Embed Size (px)
Citation preview

An Update On Pediatric
Endoscopy
Jie Chen , MD, phD
The Chidren’s Hospital of Zhejiang University School of Medicine
2016-3-4 Xi’an 2016CIP

Indication
• Diagonostic endoscopy
– Esophagogastroduodenoscopy (EGD)
– Colonoscopy
Routeine
•Acid peptic disease
•Suspion of mucosal inflammation
•Chronic diarrhea/malabsorption
•Chronic abdominal pain (with anemia,weight loss, vomiting)
•Hematemesia or enema,hematochezia
•Dsphagia or odynophagia
•Caustic ingestion,forgein body ingestion
•Recuurent vomiting
•GER,faliure for thrive…….
•Lower GI hemorrhage
•Chronic diarrhea
•Suspected IBD
•Cancer survellance(IBD, polyposis syndrome)
•Low GI tract lessions seen on imaging study
•Others:anemia unexplained, faliure to thrive, abdominal
pain…..

Indication
• Diagonostic endoscopy
– Esophagogastroduodenoscopy (EGD)
– Colonoscopy
– Double ballon enteroscopy
– Wireless capsule endoscopy
Routeine
Investigation of the small intestine

Indication
• Therapeutic endoscopy – Polypectomy
– Foreign bodies removal
– Hemostasis
– Ligation of esophageal varices
– Reset(gastric vovulus,intessuception)
– Dilation of strictures
– Stent placement
– Catheter placement (nasogastrojejunal tube, PEG,PEGJ,PEJ)
– POEM
– ERCP
• Evaluation & Followup

Contraindication_ absolute
• Severe heart and pulmonary disease
• Shock
• gastrointestinal perforation
• Suspected Aneurism of thoracic aortic
• Stroke

Contraindication_relative
• Bleeding disorders
• Recent histroy of bowel surgery
• Toxic dilation of the bowel
• Partial or complete bowel obstruction
• Aneurism of abdoninal or ileac aorta
• Acute inflammation with errosive of mouth,
throat, and GI tract
• Mental illness

Personnel
• Physician: Pediatric gastoenterogists
• Assistant specially trained
– Meet , explain to child & hold, reasurre child
throughout procedure
– Abtain ,process tissure & assist other equipments
• Competent physician in anesthesia and
resusitation

Facilities and Equipment
• Routine endoscopy :outpatient setting,
Hospital bedside or operating room
• Occasionally, more invasive and therapeutic
procedure
• Equipment for monitoring: BP , pulse,SpO2
• emergency medication + resussitation
• Good endoscopy system with size and type
approptiated for pediatric use




Diagnostic Endoscopy

Duodenal ulcer & gastric ulcer

1.Peptic ulcer 2.Hemorrhagic gastritis
3 Deulifoy disease 4.Esophegeal varices
GI Bleeding

Colon polyps

Intestinal lymphangiectasis (duodenum)

Pseudomembranous colitis
‘’ ‘’

Eosinophilic esophagitis

Eosinophilic gastroenteritis

Ulcerative Colitis

UC & CD

HSP
gastric autrum spotting Spotting in duodenum
erosion&ulcer in duo Blue plaques in duo

Endoscopic diagnosis of small bowel
diseases

Diagnosis rate via routine techniques
• Radiology (KUB、SBFT)
• Abdominal ultrasound
• ECT
• Agiography
• EGD/Colonscpy
Diagostic rate
10%-15%

Endospopy for investigation of SBD
• EGD、colonoscopy
• Small bowel enteroscopy (SBE)
– Push enteroscopy
– Double ballon enteroscopy
• WCE
• EUS
• Intraoperative endoscopy
• Laparoscopy

EGD & colonoscopy in the diagnosis of
intestinal diseases
• EGD
– For observation of upper jejunum lesions in
patients with gastrojejunostomy
• Colonoscopy
– Be able to investigating the terminal ileum

EUS in the diagnosis of intestinal
diseases
• Valuable at duodenal lesions
– To identification of the inner wall and the outer
wall of the duodenum disease
– To investigation of duodenal periampullary tumor

SBE techniques
• Push enteroscopy
• 2.5 meter long push
eneroscopy
• Sona & rope way enteroscopy
• Bougie enteroscopy
• SBE
• DBE
In China better value in
unexplained intestinal
bleeding and small
bowel obstruction
Valuable to determine
the treatment options

DBE
• Oral or transanal
• Entire small bowel examination
• Indication – Obscure GI Bleeding
– Suspected crohns disease
– Angiography / GI imaging abnormality
– Chronic diarrhea or abdorminal pain _suspected SBD
– Multiple intestinal polypus
– Suspeted small intestine cancer
– Therapeutic intervention in small intestine

Ileum erosion Jejunum erosion Cobblestone levy (CD)
CD: Jejunum ulcer Intestinal bachet’s disease

Mechel’s diverticulum Diverticular ulcer

Disadvantages
• Technically difficult procedure
• Very time consuming (Procedure can take > 3 hours)
• Higher risk of small bowel perforation
• Case reports of pancreatitis and intestinal necrosis
• Reported incidents of aspiration and pneumonia

WCE evaluation of small intestine
• Obscure gastrointestinal bleeding and /or
anemia
• Evaluation of extent of small intestinal
disorders such as Crohn’s disease
• Small-intestinal abnormalities on SBFT or CT
• Suspected malabsorption
• Surveillance of polyposis syndromes
involving small intestine

Contraindications
Absolute:
• Suspected small intestinal obstruction
• Pregnancy
Relative:
• Motility disturbances: Gastroparesis/ Achalasia
• Small bowel diverticulosis
• Poor surgical candidates

Types of endoscopic capsule


Imaging rapid viewing system
QuickView v5
Setting Selectable:
High/Normal/Low
Image Adjustment
One-click on/off
IA button
Lewis
Score
Study Manager
A–Mode or M-
mode
(when RAPID
is M-mode
enabled)
(CapsuleEndoscopy.org, 2008)

WCE in pediatric patients
• The detection rate 50%
– New diagnosis: 49%
• Complication :
– Retention of capsule 1.5-2.2%
– Aspitation: rare
CD:83.3%
Obscure GI bleeding :73.3%

Phlebectasia Hemangioma
HSP Jejunum Bleeding

lymphoma GIST
Polypoid mass polyps

Meckel’s
diverticulum Intestinal lymphangiectasis
Sprue malabsorption

Crohn`s disease
Linar erosions
Linar erosion
ulceration
ileutitis
Inflammato
ry polyp

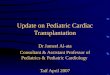
WCE for Crohn`s disease
• Diagonosis determination
• Management options
• Mucosal healing detection

0
1
2
3
4
5
6
7G
astr
ic
Duoden
Jeju
num
Ileum
J +
I
CD (n 21)
UC/IC (n 7)
Cohen et al. JPGN 2008;47(1):31-36.
Detection of new lesions

•5/7 (71%) UC/IC is CD
•13/21 (62%) CD
extesive small
intestine involved
•Modified medical cures
for the CD cases new
diagnosed
0
10
20
30
40
50
60
70
80
90
100
UC/IC CD
Reclassified
Cohen et al. JPGN 2008;47(1):31-36.
Reclassified diagnosis

0102030405060708090
100
diag
nosi
sde
cisi
ons
man
agem
ent
CE
N = 18
Gralnak et al, Digest Dis Sci 2011
Modified management option

Detection of mucosal healing
PRE PCDAI 30;
12Wks afte treatment PCDAI 10;
AZA

Proposed Algorithm For Diagnosis of
Suspected Crohn’s Disease
Colonoscopy/Ileoscopy +
Stop
_
Obstructive Symptoms?
_
Capsule Endoscopy
+
SBFT +
Stop
_

• WCE vs push enteroscopy
– 2 meta analysis:
• 63% vs. 28%
• 87% vs. 14.8%
• WCE vs SBFT
• 42% vs. 6%
• 87% vs. 9.9%
• CE vs DBE
• 60%vs 57%
Value of WCE for investigation of obscure
GI Bleeding
Treister et al. Am J Gastroenterol. 2005;39:684-8.
Lewis et al. Endoscopy. 2005;37:960-5.
Pasha et al. Clin Gastroenterol Hepatol. 2008;6:671-6.

Endospopy for investigation of SBD
• EGD、colonoscopy
• enteroscopy
– Push enteroscopy
– Double ballon enteroscopy
• WCE
• EUS
• Intraoperative endoscopy
• Laparoscopic

Therapeutic endoscopy

Polypctomy

Types of intestinal polyps

Indication
• Polyp on stalk , small or large
– Larger polyps can be divided into sub-removal
– Multiple polyps ,from distal to proximal, once or
more times
• Flat board polyp < 2cm
Contraindication
• Flat board polyp 2cm
• Familial adenomatous polyposis
• Intesive adema
• Endoscopy contraindication





complication
• Bleeding
• Burns
• Perforation

Cause of foreign body ingestion
• swallow 80% -90%
– (coins, button battery, keys, needle, clips。。。。。 )
• Gastrointestinal stenosis
• Iatrogenic
• Diospyrobezoar
• Other: mental illness, abuse

Endoscopic foreign body removal
• Indication
– At Upper GI foreign body or At large
intestine but cannot be discharged
– Emergency ,especially for sharp or toxic
• Contraindication
– Suspected perforation
– Huge forgein mass
– Endoscopy contraindication

Coins in esophagus

Date nutlet incarcerated in esophagus

Stapler nail in stomach

Duodenum_ needle

Upper GI bleeding control
• Non-variceal upper gastrointestinal bleeding
– PU
– Hemorragic gastritis
– Others
• Dieufoy disease, HSP, mellory-weiss
syndrom。。。
• Gastroesophageal varices
•Spout Hemostatic agents
•Ingection (histoacryl。。。)
•clips
Scelotherapy or ligation

Tetanium folder hemostasis

Esophageal varices sclerotherapy

Esophageal varices ligation

preoperative intraoperative
1 wk postoperative 4 months postoperative

Endoscopic treatment of
esophageal stenosis
• Dilation
– Ballon dilator
– Water ballon dilator
– Savary bougies
• Stent placement
• Laser
• Heat
• High frequency electrocoagulation

Water ballon dialation

Savary-Gilliard bougie dilation

Heat treatment for webbed esophagus

POEM for achalacia
(Peroral endoscopic myotomy)
— Fang Y, et al. 2015

Percutaneous Endoscopic gastrostomy
(PEG)
• Indication : Malnutrition due to various feeding
difficulty need long term nutritional support with
normal gastrointestinal function
– Dysphagia caused by Nervous diseases and
systemic disease
– Long term PN with infection
– Severe biliary fistula leading bile back to the
gastrointestinal tract
– EN more than 1 momths

PEG/PEGJ

Percutaneous Endoscopic Gastro-Jejeunostomy
(PEGJ)
• Not torelate gastric tube feeding
– Gastric relaxation
– Gastroesophageal reflux
• PEG ajusted to PEGJ
• Enteral Feeding tubes inserted into the
duodenum through the stomach feeding tube

PEGJ

Endoscopic retrograde
cholangiopancretography (ERCP)

ERCP
• To confirm duct stone
• To clear the cause and nature site of
obstruction judice
• To diagose chronic pancreatitis
• To get pacreatic juice for gene detection
• Only way to diagnose pancreas
schizophrenia

EST
• EST lithotomy
• Acute obstructive suppurative
cholangitis
• Acute gallstone pancreatitis
• Biliary obstruction
• Biliary stent placement

pancreas schizophrenia

Normal Chronic
pancreatitis

Chronic pancreatitis,duct cyst

In the future
• Standardization of pediatric endoscopy
• Actively expand the field of endoscopic therapy
• Improve the diagnosis and treatment of small bowel diseases
• Strictly regulate the endoscope cleaning and disinfection processes
• To find and issue the guideline and trainee program for improing medical care

Conclusion
• Endoscopic procedure in the pediatric
population is safe and effectiveness
• Consideration for appropriate indication
• Be ware of potetial risk and complication