Embed Size (px)
Citation preview

www.currentmedicine.org
Current Medicine Volume 2 Issue 1 pages 1-4 Pathology
Current Medicine
Current Medicine Volume 2 Issue 1 Pages 1-4 Pathology
An Unnecessary Hepatectomy as Consequence of a False Positive of
Liver Biopsy
Massimo Bolognesi*, MD
General Practice Medicine, Internal Medicine Specialist, AUSL della Romagna, District of Cesena,
Via Ungaretti, 494 47521, Cesena (FC), Italy
Correspondence: Tel: +390547645074, E-mail: [email protected]
Accepted date: 10 May 2019
Citation: Bolognesi M. An Unnecessary Hepatectomy as Consequence of a False Positive of Liver
Biopsy. Curr Med. 2019; 2(1):1-4.
Copyright: ©2019, Current Medicine. Reprints: [email protected]
ABSTRACT
Pathological anatomy is a branch of medicine that can easily be involved in diagnostic errors, primarily because the
examination procedure is complex and demanding. One of the most frequent errors is the so-called false-positive diagnosis
(e.g. diagnosed incorrectly a liver adenoma as carcinoma). In fact, here the author describes an unexpected error that was
consequent from a misinterpretation of a liver biopsy of a liver mass of uncertain interpretation as described from
radiological images that has subsequently led to incorrect patient management plans.
Keywords: Pathologic mistake; Hepatocellular Carcinoma (HCC); Hepatic biopsy
INTRODUCTION
Nowadays, the role of the aspirated needle biopsy (FNA) of the liver has changed dramatically. Technological
developments in imaging methods have reduced the need for tissue confirmation in hepatocellular carcinoma
(HCC). Otherwise, there are many difficulties in the cytodiagnosis of HCC, which mainly include how to
correctly distinguish malignant neoplastic lesions from benign hepatocellular lesions, such as regenerative
nodules, dysplastic nodules, focal nodular hyperplasia and hepatocellular adenoma from reactive hepatocytes. It
follows that the best possible result depends on a number of clinical and instrumental factors that require
supervision and collaboration between clinical physicians and pathologists, in order to avoid interpretative
errors to reduce indeterminate diagnosis of highly differentiated hepatocellular lesions.
CASE REPORT
A 69-year-old male obese patient was recently operated on suspected well-differentiated hepatocellular
Carcinoma. The patient’s history is as follows: inguinal cryptorchidism; diabetes mellitus type 2;
hypercholesterolemia; hypertension; obesity. In March 2008 he underwent radical robotic prostatectomy (onset
PSA=14; Gleason score 8; pT2bN0Mx) with good outcomes. In the follow up the PSA had risen and he

Bolognesi, 2019
Current Medicine Volume 2 Issue 1 pages 1
underwent Radio-Therapy treatment was completed in April 2010 (64 Gy on the prostate l
initial reduction, increased to 2.33 (December 2010), so a scintigraphy and PET
were performed and resulted negative for disease localization.
hyperaccumulation of the prostate lodge indicative of recurrence of disease and doubt of lympha
inguinal right (<1 cm). A subsequent specialist examination of radiotherapy did not give an indication for
radiotherapy reprocessing. Because of PSA <0.003, bhcg <0.1, alphetop
was suspended in January 2016). However, in October 2016, a follow
formation of about 40 mm in the left liver lobe. The m
adenoma in relation to hormonal therapy. However,
CT-guided liver biopsy which showed specimen features of Hepatic Steatosis. In November 2018 an
oncological follow up with CT scan found in
currently 70 × 68 mm (Vs 40 × 40 mm) suggestive for adenoma or maybe for primary hepatic lesion. A few
slightly enlarged lymph nodes near the hepatic hilum, the largest in the porto
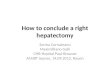
stable. Oncologists decided to carry out another biopsy of the liver mass that showed needle
liver parenchyma with small cell dysplasia, reticulum alteration, and absence of portal spaces (
staining showed capillarization. In conclusion, the findings of specimens were difficult to interpret but the
totality of the data favored the hypothesis of well
discussed at a multidisciplinary meeting, where resect
consent. Hepatic lobectomy was performed on 12 February, 2019. The report of the pathologist described a
typical Hepatocellular adenoma (Figure 2)
glutamine-synthetase, glypican-3 and showed a very low proliferative index (Ki
immunohistochemical investigation. Beta
The hepatocytes appeared rather regular and only at times, they showed images of discreet nuclear
polymorphism. The morphological characteristics of the lesion were similar to those of the previous histological
biopsy. In view of the histological picture obviously no indication of
In spite of this clear histological picture no indication whatsoever of medical treatment was given. In the end,
only the oncologist requested a complete abdomen ultrasound in 6 months and complete blood count wi
formula, liver function, kidney, blood sugar, vit. D and PSA reflex.
Figure 1: Hystologic findings of hepatic biopsy that showed needle
small cell dysplasia, reticulum alteration, and absence of portal spaces.
Issue 1 pages 1-4
Therapy treatment was completed in April 2010 (64 Gy on the prostate lodge). PSA, after
initial reduction, increased to 2.33 (December 2010), so a scintigraphy and PET-TC choline (January 201
ative for disease localization. A subsequent PET with carbon acetate showed
prostate lodge indicative of recurrence of disease and doubt of lympha
). A subsequent specialist examination of radiotherapy did not give an indication for
PSA <0.003, bhcg <0.1, alphetoprotein 1.9 values, Enantone drug therap
). However, in October 2016, a follow-up abdomen CT scan revealed a hepatic
formation of about 40 mm in the left liver lobe. The most likely hypothesis expressed after an MRI was for
to hormonal therapy. However, biopsy confirmation was recommended. So, he underwent a
guided liver biopsy which showed specimen features of Hepatic Steatosis. In November 2018 an
oncological follow up with CT scan found in the context of liver steatosis a growing mass of the II segment
40 mm) suggestive for adenoma or maybe for primary hepatic lesion. A few
slightly enlarged lymph nodes near the hepatic hilum, the largest in the porto-caval site of 23 ×
stable. Oncologists decided to carry out another biopsy of the liver mass that showed needle-
liver parenchyma with small cell dysplasia, reticulum alteration, and absence of portal spaces (Figure 1
larization. In conclusion, the findings of specimens were difficult to interpret but the
totality of the data favored the hypothesis of well-differentiated hepatocarcinoma, stage G1. Then this case was
multidisciplinary meeting, where resection surgery was deemed necessary. The patient gave his
consent. Hepatic lobectomy was performed on 12 February, 2019. The report of the pathologist described a
(Figure 2) with focal dysplastic aspects. In fact, the lesion wa
3 and showed a very low proliferative index (Ki-67), equal to about 1% in the
immunohistochemical investigation. Beta-catenin had a normal membrane expression. No mitosis was observed.
rather regular and only at times, they showed images of discreet nuclear
polymorphism. The morphological characteristics of the lesion were similar to those of the previous histological
biopsy. In view of the histological picture obviously no indication of any kind of medical treatment to complete.
In spite of this clear histological picture no indication whatsoever of medical treatment was given. In the end,
only the oncologist requested a complete abdomen ultrasound in 6 months and complete blood count wi
formula, liver function, kidney, blood sugar, vit. D and PSA reflex.
Hystologic findings of hepatic biopsy that showed needle-like frustules of liver parenchyma with
small cell dysplasia, reticulum alteration, and absence of portal spaces.
Curr Med 2(1): 1-4
Pathology
odge). PSA, after
TC choline (January 2011)
A subsequent PET with carbon acetate showed
prostate lodge indicative of recurrence of disease and doubt of lymphadenopathy
). A subsequent specialist examination of radiotherapy did not give an indication for
rotein 1.9 values, Enantone drug therapy
up abdomen CT scan revealed a hepatic
likely hypothesis expressed after an MRI was for
biopsy confirmation was recommended. So, he underwent a
guided liver biopsy which showed specimen features of Hepatic Steatosis. In November 2018 an
a growing mass of the II segment
40 mm) suggestive for adenoma or maybe for primary hepatic lesion. A few
× 11 mm, resulted
-like frustules of
Figure 1). CD34
larization. In conclusion, the findings of specimens were difficult to interpret but the
differentiated hepatocarcinoma, stage G1. Then this case was
The patient gave his
consent. Hepatic lobectomy was performed on 12 February, 2019. The report of the pathologist described a
with focal dysplastic aspects. In fact, the lesion was negative for
67), equal to about 1% in the
catenin had a normal membrane expression. No mitosis was observed.
rather regular and only at times, they showed images of discreet nuclear
polymorphism. The morphological characteristics of the lesion were similar to those of the previous histological
any kind of medical treatment to complete.
In spite of this clear histological picture no indication whatsoever of medical treatment was given. In the end,
only the oncologist requested a complete abdomen ultrasound in 6 months and complete blood count with
like frustules of liver parenchyma with

Bolognesi, 2019
Current Medicine Volume 2 Issue 1 pages 1
Figure 2: The definitive hystologic findings of the liver mass showed the typical features of Hepatocellular
adenoma. No mitosis was observed. The hepatocytes appeared rather regular and only at times, they showed
images of discreet nuclear pol
Hepatocellular carcinoma (HCC) is a primary malignant cancer of the liver which mainly affects patients
suffering from a pre-existing condition, i.e. chronic liver disease and/or cirrhosis
of the liver is generally diagnosed at an advanced stage, the reoccurrence rate is high and the chances of
successful treatment are narrow. Thus the prognosis is very poor
diagnosis and prognosis of HCC [3]. However, as a result of the considerable progress which has been made in
imaging technology, some recommendations and guidelines have been set which limit the use of biopsy to
specific cases only. This is the reason why carrying ou
hepatocellular carcinoma is more than often subject to controversy. Moreover, biopsy may also cause side
effects such as needle tract seeding of tumour, a minor risk of complications. But above all technica
interpretative errors are likely [4]. Besides, tissue analysis of the lesion is frequently necessary owing to the fact
that the imaging is sometimes unclear. This is due to limited experience and lack of advanced technology in
several centers, especially when it comes to imaging limits for the diagnosis of initial or mixed forms of HCC.
Furthermore, biopsies are quite often needed for trials on new drugs and targeted therapies
characteristics and morphology based correlates of mol
the management and prognosis of the disease. This brief report has provided a description of how
histopathology mistakes and the role of biopsy in the diagnosis, management and prognosis of HCC may be
cause of errors in plans and inappropriate surgery. Taking into account that the evidence in literature concerning
diagnostic error is poor, clinicians should play a key role in reducing pathology mistakes by adopting several
approaches, such as the appropriate order of the tests, gaining precise clinical information regarding the patients,
obtaining high quality samples and acquiring second opinions
clinical impression and pathology diagnosis).
CONFLICT
The author declared there is no conflict of interest
Issue 1 pages 1-4
The definitive hystologic findings of the liver mass showed the typical features of Hepatocellular
adenoma. No mitosis was observed. The hepatocytes appeared rather regular and only at times, they showed
images of discreet nuclear polymorphism.
DISCUSSION
Hepatocellular carcinoma (HCC) is a primary malignant cancer of the liver which mainly affects patients
existing condition, i.e. chronic liver disease and/or cirrhosis [1]. Unfortunately, carcinoma
of the liver is generally diagnosed at an advanced stage, the reoccurrence rate is high and the chances of
successful treatment are narrow. Thus the prognosis is very poor [2]. Liver biopsy plays a crucial role in the
. However, as a result of the considerable progress which has been made in
imaging technology, some recommendations and guidelines have been set which limit the use of biopsy to
specific cases only. This is the reason why carrying out a biopsy on a mass or lesion suspected of being
hepatocellular carcinoma is more than often subject to controversy. Moreover, biopsy may also cause side
effects such as needle tract seeding of tumour, a minor risk of complications. But above all technica
. Besides, tissue analysis of the lesion is frequently necessary owing to the fact
that the imaging is sometimes unclear. This is due to limited experience and lack of advanced technology in
ally when it comes to imaging limits for the diagnosis of initial or mixed forms of HCC.
Furthermore, biopsies are quite often needed for trials on new drugs and targeted therapies [5]
characteristics and morphology based correlates of molecular subtypes give extremely helpful information for
the management and prognosis of the disease. This brief report has provided a description of how
histopathology mistakes and the role of biopsy in the diagnosis, management and prognosis of HCC may be
cause of errors in plans and inappropriate surgery. Taking into account that the evidence in literature concerning
diagnostic error is poor, clinicians should play a key role in reducing pathology mistakes by adopting several
propriate order of the tests, gaining precise clinical information regarding the patients,
s and acquiring second opinions in specific situations (e.g. incongruity between
clinical impression and pathology diagnosis).
CONFLICT OF INTEREST
The author declared there is no conflict of interest.
Curr Med 2(1): 1-4
Pathology
The definitive hystologic findings of the liver mass showed the typical features of Hepatocellular
adenoma. No mitosis was observed. The hepatocytes appeared rather regular and only at times, they showed
Hepatocellular carcinoma (HCC) is a primary malignant cancer of the liver which mainly affects patients
. Unfortunately, carcinoma
of the liver is generally diagnosed at an advanced stage, the reoccurrence rate is high and the chances of
. Liver biopsy plays a crucial role in the
. However, as a result of the considerable progress which has been made in
imaging technology, some recommendations and guidelines have been set which limit the use of biopsy to
t a biopsy on a mass or lesion suspected of being
hepatocellular carcinoma is more than often subject to controversy. Moreover, biopsy may also cause side
effects such as needle tract seeding of tumour, a minor risk of complications. But above all technical and
. Besides, tissue analysis of the lesion is frequently necessary owing to the fact
that the imaging is sometimes unclear. This is due to limited experience and lack of advanced technology in
ally when it comes to imaging limits for the diagnosis of initial or mixed forms of HCC.
]. Finally, tissue
ecular subtypes give extremely helpful information for
the management and prognosis of the disease. This brief report has provided a description of how
histopathology mistakes and the role of biopsy in the diagnosis, management and prognosis of HCC may be the
cause of errors in plans and inappropriate surgery. Taking into account that the evidence in literature concerning
diagnostic error is poor, clinicians should play a key role in reducing pathology mistakes by adopting several
propriate order of the tests, gaining precise clinical information regarding the patients,
in specific situations (e.g. incongruity between

Bolognesi, 2019 Curr Med 2(1): 1-4
Current Medicine Volume 2 Issue 1 pages 1-4 Pathology
REFERENCES
1. Llovet JM, Fuster J, Bruix J, Barcelona-Clínic Liver Cancer Group. The Barcelona approach:
diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004; 10: S115-20.
2. Beasley RP, Hwang LY, Lin CC, Chien CS. Hepatocellular carcinoma and hepatitis B virus. A
prospective study of 22 707 men in Taiwan. Lancet. 1981; 2 (8256): 1129-33.
3. Sparchez Z, Mocan T. Contemporary role of liver biopsy in hepatocellular carcinoma. World J
Hepatol. 2018; 10(7): 452–461.
4. Doyle A, Morris S. Liver Biopsy for Hepatocellular Carcinoma (HCC): Should this be a Routine?
Current Hepatology Reports. 2017; 16: 46–50.
5. Richard SF. The Role of Liver Biopsy in Hepatocellular Carcinoma. Gastroenterol Hepatol (NY).
2016; 12(10): 628–630.
This article is accepted and published in under the section of Pathology in “Current Medicine” open magazine. The copy
rights reserved; however, can be cited as per the international publication guidelines.


![, Xavier Llovet - Redalyc file2 melgarejo et al. 1. introducción &rqiuhfxhqfld hohvwxglrtxhvhuhdol]dsdudodydorud flyqghxqghsyvlwrplqhudolpsolfdwdqvyorhohvwxglrjh qpulfrghodvoh ...Cited](https://img.pdfslide.net/doc/110x75/5c5bf3af09d3f245368ca5df/-xavier-llovet-melgarejo-et-al-1-introduccion-rqiuhfxhqfld-hohvwxglrtxhvhuhdoldsdudodydorud.jpg)