-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
1/10
Analysis of the frequency and nature of hyaline
ring granulomas in inflammatory odontogenic
cysts
A. C. G. Henriques1, J. S. Pereira1, C. F. W. Nonaka2, R. A.
Freitas1, L. P. Pinto1 &
M. C. C. Miguel1
1Department of Dentistry, Federal University of Rio Grande do
Norte, Natal, RN, Brazil; and 2Department of Dentistry, State
University of Paraba, Campina Grande, PB, Brazil
Abstract
Henriques ACG, Pereira JS, Nonaka CFW, Freitas RA,
Pinto LP, Miguel MCC. Analysis of the frequency and nat-
ure of hyaline ring granulomas in inflammatory odontogeniccysts.
International Endodontic Journal, 46, 2029, 2013.
Aim To determine the prevalence of hyaline ring
granulomas (HRGs) in a large case series of inflam-
matory odontogenic cysts, and to investigate the nat-
ure of these structures.
Methodology All records from the patients diag-
nosed with inflammatory odontogenic cysts between
January 1970 and April 2009 were reviewed. Histo-
logic sections were evaluated by light microscopy and
cases with HRGs for which sufficient biological mate-
rial was available were submitted to histochemical
analysis (Massons trichrome) and immunohistochem-istry (CD34,
CD68 and collagen IV).
Results Twenty-two (3.3%) of the 661 cases of
inflammatory odontogenic cysts diagnosed during the
study period presented HRGs. The relative frequency
of HRGs was higher amongst residual radicular cysts
(6.1%), followed by paradental cysts (5.6%) and
radicular cysts (3.0%). HRGs appeared as roughly
circular homogeneous/fibrillar masses in 14 (63.6%)
cases and as round structures enclosing amorphous
material in 3 (13.6%) cases. Most (77.8%) roughly
circular homogeneous/fibrillar masses were positive
for collagen, whereas all (100.0%) round structures
enclosing amorphous material were negative for this
protein. Immunohistochemistry showed that most
mononucleated cells and all multinucleated giant cells
were positive for CD68, but negative for CD34, in all
cases. In addition, collagen IV immunostaining was
negative in amorphous structures and weakly positive
in homogeneous/fibrillar masses.
Conclusions The present results suggest a very
low frequency of HRGs in inflammatory odontogenic
cysts and support the hypothesis that these structures
arise from the implantation of foreign material, most
likely food particles of plant or vegetable origin. Thediverse
microscopic features of HRG possibly represent
different developmental stages of this structure.
Keywords: histochemistry, hyaline ring granu-
loma, immunohistochemistry, inflammatory odonto-
genic cysts.
Received 16 October 2011; accepted 19 May 2012
Introduction
Hyaline ring granuloma (HRG) is an uncommon histo-
pathologic finding characterized by hyaline rings or
ovoid homogeneous/fibrillar hyaline masses lying
within fibrous connective tissue, which contain vari-
able numbers of inflammatory cells and multinucleat-
ed giant cells (Talacko & Radden 1988a, Zhai &
Maluf 2004). This microscopic finding has been
reported in lesions located in the oral cavity, lung,
intestine, skin, gallbladder and uterine tube (Knoblich
1969, Zhai & Maluf 2004, Rhee & Wu 2006, Gueiros
et al. 2008). In the oral cavity, HRGs have been
found in extraosseous lesions such as inflammatory
Correspondence: Marcia Cristina da Costa Miguel, Universid-
ade Federal do Rio Grande do Norte, Departamento de
Odontologia, Av. Senador Salgado Filho, 1787, Lagoa Nova,
Natal, RN, CEP 59056-000 Brasil (Tel./Fax:
+55 84 3215 4138; e-mail: [email protected]).
2012 International Endodontic JournalInternational Endodontic
Journal, 46, 2029, 2013
doi:10.1111/j.1365-2591.2012.02086.x
20
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
2/10
fibrous hyperplasia (Gueiros et al. 2008) and in
intraosseous lesions such as periapical granulomas
(Pola et al. 2003, Gueiros et al. 2008) and odonto-
genic cysts (Chen et al. 1981, Talacko & Radden
1988a, Marcussen et al. 1993).
Oral HRG was initially described by Lewars (1971)
as chronic periostitis, which was characterized bythe presence
of palely stained eosinophilic structure-
less material, so-called hyaline rings. Since then, a
variety of terms have been used to describe this
entity, including giant-cell hyaline angiopathy
(Dunlap & Barker 1977, McMillan et al. 1981,
Ferguson & Smillie 1986), pulse granuloma (Mincer
et al. 1979, McMillan et al. 1981), granuloma tissue
with giant cells and hyaline change (McMillan et al.
1981), oral vegetable granuloma (Harrison & Martin
1986), food-induced granuloma (Brown & Theaker
1987) and le granulome alimentaire des maxillares
(Iriarte Ortabe et al. 1991). In addition, some authors
have caused confusion by mixing up the term hyaline
rings with hyaline bodies (Chen et al. 1981, Keirby &
Soames 1985, Yang & Barnett 1985). The latter
structures, also called Rushton bodies, are morpho-
logically and aetiologically different from hyaline
rings (Philipsen & Reichart 2010).
Two opposing theories regarding the aetiopatho-
genesis of HRGs have been proposed (Philipsen &
Reichart 2010). The exogenous theory suggests that
these structures arise from the implantation of foreign
material (food particles of plant or vegetable origin,
therapeutic agents) (Lewars 1971, Mincer et al.
1979, Talacko & Radden 1988a, LaMear et al. 1994).The
endogenous theory proposes that HRGs represent
hyaline degeneration of the walls of blood vessels
(Dunlap & Barker 1977). Although the origin of these
structures is not clear, the use of the descriptive term
HRG has been suggested, which seems more suitable
and also avoids misunderstanding (Chou et al. 1990,
Gueiros et al. 2008).
Data on the occurrence of HRGs in inflammatory
odontogenic cysts are basically limited to case reports
(Chen et al. 1981, Yang & Barnett 1985, Lin et al.
1993, Keskin et al. 2000, Pola et al. 2003), and only
a few retrospective studies are available (Talacko &
Radden 1988a, Marcussen et al. 1993, Philipsen &
Reichart 2010). Therefore, the objective of the present
investigation was to determine the frequency of HRGs
in a large case series of inflammatory odontogenic
cysts. In addition, histochemical and immunohisto-
chemical analyses were performed to gain insights
into the nature of these structures.
Materials and methods
Clinical analysis
After approval of the study by the Research Ethics
Committee of the Federal University of Rio Grande do
Norte (UFRN), case records from 661 patients with
inflammatory odontogenic cysts (594 radicular cysts,
49 residual radicular cysts and 18 paradental cysts)
diagnosed between January 1970 and April 2009
were retrieved from the archives of the Oral Pathol-
ogy Service at UFRN. Data regarding age, gender and
anatomic location were compiled from the clinical
data sent together with the biopsy reports.
Histopathologic analysis
For histopathologic analysis, all slides containing
haematoxylin-/eosin-stained 5-lm-thick sections were
reassessed. The tissue sections were examined under alight
microscope (Olympus CX31, Tokyo, Japan) by
three observers, and cases were classified according to
the presence or absence of HRGs. In addition, HRGs
were classified according to the following morphologic
patterns of the hyaline material: round structures
enclosing eosinophilic amorphous material (Gueiros
et al. 2008) or roughly circular homogeneous/fibrillar
masses (Philipsen & Reichart 2010). The presence of
calcification (Talacko & Radden 1988a, Philipsen &
Reichart 2010), metaplastic bone formation (Talacko
& Radden 1988a) and haemosiderin pigmentation
(Chen et al. 1981) were also analysed.
Histochemical and immunohistochemical analysis
To evaluate the nature of the material composing the
hyaline rings, 5-lm-thick sections were cut from paraf-
fin-embedded tissue blocks and stained with Massons
trichrome (EasyPath; Bio-Optica Milano SpA, Milan,
Italy). Three observers then examined the reactivity of
the hyaline material to Massons trichrome stain under
a light microscope (Olympus CX31) according to the
morphologic pattern of these structures.
Immunohistochemical staining for CD34 and CD68
was used to elucidate the nature of mononucleated
cells and multinucleated giant cells associated with
HRGs, and staining for collagen IV to gain insights into
the nature of the hyaline ring material. Briefly, 3-lm-
thick sections were cut from paraffin-embedded tissue
blocks, deparaffinized and immersed in 3% hydrogen
peroxide to block endogenous peroxidase activity. The
Henriques et al. Hyaline ring granulomas in odontogenic
cysts
2012 International Endodontic Journal International Endodontic
Journal, 46, 2029, 2013 21
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
3/10
sections were then washed in phosphate-buffered saline
(PBS) and submitted to antigen retrieval (Table 1).
After treatment with normal serum, the sections were
incubated with the primary anti-CD34, anti-CD68 and
anti-collagen IV antibodies in a moist chamber
(Table 1). The sections were then washed twice in PBS
and incubated at room temperature with the labelledstreptavidin
biotin complex (LSAB+ System-HRP; Dako,
Carpinteria, CA, USA) for anti-CD34 and anti-CD68
antibodies and with a polymer-based complex (Advan-
ceTM HRP; Dako) for anti-collagen IV antibody. Peroxi-
dase activity was visualized by immersing the tissue
sections in diaminobenzidine (Liquid DAB+ Substrate;
Dako), which resulted in a brown reaction product.
Finally, the sections were counterstained with Mayers
haematoxylin and coverslipped. Blood vessels and
macrophages present in all specimens served as inter-
nal positive controls for CD34 and CD68, respectively.
Immunostaining of blood vessels in the basement mem-
brane was used as internal positive control for collagen
IV. As negative control, the samples were treated as
described above, except that the primary antibody was
replaced with a solution of bovine serum albumin in
PBS.
The slides were analysed by three observers under
a light microscope (Olympus CX31). Positive or
negative staining for CD34 and CD68 was evaluated
in mononucleated cells and multinucleated giant cells
present inside and adjacent to HRGs. For collagen IV,
positive or negative staining was evaluated in the
hyaline material of HRGs.
The results were tabulated and analysed by descrip-tive
statistics using the Statistical Package for the Social
Sciences, version 17.0 (SPSS, Inc., Chicago, IL, USA).
Results
Clinical analysis
A total of 661 cases of inflammatory odontogenic cysts
were identified during the study period. Of these, 594
(89.9%) were radicular cysts, 49 (7.4%) were residual
radicular cysts and 18 (2.7%) were paradental cysts.
HRGs were observed in 22 (3.3%) cases. Of these, 18
(81.8%) were radicular cysts, 3 (13.6%) were residual
radicular cysts and 1 (4.5%) was a paradental cyst.
Analysis of the distribution of cases according to the
type of inflammatory odontogenic cyst revealed a
higher relative frequency of HRGs amongst residual
radicular cysts (3/49; 6.1%), followed by paradentalcysts (1/18;
5.6%) and radicular cysts (18/594; 3.0%)
(Table 2).
With respect to gender, cysts containing HRGs were
commonly diagnosed in women (63.6%), with a
female-to-male ratio of 1.75 : 1. Similarly, most cysts
without HRGs were also diagnosed in women
(59.8%), with a female-to-male ratio of 1.49 : 1
(Table 2). The mean patient age for cases with and
without HRGs was 26.76 years (range 667) and
32.41 years (range 486), respectively (Table 2).
Information regarding the anatomic location of
cysts containing HRGs was available for 20 cases. Of
these, 11 (55.0%) were located in the maxilla and 9
(45.0%) in the mandible (Table 2). Maxillary lesions
were commonly located in the anterior region
(81.8%), whereas mandibular lesions were usually
found in the posterior region (88.9%) (Table 2).
Histopathologic analysis
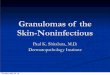
Both morphologic patterns of hyaline material could
be observed in the present series of inflammatory
odontogenic cysts: round structures enclosing eosino-
philic amorphous material consistent with degener-
ated starch cells (Fig. 1a,b) and roughly circularhomogeneous or
fibrillar masses exhibiting a
corrugated border (Fig. 1c,d). In both morphologic
patterns, the hyaline material was found lying in
chronically and, less often, acutely inflamed fibrous
connective tissue. In addition, mononucleated cells
and multinucleated giant cells were observed inside
and adjacent to the hyaline material (Fig. 1ad).
Three (13.6%) cases exhibited only round structures
enclosing amorphous material, 14 (63.6%) cases
showed only roughly circular homogeneous or
fibrillar masses and both morphologic patterns were
Table 1 Manufacturer, clone, antigen retrieval, dilution and
incubation period of the primary antibodies
Antibody Manufacturer Clone Antigen retrieval Dilution
Incubation
CD68 Dako KP1 Citrate, pH 6.0, Pascal, 121 C, 3 min 1 : 50
Overnight
CD34 Dako QBEnd10 Tris/EDTA, pH 9.0, Pascal, 121 C, 3 min 1 : 50
Overnight
Collagen IV Dako CIV22 Citrate, pH 6.0, Pascal, 121 C, 3 min 1 :
25 Overnight
Hyaline ring granulomas in odontogenic cysts Henriques et
al.
2012 International Endodontic JournalInternational Endodontic
Journal, 46, 2029, 201322
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
4/10
present in 5 (22.7%) cases (Table 3). One case (4.5%)
presented calcifications in the form of small, coalesced
basophilic droplets inside the hyaline material
(Fig. 1e, Table 3). In one case (4.5%), haemosiderin
pigmentation was found scattered within the hyaline
material and in the cytoplasm of mononucleated andmultinucleated
giant cells (Fig. 1f, Table 3). None of
the cases showed metaplastic bone formation.
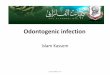
Histochemical and immunohistochemical analysis
Analysis of tissue sections stained with Massons
trichrome revealed the presence of hyaline material in
the form of roughly circular homogeneous or fibrillar
masses in nine cases and in the form of round
structures enclosing amorphous material in three
cases. Seven (77.8%) of the cases of roughly circular
homogeneous or fibrillar masses exhibited variable
amounts of collagen (Fig. 2a,b), and 2 (22.8%) were
negative for collagen (Fig. 2c). On the other hand, all
HRGs characterized by round structures enclosing
eosinophilic amorphous material were negative for
collagen (Fig. 2d).
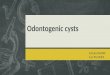
All cysts containing HRGs were submitted to immu-
nohistochemistry. However, because of the small size
of some HRGs, these structures could be identified in
only 15 of the 22 cases treated with the anti-CD68
antibody, in 12 of the 22 cases treated with the anti-
CD34 antibody and in eight of the 22 cases treated
with the anti-collagen IV antibody. Most mononucle-
ated cells and all multinucleated giant cells inside andadjacent
to HRGs were positive for CD68 in all cases
(Fig. 3a). In contrast, most mononucleated cells and
all multinucleated giant cells inside and adjacent to
HRGs were negative for CD34 (Fig. 3b). In fact, CD34
highlighted the presence of small blood vessels near
the HRGs. No significant difference in the immuno-
expression of CD68 or CD34 was observed between
the two morphologic patterns of hyaline material
(Fig. 3c,d). Furthermore, all HRGs appearing in the
form of roughly circular homogeneous or fibrillar
masses were weakly positive for collagen IV (Fig. 3e).
On the other hand, all HRGs characterized by round
structures enclosing eosinophilic amorphous material
were negative for this protein (Fig. 3f).
Discussion
HRGs have been described in both extraosseous and
intraosseous oral lesions (Lewars 1971, Dunlap &
Table 2 Number of cases, gender, age and anatomic location
according to the presence or absence of hyaline ring granulomas
in inflammatory odontogenic cysts
Group n (%)
Gender
Age (years); mean (range)
Anatomic location
Female Male
Maxilla Mandible
A P A/P A P A/P
Radicular cystsa
Absence 576 (97.0) 349 227 31.59 (486) 186 137 7 34 152 6
Presence 18 (3.0) 11 7 24.78 (660) 9 1 0 0 7 1
Total 594 (100.0) 360 234 31.38 (486) 195 138 7 34 159 7
Residual radicular cysta
Absence 46 (93.9) 20 26 44.23 (1678) 14 9 2 6 10 2
Presence 3 (6.1)b 2 1 47.50 (2867) 0 1 0 0 0 0
Total 49 (100.0) 22 27 44.37 (1678) 14 10 2 6 10 2
Paradental cysta
Absence 17 (94.4)c 13 3 28.07 (1768) 0 1 0 0 14 0
Presence 1 (5.6) 1 0 0 0 0 0 1 0
Total 18 (100.0) 14 3 27.63 (1768) 0 1 0 0 15 0
All cysts
Absence 639 (96.7) 382 256 32.41 (486) 200 147 9 40 176 8
Presence 22 (3.3) 14 8 26.76 (667) 9 2 0 0 8 1
Total 661 (100.0) 396 264 32.22 (4
86) 209 149 9 40 184 9
A, anterior; P, posterior; A/P, anterior and
posterior.aInformation regarding anatomic location was not
available for 54 radicular cysts, five residual radicular cysts and
two paradental
cysts.bInformation regarding age was not available for one
case.cInformation regarding gender was not available for one
case.
Henriques et al. Hyaline ring granulomas in odontogenic
cysts
2012 International Endodontic Journal International Endodontic
Journal, 46, 2029, 2013 23
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
5/10
Barker 1977, Chen et al. 1981, Talacko & Radden
1988a, Marcussen et al. 1993, Pola et al. 2003,
Gueiros et al. 2008). Despite these reports, the aetio-
pathogenesis of these unusual histopathologic findings
remains a matter of discussion and data regarding
their prevalence in inflammatory odontogenic cysts
are scarce. Therefore, this study determined the fre-
quency of HRGs in a large case series of inflammatory
odontogenic cysts. In addition, histochemical and
immunohistochemical analysis was performed to gain
insights into the nature of these structures.
In a retrospective study of oral HRGs, Talacko & Rad-
den (1988a) only found minimal evidence of these
structures in odontogenic cysts and periapical lesions
and suggested that HRGs in these lesions might have
been overlooked in the past. In the present study, HRGs
were usually small and inconspicuous. Nevertheless,
even after careful and thorough microscopic examina-
tion, HRGs were found in only 22 (3.3%) of the 661
cases of inflammatory odontogenic cysts studied,
suggesting a very low frequency of these microscopic
features in these lesions.
The age range of affected individuals was 667 years
in the present series and in 36 previous reports of
HRGs in inflammatory odontogenic cysts (Table 4),
with a slight predominance amongst females (54.8%).
In a review of 173 cases of oral HRGs, Philipsen &
Reichart (2010) observed that more than two-thirds
of the lesions occurred in the mandible, particularly
in the posterior region where food stagnation is
(a) (b)
(c) (d)
(e) (f)
Figure 1 (a) Hyaline ring granuloma (HRG) appearing as round
structure enclosing eosinophilic amorphous material (HE,
9400). (b) HRGs lying in fibrous connective tissue densely
infiltrated by acute and chronic inflammatory cells (HE, 9400).
(c)
HRGs in the form of roughly circular homogeneous or fibrillar
masses exhibiting a corrugated border (HE, 9400). (d) Multinu-
cleated giant cells inside and adjacent to hyaline material (HE,
9400). (e) Calcification in the form of small, coalescing
baso-philic droplets inside the hyaline material (HE, 9400). (f)
Haemosiderin pigmentation scattered within the hyaline material
and in the cytoplasm of mononucleated cells and multinucleated
giant cells (HE, 9400).
Hyaline ring granulomas in odontogenic cysts Henriques et
al.
2012 International Endodontic JournalInternational Endodontic
Journal, 46, 2029, 201324
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
6/10
common. However, when only inflammatory odonto-
genic cysts are analysed (Table 4), there is a slightly
higher percentage of HRGs in the maxilla (55.4%).
Nevertheless, in the present sample, most (88.9%) of
the inflammatory odontogenic cysts with HRGs
located in the mandible were found in the posterior
region, in agreement with Philipsen & Reichart
(2010).
Amongst the 22 inflammatory odontogenic cysts
with HRGs found in this study, 18 (81.8%) were
radicular cysts, 3 (13.6%) were residual radicular
cysts and 1 (4.5%) was a paradental cyst. As radicu-
Table 3 Microscopic features of hyaline ring granulomas
according to the type of inflammatory odontogenic cyst
Microscopic features
Cyst type
Radicular
cyst
Residual
radicular cyst
Paradental
cyst
Morphological pattern
Round structures enclosing eosinophilic amorphous material 3 0
0
Roughly circular homogeneous or fibrillar masses 11 2 1
Round structures enclosing eosinophilic amorphous material
and roughly circular homogeneous or fibrillar masses
4 1 0
Calcification
Presence 1 0 0
Absence 17 3 1
Haemosiderin pigmentation
Presence 1 0 0
Absence 17 3 1
Metaplastic bone formation
Presence 0 0 0
Absence 18 3 1
(a) (b)
(c) (d)
Figure 2 (a) Focal positivity for collagen in hyaline ring
granuloma (HRG) presenting as roughly circular homogeneous mass
(Massons trichrome, 9400). (b) Diffuse positivity for collagen
in HRGs presenting as roughly circular homogeneous masses
(Massons trichrome, 9400). (c) Negativity for collagen in HRGs
appearing as roughly circular homogeneous masses (Massons
trichrome, 9400). (d) Negativity for collagen in HRG appearing
as round structure enclosing amorphous material (Massons
trichrome, 9400).
Henriques et al. Hyaline ring granulomas in odontogenic
cysts
2012 International Endodontic Journal International Endodontic
Journal, 46, 2029, 2013 25
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
7/10
lar cysts are the most frequent type of odontogenic
cyst and residual radicular cysts and paradental cysts
are relatively uncommon (de Souza et al. 2010), the
frequency of HRGs was determined according to the
type of cyst to avoid bias. There was a higher relative
frequency of HRGs amongst residual radicular cysts
(6.1%), followed by paradental cysts (5.6%) and radic-
ular cysts (3.0%). As extraction sites and pericoronitis
around the lower third molars, associated with food
stagnation in the area, are possible pathways for the
implantation of foreign bodies, especially food parti-
cles, the present findings support the concept of an
exogenous origin of oral HRGs (Lewars 1971, Mincer
et al. 1979, Talacko & Radden 1988a, LaMear et al.
1994). Moreover, in view of the low relative
frequency of HRGs in radicular cysts, it may be sug-
gested that carious teeth or root canals left open to
the oral cavity are less efficient portals of entry for
food particles than extraction sites and pericoronitis.
Nevertheless, further studies including large series of
residual radicular cysts and paradental cysts are
needed to confirm this hypothesis.
Microscopically, oral HRGs can manifest as round
structures enclosing eosinophilic amorphous material
(Gueiros et al. 2008) or as roughly circular homo-
geneous/fibrillar masses (Philipsen & Reichart
(a) (b)
(c) (d)
(e) (f)
Figure 3 (a) Positivity for CD68 in mononucleated and
multinucleated giant cells inside and adjacent to hyaline ring
granulo-
mas (HRGs) in the form of roughly circular homogeneous masses
(LSAB method, 9400). (b) Negativity for CD34 in mono-
nucleated and multinucleated giant cells inside and adjacent to
HRGs in the form of roughly circular homogeneous masses
(LSAB method, 9400). (c) Positivity for CD68 in mononucleated
and multinucleated giant cells inside and adjacent to HRGappearing
as round structure enclosing amorphous material (LSAB method,
9400). (d) Negativity for CD34 in mononucleated
and multinucleated giant cells inside and adjacent to HRG
appearing as round structure enclosing amorphous material (LSAB
method, 9400). (e) Weak positivity for collagen IV in HRGs in
the form of roughly circular homogeneous masses (Advance
method, 9400). (f) Negativity for collagen IV in HRG in the form
of round structure enclosing amorphous material (Advance
method, 9400).
Hyaline ring granulomas in odontogenic cysts Henriques et
al.
2012 International Endodontic JournalInternational Endodontic
Journal, 46, 2029, 201326
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
8/10
2010). Both patterns may be found in the same tis-
sue section (Talacko & Radden 1988a). The present
results suggest that roughly circular homogeneous
or fibrillar masses are the most common morpho-
logic pattern of oral HRGs in inflammatory odonto-
genic cysts. According to Talacko & Radden
(1988a), the hyaline material can also present a
rod-like shape or appear in the form of long,
branching filaments. None of these features were
observed in the HRGs studied here.
Calcifications are relatively uncommon in oral
HRGs and appear in the form of small basophilicdroplets either
inside the hyaline material or inside
the almost empty circular structures (Dunlap &
Barker 1977, Chen et al. 1981, Ide et al. 1982,
Talacko & Radden 1988a). Occasionally, calcification
of the entire hyaline structure is observed (McMillan
et al. 1981, Ide et al. 1982, Talacko & Radden
1988a, Philipsen & Reichart 2010). In the present
series, calcification was seen in only one case (4.5%)
of radicular cyst, confirming the low frequency of this
microscopic feature in oral HRGs.
Haemosiderin pigmentation was found scattered
within the hyaline material and in the cytoplasm of
mononucleated and multinucleated giant cells in only
one case (4.5%) of radicular cyst. These findings are
in agreement with those reported by Chen et al.
(1981). Metaplastic bone formation is very uncom-
mon in oral HRGs, with only one case described in the
literature (Ide et al. 1982). Coherently, this feature
was not observed in the present series of HRGs.
The aetiopathogenesis of oral HRG is still unclear
(Gueiros et al. 2008). Dunlap & Barker (1977) sug-
gested that oral HRGs represent hyaline degeneration
of the walls of blood vessels precipitated by localized
acute vasculitis. According to other studies, oral HRGs
may be formed by pooling and coagulation of extra-
vasated serum proteins (Chen et al. 1981) or degener-
ated collagen (El-Labban & Kramer 1981). In contrast,
evidence from an experimental animal model (Talacko
& Radden 1988b) and the results of histopathologic
(Marcussen et al. 1993, Sato et al. 2005, Gueiros et al.
2008) and ultrastructural (Harrison & Martin 1986,Pola et
al. 2003, Sato et al. 2005, Gueiros et al. 2008)
studies support the viewpoint that exogenous foreign
material, especially from leguminous food, is responsi-
ble for the formation of oral HRGs. As the cellulose part
of plant foods is indigestible, it may persist in human
tissues in the form of hyaline material that elicits a
chronic granulomatous response (Talacko & Radden
1988a, Philipsen & Reichart 2010).
In the present study, most mononucleated cells and
all multinucleated giant cells inside and adjacent to
HRGs were positive for CD68 in all cases, regardless of
the morphologic pattern of the hyaline material. On
the other hand, these cell types were negative for CD34
in all cases, irrespective of the morphologic pattern of
the hyaline material. This negative staining for CD34
near the hyaline structure rules out a possible endo-
genous origin as a result of hyaline degeneration of the
vessel wall. Positive staining for CD68 indicates the
presence of cells of the macrophage lineage, which is
Table 4 Distribution of the cases of inflammatory odontogenic
cysts with hyaline ring granulomas reported in the literature
according to cyst type, age, gender and anatomic location
Author No. of cases Cyst type Age (years)
Gender Anatomic location
Male Female M axilla Mandible
Chen et al. (1981) 1 Residual radicular cyst 59 1 1
Yang & Barnett (1985) 1 Radicular cyst 67 1 1
Talacko & Radden (1988a) 27 Radicular cyst (13) NS NS NS 10
3
Residual radicular cyst (12) NS NS NS 5 7
Paradental cyst (2) NS NS NS 2
Lin et al. (1993) 1 Residual radicular cyst 20 1 1
Marcussen et al. (1993) 3 Residual radicular cyst 30, 34 and 57
2 1 2 1
Keskin et al. (2000) 2 Radicular cyst 18 and 38 2 1 1
Pola et al. (2003) 1 Radicular cyst 16 1 1
Current study 22 Radicular cyst (18) 660 7 11 10 8
Residual radicular cyst (3)a 28 and 67 1 2 1
Paradental cyst (1) 21 1 1
NS, not stated.aInformation regarding anatomic location was not
available for two cases. Information regarding age was not
available for one
case.
Henriques et al. Hyaline ring granulomas in odontogenic
cysts
2012 International Endodontic Journal International Endodontic
Journal, 46, 2029, 2013 27
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
9/10
compatible with a foreign body granulomatous reac-
tion. In fact, CD34 highlighted the presence of small
blood vessels near the HRGs. These small vascular
structures found near the hyaline ring, but not inside,
would participate in the granulomatous reaction
together with macrophages. Taken together, these
findings do not lend support to the endogenous theoryproposed by
Dunlap & Barker (1977), but rather rein-
force the exogenous theory, which suggests that oral
HRGs arise from the implantation of foreign material,
most likely leguminous foods (Lewars 1971, Mincer
et al. 1979, Talacko & Radden 1988a, LaMear et al.
1994, Philipsen & Reichart 2010).
The different microscopic features of oral HRGs
have been suggested to be related to distinct
evolutionary stages (Gueiros et al. 2008). In this
respect, the round structures enclosing eosinophilic
amorphous material may represent a more recent
stage in the development of oral HRGs when com-
pared with the roughly circular homogeneous/fibrillar
masses (Gueiros et al. 2008). The present histochemi-
cal findings support this suggestion because all HRGs
characterized by round structures enclosing eosino-
philic amorphous material were negative for collagen,
whereas most HRGs in the form of roughly circular
homogeneous or fibrillar masses exhibited variable
amounts of this protein. According to Harrison &
Martin (1986), hyaline rings sometimes contain both
vegetable cell wall and collagen, a fact that might
explain the variable staining of these structures with
different collagen stains (e.g. van Giesons and
Mallorys) seen in previous studies (Chen et al. 1981,Harrison
& Martin 1986, Talacko & Radden 1988a)
and in the present investigation.
Pola et al. (2003) detected no immunoreactivity to
basement membrane proteins, such as laminin or type
IV collagen, in an HRG present in the wall of a radic-
ular cyst. Coherently, all HRGs characterized by
round structures enclosing eosinophilic amorphous
material were negative for collagen IV in the present
study. However, all HRGs that appeared as roughly
circular homogeneous or fibrillar masses were weakly
positive for collagen IV, suggesting that small
amounts of this protein might be incorporated into
HRGs during their development. The fact that weak
collagen IV staining was only observed in structures
that represent a more advanced developmental stage
of oral HRG does not support the endogenous theory
proposed by Dunlap & Barker (1977).
In the case series of Gueiros et al. (2008), HRGs
appearing as round structures enclosing eosinophilic
amorphous material exhibited stronger periodic acid
Schiff and diastase-resistant staining than those
appearing in the form of roughly circular homoge-
neous/fibrillar masses. Taken together, these findings
and the present histochemical and immunohisto-
chemical results suggest that vegetable material
undergoes progressive degenerative changes, whereascollagen is
deposited during the progression of oral
HRGs. Gueiros et al. (2008) highlighted that inflam-
mation can be responsible for a distinct and persistent
evolution of HRGs, especially at an intraosseous site.
According to these authors, chronic exposure to
inflammatory enzymes probably modifies the
morphologic aspects of the hyaline rings without
compromising their antigenic potential.
Conclusion
The present results suggest a very low frequency ofHRGs in
inflammatory odontogenic cysts and support
the hypothesis that these structures arise from the
implantation of foreign material, most likely food par-
ticles of plant or vegetable origin. In addition, the
diverse microscopic features of HRG possibly represent
different developmental stages of this structure.
References
Brown AM, Theaker JM (1987) Food induced granuloma
an unusual cause of a submandibular mass with observa-
tions on the pathogenesis of hyaline bodies. British Journalof
Oral & Maxillofacial Surgery 25, 4336.
Chen SY, Fantasia JE, Miller AS (1981) Hyaline bodies in the
connective tissue wall of odontogenic cysts. Journal of Oral
Pathology 10, 14757.
Chou L, Ficarra G, Hansen LS (1990) Hyaline ring granu-
loma: a distinct oral entity. Oral Surgery Oral Medicine
Oral
Pathology 70, 31824.
Dunlap CL, Barker BF (1977) Giant-cell hyalin angiopathy.
Oral Surgery Oral Medicine Oral Pathology 44, 58791.
El-Labban NG, Kramer IR (1981) The nature of hyaline
rings in chronic periostitis and other conditions: an ultra-
structural study. Oral Surgery Oral Medicine Oral Pathology
51, 50915.
Ferguson JW, Smillie AC (1986) Giant cell hyaline angiopa-thy
presenting as a facial sinus in a patient with undiag-
nosed diabetes mellitus. New Zealand Dental Journal 82,
14951.
Gueiros LA, Santos Silva AR, Romanach MJ, Leon JE, Lopes
MA, Jorge J (2008) Distinctive aspects of oral hyaline ring
granulomas. Oral Surgery Oral Medicine Oral Pathology Oral
Radiology and Endodontics 106, e359.
Hyaline ring granulomas in odontogenic cysts Henriques et
al.
2012 International Endodontic JournalInternational Endodontic
Journal, 46, 2029, 201328
-
7/29/2019 Analysis of the Frequency and Nature of Hyaline Ring
Granulomas in Inflammatory Odontogenic Cysts
10/10
Harrison JD, Martin IC (1986) Oral vegetable granuloma:
ultrastructural and histological study. Journal of Oral
Pathology 15, 3226.
Ide F, Kusama K, Saito I, Umemura S (1982) Pulse granu-
loma in the wall of a dentigerous cyst. Journal of Oral and
Maxillofacial Surgery 40, 65962.
Iriarte Ortabe JI, Laka A, Marbaix E, Reychler H (1991)
Food granuloma of the jaws. Presentation of a new case
and review of the literature. Actualites Odonto-Stomatologi-
ques 45, 2531.
Keirby FA, Soames JV (1985) Periostitis and osteitis associ-
ated with hyaline bodies. British Journal of Oral &
Maxillo-
facial Surgery 23, 34650.
Keskin A, Duran S, Alkan A, Gunhan O (2000) Hyaline ring
granuloma in inflammatory odontogenic cysts: report of two
cases. Journal of Oral and Maxillofacial Surgery 58, 1158.
Knoblich R (1969) Pulmonary granulomatosis caused by
vegetable particles. So-called lentil pulse pneumonia.
American Review of Respiratory Disease 99, 3809.
LaMear WR, Estrem SA, Spollen LE (1994) Pulse granuloma
presenting as a facial mass. Otolaryngology Head and NeckSurgery
111, 5223.
Lewars PH (1971) Chronic periostitis in the mandible under-
neath artificial dentures. British Journal of Oral Surgery
8,
2649.
Lin SK, Chiang CP, Ou SH, Wang JT, Liu BY, Lan WH
(1993) Hyaline ring granuloma: a case report with histo-
chemical and polarized microscopic studies. Journal of the
Formosan Medical Association 92, 10013.
Marcussen LN, Peters E, Carmel D, Mickleborough M, Robin-
son C (1993) Legume associated residual cyst. Journal of
Oral Pathology & Medicine 22, 1414.
McMillan MD, Kardos TB, Edwards JL, Thorburn DN, Adams
DB, Palmer DK (1981) Giant cell hyaline angiopathy or
pulse granuloma. Oral Surgery Oral Medicine Oral Pathology52,
17886.
Mincer HH, McCoy JM, Turner JE (1979) Pulse granuloma
of the alveolar ridge. Oral Surgery Oral Medicine Oral
Pathology 48, 12630.
Philipsen HP, Reichart PA (2010) Pulse or hyaline ring
granuloma. Review of the literature on etiopathogenesis of
oral and extraoral lesions. Clinical Oral Investigations 14,
1218.
Pola JG, de la Cruz A, Bustillo F, Gallas M, Leston JS
(2003) Pulse granuloma in the wall of an inflammatory
radicular cyst. Otolaryngology Head and Neck Surgery 129,
4412.
Rhee DD, Wu ML (2006) Pulse granulomas detected in gall-
bladder, fallopian tube, and skin. Archives of Pathology
&
Laboratory Medicine 130, 183942.
Sato H, Miyate H, Fukuta Y, Satoh M (2005) Hyaline ring
granuloma of the mandibular periosteum. Oral Science
International 2, 1720.
de Souza LB, Gordon-Nunez MA, Nonaka CF, de Medeiros
MC, Torres TF, Emiliano GB (2010) Odontogenic cysts:
demographic profile in a Brazilian population over a 38-
year period. Medicina Oral Patologa Oral y Cirugia Bucal15,
e58390.
Talacko AA, Radden BG (1988a) Oral pulse granuloma: clin-
ical and histopathological features. A review of 62 cases.
International Journal of Oral & Maxillofacial Surgery
17,
3436.
Talacko AA, Radden BG (1988b) The pathogenesis of oral
pulse granuloma: an animal model. Journal of Oral Pathol-
ogy 17, 99105.
Yang ZP, Barnett F (1985) Hyaline bodies and giant cells
associated with a radicular cyst. Endodontics & Dental
Trau-
matology 1, 857.
Zhai J, Maluf HM (2004) Peridiverticular colonic hyaline
rings (pulse granulomas): report of two cases associated
with perforated diverticula. Annals of Diagnostic Pathology8,
3759.
Henriques et al. Hyaline ring granulomas in odontogenic
cysts
2012 International Endodontic Journal International Endodontic
Journal, 46, 2029, 2013 29