Embed Size (px)
Citation preview
Annotation
ANAEMIA IN EARLY INFANCY
The diagnosis of anaemia in early infancy is a far more complicated process than it is at any other time of life. During the first 3 mth of extrauterine existence, continuous changes produced by growth and development result in wcck-to-week variations in what may be regarded as the normal haemoglobin value. In addition, unique pathological processes arc operative at this age which also contribute to diagnostic confusion. These unique processes are a consequence of maternal-foetal interactions, the rapidity of growth with its attendant nutritional requirements, and the proclivity of newborns to acquire a variety of infections.
After the 34th to 35th week of gestation, the mean cord blood haemoglobiii value is approximately 17.0 g/Im ml. Valucs of less than 14.5 g/ Im ml at birth may be regarded as abnormal. During the first hours of life, the liacmoglobiii value may rise by as much as 20% in those infants whose umbilical cords were iiot clamped immediately at birth (Usher ct al, 1963). During the first week of life, in both the term and premature infant, there is very little change in the haemoglobiii concentration and values at 7 days of age are very similar to those values present a t birth.
Beyond the first week of life, the haemoglobin values begiii to decline rapidly. In the term infant, the haenioglobin value reaches its lowest level at 8-9 weeks of age. At this time, haemoglobiii values as low as 9.5 g/Ioo ml 'nay be viewed as normal. Haemoglobiti values tend to fall more rapidly and reach lower levels in apparently healthy premature infants. Between 6 and 8 weeks of age, the haemoglobhi value of infants weighing INO g or less at birth averages about 8.0 g/Ioo ml and values of 7.0 g/Im ml are fiequently observed in the absence of any recognizable patliologic process.
Regirlation ofErythropoicsis This fall in haemoglobiii levcl appears to be a normal physiological process that is in-
fluenced by both the oxygen requirements of the infant and the mechanisms governing oxygen release to the tissues. Although it appears clear that the regulation of erythropoiesis in the adult is under the influence of erythropoietin (Stohlman, I959), the modulation of foetal and newborn erythropoiesis has been more difficult to understand because of the many complex factors affecting red cell formation during this stage of development. These factors include the iiiflueiicc of maternal erythropoiesis, variations in placental function, multiple site; of red cell production in the foetus, changes in arterial oxygenation at birth, the gradual replacement of foetal haemoglobin by adult haemoglobin, and alterations in the concentration and effects of red cell a,3-diphosphoglycerate.
Red cell formation itt trtcro begins at approximately day 14 of gestation and occurs succes- sively in thc yolk sac, liver and bone marrow. Erythropoietin is produced by the foetus and appears to be responsive to the usual factors stimulating its production (Halvorsc11 & Finnc. 1968). Both term and pretcrm infants have normal or elevated erythropoietin levels when compared with normal adults (Halvorsen, 1963). Infants with erythroblastosis foetalis have
Correspondence: Dr Frank A. Oski, Upstate Medid Center, 750 Fast Adam Street. Syracuse, New York 13210, U.S.A.
I95
196 Autiotatiori
increases in crythropoictin production in thc prcscncc of anaemia (Finnc, 1966). Infants with polycythacmia a t birth also dcnionstratc clevations i n crythropoictin ICVC~S. This is see11 in iiifaiits who arc small for gestational agc or who arc post-niaturc and is associated with pIaccl1- tal insuficicncy aiid prcsuiiicd intra-utcrinc hypoxia.
Thc crythropoictiii prcsciit in the plasma of tlic ncwborn appears to bc cndogcnomly produccd aiid uiidcr foctal control. Although niatcrnal plasma crythropoictin lcvcls arc slightly clcvatccl during pregnancy, thc cord blood saniplcs from anacinic infants with crytliroblas- tosis show cvcii grcatcr crythropoictin activity (Hanimon ct a/ , 1965). Hypcrtransfusion of 13rcgiiaiit niicc docs not supprcss crythropoicsis in thcir offspriiig (Jacobscn (’1 01, 1969). Adiiii~iistratioti of crythropoictin to pregnant inice docs not appcar to increasc foctal cry- thropoicsis (Matoth & Zaizov, 1970).
Thc nornial or clcvatcd plasma crythropoictin lcvcl prcscnt at birch dcclincs to undctcctablc lcvcls within scvcral days of birth and riscs again bctwccn 60 and 90 days of lifc (Mann el a/ , 1965). It is during this pcriod that the hacmoglobiii lcvel is progressivcly falling, acconi- paiiicd by a dccrcascd ratc of crythropoicsis (Gairdncr et n/ , 1952; Scip & Halvorscn, 1956; Garby ~t nl, 1963). During this time, the bonc marrow is capable of increascd crythropoiesis incdiatcd via crythropoictin if appropriatc stimulation is prcscnt such as is obscrvcd with anacmia or thc hypoxacmia of cyanotic heart disease (Halvorscn, 1963 ; Finnc, 1966). Thus, it would appcar that the fall in liacinoglobin levcl that is obscrvcd during the first 2-3 mth of lifc occurs as a rcsult of increascd oxygcn delivery to thc tissucs with removal of thc stiniulatioii to crythropoictin production. At birth, arterial oxygcn saturation promptly riscs from thc intrautcriiic valuc of 45% to 95% (Smith & Kaplan, 1942). During thc iicxt sevcral months of lifc, tlic position of the oxygen-hacmoglobiii dissociatiori curvc gradually shifts to the right as thc hacnioglobin falls. This gradual shift in thc curve facilitatcs oxygcn rcleasc to thc tissucs. As a rcsult, the term infant at 3 nith ofagc is capablc of relcasiiig as much oxygcn to his tissucs, at a niixcd vcnous oxygcii tension of 40 rnniHg, as the nornial newborn infant dcspitc a pronounccd fall in the oxygcn carrying capacity of thc blood (Dclivoria-l’apado- poulos ct nl, 1971). This shift to thc right in tlic position of the curve is mediated by the rcplaccmcnt of foetal by adult haciiioglobiii and its iiitcraction with rcd ccll a,3-diplios- phogl yccrate.
Thc influcncc of tlic position of tlic curvc on thc regulation of crythropoicsis in sinall infants is illustrated in Fig I . Thc normal rangc for a ‘rcticulocytc indcx’ [hacmoglobin (g/Ioo nil) x reticulocytc count (%)I as a function of hacnioglobin lcvcl is dcpictcd for Q infaiits who weighed less than 1500 g at birth and wcre followcd sequcntially for a pcriod of up to 12 wccks of life. Thc values for the rcticulocytc indcx of 12 small infants who rcccivcd cxcliange transfusions for non-haeinolytic diseases in thc inimcdiatc ncwborii pcriod are similarly displayed in Fig I . Thcsc infants, as a rcsult of thcir excliangc traiisfusions, im- incdiatcly shiftcd thcir oxygcn-hacinoglobin cquilibriuni curvc to the right and obtained normal adult valucs for thcir thc partial prcssure of oxygcn, in mmHg, a t which hae- moglobin is 50% saturatcd (Dclivoria-Papadopoulos et 01, 1971). It can bc noted that a t any haemoglobin lcvcl thcsc infants dcvclopcd much lcss of a rcticulocytc response than did thc non-cxchanged infants. Their hacmoglobiii valucs fcll lowcr at 6-10 wccks of agc before a rcticulocytosis was obscrvcd. Unfortunatcly, no data arc currciitly availablc rcgardiiig ery- thropoietiii production during the first scvcral months of lifc in thc preinaturc infant and no
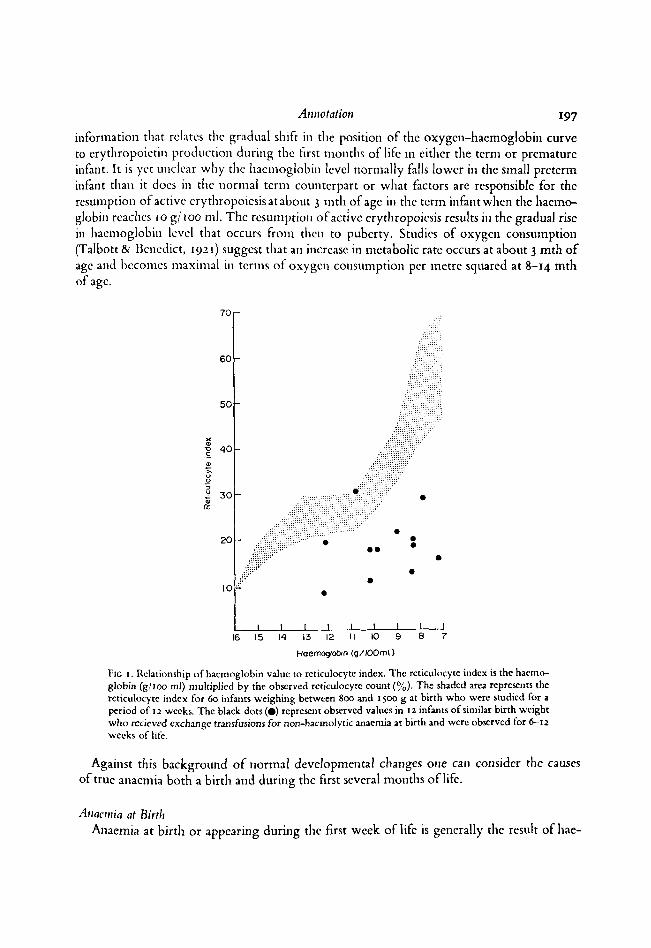
Atitiotation I97 i~iforniation that relates thc gradual shift in the position of the oxygcn-hacmoglobin curve to crytliropoictiii productioti during thc first months of lifc in cithcr the tcrni or premature infant. I t is yet ut~clcar why the haciiioglobin Icvcl tiornially falls lowcr in thc small pretcrm infant than it docs in the normal tcrm couiitcrpart or what factors arc rcsponsible for the resumption of activc crytliropoicsisat about 3 inth of agc in tlic tcrni infant whcn tlic hacmo- globin rcachcs 10 g/ 100 ml. The rcsumption of activc crytliropoicsis rcsults iii the gradual rise in hacmoglobin lcvcl that occurs frotii theti to puberty. Studies of oxygcii coi~sutnption (Talbott & 13cncdict, r c ) i r ) suggest that an iricrcasc in mctabolic rate occurs at about 3 mth of agc and bccomcs tnaximal in tcrtiis of oxygen consumptioti per nictrc squared at 8-14 mth of age.
60 -
50 -
X
$ 40- ._ 0
x " 0
3
- - .s 30- B
20 -
16 15 14 13 12 I 1 10 9 8 7
Hoemoglobin (g/100mk)
FIG I . Rclationship of haenloglobin value to reticulocyte index. The reticulocyte indcx is the haenio- globin (g/Ioo nil) multiplied by the observed reticulocyte count (%). The shaded area represcnts the rcticulocyte index for 60 infants weighing between 800 and 1500 g at birth who were studied for a period of 12 weeks. The black dots (0) represent observed values in 12 infants of similar birth weight who recieved exchange transfusions for non-hacmol ytic anaemia at birth and were obrrvcd for 6-12 weeks of life.
Against this background of normal developmctital changes one can considcr the causes of true anaemia both a birth and during the first scvcral months of lifc.
A~~acrrria ot Birth Anaemia a t birth or appearing during tlic first week of life is generally the result of hae-
198 Annotation
molysis or haemorrhage. Haemolytic anaemias occurring during this earl y period of life arc of multiple etiologies and are generally associated with scruni bilirubin levels in exceSS of 6 8 mg/ IOO ml. Haernolytic disease in the iiewborii can bc broadly classified into three Iargc categories: isoimmunization, inherited defects of the rcd C C I L and acquircd defects of the red cell. In most parts of thc world, isoimmunizatioii as a rcsult of maternal-foe~l incompatibilities in either the Rh or ABO blood group systcll1s is the Icading came of hacmolytic discasc. O f the inherited defects of the rcd cell, red cell glucosc-6-phosphatc dcliydrogctiasc dcficicncy appears to be the abnormality most co1iimo1ily associatcd with both aiiacriiia and liypcrbilirubiiiacniia. Virtually all of thc rcd CCII clizymc deficiciicics described to datc have been associatcd with anacmia and liypcrbilirubinacmia during the early days of life. The red cell nieiiibraiic disordcrs, which iiicludc hcrcditary splicrocytosis, clliptocytosis, atid stomatocytosis, may also be associatcd with anacmia in early lifc. Approxi- mately 50% of patients with hcrcditary sphcrocytosis cxperiencc hypcrbilirubinacmia during the first wcck of life (Stanley & Diamond, 1937).
Anaemia and jaundice frequently accompany profound acidosis and hypoxaemia in the young infant. In many instances, this hacmolytic anaemia may be a coiiscqucncc of the associated pathologic process of disseminatcd intravascular coagulation. Infections, inost notably those produced by congenital cytomegalovirus, toxoplasmosis, rubella, syphilis, and Gram-negative bacteria, arc other causes of anacmia during this period.
Rcd cell hypoplasia (the Diamond-Blackfan syndromc) may also manifcst itsclf at thc timc of birtli with anacniia and reticulocytopcnia.
Other inherited abnornialitics that may rcsult in aiiacniia during thc first scvcral days of lifc include dcfccts in alpha chain synthcsis (alpha-thalassacmia trait) o r ganinia chain syn- thesis (gamma-tlialassaeiiiia).
Hacmorrliagc Icading to anaciiiia a t birth or in tlic first fcw days of lifc may be broadly grouped into thrce major ctiologic catcgorics. Thcsc includc hacmorrhagc associatcd with obstetric accidents or malforiiiatioiis of tlic placcnta and cord, occult hacniorrhagc froin tlic foetus into tlic maternal circulation or from twin to twin, and internal liacmorrhages. In these situations, pallor and signs of circulatory collapse arc promiiiciit clinical fcaturcs arid jaundice is generally abscnt.
Aiiacaria at Ages 1-3 Mdz ojL$ Anaemia which may bc first detcctcd a t 1-3 inth of lifc may rcprcscnt the scquclac of a
previously undiagnosed cvciit in thc imiiicdiatc newborn pcriod. Most commonly, these would iiiclude mild isoimiiiunizatioii, foctal to niatcriial hacmorrhagc, or chronic congcnital infections.
By this pcriod of lifc, hacmoglobinopathics involving dcfccts of tlic bcta chain bccome clinically apparciit. Both tlialassacmia major (Erlandson & Hilgartncr, 1959) and sickle cell anacmia (van Baclcti ct a/, 1969) produce anacmia by 3 mth of agc.
In thc rapidly growing prciiiaturc infant, both folk acid dcficicncy and vitamin E de- ficiciicy also may producc truc anacmia by 8-10 wccks of lifc. Folic acid deficiency is most commonly obscrvcd in tliosc infants wliosc clinical coursc has bccn complicated by diarrhoea and infcctions (Robcrts cf 01, 1969). Vitamin E dcficicncy occurs dllnOSt exclusively in infants of birth wcights of less than I500 g. Thc anacmia is primarily the result o f cscessivc haemoly-

Annotation I99 sis and is accoinpanicd by reticulocytosis, poikilocytosis, rcd cell fragrncntatio~~, mild s p h e r e cytosis, tI1rombocytosis, and in the morc scvcrcly dcficicnt in fan ts, oedema may bc observed (oski& Bamcss, 1967; Ritchic et a / , 1968).
Vitamin E dcficicncy results froin a combination of factors whicI1 include: low vitalnill E Stores at birth, inadcquatc dietary iiitakc, and poor absorption of this fat-solublc vitamill.
administration of iron during the first weeks of life, citlicr in thc form of a Illcdicillal supplement (Melhorn & Gross, 1971) or incorporated into thc formula (Williams ct a/, I973), tends to aggravate the aiiacinia in these vitamin E dcficicnt premature illfa11ts.
Bccausc of tlic many causcs of aiiacinia during thc first 3 mth of life, thc pliysiciail must approach this challenging problcin with a clear understanding of what is ‘true' aiiacmia, diligciitly collect relevant in forination conccrning family history, obstetric history, the early neonatal coursc of cvciits, and dietary history, bcforc illstitutiiig a inyriad of unncccssary and ill-suited diagnostic procedures.
Dcprtiriuit of Pcdiatrics, State Univcrrity ?f New York, Upstate Medical Ccnrcr
FRANK A. OSKI JAMES A. STOCKMAN, I11
REFERENCES
DEI.IVORU-PAPADOPOULOS, M., RONCEVIC, N.P. & OSKI, F.A. (1971) Postnatal changes in oxygen transport o f term prcniaturc, and sick infants: Thc rolc of red cell ~,3-diphosphoglyceratc and adult hemoglobin. Pcdiafrir Research, 9, 235.
ERLANDSON, M.E. (L HILGARTNER, M. (1959) Hemoly- tic discasc in the nconatal period and carly infancy. Jotinial o j Pediatrics, 54, 566.
FINNE, P.H. (1966) Erythropoietin lcvels in cord blood as an indicator of intrautcrinc hypoxia. Arta Poediatrica Srcuidimoica, 55, 478.
GAIRDNER, D., MARKS, J. & ROSCOE, J.D. (1952) Blood formation in infancy. Part I. The normal bonc marrow. Archives o j Disease ita Childhood, 27, 128.
GARBY, L., SJOLIN, S . ei VAILLE, J.C. (1963) Studics on crythro-kinetics in infancy, 111. Disappcarancc fro111 plasma and rcd-ccll uptakc of radio-active iron itijcctcd intravenously. Aria Pdediafrica Star idi tmh, 52. 537.
GUEST, G.M. & BROWN, E.W. (1957) Erythrocytes and hcmoglobin of the blood in infancy and childhood. Ill. Factors in variability. statistical studies. Atwritan Joiirtial c?f Diseases of Children, 93, 486.
I4ALVORSEN, S . (1963) Plasma rrythropoietin kvCk in cord blood and in blood during the first weeks of life. Atfa Pacdintrica Scanditravica, 52, 425.
HALWSEN, S. 6 FINNE, P.H. (1968) Erythropoietin production in the human fctus and newborn. A m d ~ c f t k r Nrrv York Arademy oJSciettccss, 149, 576.
HAMMON, D., I~HIKAWA, A. & KEIGHLEY, G. (1962) Relationship between crythropoictin and severity of ruicmia in hypoplastic and hemolytic states. In: Erytlrropoiesis (Ed. by I.. 0. Jacobsen and M. Doyle). Grune & Stratton, New Yo&.
JACOBSEN. L.O., MARKS, E.K. & GASTON, E.O. (1959) Studies on erythropoiesis. XII. The effect of transfusion-induced polycythemia in the mother on the fetus. Blood, 14, 644.
MA”, D.L., SITES, M.L., DONATI, R.M. & GAL- LAGHER, N.1. (1965) Erythropoietic stimulating activity during the first ninety days of life. Procecd- icigs of fhe Sotiefy for Experitnental Biology and Medicine, 118, 212.
MATOTH, Y. & ZAIZOV, R. (1970) Regulation of erythropoiesis in the fetal rat. Proceedings o j fke Tel Aviv University C o t ~ r e n t e 0th Erytltropoicsis, Pefak Tikva.
MATOTH, Y., ZAIZOV, R. & VARSANO, 1. (1971) Postnatal changes in some red cell parameters. Acfa Paediatrica Struidinavica, 60, 3 17.
MELHORN, D.K. & GROSS, S. (1971) Vitamin-E dependent anemia in the prematurc infant. I. Effccts of large dogs of nicdicirlal iron. Jmnral .f Pediahirs, 75, 5%.
OSKI F.A. B BARNES, L.A. (1967) Vitamin E dc- ftciency : A previously unrecognized cause of hemolytic ancmia in the premature infant. Joitrnal of Pediatrics, 70, 211.
RITCHIE, J.H., MATHEW, B.F., MCMASTERS, V. R- GROSSMAN, M. (1968) Edcnia and hemolytic anenlia

200 Attriotation
in prcmaturc infants. A vitamin E dcficicncy syndromc. Ntw Errglarid Joiirrial of Medicitre, 279. 1 1 8 j .
MONK-JONES, M.E. (1969) Folatc statc of prcmaturc infarits. Arrhivcs ‘$ Disease it1 Cliildliuod, 44, 637.
SEIP. M. & HAI.VORSEN, S. (1956) Erythrocytc produc- tion and iron storcs in prcmaturc infants during thc first nionth of life. Acla Puediatrica Scarzdiriuvica,
SMITH, C.A. K. KAPLAN, E. (1942) Adjustnicnt of blood oxygen lcvcls in nconatal lifc. Arriericari Joimral qf Disrases ojCliildrcri, 6 4 , 843.
STAMEY, C.C. 8 DIAMOND, L.K. (1957) Congcnital hcmolytic ancrnia in the ncwboni. AiricrirnriJoimtnl OJ-Discuses of Cliildreri, 94, 616.
IlOBLRTS, 1’.M., ARROWSMITH, D.E., RAU, S.M. &
453 600.
STOHLMAN, F., JR (1959) Observations on the physiol- ogy of crythropoietin and its role in the regulation of red ccll production. AfIrrds @f the New york Academy of Sciorcc, n, 710.
arid CroiiJtli ,fioiri Birth to Ptrberty. p 174. Publication No. 302, Carncgic Lnstitutc ofwashington.
USHER, R., SEfEPARD, M. & LIND, J. (1963) The blood volunie of the newborn infant and placental ems fusion. Actu puedialrica, 52, 497.
V A N BAELEN, H., VANDEPITTE, J. & EECKELS, R. (1969) Obscrvations on sickle ccll anemia and hacmoglobi,, Bart’s in C o n g o l e ~ ~ n c o n a t ~ ~ . Armales de la Soci& Bdpe de MCdicirre Tropicale, 49, 157.
(1973) Unpublishcd obscrvatiotis.
TALBOT, F.B. Bi BENEDICT, F.G. (1921) Mtt&lism
WILLIAMS, M. , SHOIT, R., O’NML, P. 81 OSKI, F.A.