Embed Size (px)
Citation preview
TH Integrated Care NIS 2015/16
Coding requirementsAna Gutierrez
CEG Primary Care Facilitator
Quick update on AUA
Step 1: code eligibility
Step 2: obtain and code consent
Step 3: code entry onto IC pathway
Step 4: Level 1requirements
Step 5: Level 2 requirements
Using Excel to complete coding and create
working lists
Q&A
Agenda
Paid by NHSE
2% of adult population (Exeter figures, found in CQRS)
L/D will count for 2% this year
If register too big, remove those without care plans
(either Add 8CT2 = AA care ended or Delete 8CV4 =
AA care started
Two (simplified) self-declared reports this year (rather
than four)
Care Plan agreed or reviewed this year
AUA
Payment only for patients eligible this year
Who is eligible this year?
◦ Top 6% of Qadmissions boroughwide
◦ Level 2– formerly known as coordinated care:
Dementia, palliative care, heart failure, nursing home
Discretionary coded before 20 Aug 2013 and entered before 1 Apr
2014
Who is not eligible:
◦ Patients in the AUA register
◦ Patients who have fallen below this year’s risk bands
First task: Export top 4% patient list, and 4.1-6%
patient list, from NELIE
Eligibility for TH IC
TH IC Levels Entry level: top 4.1% to 6% QAdmissions
borough – Batch code ONCE with code EMISNQEL6 (eligible for IC)
Level 1: top 4% QAdmissions borough – Batch code ONCE with code 9NgzB (eligible for IC)
Level 2: HF/Pall/Home/Dementia/Discretionary – some are outside the 4/6% - use CEG search1 to batch add code 9NgzB (eligible for IC). You could do this monthly.

Task: Batch add eligibility codes 1

Task: Batch add eligibility codes 2
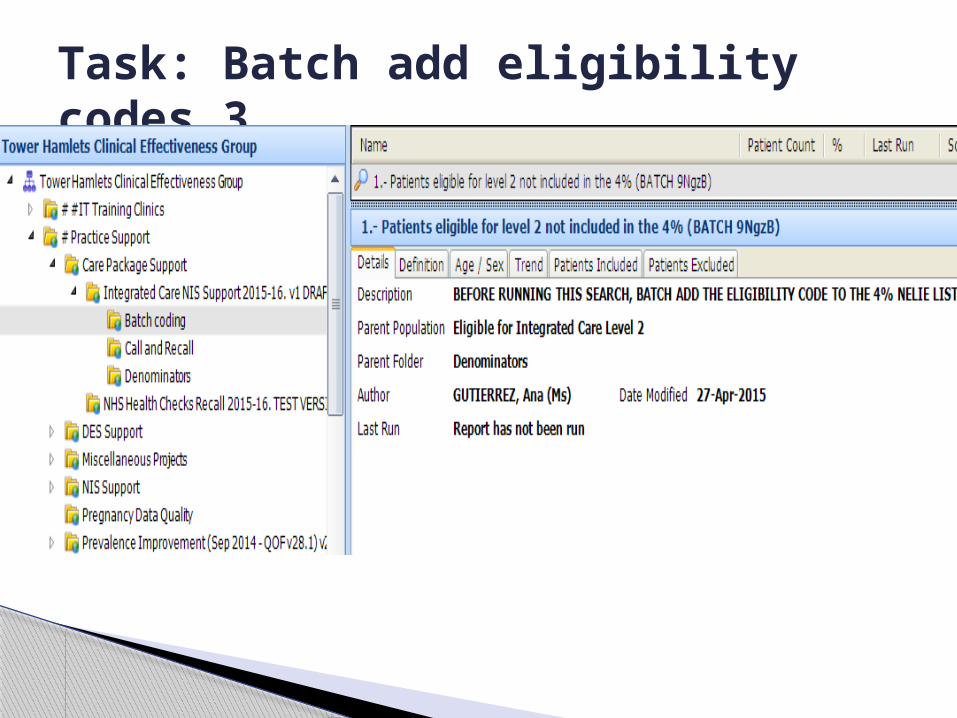
Task: Batch add eligibility codes 3
Consent to share local electronic record 93C0= Consent given for upload into shared
electronic record - Indispensable for ALL levels of Integrated Care
Only available via Sharing button◦ Select EMIS Data Sharing
Technical glitch workaround– if consent not visible in Care History, go back to the Sharing button, select Dissent, then select Consent, then go to Care History and delete Dissent.

Consent – 93C0
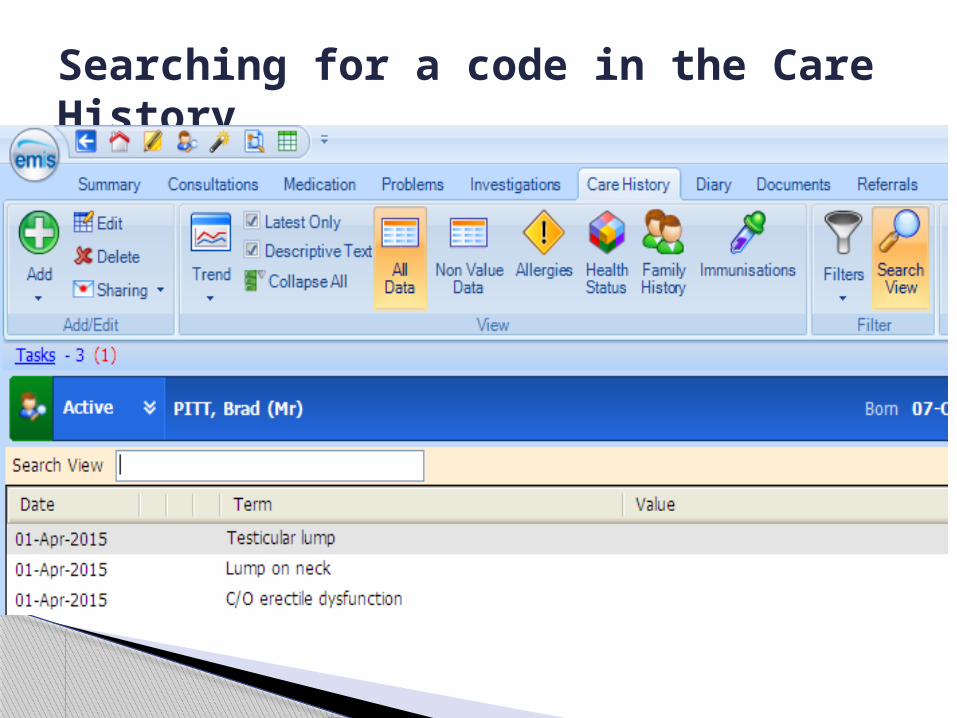
Searching for a code in the Care History
EntryYou can do this via the template once you obtain consent
For entry level: 8CMR (On IC pathway)
For level 1: 8CMR (On IC pathway)
Batch add 8CMR to eligible patients with consent (monthly) to pick up patients where you forgot to add the entry code (search 2 in the Batch Coding folder CEG Support)
For level 2: 8CMR + EMISNQON5 (On frailty reg.)
Level 1 requirements
Accountable GP (67DJ) - ever Crisis Plan agreed or reviewed (aka. AUA
care plan or level 1 care plan 8CSB or 8CMG3) – this financial year
PAM (38Qo) – this financial year, the second one at least 90 days after first one
Use CEG support search for list of patients due in 1 month or overdue for crisis plan

Level 2 requirements Accountable GP (67DJ) - ever Crisis Plan agreed or reviewed (aka. AUA
care plan or level 1 care plan 8CSB or 8CMG3) – this financial year
Care Coordinator (EMISQCA4) – ever Person centred care plan (aka.
Coordinated Care Plan 8CM8) this financial year
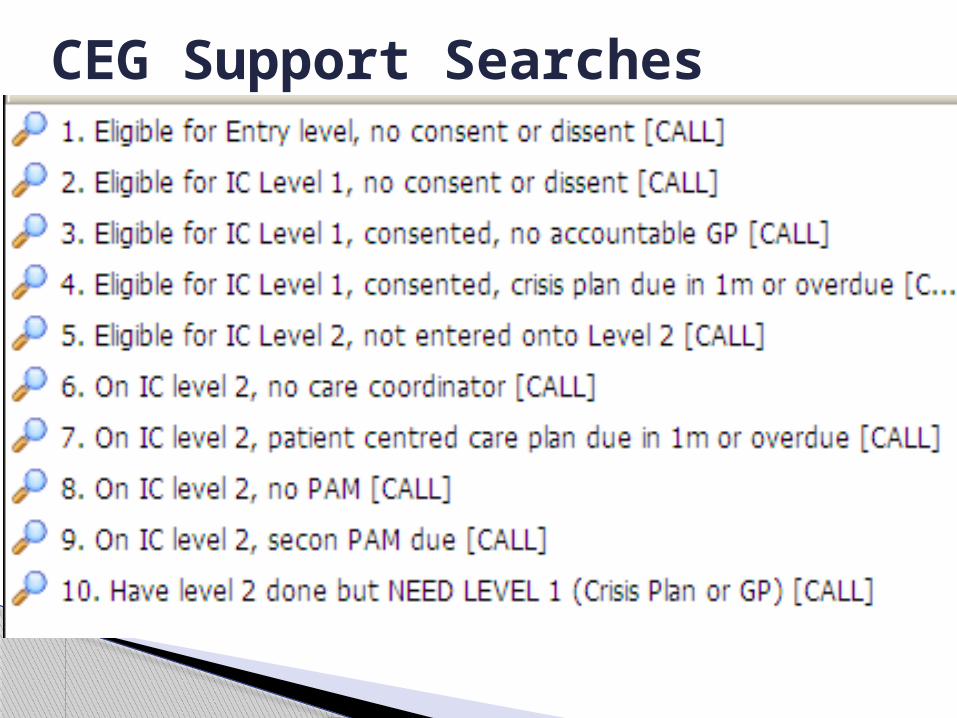
CEG Support Searches

CEG Support Advanced
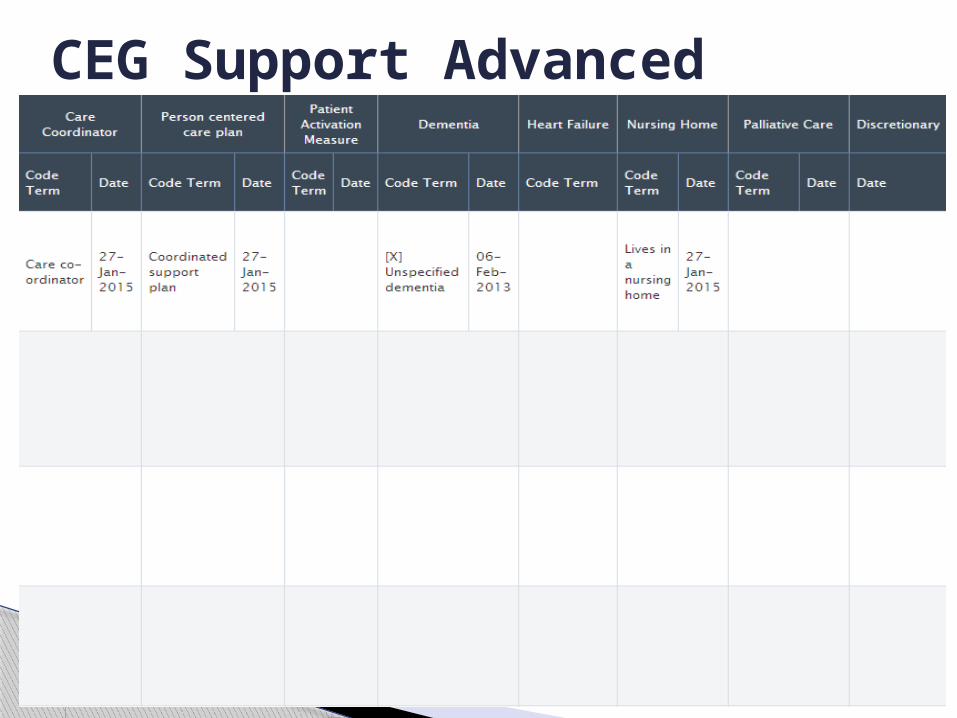
CEG Support Advanced
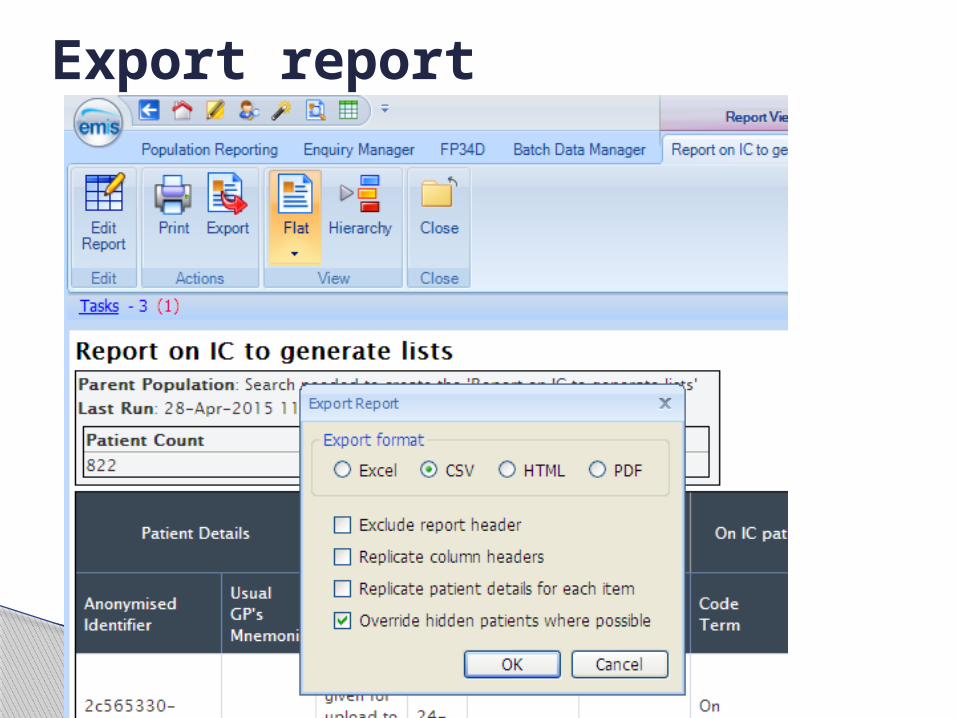
Export report
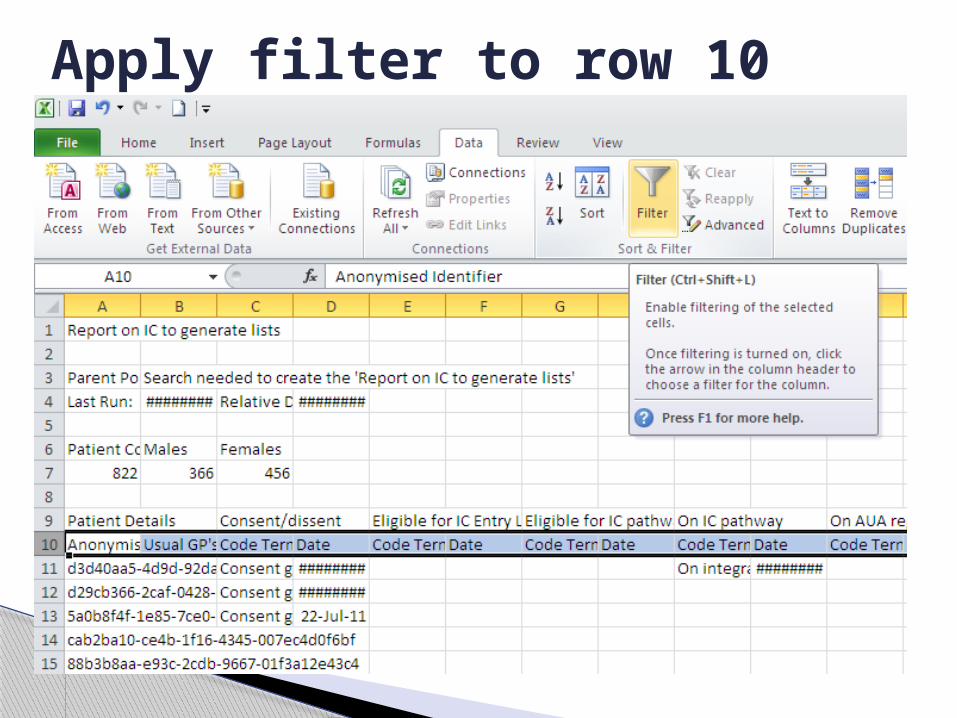
Apply filter to row 10
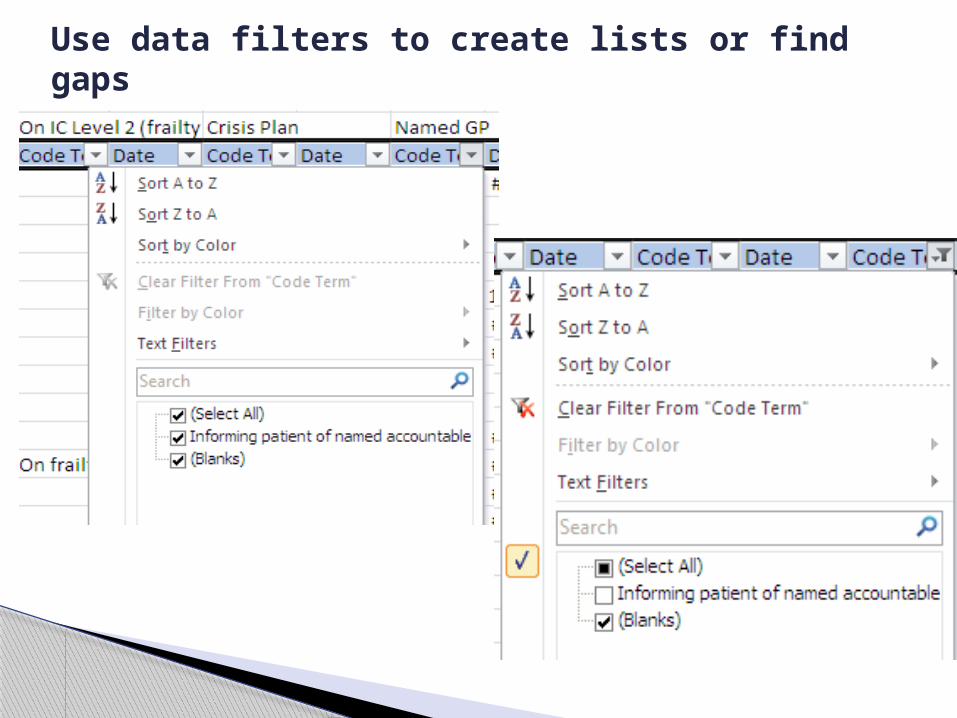
Use data filters to create lists or find gaps
Level 2 quality standards
Record Carer Status (even if there is no carer) and carer’s details (which will be pulled through to care plans) via Integrated Care template
Record in IC template if patient is ‘in last days of life’ and send expected death letter to OOH
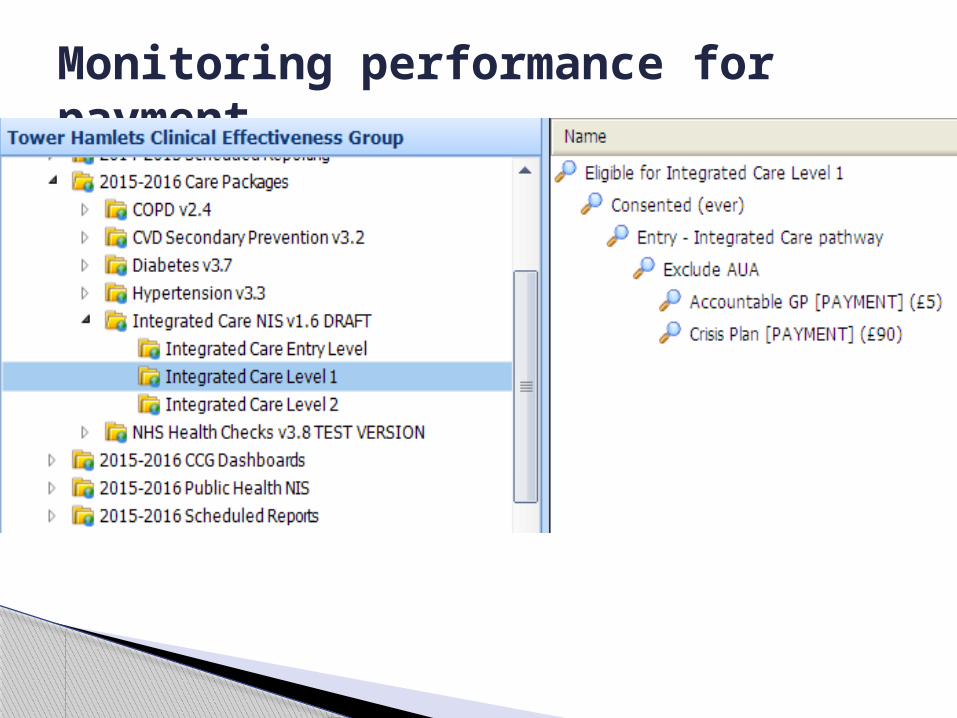
Monitoring performance for payment