Embed Size (px)
Citation preview

Anaesthesia and the Obese Patient
Lucy SmithConsultant Anaesthetist, St George’s Hospital15th January 2009

Outline
Definitions/ EpidemiologyDefinitions/ Epidemiology Physiology of ObesityPhysiology of Obesity ComorbiditiesComorbidities Practical Aspects of AnaesthesiaPractical Aspects of Anaesthesia Bariatric SurgeryBariatric Surgery

Definitions based on BMI
BMI (kgmBMI (kgm-2-2)) DefinitionDefinition
<18.5<18.5 UnderweightUnderweight
18.5-24.918.5-24.9 Ideal WeightIdeal Weight
25-29.925-29.9 OverweightOverweight
30-39.930-39.9 ObeseObese
40-49.9 or 35-49.9 40-49.9 or 35-49.9 withwith
obesity-related comorbidityobesity-related comorbidity
Morbidly ObeseMorbidly Obese
50-59.950-59.9 Super ObeseSuper Obese
60-69.960-69.9 Super Super ObeseSuper Super Obese
>70>70 Hyper ObeseHyper Obese

Limitations BMI
Not a direct measure of adiposityNot a direct measure of adiposity No account of fat distributionNo account of fat distribution No account of duration of obesityNo account of duration of obesity Inaccurate at extremes of heightInaccurate at extremes of height Inaccurate with extremes of lean body mass Inaccurate with extremes of lean body mass
(eg athletes, elderly)(eg athletes, elderly) Waist or collar circumference more Waist or collar circumference more
predictive of cardio-respiratory comorbiditypredictive of cardio-respiratory comorbidity

Fat Distribution
AndroidAndroid Central distributionCentral distribution High intra-peritoneal fat contentHigh intra-peritoneal fat content Increased neck circumferenceIncreased neck circumference Waist-hip ratio >0.8 women, >1.0 menWaist-hip ratio >0.8 women, >1.0 men Increased morbidity (airway, CVS, Increased morbidity (airway, CVS,
metabolic, surgical)metabolic, surgical)
GynaecoidGynaecoid Peripheral sites (arms, legs, buttocks)Peripheral sites (arms, legs, buttocks)

Epidemiology of Obesity
Epidemic in developed worldEpidemic in developed world Increasing prevalenceIncreasing prevalence Major healthcare challengeMajor healthcare challenge DOH reports:DOH reports:
Overweight ObeseOverweight Obese
MM FF MM FF
20012001 43%43% 29%29% 13%13% 16%16%
20062006 43%43% 33%33% 22%22% 23%23%

Treatment Strategies
Multidisciplinary approachMultidisciplinary approach DietDiet Physical activitiesPhysical activities Behavioral interventionsBehavioral interventions DrugsDrugs SurgerySurgery

Physiology of Obesity
Multifactorial - genetic, environmentalMultifactorial - genetic, environmental Complex regulation of appetite and satietyComplex regulation of appetite and satiety Multiple humoral and neurological Multiple humoral and neurological
mechanismsmechanisms Integrated and processed in hypothalamusIntegrated and processed in hypothalamus Hormones include leptin, insulin, ghrelin, Hormones include leptin, insulin, ghrelin,
peptide YYpeptide YY3-363-36
Energy balance and appetite reflexes Energy balance and appetite reflexes mediated by ANSmediated by ANS

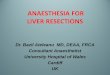
Pathways of energy balance
HYPOTHALAMUS ventromedial
HYPOTHALAMUS paraventricular nucleus lateral hypothalamic area
LEPTIN adipose tissue content
INSULIN acute metabolic status
GHRELIN from stomach signal hunger
Peptide YY3-36 from small intestine signals satiety
APPETITE REGULATION ⇑ neuropeptide Y ⇓ melanocyte stimulating hormone
FOOD SEEKING BEHAVIOUR
AUTONO MICNERVOUS SYSTEM
SNS- ⇑ energy use
PNS– insulin secretion and energy storage
CNS inputs

Models of obesity pathology
Overeating and inactivity simplistic viewOvereating and inactivity simplistic view Various pathways suggestedVarious pathways suggested Interactions not clearly establishedInteractions not clearly established Key features includeKey features include
Hyperinsulinaemia (Hyperinsulinaemia (fat deposition)fat deposition) Insulin resistance (type 2 diabetes)Insulin resistance (type 2 diabetes) Defective leptin signalling (Defective leptin signalling (satiety)satiety) food reward 2food reward 200 to to dopamine clearance in dopamine clearance in
brain (insulin-mediated)brain (insulin-mediated)

Obesity-related Comorbidities
Prevalence increases with Prevalence increases with BMI and BMI and duration of obesityduration of obesity
May be reason to undergo surgeryMay be reason to undergo surgery Severity may be masked by sedentary Severity may be masked by sedentary
lifestylelifestyle Major impact in perioperative periodMajor impact in perioperative period

Pathophysiology - Respiratory
Higher energy turnoverHigher energy turnover OO22 consumption, consumption, CO CO2 2 productionproduction +/- chronic hybercarbia with renal +/- chronic hybercarbia with renal
compensation and altered COcompensation and altered CO2 2 sensitivitysensitivity FRC, FRC, VC, VC, (A-a) O(A-a) O2, 2, shuntshunt Airway closure (CC greater than FRC)Airway closure (CC greater than FRC) chest wall compliance and chest wall compliance and lung lung
compliance compliance work of breathingwork of breathing

Respiratory Comorbidity
AirwayAirway Obstructive Sleep ApnoeaObstructive Sleep Apnoea Obesity Hypoventilation SyndromeObesity Hypoventilation Syndrome AsthmaAsthma Pulmonary HypertensionPulmonary Hypertension

Airway
Difficulty predicted by OSA, short thick Difficulty predicted by OSA, short thick neck and neck and BMIBMI
Fatty infiltration pharyngeal wallFatty infiltration pharyngeal wall pharyngeal wall compliancepharyngeal wall compliance Difficult to ventilate by face maskDifficult to ventilate by face mask Rapid desaturationRapid desaturation Consider awake fibreoptic intubationConsider awake fibreoptic intubation

Obstructive Sleep Apnoea
Apnoeic episodes 2˚ to pharyngeal collapse Apnoeic episodes 2˚ to pharyngeal collapse occurring during sleepoccurring during sleep
Airfow ceases, ongoing effort, closed airwayAirfow ceases, ongoing effort, closed airway >10s, >5/hour, >30/night>10s, >5/hour, >30/night Snoring, daytime somnolence, am headachesSnoring, daytime somnolence, am headaches Hypoxaemia, 2˚polycythaemia, systemic Hypoxaemia, 2˚polycythaemia, systemic
vasoconstriction, hypercarbia, pulmonary vasoconstriction, hypercarbia, pulmonary vasoconstriction, RVFvasoconstriction, RVF

Obesity Hypoventilation Syndrome
Altered control of breathingAltered control of breathing Diurnal variationDiurnal variation PaCOPaCO22 >5.9kPa with >5.9kPa with 1.3kPa asleep1.3kPa asleep sOsO22 not explained by obstruction not explained by obstruction ventilatory response to COventilatory response to CO22
Often coexists with OSAOften coexists with OSA (OSAHS- Obstructive Sleep Apnoea (OSAHS- Obstructive Sleep Apnoea
Hypopnoea Syndrome)Hypopnoea Syndrome)

Asthma
Multiple factorsMultiple factors Acid reflux and micro aspirationAcid reflux and micro aspiration Sleep apnoea and partial obstructionSleep apnoea and partial obstruction Peripheral airway closure Peripheral airway closure sheer stressessheer stresses
proinflammatory responseproinflammatory response Bariatric surgery Bariatric surgery 80-100% resolution 80-100% resolution

Pathophysiology - Cardiovascular
blood volume + blood volume + cardiac outputcardiac output ventricular workloadventricular workload myocardial fat content + myocardial fat content + contractilitycontractility Endothelial dysfunction +Endothelial dysfunction +vascular resistancevascular resistance 50% moderate HT, 5-10% severe HT50% moderate HT, 5-10% severe HT +/- progressive +/- progressive PVR and PAPPVR and PAP Progresses to RVF. Oedema and hepatic Progresses to RVF. Oedema and hepatic
congestioncongestion

Cardiovascular Comorbidity
HypertensionHypertension Obesity cardiomyopathyObesity cardiomyopathy Ischaemic Heart Disease (multiple factors)Ischaemic Heart Disease (multiple factors) Arrhythmias (hypoxaemia, hypertrophy, Arrhythmias (hypoxaemia, hypertrophy,
hypokalaemia, coronary art disease, raised hypokalaemia, coronary art disease, raised catecholamines, OSA, fatty infiltration catecholamines, OSA, fatty infiltration conducting and pacing systems)conducting and pacing systems)
Cor pulmonaleCor pulmonale

Gastrointestinal Comorbidity
Type 2 diabetesType 2 diabetes intra-abdominal pressureintra-abdominal pressure FRC, aortocaval compression,FRC, aortocaval compression,
tissue perfusion,tissue perfusion,risk abdo compartment syndromerisk abdo compartment syndrome
Fatty liver, steatohepatitis, cirrhosisFatty liver, steatohepatitis, cirrhosis Hiatus hernia, gastro-oesophageal refluxHiatus hernia, gastro-oesophageal reflux HyperlipidaemiaHyperlipidaemia

Musculo-skeletal and Other
OsteoarthritisOsteoarthritis Compression fracturesCompression fractures Increased risk of injuryIncreased risk of injury Urinary incontinenceUrinary incontinence Skin infections, candidiasis, poor hygieneSkin infections, candidiasis, poor hygiene Varicose veinsVaricose veins LymphoedemaLymphoedema

Preoperative Assessment
Anaesthetic historyAnaesthetic history Details of ComorbiditiesDetails of Comorbidities Drug history (appetite suppressants)Drug history (appetite suppressants) Airway (MP, neck extension, circumference)Airway (MP, neck extension, circumference) Ability to tolerate supine positionAbility to tolerate supine position Routine and specific investigations (may Routine and specific investigations (may
include baseline ABG, lung function tests, include baseline ABG, lung function tests, sleep studies, Echo, cardiac cath and PA sleep studies, Echo, cardiac cath and PA pressure studies)pressure studies)

Practical Aspects of Anaesthesia Location: Operating theatre onlyLocation: Operating theatre only Staff: plenty of strong, trained people!Staff: plenty of strong, trained people! Equipment: appropriate trolleys + table, Equipment: appropriate trolleys + table,
electric beds, large BP cuffs, pillows,electric beds, large BP cuffs, pillows,
patslide/ hover mattress, airwaypatslide/ hover mattress, airway Premed: HPremed: H2 2 antagonist/ PPIantagonist/ PPI
Positioning: Patient climb onto table,Positioning: Patient climb onto table,
head up tilt 30˚, ‘ramped’- wedge under head up tilt 30˚, ‘ramped’- wedge under shoulders (sternum to thyroid cartilage - shoulders (sternum to thyroid cartilage - horizontal level)horizontal level)

Induction
iv access (dorsum hand, flexor aspect iv access (dorsum hand, flexor aspect forearm, central with US guidance)forearm, central with US guidance)
Consider arterial lineConsider arterial line Preoxygenation at least 5 minsPreoxygenation at least 5 mins +/- RSI (dose sux 1mg/kg real body wt)+/- RSI (dose sux 1mg/kg real body wt) Intubation (short handle, long blade,)Intubation (short handle, long blade,) Awake fibreoptic intubation if indicatedAwake fibreoptic intubation if indicated

Maintenance Short acting agents eg sevoflurane, Short acting agents eg sevoflurane,
desflurane, remifentanildesflurane, remifentanil Temperature maintenanceTemperature maintenance Neuromuscular monitoringNeuromuscular monitoring Ventilate with PEEPVentilate with PEEP Pressure areas and skinPressure areas and skin Calf compressionCalf compression Fluids - insensible losses Fluids - insensible losses BSA BSA SV/ pulse pressure optimisationSV/ pulse pressure optimisation

Recovery
Aim: rapid emergence with good airway Aim: rapid emergence with good airway controlcontrol
Risks: loss of airway control, inadequate Risks: loss of airway control, inadequate respiration, aspiration, postop chest respiration, aspiration, postop chest complications, CVS stress and instabilitycomplications, CVS stress and instability
Extubate wide-awake and sitting up +/- CPAPExtubate wide-awake and sitting up +/- CPAP
recruitment procedure prior to extubationrecruitment procedure prior to extubation Appropriate postop environmentAppropriate postop environment

Analgesia
Multimodal - paracetamol, NSAIDs, Multimodal - paracetamol, NSAIDs, opioids, LA, regionalopioids, LA, regional
Paracetamol - central compartment so normal Paracetamol - central compartment so normal dose, dose, clearance clearance dose frequencydose frequency
NSAIDs - NSAIDs - risk renal dysfunctionrisk renal dysfunction Opioids - Opioids - risk respiratory depressionrisk respiratory depression Regional - higher failure rateRegional - higher failure rate

Bariatric Surgery
Weight loss surgeryWeight loss surgery Procedures to treat obesity by Procedures to treat obesity by
modification of GI tract to reduce nutrient modification of GI tract to reduce nutrient intake and/or reduce absorptionintake and/or reduce absorption
‘‘Tool’ enabling patient to alter lifestyle Tool’ enabling patient to alter lifestyle and eating habits to achieve effective and and eating habits to achieve effective and permanent management of obesity and permanent management of obesity and eating behavioureating behaviour

Bariatric SurgeryNICE Dec 2006 (CG43)
Recommended as option if:Recommended as option if: BMI>40 (or 35 with significant BMI>40 (or 35 with significant
comorbidity or severe DM)comorbidity or severe DM) All non-surgical measures tried and failedAll non-surgical measures tried and failed Specialist obesity service involvedSpecialist obesity service involved Fit for anaesthesia and surgeryFit for anaesthesia and surgery Committed to long-term follow upCommitted to long-term follow up First line option when BMI>50First line option when BMI>50

Principles of Bariatric Surgery
Reduction of stomach size (restrictive)Reduction of stomach size (restrictive)
food enters small upper gastric pouchfood enters small upper gastric pouch
passes into lower stomach or intestinepasses into lower stomach or intestine
early filling, discomfort on eating moreearly filling, discomfort on eating more Restriction of size of gastric outletRestriction of size of gastric outlet
pouch or stomach remain full for longerpouch or stomach remain full for longer Induction of malabsorption by intestinal bypassInduction of malabsorption by intestinal bypass

Vertical Banded Gastroplasty
RestrictiveRestrictive ‘‘Stomach stapling’Stomach stapling’ Smaller pre-stomach Smaller pre-stomach
pouchpouch Small communicationSmall communication Rapid satietyRapid satiety Upper part may Upper part may
distend over timedistend over time

Adjustable Gastric Band
RestrictiveRestrictive Silicone bandSilicone band Small upper pouch Small upper pouch
approx 25mlapprox 25ml Inject saline via s/c Inject saline via s/c
port to adjust band to port to adjust band to early satietyearly satiety
Upper pouch can Upper pouch can distenddistend
Band can become Band can become displaceddisplaced

Sleeve Gastrectomy
RestrictiveRestrictive Reduces stomach to 15% original sizeReduces stomach to 15% original size Remove large portion following greater Remove large portion following greater
curvecurve Open edges joined to form sleeve or tubeOpen edges joined to form sleeve or tube Early fullness, no outflow obstructionEarly fullness, no outflow obstruction May be converted in 2nd stage procedure May be converted in 2nd stage procedure
to gastric bypass or duodenal switchto gastric bypass or duodenal switch

Roux-en-Y Gastric Bypass
Mixed restrictive and Mixed restrictive and malabsorptivemalabsorptive
Small stomach pouchSmall stomach pouch Connect pouch to Connect pouch to
small intestinesmall intestine Upper small intestine Upper small intestine
re-attached in y-shape re-attached in y-shape approx 45cm below approx 45cm below stomach outletstomach outlet

Sleeve Gastrectomy with Duodenal Switch
Mixed restrictive and Mixed restrictive and malabsorptivemalabsorptive
Stomach Stomach disconnected from disconnected from duodenumduodenum
Connected to distal Connected to distal small intestinesmall intestine
Duodenum and upper Duodenum and upper small intestine small intestine attached 75-100cm attached 75-100cm from colonfrom colon

Jejunoileal Bypass
Malabsorptive procedure no longer Malabsorptive procedure no longer performedperformed
Proximal jejunum anastomosed to distal Proximal jejunum anastomosed to distal ileum, 10cm before caecumileum, 10cm before caecum
Short length functional bowelShort length functional bowel Long blind loopLong blind loop Problems with severe malabsorption, Problems with severe malabsorption,
dumping, liver failure, cardiac failure, dumping, liver failure, cardiac failure, renal stonesrenal stones

Laparoscopic Bariatric Surgery Head-up position (up to 45˚)Head-up position (up to 45˚)
venous pooling in lower limbsvenous pooling in lower limbsvenous return, venous return, cardiac outputcardiac output
PneumoperitoneumPneumoperitoneumvenous return, venous return, cardiac outputcardiac outputintra-abdominal pressureintra-abdominal pressuremigration gas into tissuesmigration gas into tissues
progressive progressive pCOpCO22
activation SNS - arrythmias, activation SNS - arrythmias, SVR, SVR, BPBP
PAP, PAP, ICPICPHigh inpiratory pressure + PEEPHigh inpiratory pressure + PEEP

Complications of Bariatric Surgery
GeneralGeneral
infection, haemorrhage, incisional infection, haemorrhage, incisional hernia, bowel obstruction, VTEhernia, bowel obstruction, VTE
SpecificSpecific
anastomotic leak, anastomotic anastomotic leak, anastomotic stricture, dumping syndrome, stricture, dumping syndrome, nutritional deficiencies (iron, vit Bnutritional deficiencies (iron, vit B1212, ,
thiamine, protein malnutrition, vit A)thiamine, protein malnutrition, vit A)

Risk Factors for Complications
M>FM>F Age >65Age >65 Open SurgeryOpen Surgery Long operation timeLong operation time Cardiac and Respiratory comorbiditiesCardiac and Respiratory comorbidities DiabetesDiabetes Low case loadLow case load

Health Benefits Sustained loss of 65-80% excess body weightSustained loss of 65-80% excess body weight Diabetes resolves very rapidlyDiabetes resolves very rapidly Asthma resolves early onAsthma resolves early on OSA - most asymptomatic in 1 yearOSA - most asymptomatic in 1 year Hyperlipidaemia resolved in >70%Hyperlipidaemia resolved in >70% Essential hypertension resolved in >70%Essential hypertension resolved in >70% GOR relieved in mostGOR relieved in most Low back pain and joint pain relieved in mostLow back pain and joint pain relieved in most self esteem, self esteem, participation in social activitiesparticipation in social activities

Summary
Obesity is a major healthcare challengeObesity is a major healthcare challenge Daily challenge for anaesthetistsDaily challenge for anaesthetists Obese patients are at risk from Obese patients are at risk from
comorbidities and pathophysiological comorbidities and pathophysiological changes of obesitychanges of obesity
Bariatric surgery is a beneficial and cost-Bariatric surgery is a beneficial and cost-effective healthcare interventioneffective healthcare intervention