-
8/12/2019 Analysis of Sway in Parkinsons Disease
1/7
Analysis of Sway in Parkinsons Disease Using a
NewInclinometry-Based Method
Maria K. Viitasalo, MD, 1 Ville Kampman, 2 Kyosti A. Sotaniemi,
MD, 1 Seppo Leppavuori, TD, 2
Vilho V. Myllyla, MD, 1 and Juha T. Korpelainen, MD 1 *
1 Department of Neurology, University of Oulu, Oulu, Finland 2
Department of Laboratory of Microelectronics, University of Oulu,
Oulu, Finland
Abstract: In order to analyze balance control, we developed anew
inclinometry-based method to provide direct informationabout body
sway in the side-to-side and forwardbackward
directions. We tested the clinical utility of this method
foranalyzing balance in Parkinsons disease (PD), and studied
theclinical correlates of the balance measures in PD. Postural
swaywas measured during quiet stance with eyes open and eyesclosed
in 28 PD patients and in 32 age- and sex-matched con-trol subjects.
Postural sway was modeled using side-to-side andforwardbackward
directional sway movements, sway veloc-ity, and sway area. The
amount of postural sway in the PDpatients was greater than in the
control subjects, the higherlevel being most marked in patients
with severe or long-
duration PD. All the side-to-side directional sway
parameterswere abnormal in the PD patients compared with the
controlsubjects ( P < 0.05), whereas the forwardbackward
directional
parameters did not differentiate the two groups. The most
sen-sitive measures of sway were path length, velocity, and
area.The duration and severity of PD seem to be particularly
asso-ciated with the amount of side-to-side directional
posturalsway. This new inclinometric method appears to be useful
inquantifying postural sway and evaluating balance impairmentin PD.
2002 Movement Disorder Society
Key words: postural sway; balance impairment;
Parkinsonsdisease
Because of degeneration of dopaminergic nigrostriatal
projections and other motor control centers,
parkinsonianpatients suffer from postural instability, stooped
posture,and gait difficulties. Impairment of balance is an
impor-tant feature of Parkinsons disease (PD), often leading
tofalls and injuries. It has recently been shown that PDpatients
have an increased risk of death strongly relatedto the presence of
gait disturbances. 1 Because posturalinstability is associated with
advanced stages of PD withdiminished functional ability and poor
prognosis, 2 an ac-curate method for analyzing balance is
needed.
In the clinical setting, balance evaluation in PD hasmainly been
based on bedside tests such as the patientsability to recover
equilibrium when knocked off balanceby pulling suddenly backwards
on the shoulders, or fall-
ing frequency, gait difficulties, and the need for postural
support. However, these kinds of tests are inaccurate andtheir
sensitivity and reliability is limited. In the labora-tory, the
amount of postural sway reflecting balance dis-orders in PD has
previously been assessed indirectly byrecording ground reaction
forces as a subject stands on aplatform equipped with force
transducers. 37 Thismethod has been used to evaluate postural
stability undervarying sensory conditions 810 and to investigate
pos-tural reflexes. 37,10 Movements of the center of gravityhave
also been measured with a platform-mounted po-tentiometer attached
to the body. 4,5,11 Other motion mea-suring instruments, for
example infrared emitting di-
odes,12,13
have also been used for balance measurementsin PD. However, all
of these methods have severe limi-tations when quantifying balance
disorders in a clinicalsetting.
We developed an inclinometry-based method to pro-vide direct
information about body sway in the side-to-side and forwardbackward
directions. We tested theclinical utility of this method of
recognizing balance im-
*Correspondence to: Juha T. Korpelainen, Department of
Neurol-ogy, University of Oulu, PO Box 5000, 90014 Oulun yliopisto,
Finland.E-mail: [email protected]
Received 16 March 2001; Revised 17 July 2001; Accepted 25
July2001
Published online 7 January 2002 in Wiley InterScience
(www.interscience.wiley.com). DOI 10.1002/mds.10023
Movement DisordersVol. 17, No. 4, 2002, pp. 663669 2002 Movement
Disorder Society
663
-
8/12/2019 Analysis of Sway in Parkinsons Disease
2/7
pairment, assessed postural instability in PD by compar-ing the
amount of sway of PD patients with that of healthy controls, and
evaluated the clinical correlates of balance impairment in PD.
SUBJECTS AND METHODS
SubjectsThe protocol was approved by the Ethics Committee
of the local Medical Faculty, and informed consent wasobtained
from each subject. Twenty-eight patients withPD (14 men and 14
women) and 32 age- and sex-matched control subjects participated in
the study (Table1). The severity of PD was evaluated by the Hoehn
andYahr stage 14 and by the motor subscale of the UnifiedParkinson
s Disease Rating Scale (UPDRS). 15 For fur-ther analyses, the
patients were divided into subgroupsaccording to their motor scores
on the UPDRS subscale:Group 1, 25 (n 8). Subjects were further
divided intotwo subgroups according to the duration of the
disease:(1) 5 years or less (n 18); (2) more than 5 years (n10).
The mean age of the patients of the subgroups andthat of the
controls was similar. All the PD patients wereclinically examined
and their postural sway was mea-sured during the on-period at the
moment when dyski-nesia was not present.
All the PD patients were on levodopa medication.Levodopa was
used as a monotherapy in five cases andin combination with a
dopamine agonist in 10 patients,with entacapone in 19 and with
selegiline in eight.Twelve patients had a concomitant
cardiovascular dis-
ease, either arterial hypertension or coronary heart dis-ease.
Seven patients had a musculoskeletal disease, twobronchial asthma,
one noninsulin-dependent diabetesmellitus, and two had
hypothyreosis (Table 2). Three of the patients used nitrates, three
diuretics, six beta block-ers, one a calcium channel blocker, two
acetylsalicylicacid, one dipyridamole, one thyroxine, one
benzodiaze-pine, one zopiclone, one hydroxyzine, and two had
medi-cation for bronchial asthma.
The control group consisted of 32 sex- and age-matched subjects,
who were spouses or acquaintances of the patients. Twelve had
cardiovascular diseases, eitherarterial hypertension or coronary
heart disease, and onehad chronic atrial fibrillation. Six had
musculoskeletaldiseases, six had bronchial asthma, and four had
hypo-thyreosis. One used nitrates, one digoxin, two diuretics,five
beta blockers, one a calcium channel blocker, one anangiotensin
converting enzyme inhibitor, four acetylsali-cylic acid, one
dipyridamole, one warfarin, four thyrox-ine, one benzodiazepine ,
one amitriptyline, and fivemedication for bronchial asthma. None of
the controlsubjects had any difficulty in standing without
supportduring the measurements.
MethodsPostural sway measurements were performed under
standardized conditions. Every test was visually con-trolled by
the same investigator. The measurements weretaken during normal
standing both with eyes open andeyes closed and they were repeated
once. Each recordinglasted 60 seconds. The mean value of the two
consecu-
tive recordings was used in the analysis. During the test,the
subjects stood at attention, without shoes, with theirfeet together
and arms beside the body. In the eyes-opentest, subjects were asked
to look straight ahead at a mark on the facing wall.
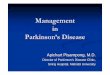
The inclinometric device consisted of a belt fastenedfirmly at
the level of the iliac crist, an inflexible mea-suring rod, an
inclinometric module, a joint structurelying on the ground, a power
unit, and a personal com-puter. The measuring rod transmitted
movements of thebody to the detecting inclinometric module located
on itsthe lower end (Fig. 1). The bottom end of the rod wasattached
to a joint structure that was designed to avoid
both the rod and the sensor module rotating around
thelongitudinal axis during the measurement. The height of the
measuring rod was adjusted according to the heightof the subject.
The deviating movement ( D) of the mea-suring rod was calculated
separately for the side-to-side( x ) and forward backward ( y)
directions using the equa-tion D
x,y=tan
x,y x h, where
x,yis the measured inclination
in the x or y direction, and h the selected calculation
TABLE 1. Clinical characteristics of Parkinsons disease patients
and control subjects
Characteristics Patients(n 28) Controls(n 32)
Gender (M/F) 14/14 16/16Mean age, yr (range) 64.9 (50 83) 63.1
(46 77)Mean duration of PD, yr (range) 7.1 (2 17) Mean Hoehn and
Yahr stage (S.D.) 2.4 (0.8) Mean UPDRS motor score (S.D.) 18.2
(10.1) Motor fluctuations or dyskinesias 14
UPDRS, Unified Parkinson s Disease Rating Scale.
TABLE 2. Concomitant diseases of Parkinsons disease patients and
control subjects
DiseasePatients
(n 28)Controls(n 32)
Cardiovascular disease 12 12Asthma 2 6
Noninsulin-dependent diabetes mellitus 1 0Hypothyreosis 2
4Musculoskeletal disease 7 6
M.K. VIITASALO ET AL.664
Movement Disorders, Vol. 17, No. 4, 2002
-
8/12/2019 Analysis of Sway in Parkinsons Disease
3/7
height (Fig. 1). By combining these two calculated de-flections
( D
x,y), the movement of the rod was presented as
an x-y coordinate.A two-axis electrolytic liquid-based
inclinometric
module including signal conditioning was used as a de-
tecting sensor. The module had two output voltages pro-portional
to the x- and y-axis inclination of the measur-ing rod. These two
voltages were converted to digitaldata using two 12-bit analog to
digital (A/D)-converters.The A/D-conversion frequency of both
channels was 20Hz. The converted data was filtered using an
8-orderlow-pass digital filter (cut frequency 3 Hz) to avoid
high-frequency noise. Digital data were calculated for the
sway parameters and displayed between every A/D-conversion to
provide a real-time display.
A constant calculation height ( h 0.8 m) was usedfor analyzing
the sway parameters of all the subjects. Byusing this constant
value h, any possible effect of thedifferent heights of the
subjects on the results was elimi-nated. Thus, all the calculated
sway parameters repre-sented the measuring rod movements on the
horizontalplane at the height of 0.8 m. The measurement
resolutionof the inclinometric module was 0.006 degrees, and
therepeatability was less than 0.02 degrees. Thus, the mea-surement
repeatability of the rod movement at the 0.8-mlevel, for example,
was less than 0.4 mm ([tan 0.03] 800 mm). The response time of the
module to inclinationchange (10 90%) was 40 ms.
The recorded sway parameters were the total pathlength of
postural sway movements (at the 0.8-m level),mean velocity, maximum
deflection ( ) for the x - and y-directional sway separately, 90%
of the x - and y-directional sway, the standard deviation (S.D.) of
the x -and y-directional sway, and the total sway area. The
pathlength was obtained by calculating the distance betweenthe
sequential location points of each sample, and afterthat, summing
the values. The mean velocity was ob-tained by calculating the
average of all the velocity val-ues between sequential samples. The
x and y werecalculated by assessing the maximum and minimum x -and
y-directional deflections and subtracting the assessedvalues for
each direction. Ninety percent x and y de-scribed the smallest
possible difference where 90% of the calculated deflection points
was located. The S.D.
was calculated for both directions to provide
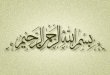
statisticalinformation about a subject s sway. Finally, the
algo-rithm of the software approximated the outlines of thesway
graph and calculated the total sway area on thegraph (Fig. 2).
The data were analyzed using SPSS for Windows soft-ware (SPSS,
Chicago, IL). The Mann-Whitney two-sample test was used to compare
the measures of thecontrol subjects with those of the PD patients.
Pearsoncorrelation coefficients were used to evaluate the
clinicalcorrelates of balance impairment in PD.
RESULTS
Table 3 shows the results of the sway measurements of both the
PD patients and the control subjects. Signifi-cantly greater
postural sway was detected in the PD pa-tients than in the control
subjects (eyes open test: veloc-ity, P 0.003; path length, P 0.004;
area, P 0.033;
x , P 0.005; 90% x -direction, P 0.012; S.D. x -direction, P
0.011; eyes closed test: velocity, P0.012; path length, P 0.013;
area, P 0.016). No
FIG. 1. A subject s waistline movement during standardized
stancewas analyzed using a belt, a measuring rod, and a two-axis
inclino-mentric sensor. The movement of the rod ( Dx,y) was
calculated usinga constant height (h 80 cm) for all the subjects
independent of theheight of the belt.
SWAY IN PARKINSON S DISEASE 665
Movement Disorders, Vol. 17, No. 4, 2002
-
8/12/2019 Analysis of Sway in Parkinsons Disease
4/7
differences in the y-directional (forward backward)sway
parameters were found between PD patients andcontrol subjects.
The increase of postural sway was related to the du-ration of
the PD, the amount of sway being most pro-
nounced in patients with long-term disease (durationmore than 5
years; Table 4). Comparing the results of thepatients with
long-term disease with those of the controlsubjects, a marked
difference was found in most of theparameters (eyes open: velocity,
P 0.004; path length,P 0.005; area, P 0.018; x , P 0.014; 90%
TABLE 3. Postural sway in Parkinson s disease patients(n = 28)
and control subjects (n = 32)
Variable PD patients Control subjects P-value
Eyes openVelocity (cm/sec) 0.50 0.15 0.40 0.11 0.003Length (cm)
29.95 9.37 24.02 6.74 0.004Area (cm 2 ) 1.60 0.91 1.23 0.95
0.033
x (cm) 2.01 0.59 1.64 0.46 0.005 y (cm) 1.85 0.61 1.77 0.77
0.218
90% x (cm) 1.29 0.39 1.07 0.31 0.01290% y (cm) 1.23 0.42 1.28
0.62 0.673S.D. x (cm) 0.41 0.12 0.34 0.11 0.011S.D. y (cm) 0.40
0.14 0.41 0.20 0.534
Eyes closedVelocity (cm/sec) 0.74 0.26 0.60 0.16 0.013Length
(cm) 44.68 15.34 35.80 9.81 0.013Area (cm 2 ) 3.17 1.62 2.38 1.47
0.016
x (cm) 2.65 0.76 2.36 0.83 0.066 y (cm) 2.47 0.68 2.31 0.68
0.346
90% x (cm) 1.71 0.53 1.53 0.55 0.16490% y (cm) 1.62 0.45 1.50
0.50 0.254S.D. x (cm) 0.56 0.20 0.48 0.17 0.132S.D. y (cm) 0.53
0.15 0.48 0.17 0.131
Values are expressed as mean S.D.*P -values for the Mann-Whitney
test comparing control subjects and
patients with each other.x indicates maximum side-to-side
deflection; y indicates forward-
backward deflection.90% x, y indicates the smallest possible
difference where 90% of the
calculated deflection points were located. S.D. x, y indicates
standarddeviation of side-to-side and forward backward directional
sway.
TABLE 4. Postural sway in patients with short-termParkinson s
disease (n = 18) and long-term (n = 10)Parkinson s disease and in
control subjects (n = 32)
Variable PD 5 yr PD > 5 yr Controlsubjects
Eyes openVelocity (cm/sec) 0.46 0.11 0.53 0.17** 0.40 0.11Length
(cm) 27.4 6.64 31.36 10.50* 24.02 6.74Area (cm 2 ) 1.29 0.59 1.78
1.02* 1.23 0.95
x (cm) 1.90 0.36* 2.07 0.69* 1.64 0.46 y (cm) 1.54 0.29 2.02
0.67 1.77 0.77
90% x (cm) 1.21 0.31 1.34 0.43* 1.07 0.3190% y (cm) 1.01 0.21
1.35 0.47 1.28 0.62S.D. x (cm) 0.38 0.09 0.42 0.14* 0.34 0.11S.D. y
(cm) 0.32 0.06 0.45 0.15 0.41 0.20
Eyes closedVelocity (cm/sec) 0.74 0.25* 0.75 0.27* 0.60
0.16Length (cm) 44.55 15.09* 44.75 15.91* 35.80 9.81Area (cm 2 )
3.05 1.56 3.23 1.69* 2.38 1.47
x (cm) 2.66 0.93 2.64 0.68 2.36 0.83 y (cm) 2.49 0.76 2.46 0.65
2.31 0.68
90% x (cm) 1.73 0.63 1.70 0.49 1.53 0.5590% y (cm) 1.55 0.43
1.66 0.47 1.50 0.50S.D. x (cm) 0.54 0.20 0.57 0.20 0.48 0.17S.D. y
(cm) 0.51 0.15 0.53 0.15 0.48 0.17
Values are expressed as mean S.D.*P < 0.05; ** P < 0.01.
P-values are for the Mann-Whitney test
comparing control subjects with short-term PD and long-term
PD.See Table 3 for abbreviations.
FIG. 2. Graph represents postural sway movements in a
77-year-old male patient ( A) and in a 67-year-old male control
subject ( B) in the x and y
coordinates.
M.K. VIITASALO ET AL.666
Movement Disorders, Vol. 17, No. 4, 2002
-
8/12/2019 Analysis of Sway in Parkinsons Disease
5/7
-
8/12/2019 Analysis of Sway in Parkinsons Disease
6/7
rapid alternating movements of hands. The correlationswere
stronger in the eyes open test than in the eyes closedtest.
DISCUSSION
We have demonstrated that postural sway is markedlygreater in PD
patients than in healthy controls, and that itcorrelates with the
duration and severity of PD and theclinical test scores for
postural stability, body bradyki-nesia, gait disorders, posture,
and lower extremity func-tions. Side-to-side directional sway seems
to be pro-nounced in PD. The presented new inclinometry-basedmethod
for measuring postural stability proved to be use-ful in detecting
differences in postural sway between PDpatients and control
subjects, the most sensitive param-eters being velocity, path
length, and total sway area.
Although the pathophysiology underlying balance im-pairment in
PD still remains obscure, several contribut-ing factors are known.
First, both selection and executionof postural reflexes seem to be
disturbed in PD. Sec-ondly, poor control of voluntary movements,
partly dueto bradykinesia, rigidity, and intrinsic muscle
stiffness,and additional factors such as adverse effects of
medi-cation, orthostatic hypotension, and gait abnormalitiesmay be
involved. 16 There are also reports 5, 17 suggestingthat gait
disorders and postural instability may resultfrom advanced
nondopaminergic cerebral pathology andtherefore these symptoms do
not respond to levodopa.Impairment of balance in PD has been shown
to be as-sociated with a poor prognosis, a more rapidly
progres-sive form of the disease, a higher mortality rate, and
an
increased prevalence of dementia.18
Here, postural swaywas most markedly increased in PD patients
with severe(UPDRS motor subscore > 25) or long-term
disease.Among PD patients with moderate disease (motor score1025),
only the most sensitive sway parameters, i.e.,velocity and path
length, were increased, while the val-ues of PD patients with mild
disease were equal to thoseof the controls. Moreover, increased
postural sway wasobserved in patients with high Hoehn and Yahr
stage,impaired leg agility, slowness in arising from chair,stooped
posture, gait disorders, impaired postural stabil-ity, or body
bradykinesia. On the other hand, the amountof tremor, rigidity, or
impaired movements of the higher
extremity were not related to postural sway.Previous results
concerning postural sway during quiet
stance have been inconsistent. Some reports 11,12,18,19
suggest that postural sway is pathognomic in PD,whereas others 7
have not found differences between PDpatients and control subjects.
Methodological heteroge-neity has been obvious. The prevailing
method has beenforce platform posturography, although many
other
methods have been introduced. 4,5,11 13 Force platformstudies
have mainly been focused on altered reflexpatterns 3 5,7,10 and
changes in center of foot pressure 9,10
elicited by various stimuli. Postural sway during freequiet
standing has been studied less frequently.
One study comparing the predictive abilities of a widerange of
balance tests and measures concluded that lat-eral instability may
be a major predictor of future fallingrisk in elderly individuals.
20 Our findings showed thatpostural sway, especially side-to-side
directional sway, isincreased in PD patients compared to that of
controlsubjects.
The commonly used force platform method analysespostural sway
indirectly on the basis of ground reactionforces. However, its
informative value is limited becauseof the assumption that a human
body acts during quietstanding like a single pendulum 21 where
motions onlyoccur around the ankle joint, and movements of the
kneeand hip joints as well as those of the upper body areignored.
Another problematic issue in the force platformmethod is how to
solve the displacements of the center of gravity from the center of
pressure. During the measure-ment, the center of pressure
oscillates around the centerof gravity position projection because
of the subject sbody segment dynamics. These facts may result in
sys-tematic errors, usually the overestimation of the center of
gravity movements compared with actual ones. 22,23 Un-like
conventional platform posturography, our inclino-metric method is
not based on such assumptions as itdirectly measures absolute
movements of the body, pro-
viding both momentary and cumulative values for swayparameters
without complex mathematical and statisticalestimations. This
inclinometric device was also designedto avoid rotational artifacts
by using a special joint struc-ture, and to detect body movements
at the level of theestimated center of gravity caused by multiple
simulta-neous motions of the lower extremity joints.
Anotheradvantage of this system is that it is lightweight
andportable, and has a simple interface with the
customizedsoftware.
In conclusion, the present inclinometric device seemsto be
useful in detecting abnormalities of postural sway
in PD. It appears to show that the amount of
side-to-sidedirectional sway is greater in PD patients than in
healthysubjects, and this sway correlates with the severity
andduration of the disease, and with the degree of bradyki-nesia,
gait disorders, and lower extremity dysfunction.However, further
studies with other patients sufferingfrom balance disorders are
needed to establish the widerclinical utility of this new
method.
M.K. VIITASALO ET AL.668
Movement Disorders, Vol. 17, No. 4, 2002
-
8/12/2019 Analysis of Sway in Parkinsons Disease
7/7
REFERENCES
1. Bennet DA, Beckett LA, Murray AM, Shannon KM, Goetz
CG,Pilgrim D, Evans DA. Prevalence of parkinsonian signs and
asso-ciated mortality in a community population of older people.
NewEngl J Med 1996;334:71 76.
2. Rogers MW. Disorders of posture, balance, and gait in
Parkinson sdisease. Clin Ger Med 1996;12:825 845.
3. Beckley DJ, Bloem BR, van Dijk JG, Roos RA, Remler
MP.Electrophysiological correlates of postural instability in
Parkin-son s disease. Electroencephalogr Clin Neurophysiol
1991;81:263 268.
4. Bloem BR, Beckley DJ, Remler MP, Roos RA, van Dijk
JG.Postural reflexes in Parkinson s disease during resist and yield
tasks. J Neurol Sci 1995;129:109 119.
5. Bloem BR, Beckley DJ, van Dijk JG, Zwinderman AH, RemlerMP,
Roos RA. Influence of dopaminergic medication on auto-nomic
postural responses and balance impairment in Parkinson sdisease.
Mov Disord 1996;11:509 521.
6. Burleigh AL, Horak FB, Burchiel KJ, Nutt JG. Effects of
thalamicstimulation on tremor, balance, and step initiation: a
single subjectstudy. Mov Disord 1993;8:519 524.
7. Schieppati M, Nardone A. Free and supported stance in
Parkin-sons disease. Brain 1991;114:1227 1244.
8. Bronstein AM, Hood JD, Gresty MA, Panagi C. Visual control
of
balance in cerebellar and parkinsonian syndromes. Brain
1990;113:767 779.
9. Trenkwalder C, Paulus W, Krafczyk S, Hawken M, Oertel
WH,Brandt T. Postural stability differentiates lower body from
idio-pathic parkinsonism. Acta Neurol Scand 1995;91:444 452.
10. Toole T, Park S, Hirsh MA, Lehman DA, Maitland CG. The
mul-ticomponent nature of equilibrium in persons with parkinsonism:
aregression approach. J Neurol Transm Gen Sect 1996;103:561
580.
11. Horak FB, Nutt JG, Nashner LM. Postural inflexibility in
parkin-sonian subjects. J Neurol Sci 1992;111:46 58.
12. Pastor MA, Day BL, Marsden CD. Vestibular induced responses
inParkonson s disease. Brain 1993;116:1177 1190.
13. Jobb gy A, Furne e EH, Harcos P, T rczy M. Early detection
of Parkinson s disease through automatic movement evaluation.IEEE
Eng Med Biol Mag 1998;17:81 88.
14. Hoehn MM, Yahr MD. Parkinsonism: onset, progression, and
mor-tality. Neurology 1967;17:427 442.
15. Fahn S, Elton RL, members of the UPDRS Development
Com-mittee. The Unified Parkinson s Disease Rating Scale. In: Fahn
S,Marsden CD, Calne DB, Goldstein M, editors. Recent develop-ments
in Parkinson s disease, vol 2. Florham Park, NJ: MacMillanHealth
Care; 1987. p 153 164.
16. Bloem BR. Postural instability in Parkinson s disease. Clin
NeurolNeurosurg 1992;94:S41 S45.
17. Bonnet AM, Loria Y, Saint-Hilaire MH, Lhermitte F, Agid
Y.Does long-term aggravation of Parkinson s disease result
fromnondopaminergic lesions? Neurology 1987;37:1539 1542.
18. Hely MA, Morris JGL, Reid WGJ, O Sullivan DJ, WilliamsonPM,
Broe GA, Adena MA. Age of onset: the major determinant of outcome
in Parkinson s disease. Acta Neurol Scand 1995;92:455 463.
19. Mitchell SL, Collins JJ, De Luca CJ, Burrows A, Lipsitz
LA.Open-loop and closed-loop postural control mechanisms in
Par-kinson s disease: increased mediolateral activity during
quietstanding. Neurosci Lett 1995;197:133 136.
20. Maki BE, Holliday PJ, Topper AK. A prospective study of
posturalbalance and risk of falling in an ambulatory and
independent el-derly population. J Gerontol 1994;49:M72 M84.
21. Accles W, Fortney V, Zatsiorsky V. Can quiet standing be
mod-elled as a single pendulum? Proceedings of the twenty-first
annualmeeting of the American Society of Biomechanics, Clemson
Uni-versity, South Carolina; 1997.
22. Barin K. Dynamic posturography. Analysis of error in force
platemeasurement of postural sway. IEEE Eng Med Biol 1992;11:52
56.
23. Barin K. Evaluation of a generalized model of human
posturaldynamics and control in the sagittal plane. Biol Cybern
1989;61:3750.
SWAY IN PARKINSON S DISEASE 669
Movement Disorders, Vol. 17, No. 4, 2002