Embed Size (px)
Citation preview

06.04.16
1
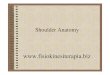
MRI of the shoulder The rotator cuff
Roar Pedersen
Gøteborg, april 2015
Topics
• Anatomy of the cuff
• What is impingement?
• Tendinosis, partial rupture, total rupture
• Calcific tendinopathy • A few words about the biceps tendon
• Pitfalls
• How to report
Anatomy
• Tendons of the rotatorcuff
• Footprint
• Rotator cable
• Biceps tendon

06.04.16
2

06.04.16
3
Impingement
• Extrinsic causes
• Intrinsic factors
– Tendon degeneration, hypovascular critical zone.
• Subcoracoid impingement
Extrinsic causes
• Progressive process caused by extrinsic factors (such as acromial shape and slope, subacromial entesophyte, spur
at insertion of coracohumeral ligament) (Neer):
– Bursitis with subacromial edema and hemorrhage
– Tendinosis of rotatorcuff
– Stress on fibers in rotator cuff; • Partial thickness tear
• Progress to full thickness tear
Clinical diagnosis of impingement
• Pain over deltoid made worse by resisted
abduction
• Neer and Hawkins test, and others
• Overall accuracy for diagnosis of FTT of STT
– Neer: 51.8 %
– Hawkins: 56.1 %
Imaging of impingement • Etiology or results of impingement:
– Osteoarthritis ACJ: inferior osteophyte, acromial
entesophyte.
– Coracoacromial ligament: spur formation, thickening
– Acromial morphology: 2 sections away from joint
– Subacromial bursitis
– Tendon pathology: tendinosis, tears, calcification

06.04.16
4
Tendinosis
• Most important finding: Thickened tendon
with high signal!
• Do not overcall tendinosis
• Can be a result of wear/tear, impingement
• Important to rule out partial or total RC tear
Tendinosis

06.04.16
5
Tendinosis / tendinopathy
• Usually supraspinatus, less often infraspinatus or subscapularis
• +/-‐ subdeltoid bursitis
• High signal T2/PD, but not as high as fluid
• Pitfalls: Magic angle, partial tear Magic angle
Tendinosis

06.04.16
6
Rupture of the RC – some facts
• SS is most often affected, in the middle and posterior part of the
tendon
• Rupture of SS in the anterior part more often lead to muscular atrophy
• It may be difficult to decide if the rupture is in IS or SS, or both at the
transitional zone
• Rupture of SSc is probably underdiagnosed (1/3 of RC ruptures).
Rupture of middle and lower parts may be difficult to see by
arthroscopy.
• Discrepancy between clinical symptoms and findings! Large ruptures
may be asymptomatic. Bursitis may elicit symptoms.
Partial rupture
• Articular side 2-‐3x >> bursal side – Prognosis worse with larger tears and atraumatic presentation
– Rim rent/PASTA/PAINT
• Intratendinous partial tear is common!
– Delamination of fibers, may lead to articular sided tears
– May develop synovial lining, inhibits healing
• Bursal tears often associated with impingement, are more
often symptomatic, often at bone-‐tendon interface
Par-al, ar-cular sided rupture of supraspinatus

06.04.16
7
Par-al bursal sided rupture of supraspinatus
Bursal sided tear… or full thickness tear? Look for:
• The footprint!
• The tendon signal!
• Fluid signal!
• Cystic collections!
• The surface!
• Cysts of the anterior tuberculum majus!

06.04.16
8
RIM RENT
Full thickness rupture
• Easier to identify
– Focal area of discontinuity, from joint to bursa
– Small (<1cm), medium (3-‐5), massive (>5)
– Large tears extend into IS or SSc, may see
degeneration of long head of biceps
• Sensitivity of MRI: 84-‐96%
Total rupture of Supraspinatus

06.04.16
9
Remember!
• Parts of the tendon may be intact!
• Describe retraction, atrophy of the
muscle, tendinosis!
Subscapularis
• Subcoracoid impingement – does it exist?
• Isolated rupture is rare
• Usually tears are superior and lateral, articular
sided
Subscapular rupture a@er trauma

06.04.16
10
Isolated total ruptur of subscapular tendon – hanging from arm
after trauma
Total rupture subscapular tendon
Total subscapular rupture, medial luxation of biceps
Calcific tendinopathy
• Calcification of the tendon and soft tissue may be
difficult to identify on MRI
• May be asymptomatic
• May contribute to impingement
• Usually SS, but may occur in all tendons
• Inflammation, erosion, cysts in caput may be severe
and confusing

06.04.16
11
Calcific tendinopathy-‐ severe calcifica-on
Unusual location
Calcific tendinopathy
Calcific tendinopathy with severe inflammation

06.04.16
12
A few words about biceps

06.04.16
13
Pitfalls for the more advanced
• Scar or granulation tissue
• The rotator cable
Scar tissue
• Some tears are relatively low signal on T2
• This makes MR interpretation difficult
• Other signs may give the diagnosis: change in signal or
contour, retraction of fibers, fatty atrophy
• Scar tissue may be impenetrable for fluid/contrast,
and may even appear as normal tendon at arthroscopy
1. Photo courtesy of Thomas Dovan, MD. Elite Orthopaedics and Sports Medicine, Nashville, TN. By permission from RadSource.
Scar tissue Rotator cable

06.04.16
14
Rotator cable • Report: – Impingement:
• AC-‐joint, entesophytes, osteophytes, os acromiale,
calcification, acromion, bursa.
– Partial tear: • articular, bursal, intraarticular, size of the tear, footprint.
– Full thickness tear: • the entire tendon?, measure retraction, tendinosis, atrophy.
Summary
• Anatomy
• Impingement
• Tendinopathy
• Partial tear
• Full thickness tear
• Subscapularis
• Calcific tendinopathy
• Pitfalls – scar tissue, rotator cable
• Reporting