Embed Size (px)
Citation preview
AIa
J
T2Cisdio
adndnEmacritin
alssa
i
2
t
atC
t(
P
natomy and Pathophysiology of Spinal Cordnjury Associated With Regional Anesthesiand Pain Medicine
oseph M. Neal, M.D.
bmaitpsr
M
osttcttr
D
rwtmsiaatttcttpAusLi
he American Society of Regional Anesthesia andPain Medicine (ASRA) convened a panel in April
005 to create a Practice Advisory on the Neurologicomplications of Regional Anesthesia and Pain Med-
cine. This review deals with the pathophysiology ofpinal cord injury. The Practice Advisory recommen-ations are based on extensive review of existing an-mal and human studies, case reports, pathophysiol-gy, and expert opinion.The pathophysiology of spinal cord injury associ-
ted with anesthesia techniques is reviewed inepth, including mechanical trauma from directeedle injury or mass lesions, vascular injury fromirect needle trauma or spinal cord infarction, andeurotoxicity from local anesthetics and adjuvants.ight specific recommendations are offered thatay reduce the likelihood of spinal cord injury
ssociated with regional anesthetic or pain medi-ine techniques. Spinal cord injuries associated withegional anesthesia and pain medicine are exceed-ngly rare. The Practice Advisory’s recommenda-ions may, in selected cases, reduce the likelihood ofnjury, but the vast majority of these injuries areeither predictable nor preventable.Injury to the neuraxis as a consequence of regional
nesthesia or pain medicine procedures is ultimatelyinked to anatomic and/or physiologic damage to thepinal cord, the spinal nerve roots, or their bloodupply. Mechanisms of injury are sometimes identifi-ble, as in the case of epidural hematoma, but can also
From the Department of Anesthesiology, Virginia Mason Med-cal Center, Seattle, WA.
Accepted for publication October 3, 2006. Updated July 3,008.James P. Rathmell, M.D. served as acting Editor-in-Chief for
his manuscript.Presented as part of the American Society of Regional Anesthesia
nd Pain Medicine’s Practice Advisory on Neurological Complica-ions of Regional Anesthesia and Pain Medicine, Toronto, ON,anada, April 23, 2005.Reprint requests: Joseph M. Neal, M.D., Department of Anes-
hesiology, Virginia Mason Medical Center, 1100 Ninth AvenueB2-AN), Seattle, WA 98101. E-mail: [email protected]
© 2008 by the American Society of Regional Anesthesia andain Medicine.
r1098-7339/08/3305-0001$34.00/0doi:10.1016/j.rapm.2006.10.014
Regional Anesthesia and Pain Medicine, Vol 33, No
e exceedingly difficult to pinpoint, as exemplified byost cases of presumed spinal vascular injury. This
rticle will review the pathophysiology of spinal cordnjury, including mechanical, vascular, and neuro-oxic etiologies. Its goal is to provide an anatomic andathophysiologic basis from which to build an under-tanding of neuraxial complications associated withegional anesthesia and pain medicine.
echanical Injury
Many neuraxial anesthetic complications are sec-ndary to mechanical injury of the spinal cord,pinal nerve roots, or the spinal nerves as they exithe intervertebral foramina. Injury to these struc-ures may involve the vertebral column, space-oc-upying lesions within the vertebral canal, or directrauma. These various mechanisms ultimately leado loss of anatomic and/or physiologic neural integ-ity and often result in permanent injury.1
irect Needle Trauma
The vertebral column acts as a protective bar-ier to the sensitive neural structures containedithin. The anesthesiologist desires to gain access
o these underlying spaces in a controlled, preciseanner. Deposition of anesthetic agents into the
ubarachnoid space presumes that the needle isntroduced caudad to the conus medullaris, therebyvoiding contact with the spinal cord. Case reportsnd medicolegal review suggest that direct spinal cordrauma has been associated with excessively caudadermination of the spinal cord and/or inaccurate de-ermination of bony landmarks that overlie where theonus medullaris ends.1,2 The spinal cord’s termina-ion typically coincides with the L1-2 vertebral in-erspace, but wide variation exists, with the terminusotentially occurring as high as T12 or as low as L4.3
line drawn between the iliac crests (Tuffier’s line)sually corresponds to the L4-5 interspace or the L4pinous process, but may instead cross the L3-4 or5-S1 interspaces.3 Furthermore, a practitioner’s
dentification of a vertebral interspace is often inaccu-
ate by 1 level cephalad or caudad, and up to 4 levels5 (September–October), 2008: pp 423–434 423
ipte
usdiilmrolopSiptitmttdoccltmiiq
r
Mswildctfnnpn
FNtirR
Fnsttpapto
424 Regional Anesthesia and Pain Medicine Vol. 33 No. 5 September–October 2008
n patients whose surface landmarks are difficult toalpate.2,4 These anatomic variations potentially leado needle placement more cephalad than intended,xposing the spinal cord to direct trauma.Two other anatomic occurrences contribute to
nintentionally placing a needle too close to thepinal cord. Accurate placement of an epidural nee-le relies on the ligamentum flavum to signal prox-mity to the epidural space and to indicate entrynto it when loss of resistance occurs. However, theigamentum flavum does not always fuse in the
idline,5 potentially permitting needle passage di-ectly into the epidural or subarachnoid space with-ut benefit of the customary firmness followed byoss of resistance (Fig 1). This anatomic anomalyccurs throughout the neuraxis, but is particularlyrevalent in the upper thoracic and cervical regions.5,6
imilar failure to contact identifiable landmarks dur-ng needle passage can arise with congenital dysra-hisms, such as spina bifida occulta. Second, the po-ential to unintentionally penetrate the meningesncreases substantially as one moves cephalad alonghe neuraxis, because the posterior-to-anterior di-ensions of the epidural space decrease from 5 mm
o 8 mm in the lumbar spine to 1 mm to 2 mm inhe upper thoracic and cervical spine.5 Once a nee-le enters the spinal cord, damage occurs as a resultf physical disruption of neural elements with ac-ompanying edema or hematoma,7,8 central syrinxreation from injected local anesthetic solution,9,10
ocal anesthetic or adjuvant toxicity, or a combina-ion of these mechanisms.11 Permanent damage isore likely to accompany the injection of solutions
nto the spinal cord; the simple passage of a needlento the spinal cord or nerve roots without subse-uent injection may not necessarily cause injury.Trauma to spinal nerve roots or spinal nerves
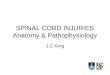
ig 1. Cryomicrotome axial section of the C7-T1 spine.ote that the ligamentum flavum has failed to fuse in
he midline (arrow), thereby permitting needle entrynto the epidural space without the customary loss ofesistance. Cryomicrotome from Quinn H. Hogan, M.D.eprinted from Hogan.5
epresents another cause of mechanical injury. b
idline or paramedian approaches to the neuraxishould easily avoid contact with spinal nerves,hich are partially protected by the vertebral lam-
nae and transverse processes, and are sufficientlyateral to avoid contact with medially directed nee-les. Needles that unintentionally deviate lateralan contact the spinal nerve or the anterior or pos-erior ramus outside the foramen; or if medial to theacet within the lateral recess, can contact the dorsalerve roots. Spinal nerves are also vulnerable toeedle injury during perispinal techniques such asaravertebral block or from too medially directedeedles during psoas compartment block (Fig 2). In
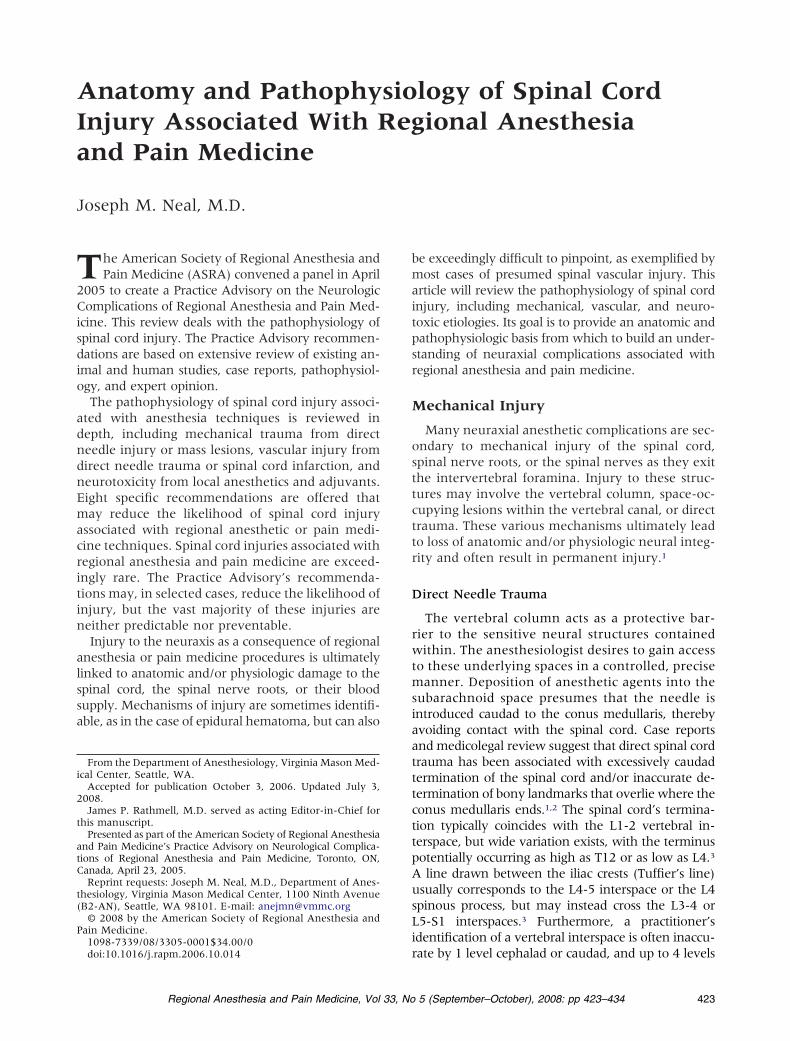
ig 2. Midline or paramedian approaches to the thoraciceuraxis (needles A and B) are unlikely to encounterpinal nerves or major feeding arteries. However, unin-entionally lateral approaches (needle C) are most likelyo contact the spinal nerve or the anterior or posteriorrimary ramus outside of the foramen. A transforaminalpproach (needle D) has the potential to come in closeroximity to the spinal nerve or spinal artery branch. Notehat transforaminal approaches are typically at the cervicalr lumbar levels, not the T6 level as illustrated. Illustration
y Gary J. Nelson. Reprinted from Neal and Rathmell.12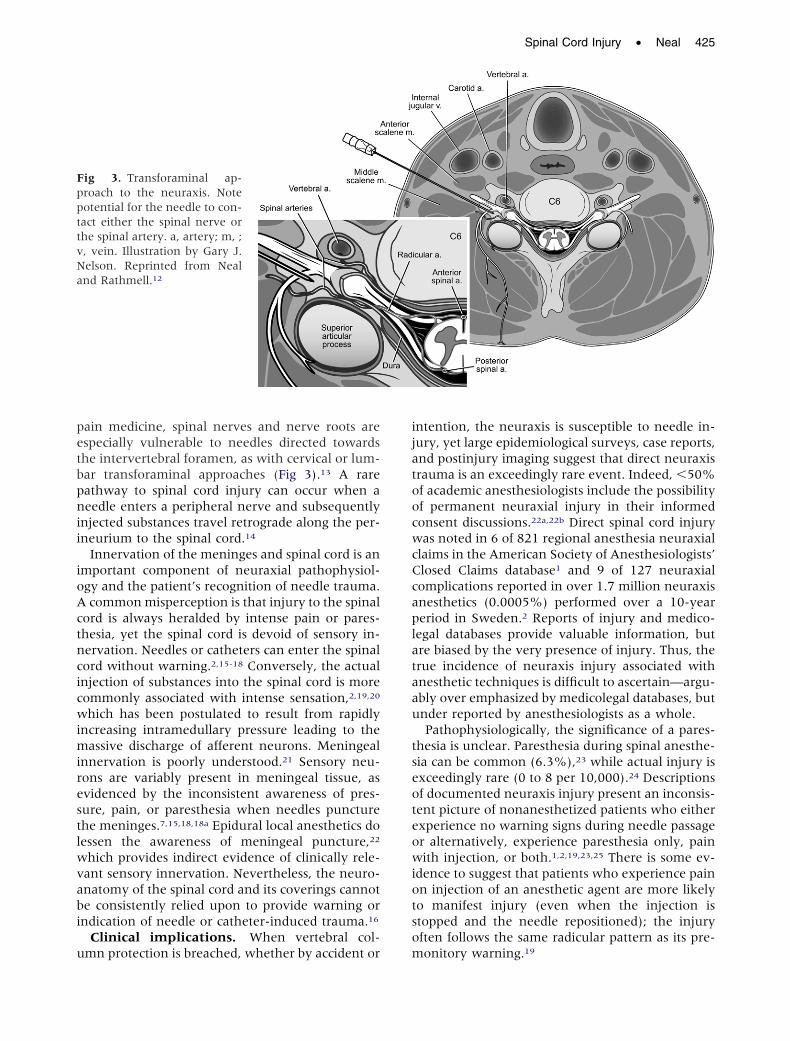
petbpnii
ioActncicwimirestlwvabi
u
ijatoocwcCcaplataau
tseoteowiotso
FppttvNa
Spinal Cord Injury • Neal 425
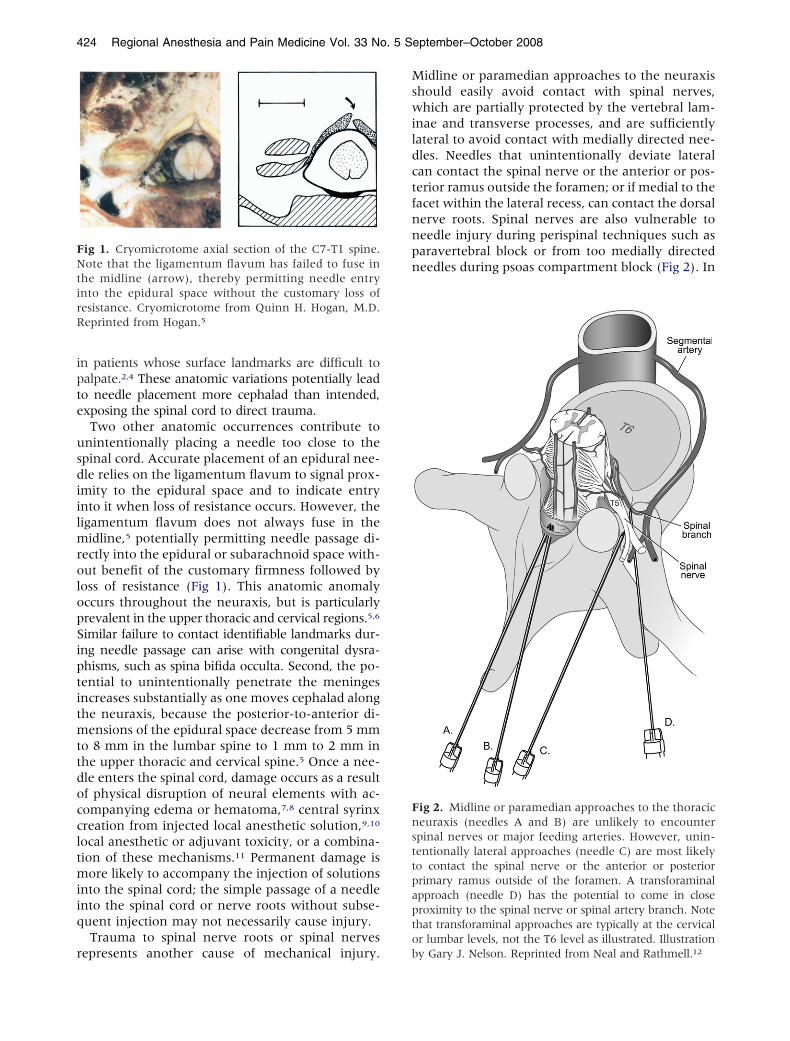
ain medicine, spinal nerves and nerve roots arespecially vulnerable to needles directed towardshe intervertebral foramen, as with cervical or lum-ar transforaminal approaches (Fig 3).13 A rareathway to spinal cord injury can occur when aeedle enters a peripheral nerve and subsequently
njected substances travel retrograde along the per-neurium to the spinal cord.14
Innervation of the meninges and spinal cord is anmportant component of neuraxial pathophysiol-gy and the patient’s recognition of needle trauma.common misperception is that injury to the spinal
ord is always heralded by intense pain or pares-hesia, yet the spinal cord is devoid of sensory in-ervation. Needles or catheters can enter the spinalord without warning.2,15-18 Conversely, the actualnjection of substances into the spinal cord is moreommonly associated with intense sensation,2,19,20
hich has been postulated to result from rapidlyncreasing intramedullary pressure leading to the
assive discharge of afferent neurons. Meningealnnervation is poorly understood.21 Sensory neu-ons are variably present in meningeal tissue, asvidenced by the inconsistent awareness of pres-ure, pain, or paresthesia when needles puncturehe meninges.7,15,18,18a Epidural local anesthetics doessen the awareness of meningeal puncture,22
hich provides indirect evidence of clinically rele-ant sensory innervation. Nevertheless, the neuro-natomy of the spinal cord and its coverings cannote consistently relied upon to provide warning orndication of needle or catheter-induced trauma.16
Clinical implications. When vertebral col-
ig 3. Transforaminal ap-roach to the neuraxis. Noteotential for the needle to con-act either the spinal nerve orhe spinal artery. a, artery; m, ;, vein. Illustration by Gary J.elson. Reprinted from Nealnd Rathmell.12
mn protection is breached, whether by accident or m
ntention, the neuraxis is susceptible to needle in-ury, yet large epidemiological surveys, case reports,nd postinjury imaging suggest that direct neuraxisrauma is an exceedingly rare event. Indeed, �50%f academic anesthesiologists include the possibilityf permanent neuraxial injury in their informedonsent discussions.22a,22b Direct spinal cord injuryas noted in 6 of 821 regional anesthesia neuraxial
laims in the American Society of Anesthesiologists’losed Claims database1 and 9 of 127 neuraxialomplications reported in over 1.7 million neuraxisnesthetics (0.0005%) performed over a 10-yeareriod in Sweden.2 Reports of injury and medico-egal databases provide valuable information, butre biased by the very presence of injury. Thus, therue incidence of neuraxis injury associated withnesthetic techniques is difficult to ascertain—argu-bly over emphasized by medicolegal databases, butnder reported by anesthesiologists as a whole.Pathophysiologically, the significance of a pares-
hesia is unclear. Paresthesia during spinal anesthe-ia can be common (6.3%),23 while actual injury isxceedingly rare (0 to 8 per 10,000).24 Descriptionsf documented neuraxis injury present an inconsis-ent picture of nonanesthetized patients who eitherxperience no warning signs during needle passager alternatively, experience paresthesia only, painith injection, or both.1,2,19,23,25 There is some ev-
dence to suggest that patients who experience painn injection of an anesthetic agent are more likelyo manifest injury (even when the injection istopped and the needle repositioned); the injuryften follows the same radicular pattern as its pre-
onitory warning.19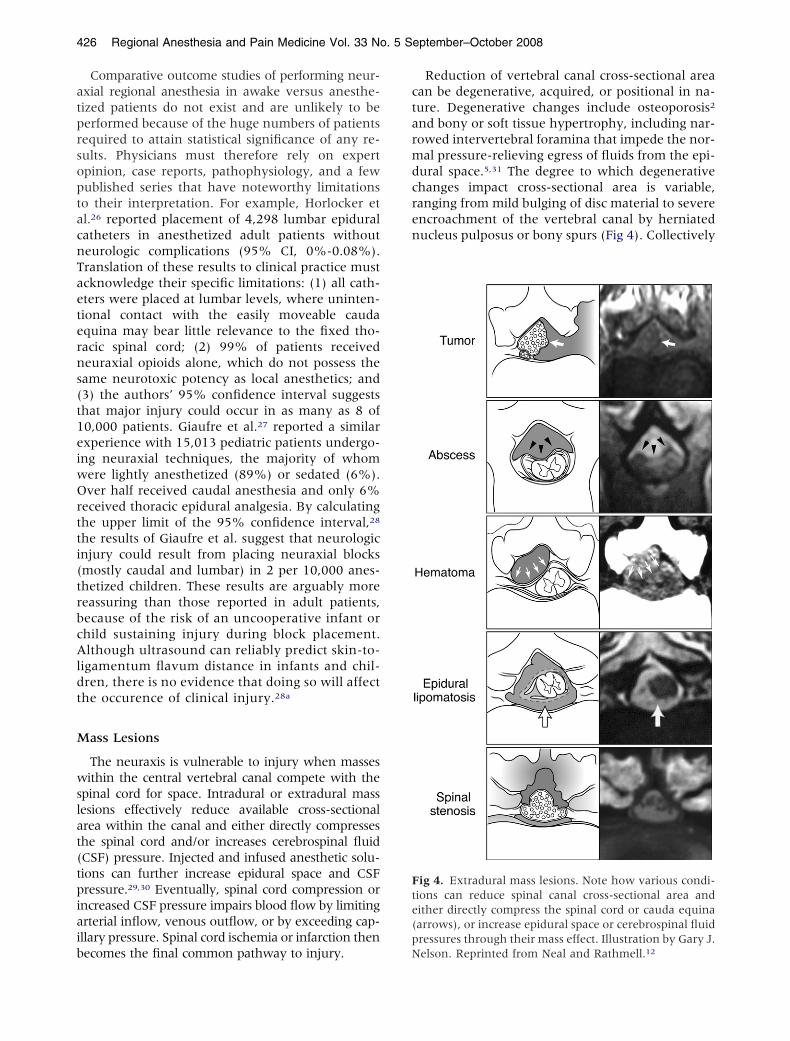
atprsoptacnTaeterns(t1eiwOrtti(trbcAldt
M
wslat(tpiaib
ctarmdcren
Fte(p
426 Regional Anesthesia and Pain Medicine Vol. 33 No. 5 September–October 2008
Comparative outcome studies of performing neur-xial regional anesthesia in awake versus anesthe-ized patients do not exist and are unlikely to beerformed because of the huge numbers of patientsequired to attain statistical significance of any re-ults. Physicians must therefore rely on expertpinion, case reports, pathophysiology, and a fewublished series that have noteworthy limitationso their interpretation. For example, Horlocker etl.26 reported placement of 4,298 lumbar epiduralatheters in anesthetized adult patients withouteurologic complications (95% CI, 0%-0.08%).ranslation of these results to clinical practice mustcknowledge their specific limitations: (1) all cath-ters were placed at lumbar levels, where uninten-ional contact with the easily moveable caudaquina may bear little relevance to the fixed tho-acic spinal cord; (2) 99% of patients receivedeuraxial opioids alone, which do not possess theame neurotoxic potency as local anesthetics; and3) the authors’ 95% confidence interval suggestshat major injury could occur in as many as 8 of0,000 patients. Giaufre et al.27 reported a similarxperience with 15,013 pediatric patients undergo-ng neuraxial techniques, the majority of whomere lightly anesthetized (89%) or sedated (6%).ver half received caudal anesthesia and only 6%
eceived thoracic epidural analgesia. By calculatinghe upper limit of the 95% confidence interval,28
he results of Giaufre et al. suggest that neurologicnjury could result from placing neuraxial blocksmostly caudal and lumbar) in 2 per 10,000 anes-hetized children. These results are arguably moreeassuring than those reported in adult patients,ecause of the risk of an uncooperative infant orhild sustaining injury during block placement.lthough ultrasound can reliably predict skin-to-
igamentum flavum distance in infants and chil-ren, there is no evidence that doing so will affecthe occurence of clinical injury.28a
ass Lesions
The neuraxis is vulnerable to injury when massesithin the central vertebral canal compete with the
pinal cord for space. Intradural or extradural massesions effectively reduce available cross-sectionalrea within the canal and either directly compresseshe spinal cord and/or increases cerebrospinal fluidCSF) pressure. Injected and infused anesthetic solu-ions can further increase epidural space and CSFressure.29,30 Eventually, spinal cord compression orncreased CSF pressure impairs blood flow by limitingrterial inflow, venous outflow, or by exceeding cap-llary pressure. Spinal cord ischemia or infarction then
ecomes the final common pathway to injury. NReduction of vertebral canal cross-sectional areaan be degenerative, acquired, or positional in na-ure. Degenerative changes include osteoporosis2
nd bony or soft tissue hypertrophy, including nar-owed intervertebral foramina that impede the nor-al pressure-relieving egress of fluids from the epi-
ural space.5,31 The degree to which degenerativehanges impact cross-sectional area is variable,anging from mild bulging of disc material to severencroachment of the vertebral canal by herniateducleus pulposus or bony spurs (Fig 4). Collectively
ig 4. Extradural mass lesions. Note how various condi-ions can reduce spinal canal cross-sectional area andither directly compress the spinal cord or cauda equinaarrows), or increase epidural space or cerebrospinal fluidressures through their mass effect. Illustration by Gary J.
elson. Reprinted from Neal and Rathmell.12
ttetTcmlontseti
tBcccdrtm
sinwegtcwl
csmcieCege
V
cedas
cr
SmotbauampthacnfbmAlnbhtcriraoms
r1mgslbdssS6sd
D
v
Spinal Cord Injury • Neal 427
ermed spinal stenosis, these changes are postulatedo contribute to neuraxis injury and may partiallyxplain why clinically significant epidural hema-oma happens more frequently in elderly patients.2
he clinical variability of spinal stenosis implies thatlinical decisions with respect to neuraxial blockust be individually based. For instance, known
umbar spinal stenosis may have little if any impactn thoracic epidural space pressure-volume dy-amics and would not be ipso facto a contraindica-ion to thoracic epidural anesthesia. Further, de-pite injected epidural solutions temporarily raisingpidural space pressure, there is no clear evidencehat their administration has caused spinal cordnjury in patients with spinal stenosis.
Acquired conditions affecting spinal canal cross-sec-ional area include intradural and extradural masses.esides intramedullary tumors, intradural space-oc-upying lesions can result from morphinoid-inducedatheter granulomas associated with chronic intrathe-al infusions.32,33 Extradural mass lesions include epi-ural hematoma and epidural abscess, in addition toarer conditions such as ligamentum flavum hyper-rophy or epidural tumor,34 lipomatosis,35-37 sclerede-a,38 or ependymoma39 (Fig 4).Patient positioning can also affect spinal canal cross-
ectional area. For example, available area decreasesn the lithotomy position.40 Case reports describeeuraxis injury associated with neuraxial blockadeherein it is speculated that the injury was at least
xacerbated by extreme lordosis (in a patient undereneral anesthesia),36 the lithotomy position in a pa-ient with spinal stenosis and facet joint synovialysts,41 or the lateral thoracotomy position in a patientith stenosed spinal arteries and ankylosing spondy-
itis.42
In summary, mechanical injury to the neuraxisan arise consequent to direct needle trauma or topace-occupying lesions whose mass effect compro-ises spinal cord blood flow. Evidence to support
ontribution to injury varies with the mechanism ofnjury. In the case of epidural hematoma or abscess,xtensive literature supports causation.1,2,19,25,43-45
onversely, neuraxis injury in the setting of rarextraspinal mass lesions, or relatively common sur-ical positions, spinal stenosis, or osteoporosis, onlystablishes association or chance occurrence.
ascular Injury
Disruption of spinal cord blood flow (SCBF) withonsequent spinal cord injury is a decidedly rarevent in which a precise mechanism of injury isifficult to pinpoint. This impreciseness results frommultitude of factors, including inexact imaging of
mall spinal blood vessels, complex interactions of q
oexisting disease processes, and a probable over-eliance on diagnosis of exclusion.
Anatomic and physiologic processes determineCBF. Arterial blood supply originates from seg-ental arteries that derive from the vertebral artery
r various primary and secondary branches fromhe aorta. Segmental arteries give rise to spinalranches, which enter an intervertebral foramennd continue as an anterior and/or posterior radic-lar artery. Medullary arteries are those radicularrteries that extend to the spinal cord to anasto-ose with the anterior spinal artery (ASA) and
aired posterior spinal arteries. Most medullary ar-eries supply the posterior circulation; fewer thanalf significantly serve the anterior spinal cord46
nd these are disproportionately distributed in theervical region.46a,46b Yet the cauda equina and spi-al cord receive two thirds of their blood supply
rom the ASA system. The lower thoracic and lum-osacral spinal cord is typically supplied by a singleajor artery (the radicularis magna or artery ofdamkiewicz) that connects to the ASA. The radicu-
aris magna artery arises from the left and enters theeuraxis between T9 and L1 in 80% of humans,47,48
ut may enter as high as T5 or as low as L5 in dogs andumans.47,49-51 The radicularis magna provides 25%o 50% of total SCBF. There also exists a nonrobustollateral circulation between the anterior and poste-ior systems via the vasa coronae; moreover, the ASAs continuous throughout its course.47 Nevertheless,egions of the innermost spinal cord are watershedreas at risk for inadequate circulation.46-48 Disruptionf a major reinforcing artery anywhere from the seg-ental arteries to the ASA could potentially cause
pinal cord infarction (Fig 5).Physiologically, SCBF is autoregulated within a
ange of 50 mmHg to 60 mmHg to 120 mmHg to35 mmHg mean arterial pressure (MAP) in animalodels.52,53 Spinal cord circulation is thus analo-
ous to cerebral circulation. SCBF varies in re-ponse to metabolic demand.54,55 Indeed, neuraxialocal anesthetic blockade is likely neuroprotectiveecause these agents reduce spinal cord metabolicemand.54-57 Only extreme degrees of hypotensionhould adversely affect SCBF in patients with intactpinal cord-blood barriers. In hemorrhaged dogs,CBF only decreased when the MAP was less than6 mmHg.58 Clinical studies in humans undergoingpinal surgery have demonstrated absence of injuryuring prolonged periods of 60 mmHg MAP.59
irect Needle Trauma
Mechanical- or drug-induced vasospasm, directascular trauma, or intravascular injection are fre-
uently offered explanations for disruption of SCBF.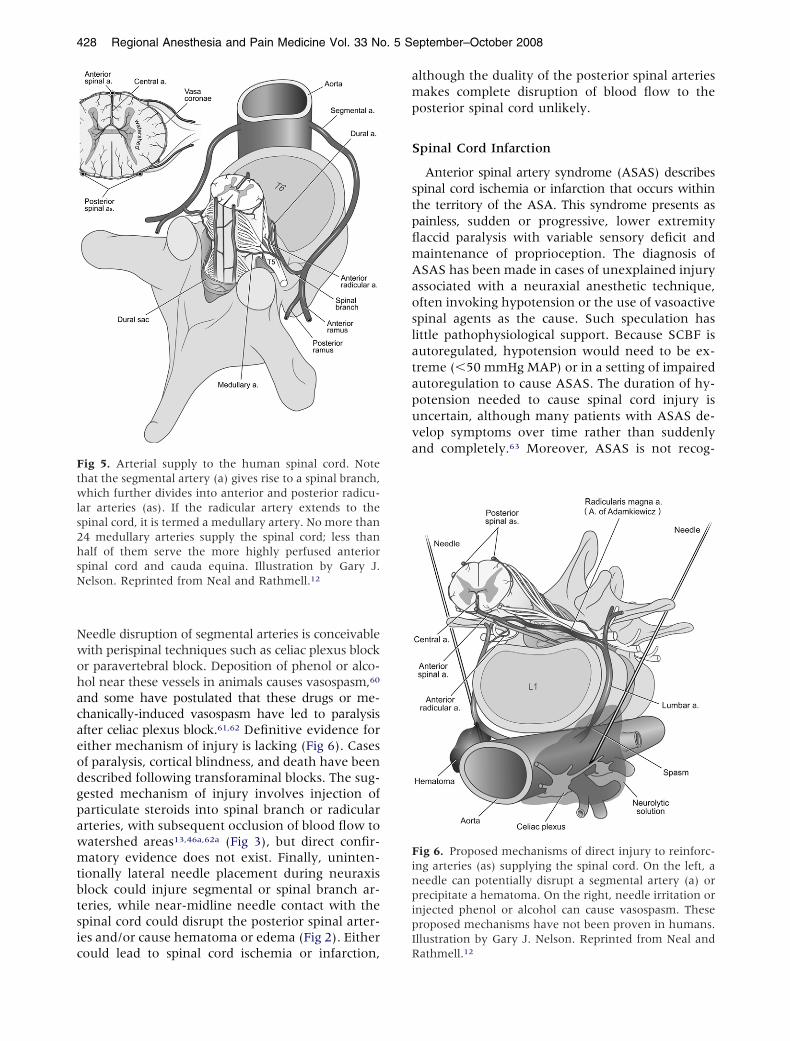
Nwohacaeodgpawmtbtsic
amp
S
stpflmAaoslatapuva
FinpipI
Ftwls2hsN
428 Regional Anesthesia and Pain Medicine Vol. 33 No. 5 September–October 2008
eedle disruption of segmental arteries is conceivableith perispinal techniques such as celiac plexus blockr paravertebral block. Deposition of phenol or alco-ol near these vessels in animals causes vasospasm,60
nd some have postulated that these drugs or me-hanically-induced vasospasm have led to paralysisfter celiac plexus block.61,62 Definitive evidence forither mechanism of injury is lacking (Fig 6). Casesf paralysis, cortical blindness, and death have beenescribed following transforaminal blocks. The sug-ested mechanism of injury involves injection ofarticulate steroids into spinal branch or radicularrteries, with subsequent occlusion of blood flow toatershed areas13,46a,62a (Fig 3), but direct confir-atory evidence does not exist. Finally, uninten-
ionally lateral needle placement during neuraxislock could injure segmental or spinal branch ar-eries, while near-midline needle contact with thepinal cord could disrupt the posterior spinal arter-es and/or cause hematoma or edema (Fig 2). Either
ig 5. Arterial supply to the human spinal cord. Notehat the segmental artery (a) gives rise to a spinal branch,hich further divides into anterior and posterior radicu-
ar arteries (as). If the radicular artery extends to thepinal cord, it is termed a medullary artery. No more than4 medullary arteries supply the spinal cord; less thanalf of them serve the more highly perfused anteriorpinal cord and cauda equina. Illustration by Gary J.elson. Reprinted from Neal and Rathmell.12
ould lead to spinal cord ischemia or infarction, R
lthough the duality of the posterior spinal arteriesakes complete disruption of blood flow to the
osterior spinal cord unlikely.
pinal Cord Infarction
Anterior spinal artery syndrome (ASAS) describespinal cord ischemia or infarction that occurs withinhe territory of the ASA. This syndrome presents asainless, sudden or progressive, lower extremityaccid paralysis with variable sensory deficit andaintenance of proprioception. The diagnosis ofSAS has been made in cases of unexplained injuryssociated with a neuraxial anesthetic technique,ften invoking hypotension or the use of vasoactivepinal agents as the cause. Such speculation hasittle pathophysiological support. Because SCBF isutoregulated, hypotension would need to be ex-reme (�50 mmHg MAP) or in a setting of impairedutoregulation to cause ASAS. The duration of hy-otension needed to cause spinal cord injury isncertain, although many patients with ASAS de-elop symptoms over time rather than suddenlynd completely.63 Moreover, ASAS is not recog-
ig 6. Proposed mechanisms of direct injury to reinforc-ng arteries (as) supplying the spinal cord. On the left, aeedle can potentially disrupt a segmental artery (a) orrecipitate a hematoma. On the right, needle irritation ornjected phenol or alcohol can cause vasospasm. Theseroposed mechanisms have not been proven in humans.llustration by Gary J. Nelson. Reprinted from Neal and
athmell.12
nprsh
dcdpSrybvotp
cricudcvpAihaA
aapcppNotrh
N
nttnblm
astncuarbnmottsrppalswncaptgtc
dtratciBtcaroesvfttappl
Spinal Cord Injury • Neal 429
ized as a complication commonly associated withrolonged low MAP conditions such as cardiac ar-est, cardiopulmonary bypass, or induced hypoten-ion of 60 mmHg or less for periods up to severalours.59,64-66
Local anesthetics have variable effects on SCBFepending on the specific local anesthetic and itsombination with adjuvant drugs,67 but their useoes not contribute to reduction in SCBF out ofroportion to reduced metabolic demand. Further,CBF in animal models is maintained through wideanges of MAP. Intravenous epinephrine or phen-lephrine does not alter central nervous systemlood flow.68 Adjuvant epinephrine does not ad-ersely affect SCBF.67 Thus, there is no animal datar pathophysiologic explanation to support the con-ention that hypotension or vasoactive agents arerobable causes of ASAS.Like direct spinal cord trauma, ASAS and spinal
ord infarct are rare complications—only 10 wereeported in 821 medicolegal claims for neuraxialnjuries.1 In a series of 54 patients with ASAS, manyases occurred spontaneously and only 1 patientnderwent a neuraxial anesthetic, which was notefinitively identified as the cause of injury.63 Theomorbidity of ASAS is more typically that of spinalascular atherosclerosis with subsequent embolichenomena or postlesion hypoperfusion. Indeed,SAS is most likely due to multiple insults includ-
ng atherosclerosis,42 aortic surgery, and/or severeypotension. There are no reliable historical or di-gnostic criteria to identify patients susceptible toSAS.In summary, direct vascular trauma from midline
nd paramedian approaches to the neuraxis is an-tomically unlikely, but possible during lateral ap-roaches or perispinal approaches such as psoasompartment or celiac plexus blocks. Injection ofarticulate matter into reinforcing arteries may ex-lain injury after transforaminal steroid techniques.o human studies confirm or refute these theoriesf causation. In ASAS, underlying patient condi-ions such as atherosclerosis are more probable andeasonable pathophysiologic explanations than areypotension or vasoactive agents.
eurotoxicity
Neurotoxicity is another pathophysiologic mecha-ism for anesthesia-related neuraxis injury. Neuro-oxicity can occur as an isolated event or in conjunc-ion with physical injury to the spinal cord or spinalerve roots.19 When physical trauma breaches thelood-spinal cord barrier, the neuraxis is exposed toocal anesthetics or vasoactive agents that are nor-
ally considered innocuous. o
Even in the absence of physical damage, uniquenatomic conditions contribute to the increasedusceptibility of certain neuraxial tissues to neuro-oxicity. For example, the cauda equina consists oferves that are partially unmyelinated.49 Its physi-al length increases surface area, making it partic-larly prone to contact with potentially neurotoxicgents. The spinal nerve roots (but not the dorsaloot ganglia) reside within the blood-spinal cordarrier, but are theoretically at increased risk foreurotoxicity because they lack the mechanical andetabolic protection afforded to peripheral nerves
r other structures within the central nervous sys-em. High-dose local anesthetics can cause localizedoxicity at the proximal portion of the posteriorpinal nerve root in rats.69 Further, spinal nerveoots have greater vascular permeability than otherarts of the spinal cord and receive a significantortion of their nutrition from diffusion via the CSFnd/or the radicular arteries. Thus, one can specu-ate that clearance of toxic substances away frompinal nerve roots may not be efficient comparedith nerves with a more robust blood supply. Spi-al nerve roots can be exposed to relatively con-entrated local anesthetics if injection is made intodural root sleeve, where small CSF volume im-
airs optimal dilution (Fig 3).49 All of these condi-ions potentially place the spinal nerve roots atreater risk for local anesthetic neurotoxicity, al-hough there are no animal or clinical studies toonfirm or refute this theory.Local anesthetic neurotoxicity is concentration-
ependent and can occur at concentrations lowerhan those used clinically.70,71 Local anesthetic neu-otoxicity is therefore determined primarily by localnesthetic concentration within the CSF, which inurn is impacted by the total dose delivered. Clini-ally, drug maldistribution and excessive drug dosencrease the CSF concentration of local anesthetics.oth of these conditions were believed contributory
o cases of cauda equina syndrome reported afterontinuous spinal anesthesia with microcatheters,72
lthough maldistribution can also occur with mac-ocatheters. Subsequent experimental models dem-nstrated that hyperbaric local anesthetics prefer-ntially remain within the lumbosacral area of theubarachnoid space when they were injected slowlyia small-bore catheters and when lumbar lordosisacilitated sacral residence of hyperbaric local anes-hetic solutions.73,74 Restricted pooling of concen-rated local anesthetic can manifest clinically as in-dequate sensory block level, which places theatient at risk for cauda equina syndrome if theractitioner responds to maldistribution by redosingocal anesthetic and exceeding the maximum rec-
mmended dose.72 Vasoconstrictors such as epi-
nmcntidi
twaegiRoaTcn2dehtrm2
tcioattnspam1
amjrvtndajwn
toetl
S
apnW
430 Regional Anesthesia and Pain Medicine Vol. 33 No. 5 September–October 2008
ephrine further worsen neurotoxicity in animalodels, most likely by reducing local anesthetic
learance,75 which is probably consequent to epi-ephrine decreasing dural blood flow.76 Recogni-ion of these conditions has resulted in expert opin-on to limit initial and, in the case of redosing, totaloses of local anesthetics and to avoid epinephrinen subarachnoid block.77
There are drug-specific examples of local anes-hetic neurotoxicity. For instance, 2-chloroprocaineas implicated in neurotoxicity following sub-
rachnoid injection of large doses intended for thepidural space. Previous experimental studies sug-ested that 2-chloroprocaine toxicity was related tots formulated acidity and bisulfite preservative.78,79
ecent animal studies challenge this concept by dem-nstrating neurotoxicity from 2-chloroprocaine itselfnd a possible neuroprotective effect of bisulfite.80
hese issues take on increased importance with theontemporary revival of 2-chloroprocaine as a spi-al anesthetic agent.81 The relative potency of-chloroprocaine and lidocaine are similar; bothrugs exhibit similar neurotoxicity in animal mod-ls.80 This suggests that 2-chloroprocaine shouldave a safety profile similar to lidocaine, providedhat both drugs are administered at or below theirecommended maximum subarachnoid doses (60g to 100 mg for lidocaine,77 40 mg to 50 mg for
-chloroprocaine82,83).Spinal lidocaine is consistently more neurotoxic
han bupivacaine in animal models.70,84 Indirectlinical evidence suggests that this may also be truen humans. In the French SOS study, the incidencef neurologic complications associated with spinalnesthesia was over 6-fold higher with lidocainehan with bupivacaine. Consistent with the theoryhat mechanical damage increases the potential foreurotoxicity, those patients with longer durationymptoms were more likely to have experienced aaresthesia or pain on injection during the spinalnesthetic. Furthermore, persistent deficit wasore often associated with high normal (75 mg to
00 mg) doses of lidocaine.25
In summary, neuraxial local anesthetics, opioids,djuvants, and preservatives in clinically recom-ended doses are remarkably safe in the vast ma-
ority of patients.85 Nevertheless, a patient mayarely be vulnerable to local anesthetic and adju-ant neurotoxicity even in “normal” clinical situa-ions. Clinical evidence comes from case reports ofeuraxis injury in patients who received standardoses of neuraxial local anesthetic with or withoutdjuvant,86 or patients who sustained neuraxis in-ury following spinal or epidural anesthesia in
hom neurotoxicity was the presumed mecha-
ism of injury.1,19,25 Neurotoxicity is more likelyo occur in conjunction with physical disruptionf the spinal cord-blood barrier by needle or cath-ter trauma, or from iatrogenic conditions leadingo maldistribution and overdosing of neuraxialocal anesthetics.
ummary
The pathophysiology of neuraxis injury associ-ted with regional anesthesia and pain medicinerocedures presumes that a mechanical, vascular,eurotoxic or a combination insult has occurred.ith the exception of epidural hematoma or ab-
Table 1. Recommendations: Factors That May LimitNeuraxial Injury
Anatomic Factors● Misidentification of vertebral level, unrecognized lateral
needle placement or deviation, abnormal caudad terminationof the spinal cord or failure of the ligamentum flavum to fusein the midline may contribute to direct needle injury to thespinal cord. Clinicians are advised to be aware of theseanatomic conditions, particularly in patients with challengingsurface anatomy. (Class I)
● Surgical positioning and specific space-occupying extradurallesions (e.g., severe spinal stenosis, epidural lipomatosis,ligamentum flavum hypertrophy, or ependymoma) havebeen associated with temporary or permanent spinal cordinjury in conjunction with neuraxial regional anesthetictechniques. These conditions are particularly relevant whenthey co-exist with an epidural hematoma or abscess.Awareness of these conditions should prompt considerationof risk-versus-benefit when contemplating neuraxial regionalanesthetic techniques. (Class II)
● Patients with known tumor in the epidural space shouldundergo neuraxial imaging studies to define the extent oftumor mass. If the tumor is close to the planned site ofepidural solution injection, alternative methods of anesthesiaor analgesia should be considered. (Class II)
● For patients receiving neuraxial injection for treatment ofpain (e.g., cervical epidural injection of steroids via aninterlaminar route) radiologic imaging studies such as CT orMRI should be used to assess the dimensions of the spinalcanal and this information should be considered in theoverall risk-to-benefit analysis as well as guiding theselection of the safest level for entry. (Class II)
Physiologic Factors● Clinicians are advised to be aware of and to avoid
conditions that have been linked to the formation of epiduralhematoma or epidural abscess, as noted in previous ASRAPractice Advisories. Such conditions include concurrent orimminent anticoagulation, the use of multiple anticoagulants,improper aseptic technique, and needle placement duringuntreated active infection. (89-93) (Class I)
● When neuraxial anesthesia is complicated by thedevelopment of mass lesions within the spinal canal (e.g.,hematoma or abscess) resultant postoperative neurologiccomplications may be more likely or more severe in patientswith preexisting severe spinal stenosis or other obstructivespinal canal pathology. (Class I)
● Warning signs such as paresthesia or pain on injection oflocal anesthetic inconsistently herald needle contact with thespinal cord. (Class I)
● Initial dosing or re-dosing of subarachnoid local anestheticin excess of the maximum recommended dose mayincrease the risk of spinal cord or spinal nerve root
neurotoxicity and should be avoided. (Class I)
samIutiiaai
R
ttfiAsGtaomeroacsRamgca
aatrv
1
1
1
1
1
1
1
Spinal Cord Injury • Neal 431
cess, the linkage of patient injury to a specificnesthetic procedure or perioperative event isostly one of association rather than causation.
mportantly, many of the factors that may contrib-te to neuraxis injury cannot be identified prospec-ively,2 which suggests that a large portion of thesenjuries is unpreventable. Fortunately, after exclud-ng relatively rare conditions such as hematoma orbscess, neuraxis injuries associated with regionalnesthesia or pain medicine procedures are exceed-ngly rare.
ecommendations
The strength of scientific evidence that is usedo arrive at these Practice Advisory recommenda-ions is not easily measured by traditional strati-cation methodologies such as the United Statesgency for Health Care Policy and Research
cheme for ranking Statements of Evidence andrades of Recommendation.87 Because of the ex-
reme rarity of the specific complications that areddressed in this manuscript, traditional method-logies such as randomized controlled trials,eta-analysis, or large human case series rarely
xist and are unlikely to exist in the future. Ourecommendations are therefore based on meth-dologies that are necessarily less robust, such asnatomic or pathophysiologic studies of humanadavers or animals, nonrandomized trials, retro-pective series, case reports, or expert opinion.ecommendations from this Practice Advisoryre based on a grading scheme that has beenodified from an American College of Cardiolo-
y/American Heart Association construct thatlassifies the strength of guidelines for perioper-tive cardiac evaluation (Appendix 1).These recommendations are intended to encour-
ge optimal patient care, but cannot ensure thevoidance of adverse outcomes. As with any prac-ice advisory recommendation, these are subject toevision as knowledge of specific complications ad-
Appendix 1. Strength of Recommendations
Classification
I Animal and/or human evidence, and/orgeneral agreement of expert opinion,support the effectiveness andusefulness of the recommendation.
II The weight of conflicting evidence and/orthe weight of expert opinion support theusefulness of the recommendation.
III The usefulness of the recommendation islimited by absent or conflicting evidenceand/or divergent expert opinion.
ances (Table 1).
References
1. Lee LA, Posner KL, Domino KB, Caplan RA, CheneyFW. Injuries associated with regional anesthesia inthe 1980s and 1990s: a closed claims analysis. Anes-thesiology 2004;101:143-152.
2. Moen V, Dahlgren N, Irestedt L. Severe neurologicalcomplications after central neuraxial blockades in Swe-den 1990-1999. Anesthesiology 2004;101:950-959.
3. Kim J, Bahk J, Sung J. Influence of age and sex onthe position of the conus medullaris and Tuffier’s linein adults. Anesthesiology 2003;99:1359-1363.
4. Broadbent CR, Maxwell WB, Ferrie R, Wilson DJ,Gawne-Cain M, Russell R. Ability of anaesthetists toidentify a marked lumbar interspace. Anaesthesia 2000;55:1122-1126.
5. Hogan QH. Epidural anatomy examined by cryomi-crotome section. Influence of age, vertebral level, anddisease. Reg Anesth 1996;21:395-406.
6. Lirk P, Kolbitsch C, Putz G, Colvin J, Colvin HP,Lorenz I, Keller C, Kirchmair L, Rieder J, Moriggi B.Cervical and high thoracic ligamentum flavum fre-quently fails to fuse in the midline. Anesthesiology2003;99:1387-1390.
7. Absalom AR, Martinelli G, Scott NB. Spinal cord in-jury caused by direct damage by local anaestheticinfiltration needle. Br J Anaesth 2001;87:512-515.
8. Reynolds F. Damage to the conus medullaris follow-ing spinal anaesthesia. Anaesthesia 2001;56:238-247.
9. Benumof JL. Permanent loss of cervical spinal cordfunction associated with interscalene block per-formed under general anesthesia. Anesthesiology 2000;93:1541-1544.
0. Hamandi K, Mottershead J, Lewis T, Ormerod IC,Ferguson IT. Irreversible damage to the spinal cordfollowing spinal anesthesia. Neurology 2002;59:624-626.
1. Kao M-C, Tsai S-K, Tsou M-Y, Lee H-K, Guo W-Y, HuJS. Paraplegia after delayed detection of inadvertentspinal cord injury during thoracic epidural catheteriza-tion in an anesthetized elderly patient. Anesth Analg2004;99:580-583.
2. Neal JM, Rathmell JP. Complications in Regional Anes-thesia and Pain Medicine. New York: Elsevier Science;2007.
3. Rathmell JP, April C, Bogduk N. Cervical transfo-raminal injection of steroids. Anesthesiology 2004;100:1595-1600.
4. Selander D, Sjostrand J. Longitudinal spread of intra-neurally injected local anesthestics. An experimentalstudy of the initial neural distribution following in-traneural injections. Acta Anaesthesiol Scand 1978;22:622-634.
5. Jacob AK, Borowiec JC, Long TR, Brown MJ, Ryd-berg CH, Wass T. Transient profound neurologic def-icit associated with thoracic epidural analgesia in anelderly patient. Anesthesiology 2004;101:1470-1471.
6. Krane EJ, Dalens BJ, Murat I, Murrell D. The safetyof epidurals placed during general anesthesia. Reg
Anesth Pain Med 1998;23:433-438.
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
432 Regional Anesthesia and Pain Medicine Vol. 33 No. 5 September–October 2008
7. Tripathi M, Nath SS, Gupta RK. Paraplegia after in-tracord injection during attempted epidural steroidinjection in an awake-patient. Anesth Analg 2005;101:1209-1211.
8. Tsui BCH, Armstrong K. Can direct spinal cord injuryoccur without paresthesia? A report of delayed spinalcord injury after epidural placement in an awakepatient. Anesth Analg 2005;101:1212-1214.
8a.Pong RP, Gmelch BS, Bernards CM. Does a paresthe-sia during spinal needle insertion indicate intrathecalneedle placement? Reg Anesth Pain Med 2008;33:inpress.
9. Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B,Samii K. Serious complications related to regionalanesthesia. Results of a prospective survey in France.Anesthesiology 1997;87:479-486.
0. Huntoon MA, Hurdle M-FB, Marsh RW, Reeves RK.Intrinsic spinal cord catheter placement: implicationsof new intractable pain in a patient with a spinal cordinjury. Anesth Analg 2004;99:1763-1765.
1. Kumar R, Berger RJ, Dunsker SB, Keller JT. Inner-vation of the spinal dura: myth or reality? Spine1996;21:18-26.
2. van den Berg AA, Sadek M, Swanson S, Ghatge S.Epidural injection of lidocaine reduces the responseto dural puncture accompanying spinal needle inser-tion when performing combined spinal-epidural an-esthesia. Anesth Analg 2005;101:882-885.
2a.Brull R, McCartney CJL, Chan VWS, Liguori GA,Hargettt MJ, Xu D, Abbas S, El-Beheiry H. Disclosureof risks associated with regional anesthesia: A surveyof academic regional anesthesiologists. Reg AnesthPain Med 2007;32:7-11.
2b.Domino KB. Informed consent for regional anesthe-sia: What is necessary? (editorial). Reg Anesth PainMed 2007;32:1-2.
3. Horlocker TT, McGregor DG, Matsushige DK, Schr-oeder DR, Besse JA. A retrospective review of 4767consecutive spinal anesthetics: central nervous sys-tem complications. Anesth Analg 1997;84:578-584.
4. Horlocker TT, Wedel DJ. Neurologic complications ofspinal and epidural anesthesia. Reg Anesth Pain Med2000;25:83-98.
5. Auroy Y, Benhamou D, Bargues L, Ecoffey C, FalissardB, Mercier F, Bouaziz H, Samii K. Major complicationsof regional anesthesia in France. The SOS regional an-esthesia hotline service. Anesthesiology 2002;97:1274-1280.
6. Horlocker TT, Abel MD, Messick JM, Schroeder DR.Small risk of serious neurologic complications relatedto lumbar epidural catheter placement in anesthe-tized patients. Anesth Analg 2003;96:1547-1552.
7. Giaufre E, Dalens B, Gombert A. Epidemiology andmorbidity of regional anesthesia in children: a one-year prospective survey of the French-Language So-ciety of Pediatric Anesthesiologists. Anesth Analg1996;83:904-912.
8. Ho AMH, Dion PW, Karmaker MK, Lee A. Estimatingwith confidence the risk of rare adverse events, in-cluding those with observed rates of zero. Reg Anesth
Pain Med 2002;27:207-210.8a.Kil HK, Cho JE, Kim WO, Koo BN, Han SW, Kim JY.Prepuncture ultrasound-measured distance: An ac-curate reflection of epidural depth in infants andchildren. Reg Anesth Pain Med 2007;32:102-106.
9. Buffington CW, Nystrom EUM. Hydrodynamics ofthe spinal epidural space in pigs determined by con-stant-flow methods. Reg Anesth Pain Med 2006;31:100-104.
0. Usubiaga JE, Wikinski JA, Usubiaga LE. Epidural pres-sure and its relation to spread of anesthetic solutions inepidural space. Anesth Analg 1967;46:440-446.
1. Hogan Q. Distribution of solution in the epiduralspace: examination by cryomicrotome section. RegAnesth Pain Med 2002;27:150-156.
2. Peng P, Massicotte EM. Spinal cord compressionfrom intrathecal catheter-tip inflammatory mass:case report and a review of etiology. Reg Anesth PainMed 2004;29:237-242.
3. Shields DC, Palma C, Khoo LT, Ferrante FM. Ex-tramedullary intrathecal catheter granuloma adher-ent to the conus medullaris presenting as cauda equiasyndrome. Anesthesiology 2005;102:1059-1061.
4. Graham GP, Dent CM, Mathews P. Paraplegia follow-ing spinal anaesthesia in a patient with prostatic me-tastases. Br J Urol 1992;70:445-452.
5. Guegan Y, Fardoun R, Launois B, Pecker J. Spinalcord compression by extradural fat after prolongedcorticosteroid therapy. J Neurosurg 1982;56:267-269.
6. Beloeil H, Albaladejo P, Hoen S, Eschwege P, Ben-hamou D. Bilateral lower limb hypoesthesia after rad-ical prostatectomy in the hyperlordotic position undergeneral anesthesia. Can J Anaesth 2003;50:653-656.
7. Hirabayashi Y, Saitoh K, Fukuda H, Igarashi T,Shimizu R, Seo N. Magnetic resonance imaging ofthe extradural space of the thoracic spine. Br J An-aesth 1997;79:563-566.
8. Eastwood DW. Anterior spinal artery syndrome afterepidural anesthesia in a pregnant diabetic patientwith scleroderma. Anesth Analg 1991;73:90-91.
9. Jaeger M, Rickels E, Schmidth A, Sami M, Blomer U.Lumbar ependymoma presenting with paraplegiafollowing attempted spinal anaesthesia. Br J Anaesth2002;88:438-440.
0. Hirabayashi Y, Igarashi T, Suzuki H, Fukuda H, SaitohK, Seo N. Mechanical effects of leg position on vertebralstructures examined by magnetic resonance imaging.Reg Anesth Pain Med 2002;27:429-432.
1. Wills JH, Wiesel S, Abram SE, Rupp FW. Synovial cystsand the lithotomy position causing cauda equina syn-drome. Reg Anesth Pain Med 2004;29:234-236.
2. Bhuiyan MS, Mallick A, Parsloe M. Post-thoracot-omy paraplegia coincident with epidural anaesthesia.Anaesthesia 1998;53:583-586.
3. Dahlgren N, Tornebrandt K. Neurological complica-tions after anaesthesia. A follow-up of 18,000 spinaland epidural anaesthetics performed over threeyears. Acta Anaesthesiol Scand 1995;39:872-880.
4. Vandermeulen EP, Van Aken H, Vermylen J. Anti-coagulants and spinal-epidural anesthesia. Anesth
Analg 1994;79:1165-1177.
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
6
7
7
7
Spinal Cord Injury • Neal 433
5. Horlocker TT, Wedel DJ, Benzon H, Brown DL, Ennek-ing FK, Heit JA, Mulroy MF, Rosenquist RW, Rowling-son J, Tryba M, Yuan C-S. Regional anesthesia in theanticoagulated patient: defining the risks (the secondASRA consensus conference on neuraxial anesthesiaand anticoagulation). Reg Anesth Pain Med 2003;28:172-197.
6. Tureen L. Circulation of the spinal cord and the effectof vascular occlusion. Res Nerv Ment Disc Proc 1938;18:394-437.
6a.Huntoon MA. Anatomy of the cervical intervertebralforamina: vulnerable arteries and ischemic neuro-logic injuries after transforaminal epidural injections.Pain 2005;117:104-111.
6b.Hoeft MA, Rathmell JP, Monsey RD, Fonda BJ. Cer-vical transforaminal injection and the radicular ar-tery: Variation in anatomical location within the cer-vical intervertebral foramina. Reg Anesth Pain Med2006;31:270-274.
7. Biglioli P, Roberto M, Cannata A, Parolari A, FumeroA, Grillo F, Maggioni M, Coggi G, Spirito R. Upperand lower spinal cord blood supply: the continuity ofthe anterior spinal artery and the relevance of thelumbar arteries. J Thorac Cardiovasc Surg 2004;127:1188-1192.
8. Alleyne CH, Cawley CM, Shengelaia GG, Barrow D.Microsurgical anatomy of the artery of Adamkiewiczand its segmental artery. J Neurosurg 1998;89:791-795.
9. Hoy K, Hansen ES, He S-Z, Soballe K, Henriksen TB,Kjolseth D, Hjortdal V, Bunger C. Regional bloodflow, plasma volume, and vascular permeability inthe spinal cord, the dural sac, and lumbar nerveroots. Spine 1994;19:2804-2811.
0. Morishita K, Murakamik G, Fujisawa Y, KawaharadaN, Fukada J, Saito T, Abe T. Anatomical study ofblood supply to the spinal cord. Ann Thorac Surg2003;76:1967-1971.
1. Sliwa JA, Maclean IC. Ischemic myelopathy: a reviewof spinal vasculature and related clinical syndromes.Arch Phys Med Rehabil 1992;73:365-371.
2. Kobrine AI, Doyle TF, Martins AN. Autoregulation ofspinal cord blood flow. Clin Neurosurg 1975;22:573-581.
3. Hickey R, Albin MS, Bunegin L, Gelineau J. Auto-regulation of spinal cord blood flow: is the cord amicrocosm of the brain? Stroke 1986;17:1183-1189.
4. Mitchell P, Goad R, Erwin CW, Camporesi EM, MoonRE, Watkins WD, Bennett PB. Effect of epidural li-docaine on spinal cord blood flow. Anesth Analg 1989;68:312-317.
5. Kuroda Y, Sakabe T, Nakakimura K, Oshita S,Maekawa T, Ishikawsa T, Takeshita H. Epidural bu-pivacaine suppresses local glucose utilization in thespinal cord and brain of rats. Anesthesiology 1990;73:944-950.
6. Cole DJ, Lin DM, Drummond JC, Shapiro HM. Spinaltetracaine decreases central nervous system metabo-lism during somatosensory stimulation in the rat. CanJ Anaesth 1990;37:231-237.
7. Crosby G. Local spinal cord blood flow and glucoseutilization during spinal anesthesia with bupivacaine
in conscious rats. Anesthesiology 1985;63:55-60.8. Dohi S, Takeshima R, Naito H. Spinal cord blood flowduring spinal anesthesia in dogs: the effects of tetra-caine, epinephrine, acute blood loss, and hypercap-nia. Anesth Analg 1987;66:599-606.
9. Tsuji T, Matsuyama Y, Sato K, Iwata H. Evaluation ofspinal cord blood flow during prostaglandin E1-in-duced hypotension with power Doppler ultrasonog-raphy. Spinal Cord 2001;39:31-36.
0. Brown DL, Rorie DK. Altered reactivity of isolatedsegmental lumbar arteries of dogs following exposureto ethanol and phenol. Pain 1994;56:139-143.
1. Lo JN, Buckley JJ. Spinal cord ischemia. A complicationof celiac plexus block. Reg Anesth 1982;7:66-68.
2. Wong GY, Brown DL. Transient paraplegia follow-ing alcohol celiac plexus block. Reg Anesth 1995;20:352-355.
2a.Benzon HT, Chew TL, McCarthy R, Benzon HA,Walega DR. Comparison of the particle sizes of thedifferent steroids and the effect of dilution: A reviewof the relative neurotoxicities of the steroids. Anes-thesiology 2007;106:331-338.
3. Nedeltchev K, Loher TJ, Stepper F, Arnold M,Schroth G, Mattle HP, Sturzenegger M. Long-termoutcome of acute spinal cord ischemia syndrome.Stroke 2004;35:560-565.
4. Sharrock NE, Ranawat CS, Urquhart B, Peterson M.Factors influencing deep vein thrombosis followingtotal hip arthroplasty under epidural anesthesia.Anesth Analg 1993;76:765-771.
5. Bernard JM, Passuti N, Pinaud M. Long-term hypo-tensive technique with nicardipine and nitroprussideduring isoflurane anesthesia for spinal surgery.Anesth Analg 1992;75:179-185.
6. Sum DC, Chung PC, Chen WC. Deliberate hypoten-sive anesthesia with labetalol in reconstructive sur-gery for scoliosis. Acta Anaesthesiol Scand 1996;34:203-207.
7. Neal JM. Effects of epinephrine in local anestheticson the central and peripheral nervous systems: neu-rotoxicity and neural blood flow. Reg Anesth Pain Med2003;28:124-134.
8. Edvinsson L, MacKenzie ET, McCulloch J. Cerebralblood flow and metabolism. In: ed. New York: RavenPress; 1993:202-210.
9. Takenami T, Yagishita S, Murase S, Hiruma H,Kawakami T, Hoka S. Neurotoxicity of intrathecallyadministered bupivacaine involves the posteriorroots/posterior white matter and is milder than lido-caine in rats. Reg Anesth Pain Med 2005;30:464-72.
0. Lambert LA, Lambert DH, Strichartz GR. Irreversibleconduction block in isolated nerve by high concen-trations of local anesthetics. Anesthesiology 1994;80:1082-1093.
1. Drasner K, Sakura S, Chan VW, Bollen AW, CirialesR. Persistent sacral sensory deficit induced by intra-thecal local anesthetic in the rat. Anesthesiology 1994;80:847-852.
2. Rigler ML, Drasner K, Krejcie TC, Yelich SJ, T. SF,DeFontes J, Bohner D. Cauda equina syndrome aftercontinuous spinal anesthesia. Anesth Analg 1991;72:
275-281.
7
7
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
9
9
9
9
A
cd
434 Regional Anesthesia and Pain Medicine Vol. 33 No. 5 September–October 2008
3. Rigler MR, Drasner K. Distribution of catheter-in-jected local anesthetic in a model of the subarachnoidspace. Anesthesiology 1991;75:684-692.
4. Ross BK, Coda B, Heath CH. Local anesthetic distri-bution in a spinal model: a possible mechanism ofneurologic injury after continuous spinal anesthesia.Reg Anesth 1992;17:69-77.
5. Hashimoto K, Hampl KF, Nakamura Y, Bollen AW,Feiner J, Drasner K. Epinephrine increases the neu-rotoxic potential of intrathecally administered lido-caine in the rat. Anesthesiology 2001;94:876-881.
6. Kozody R, Palahniuk RJ, Wade JG, Cumming MO.The effect of subarachnoid epinephrine and phenyl-ephrine on spinal cord blood flow. Can Anaesth Soc J1984;31:503-508.
7. Drasner K. Lidocaine spinal anesthesia. A vanishingtherapeutic index? Anesthesiology 1997;87:469-472.
8. Gissen AJ, Datta S, Lambert DH. The chloroprocainecontroversy I. Hypothesis to explain the neural com-plication of chloroprocaine epidural. Reg Anesth 1984;9:124-134.
9. Gissen AJ, Datta S, Lambert DH. The chloroprocainecontroversy II. Is chloroprocaine neurotoxic? RegAnesth 1984;9:135-145.
0. Taniguchi M, Bollen AW, Drasner K. Sodium bisul-fite: scapegoat for chloroprocaine neurotoxicity? An-esthesiology 2004;100:85-91.
1. Yoos JR, Kopacz DJ. Spinal 2-chloroprocaine for sur-gery: an initial 10-month experience. Anesth Analg2005;100:553-558.
2. Smith KN, Kopacz DJ, McDonald SB. Spinal 2-chlo-roprocaine: a dose-ranging study and the effect ofepinephrine. Anesth Analg 2005;98:81-88.
3. Kopacz DJ. Spinal 2-chloroprocaine: minimum effec-tive dose. Reg Anesth Pain Med 2005;30:36-42.
4. Bainton CR, Strichartz GR. Concentration depen-dence of lidocaine-induced irreversible conductionloss in frog nerve. Anesthesiology 1994;81:657-667.
5. Hodgson PS, Neal JM, Pollock JE, Liu SS. The neu-rotoxicity of drugs given intrathecally (spinal). AnesthAnalg 1999;88:797-809.
6. Gerancher JC. Cauda equina syndrome following a
single spinal administration of 5% hyperbaric lido- ccaine through a 25-gauge Whitacre needle.Anesthesiology 1997;87:687-689.
7. Acute Pain Management: Operative or Medical Proceduresand Trauma. Clinical Practice Guideline No. 1. Rockville,MD: United States Department of Health and HumanServices Agency for Healthcare Policy and Research;1993. No. 92-002:107.
8. Eagle KA, Berger PB, Calkins H, Chaitman BR, EwyGA, Fleischmann KE, Fleisher LA, Froehlich JB, Gus-berg RJ, Leppo JA, Ryan T, Schlant RC, Winters WLJ.ACC/AHA guideline update for perioperative cardio-vascular evaluation for noncardiac surgery: executivesummary: a report of the American College of Car-diology/American Heart Association Task Force onPractice Guidelines (Committee to Update the 1996Guidelines on Perioperative Cardiovascular Evalua-tion for Noncardiac Surgery). J Am Coll Cardiol 2002;39:542-553.
9. Horlocker TT, Wedel DJ, Benzon H, Brown DL, En-neking FK, Heit JA, Mulroy MF, Rosenquist RW,Rowlingson J, Tryba M, Yuan C-S. Regional anesthe-sia in the anticoagulated patient: Defining the risks(The second ASRA consensus conference onneuraxial anesthesia and anticoagulation). Reg AnesthPain Med 2003;28:172-197.
0. Hebl J. Importance and implications of aseptic tech-niques during regional anesthesia. Reg Anesth PainMed 2006;31:311-323.
1. Horlocker T. Regional anesthesia and the immuno-compromised patient. Reg Anesth Pain Med 2006;31:334-345.
2. Rathmell JP. Infectious risks of chronic pain treat-ments. Reg Anesth Pain Med 2006;31:346-352.
3. Wedel DJ. Regional anesthesia in the febrile or in-fected patient. Reg Anesth Pain Med 2006;31:324-333.
ppendix 1
This classification system (Appendix 1) is signifi-antly modified from the American College of Car-iology/American Heart Association construct for
lassifying strength of evidence.88