-
Surgery for Obesity and Related Disea
Technic xenY
Mark D h.D.c,Emma Patters H. F.A.C.S.e,Gregory Daki skey,
M.D.e,
James .D.i,
Received December 13, 2013; accepted May 21, 2014
The last 2 decades have seen a dramatic increase in
the*Correspondence: Dr. Mark Douglas Smith, 37 Duke Street,
Invercar-
numbers of bariatric operations performed in the United
Statesand worldwide. Reasons for this include the growing
epidemic
http://dx.doi.org/10.1016/j.soard.2014.05.0361550-7289/r 2015
American Society for Metabolic and Bariatric Surgery. Published by
Elsevier Inc. All rights reserved.
gill 9810, New Zealand.E-mail: [email protected], [email protected]
(Mark D. Smith)Keywords: Roux-en-Y gastric bypass; Anastomotic
leak; Technical factorsAbstract Background: Anastomotic leak is one
of the most serious complications after Roux-en-Y gastric
bypass(RYGB). Our objective was to examine the relationship between
technical factors and incidence ofclinically relevant anastomotic
leak after RYGB in longitudinal assessment of bariatric surgery
(LABS).The setting of the study was 11 bariatric centers in the
United States, university, and private practice.Methods: Patient
characteristics, technical factors of surgery, and postoperative
outcomes wereassessed by trained researchers using standardized
protocols. Correlation of surgical factors ofpatients undergoing
RYGB (n 4444) with the incidence of postoperative anastomotic leak
wasassessed by univariate 2 analysis.Results: Forty-four
participants (1.0%, 95% CI .7%1.3%) experienced a clinically
relevantanastomotic leak. Of these, 39 (89%) underwent abdominal
reoperation and 3 (7%) died. Technicalfactors associated with
anastomotic leak were open surgery (Po .0001), revision surgery(Po
.0001), and use of an abdominal drain (P .02). Provocative leak
testing, method of gas-trojejunostomy, and use of brin sealant were
not associated with anastomotic leak.Conclusions: Anastomotic leak
after RYGB was rare (1.0%). Most cases required
reintervention;however, the majority (93%) recovered from this
event. Open surgery, revision surgery, and routinedrain placement
were associated with increased leak rate. Some of these ndings may
be due todifferences in preoperative patient risk. (Surg Obes Relat
Dis 2015;11:313320.) r 2015 AmericanSociety for Metabolic and
Bariatric Surgery. Published by Elsevier Inc. All rights
reserved.INational Institute of Diabetes and Digestive and Kidney
Diseases, Bethesda, MarylandjOregon Health and Science University,
Portland, Oregonal factors associated with anastomotic leak after
Rougastric bypass
. Smith, M.B.Ch.B.a,*, Abidemi Adeniji, Ph.D.b, Abdus S. Wahed,
Pon, M.D.a, William Chapman, M.D.d, Anita P. Courcoulas, M.D.
M.P.n, M.D. F.A.C.S.f, David Flum, M.D. M.P.H. F.A.C.S.g, Carol
McCloE. Mitchell, M.D.h, Alfons Pomp, M.D. F.A.C.S.f, Myrlene
Staten, M
Bruce Wolfe, M.D. FACSjaLegacy Good Samaritan Medical Center,
Portland, Oregon
bBoehringer Ingelheim, Ridgeeld, ConnecticutcUniversity of
Pittsburgh, Pittsburgh, Pennsylvania
dDepartment of Surgery, East Carolina University School of
Medicine, Greenville, North CarolinaeUniversity of Pittsburgh
Medical Center, Pittsburgh, Pennsylvania
fCornell University, New York, New YorkgDepartment of Surgery,
University of Washington, Seattle, Washington
hNeuropsychiatric Research Institute, Fargo, North
DakotaOriginal articleses 11 (2015) 313320
-
anyone who had undergone bariatric surgery before enroll-
review of case notes and discussion with the treating
y andof obesity [1,2], the reported effectiveness of bariatric
surgeryin improving life expectancy and serious co-morbidities
[3,4],and the excellent safety prole of modern bariatric surgery
[5].Although multiple surgical options currently exist to
promotedurable weight loss, Roux-en-Y gastric bypass (RYGB)remains
one of the most commonly performed operations [6,7].Although RYGB
is effective in promoting durable weight
loss [8], it may be complicated by a number of
majorpostoperative events. Anastomotic leak after gastric bypass
israre; however, its consequences may be devastating.Reported rates
of anastomotic leak vary from .6% to 4.4%[9]. Surgical
reexploration is usually required for anastomoticleak, and hospital
stay is prolonged [10,11], resulting inincreased cost and
morbidity. Anastomotic leak is also anindependent risk factor for
early postoperative mortality [12].Factors associated with
anastomotic leak include clinical (or
patient) factors and technical factors. Identied clinical
factorsassociated with anastomotic leak include male sex, age,
andpresence of sleep apnea [12]. Unfortunately, other than
notoffering surgery to high-risk individuals, there is often
littlethat can be done to reduce clinical risk. In contrast to
clinicalrisk factors, technical risk factors are potentially
modiable bythe operating surgeon to reduce risk of anastomotic
leak.Examples of technical factors include method of
constructingthe anastomoses, intraoperative leak testing, and
routineabdominal drainage. However, the rare incidence of
anasto-motic leak after RYGB makes it difcult for a single
surgeonor center to accrue enough events to identify risk factors
orinvestigate strategies to reduce its incidence. Consequently,many
of the strategies employed by surgeons are either basedon basic
surgical principles or extrapolated from other gastro-intestinal
surgery [13,14]. A recent guideline published by theAmerican
Society of Metabolic and Bariatric Surgery foundno high-quality
evidence to support any intervention to reducethe incidence of
anastomotic leaks [15].The Longitudinal Assessment of Bariatric
Surgery (LABS)
is an 11-center consortium funded by the National Institute
ofDiabetes, Digestive and Kidney Diseases (NIDDK) in theNational
Institutes of Health (NIH) that conducts observationalcohort
studies of bariatric surgical outcomes. These involvelargely
prospective, standardized, and comprehensive collec-tions of
clinical data. LABS-1 collected 30-day outcome datain consecutive
patients, aged 18 years or older, undergoingprimary bariatric
surgery. LABS-2 comprises more detailedand ongoing data collection
in a selected cohort of patients,restricted to those who had not
had prior bariatric surgery. Thepurpose of the present study was to
describe the incidence andoutcomes of anastomotic leak after RYGB
in LABS and toexamine technical factors associated with its
occurrence.
Methods
Patients
M. D. Smith et al. / Surgery for Obesit314Patients were
recruited by LABS into either of 2 cohorts,designated LABS-1 and
LABS-2, at one of the 11surgeons. Method of gastrojejunostomy was
recorded onthe initial data collection forms as a binary response
towhether each of 3 methods (hand sewing, linear stapling,
orcircular stapling) was used in constructing the anastomosis.This
was recoded to reect the general use of these clinicalterms by
surgeons. Linear stapled with or without handsewing is treated as
predominantly linear stapled, circularstapled with or without hand
sewing is classied aspredominantly circular stapled, and hand sewn
with nostaples is classied as predominantly hand sewn.The primary
outcome for this analysis is clinically
relevant leak (CRL). Clinically relevant leak is dened asing in
LABS-2. LABS inclusion criteria and data collectionhave previously
been described in detail [16]. Data werecollected for bariatric
surgeries performed between March2005 and April 2009 and sent to
the Data CoordinatingCenter (DCC) at the University of Pittsburgh,
GraduateSchool of Public Health.The analysis included LABS patients
(LABS-1 and
LABS-2 patients) who underwent RYGB, either open orlaparoscopic,
including revision of RYGB.
Data collection
Data were collected prospectively on a large number ofclinical
and technical factors [16]; however, the site of anidentied
anastomotic leak was not part of the initial LABSdata collection
protocol. Because site of anastomotic leakwas considered important
to this analysis, this informationwas collected retrospectively by
LABS site investigators byparticipating centers: University of
Pittsburgh Medical Center(Pennsylvania), New YorkPresbyterian
Hospital (Columbia-Presbyterian or Valley Hospitals or
Weill-Cornell MedicalCollege; New York and New Jersey), East
Carolina MedicalCenter (North Carolina), the MeritCare Health
Systemsthrough the Neuropsychiatric Research Institute
(NorthDakota), Sacramento Bariatric (California), University
ofWashington Medical Center or Virginia Mason MedicalCenter
(Washington), and Oregon Health and Sciences Uni-versity or Legacy
Good Samaritan Medical Center (Oregon).The LABS protocols and
consent forms were approved by theInstitutional Review Board at
each institution.
Protocols
LABS-1, a study of 30-day outcomes, included allconsecutive
patients at least 18 years of age who consentedto participate.
LABS-2 involves long-term follow-up anddata collection.
Accordingly, in contrast to LABS-1, non-consecutive patients who
would be able to undertake therequired follow-up were selected for
recruitment, excluding
Related Diseases 11 (2015) 313320patients undergoing readmission
or reintervention for asuspected anastomotic leak, where the
presence of a leak
-
was subsequently conrmed by the investigator or LABSadjudication
subcommittee on review of the medical record.Anastomotic leaks
diagnosed on the basis of radiology oranalysis of abdominal drain
contents, which did not requirereadmission or reintervention, were
not considered CRLsfor the purpose of this analysis.
Statistical analysis
Baseline demographic characteristics are presented asfrequencies
and percentages for categorical variables andcompared between
groups (e.g., participants with and with-out anastomosis test)
using 2 test or the exact equivalent(e.g., Fishers exact test) as
appropriate. Continuous charac-teristics such as the duration of
surgery are summarized withmedians and interquartile ranges and are
compared betweengroups using the Wilcoxon rank-sum test. Incidence
of CRLin the overall sample and in the subgroups is presented
asfrequencies and percentages. The association between base-line
demographic characteristics, co-morbidities, intraopera-tive
factors, and routine leak testing with the likelihood ofclinically
relevant leak was evaluated using 2 test or its
exact version (when the expected frequencies were smallerthan
5), separately for each variable. Pair-wise comparisonsbetween
various methods of anastomosis were conductedusing Holms step-down
method to adjust for multiplicity.We did not consider a
multivariable adjusted analysis
because the outcome CRL was rare (approximately 1%) andhence the
sample size was too small to conduct a statisti-cally powered
adjusted analysis. For all statistical analyses,Statistical
Analysis Systems (SAS) version 9.3 (SASInstitute; Cary, NC) was
used. A cut-off of o.05 was usedto determine statistical
signicance.
Results
The analysis included 4444 patients who had RYGBsurgery in LABS
consortium (LABS-1 and LABS-2).Patient clinical characteristics are
presented in Table 1.
Clinically relevant leaks
Of the included 4444 patients, 44 suffered a CRL (1%).The most
common site of leak was the gastrojejunostomy
Table 1Participant demographic characteristics, overall and by
anastomosis test
Characteristic Total (N 4444) Patients without anastomosis
test(n 636)
Patients with anastomosis test(n 3803)
P
Surgery performed n % n % n % o.0001
Laparoscopic gastric bypass 3841 86.4 379 59.6 3458 90.9Open
gastric bypass 603 13.6 257 40.4 345 9.1
18.0
811641871525217.8
654321 50.5 2024 53.219164
493143
40594
62312
503132
Technical Factors and Anastomotic Leak after RYGB / Surgery for
Obesity and Related Diseases 11 (2015) 313320 315Patient age (yr),
range 18.075.0Median (Q1, Q3) 45.0 (36.0,53.0)Age (yr)o30 431
9.73039 1126 25.34049 1302 29.35059 1179 26.560 406 9.1
BMI (kg/m2), range 17.8107.4Median (Q1, Q3) 46.9 (42.6, 52.6)BMI
(kg/m2)o35 66 1.535o 40 462 10.440o 50 2346 52.850o 60 1174 26.460
396 8.9
MaleNo 3574 80.4Yes 870 19.6
White/Caucasian (41 missing)No 509 11.6Yes 3894 88.4
Hispanic (2 missing)No 4186 94.2Yes 256 5.8
Current or recent smoker (13 missing)No 3766 85.0Yes 665 15.0BMI
body mass index.30.0 982 25.810.1 332 8.7
.0477.5 3078 80.922.5 725 19.1
o.00016.3 468 12.493.7 3296 87.6
o.000198.1 3558 93.61.9 244 6.4
o.000179.2 3258 85.920.8 533 14.123.9 1025 27.08.2 354 9.3
79.7 19.2107.4 .00648.1 (43.1, 53.6) 46.8 (42.5, 52.4)
.0530.9 58 1.58.5 407 10.775.0 18.073.0 .05744.0 (35.5, 52.0)
45.0 (36.0, 53.0)
.0412.7 349 9.225.8 962 25.329.4 1113 29.3
-
(28/44, Table 2), followed by the jejunojenostomy
(7/44).Clinical characteristics of the patients with and withoutCRL
are presented in Table 3. Although not statisticallyadequately
powered (because of low incidence rate), weexplored the bivariate
association (unadjusted) betweenpatient and surgeon characteristics
with incidence of CRL.In unadjusted analysis, no demographic
characteristics weresignicantly associated with the incidence of
CRL.Of the 44 patients with a CRL, 39 required reoperation
(17 laparoscopic, 12 open). The median time betweenRYGB and
reintervention was 5.5 days (range 125 d).Median length of stay was
7.0 days in those with a CRLcompared with 2.0 days for those
without. Approximately
method of gastrojejunostomy is unlikely to affect CRL at
Table 3a. Clinically relevant leak by demographic
characteristics
Characteristic N CRL P
n %
Age (yr) .46
o30 431 2 .53039 1126 8 .74049 1302 15 1.25059 1179 13 1.160 406
6 1.5
BMI (kg/m2) .07o35 66 2 3.035o 40 462 7 1.540o 50 2346 16 .750o
60 1174 12 1.0
60 396 7 1.8Male .88No 3574 35 .9Yes 870 9 1.0
White/Caucasian (41 missing) .61No 509 4 .8Yes 3894 40 1.0
Hispanic (2 missing) .76No 4186 41 .9Yes 256 3 1.2
Current or recent smoker (13 missing) .13No 3766 41 1.1Yes 665 3
.5
Albumin (g/dL) (394 missing) .65Low:o3 g/dL 24 0 0Normal: 36
g/dL 4026 35 .9
CRL clinically relevant leak; BMI body mass index.Table 3b.
Clinically relevant leak by health status
Characteristic N CRL P
n %
Hypertension .39No 1897 16 .8Yes 2547 28 1.1Hypertension therapy
(75 missing) .77No medication 263 4 1.5Single medication 1099 11
1.0Multiple medication 1110 13 1.2
Diabetes .10No 2849 23 .8Yes 1595 21 1.3
Type of diabetes medication (4 missing) .42No diabetes
medication 232 1 .4Single oral medication 476 5 1.1Multiple oral
medication 369 7 1.9Insulin (with or without oral meds) 514 8
1.6
Congestive heart failure .27No 4348 42 .9Yes 96 2 2.1
Asthma .89No 3373 33 1.0Yes 1071 11 1.0
Inability to walk 200 ft (1 missing) .19
M. D. Smith et al. / Surgery for Obesity and Related Diseases 11
(2015) 313320316sites other than the gastrojejunostomy, sensitivity
analysiswas conducted by restricting the analysis to leaks
occurringat the gastrojejunostomy only. In this analysis the
incidenceof CRL at gastrojejunostomy was .31% versus .64%
versus.92% for predominantly linear-stapled versus
predominantly
Table 2Site of clinically relevant leak*
Site of leak Total (N 43)Gastric pouch staple line 5
11.4Gastrojejunostomy 28 63.6Gastric remnant staple line 2
4.6Jejunojejunostomy 7 15.9Small intestine other 1 2.3Others 4
9.1
*Clinically relevant leak is a conrmed leak at gastric pouch
staple lineor gastrojejunostomy.
Multiple sites may apply.1 participant missing site of leak
form.List of others (n 4): colon; intraabdominal
abscessexploratory98% of those with no CRL had a length of hospital
stayo7days, compared with 50% with a CRL.The mortality rate was
6.8% (3/44) among those with a
CRL compared with .3% (13/4400) among those withno CRL.
Technical factors
A CRL was more common among those undergoing arevision RYGB
compared with a primary surgery(Table 4), and after open compared
with laparoscopicRYGB. Placement of an abdominal drain was
alsoassociated with an increased incidence of CRL. The useof brin
sealant was not associated with CRL in LABS.These associations
persisted when analysis was restrictedto leaks occurring at the
gastrojejunostomy or gastricpouch only.In the initial analysis CRL
was observed less often after a
linear stapled gastrojejunostomy compared with circular-stapled
or hand-sewn gastrojejunostomy. However, becausesurgery negative;
gastric fundus; esophageal leak.No 4359 42 1.0Yes 84 2 2.4
-
Of the 3803 with anastomosis test result, 143 (3.8%) hada
positive leak test. No demographic or clinical character-istics had
any trend of association with the likelihood of apositive leak test
(data not shown). No statistically
Table 4a. Clinically relevant leak by technical factors
Characteristic N CRL P
n %
Surgery type o.0001
Primary surgery 4286 34 .8
urgery for Obesity and Related Diseases 11 (2015) 313320
317Table 3Continued.
Table 3b. Clinically relevant leak by health status
Characteristic N CRL P
n %
History of DVT or PE .07No 4271 40 .9Yes 173 4 2.3
Sleep apnea .42No 2187 19 .9Yes 2257 25 1.1CPAP .23No 423 7
1.7
Technical Factors and Anastomotic Leak after RYGB /
Scircular-stapled versus hand-sewn gastrojejunal anastomo-sis,
respectively (P .12).
Provocative leak testing
Of the 33 surgeons who had done at least 10 LABSsurgeries, 29
surgeons (87.8%) routinely tested (in Z90%cases) the gastrojejunal
anastomosis during surgery. Of the3803 (85.7%) patients who
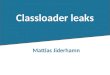
underwent provocative leaktesting, 143 (3.8%) had a positive test.
The anastomosis testwas done by 3 methods: 548 were tested with
air, of whom10 (1.8%) tested positive; 2011 were tested with
endoscopy,of whom 114 (5.6%) tested positive; and 1515 were
testedwith methylene blue, of whom 20 (1.3%) tested positive(Fig.
1).
Yes 1834 18 1.0Supplemental oxygen dependent (9 missing) .93No
2165 24 1.1Yes 83 1 1.2
Ischemic heart disease .63No 4213 41 1.0Yes 231 3 1.3
Pulmonary hypertension .47No 4394 43 1.0Yes 50 1 2.0
Venous edema w/ulcerations (280 missing) .0003No 3961 34 .9Yes
203 7 3.4
Beta-blocker (61 missing) .45No 3558 33 .9Yes 825 10 1.2
Statin/lipid-lowering agent .0827No 3241 27 .8Yes 1203 17
1.4
Therapeutic anticoagulation .06No 4227 39 .9Yes 217 5 2.3
Narcotic .22No 3645 33 .9Yes 799 11 1.4
Antidepressant (61 missing) .005No 2545 16 .6Yes 1838 27 1.5
CRL clinically relevant leak; DVT deep vein thrombosis; PE
pulmonary embolism; CPAP continuous positive airway pressure.
Revision surgery 149 10 6.7Neither primary or revision surgery 9
0 0
Surgery performed o.0001Laparoscopic gastric bypass 3841 29
.8Open gastric bypass 603 15 2.5
Gastrojejunostomy sealed (22 missing) .36No 1854 21 1.1Yes 2568
22 .9
Drain placed at gastrojejunostomy .02No 3711 31 .8Yes 733 13
1.8
Method of gastrojejunostomy (33 missing) .02Predominantly linear
stapled 1594 9 .6Predominantly EEA 1731 17 1.0Predominantly hand
sewn 1086 18 1.7
Anastomosis tested (5 missing) .06No 636 2 .3Yes 3803 42 1.1
CRL clinically relevant leak; EEA end to end anastomosis
(circular)stapled.
Table 4b. Clinically relevant leak at gastrojejunostomy or
gastric pouch bytechnical factors
Characteristic N CRL at GJ P
n %
Surgery type o.0001Primary surgery 4286 25 .6Revision surgery
149 7 4.7Not rst time and not revision 9 0 0Surgery performed
o.0001Laparoscopic gastric bypass 3841 21 .5Open gastric bypass 603
11 1.8
Gastrojejunostomy sealed (22 missing) .999No 1854 13 .7Yes 2568
18 .7Drain placed at gastrojejunostomy .02No 3711 22 .6Yes 733 10
1.4Method of gastrojejunostomy (33 missing) .02Predominantly linear
stapled 1594 6 .4
Predominantly EEA 1731 12 .7Predominantly hand sewn 1086 14
1.3
Anastomosis tested (5 missing) .07No 636 1 .2Yes 3803 31 .8CRL
clinically relevant leak; GJ gastrojejunostomy; EEA end toend
anastomosis (circular) stapled.
-
signicant difference in CRL rate was found between those
GB su
stom
%) -ve
.4%) sCR
0 confi
y met
y andundergoing positive, negative, or no provocative leak
test.Median operative time (skin incision to skin closed) was
similar for those surgeries that included anastomosis
testcompared with those that did not (136 versus 138 minutes,P
.14).4444 RY
4439 with ana
3803 tested*548 By air 2011 By endoscopy1515 By methylene
blue
143 (3.8%) +ve**10 (1.8%) Air 114 (5.6%) Endoscopy20 (1.3%)
Meth. blue
3660 (96.2
52 (11 (0.7%) suspected CRL***
*Some were tested by multiple methods** 1 was tested positive by
both air and endoscopy
***This person was tested positive for anastomotic leak by
air
1 confirmed 3
Fig. 1. Clinically relevant leak b
M. D. Smith et al. / Surgery for Obesit318Discussion
This analysis found the incidence of CRL after RYGB inLABS is
rare at 1%. Clinically relevant leaks were morecommon after open
and revision surgery and when anabdominal drain was placed at the
time of surgery. Nodifference in CRL at the gastrojejunostomy was
observedbetween the different methods of constructing this
anasto-mosis. Provocative leak testing was not associated with
theincidence of gastrojejunostomy CRL in LABS. Most casesof CRL
required reintervention with consequent increase inhospital stay
and mortality risk; however, most cases alsorecovered from this
event.The ndings of the present study compare favorably with
other large series on anastomotic leak after RYGB. A
single-center series examining the outcomes of 3828
patientsundergoing RYGB over a 23-year period found an anasto-motic
leak rate of 3.9% [10]. Anastomotic leaks were morecommon after
revisional RYGB (8.0%); however, in contrastto LABS, leaks were
more common after laparoscopicRYGB (5.2%) than open RYGB (2.6%). It
is important tonote that this series includes the period when
laparoscopicRYGB was introduced and thato1/3 procedures
werelaparoscopic (1080/3828). In this series, the overall
mortalityafter anastomotic leak was 14.7%, although mortality
washigher after leak at the jejunojeunostomy (40%) than
thegastrojejunostomy (9%). Sixty-eight percent of patients inthis
series with anastomotic leak at the gastrojejunostomywere managed
nonoperatively, with none of these requiringlater surgical
intervention and no mortality in this group.Another single center
series examined the outcomes of 60
patients with anastomotic leak from a total of 1764 under-
rgeries
osis test data
5 did not have data on anastomosis testof which 1 had a
suspected CRL
636 not tested
2 (0.31%) suspected CRL
uspected L
1 confirmedrmed
hod of anastomotic leak testing.
Related Diseases 11 (2015) 313320going RYGB (leak rate 3.4%)
[17]. Again approximatelyone third (n 573) of patients had RYGB
performed via alaparoscopic approach. The authors of this series
dividedleaks into localized subclinical leaks (n 12) and thosewhere
the patients exhibited clinical signs of sepsis(n 48). The overall
mortality rate from anastomotic leakwas 10%, 1 of the 3 patients
with a leak from thejejunojejunostomy died (mortality rate 33%).
None ofthe patients with subclinical leaks died.A systematic review
focusing specically on patients
undergoing laparoscopic RYGB identied 10 studies includ-ing 3464
patients. A total of 71 anastomotic leaks wereidentied to give an
unadjusted anastomotic leak rate of 2%.Although this anastomotic
leak rate was more in keepingwith that found in LABS, the included
studies may haveincorporated patients receiving surgery early in
the experi-ence of laparoscopic RYGB. Because of the nature of
thisreview, no analysis was conducted exploring the associationsof
clinical or technical factors with anastomotic leak.A MEDLINE-based
literature search was unable to
identify any large studies exploring the relationshipsbetween
multiple technical factors and anastomotic leakafter RYGB.
Nevertheless individual technical factors havebeen investigated in
numerous clinical studies. One suchfactor is whether the
gastrojejunostomy is constructed using
-
urgera linear-stapled, circular-stapled, or hand-sewn
technique.One of the interesting ndings of the present analysis
wasthe decreased overall anastomotic leak rate after linearstapled
anastomoses in LABS; however, this nding failedto persist when
restricted to leaks at the gastrojejunostomyonly. This corresponds
with the ndings of a MichiganBariatric Surgery Collaborative survey
where reported leakrates were identical for these 3 anastomosis
techniques [18],although circular stapled gastrojejunostomies were
associ-ated with an increased risk of anastomotic hemorrhage
andwound infection. A meta-analysis of studies
comparinglinear-stapled with circular-stapled anastomoses also
foundno difference between anastomotic leak rates but did showan
increased stricture rate with circular stapled anastomoses[19].
Because plausible explanations as to how method ofgastrojejunostomy
would affect leaks at other sites arelacking, this nding from LABS
may have resulted fromchance alone.The use of tissue sealants was
not associated with
alteration of the anastomosis leak rate in LABS. This
isconsistent with the results of a randomized trial of brinsealant
after RYGB where no difference in anastomotic leakrate was observed
between the treatment and control groups[20], although the use of
brin sealant was associated with areduced risk of anastomotic
hemorrhage.Placement of an abdominal drain was associated with
an
increased incidence of CRL in LABS. This study is not
arandomized trial of drain usage, and data were not collectedon the
reason for drain placement. It is possible that drainswere more
likely to be placed when a surgeon was concernedabout an elevated
risk of CRL. These results, however, donot support the assumption
that abdominal drainage reducesthe need for reintervention for CRL.
This nding isconsistent with previous comparative studies showing
routinedrain placement to be unnecessary after RYGB [21].Randomized
trials evaluating the use of routine drainageafter other major
abdominal surgery have also failed to ndbenet, even suggesting an
increased complication rate withdrain placement after
cholecystectomy [2225].No randomized trials could be identied of
intraoperative
leak testing for RYGB; however, a randomized trial ofpneumatic
testing in colorectal anastomoses found adecreased CRL rate in
tested patients [13]. Three series ofpatients undergoing RYGB with
routine endoscopic intra-operative leak testing report CRL rates of
o1% [2628].Another study compared leak testing via methylene
bluedelivered by orogastric tube with endoscopic leak testing[29].
In this study endoscopic leak testing had a higher rateof positive
leak tests intraoperatively but a lower rate ofpostoperative CRL.
Analysis of LABS data also indicatedmore positive leak tests after
endoscopic testing comparedwith other methods. However, because
only a handful ofpatients (269) were tested by multiple methods, we
do not
Technical Factors and Anastomotic Leak after RYGB / Shave
sufcient data to compare different methods of testing.Although no
difference was found in CRL betweenparticipants undergoing
positive, negative or no provocativeleak test, these ndings should
be interpreted with caution.The number of CRLs was small and, as
with drain place-ment, no data were collected on intraoperative
events thatcould have inuenced a surgeons decision to perform
leaktesting. Furthermore, the presence of a positive leak testwould
usually result in the operating surgeon reinforcing orrevising the
anastomosis, preventing CRL. Unfortunatelydata on the management of
a positive leak test were notcollected in LABS. Difference in
patient risk or technicalfactors not measured or corrected for in
LABS could alsopartially explain the ndings of the present
analysis.LABS is a large multicenter study incorporating
university
hospitals and private clinics. Despite the large numbers
ofincluded patients and comprehensive data collection, thepresent
study has revealed several counterintuitive ndings.One explanation
for this is the design of LABS as anobservational study rather than
a randomized trial. Random-ized trials are the only study design
able to account fornonmeasured confounding factors; however, large
random-ized trials are expensive, time consuming, and only able
todraw strong conclusions regarding the randomized interven-tion.
Despite this limitation, LABS data collection and riskadjustment
was prespecied to include all variables deemedpotentially
clinically relevant study investigators. Neverthe-less it is
possible that unmeasured clinical or technical factorsmay have
contributed to some of the unexpected ndings ofthis analysis.
Participants may have undergone open RYGBbecause of anticipated
technical difculty; and surgeons mayhave chosen to use brin
sealant, place a drain, and conductprovocative leak testing when
they already had concernsabout the integrity of an anastomosis.The
denition of CRL used in this study is another
potential weakness. Because of the prespecied design fordenition
and capture of postoperative complications, it wasnot possible to
identify anastomotic leaks that did notrequire readmission to
hospital or endoscopic, radiologic, orsurgical reintervention. We
hypothesize that the only likelysituation where this would occur is
if a drain left at theinitial RYGB was completely successful in
draining theleak. However, the nding of increased rates of CRL in
apatient where a drain was placed at the initial RYGB makesthis
outcome unlikely.Another potential weakness of this study is the
small
number of CRLs. Although a testament to the excellentsafety
prole of modern RYGB surgery, this limited ourability to perform
adjusted analyses of associations. Also,univariable associations
presented were not adequatelypowered. Therefore, the conclusions
drawn should be takenas observations from a large prospective
multicenter study.The low number of CRLs in the present study also
limitsthe ability to extrapolate these ndings to centers with
ahigher rate of CRL.
y for Obesity and Related Diseases 11 (2015) 313320 319The
results of the present study conrm the low incidenceof CRL in
modern RYGB surgery. Although revision
-
y andsurgery continues to present an increased risk of CRL,
ourndings do not support increased leak rates after laparo-scopic
RYGB compared with the open approach. In fact,the reverse now
appears to be true. Although anastomoticleak remains a major
complication, with prompt diagnosisand appropriate management,
resulting mortality is rare.Some of the unexpected or
counterintuitive ndings of
the present study might be addressed by future research.The
question of whether or not to test gastrojejunalanastomosis
intraoperatively would be best addressed bymulticenter randomized,
controlled trials. However, todetect a doubling of anastomotic leak
rate from 1% to 2%would require randomizing 45000 patients. Such
trials arelogistically difcult and expensive to conduct. An
alter-native is systematic review and meta-analysis of
smallerrandomized trials. Universally agreed endpoints and
well-designed studies would facilitate later quantitative summaryof
the results.
Conclusions
Anastomotic leak after RYGB in LABS was rare, limit-ing the
power of even this large multicenter study toexamine associated
factors. Method of gastrojejunostomy,routine provocative leak
testing, and use of brin sealantwere not associated with incidence
of CRL in LABS. In thisnonrandomized study, increased incidence of
CRL wasobserved after revision or open RYGB compared withprimary
laparoscopic surgery. No technical factors wereidentied as
associated with a reduced incidence of CRL.
Disclosures
The authors have no commercial associations that mightbe a
conict of interest in relation to this article.
References
[1] Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and
trendsin obesity among US adults, 1999-2008. JAMA
2010;303:23541.
[2] Ford ES, Mokdad AH. Epidemiology of obesity in the
WesternHemisphere. J Clin Endocrinol Metab 2008;93:S18.
[3] Adams TD, Gress RE, Smith SC, et al. Long-term mortality
aftergastric bypass surgery. N Engl J Med 2007;357:75361.
[4] Sjostrom L, Narbro K, Sjostrom CD, et al. Effects of
bariatric surgeryon mortality in Swedish obese subjects. N Engl J
Med 2007;357:74152.
[5] Flum DR, Belle SH, King WC, et al. Perioperative safety in
thelongitudinal assessment of bariatric surgery. N Engl J Med
2009;361:44554.
[6] Hinojosa MW, Varela JE, Parikh D, Smith BR, Nguyen XM,
NguyenNT. National trends in use and outcome of laparoscopic
adjustablegastric banding. Surg Obes Relat Dis 2009;5:1505.
[7] Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric
surgicalprocedures. JAMA 2005;294:190917.
[8] White S, Brooks E, Jurikova L, Stubbs RS. Long-term outcomes
aftergastric bypass. Obes Surg 2005;15:15563.
M. D. Smith et al. / Surgery for Obesit320[9] Nguyen NT, Wilson
SE. Complications of antiobesity surgery. NatClin Pract
Gastroenterol Hepatol 2007;4:13847.[10] Lee S, Carmody B, Wolfe L,
et al. Effect of location and speed ofdiagnosis on anastomotic leak
outcomes in 3828 gastric bypass cases.J Gastrointest Surg
2007;11:70813.
[11] Marshall JS, Srivastava A, Gupta SK, Rossi TR, DeBord JR.
Roux-en-Y gastric bypass leak complications. Arch Surg
2003;138:5203. (discussion 523).
[12] Fernandez AZJ, DeMaria EJ, Tichansky DS, et al. Experience
withover 3,000 open and laparoscopic bariatric procedures:
multivariateanalysis of factors related to leak and resultant
mortality. Surg Endosc2004;18:1937.
[13] Beard JD, Nicholson ML, Sayers RD, Lloyd D, Everson
NW.Intraoperative air testing of colorectal anastomoses: a
prospective,randomized trial. Br J Surg 1990;77:10957.
[14] Ricciardi R, Roberts PL, Marcello PW, Hall JF, Read TE,
SchoetzDJ. Anastomotic leak testing after colorectal resection:
what are thedata? Arch Surg 2009;144:40711 (discussion 411).
[15] ASMBS guideline on the prevention and detection of
gastrointestinalleak after gastric bypass including the role of
imaging and surgicalexploration. Surg Obes Relat Dis
2009;5:2936.
[16] Belle SH, Berk PD, Courcoulas AP, et al. Safety and efcacy
ofbariatric surgery: Longitudinal Assessment of Bariatric Surgery.
SurgObes Relat Dis 2007;3:11626.
[17] Csendes A, Burgos AM, Braghetto I. Classication and
managementof leaks after gastric bypass for patients with morbid
obesity:a prospective study of 60 patients. Obes Surg
2012;22:85562.
[18] Finks JF, Carlin A, Share D, et al. Effect of surgical
techniques onclinical outcomes after laparoscopic gastric
bypassresults from theMichigan Bariatric Surgery Collaborative.
Surg Obes Relat Dis2011;7:2849.
[19] Giordano S, Salminen P, Biancari F, Victorzon M. Linear
staplertechnique may be safer than circular in gastrojejunal
anastomosis forlaparoscopic Roux-en-Y gastric bypass: a
meta-analysis of compara-tive studies. Obes Surg
2011;21:195864.
[20] Silecchia G, Boru CE, Mouiel J, et al. The use of brin
sealant to preventmajor complications following laparoscopic
gastric bypass: results of amulticenter, randomized trial. Surg
Endosc 2008;22:24927.
[21] Kavuturu S, Rogers AM, Haluck RS. Routine drain placement
inRoux-en-Y gastric bypass: an expanded retrospective
comparativestudy of 755 patients and review of the literature. Obes
Surg 2012;22:17781.
[22] Gurusamy KS, Samraj K. Routine abdominal drainage for
uncompli-cated open cholecystectomy. Cochrane Database Syst Rev
2007.(CD006003.).
[23] Gurusamy KS, Samraj K, Davidson BR. Routine abdominal
drainagefor uncomplicated liver resection. Cochrane Database Syst
Rev 2007.(CD006232.).
[24] Gurusamy KS, Samraj K, Mullerat P, Davidson BR.
Routineabdominal drainage for uncomplicated laparoscopic
cholecystectomy.Cochrane Database Syst Rev 2007. (CD006003.).
[25] Jesus EC, Karliczek A, Matos D, Castro AA, Atallah AN.
Prophy-lactic anastomotic drainage for colorectal surgery. Cochrane
DatabaseSyst Rev 2004. (CD002100.).
[26] Alasfar F, Chand B. Intraoperative endoscopy for
laparoscopic Roux-en-Y gastric bypass: leak test and beyond. Surg
Laparosc EndoscPercutan Tech 2010;20:4247.
[27] Kligman MD. Intraoperative endoscopic pneumatic testing for
gastro-jejunal anastomotic integrity during laparoscopic Roux-en-Y
gastricbypass. Surg Endosc 2007;21:14035.
[28] Shin RB. Intraoperative endoscopic test resulting in no
postoperativeleaks from the gastric pouch and gastrojejunal
anastomosis in 366laparoscopic Roux-en-Y gastric bypasses. Obes
Surg 2004;14:10679.
[29] Alaedeen D, Madan AK, Ro CY, Khan KA, Martinez JM,
Tichansky
Related Diseases 11 (2015) 313320DS. Intraoperative endoscopy
and leaks after laparoscopic Roux-en-Ygastric bypass. Am Surg
2009;75:4858. (discussion 488).
Technical factors associated with anastomotic leak after
Roux-en-Y gastric bypassMethodsPatientsProtocolsData
collectionStatistical analysis
ResultsClinically relevant leaksTechnical factorsProvocative
leak testing
DiscussionConclusionsDisclosuresReferences