Embed Size (px)
DESCRIPTION
dental radiology
Citation preview
Knowledge for Clinical Practice
WWW.DENTALLEARNING.NET
A PEER-REVIEWED PUBLICATIONA PEER-REVIEWED PUBLICATION
DENTAL LEARNINGVOLUME 2 | ISSUE 6
INSIDEEarn 2
CECredits
Written fordentists, hygienists
and assistants
AN UPDATE ON
Bitewing Radiography TechnologyBrad Potter, DDS, MS — Page 3

3OCTOBER 2013
EDUCATIONAL OBJECTIVES
The overall goal of this article is to provide the reader with informa-tion on the use of radiography for caries detection. On completion of this article, the participant will be able to:
1. Review the types of oral radiographs used for caries detection2. De� ne sensitivity and speci� city 3. Contrast and compare the methodology and results for radio-
graphic caries detection4. List and describe the methods by which radiation exposure is
reduced as well as the relative radiation exposure with different radiographic methodologies for caries detection.
SPONSOR/PROVIDER: This is a Dental Learning, LLC continuing education activity. COMMERCIAL SUPPORTER: This course has been made possible through an unrestricted educational grant from INSTRUMENTARIUM. DESIGNATION STATEMENTS: Dental Learning, LLC is an ADA CERP recognized provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Dental Learning, LLC designates this activity for 2 CE credits. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 2/1/2012 - 1/31/2016. Provider ID: # 346890. EDUCATIONAL METHODS: This course is a self-instructional journal and web activity. Information shared in this course is based on current information and evidence. REGISTRATION: The cost of this CE course is $29.00 for 2 CE credits. PUBLICATION DATE: October, 2013. EXPIRATION DATE: September, 2016. REQUIREMENTS FOR SUCCESSFUL COMPLETION: To obtain 2 CE credits for this educational activity, participants must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%. AUTHENTICITY STATEMENT: The images in this course have not been altered. SCIENTIFIC INTEGRITY STATEMENT: Information shared in this continuing education activity is developed from clinical research and represents the most current information available from evidence-based dentistry. KNOWN BENEFITS AND LIMITATIONS: Information in this continuing education activity is derived from data and information obtained from the reference section. EDUCATIONAL DISCLAIMER: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the � eld related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. PROVIDER DISCLOSURE: Dental Learning does not have a leadership position or a commercial interest in any products that are mentioned in this article. No manufacturer or third party has had any input into the development of course content. CE PLANNER DISCLOSURE: The planner of this course, Tricia Branch, does not have a leadership or commercial interest in any products or services discussed in this educational activity. She can be reached at [email protected]. TARGET AUDIENCE: This course was written for dentists, dental hygienists, and assistants, from novice to skilled. CANCELLATION/REFUND POLICY: Any participant who is not 100% satis� ed with this course can request a full refund by contacting Dental Learning, LLC, in writing. Go Green, Go Online to www.dentallearning.net take your course. Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected].
Unfortunately, dental caries continues to be a primary oral health issue, which requires a comprehensive consideration of caries risks, preventative oral health care by the patient and dental profes-sional, and a series of clinical techniques to determine the presence and extent of caries involvement. Total patient care requires radio-graphic assessment of dental disease and is considered an essential tool in this assessment. Bitewing radiographs remain the primary diagnostic image for intraoral caries assessment with periapical imaging and extraoral imaging being used as adjunctive tools. Both � lm-based and digital intraoral bitewing images continue to provide the necessary resolution and evidence-based accuracy for diagnosis, while extraoral techniques require further study.
ABSTRACT
An Update on Bitewing Radiography Technology
Introduction
The discovery of X-rays by Röntgen, and early work by dentists, including Dr. C. Edmund Kells, led to signi� cant developments and improvements over
time in the ability of clinicians to diagnose medical and later dental conditions. Since these early developments, advances in oral radiography have resulted in a wide range of diag-nostic options and improved capabilities for the detection of pathological lesions and other anomalies. The overall goals of caries detection are to determine whether caries is present, to determine its extent, and to detect it at an early stage when it is still susceptible to remineralization with the use of preventive agents, in particular � uoride. Incipient carious lesions are con� ned to enamel and have not yet breached the dentinoenamel junction (DEJ). Ideally, lesions will not develop but if they do it is optimal to detect them while they are still in the outer enamel, at which time there
Integrated Media Solutions/Dental Learning LLC is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Integrated Media Solutions/Dental Learning LLC designates this activity for 2 continuing education credits.
Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement.2/1/2012 - 1/31/2016 Provider ID: # 346890AGD Subject Code: 130
Brad Potter, DDS, MS Dr. Brad Potter graduated from Northwestern University School of Dentistry in 1979. After private practice in general dentistry in Colo-rado for 10 years, he returned to school at The University of Texas Health Science Center at San Antonio where he earned a Certi� cate and an M.S. in Dental Diagnostic Sciences. Dr. Pot-ter’s current appointment is in the Department
of Diagnostic and Biologic Sciences and he also serves as Senior Associate Dean of Academic Affairs at the University of Colorado School of Dental Medicine. In addition to his academic roles, he maintains a private practice in oral and maxillofacial radiology.
He is a diplomate of the American Board of Oral and Maxillofa-cial Radiology, and a fellow of the American College of Dentists, International College of Dentists, and the American Academy of Oral and Maxillofacial Radiology. Dr. Potter can be reached at [email protected].
ABOUT THE AUTHOR
Dental Learning, LLC is a Dental Board of California CE Provider. The California Provider # is RP5062. All of the information contained on this certi� cate is truthful and accurate. Completion of this course does not constitute authorization for the attendee to perform any services that he or she is not legally authorized to perform based on his or her license or permit type. This course meets the Dental Board of California’s requirements for 2 units of continuing educa-tion. CA course code is 02-5062-13021.
DENTAL LEARNING www.dentallearning.net
4 VOLUME 2 | ISSUE 6
is the greatest opportunity to remineralize or arrest them. Paradoxically, incipient lesions are the most dif�cult to detect radiographically.1 Options for caries detection in addition to visual examination include oral radiography, transillumination, �uorescence and laser �uorescence. At the current time, visual examination plus oral radiography is the most commonly used method for caries detection and other technologies, including panoramic bitewings, are recom-mended as adjunctive devices.
Radiography for caries detection and the assessment of the depth of caries present involves the differential attenua-tion of X-rays through hard tooth structure that is sound or partially demineralized, with more X-rays passing through the less dense demineralized tooth structure to reach the image receptor. Use of a standardized and strict methodol-ogy for caries detection is necessary to enable appropriate preventive and restorative care. In addition to diagnostic accuracy, a further consideration of importance is the risk versus bene�t of exposure to radiation and risk reduction through minimization of radiation exposure.
Desirable characteristics for any diagnostic tool require that a method offer high sensitivity, high speci�city and high reliability. Sensitivity refers to the ability of a test to cor-rectly identify when a condition is present – in the case of dental caries, sensitivity refers to the ability of an image to correctly identify when a carious lesion is present. Speci�city,
on the other hand, refers to the ability of images to detect when the tooth is sound and no carious lesion is present. Low sensitivity results in carious lesions being missed (and therefore not being treated preventively or restored), while low speci�city would result in treatment of a lesion that in fact was not present.
Radiographic Caries DetectionCurrent radiographic techniques typically used for caries
detection include the use of intraoral bitewings, panoramic radiographs, and extraoral “bitewings” from panoramic ra-diography. In addition to the detection of dental caries, other indications and uses of bitewings include monitoring the pro-gression (and arrestment/reversal) of carious lesions as well as assessing existing restorations and periodontal status.
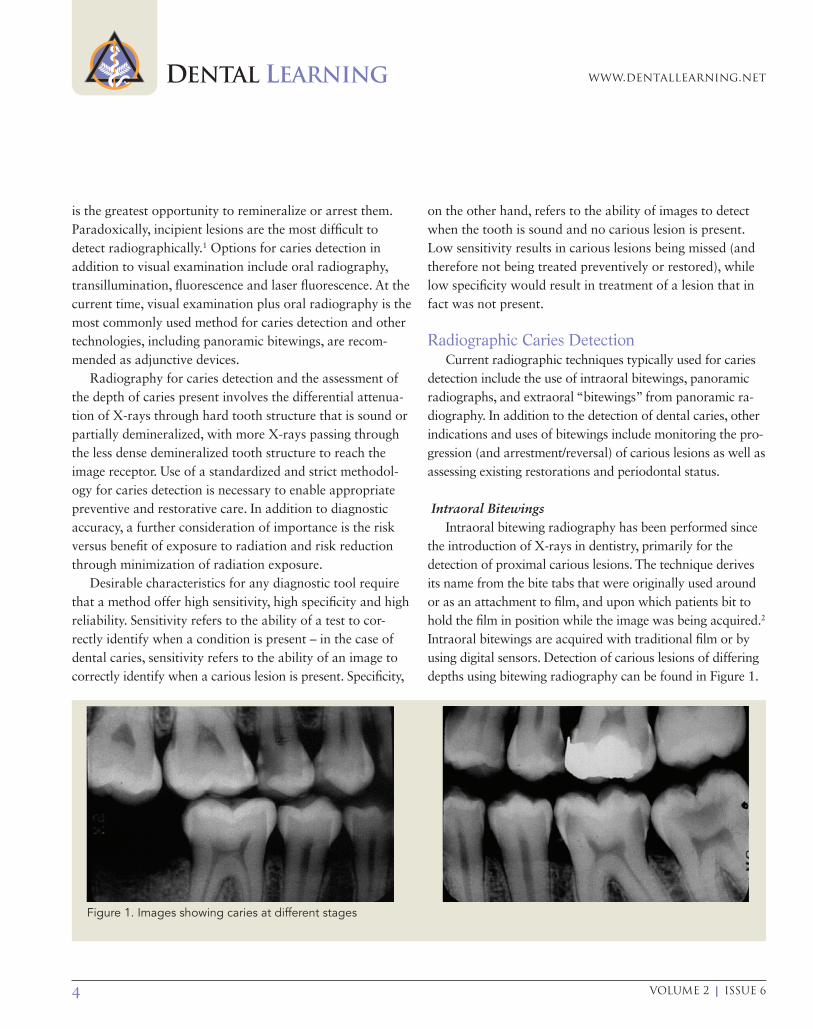
Intraoral BitewingsIntraoral bitewing radiography has been performed since
the introduction of X-rays in dentistry, primarily for the detection of proximal carious lesions. The technique derives its name from the bite tabs that were originally used around or as an attachment to �lm, and upon which patients bit to hold the �lm in position while the image was being acquired.2
Intraoral bitewings are acquired with traditional �lm or by using digital sensors. Detection of carious lesions of differing depths using bitewing radiography can be found in Figure 1.
Figure 1. Images showing caries at different stages
An Update on Bitewing Radiography Technology
5OCTOBER 2013
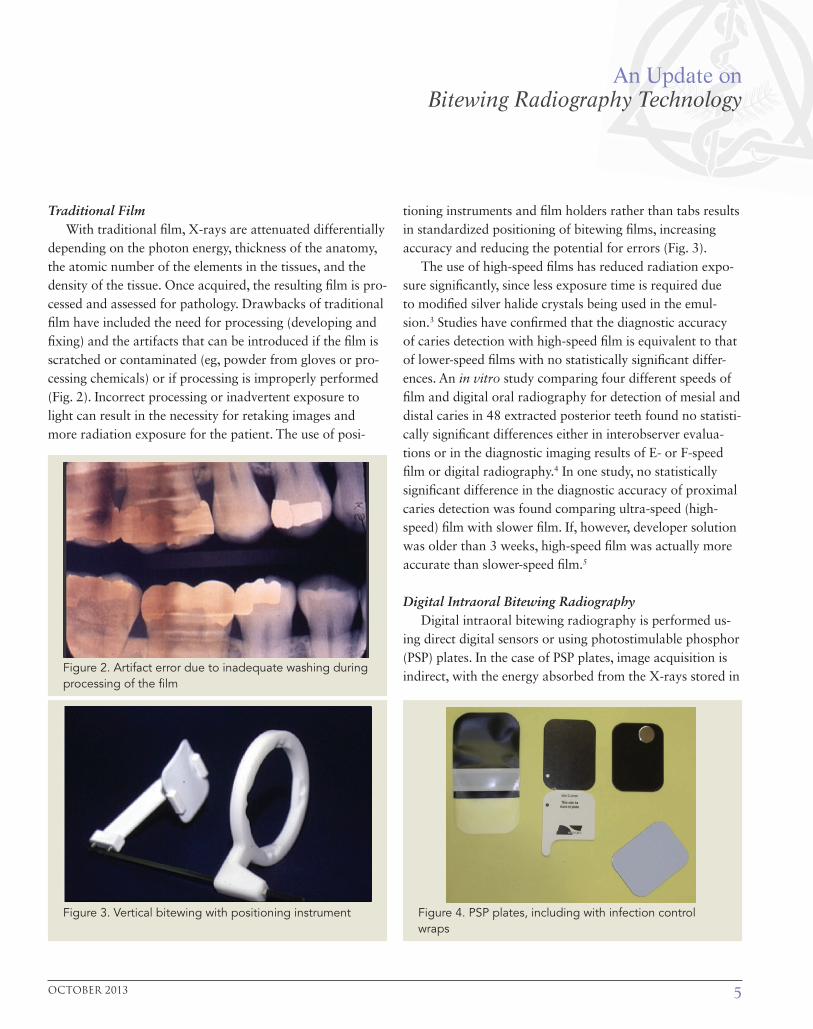
Traditional FilmWith traditional �lm, X-rays are attenuated differentially
depending on the photon energy, thickness of the anatomy, the atomic number of the elements in the tissues, and the density of the tissue. Once acquired, the resulting �lm is pro-cessed and assessed for pathology. Drawbacks of traditional �lm have included the need for processing (developing and �xing) and the artifacts that can be introduced if the �lm is scratched or contaminated (eg, powder from gloves or pro-cessing chemicals) or if processing is improperly performed (Fig. 2). Incorrect processing or inadvertent exposure to light can result in the necessity for retaking images and more radiation exposure for the patient. The use of posi-
tioning instruments and �lm holders rather than tabs results in standardized positioning of bitewing �lms, increasing accuracy and reducing the potential for errors (Fig. 3).
The use of high-speed �lms has reduced radiation expo-sure signi�cantly, since less exposure time is required due to modi�ed silver halide crystals being used in the emul-sion.3 Studies have con�rmed that the diagnostic accuracy of caries detection with high-speed �lm is equivalent to that of lower-speed �lms with no statistically signi�cant differ-ences. An in vitro study comparing four different speeds of �lm and digital oral radiography for detection of mesial and distal caries in 48 extracted posterior teeth found no statisti-cally signi�cant differences either in interobserver evalua-tions or in the diagnostic imaging results of E- or F-speed �lm or digital radiography.4 In one study, no statistically signi�cant difference in the diagnostic accuracy of proximal caries detection was found comparing ultra-speed (high-speed) �lm with slower �lm. If, however, developer solution was older than 3 weeks, high-speed �lm was actually more accurate than slower-speed �lm.5
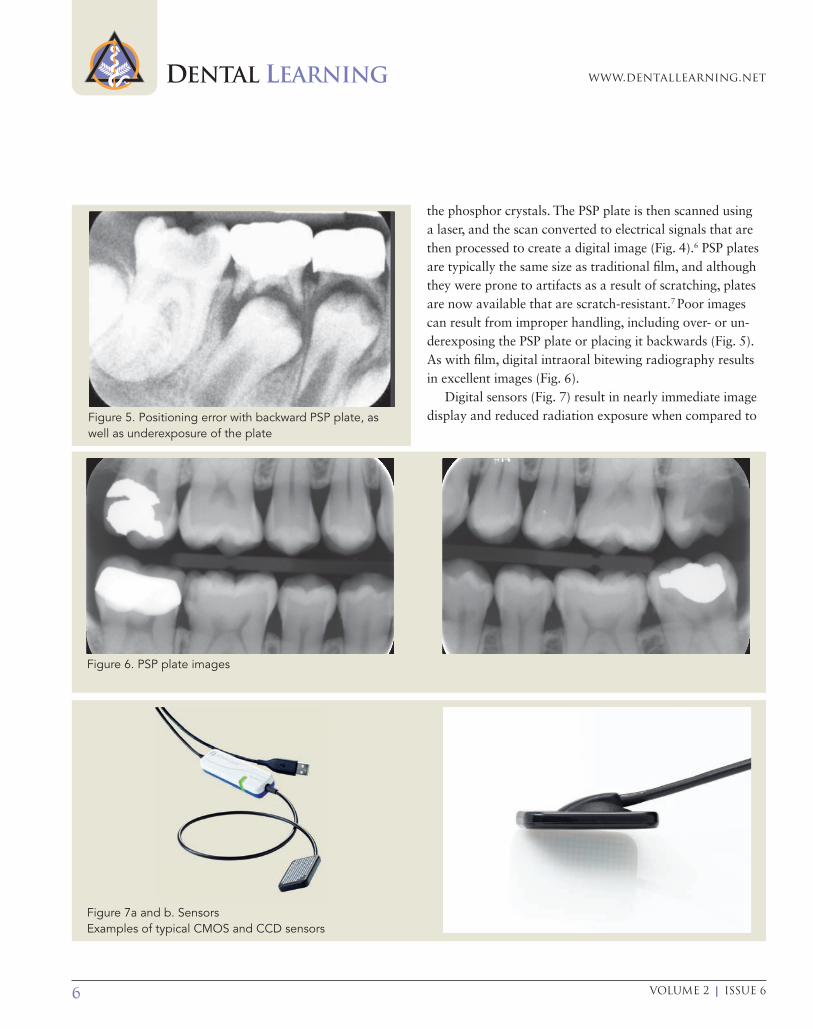
Digital Intraoral Bitewing RadiographyDigital intraoral bitewing radiography is performed us-
ing direct digital sensors or using photostimulable phosphor (PSP) plates. In the case of PSP plates, image acquisition is indirect, with the energy absorbed from the X-rays stored in
Figure 3. Vertical bitewing with positioning instrument
Figure 2. Artifact error due to inadequate washing during processing of the �lm
Figure 4. PSP plates, including with infection control wraps
DENTAL LEARNING www.dentallearning.net
6 VOLUME 2 | ISSUE 6
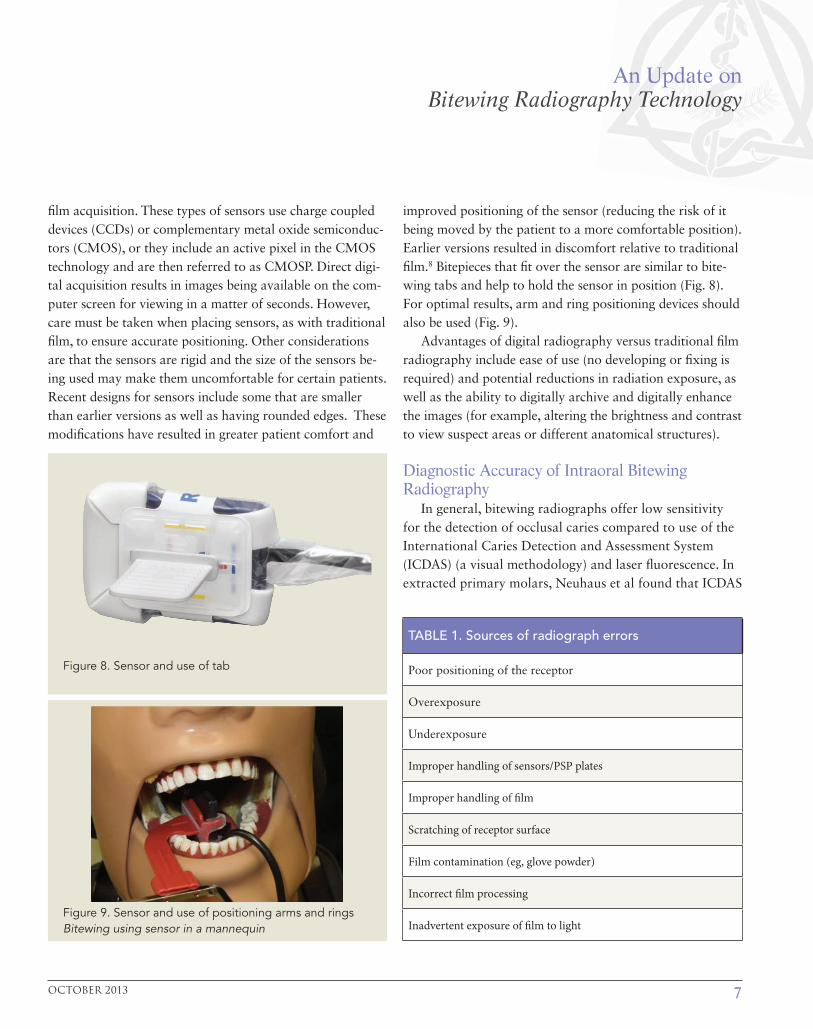
the phosphor crystals. The PSP plate is then scanned using a laser, and the scan converted to electrical signals that are then processed to create a digital image (Fig. 4).6 PSP plates are typically the same size as traditional � lm, and although they were prone to artifacts as a result of scratching, plates are now available that are scratch-resistant.7 Poor images can result from improper handling, including over- or un-derexposing the PSP plate or placing it backwards (Fig. 5). As with � lm, digital intraoral bitewing radiography results in excellent images (Fig. 6).
Digital sensors (Fig. 7) result in nearly immediate image display and reduced radiation exposure when compared to
Figure 6. PSP plate images
Figure 7a and b. SensorsExamples of typical CMOS and CCD sensors
Figure 5. Positioning error with backward PSP plate, as well as underexposure of the plate
An Update on Bitewing Radiography Technology
7OCTOBER 2013
�lm acquisition. These types of sensors use charge coupled devices (CCDs) or complementary metal oxide semiconduc-tors (CMOS), or they include an active pixel in the CMOS technology and are then referred to as CMOSP. Direct digi-tal acquisition results in images being available on the com-puter screen for viewing in a matter of seconds. However, care must be taken when placing sensors, as with traditional �lm, to ensure accurate positioning. Other considerations are that the sensors are rigid and the size of the sensors be-ing used may make them uncomfortable for certain patients. Recent designs for sensors include some that are smaller than earlier versions as well as having rounded edges. These modi�cations have resulted in greater patient comfort and
improved positioning of the sensor (reducing the risk of it being moved by the patient to a more comfortable position). Earlier versions resulted in discomfort relative to traditional �lm.8 Bitepieces that �t over the sensor are similar to bite-wing tabs and help to hold the sensor in position (Fig. 8). For optimal results, arm and ring positioning devices should also be used (Fig. 9).
Advantages of digital radiography versus traditional �lm radiography include ease of use (no developing or �xing is required) and potential reductions in radiation exposure, as well as the ability to digitally archive and digitally enhance the images (for example, altering the brightness and contrast to view suspect areas or different anatomical structures).
Diagnostic Accuracy of Intraoral Bitewing Radiography
In general, bitewing radiographs offer low sensitivity for the detection of occlusal caries compared to use of the International Caries Detection and Assessment System (ICDAS) (a visual methodology) and laser �uorescence. In extracted primary molars, Neuhaus et al found that ICDAS
Figure 9. Sensor and use of positioning arms and rings Bitewing using sensor in a mannequin
Figure 8. Sensor and use of tab
TABLE 1. Sources of radiograph errors
Poor positioning of the receptor
Overexposure
Underexposure
Improper handling of sensors/PSP plates
Improper handling of �lm
Scratching of receptor surface
Film contamination (eg, glove powder)
Incorrect �lm processing
Inadvertent exposure of �lm to light

DENTAL LEARNING www.dentallearning.net
8 VOLUME 2 | ISSUE 6
and laser �uorescence devices offered greater accuracy for occlusal caries detection.9 In other studies of occlusal car-ies detection, a bitewing radiograph was found to be less accurate than other methods. Diniz et al studied occlusal caries in permanent molars in an in vivo study, comparing the use of ICDAS, bitewing radiography, laser �uorescence and a �uorescence camera. Histological comparison was used as the gold standard after extraction. Visual inspec-tion (ICDAS) was found to be more accurate than bitewing radiography and the �uorescence camera.10 Another study using the same detection methods for occlusal surfaces in primary molars found that bitewings offered the highest speci�city at the D1 lesion level. However, overall, for the detection of both enamel and dentinal lesions, bitewing radiography offered less speci�city and sensitivity than the other methods used.11 On proximal surfaces in extracted primary molars (n=135), Chawla et al compared car-ies detection with laser �uorescence, digital radiography and transillumination. Histology sections were used as the gold standard against which speci�city and sensitivity were measured. Visual inspection was the most accurate detection method for dentinal lesions and the second most accurate for enamel plus dentinal lesions, while digital radiography was most accurate for dentinal lesions and the second most accurate method for enamel plus dentinal lesions. Transillumination and laser �uorescence were less accurate than either digital radiography or visual inspec-tion. Although visual inspection was found to be the most accurate, these were proximal lesions and in vivo this would be possible only if suf�cient spacing was present or if interproximal wedges were used.12 Bitewing radiographs were found in another study to be more accurate than visual inspection of visible proximal lesions once the lesion reached beyond the outer third of the dentin.13
Given that bitewings are primarily indicated for the detection and monitoring of proximal caries in the presence of contact points (ie, where the surfaces are not accessible for visual inspection), the more interesting question is the di-agnostic accuracy of intraoral bitewing radiography for the detection of proximal caries.
Proximal Caries Detection with Intraoral Bitewing Radiography
In combination with visual inspection, bitewing radiog-raphy has been found to be diagnostically accurate for the detection of proximal caries. Studies have compared the use of faster-speed �lm versus slower-speed �lm and the accuracy of traditional �lm bitewing radiography versus digital intraoral bitewing radiography. In a comparison of proximal caries diagnostic accuracy with traditional X-ray �lms (Ektaspeed Plus) and digital radiography with a charge-coupled (CMOS) sensor, an assessment by 6 ob-servers of the proximal surfaces of 40 extracted teeth using these techniques led to the conclusion that these techniques were similar, with no statistically signi�cant differences in diagnostic accuracy for the �lm or low- or high-resolution digital radiographs (P = 0.70).14 In contrast, in a study comparing the use of E- or F-speed �lm with digital radiography (CCD) for the detection of proximal caries in the mixed dentition, with 5 pediatric dentists assessing 270 proximal surfaces in extracted teeth (primary canine to �rst permanent molar), it was found that the diagnos-tic accuracy of the clinicians, using a 4-point scale, was greater with the use of E- or F-speed �lm than with digital radiography. However, the accuracy of some of the observ-ers increased the second time they viewed the direct digital images. Comparisons were made with histology sections of all observed teeth to determine the actual versus diagnosed proximal caries.15 Another study, involving 48 extracted posterior permanent teeth, found no statistically signi�cant differences in the diagnostic accuracy of traditional bite-wing �lm and digital intraoral radiographs for the detec-tion of proximal caries.16
Hintze et al assessed the diagnostic accuracy of proxi-mal enamel caries and occlusal dentinal caries detection using D- or E-speed �lm or digital radiography. The study included 122 proximal surfaces assessed by 3 observers and 65 occlusal surfaces assessed by 2 observers. The evaluations were also compared with histology sections of all sampled teeth. No statistically signi�cant differences were found in the accuracy of any of the methods stud-

An Update on Bitewing Radiography Technology
9OCTOBER 2013
ied, although all were found to be of very limited value in detecting proximal enamel caries and of some value in the detection of dentinal occlusal caries.17 In a study of 56 premolar surfaces, two different E-speed �lms, two CCD digital radiography brands and two PSP digital radiog-raphy brands were compared. No statistically signi�cant differences were found in the diagnostic accuracy of any of the methodologies used.18
The diagnostic �delity of both traditional �lm and digital radiographic images is in�uenced by the manner in which these receptors are handled and processed. Artifacts with traditional �lm include areas on the �lm that have been
scratched, where deposits were present during processing (eg, powder from gloves), and due to contamination by developer and �xer. In digital radiography, image process-ing can result in artifacts that appear to be pathological lesions, as con�rmed in a 2011 audience participation test at a specialist radiographic conference.19 Therefore, regard-less of the method used, attention to detail and following a standard protocol are essential.
In summary, overall studies of �lm and intraoral digital bitewing radiography support the accuracy of both tech-niques for the detection and monitoring of proximal caries lesions.20,21,22,23
Figure 10. Overlapping proximal surfaces on a panoramic radiograph
DENTAL LEARNING www.dentallearning.net
10 VOLUME 2 | ISSUE 6
Panoramic and Extraoral Panoramic Bitewing Radiography
Traditional panoramic radiography provides an over-view of the maxilla and mandible in 1 two-dimensional image. Panoramic radiography, however, is known to have low diagnostic capabilities for the detection of proximal car-ies, in part due to the overlapping of proximal surfaces on the radiograph and to decreased resolution when compared to intraoral imaging (Fig. 10). Several studies have been conducted comparing the diagnostic accuracy of extraoral and intraoral radiography.
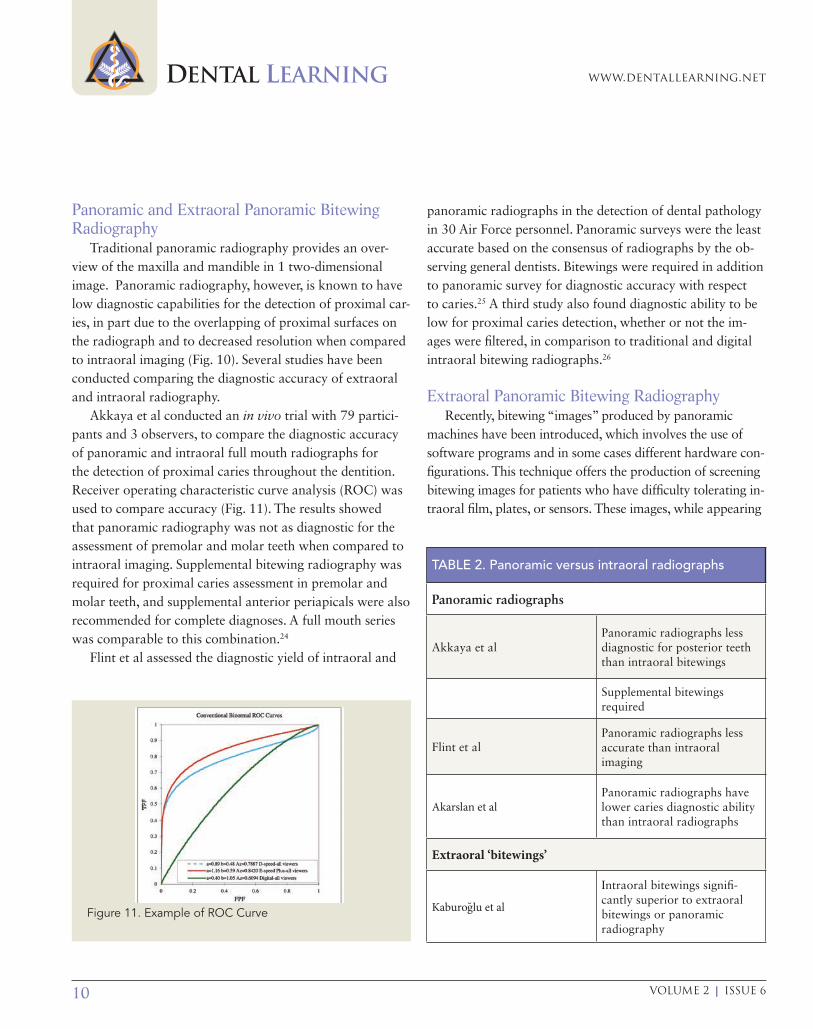
Akkaya et al conducted an in vivo trial with 79 partici-pants and 3 observers, to compare the diagnostic accuracy of panoramic and intraoral full mouth radiographs for the detection of proximal caries throughout the dentition. Receiver operating characteristic curve analysis (ROC) was used to compare accuracy (Fig. 11). The results showed that panoramic radiography was not as diagnostic for the assessment of premolar and molar teeth when compared to intraoral imaging. Supplemental bitewing radiography was required for proximal caries assessment in premolar and molar teeth, and supplemental anterior periapicals were also recommended for complete diagnoses. A full mouth series was comparable to this combination.24
Flint et al assessed the diagnostic yield of intraoral and
panoramic radiographs in the detection of dental pathology in 30 Air Force personnel. Panoramic surveys were the least accurate based on the consensus of radiographs by the ob-serving general dentists. Bitewings were required in addition to panoramic survey for diagnostic accuracy with respect to caries.25 A third study also found diagnostic ability to be low for proximal caries detection, whether or not the im-ages were �ltered, in comparison to traditional and digital intraoral bitewing radiographs.26
Extraoral Panoramic Bitewing RadiographyRecently, bitewing “images” produced by panoramic
machines have been introduced, which involves the use of software programs and in some cases different hardware con-�gurations. This technique offers the production of screening bitewing images for patients who have dif�culty tolerating in-traoral �lm, plates, or sensors. These images, while appearing
Figure 11. Example of ROC Curve
TABLE 2. Panoramic versus intraoral radiographs
Panoramic radiographs
Akkaya et alPanoramic radiographs less diagnostic for posterior teeth than intraoral bitewings
Supplemental bitewings required
Flint et alPanoramic radiographs less accurate than intraoral imaging
Akarslan et alPanoramic radiographs have lower caries diagnostic ability than intraoral radiographs
Extraoral ‘bitewings’
Kaburoglu et al
Intraoral bitewings signi�-cantly superior to extraoral bitewings or panoramic radiography
An Update on Bitewing Radiography Technology
11OCTOBER 2013
similar to intraoral bitewings, frequently exhibit horizontal overlap of the premolar contacts and often lack the resolution necessary to clearly de�ne the true extent of caries.
Diagnostic AccuracyIn a study comparing extraoral bitewing radiography,
traditional high-speed �lm radiography, and panoramic radiography, 80 extracted molar and premolar teeth were evaluated by 3 observers twice for the detection of mesial and distal caries, and the diagnoses compared with gold standard histology sections of the teeth. The assessment of accuracy used the Receiver Operating Characteristics (ROC) test, which considers both sensitivity and speci�city curves. No statistically signi�cant differences in accuracy were found between the extraoral bitewings and extraoral panoramic radiographs. Statistically signi�cant differences
in diagnostic accuracy were found between intraoral and extraoral bitewing radiographs, with intraoral bitewing radiography found to be signi�cantly superior to the use of extraoral bitewing and panoramic radiography and with similar results found for each observer and between observ-ers.27
Radiation ExposureAcquiring clinically justi�ed radiographs also involves con-
sideration of the risks and bene�ts of radiation exposure. The ALARA (As Low As Reasonably Achievable) principle serves as a guideline to all diagnostic imaging in dentistry.
Methods to reduce exposure to radiation also include using lead aprons during imaging and using rectangular col-limation. Lead collars, which protect the thyroid, should also be used, except when taking panoramic radiographs as they obstruct taking these radiographs.28 Signi�cant reductions in radiation result from these precautions. Acquiring as few radiographs as necessary for diagnosis and only when they are needed, selecting radiograph imaging that results in less exposure to radiation and taking care to use a precise tech-nique to avoid retakes all helps to reduce potential radiation exposure.29
When acquiring intraoral bitewing radiographs, appropri-ate collimation and �ltration of the X-ray beam will reduce
TABLE 3. Methods for reducing radiation exposure
Rectangular collimation
X-ray �lter
Lead aprons
Lead collar
Take only essential radiographs
Use of positioning arms and rings
Avoid overexposure
Avoid underexposure
A precise technique
Select methods with least exposure
High-speed if traditional �lm
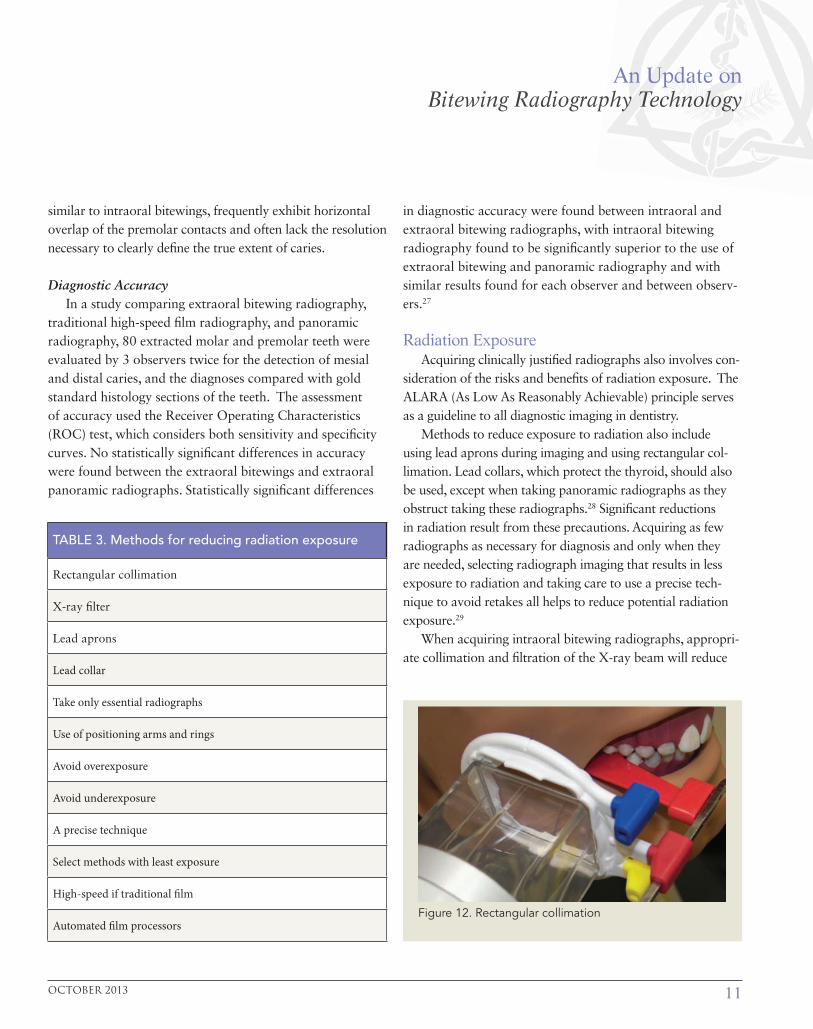
Automated �lm processorsFigure 12. Rectangular collimation

DENTAL LEARNING www.dentallearning.net
12 VOLUME 2 | ISSUE 6
exposure to radiation. There are two types of collimation — rectangular and circular. Rectangular collimation reduces the X-ray beam exposure area considerably compared to circular collimation, decreasing scatter (Fig. 12). Reducing scatter will improve image quality, aiding diagnosis and reduc-ing the likelihood of a retake being necessary. Higher-speed traditional bitewing �lms have reduced the time required to take the radiograph, reducing exposure compared to older, slower-speed (D) �lms. Automated �lm processors also help to reduce processing errors and the need for retakes.
With earlier versions of panoramic �lm radiography ver-sus �lm bitewings, the reduction in radiation exposure was up to 50%; however, the use of faster-speed �lms and digital imaging has reduced these differences. Also, although pan-oramic radiographs result in less radiation exposure than a full-mouth series, for caries detection supplemental bitewing radiographs are necessary to improve caries diagnoses, and extraoral panoramic bitewing radiography is less accurate than intraoral radiography.30 Compared to traditional bite-wing radiographs, digital bitewing radiography in principle offers a lower radiation dose. Care must be taken to capture images that offer diagnostic ability and to avoid retakes by following sound protocols, and all principles of ALARA should be followed when performing oral radiography.
ConclusionRadiographic imaging is an integral tool in the assess-
ment and diagnosis of dental caries. The evidence clearly shows that with prudent and careful consideration of its use, intraoral bitewing imaging is still the modality of choice when assessing the presence and extent of caries in proxi-mal tooth structure. While techniques such as panoramic bitewing imaging are being further developed to use in diagnosis, it remains to be seen if the evidence will support its exclusive use for complete diagnoses.
References1. Pine CM, ten Bosch JJ. Dynamics of and diagnostic methods for detecting small carious lesions. Caries Res. 1996; 30: 381–8.
2. Cawson RA, Odell EW. Cawson’s essentials of oral pathology and oral medicine. New York: Churchill Living-stone; 2002.
3. ibid.
4. Alkurt MT, Peker I, Bala O, Altunkaynak B. In vitro comparison of four different dental X-ray films and direct digital radiography for proximal caries detection. Oper Dent. 2007 Sep-Oct;32(5):504-9.
5. Syriopoulos K, Velders XL, Sanderink GC, van Ginkel FC, van Amerongen JP, van der Stelt PF. The effect of develop-er age on the detection of approximal caries using three dental films. Dentomaxillofac Radiol. 1999 Jul;28(4):208-13.
6. Wenzel A. Digital imaging for dental caries. Dent Clin North Am. 2000; 44: 319–38.
7. Bedard A, Davis TD, Angelopoulos, C. Storage phos-phor plates: How durable are they as a digital dental radio-graphic system? J Contemp Dent Pract. 2004;5:57-69.
8. Versteeg CH, et al. An evaluation of periapical radiogra-phy with a charge-coupled device. Dentomaxillofac Radiol. 1998;27:97-101.
9. Neuhaus KW, Rodrigues JA, Hug I, Stich H, Lussi A. Per-formance of laser fluorescence devices, visual and radio-graphic examination for the detection of occlusal caries in primary molars. Clin Oral Investig. 2011 Oct;15(5):635-41.
10. Diniz MB, Boldieri T, Rodrigues JA, Santos-Pinto L, Lussi A, Cordeiro RC. The performance of conventional and fluorescence-based methods for occlusal caries detec-tion: an in vivo study with histologic validation. J Am Dent Assoc. 2012 Apr;143(4):339-50.
11. Souza JF, Boldieri T, Diniz MB, Rodrigues JA, Lussi A, Cordeiro RC. Traditional and novel methods for occlusal caries detection: performance on primary teeth. Lasers Med Sci. 2013 Jan;28(1):287-95.
12. Chawla N, Messer LB, Adams GG, Manton DJ. An in vi-tro comparison of detection methods for approximal cari-ous lesions in primary molars. Caries Res. 2012;46(2):161-9.
13. Ekstrand KR, Luna LE, Promisiero L, Cortes A, Cuevas S, Reyes JF, Torres CE, Martignon S. The reliability and accuracy of two methods for proximal caries detection and depth on directly visible proximal surfaces: an in vitro study. Caries Res. 2011;45(2):93-9.
14. Abreu M Jr, Mol A, Ludlow JB. Performance of RVGui

An Update on Bitewing Radiography Technology
13OCTOBER 2013
sensor and Kodak Ektaspeed Plus film for proximal caries detection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001 Mar;91(3):381-5.
15. Uprichard KK, Potter BJ, Russell CM, Schafer TE, Adair S, Weller RN. Comparison of direct digital and conven-tional radiography for the detection of proximal surface caries in the mixed dentition. Pediatr Dent. 2000 Jan-Feb;22(1):9-15.
16. Peker I, Toraman Alkurt M, Altunkaynak B. Film tomog-raphy compared with film and digital bitewing radiography for proximal caries detection. Dentomaxillofac Radiol. 2007 Dec;36(8):495-9.
17. Hintze H, Wenzel A, Jones C. In vitro comparison of D- and E-speed film radiography, RVG, and visualix digital radiography for the detection of enamel ap-proximal and dentinal occlusal caries lesions. Caries Res. 1994;28(5):363-7.
18. Syriopoulos K, Sanderink GC, Velders XL, van der Stelt PF. Radiographic detection of approximal caries: a comparison of dental films and digital imaging systems. Dentomaxillofac Radiol. 2000 Sep;29(5):312-8.
19. Brettle D, Carmichael F. The impact of digital im-age processing artifacts mimicking pathological fea-tures associated with restorations. Br Dent J. 2011 Aug 26;211(4):167-70.
20. Wenzel A. A review of dentists’ use of digital radiogra-phy and caries diagnosis with digital systems. Dentomaxil-lofac Radiol. 2006;35(5):307-14.
21. Senel B, Kamburoglu K, Ucok O, et al. Diagnostic accuracy of different imaging modalities in detection of proximal caries. Dentomaxillofac Radiol. 2010;39(8):501-11.
22. Pontual AA, de Melo DP, de Almeida SM, et al. Com-parison of digital systems and conventional dental film for the detection of approximal enamel caries. Dentomaxillo-fac Radiol. 2010;39(7):431-6.
23. Castro VM, Katz JO, Hardman PK, et al. In vitro com-parison of conventional film and direct digital imaging in the detection of approximal caries. Dentomaxillofac Radiol. 2007;36(3):138-42.
24. Akkaya N, Kansu O, Kansu H, Cagirankaya LB, Arslan
U. Comparing the accuracy of panoramic and intraoral ra-diography in the diagnosis of proximal caries. Dentomaxil-lofac Radiol. 2006 May;35(3):170-4.
25. Flint DJ, Paunovich E, Moore WS, Wofford DT, Her-mesch CB. A diagnostic comparison of panoramic and intraoral radiographs. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jun;85(6):731-5.
26. Akarslan ZZ, Akdevelio�lu M, Güngör K, Erten H. A comparison of the diagnostic accuracy of bitewing, peri-apical, unfiltered and filtered digital panoramic images for approximal caries detection in posterior teeth. Dentomax-illofac Radiol. 2008 Dec;37(8):458-63.
27. Kamburoglu K, Kolsuz E, Murat S, Yüksel S, Ozen T. Proximal caries detection accuracy using intraoral bite-wing radiography, extraoral bitewing radiography and panoramic radiography. Dentomaxillofac Radiol. 2012 Sep;41(6):450-9.
28. National Council on Radiation Protection and Measure-ments. Radiation Protection in Dentistry. NCRP Report No. 145. Bethesda, MD. NCRP 2003, Revised 2004;14-27.
29. Williamson GF. Intraoral Radiography: Positioning and Radiation Protection. Academy of Dental Therapeutics and Stomatology, Chesterland, OH, 2007.
30. Molander B, Ahlqwist M, Gröndahl HG. Panoramic and restrictive intraoral radiography in comprehen-sive oral radiographic diagnosis. Eur J Oral Sci. 1995 Aug;103(4):191-8.
WebliographyAmerican Dental Association. Dental radiographs. Benefits and safety. Available at: http://www.ada.org/ sections/scienceAndResearch/pdfs
Federal Drug Administration. The Selection of Patients for Dental Radiographic Examinations. (2012). Retrieved on June 6, 2013, from http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsand Procedures/ MedicalImaging/MedicalX-Rays/ucm116504.htm#patient_selection_criteria
DENTAL LEARNING www.dentallearning.net
14 VOLUME 2 | ISSUE 6
1. The overall goal of caries detection is to __________.a. determine whether caries is present b. determine the extent of cariesc. detect caries at an early staged. all of the above
2. When photostimulable phosphor (PSP) plates are used for im-ages, their acquisition is __________.a. indirectb. directc. inferior to traditional �lmd. none of the above
3. Radiography for caries detection and assessment involves the differential __________ of X-rays through hard tooth structure that is sound or partially demineralized. a. re�ectionb. attenuationc. scatteringd. refraction
4. High-speed traditional �lms involve the use of __________ in the emulsion.a. modi�ed silver halide crystalsb. modi�ed silver iodide crystalsc. modi�ed silver bromide crystalsd. none of the above
5. Sensitivity refers to the ability of a test to correctly identify when a condition is __________. a. presentb. absentc. amelioratingd. none of the above
6. Speci�city refers to the ability of images to detect __________. a. the extent and severity of a lesionb. the absence of a lesionc. the presence of anomaliesd. all of the above
7. Intraoral bitewing radiography has been performed since the introduction of X-rays in dentistry, primarily for the detection of __________ lesions.a. periapical b. proximal cariousc. occlusal cariousd. b and c
8. The __________ affects the attenuation of X-rays used for traditional �lm. a. photon energyb. thickness of the anatomy and density of the tissue being
radiographed c. atomic number of the elements in the tissues being
radiographedd. all of the above
9. The use of positioning instruments and �lm holders rather than ‘tabs’ results in __________.a. standardized positioning of bitewing �lmsb. increased accuracyc. reduced potential for errorsd. all of the above
10. Studies have con�rmed that the diagnostic accuracy of caries detection with high-speed �lm is __________ to that of lower-speed �lms, with no statistically signi�cant differences. a. inferiorb. equivalentc. superiord. none of the above
11. __________ lesions are the most dif�cult to detect radiographically.a. Dentinalb. Advancedc. Incipientd. Pulpal
12. PSP plates are __________.a. typically the same size as traditional �lmb. now available as plates that are scratch-resistantc. prone to chemical contaminationd. a and b
13. Digital sensors result in __________. a. nearly immediate image display b. indirect image acquisitionc. reduced radiation exposure when compared to �lm acquisition d. a and c
14. __________ is an advantage of digital radiography versus tradi-tional �lm radiography. a. Ease of useb. Potential reductions in radiation exposure c. The ability to digitally archive and enhance images d. all of the above
CEQuizTo complete this quiz online and immediately download your CE veri�cation document, visit www.dentallearning.net/BWT-ce, then log into your account (or register to create an account). Upon completion and passing of the exam, you can immediately download your CE veri�cation document. We accept Visa, MasterCard, and American Express.

An Update on Bitewing Radiography Technology
15OCTOBER 2013
15. __________ can cause an artifact on traditional �lm images.a. Scratches on the �lmb. Powder on the �lm from glovesc. Contamination by �xer and developerd. all of the above
16. Proximal caries diagnostic accuracy with traditional high-speed X-ray �lms and digital radiography with a charge-coupled sensor have overall been found to be __________.a. equally accurate diagnosticallyb. inferior to PSPc. differentially accurated. none of the above
17. The diagnostic �delity of traditional �lm and digital radiographic images is in�uenced by __________. a. the manner in which these receptors are handled and processed b. the size of the lesionc. the X-ray beamd. none of the above
18. Receiver operating characteristic curve analysis is used to compare the __________ of radiography techniques.a. imagesb. accuracyc. costd. all of the above
19. Panoramic radiography is known to have low diagnostic capabilities for the detection of proximal caries, in part due to the __________. a. overlapping of proximal surfaces on the radiograph b. size of the �lm c. decreased resolution when compared to intraoral imaging d. a and c
20. If using panoramic radiography, __________ are required for proximal caries assessment in premolar and molar teeth.a. supplemental periapical radiographsb. supplemental bitewing radiographsc. supplemental lateral �lmsd. all of the above
21. Bitewing images produced by panoramic machines __________.a. involve the use of software programsb. in some cases involves different hardware con�gurations c. are necessaryd. a and b
22. Reducing scatter __________. a. improves image quality b. aids diagnosisc. reduces the likelihood of a retake being necessary d. all of the above
23. Panoramic bitewing images offer the production of bitewings for patients who have dif�culty tolerating __________. a. intraoral �lm b. platesc. sensors d. all of the above
24. __________ is/are a frequent occurrence with panoramic bitewing images. a. Horizontal overlap of the premolar contacts b. Vertical overlap of the molar contact c. Artifacts d. all of the above
25. Intraoral bitewing radiography has been found to be __________ to the use of extraoral bitewing and panoramic radiography.a. signi�cantly superiorb. signi�cantly inferiorc. equivalentd. none of the above
26. The ALARA principle is related to radiation exposure and stands for __________. a. ‘As Low As Reasonably Accessible’ b. ‘As Low As Reasonably Achievable’c. ‘As Light As Reasonably Achievable’d. none of the above
27. Lead collars __________.a. protect the thyroid b. should be used when taking any radiographc. should be used except when taking panoramic radiographs
as they obstruct the taking of these radiographsd. a and c
28. Using __________ is a method to reduce exposure to radiation. a. a lead apronb. a lead collarc. rectangular collimationd. all of the above
29. __________ collimation reduces the X-ray beam exposure area considerably compared to __________ collimation.a. Circular; verticalb. Circular; rectangularc. Rectangular; circulard. Rectangular; oblique
30. Compared to __________, __________ in principle offer a lower radiation dose.a. digital bitewing radiography; traditional bitewing radiographsb. traditional bitewing radiographs; digital bitewing radiographyc. traditional bitewing radiographs; chest X-raysd. none of the above
CE QUIZ
Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. COURSE EVALUATION and PARTICIPANT FEEDBACK: We encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. INSTRUCTIONS: All questions should have only one answer. Participants will receive con�rmation of passing by receipt of a veri�cation form. Veri�cation forms will be mailed within two weeks after taking an examina tion. EDUCATIONAL DISCLAIMER: The content in this course is derived from current information and evidence. Any opinions of ef�cacy or perceived value of any products mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily re�ect those of Dental Learning. Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the �eld related to the course topic. It is a combination of many educa-tional courses and clinical experience that allows the participant to develop skills and expertise. COURSE CREDITS/COST: All participants scoring at least 70% on the examination will receive a veri�cation form verifying 2 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact Dental Learning, LLC for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. Dental Learning, LLC is a California Provider. The California Provider number is RP5062. The cost for courses ranges from $29.00 to $110.00. Many Dental Learning, LLC self-study courses have been approved by the Dental Assisting National Board, Inc. (DANB). To �nd out if this course or any other Dental Learning, LLC course has been approved by DANB, please RECORD KEEPING: Dental Learning, LLC maintains records of your successful completion of any exam. Please contact our of�ces for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within �ve business days of receipt. CANCELLATION/REFUND POLICY: Any participant who is not 100% satis�ed with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. © 2013
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
21. A B C D
22. A B C D
23. A B C D
24. A B C D
25. A B C D
26. A B C D
27. A B C D
28. A B C D
29. A B C D
30. A B C D
Fill in the circle of the appropriate answer that corresponds to the question on previous pages.
EDUCATIONAL OBJECTIVES• Review the types of oral radiographs used for caries detection• De�ne sensitivity and speci�city • Contrast and compare the methodology and results for radiographic caries detection• List and describe the methods by which radiation exposure is reduced as well as the relative
radiation exposure with different radiographic methodologies for caries detection.
If you have any questions, please email [email protected] or call Dental Learning at 888-724-5230.
CE ANSWER FORM (E-mail address required for processing)
To obtain credits:
1. Read the entire course.
2. Complete this entire answer sheet in either pen or pencil.
3. Mark only one answer for each question.
4. A score of 70% will earn your credits.
OR
For Immediate results:
1. Read the entire course
2. Go to www.dentallearning.net/EIT-ce
3. Choose this course from the course listing
4. Log in to your account or register to create an account
5. Complete course and submit for grading to receive your CE veri�cation document
Dental Learning, LLC
500 Craig Road, Floor One
Manalapan, NJ 07726
*If paying by credit card, please note:
Master Card | Visa | AmEx | Discover
*Account Number ______________________________
*Expiration Date _______________________________
The $29 charge will appear as Dental Learning, LLC.
If paying by check, make check payable to Dental Learning, LLC.
AGD Code: 130
ALL FIELDS MARKED WITH AN ASTERISK (*) ARE REQUIRED
COURSE EVALUATIONPlease evaluate this course using a scale of 5 to 1, where 5 is excellent and 1 is poor
1. To what extent were the course objectives accomplished overall? 5 4 3 2 1
2. Please rate your overall mastery of the educations objectives? 5 4 3 2 1
3. How would you rate the educational methods? 5 4 3 2 1
4. How do you rate the author’s mastery of the topic? 5 4 3 2 1
5. Please rate the instructor’s effectiveness. 5 4 3 2 1
6. Do you feel the references were adequate? 5 4 3 2 1
7. Would you participate in a similar course? 5 4 3 2 1
8. Was any subject matter confusing – please describe. 5 4 3 2 1
Price: $29 CE Credits: 2Save time and the environment by taking this course online.
An Update on Bitewing Radiography Technology
*Name: Title: Specialty:
*Address: *E-mail:
*City: *State: *Zip:
*Telephone: License renewal date: AGD Identi�cation No.
Practice Name NPI No.
VOLUME 2 | ISSUE 616
CA Dental Professionals: Will you need a CA veri�cation form for the Dental Board of California? Yes n No n�e CA course code is 02-5062-13021.