form must be completed with a record of events only - NOT opinion. • Submit the completed *form to the department manager/deputy for grading without
delay, preferably on the day of the incident. • If the individual reporting the incident, is the clinician involved they may take the lead
in informing the patient of the event in accordance with the Being Open Policy (Appendix F).
• The form should not be filed in patients’ medical records • Incident reporting will be moving to an online process during 2009
* Forms must be available and accessible and identifiable to all staff in all departments/areas
Non UH Bristol Trust Employees Responsibilities
• Non-UH Bristol Trust employees (e.g. university students, agency staff) must comply with this policy and guidelines and should seek guidance from Trust employees.
4.2 Role of Line Manager (or Deputy) Assess and grade the degree of injury/harm/damage sustained using the risk matrix (Appendix C) • Assess and determine the risk, using the ‘likelihood of recurrence’ and ‘consequence’
tables; plot the outcome on the 5x5 matrix. • Calculate the ‘risk rating’ to determine the level of investigation to be undertaken • Forward all Adverse Incident forms to the Divisional General Office for data inputting
or Safety Department as appropriate. • Investigate ‘Very Low’ and ‘Low’ risk incidents and produce actions to prevent
future occurrences, recording them on the incident form. • Ensure that relevant individual managers/departments are notified and sent a copy of
the form in accordance with Section 9 on the form (Appendix A) • High Risk Incidents:
1. For Patient Safety Incidents notify the Divisional Patient Safety Advisor/Lead of ‘high risk’ incidents and ‘fast track’ (fax.) the form to the Medical Director, Director of Nursing and Trust Patient Safety Manager within 24 hours of identification of occurrence. Both the Central Executive Team and the Divisional Patient Safety Lead need to have prompt notification of such incidents. The Lead Clinician should also be informed at the earliest opportunity. Use of the High Risk Checklist Appendix A will assist in confirming the relevant people have been notified

9
2. Health and Safety (RIDDOR reportable) Incidents: Fast track (fax) non-clinical incidents within the RIDDOR category (Appendix A) to the Trust Safety department. Inform other relevant departments and organisations
• Refer to the Serious Untoward Clinical Incident Policy to determine whether this should be instigated and call the On-call Manager for advice. (Appendix F)
• Ensure that the patient and/or relatives (if appropriate) have been informed where harm has occurred in accordance with the Being Open Policy (Appendix F).
• Investigate ‘High’ (and relevant ‘Moderate’) risk incidents, in conjunction with senior Nurse/Matron/Doctor, Divisional Patient Safety Lead/Advisor, Health and Safety Advisor etc., as required.
• Provide supplementary reports as required, as part of the investigation (Appendix G writing statements)
• Staff must receive feedback– with positive learning and actions to prevent a recurrence.
4.3 Role of Senior Manager for Division For all incidents • Ensure adverse incident reporting forms are easily accessible and available to all
staff. • Ensure all staff are conversant with the use of the form and reporting process. • Ensure all department managers/ deputies understand the grading of incidents. • Discuss and provide feedback relating to all accidents/incidents at relevant Divisional
fora and an assurance report is provided to the Divisional Board on an agreed basis • Ensure action plans are completed within agreed timeframes
For non clinical incidents • Divisional Senior Managers (including senior clinicians) must ensure all non-clinical
related incidents and accidents are investigated and acted upon. Outcomes from these should be sent to the Safety Department within three weeks.
For patient safety incidents (usually delegated to Patient Safety Leads and Advisors)
• Ensure all patient safety incidents for the Division are entered onto the ‘Ulysses’
database by a designated individual, within 1 week of the notification of the incident and are updated with the conclusions of the completed incident investigation.
• Ensure ‘high-risk’ incidents are reviewed to establish the underlying root causes; this may require a root cause analysis and will include:
A detailed review of documentation Interviewing staff Obtaining written accounts of staff involvement (Appendix G) Identifying contributory factors (Appendix H) Making recommendations & action plan. Ensuring implementation of procedural changes and training is undertaken in
response to recommendations Agreed actions are reviewed and modified where necessary Where practicable that patients and parents of child patients receive some
feedback on the investigation outcome • Instigate the Serious Untoward Clinical Incident Policy where appropriate

10
• Staff must receive feedback – with positive learning and actions to prevent a recurrence. For high and moderate incidents, face to face feedback is essential.
• Ensure a quarterly incident report is prepared for the relevant Divisional Clinical Governance/Risk Management meeting.
• Provide assurance to the Divisional Board and Trust Clinical Risk Assurance Committee on patient safety within the Division.
• Ensure the Divisional Risk Register is updated with risks identified as a result of incident investigations and that the Register is reviewed regularly
• Oversee all patient safety activities and ensure training programmes are supported and staff are developed in the area of patient safety including use of the Ulysses database where relevant
• Promote a culture of patient safety within the Division including provision of feedback from incident investigations.
• Provide assistance to staff with patient safety incident investigations, which require a root cause analysis.
• If the patient safety incident involves more than one Division, the Divisional Patient Safety Lead or Advisor for the associated areas must agree a lead for the investigation.
• The Divisional Patient Safety Lead should undertake quarterly trend analysis for ‘Very Low’ and ‘Low’ incidents and advise Departments of local trends.
• Identification of relevant audits should arise from review of specific incidents and overall trends and changes in incident activity
4.4 Role of UH Bristol Trust risk manager/equivalent • The Trust Patient Safety Manager and Head of Health and Safety Services advise
and support the implementation of the policy. • The Patient Safety Manager will ensure all completed high risk patient safety incident
investigation reports are reviewed by the Clinical Risk Assurance Committee and that Divisions provide assurance of implementation of action plans.
• The Patient Safety Manager will ensure all patient safety incidents (anonymised) are reported to the NRLS at the NPSA on an agreed basis
• The Patient Safety Manager, or nominated deputy, will attend the monthly Trust Clinical Risk Assurance Committee (CRAC) in conjunction with the Divisional Patient Safety Leads to provide assurance on the appropriate investigation of high risk incidents. In addition the Patient Safety Manager will provide assurance to the Trust Governance and Risk Management Committee and CRAC on the quarterly trends and key learning from incident reporting and investigation (Appendix E External and Internal Stakeholders)
• The Trust Patient Safety Manager will ensure quarterly reports are prepared for the Trust Governance and Risk Management Committee from the Joint Working Group for review of incidents, claims and complaints
• The Head of Health and Safety Services will inform the HSE of reportable incidents and provide a summary report on request. The Head of Health & Safety Services will attend quarterly Trust Health and Safety Committee, providing feedback to the Board and Divisional Health & Safety Advisors. (Appendix E External and Internal Stakeholders)
• The Head of Health and Safety Services will attend quarterly Trust Governance & Risk Management Committee meetings. (Appendix E External and Internal Stakeholders)
4.5 Role of nominated director(s) including the non executive directors

11
Risk Management Strategy section 6 details roles and responsibilities of Directors including non executive directors. (Appendix F) The appointment of external investigators of serious incidents where deemed suitable. See also appendix E for internal and external stakeholders
4.6 Role of Chief Executive
As above
4.7 Role of Board
As above for responsibilities See Appendix E for External and Internal Stakeholders Board receives mins of Trust Governance and Risk Committee as assurance of review of all incident activity and detailed investigation of high risk incidents. Deaths attributed to system failure within the Trust could fall under the provisions of the Corporate Manslaughter Act.
4.8 Role of committee with the overarching responsibility for risk
management See Appendix 10 of Risk Management Strategy for Terms of Reference of Governance and Risk Management Committee (Appendix F)
4.9 Role of other committees/groups with responsibilities for incident
management The review of action plans arising from incident investigations lies with: • Clinical Divisions for all incidents arising in their area of responsibility • Clinical Risk Assurance Committee for patient safety incidents graded high risk
and overall incident activity (Appendix F) • Health and Safety Committee and Fire Safety Committee for non-clinical
incident activity and review of reportable incidents. (Appendix F)
5 Communication and Notification
See section 4 Duties for details of UH Bristol Trust expectations regarding the communication of incidents and near misses. See Appendices section for guidance on completion of incident reports, grading of incidents and notification of internal and external agencies. (Appendices A, B, C, D and E)
5.1 Patient/relative/visitor/contractor communication & support
All patients have the right to be informed that an untoward incident has taken place and clinicians and managers must make sure that they are informed. In the case of actual harm, this is essential. A record of discussions must be made in the patient’s notes.

12
UH Bristol Trust expectations and detailed guidance for communication with patients and others is provided in the Being Open Policy. This policy is based on guidance from the NPSA and refers explicitly to patients and relatives. The principles encompassed in this guidance are equally applicable to any visitor to UH Bristol Trust premises. Investigations of incidents involving individually appointed external investigators are made available on the Trust internet website. Examples include Toft Report (Heparin Flush incidents) and Gritten Report (cardiac perfusion) http://connect/Governance/patientsafety/Pages/PatientSafetyNews.aspx The Ulysses reporting system allows linkage between incidents, complaints and litigation enabling risk reduction and service improvement to be identified. Where appropriate, the Trust will seek views, of patients, Foundation Trust Members and other members of the public to reduce risks and improve patient safety.
5.2 Process by which to raise concerns UH Bristol Trust expectations and detailed guidance for communication of concerns about practice with an adverse impact on safety is available in the Human Resources policies on incident investigation and ‘speaking out’ (Appendix F) UH Bristol Trust expectations re feedback to staff following completed incident investigations see section 4 Duties. See Appendices section for guidance on feedback following incident investigations. (Appendices A, B, C, D and E) Further advice re the provision of support to staff following incidents is available in the Being Open Policy and related Human Resource policies for work related stress. (Appendix F)
5.3 Internal communication See section 4 Duties for details of the requirements for internal communication for all incidents Appendix E List of internal and external stakeholders
5.4 External stakeholder notification All patient safety incidents are reported (in an anonymised form) to the National Patient Safety Agency (NPSA) via the National Reporting and Learning System (NRLS). RIDDOR reportable incidents are reported to the Health and Safety Executive. (Appendices A, B and D) Incidents involving other health care providers must be referred to the relevant NHS Trust or provider. See Cross Organisational Incident Reporting Policy (Appendix F)
5.5 Media Involvement
Guidance on the provision of information to media representatives is available in the Serious Untoward Incident Policy and the Protocol for Media Enquiries (Appendix F)

13
The patient/staff member/relatives and others directly involved in the event eg contractors must be informed in advance of press publication. The media team provide advice and assistance to staff.
6 Incident Investigation Procedure
Reporting Patient Safety Incidents
• Complete an adverse incident report form (Appendix A) at the time or as soon as possible following detection (guidance, Appendix B)
• If medication incident/near miss has occurred, a Medication Error Monitoring Proforma must also be completed (Appendix A)
• Inform the patient and or relative of the incident where harm has occurred in accordance with the Being Open Policy; Document details in the patient’s notes
• To determine severity, a grading process will be applied and based upon several factors (details - Appendix C). The manager will undertake this process but this may include the need of a consensus from the multi-disciplinary team to assist in the grading.
• Fax ‘high risk’ incidents and ‘fast track’ the form to the Medical Director, Director of Nursing and Trust Patient Safety Manager within 24 hours of recognition of occurrence
• Online incident reporting will remove the need for this faxing procedure in pilot stage for implementation Autumn 2008
Externally Occurring Patient Safety Incidents
• Divisional Managers/Patient Safety Leads will notify the originating hospital (preferably the corresponding patient safety manager) if it is clear that a patient referred to UH Bristol Trust suffered harm in another organisation
• The Manager will seek the support of the Trust Patient Safety Manager if this is proving difficult.
• The Manager will agree the reporting and investigation actions with the external organisation
• It is expected that the originating hospital will provide feedback to the Trust and where necessary, the Trust will liaise and assist in any investigation with a joint review to prevent a recurrence
• Likewise, if an incident originated in UH Bristol Trust and is reported by another organisation, the relevant department in UH Bristol Trust will investigate the incident, liaising with the Trust Patient Safety Manager and arrangement will be made to provide feedback to the reporting organisation. See cross organisation incident guidance (Appendix F)
Reporting non-clinical Accidents/Incidents. • Appendix A and D provides guidance for reporting of RIDDOR reportable incidents Reporting claims and complaints • Appendix F for details of separate procedures for complaints (including PALS
enquiries) • Appendix F for details of separate procedure for claims handling • The monitoring of learning arising from review of complaints claims and incidents is
carried out by the Joint Working Group and Trust Governance and Risk Management Committee (Appendix E Internal and External Stakeholders)

14
6.1 Incident grading and appropriate levels of investigations
See Appendices A, B, C and H for guidance in determining appropriate level of incident investigation. At the conclusion of the incident investigation it may be necessary to review the original grading. Identified risks should be reported and logged on the relevant Risk Register
6.2 Responsibility for investigation See section 4 Duties for details of staff responsibilities for investigation of incidents. Staff must be suitably prepared for this responsibility. Details of the training for all staff is available in the Training Needs Analysis section of the Trust Annual Training Plan and the Risk Management Strategy Appendix F All staff will receive training in the importance of incident reporting and their responsibility to inform the organisation of any adverse incidents or accidents on Trust property.
Basic training will be provided within the general induction programme and statutory update training days. Further staff development can be provided on request to the Patient Safety and Health and Safety Departments
Health and Safety representatives will receive basic training and updating through the Trust Health and Safety Department.
Root Cause Analysis training will be provided for all Divisional Patient Safety Leads/Advisors, supported by the Patient Safety Team and intranet website.
Divisional Patient Safety Leads and Advisors will support this training programme by referral of departmental managers and other relevant staff as required. Local initiatives in training should be developed within Divisions but also in conjunction with the central Patient Safety Team
6.3 Root Cause Analysis See Patient Safety intranet site and (Appendix) for tools to assist with RCA investigations. Some key points:
Investigations will require the support of an individual familiar with RCA techniques All suspected faulty equipment MUST be withdrawn from circulation and labelled; it must NOT be tampered with. This may affect the investigation.
Suspected faulty disposable items must be retained for inspection.
Once care management problems have been identified and agreed, contributory factors need to be explored, focusing upon systems and processes - not individuals - which possibly led to the occurrence. A cause and effect chart may assist in identifying contributory factors. (Appendix H) provides a checklist to ensure all possible factors have been considered.
If an individual’s actions or conduct are identified as a significant factor influencing the course of an incident, managers should refer to the Incident Decision Tree3 to apply a standardised assessment of those actions
3 Incident Decision Tree 2005 (NPSA) http://connect/Governance/patientsafety/Pages/default.aspx

15
A first draft of the report should be circulated to all staff involved in the incident for comment. Include key staff who will be involved in the implementation of recommendations and improvement strategies. Completed reports are anonymised, but a numerical reference will be provided to allow tracking of the incident on the Ulysses database system. For clinical incidents, the synopsis Investigation Report Template should be used (example – Appendix H) and considered for inclusion in the Clinical Risk Assurance Committee report where a full RCA investigation has been carried out to inform committee members
Some incidents will cross departments and Divisions and in such cases the Patient Safety lead must refer to the relevant individual to discuss the incident and agree who will lead the investigation. All Divisions must be fully involved, be kept informed of the investigation and provided with sharing learning. Catastrophic incidents All incidents graded as causing ‘catastrophic harm’ and high risk rated incidents may need to be considered for reporting and investigation under the principles of the Serious Untoward Incident Policy (Appendix F)
An incident of this nature is defined as –
‘……… an event which is likely to produce significant legal, media or other interest which, if not properly managed, may result in loss of the Trust’s reputation and assets…’
The key determination in relation to patient death is whether the death was avoidable or unavoidable. An example would be a patient who dies in the immediate peri-operative period. This may be an unavoidable death however the details will need to be reviewed by the clinical team to determine if any incident investigation is required. Advice may need to be be sought from the patient safety lead for the Division or central patient safety team.
6.4 Recommendations and action planning
See section 4 Duties for details of who should be involved in the identification of actions arising from incident investigations. Local Actions Actions must be identified locally within the Division following the incident investigation. Staff must receive feedback from the findings of the investigation. This provides individual/s with an outcome and enables learning from errors. For very low and low incidents the staff should receive positive verbal sharing of learning, which involves a scrutiny of systems and processes in an environment of fair blame. For the individuals directly involved in moderate and high incidents, face to face supportive feedback is important.
Cross Divisional and Trust-wide actions including externally to UH Bristol Trust Wider learning from incidents should be shared across divisions via newsletters/team briefs; those with trust wide implications should be sent to the Patient Safety Manager/THSA for inclusion in Trust media. Actions of Trust-wide implication may need to be referred to the relevant Corporate Committee for approval. The audit or onward monitoring of changes in practice must be included in this process.

16
An Annual Report will be submitted to the Trust Board via the Governance and Risk Management Committee.
6.5 Monitoring of action plans Agreed actions must be implemented within the Division where the incident originated and in other Divisions where relevant. The non implementation or partial implementation of agreed actions will need to be reported (with reasons) on the Divisional Risk Register and reviewed via the local Governance Group. Actions requiring formal review for effectiveness may be subject to local audits and reported via the same mechanism.
Implementation of agreed actions will be reviewed by the Trust Governance and Risk Management Committee in conjunction with the Divisional Managers on a rota basis. An audit will be completed to confirm compliance with this process. Divisional Patient Safety Leads report to CRAC on patient safety matters of relevance including the implementation and review of agreed actions arising from incident investigations. Divisional Health and Safety Leads report to their Divisional Board and Health and Safety Fora on non clinical matters of relevance.
6.6 Process of ensuring continual risk reduction following the implementation of action plans The ongoing monitoring of risk reduction measures via review of incident action plans, risk registers and audit reports will reduce the likelihood of inadvertent transfer of a known risk or development of a new risk. However all staff involved in reviewing risks both locally and Trust-wide should keep this possibility in mind. Tracking and trending incident activity will assist with this.
6.7 Involvement of relevant stakeholders Where there is a legal requirement or where it is considered advisable to refer an incident to an external agency advice should be sought from the following UH Bristol Trust departments by those investigating the incident in conjunction with the relevant manager. See (Appendix E) for full list
6.8 Sharing of lessons learnt See section 6.4 and section 4 Duties for details of the expectations regarding feedback on incident investigations. From a systematic review of reported incidents and the sharing and implementation of risk reduction measures the aim is to reduced the number of high risk incidents occurring in UH Bristol Trust on a year by year basis. Specific objectives for patient safety incidents are detailed in the Trust Patient Safety Strategy 4 The review of incident activity and learning with neighbouring Trusts is encouraged via individual contacts and meetings including:
• Attendance of Trust Patient Safety Manager at meetings with the Avon, Gloucestershire and Wiltshire Risk Managers Forum (renamed as Patient Safety Network)
4 UHB TRUST and North Bristol NHS Trusts involvement in the Safer Patient Initiative which aims to achieve a 10% annual incident reduction figure.

17
• Attendance at the national Association of Healthcare Safety and Risk Practitioners by the Head of Health and Safety
7 Incident & Causal Factor Analysis
7.1 Responsibility for incident analysis
See section 4 duties and (Appendix E) committee map for details of which staff are responsible for the analysis and reporting of incidents. The reported analysis of incidents should include details on the following however not all reports will require all these areas to be covered. It depends on the specific purpose of the report and the audience:
• Incident activity • Incident grading • Incident investigation findings for high risk incidents • Proposed actions for risk reduction • Trends or new hazards • Time and date of incident activity • Repeat or persistent incident themes • Training, budgetary and changes in professional practice implications
7.2 Responsibility for causal factor analysis post investigation
See section 4 Duties for details of which staff are responsible for the identification of trends. See (Appendix H) incident investigation techniques, for details of tools to assist with review of a series of incidents especially those graded as high risk. From these incident investigations it is possible that a number of causal factors will emerge which will have implications for practice and training. These are to be identified locally initially but where relevant Trust-wide or across Divisions, the details must be shared. Basic graphical depiction of incident trends and activity is provided monthly in relation to patient safety incidents. See CRAC intranet site or Divisional Patient Safety Leads for reports. All Health and Safety Committee and CRAC Incident Reports are presented to the Governance and Risk Management Committee on a quarterly basis. See Appendix E (Internal and External Stakeholders).
8 Hotline Arrangements
For incidents which meet the classification of a Serious Untoward Incident (see 6.3 for definition) there will be a need to ensure the correct notification of affected people whether staff members, trust visitors or patients. Full details of hotline arrangements are included in the SUI Policy (Appendix F). The policy provides guidance on the following: 8.1 Management responsibility 8.2 Phone lines 8.3 Staffing 8.4 Capacity to manage calls over time 8.5 Documentation 8.6 Record keeping 8.7 IT and postal arrangements

9 Process for monitoring the effectiveness of; the organisational wide policy for the management of incidents NHSLA Requirement Policy Reference What is the Evidence Who Reviews the
Evidence and Frequency
Who Prepares the Evidence
Duties patient safety (clinical) incidents
Section 4 1. Div Incident Reports 2. CRAC Monthly High Risk and 1/4rly overall incident activity 3. CRAC 1/4rly report 4. Mins Gov and RM Committee
Divisional Board or Gov Committee at least 1/4rly CRAC Gov and RM Committee 1/4rly Trust Board 1/4rly
Divisional PS Lead/Advisor Trust PS Team Trust PS Team Chair Gov and RM Committee
Duties non patient safety incidents
Section 4 1. Quarterly and annual trust overview 2. Div 1/4rly reports
Trust H&S Committee Divisional Boards
Health & Safety Team Div H&S Leads
Process for reporting patient safety incidents
Section 4, 6 and Appendices + Serious Untoward Incident Policy
1. Activity Reports as detailed above 2. Serious Untoward Incident Report 3. Internal Audits of elements of incident reporting
See above Gov and RM Committee CRAC alternate years
See above Chief Nurse Internal Audit Team
Process for reporting non clinical incidents
Section 4, 6 and Appendices 1. As above for clinical 2. RIDDOR report 3. As above
Process for reporting clinical incidents to external agencies
Section 5.4 and Appendix E and F
1. NPSA Extranet Report review 2. Serious Untoward Incident report
CRAC 6 monthly Gov and RM Committee
Informatics Senior Nurse Chief Nurse
Process for reporting non clinical incidents to external agencies
Section 5.4 and Appendix E Completion of HSE RIDDOR report-F2508
Trust H&S Committee Gov and RM Committee
Health and Safety Team
Process for staff to raise concerns
Section 5.2 and Appendix F Report Grievance and Disciplinary cases Harassment and Bullying Report
Monthly Div HR Manager Corporate HR Manager

10 Dissemination, Implementation and Access to this Document
This Policy and all the linked Policies are available on the UH Bristol Trust intranet via the Document Management System and subject to a regular review procedure. Reporting and investigation of incidents is included in the UH Bristol Trust Corporate Induction Programme for all new permanent members of staff. Update training is also provided. Training on additional incident investigation techniques are detailed in the UH Bristol Trust Training Plan.
11 Review, Updating and Archiving of this Document
This Policy is archived on the Document Management System and subject to a 3 yearly review. UH Bristol Trust is moving to an online incident reporting process in 2009 and the Policy will be reviewed to reflect this change.
12 References 1. National Patient Safety Agency (NPSA) Seven Steps to Patient Safety. The full reference guide.
Available at www.npsa.nhs.uk/sevensteps April 2004 2. Health and Safety Executive (HSE) The Reporting of Injuries, Diseases and Dangerous Occurrences
Regulations 1995 (RIDDOR), HSE Books.

20
Appendices Appendix A Incident Reporting
Incident reporting form
Guidance for managers re completion and communication
RIDDOR incidents
• Flow Chart
• Example
Further details required for medication incidents
Appendix B Guide to incident form completion
Appendix C Incident Investigation
Risk matrix
Manager’s guide to grading
Manager’s guide to investigation of high risk incidents
Appendix D Example list of reportable incidents Clinical and Non clinical
Required RIDDOR reportable incidents
Appendix E List of internal and external stakeholders
Internal groups and committees + electronic links
External bodies
Appendix F List of associated UH Bristol Trust policies and electronic links
Appendix G Guidance on writing statements for incident investigations
Appendix H Incident investigation techniques
Gathering information ‘5 Whys’
Mapping of contributory factors ‘Fishbone’
NPSA, ALARM and RIDDOR examples of contributory factors
NPSA incident decision tree
Incident investigation report template

21
Appendix A

22

23
Division of ……………………………… High Risk Patient Safety Incident Checklist
Incident number:
Named Lead Professional:
Incident detail:
Actual Harm:
RCA needed: If not - why
Nominated RCA Lead:
Time frame to review incident:
Who is responsible for communicating with family/patient
On call Supervisor of Midwives: Senior Nurse: Named Consultant: Assistant Divisional Manager:
Debriefing for staff:
Patient Safety Advisor: Staff offered ongoing support
Occupational health Supervision Senior Nurse Education Supervisor
Agreed by:

24
Adverse Incident/Near Miss Report Forms: Instructions for Manager
Please print all details clearly and complete all relevant sections Record only known facts – do not record opinions. Please ensure any equipment involved should be retained in safe keeping for examination and not used until deemed safe to do so. Section 8. Type of incident Please indicate if you think this incident is either a clinical μ, non-clinical or near miss ( clinical)μ / (non-clinical) . If non-clinical or near miss non-clincial please indicate the type by ticking the relevant box in this section. For clincial incidents/near misses please refer to the trigger list for the list of clinical incident codes. Please enter the most appropriate code onto the form which best desribes the nature of the incident. Section 9. Notifying Others Medical equipment – refers to any equipment used in support of patients &/or their treatment (including wheel
chairs and other mobility aids). Please tick this section if any medical equipment was involved in the incident/near miss. Please ensure this is retained for inspection. Please also record the MEMO number on the incident form.
Drug Errors – Where possible please indicate if the error related to either the prescribing, dispensing, administartion or some other aspect. Please complete the supplementary drug investigation form when investigating any drug related incidents.
Section 10. Injury or Ill Health Please complete this section if the person involved in the incident suffered any harm or ill health. If the injured person is a memebr of staff please ensure the Health & Safety department are fully informed. Please refer to the Incident Reporting Policy and Guidelines, for advice on: needlestick or sharps injury; Radiation related incidents; security related incidents; dangerous occurrences or major injury or death at work (see flow chart below). If no injury or ill health was suffered please move directly to section 4. Section 11. Grading Process and Classifcation of Risk All incidents, regardless of type must be graded and risk assessed using the risk matrix (Appendix C) for guidance. Section 12. Action taken to minimise the chance of a recurrence of this accident/incident Please ensure that all immediate actions to safe guard the indivdiual/area have taken place i.e. obtaining medical aid if required, closing affected areas if necessary, calling for outside assistance e.g. fire brigade. Once the incident has been graded and risk assessed an investigation should be carried out appropriate to the level of risk identified i.e. very low, low, moderate or high. For very low and low incidents the investigation should be undertaken by the ward/line/department manager or their deputy and completed within seven days. The actions arising from the investigation should be recorded on the incident form and sent to the Divisional Patient Safety Lead/Health & Safety dept (as appropriate). For moderate incidents, a more detailed investigation is required, with the written report being shared within the Division and where relevant eg affects more than 1 Division a copy sent to the Trust Patient Safety Manager or Health & Safety Advisor (as appropriate). For all major patient safety (clinical) incidents a full and detailed investigation needs to be undertaken. The Senior Manager on duty should be informed and where appropriate the Executive on Call should be informed. Where necessary guidance should be sought from the Serious Untoward Incident Policy. A copy of the form must be faxed immediately to the Trust Patient Safety Manager. A team of people should be appointed to investigate the incident lead by an individual who is familiar with the Root Cause Analysis techniques (Appendix H). The written report, including recommendations and improvements strategies, should be submitted to the Trust Patient Safety Manager within 8 weeks of the incident date. Major non-clincial incidents/accidents - namely any major injury or death and any dangerous occurrences, are classed as reportable incidents and should be reported to the HSE. For further details of these see the flow diagram on ‘Reportable incidents’ (Appendix D). When a reportable incident occurs, whether to a member of staff, a patient, visitor or anyone else, the Trust Health & Safety Adviser should be informed immediately so that they can contact the HSE. On receipt of the incident form the Safety dept will instigate a full and detailed

25
investigation using Trustwide templates. The written report of the investigation needs to be submitted within 2 weeks of the investigation being instigated and forwarded to the Safety Dept. Sharing learning It is important to act on all incidents as soon as they occur. The majority of incidents will be of a minor nature and actions maybe minimal. However, all incidents warrant a review and feedbackto the member of staff that highlighted the incident in the first place. This can either be in the form of verbal discussions only, a group meeting for those involved or possibly a detailed written report which is made avaible to all involved as well as other interested parties. Please ensure staff are made aware of what to expect the regard to the type of feedbackanticipated. Section 3(CONT.) – Guidance for Managing Injury or Ill Health
Send details of action taken to Directorate Data Inputter for entering on to Ulysses Safeguard System
IF THE INCIDENT FALLS INTO ANY OF THE FOLLOWING CATEGORIES PLEASE ENSURE THE ACTION
Needle-stick or Sharps Injury
Radiation Related Incident
Security Related Incident (including assault)
Major Injury or Death
Dangerous Occurrence
Staff: Ensure injured person has contacted UHB TRUST Needlestick Hotline
Tel: 928 4987 or contact BRI switchboard for on-call
out of hours service Patients/Visitors: Refer to
UHB TRUST Infection Control Manual section
2.12 Action in the Event of a Contamination Injury
Inform the Radiation Protection Supervisor
immediately (as per UHB TRUST
Radiation Safety Policy)
Inform UH Bristol Trust Security Service
immediately
Inform available Senior Manager immediately
Person reporting or Senior Manager to report to UH Bristol Trust H&S Adviser immediately
UH Bristol Trust H&S Adviser to ensure incident reported to Health &
Safety Executive under RIDDOR
Copy of F2508 sent to Divisional Human Resources Department/Ward Manager and also attached to Incident Accident Notification Form
Details of RIDDOR entered onto Ulysses Safeguard System by Safety
Department

26
Managers flow chart for reporting of injuries, disease & dangerous occurrence regulations (RIDDOR) STEP 1
A If a RIDDOR type injury has occurred, collect statements from injured person and/or witnesses as soon as possible. If injured person or witness is a member of staff or patient from another department or ward, statements should be requested via the appropriate manager.
B Inspect incident area as soon as possible for any contributing factors such as surface conditions, obstacles, tripping hazards, lighting , work activities & loads. Faulty equipment etc should be kept for inspection.
STEP 2
Collect the requested documentation. This may include training records, risk assessments, written systems of work, patient information & staffing levels etc. Include any additional information/evidence such as CCTV footage or description of equipment.
Step 3 Use all the collected information to write a factual report of the findings & identify the root cause of the incident. Contact the Divisonal Health & Safety Lead or Advisor for support/advice as needed.
STEP 4
Detail the action taken to prevent an incident of a similar nature occurring to other staff/persons. This could include action taken within the ward/department, other wards/departments or other Divisions.
STEP 5
Ensure all the requested documentation has been included and return to the safety department by the requested date.
STEP 6
If feedback of formal report is indicated e.g. for patient / visitor related incidents, the appropriate General Manager should be identified early in the investigation stages. For further detail & advice please access Adverse Incident Reporting Policy & Guidelines

27
ADVERSE INCIDENT INVESTIGATION
&
ROOT CAUSE ANALYSIS
EXAMPLE SSaaffeettyy DDeeppaarrttmmeenntt, Level 5 Education Centre, Bristol
INCIDENT NUMBER: ##### BS2 8AE
TEL 0117 342 0139
FAX 0117 342 0135
DATE: 20/05/08 E-MAIL: [email protected]
Re: Investigation under RIDDOR (Reporting of Injuries Diseases and Dangerous Occurrences Regulations 1995) For: A. Nurse To: A. Manager • Date of incident: 01/05/08 • Date received: 20/05/08 • Nature of Incident: Injured whilst moving a patient • Reporting Time delay: 19 days
N.B The required time limit for reporting incidents to the Health and Safety Executive is 10 days. Non compliance is an organisational risk and may invite departmental scrutiny.
As manager of your department, would you please complete an investigation in order to help to identify the root cause of the attached adverse incident. To be returned to the Safety Department by……10/06/08………………… Please identify the measures needed to avoid future incidents of a similar nature. Statements A detailed description of the incident by the injured person(s) and any witness statements are required.

28
Wherever possible these statements should be written and signed by the people named in the incidents using their own wording. Statement Content This should include an account of the facts as they recall them, and may include any issues they consider relevant to the cause of the incident. All the information collected in this post-injury investigation can/may be submitted in a court of law. Additional information Generic / specific risk assessments, safe systems of work, guidelines, procedures and related incident information should be included as requested. Guidance For additional information refer to your IOSH folder, module 1, and /or contact your Divisional Health and Safety
Advisor (site/service) or the Safety Department.
I look forward to receiving your report by the above date.
A printed copy with a copy of the adverse incident form will be forwarded to you by post.
Kind regards
Janice Kopf Manual Handling & Ergonomics Advisor
For details of “Accident Investigation, Training for Mangers” please refer to the Training & Development website.

29
RIDDOR INVESTIGATION FORM
Please complete and return to the Safety Department by: 10/06/08
Incident Number: #####
NAME
POST Date and name of last relevant training eg H&S, Manual Handling
Injured person
A. Nurse Nursing Assistant
Clinical Governance Update 12/12/07
Manager (deputy) completing form
A. Manager
Ward Manager
Please attach a copy of the marked documents relating to this incident: Risk Assessment(s):
Generic Manual Handling (MH) Lone working Violence &Aggression (V&A) VDU Fire Pregnancy COSHH
Other documentation Local procedure/system of work
for task Staffing levels Skill mix details Patient Mobility Assessment Patient weight:
Total sickness absence = 2 Weeks
Description of incident by: Injured person Witness statements
Description of: Equipment used Environment Personal Protective Equipment
Ward/Dept Manager A. Manager cc Division H&S Lead E.g. S,H&N Manager cc Division H&S Advisor E.g. S,H&N Advisor cc Senior Nurse/ Matron E.g. S,H&N Matron

30
Managers report of Investigation Findings details of remedial actions should be completed overleaf: The incident occurred at 14.30 on Thursday 1st May. A. Nurse had stood the patient up from the chair, to use the Zimmer frame, when the patient’s legs gave way. A. Nurse tried to catch the patient to prevent her falling, and twisted awkwardly injuring her lower back in the process. The patient did manage to fall back into the chair and sustained no injury. The patient had had a stroke in February and does suffer some confusion at times so would not be a reliable witness; however the incident was witnessed by a domestic A. HSA. (see witness report) A. Nurse was signed off sick by her G.P. for two weeks with analgesia. She is to attend Physio Direct for advice and treatment as required. A. Nurse had had been updated in all Statutory training in December 07. She had referred to the patient mobility assessment and followed the instructions, but the patient was not feeling as well as normal due to an Urinary Tract Infection, so the assessment should have been updated. Staffing levels were appropriate for the Late shift. Documents enclosed; Patient Mobility assessment, Description of incident by A. Nurse and A. HSA. Patient Handover record for dates surrounding the incident Staffing levels plan for the April / May period
Identify contributory factors and add relevant comment on incident cause (remedial action to be stated below)
Communication Education & Training Equipment & resources Medication Patient factors e.g. clinical condition
Risk assessment not completed Safe system of work not identified Safe system of work not followed
Task factors Team & social factors Work & environment Staffing levels Organisation & strategic Unknown Other (please include in details below)
Identify which of the following actions will remove or reduce risk of further similar incidents
Perform risk assessment of specific task/area Review existing risk assessment Complete Patient Mobility Assessment Update existing Patient Mobility Assessment Introduce local procedure (documented) Update written instructions / local procedures Make environmental improvements Redesign task Provide or replace necessary equipment
Provide training or additional training Increase number of staff performing task Spread tasks throughout day Rotate staff performing task Increase supervision of staff / staff group Refer staff to Occupational Health for residual problems Routine monitoring of practice in department or area Other (please include in details below)

31
Detail of action taken to prevent incident of a similar nature occurring again: All staff reminded of the importance of on the spot reassessment and the updating of the mobility assessment in the event of change in patient’s condition, so it can be used as an effective tool and to prevent this type of incident. Weekly monitoring of assessments in place Monthly ward team meetings to ensure risk awareness and compliance with safe systems. Mandatory training monitored and linked to appraisals.
Please attach a copy of revised risk assessment or procedures. A copy of this report should be retained locally
Managers signature:
A. Manager A Manager
Date:
20/05/08
Received by Safety Department Signature: Post: Date:
Comments

32
Medication Error Monitoring Proforma.
Investigating + Classifying Medication Related Patient Safety Incidents To be completed by managers when investigating medication errors as type of error and process error are mandatory fields when entering details onto Ulysses database. Please tick the relevant box for type and process error and complete the drug details
Type of Error Example
Contraindication to the use of the medicine
asthmatic prescribed + given β-blocker
Failure of clinical assessment equipment
Incorrect insulin dose as problems with blood glucose monitoring
Failure to order a lab test Pt on Warfarin + INR not requested
Failure to refer to hospital follow up Pt on Warfarin and referral not sent to anticoagulation clinic
Infusion relate Could be any route eg sc/iv
Interaction E.g. Phenytoin + Amiodarone
Omitted medicine or ingredient Pt did not receive drug
Omitted signature of healthcare practitioner
Drug given twice as no record of being given
Other Incident error type does not fit any other listed type of error
Patient allergy Pt prescribed Amoxil + charted as penicillin allergic
Unknown Details of error not known
Wrong dose Pt prescribed 10mg but takes 5mg
Wrong formulation On Epilim Chrono and Epilim supplied
Wrong medicine/drug Atarax dispensed instead of Atenolol
Wrong medicines label Label for Frusemide 250mg but prescribed 40mg
Wrong method of preparation or supply
5 Fluorouracil supplied as syringe when infusion prescribed
Wrong patient
Wrong patient directions Label has wrong quantity to take
Wrong quantity 1x100ml Methadone ordered 2 x100ml supplied
Wrong route Drug given iv when should be i.m.
Wrong storage Fridge item kept at room temp

33
Appendix B - Guide to incident form completion
The Trust wide reporting form (Appendix A), must be used by all staff, to report all accidents and incidents occurring throughout the UH Bristol Trust organisation and submitted to the department manager/deputy5 for grading and risk assessment. Complete the form recording FACT ONLY and not opinion. Anonymity will be respected; however for an effective investigation, a signature is preferable. Writing must be clear and legible, with printing used where requested on the form.
5 The term ‘department manager/deputy’ refers to the Department Head/Ward Manager/Sister/Charge Nurse/Line Manager as appropriate or deputy in their absence who ever is responsible for the area. This term will be used throughout this policy.
If categorised as a High Incident complete the form and fax immediately to THQ and consider the Serious Incident
Reporting Policy & Procedure Requirements.
Personal Details – of all those involved and status e.g. staff, patient, ethnicity etc.
Describe incident, stating fact only - not opinions. Continue on a separate sheet and attach to form if
required; complete medication error monitoring proforma, for medication errors and attach to form
Immediate Action – describe type of action taken. For patient related incidents the attending doctor needs to complete this section.
Witnesses – Record name and addresses. For staff include designation and area of work.
Record your name, designation, date and signature. If anonymity is preferred you may omit this, but date the
form.
Submit completed form to the person in charge on that day to allow for immediate grading and classification of the incident.
Time and Place - state when and where incident occurred. Provide as much information as possible.
Section 1
Section 2
Sections 3 & 4
Section 6.
Section 7.
Section 5.
Once completed

34
Appendix C - Risk matrix
Definitions for Impact/Consequence (actual and potential) and likelihood of recurrence
DESCRIPTOR Actual or potential impact on the
individual Actual or potential impact
on the organisation Number of
persons affected
Catastrophic
Death (Unexpected)
Suicide/Homicide
Major Fire
Litigation expected (Inter)National adverse publicity. Disastrous failure of quality of patient services. Huge financial losses. Criminal prosecutions
Many > 50 e.g. screening errors.
MAJOR
Major Permanent injury/damage e.g. Wrong body part/wrong patient procedures Haemolytic transfusion reaction Retained instrument/other material after surgery requiring re-operation Patient receiving a radiation dose greater or less than prescribed Loss of sight or limb. Exposure to hazardous substance resulting in occupational asthma.
Litigation expected National adverse publicity. Major effect on quality of patient services. Major financial losses. Increased length of stay and/or level of care >15 days. H&S Exec investigation.
16-50 e.g. Lost
specimens
MODERATE
Semi- permanent harm/ damage (up to 1 Year to resolve)
E.g. Tissue damage from drug error, back injury
Litigation possible Local adverse publicity. Big effect on quality of patient services. High financial losses Increased length of stay and/or level of care >8-15 days
3-15 e.g. Violent
incident in A&E
Minor
Non-permanent harm/ damage (resolved < 1 month)
E.g. Inadequate care due to unsafe staffing level, slip on wet floor resulting in sprained ankle.
Litigation unlikely. Low risk of complaint Moderate effect on quality of patient services. Increased length of stay and/or level of care <1-7 days
1-2
None No obvious harm/damage Minimal impact, no service disruption, no financial loss N/A
Definitions for Impact/Consequence (actual or potential)
Likelihood Rating
Description
Almost Certain
Will undoubtedly recur, possibly frequently
Likely
Will probably recur, but it is not a persistent issue
Possible
May recur occasionally
Unlikely
Do not expect it to happen again but it is possible
Rare Can’t believe this will ever happen again

35
Step By Step To Grading Harm And Impact – Managers Guide
Step 1: Assess likely consequence of a recurrence See previous page as a guide. In the event of uncertainty, obtain a consensus view and plot against Table 1 Step 2: Grade likelihood of recurrence. See previous page to assess the likelihood of a repetition. This will depend upon the knowledge and expertise of the assessor. In the event of uncertainty, obtain a consensus view; plot against Table 1.
Risk:
Very Low
Low Moderate High
Table 1 Step 3: Plot Risk Rating
Using the 5 x 5 matrix (Table 1) the risk rating can now be identified (Table 2)
Risk Rating: Very Low Low Moderate High
Table 2 Step 4: Grade actual impact Assess the actual harm/damage or apparent outcome of the incident upon the individual or Trust property. Use Table 3 to grade the incident under the following categories;
Table 3.
Major Moderate Catastrophic Minor Insignificant
Likelihood CONSEQUENCE None Minor Moderate Major Catastrop
hiAlmost
Likely
Possible
Unlikely
Rare
36
Investigation of Incidents graded as High Risk (and some Moderate)
1. All incidents graded ‘catastrophic harm’ and high risk rated incidents may need to be considered under the Serious Untoward Clinical Incident Policy (Appendix F) See definitions section 3
2. Investigations may require the support of an individual familiar with RCA techniques (Appendix H).
3. All suspected faulty equipment MUST be withdrawn from circulation and labelled; it must NOT be tampered with. This may affect the investigation.
4. Suspected faulty disposable items must be retained for inspection.
5. Once care management problems have been identified and agreed, contributory factors need to be explored, focusing upon systems and processes - not individuals - which possibly led to the occurrence. A cause and effect chart may assist in identifying contributory factors. (Appendix H) provides a checklist to ensure all possible factors have been considered.
6. If an individual’s actions or conduct are identified as a significant factor influencing the course of an incident, managers should refer to the Incident Decision Tree to apply a standardised assessment of those actions (NPSA link - http://www.msnpsa.nhs.uk/idt2/(p0ompevfcz0rrc4534ukn1qe)/decision_tree9j.aspx?JS=1 (Appendix F)
7. A first draft of the report should be circulated to all staff involved in the incident for comment. Include key staff who will be involved in the implementation of recommendations and improvement strategies.
8. Reports are anonymised, but a numerical reference will be provided to allow tracking of the
incident on the Ulysses database system. For clinical incidents, the synopsis Proforma should be used (example – Appendix H) and submitted for inclusion in the Division’s feedbackto the Clinical Risk Assurance Committee.
9. Some incidents will cross departments and Divisions and in such cases the Divisional Patient
Safety Lead must refer to the relevant individual to discuss the incident and agree who will lead the investigation. All Divisions must be fully involved, be kept informed of the investigation and provided with sharing learning.

37
Appendix D - List of reportable incidents (including those which will be deemed serious)
Examples of Clinical and Non-Clinical Incidents
CLINICAL INCIDENTS Patients ONLY
• Drug errors • Treatments incorrectly applied • Prescribed treatment not given • Patient slip causing fracture, resulting
from incorrect mobilisation technique or assessment
• Misdiagnosis • Swabs left in patient following surgery • Preventable reactions to drugs • Clinical equipment failure with
consequences for patients’ treatment, e.g. X-ray machine errors
• Wrong calibration of radiotherapy equipment
• Hospital acquired infections • Blood transfusion errors • Still births • Neonatal deaths • Unexpected return to theatre • Unexpected post-operative death
within • hospital • Hospital re-admissions within 28 days • Irradiation of pregnant patient • Unexpected admission to intensive
care • Unexpected poor outcome • Accidental trauma • Inappropriate delay/cancellation of
treatment • Unsafe number of members of staff • Wrong body part operated on • Wrong patient operated on
NON-CLINICAL INCIDENTS
• Falls downstairs • Falls out of bed • Slips on wet floors • Patients hitting their head on
equipment etc • Non-clinical equipment failure, e.g.
tables, chairs • Burns/scalds from hot water or pipes • Fire conditions • Damage or loss of property • Violence towards anybody • Accident to patient’s visitors
REPORTABLE INCIDENTS (NON CLINICAL)
Certain incidents are reportable to the Health & Safety Executive (HSE) under the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995 (RIDDOR). The following types of incident are reportable: Major Injury or Death arising out of or in connection with work: -
Any death as a result of an accident Any fracture other than to fingers, thumbs or toes Any amputation Either of the following conditions result from the absorption of any substance by inhalation, ingestion or Dislocation
of the shoulder, hip, knee or spine Loss of sight (whether temporary or permanent) A chemical or hot metal burn to the eye or any penetrating injury to the eye Any injury resulting from an electric shock or electrical burn leading to unconsciousness or requiring resuscitation or
admittance to hospital for more than 24 hours Any other injury –
Leading to hypothermia, heat-induced illness or unconsciousness Requiring resuscitation, or Requiring admittance to hospital for more than 24 hours
Loss of consciousness caused by asphyxia or by exposure to a harmful substance or biological agent Either of the following conditions result from the absorption of any substance by inhalation, ingestion or through the
skin – Acute illness requiring medical treatment Loss of consciousness
Acute illness which requires medical treatment where there is reason to believe that this resulted from exposure to a biological agent or its toxins or infected material
The above includes: incidents involving patients & other persons not at work on healthcare premises Violence to staff resulting in any of the above
4-Day-or-More-Injuries:- Any injury to anyone at work resulting in them not being able to carry out their normal duties for 4 consecutive days
or more (including days off but excluding the day of the accident)
Dangerous Occurrences:- The collapse of, overturning, or failure of any load-bearing part of any lifting machinery (including patient hoists) The failure of any pressure system and associated pipe work Electrical short circuit or overload along with fire or explosion resulting in the stoppage of plant involved for 24 hours
or more or which has the potential to cause death to any person Any incident which resulted or could have resulted in the release or escape of a biological agent likely to cause
severe human infection or illness (in Hazard Groups 3 or 4) Malfunction of radiation generators Malfunction of breathing apparatus Complete or partial collapse of scaffolding Certain incidents relating to pipelines or pipeline works Any incident involving a vehicle used for the carriage of a dangerous substance Any unintended collapse or partial collapse of any building or structure Any explosion or fire resulting in the suspension of work for more than 24 hours due to the ignition of any material The sudden and uncontrolled release of certain quantities of flammable substances
The accidental escape or release of any substance in a quantity sufficient to cause death, major injury, or any other damage to the health
Occupational Diseases:- Particular diseases where the person affected is or has worked in a specified activity

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 39
Appendix E Internal and External Stakeholders
Incident Topic External Agency UH Bristol Trust Contact for advice
Serious non clinical incidents and accidents RIDDOR
Health and Safety Executive (HSE)
Health and Safety Team
Incidents where environmental contamination is suspected
Environmental Health Agency (EHA)
Health and Safety Team
Serious patient safety incidents/adverse events
Strategic Health Authority and NPSA
Patient Safety Team Executive Lead on call
Patient Safety incidents NPSA (via NRLS) Patient Safety Team
Incidents which involve medicines or medical devices
Medicines and Healthcare Products Regulatory
Agency (MHRA)
Medicines: Pharmacy Safety Manager
Medical Devices: MEMO Dept
Blood Transfusion incidents MRHA and SHOT Transfusion Practitioner or Haematology Dept
Incidents involving possible criminal activity
Police Legal Services
Incidents where child or vulnerable adult abuse is suspected
Police or Social Services Legal Services Child Protection Team Vulnerable Adults Lead for UH Bristol Trust
Incidents where press enquiries are anticipated
Print, Radio and Television Media Organisations
Press Office and see Serious Untoward Incident Policy
Appendix F
Incidents where Professional Regulatory or Defence Organisations
are Likely to be involved
GMC, NMC or Health Professionals Council
Professional Defence Organisations
Divisional Lead Doctor/Nurse/Midwife/Allied Health
Professional Medical Director or Chief Nurse
Communicable disease events and MRSA bacteraemia incidents
HPA Infection Control Team
Serious untoward infection related incidents
HPU Infection Control Team
Perioperative deaths NCEPOD Confidential Enquiry Manager Trust Hq
Maternal and neonatal deaths CEMACH Maternity Services Risk Manager St Michaels Hospital or Confidential
Enquiry Manager Trust Hq Other unexpected deaths Referral to HM Coroner Legal Services
Incidents likely to form the basis of a negligence claim
NHS Litigation Authority Claimant Solicitors
Legal Services
Radiation incidents involving staff Radiation incidents involving patients
HSE DOH and EHA
Local Radiation Protection Supervisor and Trust Radiation
Protection Advisor

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 40
Internal Joint Working Group for Incidents Complaints and Claims http://workspaces/Committees/JointReviewGroupforIncidentsClaimsComplaintsandPALs/Working%20Group%20Papers/Terms%20of%20Reference%20January%202008.pdf Governance and Risk Management Committee Appendix 10 in Risk Management Strategy: http://workspaces/Committees/GovernanceandRiskManagementCommittee/default.aspx Clinical Risk Assurance Committee http://workspaces/Committees/ClinicalRiskAssuranceCommittee/default.aspx Health and Safety Committee http://workspaces/Committees/HealthandSafetyTrustHealthandSafety%20CommitteeFireSafety/default.aspx

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 41
Appendix F Associated Policies Incidents and communication Major Incident Procedure http://nww.bristolacutescp.nhs.uk/ubhtarea/Mass%20Casualty%20(Major%20Incident)%20Plan.htm Serious Untoward Incident Policy and Procedure 2007 http://nww.avon.nhs.uk/dms/download.aspx?did=3937 Protocol for handling press enquiries 2007 http://www.UHB Trust.nhs.uk/documents/media_handling_protocol.doc Policy for cross organisational incident investigation http://nww.avon.nhs.uk/dms/download.aspx?did=8059 Investigation Policies Claims handling policy http://nww.avon.nhs.uk/dms/download.aspx?did=7048 Complaints policy http://nww.avon.nhs.uk/dms/download.aspx?did=7049 Research Related Serious Adverse Event Reporting Policy 2005 http://www.uhbristol.nhs.uk/research/information-for-researchers/information-and-guidance/Research_related_AE%20policy_%20version_3.2_13-08-07.pdf Radiation Protection http://nww.avon.nhs.uk/dms/download.aspx?did=8468 Risk Policies and specific patient/staff groups Risk Management Strategy http://nww.avon.nhs.uk/dms/download.aspx?did=7054 Infection Control Manual http://nww.avon.nhs.uk/dms/download.aspx?did=1850 Health and Safety Policy http://nww.avon.nhs.uk/dms/download.aspx?did=3219 Medical Equipment http://nww.avon.nhs.uk/dms/download.aspx?did=3921 Blood Transfusion http://nww.avon.nhs.uk/dms/download.aspx?did=3938 Medicines Code http://nww.avon.nhs.uk/dms/download.aspx?did=3477 Safeguarding Children http://nww.avon.nhs.uk/dms/download.aspx?did=3905 Vulnerable Adults http://nww.avon.nhs.uk/dms/download.aspx?did=3932 Resuscitation http://nww.avon.nhs.uk/dms/download.aspx?did=3934 Violence and Aggression http://nww.avon.nhs.uk/dms/download.aspx?did=5346 Human Resource and staff support policies Available on HR Web - http://hrweb/Pages/A-ZofHRPolicies.aspx Being Open Policy Policy Statement on Incident Report and Disciplinary Action Speaking Out Raising Concerns about malpractice at work Work Related Pressure Policy and Guidance

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 42
Appendix G - Guidance on how to write a statement
GUIDANCE on WRITING a PERSONAL ACCOUNT of EVENTS FOLLOWING INCIDENTS
(CLINICAL AND NON CLINICAL)
Some questions and answers Why are statements or accounts needed? When an adverse incident has occurred involving a patient, member of staff or visitor, the Manager or Clinical Risk Lead may request a written report from all members of staff involved. These accounts will then be used as part of the incident investigation and may be referred to the Legal Services Dept if it is anticipated the incident may lead to litigation or an Inquest. What should be in an account? 1. Basic information – layout of account When preparing an account of events leading up to and after an incident the following should be included:
• Full name of member of staff, the Incident Number (if known) and the patients name the statement refers to on each sheet of paper.
• Post held at the time of the incident and at the time of preparing the report, if different • All accounts should be signed except …… • If the account is clearly an interim report and likely to be changed further it needs to be
labeled as such and no signature is required • Accounts should be typed if possible • Staff should retain a copy of their own account both electronic and paper
2. About the incident • A chronological account of your involvement with the patient. • Who you communicated with during the incident • Where applicable commentary on why decisions were made by the member of staff and/or a
course of treatment or plan of support implemented. • A full account of what happened and what was observed (if appropriate) in relation to other
persons involved • When you have had extensive involvement with an incident, it would be impractical to
transcribe every detail from the case notes for inclusion in the statement. However a description of key events when the member of staff was either directly involved or witness to the event, should be included
3. No opinions Accounts should be factual: hearsay or second/third hand information should not be included unless necessary. However………. Any facts, which the member of staff in their professional judgment, feels to be relevant to the incident, should be included 4. Other things to remember
2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 43
• Accounts should be written in the first person. • The date, time and place (if appropriate) of the incident. • The names of other persons involved or who witnessed the incident • Any pertinent information relating to events leading up to the incident • Where you are using a document from the case notes refer to this clearly so it can easily be
identified eg nursing care plan 14th Oct • If other related incidents have occurred for which incident forms have been completed, then
the relevant forms can be attached to the account with a brief description of the incident and a reference to the incident form
• In the event of a sudden death where the Police are involved, they will request a formal statement from the staff directly involved at the time of death. Staff will be given a copy to retain. These can be used for the purpose of the internal incident enquiry with any additions attached as appropriate.
5. Where can I get some help with this?
• Staff may seek advice from senior colleagues who may point out spelling or grammar mistakes, discrepancies, omissions or contradictions. However, instruction cannot be given, as responsibility for the content of the statements, must lie with the author
• Your divisional clinical risk lead • The corporate clinical risk team can offer advice and have the advantage of not being
directly involved in the incident x3710 • The Legal Services Team especially where you anticipate that the statement may be
required for an Coroner’s Inquest x3612 6. Final comments The aim is to investigate as quickly as possible but also to get as thorough a picture as possible. These 2 aims can be contradictory. What you say in an account immediately after an incident may be altered by the investigation as other evidence comes to light. However your account is valid if it is your honest understanding of the facts at the time of writing. You cannot know everything about an incident otherwise we would not need an incident investigation. It is common for an investigation to radically overturn the immediate likely causes

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 44
Appendix H Incident investigation techniques
Root Cause Analysis Techniques
Brain storming A well-used familiar technique with two approaches:
Structured – a facilitator asks each individual in turn to contribute a suggestion or idea. It is useful if there are dominant members in the group who may make it difficult for less confident members to contribute
Unstructured - essentially a ‘free for all’ commonly used in group meetings. Whilst it enables spontaneity and freethinking, it can result in ideas being lost and disorder amongst the group.
For successful brainstorming avoid in depth questioning and exploration of ideas, however, gather first thoughts from individuals and record them as they are spoken. All suggestions should be recorded by the facilitator. Once the initial brainstorming task is complete, ‘grouping of ideas’ can then take place. Equipment needed - flip chart, thick felt pens, and blue tack
- Uninterrupted time
Brain writing A derivative of brainstorming which ensures participants confidentiality and anonymity. It is also a way of overcoming the reticence of some members of the group to contribute. Process:
All members of the group are provided with blanks cards or post-its. Ask participants to brainstorm their personal ideas and write each one down on
separate pieces of card or paper. Allow individuals space in the room for privacy, to undertake this task. The facilitator collects the cards/papers and either writes everything down on a flip
chart or sticks the cards /post-its to the flip chart, which is easier for rearranging into to groups/themes.
Exploring issues in further depth These methods enable the group to identify the problems that require further exploration. From this point, other structured techniques can be utilised to support the group in identifying the root causes of the incident/problem.

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 45
The five ‘why’s’ This approach is used for a more indepth analysis of a problem, which poses the
question ‘why’ for each ‘cause’ - until there are no more obvious ‘causes’. The methodology is simple, but requires careful facilitation to maintain clarity,
particularly when multiple causes appear to contribute to a single problem. It is essential that only one ‘cause’ is explored at a time. It is more effective to follow
the chain of each cause to its conclusion before commencing another. As a guide, 5 ‘rounds’ of ‘why’ should be used to identify the root cause of a problem.
Diagrammatic example
No knowledge of what specimens have been sent
Problem Temporary loss of tissue specimens in
transit
Pass through a number of staff groups before reaching destination
No one signs to acknowledge receipt at
any stage of the journey
No knowledge of specimen journey
Specimens not secure
Specimens are not checked into the box to
start with
No requirement to do so
No defined process or policy
No policy/ procedure
No secure tracking system
No policy/ procedure i.e. Poor organisation
No one’s considered it an issue before
No secure locking system
No checklist for the receiving lab staff
Transportation box unlocked – any one
can open it

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 46
Cause and effect diagrams
The ‘fishbone’ is useful for mapping out all possible contributory factors. The structured approach supports the group in working through all aspects of a problem. . It is recommended that the categories below are used as per ALARM/UCL protocol. Note that the individual is only one factor. This model can be modified to reflect the NPSA 7 Steps approach to contributory factors
By exploring each spine, the root causes of events/conditions should be identified. A contributory factors checklist at hand may prompt the group when looking at a problem (see Appendix). The diagrammatic example in Appendix 6iii illustrates how the factors surrounding the wrong hand being operated on may have contributed to the incident occurring.
Individual Factors
Team Factors
Patient Factors
Equipment & Resources
Task factors
Organisational & Management
Factors
Communication
Education & training
Work Factors
Problem to be explored

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 47
Diagrammatic example: This example shows a ‘worse case scenario’ of multiple factors failing to protect the patient from a lack of nursing staff, an overworked surgeon, non-compliance with consent procedures and pre-op checking procedures in theatre. When exploring the contributory factors, one or two spines in your diagram might be left blank. However, as highlighted below, there could be many factors involving both human and system failures. It should be noted that human failures - when explored -often link back to system failures, e.g. staff not completing pre-op checking procedures may result from a lack of staff and inadequate arrangements for covering staff shortages. ‘Worse case scenario’
‘
Work Factors
2 trained staff short, skill mix poor
Very busy theatre list No written ‘out of
hours’ theatre list
No supervision for new staff
Individual factors
Verbal communication only of patient needing
hand operation
Previous delay due to equipment shortage
Surgeon had worked 12 hrs without a break
Team Factors
Patient Factors
Organisational & management
Communication factors
Pathology of both hands
No written protocol for site
marking
Patient had medical problems delaying start of operation
DoH guidelines not adhered to for
consent procedures
Patient couldn’t speak English
Adapted from the ‘Root Cause Analysis Tool Kit – NPSA Pilot
Minimal training on obtaining
consent
Education & trainingTask Factors
Nurse involved with checking patient called away to an emergency
X-Ray not transferred to theatre with patient
Poor communication between theatre &
ward staff
Wrong hand operated on

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 48
NPSA contributory factors 2004 Seven Steps to Patient Safety Steps 1 and 4 Patient factors: these are unique to the patient(s) involved in the incident, such as the complexity of their condition or factors such as their age or language. Individual factors: these are unique to the individual(s) involved in the incident. They include psychological factors, home factors, and work relationships. Task factors: these include aids that support the delivery of patient care, such as policies, guidelines and procedural documents. They need to be up to date, available, understandable, useable, relevant and correct. Communication factors: these include communication in all forms: written, verbal and non-verbal. Communication can contribute to an incident if it is inadequate, ineffective, confusing, or if it is too late. These factors are relevant between individuals, within and between teams, and within and between organisations. Team and social factors: these factors can adversely affect the cohesiveness of a team. They involve: communication within a team, management style, traditional hierarchical structures, lack of respect for less senior members of the team and perception of roles. Education and training factors: the availability and quality of training programmes for staff can directly affect their ability to perform their job or to respond to difficult or emergency circumstances. The effectiveness of training as a method of safety improvement is influenced by content, delivery style, understanding and assessment of skill acquisition, monitoring and updates. Equipment and resources factors: equipment factors include whether the equipment is fit for purpose, whether staff know how to use the equipment, where it is stored and how often it is maintained. Resource factors include the capacity to deliver the care required, budget allocation, staffing allocation and skill mix. Working conditions and environmental factors: these factors affect ability to function at optimum levels in the workplace and include distractions, interruptions, uncomfortable heat, poor lighting, noise and lack of or inappropriate use of space. Each fishbone should represent just one of the contributory factors. The investigators may not find factors for each heading and should not ‘force’ factors to have something in every category.

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 49
Check List of Potential Contributory Factors Influencing Practice University College London/ALARM (1999)
Framework Headings Performance Influencing Factors
1. Patient Specific Factors Condition Treatment Staff-patient relationship Personal History
2. Individual (Staff) Factors Knowledge and skills Mental and physical stressors Competence
3. Task Factors Availability and use of protocols Availability and accuracy of test results Decision making aids Tasks design and clarity of structure
4. Team Factors Verbal communication Written communication Supervision and seeking help Congruence/consistency of aims Leadership and responsibility Staff/colleagues response to incidents
5. Working Conditions Staffing levels and skill-mix Education and training Workload/hours of work Environment Availability and maintenance of equipment and
supplies Building and design Administrative support Movement of patients between sites Time factors (e.g. delays) Atmosphere
6. Organisational Processes and Management Factors
Organisational Structure Policy, standards and goals Safety Culture Financial resources and constraints
7. Institutional context Government policy Macro-economic factors NHS Executive CNST Regulation (GMC, NMC, etc)

2009 UHB TRUST Adverse Incident Reporting Policy & Guidelines 50
Interactive read only version available on http://www.msnpsa.nhs.uk/idt2/(p0ompevfcz0rrc4534ukn1qe)/decision_tree9j.aspx?JS=1

Local Trust version Serious Patient Safety Incident Investigation and Outcome
Incident No. SYNOPSIS AND CHRONOLOGY
JUSTIFICATION FOR HIGH-RISK RATING
CARE MANAGEMENT PROBLEMS
An Organisation-wide Policy for the Management of Incidents Including the Management of Serious Untoward Incidents
Page 2
CONTRIBUTORY FACTORS
RISK MANAGEMENT IMPLICATIONS/ RECOMMENDATIONS
ACTIONS
Investigated by…………………… Date…………………………………. Review date…………………………

An Organisation-wide Policy for the Management of Incidents Including the Management of Serious Untoward Incidents
Page 3
Trust version adopting NPSA incident reporting tools Link below to the Patient Safety NPSA Connect web page. Please follow the link under Root Cause Analysis to access the incident reporting tools.
http://connect/Governance/patientsafety/Pages/NationalPatientSafetyAgency.aspx
Patient Safety Investigation Report – Example
Summary Incident Description & Consequences Example A woman sustained an allergic reaction following IV administration of a drug she was known to be allergic to
Incident type: Medication Incident Specialty: Surgery Effect on patient: Allergic reaction Severity level: Low Scope and Level of Investigation Example Level of investigation – Concise The investigation was planned to begin at referral for admission and to conclude at final patient diagnosis of incident outcome. The investigation included referring GP practice, short stay ward, pharmacy and the patient Involvement and support of Patient and Relatives Example The incident was discussed with the Patient and her husband and an apology was given. The patient was involved in the investigation to help determine what went wrong and a copy of the investigation report will be sent in line with the patient’s wishes Chronology of events - See template below… Notable Practice Example Although none of the ward staff had experienced the situation before actions taken to summon expert help and treatment, and to inform and involve relatives were rapid and correct.

An Organisation-wide Policy for the Management of Incidents Including the Management of Serious Untoward Incidents
Page 4
Care and Service Delivery Problems (Themed and prioritised) Example Nurses on a short stay ward routinely failed to complete the section in the patient notes to highlight the existence of known allergies
Contributory Factors Example Over years numerous assessments for nutrition, pressure ulcers, falls risk etc. had been added and created a situation where short stay wards saw all the documentation as impossible to complete Root Causes Example There is no distinction between essential and desirable documentation, either within or across clinical records Lessons Learned Example When developing new or updated care plans, assessment of the wider implications of their use should be conducted and acted upon to reduce the risk of impact on patient safety Recommendations Example Agree and highlight (e.g. in grey), the essential fields to be completed within standardised assessment charts for short stay patients. Ensure these agreed essential criteria are set as mandatory fields in electronic record development/upgrade Action Plan - See template below… Implementation, monitoring and evaluation arrangements Example Involve the organisations documentation and policy group for help in amending and piloting assessment charts. Conduct an audit of short stay ward records to identify whether this solution has led to an improvement in completing essential patient assessment fields Arrangements for sharing and learning Example To share findings with other departments caring short stay patients and determine whether they can assist in piloting suggested solutions. Share findings with Patient Safety manager to identify opportunities for sharing outside the organisation Author A. Perfect-Sister Date 01.01.2000

An Organisation-wide Policy for the Management of Incidents Including the Management of Serious Untoward Incidents
Page 5
Incident No: Recommendation 1 Recommendation 2 Recommendation 3
Root CAUSE
EFFECT on patient/service
Recommendation(s) to address root cause (or rationale, if no action or recommendation is set)
Action(s) to achieve recommendations
Level of recommendation (organisation, directorate, team etc)
Implementation by whom:-
Implementation by when:-
Resource required (time)
Resource required (money)
Resource required (other)
Evidence of completion
Monitoring and evaluation arrangements
Sign-off by:-
Chronology of events
Date & Time Event - Example
30.11.1999 Patient referred for surgery by GP. …..

An Organisation-wide Policy for the Management of Incidents Including the Management of Serious Untoward Incidents
Page 6