Embed Size (px)
Citation preview

NEWSANAESTHESIA
ISSN 0959-2962 No. 314
SEPTEMBER 2013
The NewsleTTer of The
AssociATioN of ANAesTheTisTs of GreAT BriTAiN
ANd irelANd
INSIDE THIS ISSUE: National Essential Anaesthetic Drug List Who are your competitors? The NIAA’s Health Services Research Centre Giving Evidence to the Shape of Training Review

Anaesthesia News September 2013 • Issue 314 3
contents
06
18
09
The Association of Anaesthetists of Great Britain and Ireland21 Portland Place, London W1B 1PYTelephone: 020 7631 1650Fax: 020 7631 4352Email: [email protected]: www.aagbi.org
Anaesthesia NewsChair Editorial Board: Felicity Plaat Editors: Kate O’Connor and Caroline Wilson (GAT), Val Bythell, Richard Griffiths, Nancy Redfern, Sean Tighe, Iain Wilson and Tom WoodcockAddress for all correspondence, advertising or submissions: Email: [email protected]: www.aagbi.org/publications/anaesthesia-news
Design: Christopher SteerAAGBI Website & Publications Officer Telephone: 020 7631 8803Email: [email protected]: Portland Print
Copyright 2013 The Association of Anaesthetists of Great Britain and Ireland
The Association cannot be responsible for the statements or views of the contributors. No part of this newsletter may be reproduced without prior permission.
Advertisements are accepted in good faith. Readers are reminded that Anaesthesia News cannot be held responsible in any way for the quality or correctness of products or services offered in advertisements.
3
EditorialI’ve just listened to Jeremy Hunt on the radio intent on making hospital inspections more robust. Three other experts suggested that instead, an open culture where patients and staff are listened to is more likely to improve safety and quality. In this issue, a team from Dudley describe their experience of implementing change and indicate just how complex it is to ensure everyone’s views have been taken into account and hospital processes followed. They point out that having a ‘bright idea’ is easy; the difficulty is
in carrying it out. My husband, an academic scientist says ‘ideas are cheap’ it’s carrying them out that takes the genius.
Kathleen Ferguson and Tom Woodcock have been demonstrating just such genius in preparing a suggested list of essential drugs and working with the Department of Health in planning how this will be used in practice. We hope this might see the end of notices declaring that ephedrine or diamorphine are in short supply. My only thought is that coffee and tea are not included – our theatres would certainly cease to function if these weren’t available. Seriously though, Please do send your comments on this to [email protected].
The GAT committee describe the process from the other side, giving evidence to the Shape of Training Review and hoping it is heard and acted upon. Trainees concluded that current training is good quality. Dr Roy discusses medical students’ perspectives of the specialty and what influences their career choice – perhaps we don’t place enough emphasis on the quality of anaesthesia training to those making career choices.
Last month’s AAGBI council meeting was interrupted by not one but two people leaving to do BBC interviews about the challenges of anaesthesia for older people. Prince Philip was having an operation. It was good to see the Association raising the profile of our specialty, and the ‘Beeb’ realising that it is the anaesthetists’ skills that really make the difference to outcomes! I spent the week end with my own 92 year old relative. She regaled us with wartime stories, including one about their Billy goat escaping the field and nibbling everything he could reach on the washing line. He ate the feet off all of her 3 pairs of stockings and from all accounts came within an inch of the butcher’s knife as a result.
This provides a perspective on having someone biting at one’s ankles not considered in the article on ‘Who are your competitors?’. This interesting contribution from Daniele Bryden of Great British Bake Off fame, shows the effect of competition on professionalism in anaesthesia. Her view is that the best clinical care is delivered by teams striving together to achieve common goals, recognising each other’s contributions in organisations that provide opportunities for personal growth. I’m with her – a good working environment does more for patient care than a robust hospital inspection. See what you think.
Nancy redfern
10
04
Course Dates Location Organisers19–20 September 2013 Liverpool Dr Steve Roberts29–30 November 2013 Nottingham (A) Dr Nigel Bedforth 10-11 January 2014 Newcastle (A) Dr Ian Harper
Faculty will vary depending on location
10% Discount for ESRA members – 15% Discount for RA-UK (FULL) members. Cost: £400 / £500 (A) including a CD with presentations and course notes. Pre-course material can be downloaded once registered on the course – including US physics, anatomy of the brachial / lumbar plexus, current articles of interest and MCQ’s. A pre course questionnaire will be sent 30 days before each course.
ProgrammeDay 1• Ultrasoundappearanceofthenerves•Machinecharacteristicsandset-up•Imagingandneedlingtechniques•Commonapproachestothebrachialplexus/upper/lowerlimb•Workshops–usingphantoms/models/cadavericprosections(A)
Day 2•Consent/trainingandimagestorage•Upper/lowerlimbtechniques•Abdominal/thoracictechniques•Cervicalplexus/spinal/epidural/painprocedures•Workshops–usingphantoms/models/cadavericprosections(A)
(A) – Anatomy based courses / with cadaveric prosections
These courses are organised by Regional Anaesthesia UK (RA-UK) in conjunction with SonoSite Ltd for training in ultrasound guided regional anaesthetic techniques. Previous experience in regional anaesthesia is essential – Awarded 10 Catergory 1 CPD credits from the RCoA and Counts towards the EDRA.
For further information and to register logon to www.sonositeeducation.co.uk
UltrasoUnd gUided regional anaesthesia – beyond introdUctory
FUJIFILMSonoSite,Inc,.theSonoSitelogoandothertrademarksnotownedbythirdpartiesareregisteredandunregisteredtrademarksofFUJIFILMSonoSite,Inc.invariousjurisdictions.Allothertrademarksarethepropertyoftheirrespectiveowners.
©2013FUJIFILMSonoSite,Inc.Allrightsreserved.175307/13
2013 coUrse dates:
Introductory Ultrasound Guided Regional Anaesthesia25-26 November - Course Director: Dr Morné Wolmarans
Ultrasound Guided Venous Access 10 October
Ultrasound Guided Critical Care14 November
Venue: FUJIFILM SonoSite Education Centre, 240 The Village, Butterfield, Great Marlings, Luton, Bedfordshire LU2 8DL
For the full listing of SonoSite training and education courses, dates and to register go to:
www.sonositeeducation.co.uk
SonoSite, the world leader and specialist in hand-carried ultrasound, has teamed up with some of the leading specialists in the medical industry to design a series of courses, for both novice and experienced users, focusing on point-of-care ultrasound. Introductory Ultrasound Guided Regional Anaesthesia – Awarded 10 Catergory 1 CPD credits from the RCoA and Counts towards the EDRA The two-day introductory course is designed to teach those who have little or no experience in the use of ultrasound in their normal daily practice. The course comprises of didactic lectures on the physics of ultrasound, ultrasound anatomy and regional anaesthesia techniques. The lectures and hands-on sessions will concentrate on the brachial plexus, upper and lower limb blocks.
Ultrasound Guided Venous Access – Awarded 5 Category 1 RCR CPD points This one-day course is aimed at physicians and nurses involved with line placement and comprises didactic lectures, ultrasound of the neck, hands-on training with live models, in-vitro training in ultrasound guided puncture and demonstration of ultrasound guided central venous access. The emphasis is on jugular venous access, but femoral, subclavian and arm vein access will also be discussed.
Ultrasound Guided Critical Care – Awarded 5 CME Credits from the College of Emergency Medicine and FICM, 5 CPD Points from the RCoA & FICE approved This one-day course is aimed at all critical care physicians and surgeons. The programme is suitable for those who already have some basic ultrasound experience as well as those who are new to the clinical applications of focused ultrasound at the patient bedside. The course is suitable for consultant and middle grade clinicians across the spectrum of specialities (Emergency Medicine, Acute Medicine, Surgery, Paediatrics and Intensive Care Medicine for children or adults).
Fees: £375 (two-day courses) includes VAT, lunch, refreshments and course materials. £260 (one-day courses) includes VAT, lunch, refreshments and course materials.
If you have any questions or should need further information please e-mail: [email protected]
UltrasoUnd training coUrses
1753_AN Half Page Ad July 2013 v3.indd 1 16/07/2013 12:41
03 Editorial
04 National Essential Anaesthetic Drug List; the first draft 06 Who are your competitors?
09 Implementing Change: A Logistical Challenge 10 Victorian Application 12 A new experience - giving evidence to a national review body 15 Reflection on a challenging situation - Remembering the learner’s needs 18 Delivering Acute Illness Teaching in Uganda
20 Anaesthesia as a career choice - medical undergraduate views
22 Your Letters
25 Anaesthesia Digested
27 The NIAA’s Health Services Research Centre 28 Particles
30 @AAGBI Recap

4 Anaesthesia News September 2013 • Issue 314
The National Essential Anaesthetic Drug List (NEADL) is an AAGBI initiative to work with Members to identify the drugs that currently “satisfy the priority healthcare needs” of patients in Great Britain & Ireland. The stimulus to create such a list was the increasing number of shortages we have all been experiencing, and those whose job it is to ensure an uninterrupted supply needed priority guidance from us on the drugs that must be available wherever a patient is to be anaesthetised.1 We started the process by inviting delegates to the Winter Scientific Meeting 2013 to rate a list of 48 anaesthetic drugs, and received 82 full responses. All drugs nominated by the majority (> 41) as “Could not manage safely without” are included in NEADL. Curiously, no non-depolarising neuromuscular blocker made the cut, but presuming none of us could manage safely without, atracurium and rocuronium are included as the most desired. Only 23 respondents rated nitrous oxide as essential, and we therefore propose that the only essential medical gases in NEADL are oxygen and air. Ondansetron was the only anti-emetic to make the cut, but in descending order of preference the other favourites were cyclizine, metoclopromide and prochlorperazine. We should add 0.9% Sodium Chloride for flushing cannulae, diluting certain drugs prior to administration, or infusing for maintenance or resuscitation. Respondents were not asked for a view on Dantrolene, but it is essential to have rapid access to it wherever an anaesthetic is given. Along with a defibrillator, the current Resuscitation Council drugs amiodarone, adenosine, a
beta blocker and diltiazem must also be to hand. Drugs that did not make the cut, but perhaps should be on a supplementary list of drugs an anaesthetist could reasonably insist upon for special situations included remifentanil (40), thiopentone (32), ketamine (30) and sugammadex (25).
We are now inviting your comments on this first draft and asking you to help create the second by suggesting Priority Indications and Alternatives for the essential drugs. Imagine the supply of a certain drug is very restricted; tell us what indications that drug should be reserved for in order to protect patient safety. And in those cases for which the drug is not available, what alternative drug or technique should be recommended? You may e-mail [email protected] or fill in an Essential drug card template that can be downloaded from our website www.aagbi.org/safety/neadl and will be available to delegates at Annual Congress 2013 in Dublin. The Safety Committee will then be invited to ratify our second draft as the first official NEADL, and will keep the list under regular review with your ongoing input.
Tom woodcock & Kathleen ferguson
1. Ferguson K and Woodcock T. Ensuring a sustainable supply of drugs for anaesthesia and peri-operative care. Anaesthesia 2012;67;1313-16. Article first published online: 22 OCT 2012 | DOI: 10.1111/anae.12059
The National Essential Anaesthetic Drug List; first draft, 2013.
Class of drug Agent
Medical gases Oxygen
Air
Intravenous anaesthetics Propofol
Inhalational anaesthetics Sevoflurane
Anti-muscarinics Atropine
Glycopyrrolate
Sedatives (benzodiazepine) Midazolam
Non-opioid analgesics Paracetamol
Opioid analgesics Fentanyl
Morphine
Neuromuscular blocking drugs
Rocuronium
Atracurium
Suxamethonium
Reversal of NMB Neostigmine
CNS depression antagonists
Flumazenil
Naloxone
Malignant hyperpyrexia Dantrolene
Local anaesthesia Lidocaine
Levobupivacaine
heavy Bupivacaine
Glucocorticoid Dexamethasone
Anti-emetic Ondansetron
Anti-hypotensive Phenylephrine
Metaraminol
Ephedrine
Norepinephrine
Epinephrine
other Magnesium sulphate
Resuscitation Council UK; a defibrillator plus....
Amiodarone
Adenosine
Diltiazem
Metoprolol or atenolol
Flush, dilute, intravenous infusion, resuscitation
0.9% Sodium Chloride.
National Essential Anaesthetic Drug List; the first draft
Abstracts for presentation at WSM London 2014
CALL FOR ABSTRACTS
You are invited to submit an abstract for poster presentation at WSM London 2014. The deadline for submission is midnight on Monday 16 September 2013 and further instructions and information can be found on our WSM microsite: www.wsmlondon.org
After the deadline, a preliminary review of the abstracts received will determine which ones are accepted for poster presentation.
All accepted abstracts will be published in Anaesthesia in the form of a fully referenceable online supplement (NB Editor-in-Chief reserves the right to refuse publication, e.g. where there are major concerns over ethics and/or content).
Authors of the best poster(s) will be awarded ‘Editors’ Prizes’.
If you have any queries, please contact the AAGBI Secretariat on 020 7631 8807 / 8812 or [email protected]
The nomination, accompanied by a citation of up to 1000 words, should be sent to the Honorary Secretary at
[email protected] 5pm on Monday 16th September 2013
Evelyn Baker MedalNicola HeardEducational Events Manager
Direct Line: +44 (0) 20 7631 8805
21 Portland Place, London W1B 1PY
T: +44 (0) 20 7631 1650
F: +44 (0) 20 7631 4352
w: www.aagbi.org
The Evelyn Baker award was instigated by Dr Margaret Branthwaite in 1998, dedicated to the memory of one of her former patients at the Royal Brompton Hospital. The award is made for outstanding clinical competence, recognising the ‘unsung heroes’ of clinical anaesthesia and related practice. The defining characteristics of clinical competence are deemed to be technical proficiency, consistently reliable clinical judgement and wisdom and skill in communicating with patients, their relatives and colleagues. The ability to train and enthuse trainee colleagues is seen as an integral part of communication skill, extending beyond formal teaching of academic presentation. Nominees should normally still be in clinical practice.
Dr John Cole (Sheffield) was the first winner of the Evelyn Baker medal in 1998, followed by Dr Meena Choksi (Pontypridd) in 1999, Dr Neil Schofield (Oxford) in 2000, Dr Brian Steer (Eastbourne) in 2001, Dr Mark Crosse (Southampton) in 2002, Dr Paul Monks (London) in 2003, Dr Margo Lewis (Birmingham) in 2004, Dr Douglas Turner (Leicester) in 2005, Dr Martin Coates (Plymouth) in 2006, Dr Gareth Charlton (Southampton) in 2007, Dr Neville Robinson (London) in 2008, Dr Fred Roberts (Exeter) in 2009, Dr Sudheer Medakkar (Torquay) in 2010, Dr Keith Clayton (Coventry) in 2011 and Dr John Windsor (London) in 2012.
Nominations are now invited for the award to be presented at WSM London in January 2014 and may be made by any member of the Association to any practising anaesthetist who is also a member of the Association. Examples of successful previous nominations are available on request, and should include an indication that the nominee has broad support within their department.
An award for outstanding clinical competence

6 Anaesthesia News September 2013 • Issue 314 Anaesthesia News September 2013 • Issue 314 7
Iona Heath points out that the problem starts in medical school with selection based on academic ability and scientific reasoning, and then emphasis post qualification on acquisition of competences that are able to be assessed and measured. She argues that the sum of the parts does not equal the whole . In ‘Developing the Wise Doctor’ De Cossart and Fish consider that epistemology ie what you know, is thought more important than ontology ie what sort of doctor/person are you going to be? We’re answering the wrong question by emphasising expertise in what can be measured as a significant goal and the major determinant of success in identifying future senior doctors. I would argue that there needs to be a greater consideration of what our future professional selves will be and how we may need to change throughout our lives and careers to become more effective, so that we can also correctly identify when being competitive counts.
Competition at senior levels
People in medicine may not always wish to admit that, just as for any profession, the need for influence or status as a consultant is as big a motivator. It’s a given that patient care is a priority and ‘excellent’ doctors deliver this to the highest standard, so what is going to make the difference as to how to view a successful career? Competition is never very far away in medicine, whether it is for better job plans, more interesting work, opportunities for added roles, private practice or clinical excellence awards. But we are also expected to work within directorates or teams to achieve common goals. Organisations like NCAS (National Clinical Assessment Service) would consider behaviours and attitudes that don’t tie in with good teamwork to be warning signs that the doctor may be struggling in some way. About 6% of doctors have serious performance problems, but only a very small minority are simply incompetent . Stress is a far more important factor and, for senior doctors, it is their relationships with other senior doctors, complaints and fear of litigation that are major issues. There is a contradiction at the heart of consultant practice that both requires you to compete with others if you are going to control your professional destiny and also be a significant team player to improve patient care. A team spirit is important and a culture that values group success is important. Medicine isn’t an elite sport, and the team performance goal in medicine is to produce results that patients value, not to outperform other teams.
Group vs Self
Is it realistic then to accept that success can be internally created? Malcolm Gladwell’s book on Outliers has many apocryphal stories illustrating that the benefits of advantage may be hidden and not obvious. Success is often due to cumulative advantage but “because we so profoundly personalise success, we miss opportunities to lift others onto the top rung”. That is one of the issues with career medicine. We need to be thinking of the group whilst also developing the self.
Qualitative work from Larsson and Holstrom on the ideal leaders of a profession and the qualities displayed by an aspirational anaesthetist bear that out . They classified non technical skills highly: skills such as organisation, communication, situation awareness during practical work and leadership. Values and attitudes that are patient centred, humility, respecting the complexity of anaesthesia and admitting to personal fallibility were also important. This is in complete contrast to some of the perceived desirable medical of traits of assertiveness, confidence and resilience. The biggest impact we make as a leader in the profession or of a team, is how we make other people feel about themselves and about their contribution to patient care.
How we measure our professional lives is not therefore based purely on external validation and we can and should determine our own markers of success. If the team is strong, individuals can shine and achieve more and in the process it will make us better doctors for patients. Success does breed success: what sociologists call the “accumulative advantage”. Personalising success means that you miss opportunities to lift others up with you. I challenge the belief that success in medicine is about competition and suggest that really it’s about goals.
Goals and Achievements
So how are you going to measure your future goals and achievements? Two sorts of factors are important in job satisfaction. Hygiene factors are the things that stop a person from hating a job e.g. a good salary, but they’re not the ones that cause people to really love work. Those are the motivating factors. Factors where the work is challenging, where there is recognition or responsibility for change and opportunities for personal growth. New consultants are generally happy because plenty of motivators exist at the start of their job, but dissatisfaction can set in when a job plan doesn’t change and the way to work on personal motivating factors isn’t clear. I think anaesthetists often move into other areas outside the theatre environment not just because we have the relevant skills, but because we’re seeking out some of these other factors: Feelings of accomplishment and of learning, of being a key player in a team that is achieving something meaningful. This applies equally to professional roles as to personal ones. Our own definition of success in our professional lives will be based on maximising motivators and satisfying hygiene factors, and as those are personal, there really is no need to compete against anyone else.
The best competitor
The way to be successful at what we do is to be honest and authentic at work. Medicine demands that we have good social skills, not just for patients but for the teams we work with. Emotional intelligence does not replace academic ability, but it is the difference between an inspirational consultant and one who achieves only for self.
Just as the culture of an organisation is set by the Trust Board so senior doctors will still affect a department and other individuals’ priorities. Anaesthesia is a broad church, and it is easy for people to suggest they are “doing a good job for patients” concentrating on directly programmed activity and contributing very little that does not directly benefit or interest them as individuals. While that in itself is not ‘wrong’, I would argue it is ultimately more rewarding for individuals and the NHS to aim to achieve something more, and as individuals we can set the standard. No one needs to be the focus of anything to achieve success, but what is needed is for individuals to set personal goals that they work towards and others can aspire to.
Hence, I argue that if you are going to compete in your career, the only competitor you need to have is the various options for your future practising self and what you should really consider is what that self will look like, not what any of us can do in comparison to our peers.
daniele BrydenConsultant in ICM/Anaesthesia, Sheffield Teaching Hospitals NHS Foundation Trust
Who are your competitors?Apparent Competition
We are surrounded by competition in medicine and all doctors are competitive to a degree: on average 23,000 people apply for the 7,000 UK medical school places. Moreover we appear to be training too many doctors in the UK suggesting an ever greater need to continue to compete. The Centre for Workforce in Intelligence predicts that in 2020, there will be 60% more consultants trained, requiring £6bn/year more in salaries, if they are employed as at present. The costs of trained specialists might then become enormous. As a result we may move to a situation whereby less time is spent by trained specialists doing some of the more traditional consultant roles, currently being done by my cohort at consultant pay scales. At face value this seems depressing and suggests current trainees may have little to look forward to in their future careers.
The nature of competition
The medical training system leads us to believe we are competing against each other for jobs and that competition against others is the only thing that matters, but it is flawed reasoning. Unfortunately this is most apparent in postgraduate hospital training where the emphasis is on achieving a consultant post. Moreover by emphasising the acquistion of generic skills throughout training, there is often little left to distinguish between individuals when selecting consultant. People perceive they have to compete against their fellow trainees for training places and permanent posts, but they are all in the same arena, looking for new and novel ways to score points for themselves.
In 2012 I took part in filming the Great
British Bake Off competition. The
experience precipitated considerable
reflection in me, and as a result I feel
there are relevant conclusions that I can
draw about the nature of competition
and professionalism in anaesthesia
which was the subject of my Pinkerton
lecture at the April GAT meeting.
http://videoplatform.aagbi.org/videoList

Anaesthesia News September 2013 • Issue 314 9
Implementing Change: A Logistical ChallengeCritical appraisal of literature and judicious use of the best available evidence should form the cornerstone of decision-making in evidence-based medicine, and may support the provision of a particular clinical service1. However, between finding such evidence and implementing the service change there may lie a variety of challenges. We describe the process followed during the introduction of a patient controlled epidural analgesia (PCEA) service to our labour ward.
We had decided to implement PCEA on a trial basis, to see if the potential advantages of such a service were applicable in the setting of our labour ward. One of the first tasks was the acquisition of suitable equipment. Through liaison with company representatives, we obtained correctly programmed PCEA pumps with suitable handsets and giving lines. We decided upon a dosing regime based on best available evidence. With help from the hospital pharmacy, arrangements were made for the safe supply and storage of the premixed bags of epidural drugs, which up until this time had not been used on our unit.
In line with our NHS Trust’s policy, prior to the trial of PCEA we wrote a detailed Trust guideline outlining the correct management of these patients, aimed at both medical and midwifery staff. The guideline had to be ratified by the maternity and child risk management committee, and agreement was sought from obstetricians and midwives before it was distributed to staff. New forms had to be designed and distributed for the prescription of epidural drugs, recording of maternal observations and the postnatal follow-up and audit of all PCEA patients.
Prior to the trial period, we arranged training sessions for all of the anaesthetists who would be using the new PCEA pumps. Criteria to demonstrate competence using the new system were agreed. In addition, information was disseminated via posters, email newsletters and a teaching presentation to all anaesthetists and midwives so that they had the information they required prior to caring for a parturient receiving a PCEA.
We conducted an audit of maternal satisfaction with labour analgesia and compared this to our previous practice of midwife-led epidural top-up. The positive results shown in this audit led to the permanent introduction of a PCEA service in our hospital.
Facilitating a change in practice in the hospital environment is often very difficult. Coming up with a “bright idea” based on evidence is comparatively easy, but working through the necessary administrative and logistical processes is challenging. The list of skills required is long, and may include interpersonal, organisational and financial. It is probably also helpful if at least one member of your team is both optimistic and persistent! As registrars this was our first experience of the processes involved in introducing a new service. We believe that this experience would be beneficial to any senior trainee prior to embarking upon work as a consultant.
dr Andrew downs, Specialty Registrar dr rebecca Paris, Specialty Registrardr catherine Brennan, Consultant
Dudley Group of Hospitals NHS Trust
Reference:1. Sakett D, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS.
Evidence based medicine: what it is and what it isn’t. BMJ 1996;312:71
Anaesthesia News September 2013 • Issue 314 9
DIFFICULT AIRWAY SOCIETYAscot 13th - 15th November 2013
ANNUAL SCIENTIFIC MEETING
HOPE TO SEE YOU IN ASCOT
www.das2013.co.uk
Workshop: New & Exciting additions
Introducing Ultrasound guided imaging of the Airway, Live models, International
Faculty, Paediatric Difficult Airway, Awake Fibreoptic Intubation
Case Based Discussion and more ...
Scientific Programme HighlightsUltrasound & Imaging of the Airway
Airway Stenosis & The Critical AirwayControversies in Obstetric Airway
Free Papers & Posters Encompasses all levels of the CPD matrix
• Abstracts submission now open - submission to be in by midnight on Friday 30th August 2013
• Book now online and enjoy the early-bird discounts • Discounted registration for DAS members - become a member now!!

Anaesthesia News September 2013 • Issue 314 11
Approaching the end of training the need to secure a consultant appointment becomes more urgent. To this end a CV is written and re-written and references are requested. Since I shall soon reach the end of my training programme one of the anaesthetists in my current hospital showed a previous example as a guide to future job applications. Although much has changed in anaesthesia and surgery over the last 115 years the process of making a job application has perhaps retained some similarities to earlier times, as this letter of application below shows. The application was made by a Dr Leslie Beath in late 1897 or early 1898 for the position of Anaesthetist to the Royal United Hospital in Bath.
Similarly to today’s CVs this letter includes details of the applicant’s previous education and training jobs so far. The job titles have changed repeatedly – “dresser” was presumably the fore-runner of first “surgical house officer” and then “foundation trainee”, but the structure seems familiar: junior medical and surgical jobs prior to moving into anaesthetics. These are the only details however: no explanation of what experience and skill he had gained in these posts and no mention of any audits, publications, presentations or prizes. Consequently reading through applications must have been rather quicker for the hospital Election Committee – the application runs to only four pages, of which three pages are references.
The references are greater in number that current practice, with seven separate testimonials. Aside from their number they mostly appear generally unremarkable, although the referees are a distinguished group, with three of the seven later being awarded baronetcies.1-3 The standout reference is from Mr Richard Gill, who was Chief Chloroformist to St Bartholomew’s Hospital and was apparently regarded as the best anaesthetist in London.4 This
paragraph gives the only detail of Dr Beath’s experience prior to applying for the post of anaesthetist. This comprised of a grand total of 34 cases under some level of supervision over the space of a month. This is some way behind the several thousand cases accrued during training even with the reduced working hours of modern training.
Although his experience appeared to be sparse, the existence of the application suggests that Dr Beath felt prepared to undertake the role of Anaesthetist. Unfortunately it is unknown whether he was successful in his application. We do know that he subsequently became a successful GP in the bath area, finally retiring in 1945. He left behind a doctor’s bag containing an array of drugs known (adrenaline) and unknown (strychnine, nikethamide) to modern anaesthetic practice. This application letter serves to give an indication of some of the many differences (and similarities) between modern and historical medical training.
Matt Knipe,St7 Anaesthetics, Lincoln County Hospital
James craggs,Consultant Anaesthetist, Lincoln County Hospital
Refences1. Royal College of Surgeons. Plarr’s Lives of the Fellows Online. Available at
http://livesonline.rcseng.ac.uk/biogs/E000220b.htm (accessed 04/04/13)2. Wikipedia. Lauder Brunton. Available at http://en.wikipedia.org/wiki/Lauder_
Brunton (accessed 04/04/13)3. British Medical Journal. Sir Dyce Duckworth Bt M.D. LL.D. British Medical
Journal 1928; 1: 161-24. British Medical Journal. Richard Gill M.B. B.Sc. F.R.C.S. British Medical
Journal 1933; 1: 169
8th West of England Anaesthesia Update Based in Chalet Hotel St Christoph Talks cover a wide range of topics
Flights available from Bristol, Gatwick and other airports nationwide All grades of Anaesthetist welcome Attractive prices
13th – 17th January 2014 St Christoph am Arlberg (nr St Anton), Austria
www.weauconf.com [email protected]
8th West of England Anaesthesia Update
ACTA Nottingham
14th - 15th November 2013Nottingham Conference Centre
The meeting will take place in the historical city of Nottingham, home to Robin Hood and Sherwood Forest.
We have pleasure inviting you to an exciting two-day programme with parallel Echo and Thoracic Anaethesia sessions on Thursday and the Annual meeting on Friday.
Savethe
date!
Hosted by
Organising Secretariat: Millbrook Medical Conferences LtdEmail: [email protected] Tel: 01455 552559
REGISTER ONLINEactanott ingham.co.uk
• ACTA Echo Echo and beyond
• Thoracic Seminar Improving outcomes
Thursday 14th November
• ACTA Autumn Meeting Chest trauma
Research in cardiothoracic anaesthesia
Friday 15th November
12 Anaesthesia News September 2013 • Issue 314 Anaesthesia News September 2013 • Issue 314 13
Giving evidence, when the potential outcome of the review could have far reaching consequences for trainees, seemed a daunting prospect. We wanted to be well prepared and felt it was important that the evidence we gave to the Review was representative of anaesthesia trainees, not just GAT. One of the authors (CW) therefore led a short online survey, on behalf of GAT, to gauge opinion. 359 trainees responded and 170 trainees elaborated on their answers with additional comments, which we analysed to identify recurring themes. We are grateful to all anaesthesia trainees who completed the survey.
Anaesthetic trainees’ opinion about generalist training
Opinion was equally divided between those for (50.1%) and against (49.9%) a period of generalist training between foundation and anaesthesia specialty training. 70.5% thought introducing mandatory generalist training would have no adverse impact on anaesthesia. Those in favour tended to be trainees who had completed ACCS training or other specialties pre MMC. Advantages cited included increased experience, a wider skill set, improved inter-disciplinary communication and more time to choose what to specialise in. Comments included providing a ‘less blinkered anaesthesia only approach’, and a more ‘rounded’, ‘broader’ and ‘enhanced’ experience.
Reasons for not supporting generalist training included ‘foundation training providing enough generalist training’; there have been too many changes to training recently - it is ‘currently good, so why change it’; it will delay sitting professional exams which would deter people from training in anaesthesia; by consultant level the skills and knowledge learnt prior to anaesthesia training would be forgotten. Several stated that the underlying aim of the review was more likely to relate to service provision, especially in less attractive specialties, than to training.
opinion on current anaesthesia training
Overall trainees felt that current anaesthesia training is adequate. “Our training is excellent, well-structured with good access to supervision.” “I think our training in its current format is about right as we have more directly supervised lists and this apprenticeship style is unique to anaesthesia.”
Directly supervised lists were considered a good thing and to happen more than occurred historically. Mentors were also felt to be very important.
Current training is regarded as very generalist with subspecialty interests only developing towards the end. Many trainees felt that training is too inflexible with less room for diversity than there used to be, although some felt that it was insufficiently focused, especially at specialty registrar level. It was hoped that now Intensive Care Medicine is a separate specialty, less ITU service provision would be required resulting in improved anaesthesia training.
Some trainees thought they would be less prepared for management responsibilities than clinical duties. Most (81.9%) thought it would prepare them sufficiently for the consultant role. “From observation of a number of seniors who are immediately post-CCT, I am confident that the training programme will prepare me to be a consultant.”
Regarding the duration of training, 18.1% think it is too long, 74.1% about right and 7.8% think it is too short. Some trainees thought an extra year at the end of training would be useful to develop sub-specialty interests. An optional extension was also suggested to undertake more Advanced Training Modules or to improve gaps in skill sets. Some proposed instead that three years at core trainee level, or ACCS training for all, would allow more time to develop skills and to pass the primary FRCA. The trainees who thought that training was too long cited the impact of the European Working Time Regulation and service demands as reasons; if more hours were worked or service provision reduced, training could be shortened.
The oral evidence day
Two of the authors attended the oral evidence session (SG & NR). We both hail from Newcastle and the meeting was held in London. We therefore had a useful train journey to finalise how to present the majority view that anaesthetic training is fit for purpose.
We approached our one hour slot with some trepidation, anxious to get our points across, but were immediately put at ease by the three members of the Review Expert Advisory Group; Dr Peter Nightingale, (Past President Royal College of Anaesthetists), Professor Bill Reid (Postgraduate Dean South East Scotland) and Professor Paul Stewart (Dean of Medicine, University of Birmingham).
The nerves surfaced again as we took our places either side of a large table and had microphones positioned in front of us to record the session. We explained that our evidence was based on a survey of AAGBI trainee members and started by emphasising how positive the majority of trainees were about their training and its ability to prepare them for a consultant post. We illustrated this with direct quotes from survey respondents. We described the generalist nature of our training, equipping anaesthetists to deal competently with the variety of cases that would present to any district general hospital.
It quickly became clear that based on the evidence submitted from others (the Royal College of Anaesthetists had already been interviewed) that the Review Group already had a positive view of current anaesthesia training. No training programme is perfect though, and they wanted to know what could be improved. Again we used the themes identified in the survey to represent trainees’ views (tensions between service and training; ACCS viewed more favourably by many than core training; inflexibility of curriculum; limited opportunities for developing subspecialty interests within the seven year programme; often inadequate training for management and leadership roles).
We moved on to the wider role that anaesthetists have in the hospital, covering critical care and offering support to other specialties in managing acutely unwell patients. The panel commented that this was an often under-acknowledged role provided by anaesthetic trainees. Further discussion followed on whether our role as perioperative physicians could be enhanced further.
We were shown three potential models of training. Approach A is to train more generalists, approach B is to enhance the current system training specialists with more general capabilities and approach C, credentialing. These illustrations are complex with different lines drawn to represent completion of generalist training and completion of specialist training. It was difficult to see immediately how anaesthetic training would fit into any of these models. We were given more time to consider this and have submitted a further paper of additional evidence on these three approaches5.
We summed up by highlighting the positive aspects of anaesthetic training but also emphasised that the impact on current trainees of making further changes to training, should not be underestimated. Many were caught up in MTAS and are naturally suspicious that ideas are not fully thought out before implementation.
Conducting the survey meant we represented the views of anaesthetic trainees as a whole and not just those of the GAT committee. It became apparent that the current anaesthetic training programme was viewed by the members of the Expert Group present as “not broken” and hopefully not in need of fixing. We therefore felt that we had attended the session intent on defending the status quo when perhaps we could have aimed for a more aspirational approach, describing the ideal anaesthetic training programme, instead.
further opportunities to engage with the review
Following our oral evidence GAT has been invited to attend a Shape of Training Review workshop for doctors in training in late July. Four members of the GAT committee will be attending and we will report back via @AAGBI and Trainee Updates on the AAGBI website.
We wait with great anticipation to hear the resultant proposals from the Review Group, which will be sent to the sponsors this autumn. GAT is very keen to continue to ensure that we represent the views of AAGBI trainee members so please get in touch and let us know what you think about the Shape of Training Review or any other issues affecting trainees ([email protected]).
dr sarah Gibb, GAT Vice Chairdr caroline wilson, GAT Elected Memberdr Nancy redfern, AAGBI Elected Member
References1. The Shape of Training Review website. Available from:
http://www.shapeoftraining.co.uk2. Nightingale P. The Shape of Training Review. Anaesthesia News 2013; 313:
25-26. Available from: http://www.aagbi.org/sites/default/files/August_ANews_Web.pdf.
3. Wilson C. GAT Committee’s Response to the Shape of Training Review. 2013. Available from: http://www.aagbi.org/sites/default/files/images/GAT_response%20to%20rhe%20shape%20of%20training.pdf
4. Griffiths R. AAGBI response to the Shape of Training Call for Evidence Review. 2013. Available from: http://www.aagbi.org/sites/default/files/images/AAGBI%20response%20to%20Shape%20of%20Training%20Call%20for%20Evidence%20consultation%2007%2002%2013.pdf
5. Gibb S. Comments on document: Approaches to medical education and training. 2013. Available from: http://www.aagbi.org/sites/default/files/SOTR%20oral%20evidence%20GAT%2030%205%2013%20additional%20evidence.pdf
A new experience - giving evidence to a national review body
Over the last year a UK wide review of postgraduate medical training (Shape of Training Review1) has collected evidence from those involved in education and training, medical students and trainees. Peter Nightingale’s article in August’s Anaesthesia News described the review’s aims2. Both the Group of Anaesthetists in Training (GAT) and Council of the AAGBI submitted written evidence on the themes suggested by the review3,4 and subsequently GAT were called to give oral evidence at the end of May 2013.
Anaesthesia News September 2013 • Issue 314 15
In the meantime she had changed her mind and now wanted to be awake for the delivery. The staff got on with the practicalities of providing anaesthesia and performing the surgery. I was anxious how we would cope as the patient’s obvious distress was harrowing. She was sobbing uncontrollably and felt light-headed and faint. Her friend was wonderfully supportive. She had been her midwife for the labour and delivery of her first child. They reminisced about that prolonged shared experience that eventually brought such joy. It seemed so natural that they should talk about it, yet it was such a contrast to the present situation. Their tears were punctuated by laughter; happy memories helped fill the time until the present had to be faced.
We all had been apprehensive about how the baby would look. Once the operation was over, the parents viewed their dead offspring which appeared to have Down’s syndrome. An explanation for the likely cause of death was a great comfort to them. They had been aware that there was an increased risk due to maternal age but had declined investigation.
We settled them in a side room where they could mourn the loss of their much wanted second child. Relieved that everyone had remained professional, I was grateful that I would soon be able to leave them to their grief. However, before I could escape the patient thanked me profusely for the care she had received. She reminded me how fortunate NHS staff are to possess skills that are of such immense value to others, particularly in such challenging circumstances.
I discussed the case with my trainee and was reassured that I had been right to involve her. The Consultant Obstetrician revealed how, in a similar situation, he had operated alone in order to shield his female trainee from a patient’s raw emotions. Years later this trainee told him how she had had to perform her first Caesarean section for an intrauterine death as a Consultant. She had had to cope without the benefit of seeing someone else do it, and felt that he had denied her a learning opportunity.
dr diana Jolliffe Consultant Anaesthetist, Northampton General Hospital
reflection on a challenging situation - remembering the learner’s needs
The fourth section was for an intrauterine death of a foetus at term. The patient’s first pregnancy had ended in a long labour followed by caesarean section delivery. she had taken 5 years to conceive again and this time had hoped for a normal delivery. when she learned that the baby was dead she requested a caesarean section under general anaesthesia, which i had agreed to provide when she was adequately starved. she went home for a few hours and returned with her husband and a friend who was also a community midwife.
Dear Editor,I was interested in Tom Woodcock’s article about reflection in January’s Anaesthesia News. I find the process natural and very helpful – maybe because I am an Introvert on the Myers-Briggs Type Indicator. The discipline of writing helps me to clarify my thoughts and I am delighted that this is to be accepted by the GMC as evidence of Good Medical Practice. I hope that reading others’ Reflective Pearls (a great name) may help those who “face Reflection with trepidation” to feel differently about it. Dr Diana Jolliffe Consultant Anaesthetist, Northampton General Hospital
DUBLIN
To sign up, view the scientific programme or explore sponsorship & exhibition opportunities visit:www.annualcongress.org
Book your places for the AAGBI Annual Congress at the
Convention Centre Dublin, Ireland’s new world class, purpose-
built international conference and event venue, situated only 20
minutes from the airport. Indulge yourself in the programme we
have lined up for you, network with anaesthetists and industry
representatives and take this opportunity to enjoy the history
and culture of Dublin at the same time! Annual Congress Dinner & DanceThe much anticipated AAGBI Annual Dinner and Dance will be held in the historic and impressive Guinness Storehouse, a seven storied building which brings to life the history of the famous Guinness brand.
Keynote Lectures: Perioperative risk and testing – Is it worth it or should we assume the worst? Prof Mike Irwin, Hong Kong Long term perioperative outcomesProf Dan Sessler, Cleveland, USA
Plus many more informative talks, workshops
& interactive sessions
ANews_AC2013.indd 1 30/05/2013 13:52
This article has been published with kind permission of the patient.
NATIONAL SCIENTIFIC CONGRESS OF THE AUSTRALIAN SOCIETY OF ANAESTHETISTS
Australian Society of Anaesthetists
The NSC 2013 organising committee headed by Drs Mark Skacel and Paul Burt have developed a program that will appeal to a wide audience and further explore how our understanding of the basic sciences improves clinical outcomes for our patients.
Special areas of interest will include neuroscience and consciousness, fluid therapy, and outcomes for the high risk surgical patient.
Invited Speakers includeProfessor Martin Smith Queens Square LondonProfessor Colin Mackenzie University of Maryland, BaltimoreProfessor Mike Grocott University of SouthamptonProfessor Tony QuaillNewcastle University, NSW
2013
NSC AIC ADVERT 216x282.indd 1 11/8/2012 11:00:30 AM
FACILITATING RECOVERY THROUGH ACUTE PAIN MANAGEMENT
Friday 15th November, 2013(5 RCoA CPD points applied for)
We invite you to the 2nd Humberside Acute Pain Management Symposium
Programme • Enhanced Recovery a=er Surgery
Dr Paul Knight, Calderdale Royal Infirmary • The CriFcally Ill PaFent
Dr Olivia Williams, University Hospitals of Leicester • The Morbidly Obese PaFent
Dr Abhiram Mallick, Leeds Teaching Hospitals • Intrathecal Opioids
Dr Jeremy Prout, Royal Free Hospital, London • The Opioid Dependent PaFent
Dr G Baranidharan, Leeds Teaching Hospitals • Wound InfiltraFon Techniques
Dr Venkat Hariharan, Milton Keynes Hospital • The Difficult Epidural-‐ Role of Ultrasound
Dr Vijay Kumar, Scunthorpe General Hospital
• Quality Improvement in Acute Pain Management –Brainstorming Session
Organisers: • Dr Namita Singh, Consultant AnaestheFst, Scunthorpe General Hospital • Dr AarF Tahlan, Consultant AnaestheFst, Hull Royal Infirmary
Contact: Marilyn Clay, AnaestheFcs Department, Scunthorpe General Hospital
Email: [email protected] or [email protected] Fee : Consultants £100 Trainees / SAS/ Nurses £ 50
Venue : Forest Pines Hotel & Golf Resort, Ermine Street, Broughton, North Lincolnshire DN20 0AQ
13th Obstetric Anaesthesia Symposium 5th November 2013 Lumley Castle - Chester-le-Street
Labour Epidural Analgesia Associated Maternal Fever:
A Causal or Casual Relationship L Tsen Vice Chair of Anaesthesia, Harvard Medical School USA
Maintenance of Neuraxial Labour Analgesia, what’s new and what’s different
Professor M Van de Velde, University Hospitals Gasthuisberg, Belgium
Safer Spinal and Epidural Needles Dr M Kinsella Consultant Anaesthetist St Michael’s Hospital Bristol
24 Hour Consultant Presence on Labour Ward
- gold standard or just “Fool’s gold”? Mr K Hinshaw, Consultant Obstetrician, Sunderland Royal Hospital
Serious Neurological Deficit following spinal, epidural, or CSE Dr D N Lucas, Consultant Anaesthetist, Northwick Park Hospital, London
Recent Developments in Pre-eclampsia
Dr R Russell, Consultant Anaesthetist, John Radcliffe Hospital Oxford
Professionalism: Managing the Disruptive Co-worker L.Tsen Vice Chair of Anaesthesia, Harvard Medical School USA
Obstetric Haemorrhage: A philosophical approach
Dr J Bamber Consultant Anaesthetist, Addenbrooke’s Hospital Cambridge
Complications of Cell Salvage – a recent update Dr V Clark Royal Infirmary of Edinburgh
Case Presentations
Dr P Hersey, Dr V Bythell, Dr K Roberts, Dr Pasupaleti Abstracts are invited for poster presentations for details contact J Williams
Closing date for abstracts 1st September 2013
Course Organisers: Fees: Dr U Misra, Consultant Anaesthetist & Consultants £150 J Williams Anaesthetic Secretary, Sunderland Royal Hospital Staff Grades £100 Tel No: 0191 5656256 Ext 42447 Trainees £50 Email: [email protected] Midwives £40 Awarded 5 CPD Points
VACANCYChair of the National Institute of
Academic Anaesthesia Board
This post is a 3 year fixed term appointment made by
the four founding partners of the National Institute of
Academic Anaesthesia (NIAA); the Royal College of
Anaesthetists (RCoA), the Association of Anaesthetists of
Great Britain & Ireland (AAGBI), and the journals, British
Journal of Anaesthesia and Anaesthesia. The post will be
reviewed annually by the RCoA Council.
The NIAA is a partnership body, formed of four founding
partners and ten funding partners. It works, with respect
to anaesthesia and related specialties; to improve patient
care by promoting the translation of research findings
into clinical practice; develop and maximise the academic
profile of anaesthesia within the healthcare profession,
NHS, universities and major research bodies; facilitate high
profile, influential research; facilitate and support training
and continuing professional education in academia.
The successful candidate will oversee the strategic
direction of the NIAA. He/she will work closely with
Professor Robert Sneyd, Chair of the NIAA Research
Council, Professor Mike Grocott, Director of the Health
Services Research Centre, Professor Dave Lambert, NIAA
Grant Officer, Dr Ramani Moonesinghe, NIAA Academic
Trainee Co-ordinator and the NIAA administrative team
based at the Royal College of Anaesthetists.
Those who are interested are strongly advised to discuss
the role with Professor Ravi Mahajan (ravi.mahajan@
nottingham.ac.uk or Ms Sharon Drake by email (info@
niaa.org.uk) or by telephone (07713 323535 / 020 7092
1681). Applicants should submit a one page CV and
one page letter of support to [email protected]. This
must include contact details (daytime telephone and
email address). Further information including the job
description, person specification, details on how to apply
and information on the NIAA are available on the NIAA,
RCoA and AAGBI websites. Potential applicants should
also contact Clare Bunnell (NIAA Administrator) at info@
niaa.org.uk for further supporting information about the
NIAA. The role will formally commence in January 2014,
with a handover scheduled for December 2013.
Closing date for applications: Monday, 14 October 2013. Shortlisted candidates will be contacted and interviews will be held on Monday, 4 November 2013.
INNOVATIONAAGBI
The Annual AAGBI Prize for Innovation in Anaesthesia, Critical Care and Pain
www.aagbi.org/research/innovation
The Association of Anaesthetists of Great Britain and ireland invites applications for the 2014 AAGBi Prize for innovation in Anaesthesia, critical care and Pain. This prize is open to all anaesthetists, intensivists and pain specialists based in Great Britain and ireland. The emphasis is on new ideas contributing to patient safety, high quality clinical care and improvements in the working environment. The entries will be judged by a panel of experts in respective fields.
Applicants should complete the application form that can be found on the AAGBI website www.aagbi.org/research/innovation.
The closing date for applications is Monday 30 September 2013.
Three prizes will be awarded and the winners will be invited to present their work and collect their prizes at the Winter Scientific Meeting in London on 16 January 2014.
■ Awake craniotomyDr P Farling and Mrs G Trimble, Royal Victoria Hospital
■ Interventional neuroradiologyDr P Flynn, Royal Victoria Hospital
■ Neuro critical careDr B Mullan, Royal Victoria Hospital
■ CPD and revalidationDr L Brennan, Cambridge
■ RA techniquesW Harrop-Griffiths, President, AAGBI
■ Children and consentDr L Brennan, Cambridge
■ Fluid administration in childrenDr S Lamont, Royal Belfast Hospital for Sick Children
■ This house believes that guidelines spell the death of professionalismDr A Harrop, Charing Cross Hospital and Dr W Griffiths, Hammersmith Hospital
BOOKBOOKONLINEONLINEBOOKONLINE
RCoA
EVENTS
Trainee Presentation CompetitionPlease visit the RCoA Events page for more information (www.rcoa.ac.uk/education-and-eventswww.rcoa.ac.uk/education-and-events)
CPD STUDY DAY, BELFASTDate and venue:2 October 2013The Waterfront Hall, Belfast
Registration fee:£200 (£150 for registered trainees and affiliates)
Event organiser:Dr B Darling
Follow @rcoa_events
Apply:Apply: www.rcoa.ac.uk/eventsContact: 020 7092 1673 [email protected]
an-august.indd 2 06/06/2013 10:53
18 Anaesthesia News September 2013 • Issue 314 Anaesthesia News September 2013 • Issue 314 19
Delivering Acute Illness Teaching in Uganda
Participants on each course have a wide range of abilities, knowledge and competence. Each candidate sits a pre- and post-course MCQ test, which routinely demonstrates an improvement in candidate knowledge. All the candidates enjoy the format of the course. They welcome the systematic approach to the assessment and management of the acutely ill patient and especially like the interactive nature of the teaching. Post-course feedback is routinely collected. Candidates have commented how rewarding it is to be taught in multidisciplinary groups, an approach that is novel to them. They feel it helps with communication and an understanding of each other’s roles. The Doctors commented on how ‘talking the same language’ would facilitate a more informed handover between healthcare professionals. Nurses and Midwives believe the course material will serve as a tool to empower referrals to doctors and allow them to manage the patient whilst waiting for help to arrive.
A secondary objective of these trips is the exploration of behavioural change in healthcare practitioners in a Low-Income Country. Initially we used the standard course feedback structures to assess candidate’s acceptance of the courses. Feedback forms were then modified to elicit potential barriers, as perceived by the candidates, to implementing the teaching in clinical practice. Most recently, groups have been accompanied by two health psychologists from Manchester University.
In ConclusionWe have successfully delivered validated, structured AIM© courses for those treating adult and obstetric patients in Uganda and explored resultant behavioural change. Personally and professionally we have found involvement in this project very rewarding. It has allowed each of us to further our skills educators, leaders and team members, while providing a window into in healthcare in a resource-poor setting. The enthusiasm of the Ugandan Healthcare professionals, in challenging conditions, is infectious, humbling and offers a refreshing view of healthcare when compared to the UK. We envisage continued support through the Gulu-Man link, to further knowledge, maintain competencies and assess the impact of such courses. Through commitment to this endeavour, we hope to develop a critical mass of healthcare workers who will implement and utilise the AIM© approach to acutely ill patients.
dr Matthew Jackson, ST5 in Anaesthesia & Intensive Care Medicine, North Manchester General Hospital
dr Gordon Yuill, Consultant Obstetric Anaesthetist, Stepping Hill Hospital
dr Peter Alexander, Consultant Intensivist and Anaesthetist, University Hospital South Manchester
Ms helen slattery, Practice Based Educator, University Hospital South Manchester Academy
Ms sharon whiting, Practice Based Educator, North Manchester General Hospital
Ms rose Mccarthy, Midwifery Lecturer, School of Nursing, Midwifery and Social Work, University of Salford, Salford, UK
On Behalf of Manchester Optimising Health through Training Education and Research (MOHTER) Collaboration
Conflict of Interests, Funding & AcknowledgementsGY is a co-author of the Maternal-AIM course.
MJ sits on the AIM advisory committee.
Both GY & MJ are thankful to the AAGBI IRC for individual grants supporting this work.
The Gulu-Man Link is funded by the Academy at UHSM NHS Foundation Trust and an endowment from UHSM Foundation Trust.
The Greater Manchester Critical Skills Network supply course materials and fund Practice Based Educators to teach in Gulu.
References1. Information from http://apps.who.int/ghodata/?vid=20300&theme=country#,
accessed 13/11/20122. http://www.uhsm.nhs.uk/academy/Pages/GlobalHealth.aspx3. http://www.gmcriticalcareskillsinstitute.org.uk/pages/aim_course.html4. Steen C. Costello J. Teaching pre-registration student nurses to assess acutely
ill patients: an evaluation of an acute illness management programme. Nurse Education in Practice 2008; 8(5): 343-51
5. Department of Health (2009) Competencies for recognising and responding to acutely ill patients in hospital
6. National Institute for Clinical Excellence (2007) Acutely ill patients in hospital; recognition and response to acute illness in adults in hospital
7. National Patient Safety Agency (2007) Recognising and responding appropriately to early signs of deterioration in hospitalised patients
8. Centre for Maternal and Child Enquiries (2011) Saving mother’s lives 2006-2008
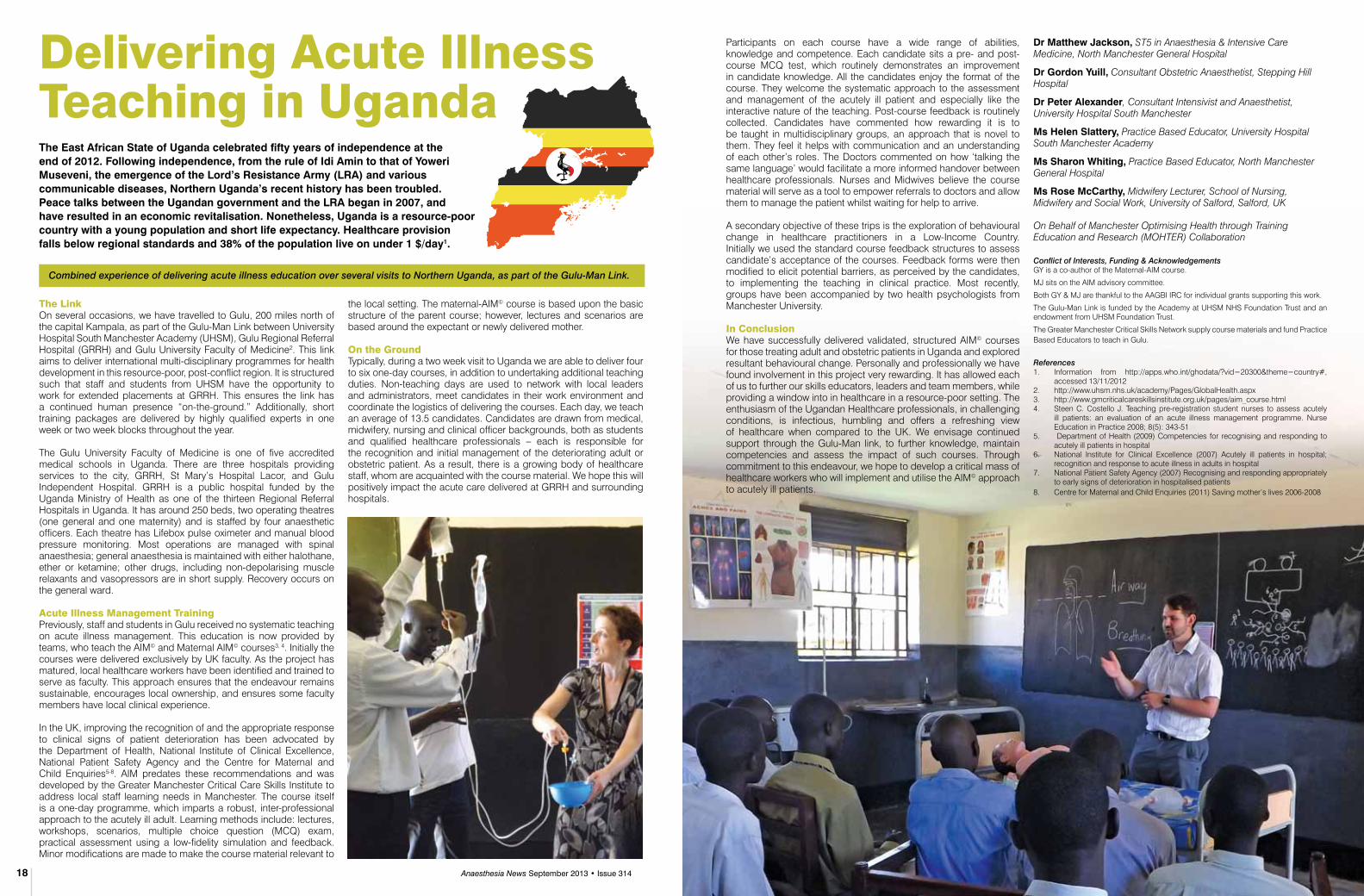
Combined experience of delivering acute illness education over several visits to Northern Uganda, as part of the Gulu-Man Link.
The east African state of Uganda celebrated fifty years of independence at the end of 2012. following independence, from the rule of idi Amin to that of Yoweri Museveni, the emergence of the lord’s resistance Army (lrA) and various communicable diseases, Northern Uganda’s recent history has been troubled. Peace talks between the Ugandan government and the lrA began in 2007, and have resulted in an economic revitalisation. Nonetheless, Uganda is a resource-poor country with a young population and short life expectancy. healthcare provision falls below regional standards and 38% of the population live on under 1 $/day1.
The LinkOn several occasions, we have travelled to Gulu, 200 miles north of the capital Kampala, as part of the Gulu-Man Link between University Hospital South Manchester Academy (UHSM), Gulu Regional Referral Hospital (GRRH) and Gulu University Faculty of Medicine2. This link aims to deliver international multi-disciplinary programmes for health development in this resource-poor, post-conflict region. It is structured such that staff and students from UHSM have the opportunity to work for extended placements at GRRH. This ensures the link has a continued human presence “on-the-ground.” Additionally, short training packages are delivered by highly qualified experts in one week or two week blocks throughout the year.
The Gulu University Faculty of Medicine is one of five accredited medical schools in Uganda. There are three hospitals providing services to the city, GRRH, St Mary’s Hospital Lacor, and Gulu Independent Hospital. GRRH is a public hospital funded by the Uganda Ministry of Health as one of the thirteen Regional Referral Hospitals in Uganda. It has around 250 beds, two operating theatres (one general and one maternity) and is staffed by four anaesthetic officers. Each theatre has Lifebox pulse oximeter and manual blood pressure monitoring. Most operations are managed with spinal anaesthesia; general anaesthesia is maintained with either halothane, ether or ketamine; other drugs, including non-depolarising muscle relaxants and vasopressors are in short supply. Recovery occurs on the general ward.
Acute Illness Management TrainingPreviously, staff and students in Gulu received no systematic teaching on acute illness management. This education is now provided by teams, who teach the AIM© and Maternal AIM© courses3, 4. Initially the courses were delivered exclusively by UK faculty. As the project has matured, local healthcare workers have been identified and trained to serve as faculty. This approach ensures that the endeavour remains sustainable, encourages local ownership, and ensures some faculty members have local clinical experience.
In the UK, improving the recognition of and the appropriate response to clinical signs of patient deterioration has been advocated by the Department of Health, National Institute of Clinical Excellence, National Patient Safety Agency and the Centre for Maternal and Child Enquiries5-8. AIM predates these recommendations and was developed by the Greater Manchester Critical Care Skills Institute to address local staff learning needs in Manchester. The course itself is a one-day programme, which imparts a robust, inter-professional approach to the acutely ill adult. Learning methods include: lectures, workshops, scenarios, multiple choice question (MCQ) exam, practical assessment using a low-fidelity simulation and feedback. Minor modifications are made to make the course material relevant to
the local setting. The maternal-AIM© course is based upon the basic structure of the parent course; however, lectures and scenarios are based around the expectant or newly delivered mother.
On the GroundTypically, during a two week visit to Uganda we are able to deliver four to six one-day courses, in addition to undertaking additional teaching duties. Non-teaching days are used to network with local leaders and administrators, meet candidates in their work environment and coordinate the logistics of delivering the courses. Each day, we teach an average of 13.5 candidates. Candidates are drawn from medical, midwifery, nursing and clinical officer backgrounds, both as students and qualified healthcare professionals – each is responsible for the recognition and initial management of the deteriorating adult or obstetric patient. As a result, there is a growing body of healthcare staff, whom are acquainted with the course material. We hope this will positively impact the acute care delivered at GRRH and surrounding hospitals.
20 Anaesthesia News September 2013 • Issue 314
Anaesthesia as a career choice - medical undergraduate views
Anaesthesia News is the official newsletter of the Association of Anaesthetists of Great Britain & ireland.
Anaesthesia News now reaches over 10,500 anaesthetists every month and is a great way of advertising your course, meeting, seminar or product.
For further information on advertising
Tel: 020 7631 8803
Dr Les GemmellImmediate Past Honorary Secretary
21 Portland Place, London W1B 1PYT: +44 (0)20 7631 1650F: +44 (0)20 7631 4352E: [email protected]
W: www.aagbi.org
or email chris steer: [email protected]/publications
An
Aes
thes
iA N
ews
Call now for a media
pack
20 Anaesthesia News September 2013 • Issue 314
Most anaesthetic departments in the West of Scotland, including our department, are facing a reduction in anaesthetic trainee numbers, expected to have a significant impact later this year. Clearly this has significant implications for training, workforce planning and healthcare delivery. An informal discussion took place in our department about the possible factors affecting the current low recruitment of trainees in Anaesthesia. Several potential reasons were hypothesised, one of which was ‘unattractiveness’ of Anaesthesia as a career choice to prospective trainees. I was scheduled to teach a group of around forty medical students later that day. It is a rarity to encounter this number of final year medical students in our discrete neuroanaesthetic department. I seized the opportunity to ask my audience about their views on choosing Anaesthesia as a career. I quickly designed a survey, the aim of which was to ascertain the factors influencing medical students in their choice of Anaesthesia (or not) as a career.
The students were given an anonymous questionnaire to fill in a few minutes before I started my tutorial. They were asked if they would choose Anaesthesia as a career or not. They were then directed to choose from a set of suggested factors affecting their decision, and were also provided with space for free text to list any additional factors which the students thought would affect their career choice. Finally, they also had a chance to indicate their opinion about the optimal duration of their undergraduate Anaesthesia posting that would assist them in deciding whether to choose the specialty.
A clear majority of the respondents said ‘No’ to Anaesthesia as a career [see Figure 1]. The less than a quarter who would choose Anaesthesia had ticked almost all suggested ‘Yes’ features which included: ‘challenging nature of work, enjoy application of scientific principles, interaction with various specialties, no clinics / ward rounds, enjoy theatre work / teamwork, excellent training, flexible working patterns, involvement with gadgets and practical procedures, etc. None of the ‘yes’ respondents would choose the specialty because anaesthetists had a ‘cool image’. However, it is noteworthy that a few of the ‘No’ respondents
thought our specialty was ‘just boring!’ and ‘stressful’ [see Table 1]. A good fraction of students thought that two weeks of exclusive exposure to anaesthesia practice would be optimal during their undergraduate training to enable to decide their career choice [see Figure 2]. In this survey I also came across a free text comment by one of the students which deserves particular mention:
“As a medical student I don’t think we have enough Anaesthesia exposure... for us, it comes under our 5 week ‘all surgery + urology block”. We raised this (issue) with the medical
school, but they replied: “Well, you will see it under surgery!”.
This survey provides a snapshot of the factors which may form the basis of decision-making of a few medical students in their final year, when they start to contemplate their future in medicine. While career choice is not based solely on the factors described in this survey, they play an important role in career decisions. Students in Glasgow have little exposure to the practice of anaesthesia during their undergraduate training. It is ironic that the largest hospital specialty gets little undergraduate attention. Nevertheless, I do not want to prematurely conclude that increasing exposure to Anaesthesia during undergraduate years alone would result in more ‘anaesthetic enthusiasts’ in the future. However, improving education and awareness of undergraduates, and even the public, about the realities and positive aspects of our specialty could broaden the appeal of Anaesthesia in future. The limitations of this survey are the small number of respondents, and that it has not examined the effect of views by gender of the respondents.
Had I known the results of my survey before my post-prandial, interactive tutorial that day, I would have edited my tutorial contents on ‘physics, physiology and pharmacology in anaesthesia’ to a lighter version, and I would have felt slightly uneasy speaking to a group of which a half do not actually share my interests.
dr Nithin roy,Consultant Neuroanaesthetist,Institute of Neurological Sciences, Glasgow
16th Anaesthesia,Critical Care and Pain Forum
Da Balaia, The AlgarvePortugal
31 September -3 October2013
www.doctorsupdates.com

22 Anaesthesia News September 2013 • Issue 314 Anaesthesia News September 2013 • Issue 314 23
yourletters
SEND YOUR LETTERS TO:
The Editor, Anaesthesia News at [email protected]
Please see instructions for authors on the AAGBI website
Dear Editor,
With the national shortage of Sodium Thiopental - we have been supplied with vials which have been less familiar. One such example is manufactured in Freiburg with all the instructions remaining in German too. In the age of safety first - I wonder whether we are right to administer a drug when many of us are unable to understand what is actually on the vial?
dr Bhavesh Gohil ST4 Anaesthetics, Homerton Hospital
Dear Editor,We would like to share our experience of the Anaesthetists Non-Technical Skills (ANTS) assessment tool. After passing the final FRCA I felt something was lacking in my performance, that knowledge and expertise were not enough to ensure safety and proficiency. I discovered the ANTS system and started using it in my own reflection.
The ANTS system was developed by a team of industrial Psychologists and Anaesthetists using the research methods derived from aviation to produce a tool specific to Anaesthesia. There are four taxonomies: Team working, Task Management, Decision Making and Situation Awareness. Each of these is associated with behavioural markers1.
I introduced this to Dr Bromley - a CT1 trainee with whom I shared on call duties. We learnt to analyse anaesthesia as a process, that success was more than the completion of a task, that team leadership, team work, contingency planning, setting triggers to call for help, discussing parameters specific to the patient and action required were also important skills. We also discussed how this was altered in different environments and how the task itself could become a distraction (“task fixation”). It provided a structure for discussion and enabled constructive feedback.
I believe the presumption that non-technical skills will develop with experience is erroneous and that an awareness of these earlier in training will enhance performance, safety and proficiency.
dr heather Gallie ST7 Dept. Anaesthesia Pinderfields General Hospital
dr Matthew Bromley CT1 Dept. Anaesthesia Pinderfields General Hospital
Reference
1. Anaesthetists Non-Technical Skills Handbook 1999-2003. Rhona Flin, Industrial Psychology University of Aberdeen www.abdn.ac.uk/ipric/ANTS
Dear Editor, schrödinger’s beds
Schrödinger’s cat is a thought experiment, sometimes described as a paradox, devised by Austrian physicist Erwin Schrödinger in 1935. It illustrates what he saw as the problem of the Copenhagen interpretation of quantum mechanics applied to everyday objects, resulting in a contradiction with common sense. The scenario presents a cat that may be both alive and dead, depending on an earlier random event.
Schrödinger’s cat, a flask of poison, and a radioactive source are placed in a sealed box. If an internal monitor detects radioactivity (i.e. a single atom decaying), the flask is shattered, releasing the poison that kills the cat. The Copenhagen interpretation of quantum mechanics implies that after a while, the cat is simultaneously alive and dead. Yet, when one looks in the box, one sees the cat either alive or dead, not both alive and dead. This poses the question of when exactly quantum superposition ends and reality collapses into one possibility or the other.
The counter-intuitive aspects of quantum mechanics have provoked philosophical debate and many interpretations. Even fundamental issues, such as Max Born’s basic rules concerning probability amplitudes and probability distributions took decades to be appreciated by society. Indeed, the renowned physicist Richard Feynman once said, “I think I can safely say that nobody understands quantum mechanics.” The inaccessibility can be understood as follows: once a measurement is done, the measured system becomes entangled with both the physicist who measured it and a huge number of other particles, including photons flying away at the speed of light towards the other end of the universe.
Could this concept be applied to NHS beds, as currently a bed can be both available and yet occupied, or a bed can exist but have no nurse in a CrCU, or a bed exist with a nurse but needs a rapid response deep clean and does the very act of inquiry of it’s state, change its status.The inaccessibility can be understood as follows: once a bed status is recorded, the measured system becomes entangled with both the manager who measured it and a huge number of other variables, some of which are choices flying away at the speed of light towards the other end of the universe.
Indeed, the little known ODP Paul Scarr once said, “I think I can safely say that nobody understands NHS management.”
dr Paul scarr
Dear Editor,There have been several descriptions of interesting and potentially hazardous foreign objects being found in anaesthetic equipment. One latest example being that of obstructing material in breathing circuits (see Letters, Anaesthesia News, November 2012).
The authors recently experienced the following similar episode in the setting of the obstetric theatre. An ASA 1 patient was undergoing spinal anaesthesia for an elective caesarean section. This had been uneventful and the newborn was delivered without any surgical difficulties. After clamping of the umbilical cord, the authors proceeded to administer 5 IU of Syntocinon.
Immediately prior to injection it was noted that the syringe contained unidentified foreign material (see Figure 1). This was retained for further inspection and a fresh syringe was used to draw up Syntocinon from another ampoule to be administered to the patient. The anaesthetic continued without incident or harm to the patient.
The original drug had been drawn up with a 1ml syringe through a 25G needle, as was the authors’ routine practice. This meant that the only plausible explanation was that it was a contaminant from the syringe manufacturing process as opposed to the ampoule itself. Further examination revealed it to be a very small piece of semi-circular coloured plastic (see Figure 2) with a similar diameter to that of the inside of the syringe.
This incident was reported both locally and nationally to the MHRA and SALG (Safe Anaesthesia Liason Group). The packaging of the syringe was kept for information regarding LOT and batch numbers, and this matter is currently under investigation. We feel this highlights the importance of vigilance when undertaking visual inspection of all anaesthetic equipment in order to prevent clinical incidents and subsequent harm to the patient.
dr Peter i.T. Paisley, MBchB, Msc ACCS (Anaesthetics) CT3, Wishaw General Hospital
dr hamish McKay, frcA
Consultant Obstetric Anaesthetist, Wishaw General Hospital
figure 1
figure 2
The Association of Anaesthetists of Great Britain & Ireland
Nottingham 27 September
Birmingham 18 October
Glasgow 01 November
Cardiff 22 November
London (2 Day) 29 & 30 November
AAG
BI 2
013 CORE
TOPICS
www.aagbi.org/educationFor further information and prices please visit:
The Preoperative Association2013 National Conference
7th November 2013York Racecourse
York
PREOP2 Poster_Layout 1 14/03/2013 09:59 Page 1
Anaesthesia News September 2013 • Issue 314 25
September 2013
Digested Routine use of dexamethasone for postoperative nausea and vomiting: the case for. Anaesthesia. doi: 10.1111/anae.12308
Kakodkar, P. S. (2013),
Routine use of dexamethasone for postoperative nausea and vomiting: the case against. Anaesthesia. doi: 10.1111/anae.12309
Bartlett, R. and Hartle, A. J. (2013),
A randomised study of intranasal dexmedetomidine and oral ketamine for premedication in children. Anaesthesia. doi: 10.1111/anae.12312
Jia, J.-E., Chen, J.-Y., Hu, X. and Li, W.-X. (2013)
Dexamethasone has been in clinical practice for ages; in fact, I cannot remember a time when I did not use it routinely in adults requiring general anaesthesia. It is an anti-emetic similar in efficacy to ondansetron, has anti-inflammatory activity and morphine-sparing effects. The Editorial Board of Anaesthesia thought it would be timely to revisit the evidence for routine use of this powerful steroid but, rather than invite a single investigator to write a systematic review or meta-analysis, felt that it would be of more interest to commission a pro/con debate on the merits, or otherwise,
of dexamethasone. I personally have always thought it a useful drug, the only obvious problem being that, if administered whilst the patient is awake, it can cause severe, albeit shortlived, perineal irritation. Is there any clear evidence that a single perioperative dose causes hyperglycaemia, neurological disturbance or leads to delayed wound healing? Drs Kakodkar, Bartlett and Hartle make entertaining arguments both for and against the routine use of dexamethasone and I leave it to you to decide its place in clinical practice.
Dexmedetomidine was introduced into U.K. clinical practice in 2011 and is still in the process of finding its niche, although it does appear to have become more popular of late [1]. It is a selective α2b−adrenergic receptor agonist and has sedative properties without causing respiratory depression; it is a more powerful hypnotic than clonidine and has been successfully used for sedation in both adults and children on Intensive care. In this article the authors have studied different doses of intranasal dexmedetomidine combined with oral ketamine as a premedicant in children before squint surgery. They found that the optimal combination was intranasal dexmedetomidine in a dose of 2 μg.kg-1 together with oral ketamine in a dose of 3 mg.kg-1 administered thirty minutes before induction of anaesthesia. This dose combination, provided administration is accurately timed, resulted in calm separation of the child from their parent and the opportunity to perform
intravenous cannulation without distressing the patient. There were no adverse effects attributable to dexmedetomidine such as bradycardia or hypotension and a low incidence of postoperative nausea and vomiting or psychiatric disturbance which may occur with higher doses of ketamine. Will this method of premedication become widespread in paediatric anaesthetic practice? The type of sedation provided by dexmedetomidine is different to that produced by midazolam due to its mode of action; “arousable sedation” has been used to describe the condition caused by dexmedetomidine whereby the child appears asleep but is rousable and cooperative to verbal command. Time will tell as to whether clinicians and nurses will become comfortable, or not, with this type of sedation and hence whether or not the use of dexmedetomidine becomes more widespread.
C.R. Bailey, Editor, Anaesthesia
25th Anaesthesia, Critical Care & Pain Update
Val d’IsereCentre de Congrés27-30 January, 2014
www.doctorsupdates.com
Reference.
1. Sleigh, J. (2012), All hands on dex. Anaesthesia, 67: 1193–1197. doi: 10.1111/j.1365-2044.2012.07334.x
N.B. the articles referred to can be found in either the latest issue or on Early View (ePub ahead of print)
Anaesthesia News September 2013 • Issue 314 27
Advanced Airways Techniques Tuesday 26th November 2013
This course has been running for many years and continues to develop. It is aimed at anaesthetists
who wish to develop advanced airways management knowledge, skills and strategy
planning to deal with a variety of clinical scenarios.
Key feature that make this course of high education value include tutor:delegate ratio of mostly 1:1;
experienced consultants as tutors; use of cadavers, animal and manikin models; and a mixture of hands-
on practice and discussion on case management.
No previous experience of advanced airways techniques is required.
Course Fee: £325
Full details and online registration available at www.dundee.ac.uk/surgicalskills
Cuschieri Skills Centre – University of Dundee
Ninewells Hospital and Medical School, Dundee, Tayside, DD1 9SY Scotland
Tel: +44(0)1382 383400 Fax: +44(0)1382 646042
Intensive Primary FRCA viva course.
6th and 7th September 2013. 29th and 30th November 2013.
Western General Hospital, Edinburgh.
Candidates will be examined in small groups and in paired vivas by tutors from our very successful in-house
course, now available to all. For more information and an
application form contact: [email protected]
Or ʻphone Keith Kelly 0131 537 1652
Fee £300 (unchanged since 2010) includes lunches, refreshments and
course dinner. Early application is recommended.
MAGILL DEPARTMENT OF ANAESTHESIA, INTENSIVE CARE & PAIN MANAGEMENT
22nd Magill Symposium ”Bariatric Medicine a preventable disease in evolution”
WEDNESDAY 20th November 2013 Gleeson Lecture Theatre,
Lower Ground Floor Time: 13:00 – 18:45 hours
Chaired by Professor Masao Takata & Dr Kevin Haire, Consultant Anaesthetist
(Imperial College London and Chelsea & Westminster Hospital, London)
Session I: Obesity under the microscope
Speakers: Professor Nicholas Finer, Dr Mike Wilson and Dr Alexandra Blakemore
Session II: Weight management – A multidisciplinary approach
Speakers: Mr Evangelous Efthimiou, Dr Kevin Haire,
Dr Suveer Singh and Professor Paul Aveyard
Magill Lecture “Bariatric anaesthesia in the UK… do we follow America?”
Professor Mark Bellamy, Critical Care & Anaesthesia St James University Hospital, Leeds
Cost: £60.00 per head. Please make cheques payable to: “Westminster Medical School Research Trust” and send to: Mr F Noormohamed, Department of Anaesthetics, Chelsea & Westminster Hospital, 369 Fulham Rd, London SW10 9NH Tel: 0203 315 8816; Fax: 0203 315 5109 email: [email protected]
ADVANCE REGISTRATION IS ESSENTIAL 4 CME credit granted by Royal College of Anaesthetists Symposium made possible with an education grant from Smiths Medical
NEW for 2013! Anaesthesia Cases
Anaesthesia Cases is an on-line, editorially-reviewed, journal of case reports in anaesthesia, pain medicine and intensive care. Users are able to submit and search case reports – a brilliant resource for trainees and consultants!
Submit a case report today www.anaesthesiacases.org
The Health Services Research Centre (HSRC) was established in March 2011 to facilitate and develop health services research relevant to anaesthesia and perioperative medicine. Two of our closest sister specialties already had well-established HSR centres: the Intensive Care National Audit & Research Centre for critical care, and the Clinical Effectiveness Unit based at the Royal College of Surgeons. HSRC’s agenda is the conduct of HSR relevant to our specialty in the perioperative setting (not just within the operating theatre).
The NiAA’s health services research centre
What is Health Services Research?
HSR covers the full range of academic endeavor involving patients rather than animals, and excludes phase I and II clinical trials or ‘bench-top’ research. It might include anything from trials of perioperative interventions, through to studies of healthcare organisation and management. The methodology used ranges from the qualitative (such as interviews and focus group discussions) through to the experimental (clinical trials) and highly quantitative (such as large scale epidemiological studies). The aim is to provide data which can lead to changes in practice and improvements in the way we look after our patients.
Structure and aims of HSRC
The HSRC is based at the Royal College of Anaesthetists and has an Executive Management Board (EMB), which is responsible for the day-to-day running, and a Scientific Advisory Board, which provides guidance on research strategy. The HSRC Director and Chair of the EMB is Professor Mike Grocott of the University of Southampton; the Scientific Advisory Board (SAB) is chaired by Professor Kathy Rowan of ICNARC. Other members of the EMB include the lead for National Audit Projects, Tim Cook, and the clinical lead for the National Emergency Laparotomy Audit, Dave Murray. There is also a clinical research fellow and a full-time academic researcher.
Within the clinical areas of anaesthesia the HSRC has three principal aims: to initiate and co-ordinate large-scale clinical audits (including NAPs); to drive methodological innovation in clinical measurement; and to conduct and facilitate research to improve patient outcome. An important part of the HSRC’s work is to assist and facilitate the efforts of the anaesthesia community in achieving these goals. Our intention is not to do all the work ourselves!
HSRC achievements
Establishing the evidence base: systematic reviews
HSRC has undertaken systematic reviews, for example about risk stratification tools used in non-cardiac surgery, and patient satisfaction questionnaires.
Oversight of National Audit Projects
The process for selecting NAP topics and for selecting project leads falls under HSRC’s remit. A key area of work is the evaluation of the impact that NAPs have had on the delivery of healthcare. For example, a survey of practice regarding airway management is currently being circulated to every anaesthetic department in order to ascertain, since NAP4 was published, local compliance with various standards of care.
Facilitating and co-ordinating anaesthesia research
The HSRC has held four highly successful Perioperative Care Research Fora. The aim is to enable actual and would-be researchers to gather and discuss projects, hopefully encouraging clinician engagement with peri-operative research. Such initiatives are aimed at ensuring that clinical research is conducted across the NHS, not just in the ‘ivory towers’.
The National Emergency Laparotomy Audit (NELA)
Perhaps the HSRC’s most significant achievement to date has been the successful bid to lead the National Emergency Laparotomy Audit, funded by the Healthcare Quality Improvement Partnership (HQIP). This is the first time that HQIP has awarded a grant to an anaesthesia-led national audit. Over 180 hospitals in England and Wales have registered to join NELA. National Clinical Audits have a good record in driving improvements in the quality and delivery of healthcare and this is a great opportunity for ‘Anaesthesia-UK’ to lead an important quality improvement initiative in a particularly vulnerable patient population.
In addition to the successful delivery of the NELA and to support NAP projects, there are a number of important initiatives on the horizon. We will be starting a programme of national ‘sprint audits’, which are short (e.g. one-week) intensive audit projects, similar in methodology to NCEPOD studies and the European Surgical Outcomes Study (EuSOS). The first sprint audit is likely to focus on the measurement of patient satisfaction with anaesthesia.
The HSRC is taking the lead on conducting a research prioritisation exercise for anaesthesia and perioperative medicine in conjunction with the James Lind Alliance.
We will be looking to appoint more research fellows. They can expect to learn research skills related to evidence synthesis (systematic review and meta-analysis) and the conduct of original research, predominantly related to epidemiology of surgical outcomes. We are keen to support trainees who want to apply for a one-year fellowship or to undertake a higher degree. Any trainee who is interested should contact us (via the HSRC website).
Finally, we want to hear more from you, particularly those who wish to collaborate on research or quality improvement projects. We wish to establish a network of Quality Audit and Research Coordinators (QuARCs) in every hospital with an anaesthetic department, so that we have local leads and points of contact for future HSRC projects. The success of the HSRC in leading and facilitating relevant patient-centered research is dependent on engagement from you and your colleagues, so please do get in touch.
ramani Moonesinghe,Consultant Anaesthetist, HSRC Board Member
Par
ticl
es
28 Anaesthesia News September 2013 • Issue 314
Post operative cognitive dysfunction and Anaesthesia
In the UK, we have a rapidly expanding elderly population with one in five (12 million) people of pensionable age1, which means most of us are, and will become geriatric anaesthetists. Post-operative cognitive dysfunction (POCD) is an important cause of morbidity and loss of independence in the elderly and could have a significant impact on health service provision2.
In a recent review by Avidan and Evers, the persistence of POCD for at least 3 months is supported3. So how as an anaesthetic body can we try to reduce the problem, as there is evidence to suggest a link between POCD and depth of anaesthesia4? It has been demonstrated that Bispectral index (BIS) guided anaesthesia reduced anaesthetic exposure and decreased the risk of POCD at 3 months after non-cardiac major surgery5. Furthermore, in a recent randomised control trial, the trial group demonstrated the potential benefits of intra-operative monitoring of anaesthetic depth and cerebral oxygenation as an intervention to reduce POCD in patients over the age of 60, in patients undergoing elective orthopaedic or abdominal surgery2.
Should we be monitoring anaesthetic depth for all our elderly patients undergoing surgery requiring a general anaesthetic? Recent NICE guidelines support the use of an EEG-based monitor (in addition to use during TIVA) in patients that are likely to experience haemodynamic instability (e.g. the elderly) or for those in whom there is concern that typical anaesthetic doses could be harmful4. Interestingly, work done for NAP5 has shown that depth of anaesthesia monitors were available in 164 centres (62%), but routinely used by only 132 (1.8%) anaesthetists6.
Should we devise an official screening protocol in the elderly as to when we should monitor anaesthetic depth, for example with BIS? We know from NCEPOD 2010 (elective and emergency surgery in the elderly) that POCD is more common in patient’s aged 75 and over, in those with a history of cognitive impairment, patients having a second procedure or a long anaesthetic/ major surgery, and in those with pre-operative confusion and frailty. With these factors we could create an ‘at risk of POCD’ assessment tool that could be performed pre-operatively. Notably, nearly one third of patients in this NCEPOD study had evidence of post-operative delirium and confusion1.
I’ll leave it up to you, the reader, to discuss further the questions posed.
samantha Black ST5, London Deanery
References1. Elective and emergency surgery in the Elderly: An Age Old Problem. The
2010 Report of the National Confidential Enquiry into Perioperative Deaths. NCEPOD. London, 2010
2. Ballard C, Jones E, Gauge N, Aarsland D, Nilsen OB, et al. (2012) Optimised Anaesthesia to Reduce Post Operative Cognitive Decline (POCD) in Older Patients Undergoing Elective Surgery, a Randomised Controlled Trial. PLoS ONE 7(6): e37410. doi:10.1371/journal.pone.0037410
3. Avidan MS, Evers AS. (2011) Review of clinical evidence for persistent cognitive decline or incident dementia attributable to surgery or general anesthesia. J Alzheimers Dis 24: 201–16.
4. National Institute for Health and Care Excellence (2012) Depth of Anaesthesia Monitors- Bispectral Index (BIS), E-Entropy and Narcotrend- Compact M [dg6] London: National Institute for Health and Care Excellence.
5. Chan MT, Cheng BC, Lee TM, Gin T; CODA Trial Group (2013) BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol, 25(1):33-42.
6. Pandit J, Cook T, Jonker W, O’Sullivan E (2013) A national survey of anaesthetists (NAP 5 Baseline) to estimate an annual incidence of accidental awareness during general anaesthesia in the UK. Br J Anaesth 110: 501–9
Snowden CP, Prentis J, Jacques B, Anderson H, Manas D, Jones D, Trenell M
cardiorespiratory fitness Predicts Mortality and hospital length of stay After Major elective surgery in older PeopleAnnals of Surgery 2013; 257(6):999-1004.
introductionIn the western world life expectancy continues to increase.1 The number of older patients requiring elective surgery will also increase substantially. Age, adjusted for comorbidities, is associated with increased risk of surgical morbidity and mortality.2 The reason for this is unclear.3 This study aims to assess the relationship between cardiopulmonary fitness and age upon mortality and length of stay in an unselected group undergoing major hepatobiliary surgery.
MethodsIn a single centre all patients considered for major hepatobiliary surgery performed a cardiopulmonary exercise test (CPET).4 Pateints undergoing a reduced surgical procedure due to extensive malignancy, laparoscopic surgery or CPET not reaching an objective measure (anaerobic threshold, AT) were excluded from the study. The surgical and anaesthetic team, were blinded to CPET results. The primary outcome measure was mortality rate; secondary outcomes were critical care and hospital length of stay as a surrogate for morbidity.
results Over 3 years, 462 patients performed preoperative CPET before major hepatobiliary surgery. 73 (16%) of patients were excluded, leaving 389 in the study group. Mean age was 65.8 and 44% were female. Overall in-hospital mortality was 18 of 389 (4.6%). Multivariate regression analysis identified the anaerobic threshold as the most significant independent predictor of postoperative mortality (OR=0.52; p=0.003). Age alone however was not predictive of outcome (OR=0.96; p=0.152). Patients with good cardiorespiratory fitness (AT>10ml/kg/min) of any age had mortality <5%. Patients with poor cardiorespiratory fitness (AT<10ml/kg/min) <75 years old had 11% mortality; >75 years old had 22% mortality.
Cox regression demonstrated cardiovascular fitness was a significant predictor of hospital and critical care stay. Patients with AT<10ml/kg/min spent longer in hospital (median= 16 vs. 12 days; p<0.001) and in the critical care unit (median= 2.6 vs. 0.9 days; p<0.001) than those with an AT>10ml/kg/min. Patients older than 75 years who had low cardiorespiratory fitness spent 11 days longer in hospital (median 23 vs. 12; P<0.0001) and 2 days longer in critical care (median 2.9 vs. 0.9; P<0.0001) than the patients with adequate cardiorespiratory fitness.
discussionThis study of patients undergoing hepatobiliary surgery showed that cardiorespiratory fitness, measured through exercise testing, is an independent predictor of mortality and length of stay and provides significantly more information than age alone. Reduced cardiorespiratory fitness is associated with increased hospital and critical care length of stay across all age groups. The authors advise that clinicians should consider both the prognostic value of cardiorespiratory testing and techniques to preserve fitness before elective surgery in older patients.
James dayST5 Oxford Deanery
References1. Oeppen J, Vaupel JW. Demography: broken limits to life expectancy.
Science. 2002;296:1029–1031.2. Bentrem DJ, Cohen ME, Hynes DM, et al. Identification of specific quality
improvement opportunities for the elderly undergoing gastrointestinal surgery. Arch Surg. 2009;144:1013–1020.
3. Kirkwood T.A systematic look at an old problem. Nature. 2008; 451:644–647.4. Hansen JE, Sue DY, Wasserman K. Predicted values for clinical exercise
testing. Am Rev Respir Dis. 1984;129:S49–S55.
Guérin C, Reignier J, Richard JC et al
Prone positioning in severe acute respiratory distress syndromeNew England Journal of Medicine 2013; 368: 2159-2168
introductionRandomised, controlled trials have shown that oxygenation of patients with severe acute respiratory distress syndrome (ARDS) can be improved by placing them in the prone position.1,2 However this physiological difference has never been seen to translate into better patient outcomes.3,4 This prospective, multicentre randomised controlled trial aimed to explore whether early application of prone positioning would improve survival among patients with ARDS.
MethodsAfter obtaining ethical approval, patients were recruited from twenty-six ICUs in France and one in Spain; all of which have used prone positioning in daily practice for more than five years. Adults who met the following criteria were included in the study: ARDS as defined according to the American-European Consensus Conference criteria;5 endotracheal intubation and mechanical ventilation for ARDS for less than 36 hours; and severe ARDS (defined as a PaO2: FiO2 ratio of <150mm Hg, with an FiO2 of ≥0.6, a PEEP of ≥5cmH2O and a tidal volume of about 6ml per kilogram of predicted body weight. (The criteria were confirmed after twelve to twenty four hours of mechanical ventilation in the participating ICUs). Four hundred and sixty six patients were randomly assigned to the supine group or the prone group. Patients in the prone group received prone positioning sessions of at least sixteen consecutive hours. Mechanical ventilation was delivered in a volume-controlled mode with constant inspiratory flow, tidal volume targeted at 6ml per kilogram of predicated body weight and the PEEP level selected from a PEEP-FiO2 table, with the aim of having an end inspiratory plateau pressure of no more than 30cmH2O and arterial plasma pH of 7.20 to 7.45. The primary end point was mortality at day 28.
results229 patients were randomised into the supine group and 237 into the prone group. Mortality at day 28 was significantly lower in the prone group than in the supine group: 16% vs. 32.8% (p<0.001). This significant difference in mortality continued at day 90. The hazard ratio for death with prone positioning was 0.39 (95% CI 0.25 - 0.63). The incidence of complications did not differ significantly between the groups, except for the incidence of cardiac arrests, which was higher in the supine group.
discussionSurvival after severe ARDS was significantly higher in the prone group than in the supine group. These findings are consistent with findings from previous meta-analyses.2 The authors suggest that prone positioning induces a decrease in lung stress and strain, which may help to prevent ventilator induced lung injury. They acknowledge that participating centres were skilled in placing patients in the prone position and the low rates of complications cannot necessarily be generalised to centres without such experience. They emphasise that the results were obtained in a sub-group of severely ill patients with ARDS.
dr Jane l GibsonST3 Anaesthetics, Northern Deanery
References1. Abroug F, Ouanes-Besbes L, Elatrous S, Brochard L. The effect of prone
positioning in acute respiratory distress syndrome or acute lung injury: a meta-analysis: areas of uncertainty and recommendations for research. Intensive Care medicine 2008;34:1002-11
2. Sud S, Friedrich JO, Taccone P et al. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: systematic review and meta-analysis. Intensive Care Medicine 2010; 36:585-99
3. Gattinoni L, Tognoni G, Pesenti A, et al. Effect of prone positioning on the survival of patients with acute respiratory failure. New England Journal of Medicine 2001;345:568-73
4. Guerin C, Gaillard S, Lemasson S et al. Effects of systematic prone positioning in hypoxemic acute respiratory failure: a randomised controlled trial. JAMA 2004;292:2379-87
5. Bernard GR, Artigas A, Brigham KL et al. The American-European Consensus Conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. AM J Respir Crit Care Med 1994; 149:818-24
30 Anaesthesia News September 2013 • Issue 314
@AAGBI recap
Latest safety updates
View the latest safety updates and Medical Device Alerts on the AAGBI website.
www.aagbi.org/safety/incidents-and-alerts
For breaking news and event information follow @AAGBI on Twitter
AAGBI Prize for Innovation in Anaesthesia, Critical Care and Pain
The deadline for applications is 30th September 2013.
Download Innovation award application form at:http://www.aagbi.org/research/innovation
INNOVATIONAAGBI
The Annual AAGBI Prize for Innovation in Anaesthesia, Critical Care and Pain
www.aagbi.org/research/innovation
Applications are invited for the 2014 round of the AAGBI Prize for Innovation in Anaesthesia, Critical Care and Pain. The prize, open to all Great Britain and Ireland based anaesthetists, intensivists and pain specialists will be presented at the AAGBI WSM London 15-17 January 2014.
New joint AAGBI & OAA guidelines on Obstetric Anaesthetics Services
This is the third version of the joint Association of Great Britain and Ireland/Obstetric Anaesthetists’ Association (AAGBI/OAA) guidelines. A major change from the last revision in 2005 is the inclusion of a section on critical care in maternity. This reflects the belated recognition of this increasingly important area of obstetrics. The number of women requiring advanced levels of care is set to increase as the trend towards an older obstetric population with increasing morbidities and levels of obesity shows no sign of abating.
As a result, obstetric anaesthetists will continue to be required to take on the role of peripartum physician (paralleling a growing enthusiasm for that of peri- operative physician in non-obstetric practice). This will inevitably mean involvement in training of staff caring for high-risk parturients and adoption of management roles to develop and maintain critical care facilities.
View the latest guideline online at:
www.aagbi.org/publications/publications-guidelines/M/R
Evelyn Baker Medal Nominations
Nominations for the 2013 Evelyn Baker Medal are open until 16th September. The award is open to all practising anaesthetists who are members of the AAGBI. The award is made for outstanding clinical competence, recognising the ‘unsung heroes’ of clinical anaesthesia and related practice.
Closing date for nominations is 5pm on Monday 16th September 2013.
Please visit the AAGBI website for further details:www.aagbi.org/about-us/awards/evelyn-baker-medal-nominations







![Consent for Anaesthesia - AAGBI consent for treatment, which can only be valid if adequate information is supplied and the patient has the ... free from coercion [2]](https://img.pdfslide.net/doc/110x75/5ad573087f8b9a075a8ce764/consent-for-anaesthesia-aagbi-consent-for-treatment-which-can-only-be-valid-if.jpg)





















