-
7/21/2019 Anaesthesia and Epilepsy
1/10
REVIEW ARTICLES
Anaesthesia and epilepsy
A. Perks1*, S. Cheema3 and R. Mohanraj2
1
Department of Anaesthesia and
2
Department of Neurology, Salford Royal Hospital, Stott Lane,
Salford M6 8HD, UK3 Bradford Royal Infirmary, Duckworth Lane,
Bradford BD9 6RJ, UK
* Corresponding author. E-mail: [email protected]
Editors key points
The authors have reviewed the mechanism
of action of old and new antiepileptic drugs.
Awareness is required regarding
seizure-provoking properties of certain
anaesthetic drugs.
Status epilepticus, refractory to two
antiepileptic drugs carries a high morbidityand requires general
anaesthesia.
For uncontrolled seizures, treatment with
midazolam, thiopental, or propofol is
acceptable; opioids should be avoided.
Summary. Epilepsy is the most common serious neurological
disorder, with a
prevalence of 0.5 1% of the population. While the traditional
antiepileptic
drugs (AEDs) still play a significant role in treatment of
seizures, there has been
an influx of newer agents over the last 20 yr, which are now in
common usage.
Anaesthetists are frequently faced with patients with epilepsy
undergoing
emergency or elective surgery and patients suffering seizures
and status
epilepticus in the intensive care unit (ICU). This review
examines perioperative
epilepsy management, the mode of action of AEDs and their
interaction with
anaesthetic agents, potential adverse effects of anaesthetic
agents, and the
acute management of seizures and refractory status epilepticus
on the ICU.
Relevant literature was identified by a Pubmed search of
epilepsy and status
epilepticus in conjunction with individual anaesthetic
agents.
Keywords:anaesthesia; anticonvulsants; epilepsy; status
epilepticus
Epilepsy is a tendency to have recurrent unprovoked
seizures.
It is the most common serious neurological disorder with a
prevalence of 0.5 1% of the population. The highest
incidence
is at the extremes of age and in those with structural or
devel-
opmental brain abnormalities. The International League
against Epilepsy (ILAE) has classified seizures into focal
(or
partial) seizures which arise from one hemisphere and gener-
alized seizures which show electrographic seizure onset over
both hemispheres.1 2 Lamotrigine and carbamazepine are
considered drugs of choice in focal epilepsies, while
valproate
is probably the most effective drug for primary generalized
sei-
zures.3 4 If the initial antiepileptic drug (AED) results in
adverse
effects, an alternative AED is tried as monotherapy. If, on
the
other hand, seizures continue in spite of adequate doses,
combination therapy is often necessary.
In the last 20 yr, there has been an influx of a new gen-
eration of AEDs.5 Many of these are the products of rational
drug development programmes, while others are modifica-
tions of previously existing molecules that result in
improved pharmacokinetic properties. The newer AEDs are
generally associated with fewer adverse effects and drug
interactions. Many anaesthetic agents affect the propensity
to seizures, both in patients with epilepsy and in those
with
no prior history of seizures. In patients taking AEDs, drug
interactions and maintenance dosing of AEDs during
periods of starvation are important considerations in the
perioperative period.
Patients with epilepsy often require anaesthesia for
elective and emergency surgery. Appropriate perioperative
management of AED therapy is vital in maintaining seizure
control in these patients. Anaesthetists need to be aware of
the pharmacological properties of commonly used AEDs.
Patients with epilepsy may also require anaesthetic care
during treatment of status epilepticus, either for airway
man-
agement or induction of general anaesthesia for refractory
status epilepticus. This article aims to examine the current
treatment of epilepsy, the mode of action of antiepileptics,
the effect of AEDs on anaesthesia, and the effect of
anaesthe-
sia on epilepsy in adults. The use of anaesthetic agents in
the
management of refractory status epilepticus is also
discussed.
Mechanisms of action of AEDs
In simple terms, a seizure can be seen as the result of
imbal-
ance between excitatory and inhibitory neuronal activity.
This leads to the generation of hyper-synchronous firing of
a large number of cortical neurones. Traditional AEDs exert
antiseizure activity by the following mechanisms:
reduce the inward voltage-gated positive currents(Na+,
Ca2+),
increase inhibitory neurotransmitter activity (GABA),
decrease excitatory neurotransmitter activity (glutam-
ate, aspartate).
The effects are summarized in Table 1. In addition, many
new AEDs possess novel mechanisms of action. Novel sites
of drug binding include synaptic vesicle (SV2) protein
(levetir-
acetam), steroid binding sites on GABAA receptors (ganaxo-
lone), and voltage-gated potassium channel (retigabine).6 7
British Journal of Anaesthesia 108 (4): 56271 (2012)
Advance Access publication 8 March 2012 .
doi:10.1093/bja/aes027
& The Author [2012]. Published by Oxford University Press on
behalf of the British Journal of Anaesthesia. All rights
reserved.
For Permissions, please email: [email protected]
mailto:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]
-
7/21/2019 Anaesthesia and Epilepsy
2/10
Effect of antiepileptics on anaesthesia
There are important pharmacokinetic and pharmacodynamic
interactions between AEDs and drugs commonly used in an-
aesthesia. These affect both drug efficacy and the risk of
seizure activity intraoperatively.8
Induction and inhibition of the cytochrome P450 isoen-
zymes in hepatic metabolism constitutes the most significant
mechanism of drug interactions involving AEDs. Many of
theolder-generation AEDs, such as carbamazepine, phenytoin,
phenobarbital, and primidone, have potent enzyme-inducing
properties. This leads to a decreased plasma concentration
of
many medications including immunosuppressants, antibacter-
ials, and cardiovascular drugs, particularly amiodarone,
b-blockers (propranolol, metoprolol), and calcium channel
antagonists (nifedipine, felodipine, nimodipine, and verap-
amil).9 In patients taking warfarin, introduction or
withdrawal
of enzyme-inducing AEDs requires close monitoring of the
international normalized ratio. Oxcarbazepine and
eslicarbaze-
pine are weaker inducers of hepatic microsomal enzymes com-
pared with carbamazepine, but the effects may be clinically
significant.10
Topiramate also induces hepatic microsomalenzymes in a
dose-dependent manner. Valproateis an inhibitor
of hepatic microsomal enzyme systems and may reduce the
clearance of many concurrently administered medications, in-
cluding other AEDs. Gabapentin, lamotrigine, levetiracetam,
tiagabine, and vigabatrin do not induce hepatic enzymes.11
Macrolide antibiotics, particularly erythromycin, are potent
inhibitors of CYP3A4, which is involved in carbamazepine me-
tabolism and can lead to carbamazepine toxicity. Concomi-
tant use of carbapenem antibiotics can lead to a
significant decrease in serum valproate concentrations.12 13
Effect of anaesthetic agents on epilepsy
Many of the agents used possess both pro-convulsant and
anticonvulsant properties, which could impact on the
choice of anaesthetic.14
Inhalational anaesthetics
Nitrous oxide (N2O) provokes seizures in animal models
(cats), but this has not been replicated in humans. In mice,
withdrawal seizures have been seen after short exposures
to N2O.15 During a case of electrocorticographic monitoring
for epilepsy surgery, N2O visibly suppressed epileptiform
ac-
tivity, which manifested again on N2O withdrawal.16 Myoclo-
nus has been observed in volunteers exposed to hyperbaric
(1.5 atm) N2O17 and when used in combination with isoflur-
ane or halothane.18
There are multiple case reports of sevoflurane-provoking
seizure-like activity, particularly in children19 and wherehigh
concentrations are used in conjunction with hypocap-
nea.20 In high concentration, enflurane exhibits periods of
suppression with paroxysmal epileptiform discharges in
cats and rats.21 There have been multiple reports of seizure
activity in humans after enflurane anaesthesia.18 22
Isoflur-
ane has well-characterized anticonvulsant properties. Both
isoflurane and desflurane can be used in refractory status
epilepticus, described in a later section.23
Opioids
Meperidine is the opioid with the strongest association with
myoclonus and tonic-clonic seizure activity.24
However, fen-tanyl, alfentanil, sufentanil, and morphine have
been
reported to cause generalized seizure patients after
low-to-moderate dose,25 26 particularly after intrathecal
use.27 29 Fentanyl and its analogues have not been shown
to possess any anticonvulsant properties.
Opioid anaesthetic agents are used to enhance EEG activ-
ity in patients with focal epilepsy. Both remifentanil and
alfentanil have been used to induce spike activity in
localiz-
ing epileptogenic zones intraoperatively during epilepsy
surgery,30 although alfentanil appears to be the more
potent activator.31 The addition of alfentanil to propofol
an-
aesthesia for electroconvulsive therapy (ECT) also increases
seizure duration.32
I.V. anaesthetic agents
The barbiturates (thiopental, methohexital, and pentobar-
bital) and propofol are well established as agents for the
treatment of refractory status epilepticus.33 35 All agents
have been reported to produce excitatory activity, such as
Table 1 Main modes of action of commonly used AEDs. 6 7 *From
the evidence, it is not clear which of the actions of valproate is
responsible for
its actions. Lamotrigine is primarily a sodium channel blocker
with some effects on T-type calcium channels
Mode of action Antiepileptic drug
Increase GABA activity
Increased frequency of Cl channel opening Benzodiazepines (binds
to BZ2receptors); tiagabine (prevents reuptake);
gabapentin (prevents reuptake)
Increased mean Cl channel opening duration Barbiturates
Blocks GABA transaminase (blocking GABA catabolism
within the neurone)
Vigabatrin
Glutamate antagonist Topiramate (at AMPA receptor)
Reduction of inward voltage-gated positive currents
Phenytoin(Na+ channel); carbamazepine (Na+channel);
ethosuximide(Ca2+ channel)
Increased outward voltage-gated positive currents Sodium
valproate (K+ channel)
Pleotropic sites of action Sodium va lproate (1, 2, 3 and 4)*;
lamo trigine (2 and 3)*; topiramate (1, 2, and 3)
Anaesthesia and epilepsy BJA
563
-
7/21/2019 Anaesthesia and Epilepsy
3/10
myoclonus, opisthotonus, and rarely generalized seizures on
induction of anaesthesia. The highest incidence appears to
be with etomidate,36 followed by thiopental, methohexital,
and propofol. Etomidate has been shown to increase
seizure duration in ECT when compared with thiopental.37
At higher doses, all agents act as anticonvulsants.38 39
Ketamine is a non-competitive glutamate antagonist
acting at N-methyl-D-aspartate receptors, a property which
could be beneficial in management of status epilepticus
re-fractory to other agents (see below). As with the other i.v.
agents, low doses may facilitate seizures, but at doses that
produce sedative or anaesthetic effects, ketamine shows
anticonvulsant properties.40
Benzodiazepines
All benzodiazepines in clinical practice possess potent
anti-
convulsant properties.41 Diazepam, midazolam, and loraze-
pam are widely used to terminate episodes of status
epilepticus (see below).
Local anaesthetics
Local anaesthetic agents readily cross the blood brain
barrier, causing sedation and analgesia followed by general-
ized convulsions at higher doses.42 43 High blood levels
result
from an accidental i.v. administration or rapid systemic ab-
sorption from a highly vascular area.44
I.V. lidocaine has been used to treat status epilepticus in
several small series, mainly in children.45 47 It was not
asso-
ciated with any major adverse events in these reports, but
its
efficacy and role in management of status epilepticus in
adults remain to be proven.
Neuromuscular blocking agentsNone of the neuromuscular blocking
agents appear to have
any pro-convulsant or anticonvulsant effects. Laudanosine,
the primary metabolite of atracurium, has been known to
cause EEG and clinical evidence of seizures in animals.48
This has not been replicated in humans, but the possibility
should be considered in patients with hepatic failure in
whom the half-life of laudanosine is significantly
prolonged.
Succinylcholine produces EEG activation related to an in-
crease in cerebral blood flow afferent muscle spindle
activity;
an effect blunted by prior administration of
non-depolarizing
neuromuscular blocking agents. It has not been associated
with seizure activity.49
Anticholinergics and anticholinesterases
The increase in acetylcholine via administration of atropine
or scopolamine can produce central cholinergic blockade
(or central anticholinergic syndrome). This manifests as
agitation with seizures, hallucinations, and restlessness
or stupor, coma, and apnoea. The most effective treat-
ment for this is physostigmine.50 Glycopyrrolate does not
cross the bloodbrain barrier, so does not produce these
effects.
Perioperative management of AEDs
In patients with a history of well-controlled epilepsy, it is
vital
that efforts are made to avoid disruption of antiepileptic
medication perioperatively. Patients should be advised to
take their regular medications on the morning of surgery
and regular dosing should be re-established as early as
prac-
ticable after surgery. If a single dose is missed (such as
that
might occur with day-case surgery), it should be taken assoon as
possible after surgery. Where multiple doses are
likely to be missed, AEDs should be administered
parenterally
where possible. I.V. forms of phenytoin, sodium valproate,
and levetiracetam are available (where i.v. doses are
equiva-
lent to oral doses) and carbamazepine is available as a sup-
pository. If the patients regular AED is not available in
parenteral formulation, advice should be sought from a neur-
ologist regarding alternatives that may be used to cover the
perioperative period.
In general, routine drug level monitoring is not required
perioperatively as anaesthetic agents do not significantly
alter the pharmacokinetics of AEDs. However, prolonged in-
tensive care unit (ICU) stay, with attendant changes inserum pH
and albumin levels and also the use of drugs
that interact with AEDs, can affect their serum concentra-
tions. Of the commonly used AEDs, phenytoin presents the
greatest challenge because of its unique pharmacokinetic
properties. In patients admitted to ICU, it is necessary to
check serum concentrations of phenytoin daily to guide
dosing.
Status epilepticus
Status epilepticus is a common medical emergency. The
traditional definition of status epilepticus as a seizure
lasting or recurring without regaining of consciousness overa 30
min period is primarily useful for epidemiological pur-
poses. In clinical practice, most convulsive seizures abate
within 23 min and a seizure that continues for more than
5 min has a low chance of terminating spontaneously, so
should be treated with emergency antiepileptic
medications.51
Physiological changes seen in status epilepticus
During the first stage of convulsive status epilepticus
(CSE),
there is an increase in cerebral metabolism, increased
blood flow, and increased glucose and lactate concentration.
This is associated with massive catecholamine release,
raised
cardiac output, hypertension, tachycardia, and increasedcentral
venous pressure. These compensatory mechanisms
prevent cerebral damage in the first 3060 min.52
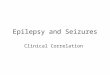
Beyond this time, if seizures are notcontrolled,the compen-
satory mechanisms start to fail and cerebral damage may
occur. Cerebral auto-regulation fails, leading to hypoxia,
hypo-
glycaemia, an increase in intracranial pressure, and
cerebral
oedema. The net result is of hyponatraemia, potassium imbal-
ance, and an evolving metabolic acidosis, which will lead to
a
consumptive coagulopathy, rhabdomyolysis, and multi-organ
failure. These changes are represented in Figure 1. Itshould
be
BJA Perkset al.
564
-
7/21/2019 Anaesthesia and Epilepsy
4/10
noted that these changes occur more rapidly in CSE, but can
also occur in non-CSE (NCSE).52
Stages of GCSE and drug treatment
Intervention is required for all convulsive seizures that
have
continued beyond 2 min longer than the patients habitual
seizures. In most cases, this means that treatment should
be administered if the seizure is continuing at 5 min.
Benzo-diazepines are the first-line agents. There is evidence
that
the longer seizures continue, the less efficacious treatment
becomes.53 This is related to altered localization of GABA
receptors on neuronal membrane induced by seizures.54
Treatment with benzodiazepines should therefore be admi-
nistered as soon as it is apparent that the seizure is not
self-
terminating. Patients who have suffered one episode of CSE,
especially those with structural brain abnormalities and
learning disability should be prescribed benzodiazepines to
be used in the community to prevent the development of
refractory CSE. Rectal diazepam has traditionally been used
for this purpose, but buccal or nasal midazolam appears
equally effective and is more acceptable to adult and paedi-
atric patients (Table2).55 56
Emergency investigations should include arterial blood
gas measurement, glucose, renal and liver function,
calcium and magnesium, full blood count (including plate-
lets), coagulation, and AED levels. Consider saving bloodand
urine samples for future analysis, including toxicology
if cause is unclear. Chest radiograph can be used to
exclude aspiration pneumonia. Other investigations will be
directed at potential aetiology, such as brain imaging or
lumbar puncture.52 During the management of CSE, due to
the sedative nature of the drug treatments used, respiratory
depression requiring intubation is not uncommon.
The underlying cause of CSE should be identified and
treated wherever possible. Alcohol withdrawal and metabolic
disturbances including hypoglycaemia and hyponatraemia
Generalizedconvulsions
Recurrent seizures
Isolated Lengthen
Seizures
Convu
lsive
Non-co
nvulsiv
e
PEDS
Respiratory compromiseHypothermia
Electro-mechanicaldissolution
Phase IIAP normalGlucosepH Lactate
Motor
EEG
Braindamage
Brainmetabolism
Systemic
Brain parenchymaoxygenation
Glucose utilization
Phase IAPLactate Glucose
CBF
Brainutilization
Brain glucose
Brain energy state
Brain lactate
Oxygenutilization
1
2
3
0 30 60
TimeMinute Hour
Transition
4
Myoclonus
Fig 1 Physiological changes occurring during prolonged status
epilepticus. Adapted from Shorvon. 106 PED, periodic epileptic
discharge; CBF,
cerebral blood flow. 1, Loss of reactivity of brain oxygen
tension; 2, mismatch between the sustained increase in oxygen and
glucose utilization
and a decrease in cerebral blood flow; 3, a depletion of
cerebral glucose and glycogen concentrations; 4, a decline in
cerebral energy state.
Anaesthesia and epilepsy BJA
565
-
7/21/2019 Anaesthesia and Epilepsy
5/10
can present with seizures. In patients with epilepsy, failure
to
adhere to prescribed medications and the resultant rapid de-
crease in serum levels can precipitate SE. Infective and in-
flammatory conditions of the brain can present with CSE,
which can negatively affect the prognosis of these condi-
tions. Failure to treat the underlying cause of CSE is a
common cause of seizures remaining refractory to antiepi-
leptic medication.
Pre-monitory stage (out of hospital or first 5 min)
Buccal midazolam or rectal diazepam can be administered
by the patients carers or emergency medical personnel.
Early stage (first 510 min)
Initial management of seizures is supportive with airway
pro-
tection, supplemental oxygen, and assessment of cardio-
respiratory function with establishment of i.v. access. If
hypoglycaemic seizures are suspected, glucose (50 ml of
50% dextrose) should be administered immediately. Inpatients
suspected of impaired nutrition or alcohol abuse,
high-dose thiamine (250 mg), should be administered with
glucose.57
Benzodiazepines are used as first line in early GCSE.58
While all benzodiazepines share the same receptor site on
the GABA receptor a subunit, their pharmacokinetic proper-
ties vary.59 Lorazepam has been shown to result in higher
rates of seizure control compared with phenytoin, phenobar-
bital, and phenytoin with diazepam, and is the agent of
choice.60 If lorazepam is unavailable, diazepam may be
used, but the risk of seizure relapse is higher owing to its
rapid redistribution.61 Where i.v. access is delayed,
further
doses of rectal diazepam or buccal or nasal midazolam
may be tried. I.M. midazolam may be an alternative, and a
randomized controlled trial is currently underway comparing
it with i.v. lorazepam, the current gold standard in the
treat-
ment of early CSE.62
Established CSE (530 min)
At present, four agents can be considered as options in the
treatment of established CSEphenytoin (or its prodrug,
fosphenytoin), valproate, phenobarbital, and
levetiracetam.63
There is little evidence regarding the relative efficacy of
these
agents and adequate trials are urgently needed.
Phenytoin is probably the most widely used drug in the UK
for management of SE that continues after benzodiazepine
administration. It is water insoluble and the vehicle for
i.v.
administration has a highly alkaline pH.64
Phenytoin shouldtherefore only be administered via a large-bore
i.v. cannula
or a central line as extravasation can result in extensive
tissue necrosis. Cardiac rhythm and arterial pressure should
also be monitored as hypotension and bradycardia can
occur, especially in the elderly. Fosphenytoin, a prodrug of
phenytoin, is rapidly converted to phenytoin after i.v.
admin-
istration.64 It can be administered more rapidly i.v. or as
an
i.m. injection and is generally associated with fewer
injection
site complications. It is, however, significantly more
expen-
sive than phenytoin and not widely available in UK
hospitals.
Table 2 Drug administration details for CSE.102 Doses are i.v.
unless stated otherwise
Drug Dose Other information
Premonitory stage of status
Midazolam 10 mg nasal or buccal Dose can be repeated if
necessary
Diazepam 1020 mg p.r . or 0.20.3 mg kg21
Early status epilepticus
Lorazepam 0.1 mg kg21
; or 4 8 mg i.v. bolus Dose can be repeated if necessaryDiazepam
I.V.same dose as above
Established CSE
Phenytoin 15 18 mg kg21 loading dose given at 50 mg min21
Administer slowly through a large-bore cannula via
a 0.2mm filter, immediately after reconstitution
Phenobarbital 1015 mg kg21 given at 100 mg min21 Risk of
respiratory depression
Sodium
valproate10725 mg kg21 over 30 min then 100 mg h21 for 24 h
Levetiracetam 20003000 mg day21
Refractory CSE
Thiopental 100250mg i.v.bolus(then50 mgincrements until
seizures
controlled) then 35 mg kg21 h21Adjust dose to maintain burst
suppression. All will require
intensive care and ventilatory support
Titrate infusion doses to EEG burst suppression
Corticosteroid replacement required if etomidate
infusion is used
Midazolam 0.1 0.3 mg kg21 bolus then 0.050.4 mg kg21 h21
infusion Consider as an alternative to barbiturates
Propofol 2 mg kg21 i.v. bolus, then 510 mg kg21 h21
Ketamine 0.4 mg kg21 h21 then titrate up to response Dose from
case reports108 up to 7.5 mg kg21 h21109
BJA Perkset al.
566
-
7/21/2019 Anaesthesia and Epilepsy
6/10
Phenobarbital has been in use as an AED for nearly a
century and remains the most commonly used AED world-
wide. I.V. phenobarbital is an alternative to phenytoin as a
second-line agent for management of status epilepticus.
High doses are often required, with the attendant risk of
sed-
ation.65 66 It is not commonly used, for fear of provoking
re-
spiratory depression when administered to patients who
have already received benzodiazepines.
Sodium valproate has been available as i.v. preparationsince the
late 1990s and is being used increasingly in the
treatment of established CSE. In a randomized comparison
of i.v. valproate and phenytoin as the first-line treatment
for CSE in 68 patients, valproate had a better seizure
cessa-
tion rate as the first-line treatment (66% vs 42%, P,0.05)
and when crossed over as the second-line treatment (79%
vs25%,P,0.005), where the other drug had failed. 67 Partici-
pants in this study did not receive benzodiazepines as the
first-line therapy, which would be the accepted standard of
care. The data regarding the relative efficacy of the study
drugs should therefore be treated with caution. Moreover,
another study comparing the two agents used as initial
treatment for SE and acute repetitive seizures failed to
find
significant differences in efficacy, but valproate appeared
to
be better tolerated.68 Acute encephalopathy and hyperam-
monaemia remain potentially serious but fortunately rare
complications of valproate therapy.69
ThenewerAED levetiracetam hasbeen reported to be effect-
iveinseveralsmallcaseseriesofCSE. 70 74 It hasveryfavourable
pharmacokinetic characteristics, with no clinically
significant
interactions or sedative properties.75 Its efficacy as a
second-
line agent for the treatment of CSE remains to be
established.
Prospective studies are lacking, but a retrospective analysis
of
187 cases of CSE treated with levetiracetam, phenytoin, or
val-
proate as second-line agents has been published recently.
Theauthors reported that levetiracetam was more likely to fail
(48.3%) than valproate (25.4%) (odds ratio 2.69, 95% confi-
dence interval: 1.196.08). Phenytoin was not statistically
dif-
ferent from the other two agents (41.4%).76
Of other AEDs, topiramate77 79 and lacosamide80 83 have
been reported to be effective in controlling CSE in small
retro-
spective case series. Their role in the management of status
epilepticus remains uncertain.
Refractory status (3060 min)
Refractory CSE (RSE), where SE continues in spite of
adminis-
tration of two AEDs (e.g. benzodiazepines and phenytoin), is
associated with a high risk of complications. These
includetachyarrhythmias, pulmonary oedema, hyperthermia,
rhabdomyolysis, and aspiration pneumonia. RSE has a high
mortality rate and less than one-third of patients recover
to their pre-morbid level of functioning.84 85
In patients not responding to other measures, general an-
aesthesia shouldbe induced and maintained with midazolam,
propofol, or barbiturates (thiopental or pentobarbital).52
High-
dose propofol infusion should be considered with caution due
to the riskof propofolinfusion syndrome, and forthisreason
is
not recommended in children.86 EEG is needed to titrate
doses
and to ensure that electrographic seizures have been abol-
ished. Maximal therapy should be maintained until 1224 h
after the last clinical or electrographic seizure, after
which
the dose should be tapered. If seizures recur, therapy can
be
re-instituted or altered.87
Both propofol and thiopental are effective treatments for
RSE. Where one treatment has failed, another may be suc-
cessful.88 89 Thiopental has a lower rate of treatmentfailure
and breakthrough seizures, but a prolonged recovery,
duration of ventilation, and hospital stay.90 91 There has
been
increasing concern relating to the prolonged use of high-
dose propofol, due to the risk of propofol infusion
syndrome.
Cardiovascular collapse and mortality has been reported in
patients with no prior history of cardiac disease.92 93
Ketamine can be effective in cases of status epilepticus re-
fractory to other agents.94 There is also experimental evi-
dence that neuronal loss induced by status epilepticus may
be reduced by treatment with ketamine.95 However, these
potential benefits have to be balanced against the risk of
ketamine-related neurotoxicity which has been observed in
some cases.96 In patients who do not respond to i.v. anaes-
thetics, inhalation anaesthetics, such as isoflurane and
des-
flurane, have been shown to cause effective EEG burst
suppression. In a case series of seven patients, concentra-
tions of 1.25% isoflurane were used over a mean of 19
days, with some recurrence after cessation of treatment.
The authors see this as a tool to control seizures while
regular treatment is instituted.23 However, there are
clearly
technical difficulties with administration of volatile
agents.
Non-convulsive status epilepticus
NCSE is the term applied to the finding of electrographic
seizure patterns on EEG without clinically detectableseizure
phenomena. In the intensive care setting, such
patients are usually unconscious.97 Such cases may repre-
sent advanced CSE, where the motor activity has become
attenuated over time. This is a grave situation with almost
uniformly poor outcome. A variety of acute neurological
insults (encephalitis, stroke, trauma, and post-cardiac
arrest) may also present with coma and electrographic sei-
zures on EEG.98 100 The finding of NCSE usually indicates a
poorer prognosis for the underlying neurological condition.
However, a proportion of these patients show improvement
in consciousness level after treatment with AEDs. Therefore,
treatment with i.v. AEDs should be mandatory in all patients
in whom EEG diagnosis of status epilepticus is made. The
EEGdiagnosis of NCSE, however, is not straightforward and EEG
patterns that require treatment can be difficult to
determine.101
In the literature, the term NCSE is also used to describe
absence or complex partial status epilepticus.102 Absence
status occurs in a variety of idiopathic and symptomatic
generalized epilepsies. Complex partial seizures are
probably under recognized and may be more common in
the elderly.103 The typical manifestations of impaired
Anaesthesia and epilepsy BJA
567
-
7/21/2019 Anaesthesia and Epilepsy
7/10
consciousness with automatisms may not always be present.
This should be considered in the differential diagnosis of
all
confusional states, especially if there is a previous
history
of epilepsy or a structural brain abnormality. Absence and
complex partial status are not associated with the same
extent of cerebral damage as generalized tonic-clonic sei-
zures. The risk-associated aggressive treatment with i.v.
drugs is therefore thought not to be justifiable. Optimizing
existing AED therapy and use of oral benzodiazepines isoften
sufficient to improve consciousness level. The EEG diag-
nosis may require administration of rapidly acting i.v. AEDs
such as diazepam during EEG recording to observe clinical
and EEG response.101
Non-epileptic attack disorder (psychogenicnon-epileptic
seizure)
It must be noted that in specialist centres, the number of
psychogenic pseudo-status outnumber the number of
status epilepticus episodes.104 Psychogenic non-epileptic
attacks may also be particularly likely to occur in the
peri-
operative period.
105
There are a number of clinical featuresthat can help distinguish
this condition from epileptic sei-
zurescareful clinical observation is key.
Conclusions
Anaesthetists encounter epilepsy commonly in the peri-
operative setting. They may also be involved in airway man-
agement and administration of general anaesthesia for
treatment of status epilepticus. Awareness of pharmaco-
logical properties of AEDs and potential interactions with
drugs used in anaesthesia is essential for adequate manage-
ment of patients with epilepsy. While certain anaesthetic
agents can provoke seizures, recovery from anaesthesia can
be associated with shivering and myoclonus, which does
not indicate epilepsy. Patients with epilepsy may experience
breakthrough seizures in the perioperative period, but psy-
chogenic non-epileptic attacks can also occur in this
setting.
Status epilepticus is a common neurological emergency
and requires urgent management. Loss of benzodiazepine
responsiveness is a prominent feature in established CSE
and prompt treatment is important for seizure termination,
in addition to appropriate resuscitation. Second-line agents
include phenytoin or fosphenytoin and valproate, with
newer agents such as levetiracetam and lacosamide yet to
demonstrate clear evidence of efficacy. For refractory
status
epilepticus, general anaesthesia with midazolam, propofol,or
thiopental is the currently accepted treatment. Opioids
should be avoided. Clinical seizures can become less promin-
ent over time and electrographic monitoring is mandatory to
ensure that seizure control is achieved. NCSE should be con-
sidered in the unconscious patient where the cause is
unclear.
Declaration of interest
Speaker fee and conference hospitality given to R.M. from
both UCB pharma (manufacturers of levetiracetam and
lacosamide) and Eisai (manufacturers of zonisamide, rufina-
mide, and eslicarbazepine).
Funding
None.
References1 Commission on Classification and Terminology of the
Inter-
national League against Epilepsy. Proposal for revised
classifica-
tion of epilepsies and epileptic syndromes. Epilepsia 1989;
30:
38999
2 Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology
and
concepts for organization of seizures and epilepsies: report
of
the ILAE Commission on Classification and Terminology,
20052009. Epilepsia2010;51: 67685
3 Marson AG, Al-Kharusi AM, Alwaidh M,et al.The SANAD study
of
effectiveness of carbamazepine, gabapentin, lamotrigine,
oxcar-
bazepine, or topiramate for treatment of partial epilepsy:
an
unblinded randomised controlled trial. Lancet 2007; 369:
100015
4 Marson AG, Al-Kharusi AM, Alwaidh M,et al.The SANAD study
ofeffectiveness of valproate, lamotrigine, or topiramate for
gener-
alised and unclassifiable epilepsy: an unblinded randomised
controlled trial. Lancet 2007; 369: 101626
5 Brodie MJ. Antiepileptic drug therapy the story so far.
Seizure
2010; 19: 6505
6 Rogawski MA, Bazil CW. New molecular targets for
antiepileptic
drugs: alpha(2)delta, SV2A, and K(v)7/KCNQ/M potassium chan-
nels.Curr Neurol Neurosci Rep 2008; 8: 34552
7 Meldrum BS, Rogawski MA. Molecular targets for
antiepileptic
drug development. Neurotherapeutics2007;4: 1861
8 Anderson J, Moor CC. Antiepileptic drugs: a guide for the
non-
neurologist.Clin Med2010;10: 548
9 Patsalos PN, Perucca E. Clinically important drug interactions
in
epilepsy: interactions between antiepileptic drugs and
otherdrugs.Lancet Neurol2003;2: 47381
10 Johannessen Landmark C, Patsalos PN. Drug interactions
involv-
ing the new second- and third-generation antiepileptic
drugs.
Expert Rev Neurother2010; 10: 11940
11 Patsalos PN, Perucca E. Clinically important drug
interactions in
epilepsy: general features and interaction between
antiepileptic
drugs.Lancet Neurol2003; 2: 34756
12 Haroutiunian S, Ratz Y, Rabinovich B, Adam M, Hoffman A.
Valproic acid plasma concentration decreases in a
dose-independent manner following administration of merope-
nem: a retrospective study.J Clin Pharmacol 2009; 49: 13639
13 Mancl EE, Gidal BE. The effect of carbapenem antibiotics
on
plasma concentrations of valproic acid. Ann Pharmacother
2009; 43: 2082714 Kofke WA. Anesthetic management of the patient
with epilepsy
or prior seizures. Curr Opin Anesthesiol 2010; 23: 3919
15 Vaughn LK, Pruhs RJ. Strain-dependent variability in
nitrous
oxide withdrawal seizure frequency. Life Sci1995; 57: 112530
16 Artru AA, Lettich E, Colley PS, Ojemann GA. Nitrous oxide:
sup-
pression of focal epileptiform activity during inhalation,
and
spreading of seizure activity following withdrawal. J
Neurosurg
Anesthesiol 1990;2: 18993
17 Hornbein TF, Eger EI II, Winter PM, Smith G, Weststone D,
Smith KH. The minimum alveolar concentration of nitrous
oxide in man. Anesth Analg1982; 61: 5536
BJA Perkset al.
568
-
7/21/2019 Anaesthesia and Epilepsy
8/10
18 Modica PA, Tempelhoff R, White PF. Pro- and
anticonvulsant
effects of anesthetics (Part I). Anesth Analg1990; 70: 30315
19 Constant I, Seeman R, Murat I. Sevoflurane and epileptiform
EEG
changes.Paediatr Anaesth2005;15: 26674
20 Mohanram A, Kumar V, Iqbal Z, Markan S, Pagel PS.
Repetitive
generalized seizure activity during emergence from
sevoflurane
anesthesia.Can J Anaesth2007; 54: 65761
21 Sleigh JW, Vizuete JA, Voss L,et al.The electrocortical
effects of
enflurane: experiment and theory. Anesth Analg 2009; 109:
125362
22 Kruczek M, Albin MS, Wolf S, Bertoni JM. Postoperative
seizure
activity following enflurane anesthesia. Anesthesiology
1980;
53: 1756
23 Mirsattari SM, Sharpe MD, Young R. Treatment of
refractory
status epilepticus with inhalational anesthetic agents
isoflurane
and desflurane. Arch Neurol 2004; 61: 12549
24 Yillar DO, Akkan AG, Akcasu A, Ozuner Z, Eskazan E,
Kucukhuseyin C. The effect of oral and subcutaneous meperi-
dine on the maximal electroshock seizure (MES) in mice.
J Basic Clin Physiol Pharmacol2009;20: 15968
25 Tortella F. Endogenous opioid peptides and epilepsy:
quieting
the seizing brain? Trends Pharmacol Sci1988;9: 36672
26 Saboory E, Derchansky M, Ismaili M, et al. Mechanisms of
mor-phine enhancement of spontaneous seizure activity. Anesth
Analg2007; 105: 172935
27 Parkinson SK, Bailey SL, Little WL, Mueller JB. Myoclonic
seizure
activity in chronic high-dose spinal opioid administration.
Anesthesiology1990; 72: 7435
28 Shih CJ, Doufas AG, Chang HC, Lin CM. Recurrent seizure
activity
after epidural morphine in a post-partum woman.Can J Anaesth
2005; 52: 7279
29 Borgeat A, Biollaz J, Depierraz B, Neff R. Grand mal
seizure
after extradural morphine analgesia. Br J Anaesth 1988; 60:
7335
30 Grnlykke L, Knudsen ML, Hgenhaven H, Moltke FB, Madsen
FF,
Kjaer TW. Remifentanil-induced spike activity as a
diagnostic
tool in epilepsy surgery. Acta Neurol Scand2008; 117: 90331
McGuire G, El-Beheiry H, Manninen P, Lozano A, Wennberg R. Ac-
tivation of electrocorticographic activity with remifentanil
and
alfentanil during neurosurgical excision of epileptogenic
focus.
Br J Anaesth 2003; 91: 6515
32 Akcaboy ZN, Akcaboy EY, Yigitbasl B,et al.Effects of
remifentanil
and alfentanil on seizure duration, stimulus amplitudes and
re-
covery parameters during ECT. Acta Anaesthesiol Scand 2005;
49: 106871
33 Lowenstein D, Aminoff M, Simon R. Barbiturate anesthesia in
the
treatment of status epilepticus: clinical experience with 14
patients. Neurology1988; 38: 395400
34 Brown A, Horton J. Status epilepticus treated by intravenous
in-
fusion of thiopentone sodium. Br Med J 1967; 1: 278
35 Power KN, Flaatten H, Gilhus NE, Engelsen BA. Propofol
treat-ment in adult refractory status epilepticus. Mortality risk
and
outcome.Epilepsy Res2011; 94: 5360
36 Hymes JA. Seizure activity during isoflurane anesthesia.
Anesth
Analg1985; 64: 3678
37 Trzepacz PT, Weniger FC, Greenhouse J. Etomidate
anesthesia
increases seizure duration during ECT. A retrospective
study.
Gen Hosp Psychiatry1993;15: 11520
38 Reddy R, Moorthy S, Dierdorf S, Deitch R, Link L. Excitatory
effects
and electroencephalographic correlation of etomidate,
thiopen-
tal, methohexital, and propofol. Anesth Analg 1993; 77:
100811
39 Smith M, Smith SJ, Scott CA, Harkness WF. Activation of the
elec-
trocorticogram by propofol during surgery for epilepsy. Br J
Anaesth1996; 76: 499502
40 Myslobodsky MS, Golovchinsky V, Mintz M. Ketamine:
convulsant
or anti-convulsant?Pharmacol Biochem Behav1981;14: 2733
41 Modica PA, Tempelhoff R, White PF. Pro- and
anticonvulsant
effects of anesthetics (Part II). Anesth Analg1990; 70:
43344
42 Usubiaga JE, Moya F, Wikinski JA, Wikinski R, Usubiaga LE.
Rela-
tionship between the passage of local anaesthetics across
the
bloodbrain barrier and their effects on the central nervous
system. Br J Anaesth1967; 39: 9437
43 Steen PA, Michenfelder JD. Neurotoxicity of anesthetics.
Anesthesiology1979; 50: 43753
44 Veering BT. Complications and local anaesthetic toxicity in
re-
gional anaesthesia. Curr Opin Anaesthesiol 2003; 16: 4559
45 Pascual J, Ciudad J, Berciano J. Role of lidocaine
(lignocaine) in
managing status epilepticus. J Neurol Neurosurg Psychiatry
1992; 55: 4951
46 Hamano S, Sugiyama N, Yamashita S, et al. Intravenous
lido-
caine for status epilepticus during childhood. Dev Med Child
Neurol 2006; 48: 2202
47 Yildiz B, Citak A, Ucsel R, Karabocuoglu M, Aydinli N, Uzel
N. Lido-
caine treatment in pediatric convulsive status
epilepticus.Pediatr Int 2008;50: 359
48 Katz Y, Weizman A, Pick CG,et al.Interactions between
laudano-
sine, GABA, and opioid subtype receptors: implication for
lauda-
nosine seizure activity. Brain Res 1994; 646: 23541
49 Lanier WL, Milde JH, Michenfelder JD. Cerebral stimulation
fol-
lowing succinylcholine in dogs. Anesthesiology1986;64: 5519
50 Schneck HJ, Rupreht J. Central anticholinergic syndrome (CAS)
in
anesthesia and intensive care. Acta Anaesthesiol
Belg1989;40:
21928
51 Lowenstein DH, Bleck T, Macdonald RL. Its time to revise
the
definition of status epilepticus. Epilepsia1999; 40: 1202
52 Kelso ARC, Cock HR. Status epilepticus.Practical Neurol
2005;5:
32233
53 Kapur J, Macdonald RL. Rapid seizure-induced reduction
ofbenzodiazepine and Zn2+ sensitivity of hippocampal dentate
granule cell GABAA receptors. J Neurosci1997; 17: 753240
54 Naylor DE, Liu H, Wasterlain CG. Trafficking of GABA(A)
receptors,
loss of inhibition, and a mechanism for pharmacoresistance
in
status epilepticus. J Neurosci2005;25: 772433
55 Ashrafi MR, Khosroshahi N, Karimi P,et al.Efficacy and
usability
of buccal midazolam in controlling acute prolonged
convulsive
seizures in children. Eur J Paediatr Neurol 2010; 14: 4348
56 Nakken KO, Lossius MI. Buccal midazolam or rectal diazepam
for
treatment of residential adult patients with serial seizures
or status epilepticus. Acta Neurol Scand 2011; 124:
99103
57 Aylward RL. Epilepsy: a review of reports, guidelines,
recommen-
dations and models for the provision of care for patients
withepilepsy.Clin Med2008;8: 4338
58 Meierkord H, Poon B, Engelsen B, et al. EFNS guideline on
the
management of status epilepticus in adults. Eur J Neurol
2010;
17: 34855
59 Schmidt D, Wilensky A. Benzodiazepines. In: Engel J, Pedly
T,
eds. Epilepsy: A Comprehensive Textbook, 2nd Edn.
Philadelphia,
PA: Lippincott Williams & Wilkins, 2008; 1531 41
60 Treiman DM, Meyers PD, Walton NY, et al. A comparison of
four
treatments for generalized convulsive status epilepticus.
Veter-
ans Affairs Status Cooperative Study Group. N Engl J Med
1998; 339: 7928
Anaesthesia and epilepsy BJA
569
-
7/21/2019 Anaesthesia and Epilepsy
9/10
61 Cock HR, Schapira AH. A comparison of lorazepam and
diaze-
pam as initial therapy in convulsive status epilepticus. QJM
2002; 95: 22531
62 Towne AR, DeLorenzo RJ. Use of intramuscular midazolam
for
status epilepticus. J Emerg Med 1999; 17: 3238
63 Trinka E. What is the relative value of the standard
anticonvul-
sants: phenytoin and fosphenytoin, phenobarbital, valproate,
and levetiracetam? Epilepsia2009; 50(Suppl. 12): 403
64 Stern J, Perrucca E, Browne T. Phenytoin, fosphenytoin and
other
hydantoins. In: Engel J, Pedly T, eds. Epilepsy: A
Comprehensive
Textbook, 2nd Edn. Philadelphia, PA: Lippincott Williams
&
Wilkins, 2008; 16202
65 Crawford TO, Mitchell WG, Fishman LS, Snodgrass SR.
Very-high-dose phenobarbital for refractory status
epilepticus
in children. Neurology1988; 38: 103540
66 Lee WK, Liu KT, Young BW. Very-high-dose phenobarbital
for
childhood refractory status epilepticus. Pediatr Neurol
2006;
34: 635
67 Misra UK, Kalita J, Patel R. Sodium valproate vs
phenytoin
in status epilepticus: a pilot study. Neurology 2006; 67:
3402
68 Gilad R, Izkovitz N, Dabby R,et al.Treatment of status
epilepticus
and acute repetitive seizures with i.v. valproic acid vs
phenytoin.
Acta Neurol Scand 2008; 118: 296300
69 Segura-Bruna N, Rodriguez-Campello A, Puente V, Roquer J.
Valproate-induced hyperammonemic encephalopathy. Acta
Neurol Scand2006;114: 17
70 Moddel G, Bunten S, Dobis C, et al. Intravenous
levetiracetam: a
new treatment alternative for refractory status epilepticus.
J Neurol Neurosurg Psychiatry2009; 80: 68992
71 Berning S, Boesebeck F, van Baalen A, Kellinghaus C.
Intraven-
ous levetiracetam as treatment for status epilepticus. J
Neurol
2009; 256: 163442
72 Gamez-Leyva G, Aristn JL, Fernandez E, Pascual J.
Experience
with intravenous levetiracetam in status epilepticus: a
retro-
spective case series. CNS Drugs2009; 23: 9837
73 Beyenburg S, Reuber M, Maraite N. Intravenous levetiracetam
forepileptic seizure emergencies in older people.
Gerontology2009;
55: 2731
74 Eue S, Grumbt M, Muller M, Schulze A. Two years of experience
in
the treatment of status epilepticus with intravenous
levetirace-
tam.Epilepsy Behav2009;15: 4679
75 Uges JW, van Huizen MD, Engelsman J, et al. Safety and
pharmacokinetics of intravenous levetiracetam infusion as
add-on in status epilepticus.Epilepsia2009;50: 41521
76 Alvarez V, Januel JM, Burnand B, Rossetti AO. Second-line
status
epilepticus treatment: comparison of phenytoin, valproate,
and
levetiracetam. Epilepsia2011; 52: 12926
77 Towne AR, Garnett LK, Waterhouse EJ, Morton LD, DeLorenzo
RJ.
The use of topiramate in refractory status epilepticus.
Neurology
2003; 60: 332478 Bensalem MK, Fakhoury TA. Topiramate and status
epilepticus:
report of three cases. Epilepsy Behav2003; 4: 75760
79 Perry MS, Holt PJ, Sladky JT. Topiramate loading for
refractory
status epilepticus in children. Epilepsia2006; 47: 10701
80 Albers JM, Moddel G, Dittrich R, et al. Intravenous
lacosamide
an effective add-on treatment of refractory status
epilepticus.
Seizure2011; 20: 42830
81 Goodwin H, Hinson HE, Shermock KM, Karanjia N, Lewin JJ
III.
The use of lacosamide in refractory status epilepticus.
Neurocrit
Care2011; 14: 34853
82 Koubeissi MZ, Mayor CL, Estephan B, Rashid S, Azar NJ.
Efficacy
and safety of intravenous lacosamide in refractory
nonconvul-
sive status epilepticus. Acta Neurol Scand2011; 123: 1426
83 Kellinghaus C, Berning S, Immisch I,et al. Intravenous
lacosa-
mide for treatment of status epilepticus. Acta Neurol Scand
2011; 123: 13741
84 Helmstaedter C. Cognitive outcome of status epilepticus
in
adults.Epilepsia2007;48(Suppl. 8): 8590
85 Cooper AD, Britton JW, Rabinstein AA. Functional and
cognitive
outcome in prolonged refractory status epilepticus. Arch
Neurol 2009; 66: 15059
86 Vasile B, Rasulo F, Candiani A, Latronico N. Propofol
infusion syn-
drome.Intensive Care Med 2003; 29: 141725
87 Holtkamp M. The anaesthetic and intensive care of status
epi-
lepticus.Curr Opin Neurol 2007;20: 18893
88 MacKenzie S, Kapadia F, Grant I. Propofol infusion for
control of
status epilepticus. Anaesthesia1990; 45: 10435
89 Pitt-Miller P, Elcock B, Maharaj M. The management of
status
epilepticus with a continuous propofol infusion. Anesth
Analg
1994; 78: 11934
90 Parviainen I, Kalviainen R, Ruokonen E. Propofol and
barbitu-
rates for the anesthesia of refractory convulsive status
epilep-
ticus: pros and cons. Neurol Res 2007; 29: 6677191 Rossetti AO,
Logroscino G, Liaudet L,et al.Status epilepticus: an
independent outcome predictor after cerebral
anoxia.Neurology
2007; 69: 25560
92 Zarovnaya EL, Jobst BC, Harris BT. Propofol-associated fatal
myo-
cardial failure and rhabdomyolysis in an adult with status
epi-
lepticus.Epilepsia2007; 48: 10026
93 Iyer V, Hoel R, Rabinstein AA. Propofol infusion syndrome
in
patients with refractory status epilepticus: an 11-year
clinical
experience.Crit Care Med2009; 37: 302430
94 Hsieh CY, Sung PS, Tsai JJ, Huang CW. Terminating prolonged
re-
fractory status epilepticus using ketamine. Clin
Neuropharmacol
2010; 33: 1657
95 Fujikawa DG. Neuroprotective effect of ketamine
administered
after status epilepticus onset. Epilepsia1995; 36: 1869596 Ubogu
EE, Sagar SM, Lerner AJ, Maddux BN, Suarez JI, Werz MA.
Ketamine for refractory status epilepticus: a case of
possible
ketamine-induced neurotoxicity. Epilepsy Behav2003; 4: 705
97 Towne AR, Waterhouse EJ, Boggs JG,et al. Prevalence of
non-
convulsive status epilepticus in comatose patients.
Neurology
2000; 54: 3405
98 Waterhouse EJ, Vaughan JK, Barnes TY,et al. Synergistic
effect
of status epilepticus and ischemic brain injury on
mortality.
Epilepsy Res1998; 29: 17583
99 Vespa PM, Nuwer MR, Nenov V,et al. Increased incidence
and
impact of nonconvulsive and convulsive seizures after
traumatic
brain injury as detected by continuous
electroencephalographic
monitoring.J Neurosurg 1999; 91: 75060
100 Rossetti AO, Milligan TA, Vulliemoz S, Michaelides C,
Bertschi M,Lee JW. A randomized trial for the treatment of
refractory status
epilepticus.Neurocrit Care2011; 14: 410
101 Jirsch J, Hirsch LJ. Nonconvulsive seizures: developing a
rational
approach to the diagnosis and management in the critically
ill
population.Clin Neurophysiol2007; 118: 166070
102 Shorvon S. What is nonconvulsive status epilepticus, and
what
are its subtypes? Epilepsia2007; 48(Suppl. 8): 358
103 Beyenburg S, Elger CE, Reuber M. Acute confusion or
altered
mental state: consider nonconvulsive status epilepticus.
Gerontology2007;53: 38896
BJA Perkset al.
570
-
7/21/2019 Anaesthesia and Epilepsy
10/10
104 Howell SJ, Owen L, Chadwick DW. Pseudostatus epilepticus.
QJM
1989; 71: 50719
105 Reuber M, EnrightSM, Goulding PJ.Postoperativepseudostatus:
not
everything that shakes is epilepsy.Anaesthesia2000; 55: 748
106 Shorvon SD. Emergency treatment of acute seizures, serial
sei-
zures, seizure cluster and status epilepticus. In: Shorvon
SD,
ed. Handbook of Epilepsy Treatment. Oxford: Blackwell
Science, 2000
107 Olsen KB, Tauboll E, Gjerstad L. Valproate is an effective,
well-
tolerated drug for treatment of status epilepticus/serial
attacks in adults. Acta Neurol Scand Suppl 2007; 187:
514
108 Pruss H, Holtkamp M. Ketamine successfully terminates
malig-
nant status epilepticus. Epilepsy Res 2008; 82: 21922
109 Sheth RD, Gidal BE. Refractory status epilepticus: response
to
ketamine. Neurology1998; 51: 176566
Anaesthesia and epilepsy BJA
571