Embed Size (px)
Citation preview

AnUnusualCaseofVisceralLeishmaniasis inanImmunosuppressedPatientwithMyastheniaGravis
CharlotteSnead1,NathanClack2,Izak Heys1,Begoña Bovill11SouthmeadHospital,NorthBristolNHSTrust&2GloucestershireHospitalsNHSFoundationTrust
InitialInvestigations
CasePresentation ManagementandClinicalCourse DiscussionA30-year-oldPolishmanpresentedwithatwo-weekhistoryoffever,nightsweats,7kgweightlossandLUQpain.• PMHx:Generalisedmyastheniagravis,thymectomy.• DHx:Prednisolone,pyridostigmine,azathioprine,
omeprazole,alendronateandamitriptyline.Azathioprinewasstoppedtwoweekspreviouslyduetopancytopaenia.
• SHx:Painteranddecorator.Nosmokingoralcohol.• TravelHx:TraveltoPolandtwiceayear.1weekholidayin
Alicante,Spain,5monthsbefore.Pets:Goldfishbutnootheranimalexposure.Noobviousbitesnorstings.
• Vitals:HR104,BP102/69,RR14,SpO2100%,swingingfevers39-40ºC. Examination:Thymectomy scarandtendersplenomegalypalpable2cmbelowcostalmargin.
• 9daysofempiricaltreatmentwithIVmeropenem,vancomycinandmicafunginà noclinicalimprovement.
• Bloodtransfusion,G-CSFandplatelettransfusion.• Bonemarrowbiopsyà noevidenceofhaematological
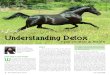
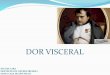
malignancyorleishmaniasis.• Splenicbiopsyatday14à Leishmaniasis amastigotesseen• RapidclinicalresponsetoliposomalAmphotericinB(4mg/kg
ondays1-5,10,17,24,31,38).• Co-trimoxazole prophylaxis(HIV–ve butCD4count67/mm3)• Remainswell9monthsaftertreatmentcompletion.
Initialdifferentialdiagnoseswereneutropenicsepsis,haematologicalmalignancy orautoimmunepathology.PositiveEBVserologyconfusedtheclinicalpictureandthediagnosisofvisceralleishmaniasis (VL)wasmadelate.Splenicbiopsywasessentialfordiagnosis,aswasadetailedtravelhistory.ThispatientwasimmunosuppressedwithimpairedTcellresponsesduetothymectomy,azathioprineandcorticosteroidtreatment,whichincreasetheriskofallinfections,inparticularthosecausedbyintracellularorganisms1.VLinimmunosuppressedpatients,includingthoseoncorticosteroids,maypresentunusually,isoftendiagnosedlateandmaybemorechallengingtotreat2,3.ThereshouldbeahighindexofsuspicionforVLinimmunosuppressedpatientspresentingwithfeverandpancytopaenia whohavetravelledtoorliveintheMediterraneanbasin4.ImmunosuppressedpatientswithVLshouldbetreatedwithliposomalAmphotericinB3,asperBHIVAguidelines5.Inthiscase,itwasimportanttomonitorcloselyformyastheniacrisis,whichmaybeprecipitatedbyinfection,andtoavoidhypokalaemia,arecognisedsideeffectofliposomalAmphotericinBwhichmayworsenmyastheniasymptoms6.
References1.StuckAEetal.Riskofinfectiouscomplicationsinpatientstakingglucocorticosteroids.RevInfectDis.1989.11(6):954-63. 2.RamosJMetal.IsVisceralLeishmaniasis DifferentinImmunocompromisedPatientsWithoutHumanImmunodeficiencyVirus?AComparative,MulticenterRetrospectiveCohortAnalysis.AmJTropMedHyg.2017,97(4):1127-11333.Pagliano P&EspositoS.Visceralleishmaniasis inimmunocompromisedhost:anupdateandliteraturereview.JChemother.2017,29(5):261-2664.Pittalis S.etal.Leishmania infantum leishmaniasis incorticosteroid– treatedpatients.BMCInfectiousDiseases2006,(6):77.5.http://www.bhiva.org/documents/Guidelines/OI/5_OIGuidelinesConsultation.pdf.6.CritchleyK.etal.Valueofexchangeableelectrolytemeasurementinthetreatmentofmyastheniagravis.JournalofNeurology,NeurosurgeryandPsychiatry.1977,40:250-252
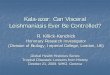
(A,B):SplenomegalyonCT.(C):Leishmaniasis amastigotes (arrows)onsplenic biopsy
A B
C
LabBloods Pancytopaenia:
U&EandLFTs:LDH:Albumin:
Hb 70g/L(nadir),WCC0.6x109/L,Neut 0.35x109/L,Plt 31x109/LNormal548U/L32g/L
Microbiology 3xbloodcultures,stoolMC&S,pneumococcalandlegionellaAg
Negative
Specialistserology
HIV,CMV,toxoplasma,letospira,flavirus,rickettsial andCoxiellaburnetti serology
Allnegative
EBVIgM Positive(viralload2,379copies/ml)Immunology ANAandrheumatoidfactor
ImmunoglobulinsNegativeIgG15.2g/L,IgA0.85g/L,IgM0.25g/L
Imaging CTC/A/P Splenomegaly19cmlongitudinalaxis,nolymphadenopathyor newcollection